
Technology-Assisted Direct Observation Methods for Hand Hygiene
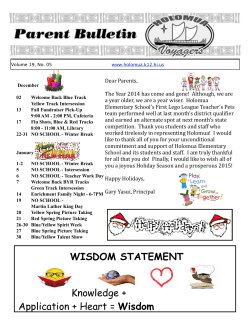
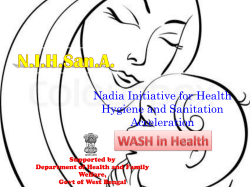
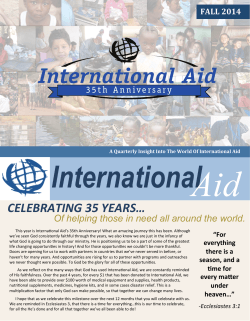
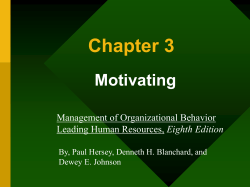
DUKE INFECTION CONTROL OUTREACH NETWORK (DICON) Infection Prevention News Volume 10, Number 5, May 2015 Technology-Assisted Direct Observation Methods for Hand Hygiene Background: Our April 2015 newsletter discussed the importance of monitoring hand hygiene compliance rates and the pros and cons of 4 hand hygiene compliance surveillance methods. In this newsletter, we discuss types of technology-assisted direct observation devices for hand hygiene compliance monitoring programs in community hospitals. The objectives of this newsletter are threefold. First, to explain the advantages of technology-assisted direct observation tools in hand hygiene compliance monitoring Second, to compare and contrast the currently available technology-assisted direct observation devices and their associated software programs Third, to make recommendations on how to implement technology-assisted direct observations in a community hospital setting Technology-assisted direct observation: Technology-assisted direct hand hygiene observation methods utilize mobile devices such as iPods, iPads, and cell phones to document hand hygiene adherence. DICON and the Society for Healthcare Epidemiology of America (SHEA) guidelines recommend using technology-assisted direct observation for hand hygiene for several reasons.1 Mobile devices are less conspicuous thus reducing the potential for confounding from the “Hawthorne Effect” [discussed and explained in the April newsletter]. In addition, mobile hand-held devices electronically capture data on hand hygiene adherence - thus eliminating or reducing the burden of manual documentation required for older “paper and pen” methods of data collection. In addition, most technology assisted methods for hand hygiene monitoring calculate unit-specific and hospital-wide rates of hand hygiene compliance in “real-time.” This facilitates rapid data feedback to hospital leadership and healthcare providers. Finally and most importantly, hospitals that utilize these methods consistently report improved hand hygiene rates.2 Operational considerations: Key operational components to consider when choosing a toolset for compliance monitoring include the time and “manpower” required to collect and then report compliance data. The most time consuming aspect of a direct observation program are data analysis and generation of meaningful reports. Without analysis and data reports, true and meaningful “stakeholder engagement” by hospital leadership is not likely to occur or be sustained. Technology-assisted direct observation electronic tools: iScrub application The iScrub application, developed by the University of Iowa,3 can be downloaded to iPhones or iPods from iTunes. This app is free and has received generally good reviews. iScrub allows for collection of observational data on compliance with isolation precautions and hand hygiene. iScrub has a “user-friendly” interface allowing for collection of data on different categories of healthcare workers that can subsequently be used to measure compliance by worker type and location (figure 1). There are two major deficiencies in the iScrub application. First, hand hygiene compliance rates must be manually calculated the resulting observation data is then emailed to users, rather than stored in a central database (i.e.“in the cloud”). Second, because this application has not recently been updated, technical bugs in customization tools and problems with data uploads have been reported. In-house software: Some large hospitals and hospital systems have created in-house software programs to digitally record hand hygiene observations. For example, Duke University Hospital developed an in-house software program that led to dramatic improvement in hand hygiene adherence rates (ranging from 86 to 97% in various care units). This improvement was attributed in large part to timely data analysis and feedback of electronic data collected on wards and care areas and then wirelessly transmitted to a central database that generated compliance reports in tabular and graphic forms.2 Similar in-house programs have also been developed by other hospitals in other countries.4 Commercial programs: Commercial programs, such as a cloud-based system from Hygistics cost as little as $15/bed/year and include an array of features that can be utilized by local infection preventionists (IPs).5 Designated hand hygiene monitoring personnel log in to the Hygistics website online via a simple and intuitive interface (figure 2). No additional software downloads or IT support is required. Almost any mobile device can be utilized to collect the data. Hygistics also can provide a customized paper form generator that can in turn be scanned to convert “paper and pencil” data into electronic data. Analysis tools provide decision support and peer benchmarking for local leadership (figure 3). Other programs: The Canadian Patient Safety Institute (CPSI), a not-for-profit patient safety organization, provides a free electronic hand hygiene observation tool for hospitals in Canada and the United States.6 In addition to its free cost, the major advantage of the CPSI program is automatically generated statistical performance data, which can then be compared to other hospitals. However, limitations exist. First, their mobile device format is still in development. Second, their current user interface is not intuitive (figure 4). Finally, the program focuses on overly detailed World Health Organization (WHO) hand hygiene standards – something not emphasized in the United States or recommended by DICON as criteria for monitoring hand hygiene compliance. Hand Hygiene Australia (HHA), an Australian hand hygiene campaign, also provides a free hand hygiene application that is accessible via any mobile device with web browsing capabilities.7 Like CPSI, handhygiene compliance reports can be easily generated via a downloaded Excel spreadsheet. Similar to the tool developed by the Canadian Patient Safety Institute, the Australian program also utilizes WHO hand hygiene compliance standards. In addition, the user interface, although better than the CPSI’s interface, is still cumbersome (figure 5). Summary/Recommendations Technology-assisted direct observation tools improve reporting accuracy by reducing the “Hawthorne effect”, reduce documentation burdens for infection preventionists, and some provide statistical analysis support tools. Although numerous technology-assisted direct observation tools exist, iScrub and commercial programs, such as Hygistics, are the two most suitable programs for community hospitals. Infection prevention staff at DICON member hospitals should consider incorporating one of these tools into their current hand-hygiene surveillance programs. We recommend the following steps: Download the free iScrub hand hygiene application to a mobile device on iTunes o Explore the iScrub app o Mandate that hand hygiene auditors document a subset of observations via both iScrub and traditional surveillance methods o Obtain feedback from hand hygiene auditors regarding both surveillance methods o Determine if iScrub is “right” for your hospital Visit the Hygistics website to determine if their technology-assisted direct observation hand hygiene surveillance tool is right for your hospital o Consider a “free trial” of the Hygistics program o Consider e-mailing the company at info@hygistics.com o Determine if Hgistics is “right” for your hospital Of note: Todd Scarcola, president of Hygistics, contributed to this newsletter by providing an example of statistical output from Hygistics (in figure 3) Figure 1. Example of two iScrub iPhone screenshots.8 Figure 2. Example of Hygistics mobile screenshot.5 Figure 3. Example of Hygistics statistical output.2 Figure 4. Canada Patient Safety Institute (CSPI) electronic hand hygiene data collection form.6 Figure 5. Hand Hygiene Australia data collection form.7 References: 1. 2. 3. 4. 5. 6. 7. 8. Ellingson K, Haas JP, Aiello AE, et al. Strategies to prevent healthcare-associated infections through hand hygiene. Infect. Control Hosp. Epidemiol. 2014;35 Suppl 2:S155-178. Chen LF, Carriker C, Staheli R, et al. Observing and improving hand hygiene compliance: implementation and refinement of an electronic-assisted direct-observer hand hygiene audit program. Infect. Control Hosp. Epidemiol. 2013;34(2):207-210. Hlady CS, Severson MA, Segre AM, Polgreen PM. A mobile handheld computing application for recording hand hygiene observations. Infect. Control Hosp. Epidemiol. 2010;31(9):975-977. Graf K, Ott E, Wolny M, et al. Hand hygiene compliance in transplant and other special patient groups: an observational study. Am. J. Infect. Control. 2013;41(6):503-508. Hygistics http://hygistics.com/ [Accessed 5/5/2015]. Canadian Patient Safety Institute Hand Hygiene Observation Tools. http://www.handhygiene.ca/English/tools/pages/hand-hygiene-observation-tools.aspx [Accessed 4/28/15]. Hand Hygiene Australia Application for International Data Collection. http://www.hha.org.au/HHComplianceSystem/hhcappwho.aspx [Accessed 4/28/15]. iScrub Program. http://compepi.cs.uiowa.edu/iscrub/ [Accessed 5/5/2015].






© Copyright 2025