
Clinical profile and prognostic value of low systolic blood
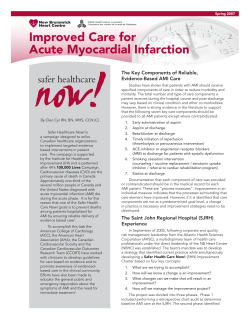
Clinical profile and prognostic value of low systolic blood pressure in patients hospitalized for heart failure with reduced ejection fraction: Insights from the Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST) trial Andrew P. Ambrosy, MD, a,i Muthiah Vaduganathan, MD, MPH, b,i Robert J. Mentz, MD, c,i Stephen J. Greene, MD, d,i Haris Subačius, MA, e,i Marvin A. Konstam, MD, f,i Aldo P. Maggioni, MD, g,i Karl Swedberg, MD, h,i and Mihai Gheorghiade, MD d,i Stanford, CA; Boston, MA; Durham, NC; Chicago, IL; Florence, Italy; and Göteborg, Sweden rC DR Background Systolic blood pressure (SBP) is related to the pathophysiologic development and progression of heart failure (HF) and is inversely associated with adverse outcomes during hospitalization for HF (HHF). The prognostic value of SBP after initiating inhospital therapy and the mode of death and etiology of cardiovascular readmissions based on SBP have not been well characterized in HHF. Methods or ia za da po A post hoc analysis was performed of the placebo group (n = 2061) of the EVEREST trial, which enrolled patients within 48 hours of admission for worsening HF with an ejection fraction (EF) ≤40% and an SBP ≥90 mm Hg, for a median followup of 9.9 months. Systolic blood pressure was measured at baseline, daily during hospitalization, and at discharge/day 7. Patients were divided into the following quartiles by SBP at baseline: ≤105, 106 to 119, 120 to 130, and ≥131 mm Hg. Outcomes were all-cause mortality (ACM) and the composite of cardiovascular mortality or HHF (CVM + HHF). The associations between baseline, discharge, and inhospital change in SBP and ACM and CVM + HHF were assessed using multivariable Cox proportional hazards regression models adjusted for known covariates. Co pi aa ut Results Median (25th, 75th) SBP at baseline was 120 (105, 130) mm Hg and ranged from 82 to 202 mm Hg. Patients with a lower SBP were younger and more likely to be male; had a higher prevalence of prior revascularization and ventricular arrhythmias; had a lower EF, worse renal function, higher natriuretic peptide concentrations, and wider QRS durations; and were more likely to require intravenous inotropes during hospitalization. Lower SBP was associated with increased mortality, driven by HF and sudden cardiac death, and cardiovascular hospitalization, primarily caused by HHF. After adjusting for potential confounders, SBP was inversely associated with risk of the coprimary end points both at baseline (ACM: hazard ratio [HR]/10-mm Hg decrease 1.15, 95% CI1.08-1.22; CVM + HHF: HR 1.09/10-mm Hg decrease, 95% CI 1.04-1.14) and at the time of discharge/day 7 (ACM: HR 1.15/10-mm Hg decrease, 95% CI 1.08-1.22; CVM + HHF: HR 1.07/10-mm Hg decrease, 95% CI 1.02-1.13), but the association with inhospital SBP change was not significant. Conclusion Systolic blood pressure is an independent clinical predictor of morbidity and mortality after initial therapy during HHF with reduced EF. (Am Heart J 2013;165:216-25.) Heart failure (HF) is a public health problem of pandemic proportions with a prevalence of 5.7 million, incidence of 670,000 new cases/y, and an annual hospitalization for HF (HHF) rate in excess of 1 million in the United States alone. 1,2 Blood pressure (BP) is a complex and dynamic clinical variable that must be From the aDepartment of Medicine, Stanford University School of Medicine, Stanford, CA, b Department of Medicine, Massachusetts General Hospital, Boston, MA, cDivision of Cardiology, Duke University Medical Center, Durham, NC, dCenter for Cardiovascular Randomized controlled trial registration no. NCT00071331. Javed Butler, MD, MPH, served as guest editor for this article. Submitted September 27, 2012; accepted November 26, 2012. Innovation, Northwestern University Feinberg School of Medicine, Chicago, IL, eDivision of Cardiology, Department of Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, fDivision of Cardiology, Department of Medicine, Tufts Medical Center, Boston, MA, gANMCO Research Center, Florence, Italy, and hDepartment of Molecular and Clinical Medicine, Sahlgrenska Academy, University of Gothenburg, Göteborg, Sweden. j On behalf of the EVEREST trial investigators. Reprint requests: Mihai Gheorghiade, MD, Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, 645 North Michigan Ave, Suite 1006, Chicago, IL 60611. E-mail: m-gheorghiade@northwestern.edu 0002-8703/$ - see front matter © 2013, Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.ahj.2012.11.004 04/04/2014 American Heart Journal Volume 165, Number 2 Ambrosy et al 217 with the Declaration of Helsinki, the protocol was independently approved by the institutional review board or ethics committee at each participating center, and written informed consent was obtained from all participants. The present analysis includes only those patients randomized to the placebo arm of the EVEREST trial because of the unclear effects of the study drug on SBP. Blood pressure measurements and laboratory testing rC DR Blood pressure measurements were taken in a supine position. Baseline SBP was defined as SBP at the time of randomization. For patients with missing baseline SBP measurements, the earliest measurement recorded up to 4 days postenrollment was substituted because very little change in SBP occurred after the first day. Patients with missing baseline measurements (n = 9) were excluded from all subsequent analyses. Discharge SBP was defined as SBP on inhospital day 7 or discharge, whichever occurred first. For patients with missing discharge SBP measurements, the latest inhospital SBP measurement was substituted. Change in SBP was defined as the difference between SBP at baseline and discharge/day 7; analyses excluded patients who died during hospitalization. Everest end points da po An independent and blinded adjudication committee determined the cause of all hospitalizations and deaths during follow-up. Rehospitalization was defined as a nonelective hospital admission for medical therapy with a duration that extended over a change in calendar date. Hospitalization for HF was defined as admission that included substantive worsening of symptoms and/or signs resulting in augmentation of oral medications or new administration of intravenous therapies or ultrafiltration. Mode of death was adjudicated as CV, non-CV, or unknown. Cardiovascular deaths were further classified as sudden cardiac death (SCD), HF death, acute myocardial infarction (AMI), stroke, or other. Non-CV death was defined as a death caused by a specific non-CV event, whereas unknown death was defined as a death for which no information surrounding the event was available. Prespecified coprimary end points were all-cause mortality (ACM) and the composite of CV mortality (CVM) or HHF (CVM + HHF). Each of the coprimary end points was analyzed as time to first event. Study overview aa Methods ut or ia za interpreted in the context of current disease status (ie, acute vs chronic), overall progression (ie, early vs endstage), and concurrent medical therapies (ie, vasodilators, inotropes, etc). 3 In the ambulatory setting, chronically uncontrolled hypertension has a well-established role in the development and progression of HF. 4 In contrast, registries enrolling patients during HHF have demonstrated that approximately 50% of patients have a systolic BP (SBP) greater than or equal to 140 mm Hg at admission and higher measurements confer a graded protective effect on mortality even at extremes of SBP. 5–7 However, the pathophysiologic significance and prognostic value of SBP after the initiation of inhospital therapy have not been well described. In addition, SBP-related differences in the cause of postdischarge death and cardiovascular (CV)-related readmissions have not been previously reported during HHF. The EVEREST trial provides an opportunity to characterize the baseline clinical features and outcomes by SBP after initiation of inhospital therapy in a large contemporary cohort of patients enrolled during HHF with reduced ejection fraction (EF). Specifically, the objectives of this post hoc analysis of the EVEREST clinical trial database were to (1) describe the profile of patients enrolled in a clinical trial presenting with low SBP in the absence of cardiogenic shock, (2) determine the breakdown of the mode of death and etiology of CV readmissions, and (3) evaluate the association of SBP after initial therapy with subsequent morbidity and mortality. Co pi The study design 8 and primary results 9,10 of the EVEREST trial have been previously reported. Briefly, EVEREST was a global, prospective, randomized, double-blind, placebo-controlled trial designed to examine the short- and long-term efficacy and safety of tolvaptan, a vasopressin-2 receptor antagonist. Patients ≥18 years of age hospitalized for worsening HF with symptoms classified as New York Heart Association (NYHA) class III or IV, with a left ventricular (LV) EF ≤40%, and presenting with 2 or more signs or symptoms of volume overload (dyspnea, pitting edema, and jugular venous distension [JVD]) were eligible for enrollment. Relevant exclusion criteria included supine SBP b90 mm Hg; hemodynamically significant uncorrected primary cardiac valvular disease; serum creatinine greater than 3.5 mg/ dL or 309.4 μmol/L; subjects currently treated with hemofiltration or dialysis, or refractory, end-stage HF (ie, defined as candidates for ventricular assist devices or continuous positive intravenous inotropic therapy); or a life expectancy of less than 6 months as determined by the enrolling clinician-investigator. Patients were randomized within 48 hours of admission to receive either 30 mg of oral tolvaptan once daily or matching placebo, both in addition to standard therapy, for a minimum of 60 days. Background HF therapy was left to the discretion of the treating physician, but guideline-based recommendations for optimal medical management were included in the study protocol. The EVEREST trial was conducted in accordance Statistical analysis All data were reported as a mean ± SD or a median (interquartile range). Patients were divided into quartiles (Q14) by SBP at baseline: ≤105, 106 to 119, 120 to 130, and ≥131 mm Hg. Baseline and discharge characteristics as well as occurrence of clinical events (ie, mode of death and etiology of CV hospitalizations) were compared across quartiles of SBP using analysis of variance, Kruskal-Wallis, and χ 2 tests, as appropriate. The associations between baseline, discharge, and inhospital change in SBP and ACM and CVM + HHF were assessed as a continuous variable using univariate and multivariable Cox proportional hazards regression models. No evidence of nonlinear effects was observed by Kolmogorov-type supremum testing for all analyses. All multivariable models were adjusted for 20 preselected clinical and laboratory variables: age, sex, geographic region, medical comorbidities (ie, diabetes, hypertension, and renal insufficiency), history of ventricular arrhythmias, EF, serum sodium, B-type natriuretic peptide (BNP)/amino terminal-proBNP, serum blood urea nitrogen 04/04/2014 American Heart Journal February 2013 218 Ambrosy et al Co pi aa ut or ia za da po rC DR Figure 1 Distribution and descriptive statistics of SBP measurements at baseline (A) and inhospital change (B). (BUN), QRS duration, NYHA class, baseline medication use (ie, β-blocker, angiotensin-converting enzyme inhibitors [ACEIs]/angiotensin receptor blockers [ARBs], mineralocorticoid receptor antagonists [MRAs], digoxin, and inotropes), and presence of atrial flutter or fibrillation on baseline electrocardiogram. Hazard ratios (HRs) are presented along with the 95% CIs per 10-mm Hg decrease in baseline, discharge, or inhospital change in SBP. Funding and manuscript preparation Otsuka Inc (Rockville, MD) provided financial and material support for the EVEREST trial. Database management was 04/04/2014 American Heart Journal Volume 165, Number 2 Ambrosy et al 219 Table I. Demographics and clinical characteristics by baseline SBP quartile Q4 131-202 mm Hg (n = 508) P 66 ± 12.6 65.4 ± 11.6 66.8 ± 10.9 .007 418 31 28 385 (87.6) (6.5) (5.9) (80.7) 460 (88) 29 (5.5) 34 (6.5) 382 (73.0) 427 48 33 347 .074 159 (33.3) 178 (37.3) 72 (15.1) 68 (14.3) 264 (50.5) 91 (17.4) 108 (20.7) 60 (11.5) 258 (50.8) 132 (26.0) 63 (12.4) 55 (10.8) b.001 377 (79.4) 238 (50.1) 344 (72.1) 269 (56.4) 106 (22.2) 117 (24.5) 99 (20.8) 24 (5.1) 66 (13.9) 312 (65.4) 254 (53.7) 149 (31.5) 109 (22.9) 92 (19.3) 187 (39.2) 153 (32.1) 54 (11.3) 403 (77.5) 236 (45.5) 373 (71.3) 265 (50.7) 65 (12.4) 82 (15.7) 118 (22.6) 22 (4.3) 59 (11.4) 395 (75.5) 287 (55.1) 105 (20.2) 49 (9.4) 47 (9) 176 (33.7) 107 (20.5) 46 (8.8) 370 (73.3) 230 (45.5) 381 (75.4) 246 (48.6) 68 (13.4) 88 (17.3) 130 (25.6) 24 (4.8) 65 (12.9) 469 (92.3) 251 (49.6) 97 (19.2) 43 (8.5) 40 (7.9) 208 (40.9) 115 (22.6) 42 (8.3) .001 .223 .001 .082 b.001 b.001 .086 .544 .380 b.001 .283 b.001 b.001 b.001 .088 b.001 .155 68.4 ± 8.9 79.3 ± 15.8 179 (37.5) 427 (91.4) 115 (24.9) 396 (84.6) 245 (51.4) 285 (59.7) 26.9 ± 8 28 (20-37.5) 1.3 (1.1-1.7) 126 (102-157) 139.2 ± 4.4 877.5 (416.8-1817.7) 4906.5 (2202-10,076) 75.7 ± 8.8 80 ± 15 215 (41.1) 472 (90.9) 156 (30.2) 414 (79.8) 310 (59.3) 299 (57.2) 28.6 ± 7.4 25 (20-33) 1.2 (1-1.5) 121 (96-144) 140.4 ± 4.5 609.5 (249-1278) 4648.8 (1971.3-8501) 84.2 ± 11.8 80.4 ± 16.4 202 (37.8) 459 (91.1) 107 (21.4) 411 (81.5) 328 (64.6) 267 (52.6) 30.7 ± 7.4 23 (18-31) 1.2 (1-1.5) 108.5 (93-136) 141.1 ± 4.4 599 (245.2-1272.5) 4416.3 (2285.9-10,457.1) b.001 .714 .521 .994 .002 .265 b.001 .015 b.001 b.001 b.001 b.001 b.001 b.001 .930 417 (87.4) 389 (81.6) 341 (71.5) 269 (56.4) 234 (49.1) 193 (40.5) 25 (5.2) 16 (3.4) 100 (21) 191 (40) 463 (88.5) 453 (86.6) 363 (69.4) 292 (55.8) 267 (51.1) 222 (42.4) 18 (3.4) 15 (2.9) 95 (18.2) 164 (31.4) 443 (87.2) 436 (85.8) 338 (66.5) 234 (46.1) 224 (44.1) 242 (47.6) 5 (1) 22 (4.3) 57 (11.2) 159 (31.3) .897 .109 .263 b.001 .142 b.001 b.001 .640 b.001 .002 368 (79.1) 385 (82.8) 343 (73.8) 391 (76.1) 448 (87.2) 381 (74.1) 361 (72.3) 438 (87.8) 380 (76.2) .092 .007 .760 po za ia or aa pi Co rC DR Q3 120-130 mm Hg (n = 523) ut Demographics Age (y), mean ± SD 64.3 ± 12.9 Race White 449 (83.6) Black 39 (7.3) Other 49 (9.1) Male 429 (79.9) Region Eastern Europe 124 (23.1) North America 220 (41.0) South America 99 (18.4) Western Europe 94 (17.5) Medical history HHF 448 (83.6) HL 269 (50.1) CAD 345 (64.2) MI 270 (50.3) PTCA 123 (22.9) CABG 156 (29.1) PVD 103 (19.3) TIA 33 (6.2) Stroke 57 (10.7) HTN 279 (52) Atrial arrhythmias 271 (51) Ventricular Arrhythmias 184 (34.7) PPM 147 (27.4) AICD 115 (21.4) Diabetes mellitus 198 (36.9) Renal insufficiency 182 (34) COPD 63 (11.7) Vital signs and symptoms and laboratory values DBP, mean ± SD 62.1 ± 8.5 HR, mean ± SD 79.5 ± 15.8 NYHA class IV 224 (41.9) Dyspnea 480 (91.3) JVD 160 (30.7) Rales 430 (81.6) Edema 258 (48.2) Murmur 333 (62) EF, mean ± SD 24 ± 8.4 BUN, median (IQR) 29 (21-45) sCr, median (IQR) 1.3 (1.1-1.8) QRS, median (IQR) 130 (104-161) Na, mean ± SD 137.8 ± 5 BNP, median (IQR) 943 (469-1846) NT-proBNP, median (IQR) 5075.9 (2307.1-8923) Admission medications Furosemide 468 (87.2) ACEI/ARB 448 (83.4) β-Blocker 384 (71.5) MRA 329 (61.3) Digoxin 264 (49.2) Nitrates 153 (28.5) Inotrope 49 (9.1) Hydralazine 20 (3.7) Antiarrhythmics 122 (22.7) Lipid-lowering agents 208 (38.7) Discharge medications Furosemide 394 (77) ACEI/ARB 416 (81.3) β-Blocker 376 (73.4) Q2 106-119 mm Hg (n = 477) da Q1 82-105 mm Hg (n = 537) (84.1) (9.5) (6.5) (68.3) b.001 (continued on next page) 04/04/2014 American Heart Journal February 2013 220 Ambrosy et al Table I (continued ) MRA Digoxin Nitrates Inotrope Hydralazine Antiarrhythmics Lipid-lowering agents Q1 82-105 mm Hg (n = 537) Q2 106-119 mm Hg (n = 477) Q3 120-130 mm Hg (n = 523) Q4 131-202 mm Hg (n = 508) P 336 (65.6) 268 (52.3) 116 (22.7) 20 (3.9) 18 (3.5) 114 (22.3) 202 (39.5) 289 (62.2) 231 (49.7) 157 (33.8) 8 (1.7) 18 (3.9) 101 (21.7) 193 (41.5) 314 (61.1) 246 (47.9) 162 (31.5) 8 (1.6) 16 (3.1) 84 (16.3) 180 (35) 277 (55.5) 206 (41.3) 190 (38.1) 0 (0) 23 (4.6) 63 (12.6) 169 (33.9) .011 .004 b.001 b.001 .636 b.001 .043 HL, Hyperlipidemia; CAD, coronary artery disease; MI, myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; CABG, coronary artery bypass graft; PVD, peripheral vascular disease; TIA, transient ischemia attack; HTN, hypertension; PPM, permanent pacemaker; AICD, automated implantable cardioverter-defibrillator; COPD, chronic obstructive pulmonary disease; DBP, diastolic BP; HR, heart rate; sCr, serum creatinine; NT-proBNP, amino terminal-proBNP. Clinical and laboratory variables On examination, patients with a lower SBP were more likely to exhibit JVD or have an audible murmur and less likely to have signs of edema, whereas other signs and symptoms of congestion were comparable across SBP quartiles. Patients with an SBP in the bottom quartile had more renal dysfunction and higher natriuretic peptide concentrations, wider QRS duration, and a lower EF. Results Baseline and discharge medications At baseline, the use of β-blockers and ACEIs/ARBs was similar between SBP quartiles. In contrast, MRAs were more likely to be prescribed to patients with a lower SBP. Patients in the lowest SBP quartile were more likely to receive inotropes, whereas those in the highest quartile tended to more often receive nitrates. Finally, patients in the bottom quartile of SBP were more likely to be taking an antiarrhythmic or lipid-lowering agent. Trends in medication use remained relatively unchanged between baseline and discharge, with the exception that patients with a lower SBP were less likely to be prescribed an ACEI or an ARB at discharge. Co pi aa ut or ia za Participants presented with a median (25th, 75th) baseline SBP of 120 (105, 130) mm Hg ranging from 82 to 202 mm Hg (Figure 1A) and experienced an inhospital change of −5 (−15, 5) mm Hg ranging from −75 to 60 mm Hg (Figure 1B). Study participants had a mean age of 65.6 ± 12.0 years, were predominantly male, and selfidentified their race as white. Most patients had an ischemic etiology of HF, and the mean EF was 27.5% ± 8.2%. Approximately 80% of patients had a history of HHF, and the prevalence of medical comorbidities was high. Patients were well treated with evidence-based therapies including β-blockers, ACEIs/ARBs, and MRAs. da po rC DR performed by the sponsor according to a prespecified plan. H.S. conducted all final analyses for this manuscript, with funding from the Center for Cardiovascular Innovation (Northwestern University Feinberg School of Medicine, Chicago, IL), using SAS version 9.3 (Cary, NC). The authors had full access to the data, take sole responsibility for its integrity, and had complete control and authority over manuscript preparation and the decision to publish. Demographics Patients with a lower SBP were younger and tended to be male (Table I). Although there was no association between baseline SBP and self-identified race, patients with an SBP in the lowest quartile were more frequently enrolled in North America and Western Europe, whereas patients with an SBP in the highest quartile were more commonly enrolled in Eastern Europe. Medical history Patients with a lower SBP were more likely to report a history of HHF. Of note, the prevalence of percutaneous transluminal coronary angioplasty and coronary artery bypass graft was almost twice as high in the bottom quartile compared with the top quartile. History of ventricular arrhythmias and cardioverter-defibrillator implantation was highest in the patient with the lowest SBP. Cause of death and rehospitalization During a median follow-up of 9.9 months, the mortality rate was 26.4% (n = 543) and the CV hospitalization rate was 38.9% (n = 772) for the entire cohort (Table II). There were significant differences in mortality (Q1 38.9% vs Q4 15.9%) and CV hospitalization (Q1 49.9% vs Q4 29.7%) by SBP. Systolic BP–related disparities in mortality were driven by HF and SCD, whereas HHF was the only subset of CV hospitalizations occurring with greater frequency in patients presenting with lower SBP. Predictive value of SBP Kaplan-Meier curves showed increased rates of both coprimary end points, ACM and CVM + HHF, in the lower SBP quartiles at baseline (log-rank test, P b .001; Figure 2) and discharge (log-rank test, P b .001; Figure 3). After adjusting for potential confounders, SBP as a continuous 04/04/2014 American Heart Journal Volume 165, Number 2 Ambrosy et al 221 Table II. Coprimary end points, mode of death, and etiology of CV hospitalization by baseline SBP quartile ACM CVM + HHF Mortality CV HF AMI SCD Stroke Other CV Non-CV Unknown CV hospitalizations CV HHF AMI Arrhythmia Stroke Other CV Q2 106-119 mm Hg (n = 477) Q3 120-130 mm Hg (n = 523) Q4 131-202 mm Hg (n = 508) Total (n = 2045) 209 (38.9) 293 (54.6) 135 (28.3) 215 (45.1) 115 (22.0) 176 (33.7) 81 (15.9) 138 (27.2) 540 (26.4) 822 (40.2) b.001 b.001 145 (28.3) 82 (16.0) 1 (0.2) 53 (10.3) 2 (0.4) 7 (1.4) 22 (4.3) 18 (3.5) 85 (18.3) 43 (9.3) 6 (1.3) 24 (5.2) 3 (0.7) 9 (1.9) 20 (4.3) 17 (3.7) 76 (14.9) 33 (6.5) 5 (1.0) 30 (5.9) 0 (0.0) 8 (1.6) 16 (3.1) 10 (2.0) 49 (9.8) 22 (4.4) 2 (0.4) 21 (4.2) 2 (0.4) 2 (0.4) 13 (2.6) 10 (2.0) 355 (17.9) 180 (9.1) 14 (0.7) 128 (6.4) 7 (0.4) 26 (1.3) 71 (3.6) 55 (2.8) b.001 b.001 .136 b.001 .366 .133 .372 .192 256 (49.9) 195 (38.0) 9 (1.8) 16 (3.1) 4 (0.8) 32 (6.2) 201 (43.3) 146 (31.5) 7 (1.5) 20 (4.3) 5 (1.1) 23 (5.0) 167 (32.8) 118 (23.1) 6 (1.2) 14 (2.8) 3 (0.6) 26 (5.1) 148 (29.7) 96 (19.2) 8 (1.6) 7 (1.4) 7 (1.4) 30 (6.0) 772 (38.9) 555 (27.9) 30 (1.5) 57 (2.9) 19 (1.0) 111 (5.6) b.001 b.001 .893 .059 .581 .762 dyssynchrony, a finding that is particularly relevant to patients presenting with low SBP, and prolonged QRS duration is an independent predictor of postdischarge morbidity and mortality. 11 Similarly, only 20% of the patients in the bottom quartile of SBP had an ICD at the time of enrollment, although nearly all these patients met the guideline-recommended criteria for primary prevention. In addition, the prevalence of ventricular arrhythmias was close to 35%, and the incidence of SCD was approximately 10% during follow-up. These findings suggest that LV dyssynchrony and ventricular arrhythmias may be undertreated in this high-risk population. However, studies examining medical device therapy in HF have been exclusively conducted in the ambulatory setting in stable patients with chronic HF on maximal medical therapy, and existing guidelines do not discuss the application of these potentially lifesaving treatments in HHF. 12 Nevertheless, some experts have advocated further research to clarify the optimal timing and application of electrophysiology diagnostics and therapeutics during HHF. 13–15 It is also notable that upward of 10% of patients in the bottom quartile of SBP required inotropic support at some point during hospitalization. Although inotropes may be clinically indicated for acute stabilization, even short-term use has been associated with increased inhospital and postdischarge mortality. 16 However, it is presently unclear whether SBP itself is simply a marker of poor prognosis or a potential targetable mediator of outcomes. Discussion Co pi aa ut or da ia za Inhospital change in SBP Inhospital change in SBP was a univariate predictor of both ACM (HR 0.93/10-mm Hg decrease, 95% CI 0.880.98) and CVM + HHF (HR 0.93/10-mm Hg decrease, 95% CI 0.89-0.97). In contrast, the change in SBP from baseline to discharge was not associated with either ACM (P = .26) or CVM + HHF (P = .61) after accounting for prespecified covariates (Table III). In addition, the association between change in SBP and the coprimary end points remained statistically nonsignificant when patients were divided by SBP quartile at baseline. P po variable was directly associated with risk of the coprimary end points both at baseline and at discharge/day 7 (Table III). rC DR Q1 82-105 mm Hg (n = 537) The present analysis contributes several additions to the existing literature on SBP during HHF. First, the distribution of SBP measurements after initial therapy was narrow. Second, the low SBP clinical profile included young men who had a higher prevalence of revascularization, ventricular arrhythmias, and ICD implantation; had a lower EF and worse laboratory profile; and were more likely to require intravenous inotropes during hospitalization. Lower SBP was associated with increased mortality, driven by progressive HF and SCD and CV hospitalizations, because of an excess of HHF. Finally, low SBP remained a poor prognostic indicator after the initiation of standard therapy and the resolution of the “acute” phase of hospitalization. Identifying targets for treatment It has already been reported that more than half of the patients without any device therapy enrolled in the EVEREST trial had electrocardiographic evidence of LV Mode of death and etiology of CV rehospitalization Despite trends toward improvement in per-capita riskadjusted HHF rates in the United States, 17,18 postdischarge mortality and readmission, respectively, may be as high as 15% and 30% within 60 to 90 days. 5 04/04/2014 American Heart Journal February 2013 222 Ambrosy et al Co pi aa ut or ia za da po rC DR Figure 2 Kaplan-Meier curves for ACM (A) and composite of CVM + HHF (B) by baseline SBP quartile (note: Q1 ≤105 mm Hg, Q2 106-119 mm Hg, Q3 120-130 mm Hg, and Q4 ≥131 mm Hg). Although it is well established that admission SBP is an important predictor of mortality, 5,19,20 this study establishes that SBP-related disparities in postdischarge mortality is principally caused by progressive HF and SCD. In contrast to the data from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry, which found allcause hospitalization to be comparable across quartiles of 04/04/2014 American Heart Journal Volume 165, Number 2 Ambrosy et al 223 Co pi aa ut or ia za da po rC DR Figure 3 Kaplan-Meier curves for ACM (A) and composite of CVM + HHF (B) by discharge SBP quartile (note: Q1 ≤ 100 mm Hg, Q2 = 101-111 mm Hg, Q3 = 112-125 mm Hg, and Q4 ≥126 mm Hg). SBP, the present analysis found lower SBP to be associated with higher CV readmission rates as a result of a greater incidence of HHF. However, it should be noted that in the EVEREST trial, approximately half of the hospitalizations occurring during follow-up were adjudicated as non-CV in etiology, highlighting the difficulty in interpreting these seemingly discrepant findings based on all-cause vs CV hospitalizations. 21 04/04/2014 American Heart Journal February 2013 224 Ambrosy et al Table III. Hazard ratios and 95% CI for risk of ACM and CVM + HHF per 10-mm Hg decrease in baseline, discharge, or inhospital change in SBP define a “reference range” and systematically study inhospital changes in SBP. ACM CVM + HHF 1.15 (1.08-1.22) 1.15 (1.08-1.22) 0.99 (0.94-1.05) 1.09 (1.04-1.14) 1.07 (1.02-1.13) 0.98 (0.94-1.03) Limitations There are several limitations to the data. First, this study was performed post hoc and is subject to the potential biases inherent to exploratory analyses of observational data. Nonetheless, data were prospectively collected, and events were adjudicated by a blinded, independent events committee. Second, enrollment was permitted up to 48 hours after admission, whereas standard therapy was likely started in the emergency department shortly after initial presentation. Third, patients with a baseline SBP b90 mm Hg and hemodynamically significant uncorrected primary cardiac valvular disease were excluded, greatly limiting the applicability of this study's findings to cardiogenic shock and other low output states. Finally, these data were collected in the context of a clinical trial; patients were well treated with background evidenced-based therapies and had prespecified postdischarge follow-up, potentially restricting the generalizability of this analysis. Baseline Discharge Inhospital change po da Conclusions Patients hospitalized for HF with low SBP tend to consist of young men with a low EF, ischemic etiology of HF, and a high-risk laboratory and neurohormonal profile. These patients may manifest comparable congestive signs and symptoms at initial presentation, respond favorably to standard therapy, but experience a dramatically higher postdischarge event rate driven by death from progressive HF and SCD and HF-related readmissions. Candidate targets for intervention include LV dyssynchrony and ventricular arrhythmias, which require prospective validation in the acute setting. Importantly, the prognostic value of SBP is not attenuated after the resolution of the acute phase and remains an independent clinical predictor of morbidity and mortality throughout admission in HHF with reduced EF. Co pi aa ut or ia za Pathophysiologic significance and prognostic value Although extremes of SBP were recorded, the later enrollment (ie, up to 48 hours after admission) after the very acute phase and initiation of standard therapy, as well as restriction of the EVEREST population to patients with reduced EF, led to a more narrow SBP distribution at enrollment than has been described in reports of registries of patients enrolled during HHF. Thus, it is notable that small increases in SBP still conferred an appreciable protective effect. Elevated BP in the acute setting is a result of high sympathetic tone, termed reactive hypertension, indicating the presence of functional cardiac reserve in the face of an acute physiologic stressor(s) (ie, pulmonary congestion). 3 In contrast, low or even normal BP at presentation, which may be the goal of treatment in the ambulatory setting, may be a more ominous finding, reflecting a low cardiac output and suboptimal or inadequate end-organ perfusion. Of note, the association of SBP increases with reduced mortality reported in the present analysis is comparable in magnitude with those reported in the primary results of OPTIMIZE-HF registry 5 and other studies, 19,20 suggesting that these pathophysiologic principles apply to SBP increases reported beyond initial presentation in the emergency department up until the time of discharge. Interestingly, after adjusting for potential confounders, inhospital change in SBP from baseline to discharge was not associated with outcomes for the overall cohort or within SBP quartile at baseline. This finding is in contrast to the hypothesis that SBP normalization might identify treatment “responders” and be associated with a decreased incidence of adverse outcomes. There are a couple of possible explanations for this neutral finding. First, the greatest change in SBP occurred within the first 24 hours of enrollment, and perhaps, a discernible effect may have been detected had study participants been enrolled closer to the time of initial presentation. Second, the pathophysiologic significance of inhospital change in SBP likely depends on starting SBP, which is why inhospital change in SBP was analyzed within each quartile of SBP at baseline. However, there are no obvious absolute physiologic “cutoffs,” making it challenging to rC DR Multivariate models are adjusted for age, sex, geographic region, medical comorbidities (ie, diabetes, hypertension, and renal insufficiency), history of ventricular arrhythmias, EF, serum sodium, BNP/amino terminal-proBNP, serum BUN, QRS duration, NYHA class, baseline medication use (ie, β-blocker, ACEIs/ ARBs, MRAs, digoxin, and inotropes), and presence of atrial flutter or fibrillation on baseline electrocardiogram. Values are presented as HR (95% CI). Disclosures Mihai Gheorghiade is a consultant for and/or has received research support from Abbott Labs, Astellas, AstraZeneca, Bayer Schering PharmaAG, CorThera Inc, Cytokinetics Inc, DebioPharm SA, ErrekappaTerapeutici (Milan, Italy), Glaxo Smith Kline, JNJ, Medtronic, Novartis Pharma AG, Otsuka, Sigma Tau, Solvay Pharmaceuticals, and Pericor Therapeutics. The other authors declare no conflicts of interest. References 1. Roger VL, Go AS, Lloyd-Jones DM, et al. Executive summary: heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation 2012;125(1):188-97. 04/04/2014 American Heart Journal Volume 165, Number 2 Ambrosy et al 225 da po rC DR 12. Hunt SA, Abraham WT, Chin MH, et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009;119(14):e391-479. 13. Wang NC, Fonarow GC, Gheorghiade M. The potential application of electrophysiology diagnostics and therapeutics in acute heart failure syndromes. Heart Fail Rev 2011;16(5):437-9. 14. Wang NC, Bhattacharya S, Gheorghiade M. The potential role of cardiac resynchronization therapy in acute heart failure syndromes. Heart Fail Rev 2011;16(5):481-90. 15. Wang NC, Piccini JP, Gheorghiade M. Implantable cardioverterdefibrillator implementation in acute heart failure syndromes: unanswered questions. Heart Fail Rev 2011;16(5):477-80. 16. Abraham WT, Adams KF, Fonarow GC, et al. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am Coll Cardiol 2005;46(1):57-64. 17. Gheorghiade M, Braunwald E. Hospitalizations for heart failure in the United States—a sign of hope. JAMA 2011;306(15):1705-6. 18. Chen J, Normand SL, Wang Y, et al. National and regional trends in heart failure hospitalization and mortality rates for Medicare beneficiaries, 1998-2008. JAMA 2011;306(15):1669-78. 19. Fonarow GC, Adams Jr KF, Abraham WT, et al. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA 2005;293(5): 572-80. 20. Lee DS, Austin PC, Rouleau JL, et al. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA 2003;290(19):2581-7. 21. O'Connor CM, Miller AB, Blair JE, et al. Causes of death and rehospitalization in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction: results from Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST) program. Am Heart J 2010;159(5):841 e1-9 e1. Co pi aa ut or ia za 2. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation 2012;125(1):e2-e220. 3. Gheorghiade M, Vaduganathan M, Ambrosy A, et al. Current management and future directions for the treatment of patients hospitalized for heart failure with low blood pressure. Heart Fail Rev 2012. 4. Harinstein ME, Flaherty JD, Fonarow GC, et al. Clinical assessment of acute heart failure syndromes: emergency department through the early post-discharge period. Heart 2011;97(19):1607-18. 5. Gheorghiade M, Abraham WT, Albert NM, et al. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006;296(18): 2217-26. 6. Adams Jr KF, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 2005;149(2):209-16. 7. Bhatia RS, Tu JV, Lee DS, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med 2006;355(3):260-9. 8. Gheorghiade M, Orlandi C, Burnett JC, et al. Rationale and design of the multicenter, randomized, double-blind, placebo-controlled study to evaluate the Efficacy of Vasopressin antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST). J Card Fail 2005;11(4): 260-9. 9. Gheorghiade M, Konstam MA, Burnett Jr JC, et al. Short-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA 2007;297(12):1332-43. 10. Konstam MA, Gheorghiade M, Burnett Jr JC, et al. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA 2007;297(12):1319-31. 11. Wang NC, Maggioni AP, Konstam MA, et al. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA 2008;299(22): 2656-66. 04/04/2014












© Copyright 2025