
Clinical presentation and immune response of Human African
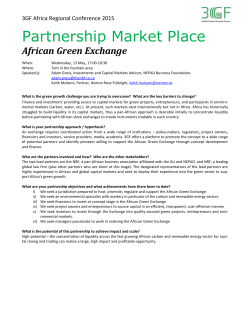
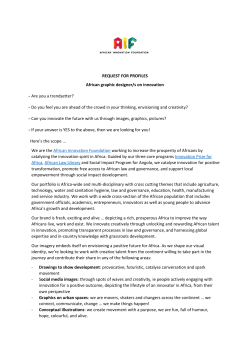
Global Advanced Research Journal of Medicine and Medical Science (ISSN: 2315-5159) Vol. 4(4) pp. 159-167, April, 2015 Available online http://garj.org/garjmms/index.htm Copyright © 2015 Global Advanced Research Journals Review Clinical presentation and immune response of Human African Trypanosomiasis – a review D. Musa*, A. O Fajinmi, R.O Kalejaiye and T. Tese Nigerian Institute for Trypanosomiasis and Onchocerciais Research (NITR) Kaduna, Nigeria Accepted 26 March, 2015 Human African trypanosomiasis or sleeping sickness is caused by infection with two subspecies of the tsetse-fly-vectored haemoflagellate parasite Trypanosomabrucei. Historically, epidemic sleeping sickness has caused massive loss of life, and related animal diseases have had a crucial impact on development in sub-Saharan Africa. After a period of moderately successful control during the mid-part of the 20th century, sleeping sickness incidence is currently rising, and control is hampered by a combination of factors, including civil unrest and the possible development of drug resistance by the parasites. The prevailing view is that the disease is invariably fatal without anti-trypanosomal drug treatment. However, there have also been intriguing reports of wide variations in disease severity as well as evidence of asymptomatic carriers of trypanosomes. These differences in the presentation of the disease will be discussed in the context of our knowledge of the immunology of trypanosomiasis. The impact of dysregulated inflammatory responses in both systemic and CNS pathology will be examined and the potential for host genotype variation in disease severity and control will be discussed. Keywords: Trypanosomiasis, tsetse-fly INTRODUCTION Human African trypanosomiasis or sleeping sickness is caused by infection with the tsetse-fly-transmitted protozoan haemoflagellates Trypanosomabrucei rhodesiense (in East and Southern Africa) and T. b. gambiense (in West and Central Africa). This disease is presently re-emergent and infection is currently estimated at over 30 000 with about 55 million people at risk of infection (WHO, 1998). These parasites, along with the non-human-infective Trypanosomabruceibrucei are zoonoses, and disease control is impeded by substantial wild and domestic *Corresponding Author E-mail: musakaus@yahoo.com animal reservoirs of infection. The taxonomic relationships of the three T. brucei subspecies have been defined using molecular markers. T. b. rhodesiense and T. b. brucei are closely related host-range variants. Human infectivity in T. b. rhodesiense is conferred by the SRA (Xong et al., 1998) gene product which renders the parasites resistant to lytic activity in normal human serum. On the other hand T. b. gambiense is distinct, with marked genetic and biochemical differences (Gibson, 2002). T. b. gambiense does not possess the SRA gene and the mechanism of human serum resistance is not known (Gibson, 2002). African trypanosomes may be adapted to growth in experimental mouse models, and much of our knowledge of the biology of these parasites comes from such studies. 160 Glo. Adv. Res. J. Med. Med. Sci. Figure 1. LIFE CYCLE AND DISEASE PROGRESSION The infection is initiated by the injection of metacyclic trypanosomes in the saliva of the tsetse fly (Figure 1). After the bite of a trypanosome-infected tsetse fly, the metacyclic forms establish in the skin, differentiate to the bloodstream stage and spread via the local draining lymph node into the vascular system. In some but not all infections, a local skin reaction or chancre occurs at the site of inoculation, which is caused by a local inflammatory response to the parasites, and subsides after 4 weeks (Fairbairn and Godfrey, 1957; Naessens et al., 2003). The early (or haemolymphatic stage) commences 1–3 weeks after an infective fly bite and presents with periods of fever lasting 1–7 days and generalized lymphadenopathy. During this period the parasites proliferate within the blood and lymphatic system. Symptoms include general malaise, anaemia, headache, pyrexia, weight loss and weakness. Immuneactivation is evident from lymph node enlargement, hepatomegaly and splenomagaly. The late (meningoencephalitic) stage of infection coincides with the invasion of the CNS by parasites and is associated with psychiatric, motor and sensory disorders, along with sleep abnormalities. If untreated, late-stage patients progress to a final stage involving seizures, somnolence, coma and death (Kennedy, 2004). Both T. b. rhodesiense and T. b. gambiense infections follow this sequence of infection stages, but with a marked difference rate of progression. T. b. gambiense presents as a chronic infection, in which progression to late stage may take several months or longer, and late-stage CNS infection may last several years (Barrett et al., 2003). On the other hand, T. b. rhodesiense is generally regarded as an acute infection, with progression to late stage occurring in a matter of weeks and the late-stage CNS infection leading to death within 3 months, although this may not always be the case, as will be discussed in this review. Figure 1. Life cycle of African trypanosomes. Infectious metacyclic trypanosomes are injected by a tsetse fly. In some cases a chancre forms at the site of infection. The parasites spread via the local draining lymph node to the vascular system. Bloodstream trypanosomes take two forms. The slender undergoes continuous asexual proliferation. Some slender forms differentiate to stumpy forms which do not proliferate but are pre-adapted for rapid establishment in the tsetse fly. IMMUNOLOGY OF INFECTION Antigenic variation and antibody responses African trypanosomes’ primary immune-evasion strategy is antigenic variation (Pays et al., 2004; Vanhamme et al., 8 2001). The parasites are covered with a coat of 10 variant surface glycoprotein (VSG) molecules attached to the trypanosome cell membrane via a glycosylphosphatidyl-inositol (GPI) anchor (Magez et al., 2002). VSG is an immunodominant antigen, capable of Musa et al. 161 eliciting both T-cell dependent and independent B-cell responses, depending on its conformation (Mansfield, 1994). Antibody opsonized trypanosomes are effectively cleared by the host lymphoreticular system (Macaskill et al., 1981). The parasite, however, undergoes antigenic variation and has a repertoire of more than 1000 transcriptionally inactive VSG genes and a single active transcription site. The genetics of this process have been reviewed elsewhere (Pays et al., 2004) and the result is a continuous stochastic switching of VSG genes at a rate of −3 −4 between 10 and 10 per cell division (Turner and Barry, 1989). This enables the parasite to maintain a state of chronic infection in the host, and the importance of the process is testified to by the fact that VSG genes occupy 10% of the trypanosome genome (Donelson, 2003). The VSG molecule therefore plays a pivotal role in host responses to African trypanosomes. The humoral response to VSG also has immunopathologicalsequelae. VSG elicits polyclonal B-cell activation, and in human infection this manifests in the generation of autoantibodies (Kazyumba et al., 1986) and immune complex disease (Lambert et al., 1981). Furthermore, in the meningoencephalitic stage of infection both trypanosome-specific IgG and IgM and polyclonal IgM responses have been detected in the cerebrospinal fluid (CSF) (Lejon et al., 1998). These may derive from modified plasma cells known as Mott or morular cells in the white matter and also plasma cells which form perivascular infiltrates in the brain (Kennedy, 2004). Cellular immune activation Most studies of the cellular response to African trypanosome infection have involved the use of experimental mouse models. In early (7–21 days) infection in mice, macrophage activation results in the release of nitric oxide, and pro-inflammatory mediators such as TNF-α and IL-1. Several mechanisms have been proposed to drive macrophage activation in African trypanosome infection. One of these involves a direct interaction with VSG and VSG-GPI anchor components. It has been estimated that with the clearance of each parastaemic peak, some 200 µg of VSG molecules are shed (Magez et al., 2002). Soluble VSG carrying the GPI anchor glycosylinositol phosphate (GIP-sVSG) core and the residual dimyristoylglycerol glycerol (DMG) anchor moiety are potent macrophage-activating factors (Magez et al., 1998) which appear to have different modes of action. The GIP moiety directly induces macrophage activation (Coller et al., 2003) and TNF-α induction (Coller et al., 2003) in macrophages after IFN-γ stimulation, whereas the DMG component of the VSG anchor does not itself induce TNF-α but is involved in macrophage priming. This may account for earlier observations of a synergy between parasite-soluble factors and IFN-γ in the in vitro activation of nitric oxide synthesis in macrophages (Sternberg and Mabbott, 1996). Interestingly, the timing of IFN-γ stimulation seems to be important, and it has been observed that if macrophages are exposed to GIP-sVSG before IFN-γ, there is a dose-dependent inhibition of macrophage IFNγ-dependent STAT1 phosphorylation and activation (Coller et al., 2003). It has been long known that IFN-γ is produced in murine trypanosomiais (Bancroft et al., 1983), and recently this has been confirmed in plasma samples from clinical cases (MacLean et al., 2001). + Considerable experimental evidence supports CD4 Tcells responding to VSG and other parasite antigens as the main cellular source of IFN-γ production in murine trypanosomiasis (Schleifer et al., 1993; Hertz et al., 1998; Schopf et al., 1998). Other putative sources of IFN-γ are + CD8 T-cells (Donelson et al., 1998) and activated NK cells (Sternberg, 1998). In mouse models, activated macrophages mediate suppression of both B- and T-cell proliferative responses (Sternberg, 1998; Schleifer and Mansfield, 1993) and contribute to the immunosuppression which is associated with trypanosomiasis (Askonas, 1985) via nitric oxide, prostaglandin and TNF-α release (Magez et al., 1999). The significance of immunosuppression in the pathology of human trypanosomiasis is unclear, but the proinflammatory cytokine TNF-α has multiple pathological targets which are consistent with the pathology observed in both HAT and experimental infections, including tissue necrosis, anaemia (Magez et al., 2004) and cachexia (Cerami and Beutler, 1988). TNF-α mediated inflammatory responses have also been proposed to be necessary for the penetration of parasites through the blood–brain barrier endothelia (Enanga et al., 2002). Experiments using genetically attenuated parasites have indicated that in subtolerant hosts which exhibit survival times of longer than 200 days there is a transition to a type II cellular response profile, with the production of counter-inflammatory cytokines including IL-10 and the development of alternatively activated macrophages (Namangala et al., 2001; De Baetselier et al., 2001). The association of this immune response profile with a relatively benign infection indicates that maintenance of a counter-inflammatory cytokine milieu may be important in allowing survival with a chronic trypanosome infection. Such a view is confirmed by the restoration of a virulent disease profile in attenuated parasites when inoculated in IL-10 knockout mice (De Baetselier et al., 2001). While such data suggest that the pro-inflammatory response triggered by the parasites is detrimental to the host, there have also been reports that TNF-α is lytic to African trypanosomes (Magez et al., 1997) and may account for the exacerbation of parasitaemia in TNF-α knockout mice. Despite elevated parasitaemia, such mice showed lower levels of histopathology and anaemia (Magez et al., 1999). This indicates that parasitaemia control and pathology are independent traits (Magez et al., 2004), and it is important when extrapolating from the mouse model to the human disease to bear in mind that it is 162 Glo. Adv. Res. J. Med. Med. Sci. pathology which is the clinically relevant trait. It should be added that a direct trypanolytic role of TNF-α is subject to some debate, and data has also been presented indicating no effect on the parasite (Kitani et al., 2002). It is possible to prevent African trypanosomes from shedding VSG and GPI anchor components and thus remove a macrophage pro-inflammatory stimulus from the host using GPI-phospholipase-C (PLC) knockout trypanosomes (Webb et al., 1997). PLC is responsible for the cleavage of the GPI anchor of the VSG molecule, and the release of GIP-sVSG and DMG from trypanosomes (Magez et al., 1998). Such parasites were able to maintain chronic infection in experimental mice over periods longer than 100 days, and this was associated with a switch from a type I inflammatory immune response to a type II response characterized by IL-10 and IL-4 and macrophages with an alternative activation phenotype (De Baetselier et al., 2001), although TNF-α levels continued to be elevated. Thus it appears that removal of a macrophage-activating stimulus allows infection-associated inflammation to be controlled. A PLC-knockout mutant has since been generated in T. b. brucei 427, where animals are overwhelmed by fulminating parasitaemia rather than infection-associated pathology, and this mutant is no less virulent than its wildtype form (Leal et al., 2001), further supporting the role of PLC-shed components in modulating inflammatory pathology. In summary, experimental studies of T. brucei infection in mice indicate that the balance of pro- and counter-inflammatory activity determines the severity of pathology and the survival time of animals. Inflammatory and counter-inflammatory cytokines in human African trypanosomiais Studies of cytokine production in sleeping sickness patients from Uganda and Congo have enabled predictions from the mouse model to be tested. With one exception, these studies have been of a before–after design, in which plasma cytokine levels are measured in a sample taken at the time of parasitological diagnosis and a subsequent sample is taken at the end of treatment. In a study of T. b. rhodesiense patients in Uganda, both early and late-stage infections were characterized by elevated levels of IFN-γ, TNF-α and IL10, although IFN-γ levels did diminish in the late-stage cases (MacLean et al., 2001; MacLean et al., 1999). This pattern of cytokine production is entirely consistent with the mouse model of moderately chronic disease progression obtained with subtolerant hosts (Magez et al., 2004) or PLC knockout trypanosomes (De Baetselier et al., 2001). The mouse model also predicts nitric oxide production in the early stages of infection. This has not been consistently observed (MacLean et al., 1999) in human subjects, and may reflect the fact that most HAT patients are diagnosed after a considerable period of infection. Although it is straightforward to determine the stage of infection, information obtained from patients on the duration of illness is often unreliable. In T. b. gambiense patients, one study demonstrated increased plasma IL-10, IL-6 and IL-8, but no detectable IFN-γ or TNF-α (Lejon et al., 2002). However, two other studies detected elevated TNF-α levels (Rhind et al., 1997; Okomo-Assoumou et al., 1995) in T. b. gambiense patients, and in one of these TNF-α concentration was significantly correlated to the severity of disease (OkomoAssoumou et al., 1995). Thus, whereas the cytokine response profile in T. b. gambiense sleeping sickness requires clarification, in rhodesiense sleeping sickness it may be interpreted as representing a balance between inflammatory mediators (TNF-α, IFN-γ) and a counterbalancing IL-10 counter-inflammatory response (Moore et al., 2001). The cellular source of these cytokines remains to be determined. Macrophages are clearly important sources of TNF-α, and in an in vitro study it was demonstrated that T. b. gambiense activated a human macrophage cell line to release TNF-α (Daulouede et al., 2001). Also TNF-α and IFN-γ transcripts have been detected by RT-PCR analysis of RNA isolated from HAT patient peripheral blood mononuclear cells (Sternberg JM and MacLean L, unpublished data). Inflammatory responses and late-stage progression in HAT The most serious and ultimately fatal consequences of the disease manifest after the invasion of the CNS by parasites in the late or meningoencephalitic stage (Kennedy, 1999). Post-mortem (Adams et al., 1986) and mouse histopathological studies (Kennedy, 1999) have indicated that the late stage of disease is characterized by inflammatory processes (Kennedy, 1999). In particular, non-specific perivascular inflammatory cell infiltrates occur in the leptomeninges and white matter, and there is a pronounced activation of microglia and astrocytes (Hunter et al., 1992). In mouse models of the late stage, the onset of these histopathological changes coincides with the up-regulation of pro-inflammatory cytokines (Hunter and Kennedy, 1992; Hunter et al., 1991). The resulting inflammatory response is most pronounced in the post-treatment reactive encephalopathy (PTRE) which occurs in 5–10% of patients after treatment with arsenical drugs (Atouguia and Costa, 1999) and which can be ameliorated in a model system by administration of anti-inflammatory agents (Hunter et al., 1992). The trypanostatic drug DFMO reduces astrocyte activation and neuroinflammatory responses, and this may be a key factor in its efficacy (Jennings et al., 1997). Thus, the mouse model predicts that the pathological sequelae of late-stage sleeping sickness are mediated by proinflammatory cytokines in the brain, released by activated astrocytes or microglia. This scenario is consistent with Musa et al. 163 Figure 2. inflammatory pathology caused by other infectious diseases in the CNS, such as tuberculous meningitis (Tsenova et al., 1999). The above prediction was not immediately borne out when the first analysis of cytokines in the CSF of sleeping sickness patients was undertaken. In both T. b. rhodesiense and T. b. gambiense patient CSFs, the late stage was associated with increased IL-10 and IL-6 but not TNF-α or IFN-γ (Lejon et al., 2002; MacLean et al., 2005). Moreover, at least in the case of T. b. rhodesiense infection, IL-10 and IL-6 were synthesized in the CNS (MacLean et al., 2005). In no cases was TNF-α or IL-1 detected. Can this result be reconciled with post-mortem histological evidence of inflammatory pathology and the results from the mouse models? One possibility is that the published mouse infection studies and the sleeping sickness studies are examining different stages of the development of latestage pathogenesis. Almost all neuropathological data from human subjects involves post-mortem studies of PTRE cases, and much of the published mouse infection data involves advanced CNS infection or PTRE models. Thus, pro-inflammatory cytokines and resultant cellular responses may be important in the ‘final stage’ of meningoencephalitic sleeping sickness, but before this is reached IL-10 down regulates the production of TNF-α and other pro-inflammatory cytokines by astrocytes and microglia, despite continued immune stimulation by the parasites. IL-10 has been demonstrated to have similar counter-inflammatory regulatory activity in cerebral toxoplasmosis (Sarciron and Gherardi, 2000) and experimental autoimmune encephalitis (Cua et al., 2001). Initial data on the temporal progression of IL-10 and TNFα levels in the brains of mice during trypanosome invasion support this hypothesis (Figure 2). Figure 2. Brain IL-10 and TNF-α levels during the development of CNS infection. Adult female CD1 mice 4 were infected with 4 × 10 T. b. brucei GVR35/CL6. In this model, parasites first enter the brain between day 7 and 14, and increasing histopathology is evident from day 21. This coincides with increased TNF-α levels and reduced IL-10 levels. *significantly increased over control, P < 0·01. Source: Sternberg JM, MacLean L, Rodgers J and Kennedy PGE, unpublished data. 164 Glo. Adv. Res. J. Med. Med. Sci. TOWARDS AN IMMUNOEPIDEMIOLOGY OF HUMAN AFRICAN TRYPANOSOMIASIS? Given the central role of inflammatory immune responses in sleeping sickness pathogenesis, it is possible that immunogenetic variation in host populations may influence disease progression and outcome. This is an area of investigation which has received scanty attention, partly because substantive field studies of trypanosomiasis immunology have only recently started, and partly because of the widely held view that infection invariably leads to death if untreated. In fact this statement is not correct, and not only is there evidence that individuals can be asymptomatic carriers, but also there are tremendous variations in the severity and speed of progression of the disease. In T. b. gambiense infection, apparently healthy carriers have been reported during large-scale population surveys (Wery and Burke, 1972; Jamonneau et al., 2004). Indeed, one widely used experimental isolate of T. b. gambiense was derived from a subject who had been asymptomatic for 20 years, and was only diagnosed while living in Europe (Lapierre and Coste, 1963). With T. b. rhodesiense infection in man there have also been reports of both asymptomatic carriers and mild infections which progress with a chronic disease evolution in the southern areas of East and Central Africa (Ormerod, 1967; Buyst, 1977), and more recently a systematic study has confirmed that subacuteT. b. rhodesiense sleeping sickness exists in Malawi (MacLean et al., 2004). These differences in disease severity do not necessarily imply variation in host resistance, as they could equally reflect genetic variation in parasite virulence. Indeed innate variation in parasite virulence is certainly manifest is experimental infections, where subclones of differing but stable virulence phenotype can be generated from a single parental clone (Inverso et al., 1988), and such variation is clearly evident in human infection in the difference in disease progression between T. b. rhodesiense and T. b. gambiense. However, experimental models also demonstrate that host genotype influences the progression of trypanosome infection. Inbred mouse models range from highly susceptible to subtolerant to trypanosome infection. Subtolerance is not related to H-2 (Clayton, 1978) and is under polygenic control (Murray et al., 1984). The genetics of the control of susceptibility/subtolerance to trypanosome infection has been studied in detail using the cattle parasite, Trypanosomacongolense in mouse infection models. Three quantitative trait loci (QTLs) have been identified, designated Tir1, Tir2, Tir3 (Kemp et al., 1997). Fine mapping (Iraqi et al., 2000) has recently led to the resolution of three QTLs within Tir3. One of these (Tir3b) maps close to the chromosomal location of both the IL-10 gene and a key regulatory gene for IL-10 synthesis on chromosome 1 (Tabel et al., 2000), although it must be emphasized that the resolution of these QTLs is still limited, with a 95% CI for Tir3b of 10 cm. Similar studies are being made to understand the genetic basis of trypanotolerance in cattle (Kemp et al., 1997). While it is important to bear in mind that there are fundamental differences in pathogenesis between T. congolense and T. brucei spp. (Taylor and Mertens, 1999), it is reasonable to ask if it is possible that a similar immunogenetic control of disease severity may be found in HAT? At present there is no definitive answer to this question, but there are some intriguing clues in a comparative study of clinical presentation, disease progression and plasma cytokine responses of T. b. rhodesiense-infected patients in Malawi and Uganda (MacLean et al., 2004). Disease in Ugandan patients was acute, with rapid progression to late stage. In contrast, in Malawi the disease was mild, no patients had chancres, and progression to late stage was slow, with some individuals remaining in early stage for several months or longer. In both localities the parasites were clearly T. b. rhodesiense, because they carried the SRA gene. When the plasma cytokine levels of the two groups were compared, dramatic differences in inflammatory/counterinflammatory responses were observed. Whereas IFN-γ and IL-10 were elevated in all cases, TNF-α was elevated only in the acute disease group from Uganda. Conversely, in the mild disease group from Malawi, TNFα levels remained normal but TGF-β levels were elevated. TGF-β has multiple functions depending on its environment and concentration, but at high concentration it suppresses TNF-α production by macrophages (Espevik et al., 1987) and NK cells (Bellone et al., 1995). If TNF-α does indeed mediate the onset of pathology and disease progression, the capacity to maintain a TGF-βmediated counter-inflammatory response may be critical to the mild presentation of T. b. rhodesiense infection and for the slow progression to CNS infection in Malawian HAT cases. TGF-β seems to have a similar role in regulating disease severity in other infectious diseases, including malaria (Omer et al., 2000). Of course, an association of cytokine responses with disease severity does not demonstrate causality, and it may yet be that the potent pro-inflammatory response observed in Ugandan patients is simply a reflection of an innately more aggressive parasite. However, there are other clues that host genotype may be involved in determining disease severity, and thus polymorphisms in immune response regulation may be significant. In a study of sleeping sickness in Zimbabwe, where the mild presentation of T. b. rhodesiense infection occurs, it was found that while all European patients developed chancres at the site of the infective tsetse fly bite and subsequent severe pyrexial illness, African patients did not develop chancre and limited data suggested a reduced severity of pyrexia (Ashworth and Goldsmid, 1975). This is consistent with the presentation of sleeping sickness in Malawi, but not in Uganda. It has been Musa et al. 165 proposed that populations of Bantu ancestry may have a degree of innate resistance to T. b. rhodesiense sleeping sickness (Buyst, 1977), and this is consistent with modern populations in the southern foci largely being of Bantu ancestry, whereas in the northern foci there are significant populations of Nilo-Hamitic descent who migrated to the lake Victoria basin from a tsetse-free area to the north. CONCLUDING REMARKS Although immunological study of African trypanosomiasis in humans is still in its infancy, dysregulated inflammatory responses appear to play a role disease progression and pathology consistent with that described in experimental mouse models, with the outcome of infection being determined by a balance between pro-inflammatory triggering by parasite components, such as GPI, and counter-inflammatory regulatory mechanisms involving IL-10 and TGF-β. An understanding of the immunological component of this disease offers new opportunities for therapeutic intervention, and already preliminary data on vaccination with GPI in mice indicates that TNFassociated immunopathology is reduced in subsequently infected mice (Magez et al., 2002). Furthermore, as the first systematic studies of trypanosomiasis patients with varying severity of disease begin (MacLean et al., 2004), it should be possible to determine if there is indeed an immunogenetic component to HAT. REFERENCES Adams JH, Haller L, Boa FY, Doua F, Dago A, Konian K (1986). Human African trypanosomiasis (T. b. gambiense): a study of 16 fatal cases of sleeping sickness with some observations on acute reactive arsenical encephalopathy. Neuropathol. Appl. Neurobiol. 12: 81–94. Ashworth TG, Goldsmid J (1975). A re-assessment of the epidemiology and clinico-pathological features of human trypanosomiasis in Rhodesia. Cent. Afr. J. Med. 21: 1–12. Askonas BA (1985). Macrophages as mediators of immunosuppression in murine African trypanosomiasis. Curr. Top. Microbiol. Immunol. 117: 119–127. Atouguia J, Costa J (1999). Therapy of human African trypanosomiasis: current situation. Mem. Inst. Oswaldo Cruz. 94: 221–224. Bancroft GJ, Sutton CJ, Morris AG, Askonas BA (1983). Production of interferons during experimental African trypanosomiasis.ClinExpImmunol; 52: 135–143. Barrett MP, Burchmore RJ, Stich A et al (2003). The trypanosomiases. Lancet. 362: 1469–1480. Bellone G, Aste-Amezaga G, Trinchieri G, Rodeck U (1995). Regulation of NK-cell functions by TGF-beta1. J. Immunol. 155: 1066–1073. Buyst H (1977). The epidemiology of sleeping sickness in the historical Luangwa valley. Ann Soc. Belge Med. Trop. 57: 349–359. Cerami A, Beutler B (1988). The role of cachectin/TNF in endotoxic shock and cachexia. Immunol. Today. 9: 28–31. Clayton CE (1978). Trypanosomabrucei: influence of host strain and parasite antigenic type on infections in mice. Exp. Parasitol. 44: 202– 208. Coller SP, Mansfield JM, Paulnock DM (2003). Glycosylinositolphosphate soluble variant surface glycoprotein inhibits IFN-gamma-induced nitric oxide production via reduction in STAT1 phosphorylation in African trypanosomiasis. J. Immunol. 171: 1466–1472. Cua DJ, Hutchins B, LaFace DM, Stohlman SA, Coffman RL (2001). Central nervous system expression of IL-10 inhibits autoimmune encephalomyelitis. J. Immunol. 166: 602–608. Daulouede S, Bouteille B, Moynet D, et al (2001). Human macrophage tumor necrosis factor (TNF)-alpha production induced by Trypanosomabruceigambiense and the role of TNF-alpha in parasite control. J. Infect. Dis. 183: 988–991. De Baetselier P, Namangala B, Noel W, Brys L, Pays E, Beschin A (2001). Alternative versus classical macrophage activation during experimental African trypanosomosis. Int. J. Parasitol. 31: 575–587. Donelson JE (2003). Antigenic variation and the African trypanosome genome. Acta Trop. 85: 391–404. Donelson JE, Hill KL, El-Sayed NM (1998). Multiple mechanisms of immune evasion by African trypanosomes. Mol. Biochem. Parasitol. 91: 51–66. Enanga B, Burchmore RS, Stewart ML, Barrett MP (2002). Sleeping sickness and the brain. Cell Mol. Life Sci. 59: 845–858. Espevik T, Figari IS, Shalaby MR, et al (1987). Inhibition of cytokine production by cyclosporin-A and Transforming Growth Factor-beta. J. Exp. Med. 166: 571–576. Fairbairn H, Godfrey DG (1957). The local reaction in man at the site of infection with Trypanosomarhodesiense. Ann. Trop. Med. Parasitol. 51: 464–470. Gibson W (2002). Will the real Trypanosomabrucei please step forward? Trends Parasitol. 18: 486–490. Hertz CJ, Filutowicz H, Mansfield JM (1998). Resistance to the African trypanosomes is IFN-gamma dependent. J. Immunol. 161: 6775– 6783. Hunter CA, Gow JW, Kennedy PG, Jennings FW, Murray M (1991). Immunopathology of experimental African sleeping sickness: detection of cytokine mRNA in the brains of Trypanosomabruceibrucei-infected mice. Infect. Immun. 59: 4636– 4640. Hunter CA, Jennings FW, Kennedy PG, Murray M (1992). Astrocyte activation correlates with cytokine production in central nervous system of Trypanosomabruceibrucei-infected mice. Laboratory Invest. 67: 635–642. Hunter CA, Jennings FW, Kennedy PG, Murray M (1992). The use of azathioprine to ameliorate post-treatment encephalopathy associated with African trypanosomiasis. Neuropathol. Appl. Neurobiol. 18: 619– 625. Hunter CA, Kennedy PG (1992). Immunopathology in central nervous system human African trypanosomiasis. J. Neuroimmunol. 36: 91–95. Inverso JA, De Gee AL, Mansfield JM (1988). Genetics of resistance to the African trypanosomes. VII. Trypanosome virulence is not linked to variable surface glycoprotein expression. J. Immunol. 140: 289–293. Iraqi F, Clapcott SJ, Kumari P, Haley CS, Kemp SJ, Teale AJ (2000). Fine mapping of trypanosomiasis resistance loci in murine advanced intercross lines. Mamm Genome. 11: 645–648. Jamonneau V, Garcia A, Frezil JL, et al (2000). Clinical and biological evolution of human trypanosomiasis in Cote d’Ivoire. Ann. Trop. Med. Parasitol. 94: 831–835. Jamonneau V, Garcia A, Ravel S, et al (2002). Genetic characterization of Trypanosomabruceigambiense and clinical evolution of human African trypanosomiasis in Cote d’Ivoire. Trop. Med. Int. Health. 7: 610–621. Jamonneau V, Ravel S, Garcia A, et al (2004). Characterization of Trypanosomabrucei s.1. infecting asymptomatic sleeping-sickness patients in Cote d’Ivoire: a new genetic group? Ann. Trop. Med. Parasitol. 98: 329–337. Jennings FW, Gichuki CW, Kennedy PG, et al (1997). The role of the polyamine inhibitor eflornithine in the neuropathogenesis of experimental murine African trypanosomiasis. Neuropathol. Appl. Neurobiol. 23: 225–234. 166 Glo. Adv. Res. J. Med. Med. Sci. Kazyumba G, Berney M, Brighouse G, Cruchaud A, Lambert PH (1986). Expression of the B cell repertoire and autoantibodies in human African trypanosomiasis. Clin. ExpImmunol. 65: 10–18. Kemp SJ, Iraqi F, Darvasi A, Soller M, Teale AJ (1997). Localization of genes controlling resistance to trypanosomiasis in mice. Nat. Genet. 16: 194–196. Kennedy PG (1999). The pathogenesis and modulation of the posttreatment reactive encephalopathy in a mouse model of Human African Trypanosomiasis. J. Neuroimmunol. 100: 36–41. Kennedy PGE (2004). Human African Trypanosomiasis of the CNS: current issues and challenges. J. Clin. Invest. 113: 496–504. Kitani H, Black SJ, Nakamura Y et al (2002). Recombinant tumor necrosis factor alpha does not inhibit the growth of African trypanosomes in axenic cultures. Infect. Immun. 70: 2210–2214. Lambert PH, Berney M, Kazyumba G (1981). Immune complexes in serum and in cerebrospinal fluid in African trypanosomiasis. Correlation with polyclonal B cell activation and with intracerebral immunoglobulin synthesis. J. Clin. Invest. 67: 77–85. Lapierre J, Coste M (1963). [Contribution to the study of a Trypanosomagambiense (Feo) strain isolated from a human case characterized by a duration of more than 20 years of clinically inapparentparasitemia]. Ann. Parasitol. Hum. Comp. 38: 757–782. Leal S, Acosta-Serrano A, Morita YS, Englund PT, Bohme U, Cross GA (2001). Virulence of Trypanosomabrucei strain 427 is not affected by the absence of glycosylphosphatidylinositol phospholipase C. Mol. Biochem. Parasitol. 114: 245–247. Lejon V, Buscher P, Magnus E, Moons A, Wouters I, Van Meirvenne N (1998). A semi-quantitative ELISA for detection of Trypanosomabruceigambiense specific antibodies in serum and cerebrospinal fluid of sleeping sickness patients. Acta Trop. 69: 151– 164. Lejon V, Lardon J, Kenis G, et al (2002). Interleukin (IL)-6, IL-8 and IL10 in serum and CSF of Trypanosomabruceigambiense sleeping sickness patients before and after treatment. Trans R Soc. Trop. Med. Hyg. 96: 329–333. Macaskill JA, Holmes PH, Jennings FW, Urquhart GM (1981). Immunological clearance of 75Se-labelled Trypanosomabrucei in mice. III. Studies in animals with acute infections. Immunol. 43: 691– 698. MacLean L, Chisi JE, Odiit M, et al (2004). Severity of Human African Trypanosomiasis in East Africa is associated with geographic location, parasite genotype and host-inflammatory cytokine response profile. Infect Immun. 72: 7040–7044. MacLean L, Odiit M, Okitoi D, Sternberg JM (1999). Plasma nitrate and interferon-gamma in Trypanosomabruceirhodesiense infections: evidence that nitric oxide production is induced during both early blood-stage and late meningoencephalitic-stage infections. Trans. R Soc. Trop. Med. Hyg. 93: 169–170. MacLean L, Odiit M, Sternberg JM (2001). Nitric oxide and cytokine synthesis in human African trypanosomiasis. J. Infect. Dis. 184: 1086–1090. MacLean L, Odiit M, Sternberg JM (2005). Intrathecal cytokine responses in Trypanosomabruceirhodesiense sleeping sickness patients. Trans. R Soc. Trop. Med. Hyg. Magez S, Geuskens M, Beschin A, et al (1997). Specific uptake of tumor necrosis factor-alpha is involved in growth control of Trypanosomabrucei. J. Cell Biol. 137: 715–727. Magez S, Radwanska M, Beschin A, Sekikawa K, De Baetselier P (1999). Tumor necrosis factor alpha is a key mediator in the regulation of experimental Trypanosomabrucei infections. Infect. Immun. 67: 3128–3132. Magez S, Stijlemans B, Baral T, De Baetselier P (2002). VSG-GPI anchors of African trypanosomes: Their role in macrophage activation and induction of infection-associated immunopathology. Microbes Infection; 4: 999–1006. Magez S, Stijlemans B, Radwanska M, Pays E, Ferguson MA, De Baetselier P (1998). The glycosyl-inositol-phosphate and dimyristoylglycerol moieties of the glycosylphosphatidylinositolanchor of the trypanosome variant-specific surface glycoprotein are distinct macrophage-activating factors. J. Immunol. 160: 1949–1956. Magez S, Truyens C, Merimi M, et al (2004). P75 tumor necrosis factorreceptor shedding occurs as a protective host response during African trypanosomiasis. J. Infect. Dis. 189: 527–539. Mansfield JM (1994). T-cell responses to the trypanosome variant surface glycoprotein: a new paradigm? Parasitol. Today. 10: 267– 270. Moore KW, De Waal Malefyt R, Coffman RL, O'Garra A (2001). Interleukin-10 and the interleukin-10 receptor. Annu. Rev. Immunol.; 19: 683–765. Murray M, Trail JC, Davis CE, Black SJ (1984). Genetic resistance to African Trypanosomiasis. J. Infect. Dis. 149: 311–319. Naessens J, Mwangi DM, Buza J, Moloo SK (2003). Local skin reaction (chancre) induced following inoculation of metacyclic trypanosomes in cattle by tsetse flies is dependent on CD4 T lymphocytes. Parasite Immunol. 25: 413–419. Namangala B, De Baetselier P, Noel W, Brys L, Beschin A (2001). Alternative versus classical macrophage activation during experimental African trypanosomosis. J. Leukoc. Biol. 69: 387–396. Okomo-Assoumou MC, Daulouede S, Lemesre JL, N’Zila-Mouanda A, Vincendeau P (1995). Correlation of high serum levels of tumor necrosis factor-alpha with disease severity in human African trypanosomiasis. Am. J. Trop. Med. Hyg. 53: 539–543. Omer FM, Kurtzhals JA, Riley EM (2000). Maintaining the immunological balance in parasitic infections: a role for TGF-beta? Parasitol. Today. 16: 18–23. Ormerod WE (1967). Taxonomy of the Sleeping Sickness Trypanosomes. J. Parasitol. 53: 824–830. Pays E, Vanhamme L, Perez-Morga D (2004). Antigenic variation in Trypanosomabrucei: facts, challenges and mysteries. Curr. Opin. Microbiol. 7: 369–374. Rhind SG, Sabiston BH, Shek PN et al (1997). Effect of melarsoprol treatment on circulating IL-10 and TNF-alpha levels in human African trypanosomiasis. Clin. Immunol. Immunopathol. 83: 185–189. Sarciron ME, Gherardi A (2000). Cytokines involved in Toxoplasmic encephalitis. Scand. J. Immunol. 52: 534–543. Schleifer KW, Filutowicz H, Schopf LR & Mansfield JM (1993). Characterization of T helper cell responses to the trypanosome variant surface glycoprotein. J. Immunol. 150: 2910–2919. Schleifer KW, Mansfield JM (1993). Suppressor macrophages in African trypanosomiasis inhibit T cell proliferative responses by nitric oxide and prostaglandins. J. Immunol. 151: 5492–5503. Schopf LR, Filutowicz H, Bi XJ & Mansfield JM (1998). Interleukin-4dependent immunoglobulin G1 isotype switch in the presence of a polarized antigen-specific Th1-cell response to the trypanosome variant surface glycoprotein. Infect. Immun. 66: 451–461. Sternberg JM (1998). Immunobiology of African trypanosomiasis. Chem. Immunol. 70: 186–199. Sternberg MJ, Mabbott NA (1996). Nitric oxide-mediated suppression of T cell responses during Trypanosomabrucei infection: soluble trypanosome products and interferon-gamma are synergistic inducers of nitric oxide synthase. Eur. J. Immunol. 26: 539–543. Tabel H, Kaushik RS, Uzonna JE (2000). Susceptibility and resistance to Trypanosomacongolense infections. Microbes Infect. 2: 1619– 1629. Taylor KA, Mertens B (1999). Immune response of cattle infected with African trypanosomes. Mem. Inst. Oswaldo Cruz. 94: 239–244. Tsenova L, Bergtold A, Freedman VH, Young RA, Kaplan G (1999). Tumor necrosis factor alpha is a determinant of pathogenesis and disease progression in mycobacterial infection in the central nervous system. Proc. Natl. Acad. Sci. USA. 96: 5657–5662. Turner CM, Barry JD (1989). High frequency of antigenic variation in Trypanosomabruceirhodesiense infections. Parasitol. 99: 67–75. Vanhamme L, Pays E, McCulloch R, Barry JD (2001). An update on antigenic variation in African trypanosomes. Trends Parasitol. 17: 338–343. Webb H, Carnall N, Vanhamme L, et al (1997). The GPI-phospholipase C of Trypanosomabrucei is nonessential but influences parasitemia in mice. J. Cell Biol. 139: 103–114. Musa et al. 167 Wery M, Burke J (1972). Human ‘healthy carriers’ of Trypanosoma (brucei type) discovered by immunofluorescence test in the Republique Democratique du Congo. Trans. R. Soc. Trop. Med. Hyg. 66: 332–333. WHO (1998). Control and Surveillance of African Trypanosomiasis. WHO Tech Report Series. 881: 1–113. Xong HV, Vanhamme L, Chamekh M, et al (1998). A VSG expression site-associated gene confers resistance to human serum in Trypanosomarhodesiense. Cell. 95: 839–846.







© Copyright 2025