
Clinical Practice Guidelines for the Prevention and Gastrointestinal Mucositis
2026 Mucositis: Perspectives and Clinical Practice Guidelines Supplement to Cancer Clinical Practice Guidelines for the Prevention and Treatment of Cancer Therapy–Induced Oral and Gastrointestinal Mucositis Edward B. Rubenstein, M.D.1 Douglas E. Peterson, D.M.D., Ph.D.2 Mark Schubert, D.D.S., M.S.D.3 Dorothy Keefe, M.D.4 Deborah McGuire, R.N., Ph.D.5 Joel Epstein, D.M.D., M.S.D.6 Linda S. Elting, Dr.P.H.7 Philip C. Fox, D.D.S.8 Catherine Cooksley, Ph.D.7 Stephen T. Sonis, D.M.D., D.M.Sc.9 for the Mucositis Study Section of the Multinational Association of Supportive Care in Cancer and the International Society for Oral Oncology. 1 Department of Palliative Care and Rehabilitation Medicine, The University of Texas M. D. Anderson Cancer Center, Houston, Texas. BACKGROUND. Oral and gastrointestinal (GI) mucositis can affect up to 100% of patients undergoing high-dose chemotherapy and hematopoietic stem cell transplantation, 80% of patients with malignancies of the head and neck receiving radiotherapy, and a wide range of patients receiving chemotherapy. Alimentary track mucositis increases mortality and morbidity and contributes to rising health care costs. Consequently, the Multinational Association of Supportive Care in Cancer and the International Society for Oral Oncology assembled an expert panel to evaluate the literature and to create evidence-based guidelines for preventing, evaluating, and treating mucositis. METHODS. Thirty-six panelists reviewed literature published between January 1966 and May 2002. An initial meeting in January 2002 produced a preliminary draft of guidelines that was reviewed at a second meeting the same year. Thereafter, a writing committee produced a report on mucositis pathogenesis, epidemiology, and scoring (also included in this issue), as well as clinical practice guidelines. RESULTS. Panelists created recommendations from higher levels of evidence and suggestions when evidence was of a lower level and there was a consensus regard- 2 Department of Oral Diagnosis, University of Connecticut Health Center, Farmington, Connecticut. 3 Department of Oral Medicine, Fred Hutchinson Cancer Research Center, Seattle, Washington. 4 Department of Medical Oncology, Royal Adelaide Hospital, Adelaide, Australia. 5 School of Nursing, University of Pennsylvania, Philadelphia, Pennsylvania. 6 Department of Oral Medicine and Diagnostic Sciences, College of Dentistry, Chicago, Illinois. 7 Department of Biostatistics and Applied Mathematics, The University of Texas M. D. Anderson Cancer Center, Houston, Texas. 8 Department of Oral Medicine, Carolinas Medical Center, Charlotte, North Carolina. 9 Division of Oral Medicine, Brigham and Women’s Hospital, Boston, Massachusetts. Supported by unrestricted educational grants to the Mucositis Study Section of the Multinational Association of Supportive Care in Cancer (MASCC) and the International Society for Oral Oncology (ISOO). Cor- porate sponsors include Amgen (Thousand Oaks, CA), GelTex Pharmaceuticals (Waltham, MA), Helsinn Healthcare SA (Pazzallo, Switzerland), Human Genome Sciences (Rockville, MD), McNeil Consumer and Specialty Pharmaceuticals (Fort Washington, PA), MGI Pharma (Bloomington, MN), MedImmune (Gaithersburg, MD), OraPharma (Warminster, PA), and RxKinetix (Louisville, CO). Panelists included the following individuals: Andrei Barasch, D.M.D., M.D.Sc., University of Detroit Mercy School of Dentistry (Detroit, MI); B. Nebiyou Bekele, Ph.D., The University of Texas M. D. Anderson Cancer Center (Houston, TX); Rene-Jean Bensadoun, M.D., Center Antoine-Lacassagne (Nice, France); Michael Brennan, D.D.S., M.H.S., Carolinas Medical Center (Charlotte, NC); Mark Chambers, D.D.S., The University of Texas M. D. Anderson Cancer Center (Houston, TX); Catherine Cooksley, Ph.D., The University of Texas M. D. Anderson Cancer Center (Houston, TX); Marcio Da Fonseca, D.D.S., M.S., University of Michigan School of Dentistry (Ann Arbor, MI); Kathryn L. Damato, R.D.H., M.S., C.C.R.P., University of Connecticut Health Center (Farmington, CT); Betty © 2004 American Cancer Society DOI 10.1002/cncr.20163 Published online in Wiley InterScience (www.interscience.wiley.com). Daniel, B.S.N., M.S., The University of Texas M. D. Anderson Cancer Center (Houston, TX); J. Peter Donnelly, Ph.D., University Hospital Nijmegen (Nijmegen, The Netherlands); Linda Elting, Dr.P.H., The University of Texas M. D. Anderson Cancer Center (Houston, TX); Loree Oberle-Edwards, R.D.H., M.S., Scripps Center for Dental Care (La Jolla, CA); Douglas Peterson, D.M.D., Ph.D., University of Connecticut Health Center (Farmington, CT); Judith Raber-Durlacher, D.D.S., Ph.D., Leiden University Medical Center (Leiden, The Netherlands); Ann Rose, Ph.D., Vicro (Washington, DC); Edward B. Rubenstein, M.D., The University of Texas M. D. Anderson Cancer Center (Houston, TX); Mark M. Schubert, D.D.S., M.S.D., Seattle Cancer Care Alliance (Seattle, WA); Sol Silverman, M.A., D.D.S., University of San Francisco (San Francisco, CA); Stephen T. Sonis, D.M.D., D.M.Sc., Brigham and Women’s Hospital (Boston, MA); Fred Spijkervet, D.D.S., Ph.D., University Hospital Groningen (Groningen, The Netherlands); Diane Talentowski, D.D.S., Loyola University Medical Center (Maywood, Illinois); Inger von Bu¨ltzingslo¨wen, D.D.S., Ph.D., Go¨teborg University (Gothenburg, Sweden); and Ralph Wong, M.D., University of Manitoba (Winnipeg, MB, Canada). Clinical Practice Guidelines for Mucositis/Rubenstein et al. 2027 ing the interpretation of the evidence by the panel. Panelists identified gaps in evidence that made it impossible to recommend or not recommend use of specific agents. CONCLUSIONS. Oral/GI mucositis is a common side effect of many anticancer therapies. Evidence-based clinical practice guidelines are presented as a benchmark for clinicians to use for routine care of appropriate patients and as a springboard to challenge clinical investigators to conduct high-quality trials geared toward areas in which data are either lacking or conflicting. Cancer 2004;100(9 Suppl):2026 –2046. © 2004 American Cancer Society. KEYWORDS: stomatitis, oral mucositis, gastrointestinal mucositis, clinical practice guidelines. O ral mucositis is a common complication of cytoreductive cancer chemotherapy and radiotherapy. It is the dose-limiting toxicity of treatment modalities like accelerated fractionation and hyperfractionated radiotherapy and of interventions that combine chemotherapy and radiotherapy. Its counterpart, gastrointestinal (GI) mucositis, is a well recognized toxicity associated with some standard-dose chemotherapy regimens commonly used in cancer treatment and with radiotherapy encompassing any area of the GI tract. Oral and GI mucositis may occur in up to 100% of patients undergoing high-dose chemotherapy with hematopoietic stem cell transplantation (HSCT). For patients receiving this treatment, a 1-point increase in an oral mucositis score has been found to be associated with a significant increase in days with fever, risk of infection, additional days of total parenteral nutrition, use of intravenous narcotic analgesics, total hospital charges, and 100-day mortality.1 From the patient’s perspective, oral mucositis is one of transplantation’s most debilitating side effects.2 Recognizing the dramatic clinical and psychologic effects of mucositis and the barrier that this condition sometimes becomes to what may be life-saving ther- apy, physicians, oral oncologists, investigators at the National Cancer Institute, and others have sought to bring to the attention of the oncology community the clinical and economic impact of mucosal injury secondary to high-dose cancer therapy.1 During the last 5 years, new models of the basic mechanisms of progression and healing and proposals for new research and treatment strategies have emerged.1,3 Biotechnology and pharmaceutical industry researchers have joined academic clinical investigators in their attempts to develop interventions to prevent or treat oral and GI mucositis. Although the basic mechanisms of mucosal barrier injury still are being explored, several significant findings have become evident from clinical investigations. First, because researchers employ different mucositis scoring systems, each one measuring different endpoints or using one-of-a-kind composite endpoints, comparisons across studies are difficult to make. Furthermore, no comprehensive battery of questions provides a means of uniform evaluation. Second, variations among designs of investigations have prevented generalization to related cohorts, preventing reproducibility and inhibiting progress. Third, patterns of patient care appear to have evolved from a variety of clinical practice domains, in- Edward B. Rubenstein’s current address: MGI Pharma, Bloomington, Minnesota. Address for reprints: Dorothy Keefe, M.D., Department of Medical Oncology, Royal Adelaide Hospital Cancer Center, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000, Australia; Fax: (011) 618-8232-2148; E-mail: dkeefe@mail.rah.sa.gov.au Dr. Rubenstein has received research funding from and is a member of the speakers program and advisory board at Merck (Whitehouse Station, NJ); he owns common stock in and is a member of the advisory board at MGI Pharma; and he is a member of the advisory boards at Endo Pharmaceuticals, McNeil Consumer and Specialty Pharmaceuticals, and OSI Pharmaceuticals. Dr. Peterson has served as a paid consultant for Aesgen, Inc. (Princeton, NJ). Dr. Schubert is a member of the advisory boards at Endo Pharmaceuticals, OSI Pharmaceuticals (Melville, NY), and McNeil Consumer and Specialty Pharmaceuticals. Dr. Keefe has received research funding and speaker’s honoraria from Amgen. Dr. Elting has received speaker’s honoraria from McNeil Consumer and Specialty Pharmaceuticals and from Endo Pharmaceuticals (Chadds Ford, PA). Dr. Sonis has served as a consultant for Biomodels and Affiliates (Wellesley, MA). Received December 19, 2003; accepted January 22, 2004. 2028 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 TABLE 1 Levels of Evidence, Grades of Recommendation, and Guideline Hierarchya Measure Level of evidence I II III IV V Grade of recommendation A B C D Guideline classification/hierarchy Recommendation Suggestion No guideline possible a Source of evidence Metaanalysis of multiple well designed, controlled studies; randomized trials with low false-positive and false-negative errors (high power) At least one well designed experimental study; randomized trials with high false-positive or high false-negative errors or both (low power) Well designed, quasiexperimental studies, such as nonrandomized, controlled, single-group, pretest-posttest comparison, cohort, time, or matched case–control series Well designed, nonexperimental studies, such as comparative and correlational descriptive and case studies Case reports and clinical examples Evidence of Type I or consistent findings from multiple studies of Type II, III, or IV Evidence of Type II, III, or IV and findings are generally consistent Evidence of Type II, III, or IV, but inconsistent findings Little or no systematic empiric evidence A recommendation is reserved for guidelines that are based on Level I or Level II evidence A suggestion is used for guidelines that are based on Level III, Level IV, and Level V evidence; this implies panel consensus on the interpretation of this evidence No guideline possible is used when there is insufficient evidence on which to base a guideline; this conclusion implies 1) that there is little or no evidence regarding the practice in question or 2) that the panel lacks a consensus on the interpretation of existing evidence. Adapted from: Somerfield M, Padberg J, Pfister D, et al. ASCO clinical practice guidelines: process, progress, pitfalls, and prospects. Classic Papers Current Comments. 2000;4:881–886.4 cluding oral oncology, radiation oncology, medical oncology, and hematology, and the effect of this amalgamation is unclear. Finally, because most current treatments seem to have evolved from empiricism rather than from evidence, a methodologically vigorous review of the literature on which treatments were based seemed appropriate. In response to these findings and developments, the Multinational Association of Supportive Care in Cancer and the International Society for Oral Oncology (MASCC/ISOO) created the Mucositis Study Section in 1998 to bring together experts from a number of disciplines in oncology to address important issues in mucositis treatment and research. Accordingly, in 2000, the study section established a panel of experts to develop evidenced-based guidelines for the prevention and treatment of oral and GI mucositis associated with anticancer therapy. The resulting guidelines are intended for oral health care specialists, oncology and oral medicine patients, oncologists, clinical investigators, and policy makers. This report describes the objectives, methods, and results of the MASCC/ISOO Mucositis Study Section’s deliberations. MATERIALS AND METHODS Expert Panel Composition The panel was composed of 36 oral oncologists, radiation oncologists, hematologists, medical oncologists, surgeons, pathologists, nurses, dental hygienists, basic scientists, microbiologists, epidemiologists, outcomes researchers, and a medical librarian from a comprehensive cancer center. The panel included established basic science, clinical, and health services investigators whose research involves mucosal barrier injury and who publish in the peer-reviewed literature. Process Overview Because of the anticipated scope of the literature search results and the size of the panel, the topic was subdivided into subtopics, which were assigned to working groups of two to five members. These subtopics included terminology, epidemiology (primary and agent-specific or therapy-specific), basic oral care and oral care protocols, bland oral rinses, analgesics, cryotherapy, topical anesthetics, antimicrobial agents (systemic and topical), growth factors and cytokines, biologic mucosal protectants, antiinflammatory agents, complementary and alternative medicine (including natural agents), low-energy laser therapy, and hemorrhage. The GI Mucositis Working Group was responsible for initial review of all the same areas as they related to GI mucositis. In their work, panelists employed a systematic weighting of both level and grading of the evidence (Table 1).4 – 6 Clinical Practice Guidelines for Mucositis/Rubenstein et al. Literature Review and Data Collection A medical librarian, working with the panel cochairs, conducted the initial Medline and cancer literature search. Literature was drawn from as early as January 1966 and as late as November 21, 2001. Additional work extended the search through May 31, 2002. An initial search of the English-language medical literature published from January, 1966 to October, 2001 produced more than 500,000 publications related to cancer and its therapies. Mucositis is not a National Library of Medicine medical subject heading (MeSH), so stomatitis was used as the primary search term and was combined with cancer. Because stomatitis is a National Library of Medicine MeSH heading, articles are indexed by that term, even if they use the term mucositis. Although the term stomatitis is used widely to refer to any mucosal inflammation, by definition, it is restricted to inflammatory diseases of the mouth, whereas the term mucositis has a broader definition that encompasses inflammation of any mucous membrane. After the literature was narrowed to articles about cancer therapy–related mucosal toxicity, citations were sorted using the topic areas defined for the smaller working groups, as described above. Furthermore, panel members were encouraged to contact other investigators and sources for unpublished information that could be used to assist in the guideline. Guideline Development Based on Evidence The literature was distributed to each group along with instructions and scoring sheets based on methods for reviewing and scoring the literature, according to Hadorn et al.7 Each group returned its scoring sheets along with a bibliography of all publications reviewed. These were collated, copied, and distributed to each panel member at a guideline development conference held in Houston, Texas, on January 16 –20, 2002. Each group presented draft guidelines before the entire panel using the structured literature review and guideline development methods of the American Society for Clinical Oncology.4 The guideline hierarchy allows for two subtypes of guidelines: 1) recommendations and 2) suggestions (Table 1). The panel discussed each guideline to ensure compliance with published standards for guideline development.8 The panel updated the draft guidelines at its second meeting, on June 23, 2002, in Boston, Massachusetts. The article, which was prepared by a writing committee with assistance from a medical editor, was circulated to each panel member in two draft forms, giving them two additional opportunities to comment on the levels of evidence and grading of the recom- 2029 mendations. All panel members approved the final version submitted for publication, and the guidelines are presented herein (Table 2). Conflict of Interest Disclosure and Financial Disclosure The cost of the conference and administrative services for developing the guidelines was paid from unrestricted educational grants in support of the MASCC/ ISOO Mucositis Study Section. The following companies provided grant support: Amgen (Thousand Oaks, CA), GelTex Pharmaceuticals (Waltham, MA), Helsinn Healthcare SA (Pazzallo, Switzerland), Human Genome Sciences (Rockville, MD), McNeil Consumer and Specialty Pharmaceuticals (Fort Washington, PA), MGI Pharma (Bloomington, MN), MedImmune (Gaithersburg, MD), OraPharma (Warminster, PA), and RxKinetix (Louisville, CO). Each company was allowed to have representatives attend the guideline development conference, but representatives were not allowed to attend the closed administrative sessions or participate in any of the discussions or deliberations of the panel. Furthermore, companies were informed that they would not be allowed access to the guidelines until after they were published. The methods for the guidelines’ development, all drafts, and final content and style were controlled strictly by the panel. Each panel member was required to complete a standardized conflict of interest disclosure form requiring revelation of all ties to any health care company, companies, commercial products, or products in development that potentially could be affected by the guidelines’ development and promulgation. Disclosure included employment, consultancies, stock ownership, speaking honoraria, research funding, expert testimony, and membership on company advisory boards. The panel made decisions on a case-bycase basis about whether a member’s role should be limited as a consequence of a conflict of interest. Revision Dates The panel expects to review the guidelines annually as a routine activity of the MASCC/ISOO Mucositis Study Section and to reconvene every 3 years or more frequently, as information warrants, to discuss potential changes to the guidelines. BIOLOGIC BASIS AND PATHOGENESIS Oral Mucosal Injury Mucosal injury is the collective consequence of a number of concurrent and sequential biologic processes. After radiotherapy or chemotherapy, oral mucositis is heralded by an initiation phase that is characterized by injury to tissues of the submucosa. After the up-regulation of a series of early-response genes, 2030 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 TABLE 2 Summary of Clinical Practice Guidelines for Care of Patients with Oral and Gastrointestinal Mucositis I. Oral mucositis Foundations of care 1. The panel suggests the use of oral care protocols that include patient education in an attempt to reduce the severity of mucositis from chemotherapy or radiation therapy. 2. The panel recommends patient-controlled analgesia with morphine as the treatment of choice for oral mucositis pain in patients undergoing HSCT. Radiotherapy: prevention 3. To reduce mucosal injury, the panel recommends the use of midline radiation blocks and three-dimensional radiation treatment. 4. The panel recommends benzydamine for prevention of radiation-induced mucositis in patients with head and neck cancer receiving moderate-dose radiotherapy. 5. The panel recommends that chlorhexidine not be used to prevent oral mucositis in patients with solid tumors of the head and neck who are undergoing radiotherapy. Standard-dose chemotherapy: prevention 6. The panel recommends that patients receiving bolus 5-FU chemotherapy undergo 30 min oral cryotherapy to prevent oral mucositis. 7. The panel suggests using 20–30 min oral cryotherapy in an attempt to decrease mucositis in patients treated with bolus doses of edatrexate. 8. The panel recommends that acyclovir and its analogues not be used routinely to prevent mucositis. Standard-dose chemotherapy: treatment 9. The panel recommends that chlorhexidine not be used to treat established oral mucositis. High-dose chemotherapy with or without TBI plus HSCT: prevention 10. The panel does not recommend the use of pentoxifylline to prevent mucositis in patients undergoing HSCT. 11. LLLT requires expensive equipment and specialized training. Because of interoperator variability, clinical trials are difficult to conduct, and their results are difficult to compare; nevertheless, the panel is encouraged by the accumulating evidence in support of LLLT. For centers capable of supporting the necessary technology and training, the panel suggests the use of LLLT in an attempt to reduce the incidence of oral mucositis and its associated pain in patients receiving high-dose chemotherapy or chemoradiotherapy before HSCT. II. Gastrointestinal mucositis Radiotherapy: prevention 1. The panel suggests using 500 mg oral sulfasalazine twice daily to help reduce the incidence and severity of radiation-induced enteropathy in patients receiving external-beam radiotherapy to the pelvis. 2. Oral sucralfate does not prevent acute diarrhea in patients with pelvic malignancies undergoing external beam radiotherapy; and, compared with placebo, it is associated with more gastrointestinal side effects, including rectal bleeding. Consequently, the panel recommends that oral sucralfate not be used. 3. The panel recommends that 5-aminosalicylic acid and its related compounds mesalazine and olsalazine not be used to prevent gastrointestinal mucositis. Radiotherapy: treatment 4. The panel suggests the use of sucralfate enemas to help manage chronic, radiation-induced proctitis in patients with rectal bleeding. Standard-dose and high-dose chemotherapy: prevention 5. The panel recommends either ranitidine or omeprazole for the prevention of epigastric pain after treatment with cyclophosphamide, methotrexate, and 5-FU or treatment with 5-FU with or without folinic acid chemotherapy. Standard-dose and high-dose chemotherapy: treatment 6. When loperamide fails to control diarrhea induced by standard-dose or high-dose chemotherapy associated with HSCT, the panel recommends octreotide at a dose of at least 100 g administered subcutaneously twice daily. Combined chemotherapy and radiotherapy: prevention 7. The panel suggests the use of amifostine to reduce esophagitis induced by concomitant chemotherapy and radiotherapy in patients with nonsmall cell lung cancer. HSCT: hematopoietic stem cell transplantation; 5-FU: 5-fluorouracil; TBI: total-body irradiation; LLLT: low-level laser therapy. changes are observed in the endothelium, connective tissue, and extracellular matrix that are mediated by reactive oxygen species (ROS), the ceramide pathway, and a number of transcription factors, including nuclear factor-kappa  (NF-B). The initial injury precipitates connective tissue deterioration and the rapid up-regulation of a second set of genes that results in direct and indirect signaling and early apoptosis of clonogenic stem cells in the basal epithelium. The proinflammatory cytokines (tumor necrosis factor-␣, interleukin 1, and interleukin 6) are likely to be among signaling molecules. These signaling molecules also have the ability to amplify the up-regulation of transcription factors (e.g., NF-B) further, leading to production of additional proinflammatory cytokines, tissue injury, and apoptosis. Reduced renewal of mucosal epithelium occurs despite focal bursts of hyperproliferative activity in response to the early up-regulation of genes associated with epithelium healing. Epithelial apoptosis and necrosis exceed hyperproliferative activity and result in an ulcerative phase in which full-thickness mucosal damage is apparent. The ulcerative phase is exacerbated by local bacterial colonization, which results in a barrage of cell wall products penetrating into the submucosa and amplifying damaging mechanisms. Increased transcription factor activity and levels of cytokines and other mediators drive additional local responses, including angiogenesis. Ultimately, healing occurs as healthy epithelium migrates from the wound margins, stimulated by signals from the submucosa. A complete discussion of the biologic basis and pathogenesis of oral and GI mucositis may be found in the accompanying article in this issue.9 GI Mucosal Injury The pathobiology of mucositis in the alimentary tract beyond the oral cavity is similar to that described above for oral mucositis and poses the same potential threat to successful therapy because of dose delays or dose reductions. Setting the GI tract apart in its manifestation of mucosal injury are the morphologic and functional differences between its sections. These largely account for the differences in functional and Clinical Practice Guidelines for Mucositis/Rubenstein et al. symptomatic outcomes between oral and GI mucositis induced by cancer therapy. The plethora of rapidly dividing cells in the GI tract make the tract particularly vulnerable to cytotoxic chemotherapeutic agents. On Day 1 after chemotherapy, the first abnormality observed may be an increase in apoptosis. Afterward, reductions in crypt length, villus area, and mitotic index follow, with each of these quantities reaching a nadir on Day 3. By Day 5, rebound hyperplasia is underway, and eventually, normalization follows.10 Abdominal pain, bloating, and diarrhea begin around Day 3 and settle by Day 7, when oral symptoms typically are appearing. Functional changes, such as sugar permeability, however, persist after recovery from symptoms and morphologic changes.11 Intestinal permeability is also one of a number of changes that occur during fractionated radiotherapy. Along with histologic injury, intestinal permeability actually is maximal midcourse. These improve toward the end of the radiotherapy course, despite persistent injury and noticeably increasing symptoms, because of compensatory changes.12,13 Nonetheless, in many patients, radiation’s toxicities result in such chronic functional disabilities as malabsorption and dysmotility, in contrast to chemotherapy’s more transient effects. Histologic changes include mucosal atrophy, intestinal wall fibrosis, and vascular sclerosis. Lifethreatening complications, including intestinal obstruction, perforation, or fistula formation, can characterize the clinical course. Efforts to understand better the biologic and histologic mechanisms and the quantitative roles of different factors in GI mucositis are made more difficult by the inaccessibility of significant GI segments and the problems inherent in obtaining sequential biopsy specimens. Approaches to alleviating toxicity also have included efforts to elucidate the mechanisms of action of newer drugs.12 EPIDEMIOLOGY The incidence of oral and GI mucositis varies, depending on chemotherapy regimen and on treatment modality. Prolonged or profound oral and GI mucositis leads to significant pain and morbidity, excess costs for supportive care and hospitalization, increased frequency of infection, and chemotherapy dose delays and reductions.15,16 Excluding very high-risk regimens, HSCT, and radiotherapy, rates of mucositis are generally in the 5–15% range. However, administration of 5-flurouracil (5-FU), with or without leucovorin, is associated with oral mucositis in as much as 40% of patients.17 Grade 3– 4 oral mucositis approaches 10 –15% among 5-FU recipients.18 Similarly, 2031 administration of irinotecan often is associated with severe GI mucositis, which affects ⬎ 20% of patients receiving certain doses and regimens. Approximately 75– 85% of bone marrow transplantation recipients experience mucositis, and in some studies, oral mucositis is the most common and most debilitating side effect reported.1,2 Conditioning regimens that include melphalan are associated with particularly high rates of oral mucositis.19 The risk of radiation-induced mucositis varies with the site of radiotherapy, dosage, and fractionation. Radiotherapy to the head and neck or to the pelvis or abdomen is associated with an increased incidence of Grade 3 and Grade 4 oral or GI mucositis, respectively, often exceeding 50% of patients.20 Among patients undergoing head and neck radiotherapy, pain and decreased oral function may persist long after the conclusion of therapy.21 Accelerated fractionation increases the risk of mucositis to ⬎ 70% of patients in most trials.20 Oral mucositis is particularly profound and prolonged among HSCT recipients who receive total-body irradiation for conditioning. CLINICAL PRACTICE GUIDELINES FOR CARE OF PATIENTS WITH ORAL MUCOSITIS Foundations of Care Basic oral care Lack of a consistent definition of which elements constitute basic oral care and highly variable study designs do not allow a guideline for basic oral care related to mucositis prevention or treatment. There is insufficient evidence to conclude that actions such as brushing teeth using foam ‘toothbrushes’ or swabs, flossing, or using topical fluoride will prevent or treat cancer therapy–induced mucositis. A number of topical agents (bland rinses, antimicrobial rinses) that often are included in basic oral care are addressed in other sections of the guidelines. Nonetheless, it is important to recognize that although there is not sufficient scientific evidence to provide a guideline for basic oral care, its importance in maintaining mucosal health, integrity, and function generally is accepted. The purpose of basic oral care is to reduce the impact of the oral microbial flora, reduce cancer therapy–related symptoms of pain and bleeding, and prevent soft tissue infections that may have systemic sequelae. In addition, maintenance of good oral hygiene will reduce the risk of dental complications, including caries and gingivitis. For these reasons, basic oral care is an important component of care of the patient with cancer.22 Although the importance of effective oral hygiene has been described in many articles, the methods and techniques employed typically are based on preference and anecdotal expe- 2032 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 rience. A single study23 demonstrated that tooth brushing reduced the number of oral lesions in patients receiving cancer chemotherapy. Using foam toothbrushes is not equivalent to toothbrushing and cannot be recommended for plaque control or caries prevention. Oral care protocols and patient education Guideline: The panel suggests the use of oral care protocols that include patient education in an attempt to reduce the severity of mucositis from chemotherapy or radiotherapy (level of evidence, III; grade of recommendation, B). Oral care protocols are used in an attempt to prevent and manage mucositis, with an emphasis on feasibility, adherence, and comprehensive patient education about mucositis and oral care. The current review did not evaluate specific agents or approaches used in protocols, and insufficient evidence prevents the recommendation of one protocol over any other. Because oral care has long been integral to nursing practice,24,25 nurses are the health professionals who usually provide oral care to patients with mucositis; thus, many of the reports are drawn from the nursing literature. Implementation of oral care protocols is generally a systematic process in which specific agents are not the main focus. Rather, the important components of this implementation include feasibility, adherence, performance, and outcomes. Patient education refers to comprehensive, theory-based, educational approaches that prepare individuals for medical procedures, including what to expect and how to cope, an approach that also has been termed psychoeducation,26 because it addresses both physical and psychologic aspects of the symptoms (e.g., distress, anxiety). Programmatic reports provided support (although not empiric evidence) for the value of implementing institutionalized oral care protocols or standards. Three randomized clinical trials, despite their flaws, and three nonrandomized studies also yielded support. The findings of these investigations form the foundation of the suggestion above. With the specific objective of reducing mucositis, Graham et al.27 initiated a unit-based oral care protocol and teaching program and documented a reduction in mucositis. Larson et al.28 used the PRO-SELF Mouth Aware Program in a study of outpatients receiving chemotherapy and demonstrated feasibility of the program in maintaining oral hygiene. To improve the consistency of oral care, Yeager et al.29 implemented an oral care standard in two inpatient hematology/oncology units and demonstrated feasibility, tolerability, and adherence in patients with leukemia and those undergoing transplantation. Improved oral status (i.e., reduced mucositis or increased oral comfort) was reported in three randomized clinical studies,30 –32 and only one32 study reported no change in mucositis at the conclusion of the study. Despite flaws, including failure to blind the investigator in one of the studies, measurement issues, and a wide range of sample sizes (15–150 participants), the collective results suggest that using a systematic protocol improves patient outcomes. A fourth randomized clinical trial33 did not show a statistically significant difference between controls and those undergoing the intervention; however, participants who were taught the protocols performed oral hygiene routines more frequently compared with the control group and reported feeling more prepared to manage their symptoms. Three quasiexperimental, nonrandomized studies of oral care protocols also support their use in reducing the incidence or severity of mucositis. Beck24 reported on the implementation and testing of an oral care protocol in patients with cancer and found that oral cavity physical condition improved and infection decreased with implementation of an oral care protocol. Levy-Polack et al.34 reported that pediatric patients with leukemia who followed a daily preventive protocol (plaque removal, chlorhexidine rinse, iodopovidone, and nystatin) experienced a significant decrease in moderate mucositis and candidiasis and had improved oral hygiene. Cheng et al.35 found that an oral care protocol (tooth brushing, chlorhexidine rinse [0.2%], and saline) resulted in a 38% reduction in incidence and a significant reduction in severity and associated oral pain in pediatric patients with cancer. The remaining studies did not test oral care protocols formally but, rather, surveyed institutions or health professionals about oral care. They revealed widely disparate practices and little agreement on standardized approaches to oral care.36 – 40 Palliative care (including pain management) Palliation of mucositis and acute oral pain is an important component of patient care. Approaches include the use of systemic analgesics and other individual agents, palliative mixtures of agents (sometimes called magic or miracle mouthwash), coating agents, and topical anesthetics/analgesics. Systemic analgesics. Guideline: The panel recommends patient-controlled analgesia (PCA) with morphine as the treatment of choice for oral mucositis pain in patients undergoing HSCT (level of evidence, I; grade of recommendation, A). Control of mucositis- Clinical Practice Guidelines for Mucositis/Rubenstein et al. induced pain is achieved by PCA with intravascular morphine sulfate.41– 49 Level I evidence supports PCA for oral mucositis pain in patients who undergo HSCT, but there is little evidence to recommend its use in other patients and settings. Although other opiates may achieve similar pain control, morphine appears to require relatively lower drug doses and may be tolerated better. Pediatric populations also can use PCA efficiently. Initial studies of transdermal fentanyl have been published,44,49 but further study is required to confirm its efficacy. Despite the limited evidence described above, in general, pain management for mucositis should be governed by prevailing clinical practice guidelines, such as those promulgated by the World Health Organization and the Agency for Healthcare Research and Quality for managing acute pain.50,51 These guidelines include accepted approaches for the use of nonopioids, opioids, adjuvant medications, and assessment tools. Depending on the individual patient population, numerous routes may be considered, including oral, transmucosal (oral and rectal), and transdermal routes, as well as various intravenous approaches (continuous infusion, bolus, and PCA). Topical preparations and other approaches. Various topical preparations have been in widespread use for the treatment of mucositis and its accompanying pain. The most common ingredients include viscous lidocaine, benzocaine, milk of magnesia, kaolin, pectin, chlorhexidine, and dyphenhydramine. Topical analgesics that can be considered include the single agents benzydamine (see below) and morphine.52 Many topical agents have been compounded in mixtures. There is no significant evidence of the effectiveness or tolerability of these mixtures.31,34,53– 61 Some of these preparations may be minimally superior to normal saline, although the evidence is not convincing. Thus, the lack of compelling evidence prevents the panel from recommending any palliative mixture for therapeutic intent in oral mucositis. However, because concern exists regarding absorption of amide anesthetics (e.g., lidocaine) through damaged mucosal surfaces, both individual agents and palliative mixtures require further study to determine their toxicity and efficacy. Radiotherapy: Prevention Use of blocks and three-dimensional treatment delivery Guideline: To reduce mucosal injury, the panel recommends the use of midline radiation blocks and three-dimensional radiation treatment (level of evidence, II; grade of recommendation, B). The effects of altering the delivery of cytotoxic therapy, without sig- 2033 nificant dose modification, have been studied. The quality and modest numbers of publications describing these methods preclude the establishment of specific guidelines. However, it has been shown that oral mucosal injury secondary to radiotherapy may be reduced significantly by the use of midline radiation blocks62 and by three-dimensional treatment delivery, which reduces the volume of mucosa exposed to irradiation.63 Benzydamine Guideline: The panel recommends benzydamine for the prevention of radiation-induced mucositis in patients with head and neck cancer receiving moderatedose radiotherapy (level of evidence, I; grade of recommendation, A). Benzydamine hydrochloride is a unique agent with antiinflammatory effects. It is a nonsteroidal drug (although not a classic nonsteroidal antiinflammatory drug) that is applied topically. In addition to its antiinflammatory properties, benzydamine has analgesic, anesthetic, and antimicrobial capabilities, which make exact classification of this drug difficult. Recent studies have demonstrated that benzydamine also inhibits the production and effects of proinflammatory cytokines, particularly TNF-␣. These findings favor antiinflammatory effects as the main mode of action for this agent. It has been shown in single-center and multicenter, randomized, controlled clinical trials that topical benzydamine reduces the frequency and severity of ulcerative oral lesions and decreases pain in radiation-induced oral mucositis.64 – 68 Although it is not currently available in the United States, a pivotal Phase III trial of this agent is enrolling patients actively. Benzydamine hydrochloride has been studied most extensively for the prevention and reduction of the severity of radiation-induced mucositis of the oral cavity. Several small, double-blinded, randomized trials were reported in the 1980s. Two early studies64,67 suggested that benzydamine was effective in reducing the severity of the pain associated with oral mucositis. In 2001, the results of a large, multicenter, doubleblinded, randomized trial were published68 and demonstrated that benzydamine improved the ulcer-free rate and diminished the incidence of ulceration and erythema. That study used a sophisticated mucositis scoring system that measured the severity of mucositis and duration of mucositis by using an area-under-thecurve analysis. The study also demonstrated a delay in the need for analgesics in patients who were treated with benzydamine compared with patients who were treated with placebo. The study’s conclusions were based on cumulative radiation doses of 50 grays (Gy), and the efficacy of the drug with higher doses or with 2034 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 combination chemotherapy was not established. In a small subgroup of patients who received accelerated radiation, benzydamine was not effective. Chlorhexidine Guideline: The panel recommends that chlorhexidine not be used to prevent oral mucositis in patients with solid tumors of the head and neck who are undergoing radiotherapy (level of evidence: II; grade of recommendation, B). Chlorhexidine is a broad-spectrum, topical antiseptic. The evidence from three studies was consistent in showing that this agent had no impact in preventing the development of oral mucositis in patients with solid tumors of the head and neck undergoing radiotherapy.69 –71 Chlorhexidine may be used for its antiplaque and antifungal properties as part of an oral care protocol. Standard-Dose Chemotherapy: Prevention Cryotherapy Cryotherapy with bolus doses of 5-FU. Guideline: The panel recommends that patients receiving bolus 5-FU chemotherapy undergo 30 minutes of oral cryotherapy to prevent oral mucositis (level of evidence, II; grade of recommendation, A). It was hypothesized that placing ice chips in the mouth, starting 5 minutes before 5-FU bolus injection and continuing for a total of 30 minutes, would cause cooling of the oral cavity, which would lead to vasoconstriction. It was suggested that the vasoconstriction would allow less 5-FU to reach the oral mucosa, thereby attenuating 5-FUinduced mucositis. One randomized but nonblinded study of 95 patients was conducted in patients who were receiving bolus 5-FU. Mucositis was evaluated by questionnaire. Results from that trial illustrated that the group receiving oral cryotherapy exhibited a reduction of approximately 50% in mucositis.72 Cascinu et al.73 randomly allocated 84 patients who were receiving 5-FU to receive oral cryotherapy, and again, a reduction of approximately 50% in mucositis was observed among those who received oral cryotherapy. A subsequent randomized clinical trial of oral cryotherapy for either 30 minutes or 60 minutes reported that extending the duration of oral cryotherapy did not provide additional benefit; therefore, 3-minute cryotherapy was recommended.74 A study of ocular cryotherapy (cold packs over the eyes) also showed reduction in 5-FU-induced conjunctivitis (P ⫽ 0.001).75 Cryotherapy with edatrexate. Guideline: The panel suggests using 20 –30 minutes of oral cryotherapy in an attempt to decrease mucositis in patients who are treated with bolus doses of edatrexate (level of evi- dence, IV; grade of recommendation, B). Recent nonrandomized studies suggest that oral cryotherapy may reduce oral mucositis related to edatrexate.76 –78 The rationale for its use in this situation is related to the short serum half-life of edatrexate. It should be noted that oral cryotherapy is not expected to be useful in preventing oral mucositis in patients receiving 5-FU by continuous infusion or in patients undergoing administration of such agents as methotrexate, doxorubicin, or other agents with a long serum half-lives. This therapy’s low cost and minimal toxicity justify its use. Acyclovir Guideline: The panel recommends that acyclovir and its analogues not be used routinely to prevent mucositis (level of evidence, II; grade of recommendation, B). Acyclovir is effective in reducing herpes simplex virus (HSV) infection in patients with leukemia or lymphoma,79,80 but oral mucositis still develops in patients routinely receiving acyclovir or one of its prodrugs for prophylaxis. This suggests that HSV infection plays little or no role in causing oral mucositis. Standard-Dose Chemotherapy: Treatment Chlorhexidine Guideline: The panel recommends that chlorhexidine not be used to treat established oral mucositis (level of evidence, II; grade of recommendation, A). Research has failed to produce evidence that supports the use of chlorhexidine to treat established mucositis. A well designed, multicenter, double-blind clinical trial conducted in 23 outpatient and office settings evaluated the effectiveness of a standardized oral care protocol (PRO-SELF) plus ‘magic’ mouthwash, salt and soda rinses, and chorhexidine in reducing the duration of pain associated with oral mucositis induced by stomatotoxic chemotherapy.58 Patients initially were evaluated by a physician or nurse to confirm the presence of oral mucositis. Patients then underwent a standardized oral care protocol that taught self-care, and they subsequently received a 12-day supply of study mouthwash. There was no difference in the efficacy of the three treatments in time to resolution of mucositis or in pain relief; however, the salt and soda rinses represented the least costly option. This study clearly demonstrated no significant difference in pain ratings among the treatment groups, despite the fact that magic mouthwash included lidocaine and the chlorhexidine mouthwash contained alcohol, which can sting on contact with oral mucosa. Other studies also failed to find any benefit of chlorhexidine as a treatment for established oral mucositis.81,82 Clinical Practice Guidelines for Mucositis/Rubenstein et al. High-Dose Chemotherapy With or Without Total-Body Irradiation plus HSCT: Prevention Pentoxifylline Guideline: The panel does not recommend the use of pentoxifylline to prevent mucositis in patients undergoing HSCT (level of evidence, II; grade of recommendation, B). Six clinical trials utilizing pentoxifylline to prevent mucositis were evaluated.83– 88 Five of six trials had no placebo control and no investigator blinding. No randomization was made in four of the six clinical trials. Of the six trials, four had significant flaws in their designs. Both of the well designed, randomized trials87,88 demonstrated that pentoxifylline failed to prevent the development of mucositis. Low-level laser therapy Guideline: Low-level laser therapy (LLLT) requires expensive equipment and specialized training. Because of interoperator variability, clinical trials are difficult to conduct, and their results are difficult to compare; nevertheless, the panel is encouraged by the accumulating evidence in support of LLLT. The panel suggests that at centers that are capable of supporting the necessary technology and training, LLLT should be used in an attempt to reduce the incidence of oral mucositis and its associated pain in patients who are receiving high-dose chemotherapy or chemoradiotherapy prior to HSCT (level of evidence, II; grade of recommendation, B). Over the last several years, appropriate laboratory and clinical evidence has been accumulating steadily to support the use of LLLT to promote biostimulation applications. It has been reported that LLLT promotes wound healing and reduces pain and inflammation. Different effects appear to be related to laser characteristics (wavelength and energy dose) and the particular type of tissue being treated. Helium-neon (He-Ne) laser ( ⫽ 632.8 nm) treatment has been the most frequently studied form of LLLT for the prevention or reduction of oral mucositis and oral pain associated with cancer therapy (including HSCT).89,90 Research currently is underway on the use of diode lasers with wavelengths ranging from 650 to 905 nm. It appears that laser therapy produces no toxicity and is atraumatic to patients. However, LLLT requires specific (often expensive) equipment, and treatment can be time consuming. CLINICAL PRACTICE GUIDELINES FOR THE PREVENTION AND TREATMENT OF GI MUCOSITIS Radiotherapy: Prevention Sulfasalazine Guideline: The panel suggests the use of 500 mg of sulfasalazine orally twice daily to help reduce the in- 2035 cidence and severity of radiation-induced enteropathy in patients receiving external-beam radiotherapy to the pelvis (level of evidence, II; grade of recommendation, B). Radiation-induced enteropathy with abdominal pain and diarrhea occurs in 75–90% of patients receiving external-beam radiotherapy for such common pelvic malignancies as prostate, rectal, or cervical cancer and typically begins in the second or third week of treatment. Kilic et al.91 conducted a well designed, randomized, double-blind controlled trial of sulfasalazine (500 mg twice daily) or placebo in 87 patients who had a variety of pelvic malignancies and were scheduled to receive 46 –50 Gy in 23–25 fractions of external-beam radiotherapy to the whole pelvis. Whereas the incidence of Grade 1– 4 diarrhea was 55% among sulfasalazine-treated patients, it was 86% among patients receiving the placebo (P ⫽ 0.001). None of the patients in the sulfasalazine-treated group experienced Grade 4 diarrhea, compared with 16% of patients in the placebo group. There was no significant difference in toxicity between the two treatment groups. Further work is required to explain the mechanism underlying the difference between sulfasalazine and other closely related compounds such as 5-amino salicylic acid (5-ASA), melsalazine, and olsalazine (see below). Sucralfate Guideline: Oral sucralfate does not prevent acute diarrhea in patients with pelvic malignancies who are undergoing external-beam radiotherapy. Compared with placebo, sucralfate was found to be associated with increased GI side effects, including rectal bleeding. Consequently, the panel recommends that oral sucralfate not be used. (level of evidence, I; grade of recommendation, A). The North Central Cancer Treatment Group conducted a well designed, randomized controlled trial of oral sucralfate (1.5 gm every 6 hours) and a placebo in 125 patients treated with 45–53.5 Gy external-beam radiotherapy in fractions of 1.7–2.1 Gy per day. Among the 123 evaluable patients, diarrhea was moderate to severe in 53% of patients receiving sucralfate but only 41% of patients receiving placebo. Significantly more patients in the sucralfate group reported fecal incontinence, the need for protective clothing, and more intense nausea compared with the placebo group (P ⬍ 0.05 for all comparisons).92 In a multicenter, double-blind trial involving patients with clinically localized prostate malignancies who were scheduled to receive definitive radiotherapy (ⱖ 60 Gy, with a superior limit of field below the greater sciatic notch), 335 patients were randomized to receive either 3 gm oral sucralfate twice daily or 2036 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 placebo.93 There was no significant difference in patient self-reports of stool frequency, consistency, mucus, or pain (P ⬎ 0.20 for all comparisons); however, the sucralfate-treated group had an increased incidence of rectal bleeding (64%) compared with the placebo group (47%; P ⫽ 0.001). O’Brien et al.94 evaluated the use of sucralfate rectal enemas versus a placebo, beginning at the onset of radiotherapy for prostate malignancy and continuing for 2 weeks after completion of radiotherapy, in preventing acute proctitis. Patients were assessed monthly for 3 months and then every 6 months for 5 years. Sucralfate was no better than placebo at reducing the risk of acute radiation-induced proctitis. Cox proportional hazards modeling indicated that patient self-assessment of moderate or severe rectal pain was the best predictor of subsequent development of late radiation-related toxicity. There were no significant differences in the rates of late rectal bleeding between the sucralfatetreated and placebo-treated groups.94 5-ASA, mesalazine, and olsalazine Guideline: The panel recommends that 5-ASA and the related compounds mesalazine and olsalazine not be used for the prevention of GI mucositis (level of evidence, I; grade of recommendation, A). In three separate studies,95–97 it was found that 5-ASA, mesalazine, and olsalazine were of no benefit or caused more diarrhea than placebo did in patients receiving pelvic radiotherapy. Baughan et al.95 randomized 73 patients who were undergoing pelvic radiotherapy to receive either 5-ASA or placebo and reported more diarrhea (P ⫽ 0.070), more severe diarrhea (P ⫽ 0.014), and more days per week with diarrhea (P ⫽ 0.026) in the 5-ASA group compared with the placebo group. In a doubleblind, multicenter study, Resbeut et al.96 randomized 153 patients who were receiving ⱖ 45 Gy of externalbeam pelvic radiotherapy to receive either 4 gm mesalazine per day or placebo. Diarrhea rates were similar in both groups (69% with mesalazine, compared with 66% with placebo; P ⫽ 0.22), although the mesalazine-treated group had more severe diarrhea at Day 15 compared with the placebo group (P ⫽ 0.006). Martenson et al.97 randomized patients who were undergoing pelvic radiotherapy to receive either 500 mg olsalazine administered orally twice daily or placebo. Those authors terminated the study early for the 58 evaluable patients, because diarrhea occurred more frequently and was more severe among the olsalazinetreated patients. Radiotherapy: Treatment Sucralfate enemas Guideline: The panel suggests using sucralfate enemas to help manage chronic radiation-induced proctitis in patients with rectal bleeding (level of evidence, III; grade of recommendation, B). It is believed that chronic radiation-induced proctitis or proctosigmoiditis is due to intestinal wall fibrosis along with vascular sclerosis leading to ischemia. Its incidence ranges from 2% to 20%. Risk factors for radiation-induced proctitis include higher doses of radiotherapy, intracavitary radiation, and the use of radiosensitizers. This condition may be more common in patients who have experienced it previously. Clinical manifestations include diarrhea, tenesmus, urgency, and rectal bleeding, which frequently is severe enough to require blood transfusions. Kochhar et al.98,99 randomized 37 consecutive patients with radiation-induced proctitis to a 4-week course of sulfasalazine (3 gm orally plus rectal prednisolone enemas twice daily) or rectal sucralfate enemas twice daily plus an oral placebo. Both regimens were associated with significant clinical improvement and with improvement observed at endoscopic evaluation. In a second study, the same investigators evaluated 26 consecutive patients with radiation-induced proctitis and persistent rectal bleeding whose condition had failed to respond to bulk-forming agents, sulfasalazine, and topical corticosteroids.99 All patients were treated with sucralfate rectal enemas (20 mL 10% sucralfate suspension in water twice daily). After 4 weeks of therapy, all 26 patients exhibited a reduction in the severity of rectal bleeding (P ⬍ 0.01). At a median follow-up of 45.5 months, 17 patients had no further bleeding. Other therapies for chronic radiation proctitis with bleeding include argon beam coagulation, electrocoagulation, formalin treatment, and hyperbaric oxygen treatment.100 –112 Although these therapies have not been examined in randomized controlled trials, the results from cohort studies are encouraging, especially with respect to laser and formalin treatments. Because of the lack of randomized trials and the limited experience with these therapies, the panel believes that a specific guideline is not warranted at this time. Standard-Dose Chemotherapy: Prevention Ranitidine and omeprazole Guideline: The panel recommends either ranitidine or omeprazole for the prevention of epigastric pain after treatment with cyclophosphamide, methotrexate, and 5-FU or after treatment with 5-FU with or without folinic acid chemotherapy (level of evidence, II; grade Clinical Practice Guidelines for Mucositis/Rubenstein et al. of recommendation, A). In two well designed, randomized, controlled trials led by the same principal investigator,113,114 it was found that these two drugs were beneficial. One hundred eighty-two patients with endoscopically normal gastric and duodenal mucosa (or with ⬍ 3 erosions) were assigned randomly to receive misoprostol (400 g twice daily), omeprazole (20 mg once daily), or placebo prior to treatment with cyclophosphamide, methotrexate, and 5-FU or with 5-FU alone. Seven days after completing the second course of chemotherapy, all patients underwent follow-up endoscopy. Omeprazole was more effective than either misoprostol or placebo in reducing clinically significant epigastric pain and/or heartburn, and its use was associated with fewer gastric and duodenal ulcerations.113 In a follow-up study,114 228 patients with endoscopically normal epigastric and duodenal mucosae (or with ⬍ 3 erosions) were assigned randomly to receive omeprazole (20 mg once daily), ranitidine (300 mg once daily), or placebo before treatment either with cyclophosphamide, methotrexate, and 5-FU or with 5-FU. Global endoscopic scores after chemotherapy were significantly higher than pretreatment scores in patients who were randomized to receive placebo or ranitidine, but not omeprazole. Acute ulcers were less common in patients who received omeprazole (P ⫽ 0.0001) or ranitidine (P ⫽ 0.0315) compared with patients who received placebo; likewise, epigastric pain and heartburn were significantly less common in the omeprazole (P ⫽ 0.00124) and ranitidine (P ⫽ 0.038) groups compared with the placebo group. Standard-Dose Chemotherapy: Treatment Octreotide Guideline: When loperamide fails to control diarrhea induced by standard-dose or high-dose chemotherapy associated with HSCT, the panel recommends octreotide at a dose of at least 100 g administered subcutaneously twice daily (level of evidence, II: grade of recommendation, A). Chemotherapy-induced diarrhea is a common clinical problem associated with certain drugs used to treat colon cancer and other solid tumors (5-FU, irinotecan) and with high-dose chemotherapy coupled with HSCT. Irinotecan-induced diarrhea occurs in 2 phases: an acute syndrome (within the first 24 hours), which is mediated by acetylcholine and blocked by atropine, followed by a delayed phase, which is inflammatory. The rate of National Cancer Institute Common Toxicity Criteria Grade 3– 4 delayed-phase diarrhea may approach 25%. Octreotide, a somatostatin analogue, regulates intestinal water and electrolyte transport, inhibits gut hormones (serotonin, vasoactive intestinal peptide, 2037 gastrin, insulin, secretin, glucagons, and pancreatic polypeptide), and preserves epithelial barrier function. Multiple clinical trials of octreotide have demonstrated that it is effective in reducing chemotherapyinduced diarrhea associated with standard-dose chemotherapy.115–120 Four studies involving patients who received high-dose chemotherapy with HSCT suggest that octreotide also is effective in that setting. In preclinical models of fractionated radiotherapy,121,122 octreotide administration during radiation and for 2 weeks after radiation was complete was associated with a reduction in both acute and subsequent chronic intestinal toxicity. Additional research is needed to determine the role of octreotide as a mucosal protectant for patients receiving radiotherapy with or without concomitant chemotherapy. Combined Chemotherapy and Radiotherapy: Prevention Amifostine Guideline: The panel suggests using amifostine to reduce esophagitis induced by concomitant chemotherapy and radiotherapy in patients with nonsmall cell lung cancer (level of evidence, III: grade of recommendation, C). The use of combined-modality therapy, such as concomitant radiotherapy and chemotherapy in nonsmall cell lung cancer, improves tumor control rates but is associated with higher rates of acute and chronic esophagitis.123 Consequently, investigators have employed strategies utilizing radioprotectants to minimize these toxicities. Recently, Komaki et al.124 reported interim results from a prospective randomized Phase III study of combined chemotherapy and radiotherapy with and without amifostine for patients with nonsmall cell lung cancer. Both groups received 1.2 Gy per fraction, with 2 fractions per day administered 5 times weekly, along with oral etoposide (50 mg twice daily) administered 30 minutes before radiotherapy on Days 1–10 and repeated on Day 29 and cisplatin (50 mg/m2) administered intravenously on Days 1, 8, 29, and 36. The amifostine-treated group received 500 mg amifostine intravenously twice weekly before chemoradiation. Severe esophagitis (defined as the need for morphine intake to control pain) was significantly lower in the group that received amifostine (7.4%) compared with the group that did not receive amifostine (31%; P ⫽ 0.03). These preliminary findings in 53 patients also revealed a lower rate of acute pneumonitis (3.7%) among patients who received amifostine compared with the control group (23%; P ⫽ 0.037). Transient hypotension was significantly more common in patients who received amifostine (70%) compared with the control group (3.8%; 2038 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 P ⫽ 0.0001); however, only 1 patient discontinued therapy because of hypotension. The panel has limited its suggestion to the specific clinical situation described above and offers the following to clarify its view of the evidence. Amifostine is a thiol-containing prodrug that is dephosphorylated by alkaline phosphatase to its active metabolite WR1065, which acts as a potent scavenger of ROS. Theoretically, this mechanism of action would serve as a rational basis for using amifostine as an agent to prevent the initiation of mucositis induced by chemotherapy, radiotherapy, and concomitant chemoradiotherapy. Currently, amifostine is approved by the U.S. Food and Drug Administration (FDA) only for reducing the cumulative renal toxicity associated with repeated doses of cisplatin in patients with advanced ovarian cancer or nonsmall cell lung cancer and for reducing the incidence of moderate-to-severe xerostomia in patients undergoing postoperative radiotherapy for head and neck malignancies. Some reports have demonstrated that the use of amifostine is associated with a reduction in mucositis in patients receiving radiotherapy to the head and neck,124 pelvis,125 and thorax,127 whereas other studies have failed to demonstrate similar results.128 –130 The use of amifostine is complicated by its acute toxicity (namely, nausea, emesis, hypotension, allergic reactions, and taste disturbances), which may necessitate the interruption or discontinuation of amifostine therapy. Furthermore, it is not clear whether the acute toxicity of amifostine can be reduced by performing subcutaneous administration, as opposed to intravenous administration, which is the approved technique.126,131 Another significant concern regarding the use of amifostine is the selectivity of its action on normal tissues versus its action on tumor cells. There are theoretic concerns that amifostine not only may protect normal tissue but also may protect tumor cells from the effects of radiotherapy. No adequately powered trials addressing this issue have been published, although the clinical trials in the literature do not suggest that amifostine-treated patients have a survival disadvantage compared with control groups. Accordingly, the panel considers the evidence on amifostine to be insufficient for the creation of guidelines for the settings of radiotherapy alone and chemotherapy alone. DISCUSSION Using a modern, evidence-based approach, the MASCC/ISOO panel evaluated the medical literature of the last 36 years; in general, the quality of the reported clinical trials failed to meet current standards. This is not to say that these studies do not have value; however, the methodologic deficiencies compromised the panel’s ability to construct comprehensive, prescriptive guidelines. Consequently, the panel offers the preceding guidelines as a benchmark and a starting point for future revisions. Putting these findings in a current context also requires that the Writing Committee summarize recent developments that were reported after the close of the panel’s full review. Since the panel last met, a number of agents for the prevention and treatment of mucositis have been reported at international meetings, in abstracts or articles, and in press releases from industry. Although some of these agents appear promising, and the evidence supporting their use is of a high level, the panel was unable to evaluate the evidence with the same rigor it applied to the literature, which was subjected to full panel review. Nevertheless, these agents are of sufficient interest to warrant a brief summary. Late-Breaking Reports Human keratinocyte growth factor 2 (KGF-2; repifermin) was evaluated in a multicenter Phase II trial involving 42 patients with various malignancies who received conditioning regimens with chemotherapy before undergoing autologous HSCT. Repifermin significantly reduced the incidence of Grade 2– 4 oral mucositis.132 Recombinant human keratinocyte growth factor 1 (rHuKGF-1; palifermin) was evaluated in a multicenter, randomized, double-blind, placebocontrolled Phase II trial in patients with head and neck cancer who received standard or hyperfractionated radiotherapy with concomitant chemotherapy.133 The palifermin-treated group had a lower incidence and shorter duration of mucositis compared with the group that received placebo. In a pivotal Phase III trial involving patients undergoing transplantation for a variety of hematologic malignancies, palifermin significantly reduced the incidence and duration of severe oral mucositis (P ⬍ 0.0001).134 AES-14, which is L-glutamine administered in a proprietary vehicle that increases its uptake, was evaluated in a Phase III trial in patients with solid tumors who were at high risk for chemotherapy-induced oral mucositis.135 Patients who received AES-14 had a lower incidence of Grade ⱖ 2 mucositis compared with patients who received placebo. Iseganan, an analog of protegrin-1 and a naturally occurring peptide with broad-spectrum microbicidal activity, was evaluated in a randomized, double-blind, placebo-controlled study in patients undergoing transplantation who were receiving stomatotoxic therapy. Unfortunately, 102 patients (32%) were affected by a drug-dispensing error caused by a flawed computerized allocation system. Between the 163 patients Clinical Practice Guidelines for Mucositis/Rubenstein et al. who were randomized to receive iseganan and the 160 patients who were randomized to receive placebo, the incidence of oral mucositis was not statistically significantly different.136 In a subgroup of patients who were scheduled for HSCT and who underwent conditioning regimens with high potential for inducing mucositis, oral triclosan reportedly decreased the incidence and duration of ulcerative oral mucositis.137 In 2002, Gelclair was approved by the FDA as a Class 1 medical device for the management and relief of pain associated with oral lesions of various etiologies, including oral mucositis or stomatitis, which may be caused by chemotherapy or radiotherapy. In an open-label study involving 30 patients, Gelclair appeared to be safe and effective in improving pain scores, swallowing endpoints, and nutritional endpoints. Controlled clinical trial data are not yet available for this mixture of polyvinylpyrrolidone, sodium hyaluronate, and glycyrrhetinic acid. Insufficient Evidence To facilitate future research and to point out areas that would benefit from well designed trials, the panel provides a compilation of evidence that was reviewed yet was considered insufficient to support a recommendation for or against the use of certain agents (Table 3).57,60,124,127,138 –205 The rationales and potential mechanisms of action for agents investigated as potential therapies are quite varied, and such agents include mucosal surface protectants, antiinflammatory agents, antimicrobial agents, growth factors, and agents that are difficult to classify. From a mechanistic standpoint, some of these agents are potentially attractive, because they are associated with rationales for targeting specific pathways known to be involved in the etiology of mucositis; however, the evidence in support of these agents’ efficacy is not rigorous enough for the creation of a prescriptive guideline. Amifostine is a good example of one such agent. The rationale underlying the use of other potential agents for the prevention or treatment of mucositis appears to be limited, based on our current understanding of the pathobiology of mucositis. Based on their proposed mechanisms, antimicrobial agents, such as combined polymyxin E, tobrymycin, and amphotericin or single-agent iseganan, appear to have no associated mechanistic rationale for the prevention of mucositis and probably could provide benefit only for patients with late-stage ulcerative mucositis, in which bacterial superinfection occurs. Lessons Learned and Future Directions The panel believes that many of the agents studied are potentially useful, but the trials’ shortcomings pre- 2039 vented the formulation of guidelines. Trials included single studies that were underpowered, studies that lacked an adequate control arm, studies that were not investigator blinded or patient blinded, and studies that suffered from other design deficiencies. In other instances, multiple studies reported conflicting results, which prevented the panel from establishing prescriptive recommendations or suggestions. New, well designed, sufficiently powered, and appropriately executed studies are needed to determine the value of these various agents, which may or may not be effective in preventing or treating mucositis. To be useful and to permit comparisons between studies, new investigations should include a control arm that represents the current standard of care, and they should use a mucositis scoring scale with well established psychometric properties. Standardized oral care protocols should be the minimum for the control arm. These standard elements should be coupled with protocol-prescribed analgesics and other supportive care along with appropriate investigator and patient blinding. Future mucositis trials should have adequate sample sizes for testing hypotheses. Trials of radioprotectants should include longterm follow-up to calculate time to disease progression, along with response rates and survival rates, to ensure that patients do not suffer from poor tumor control in the interest of better supportive care. Furthermore, the studies should report withdrawal rates, adverse event rates, and reasons for withdrawal. Differences in reasons for withdrawal are important, and investigators should count patients who withdraw because of mucositis treatment failure or toxicity associated with the treatment agent as well as patients who withdraw because of other toxicities associated with anticancer therapy. Important secondary endpoints should include resource utilization, functional outcomes, nutritional endpoints, infection rates, and bleeding endpoints. Alimentary tract mucositis, which encompasses both oral and GI mucositis, is a complex process. It is very unlikely that a single therapy will prevent or treat this side effect of anticancer strategies. Local or topical therapies may be useful in certain circumstances, or they may be combined with other topical agents or systemically active agents. The bioavailability of local therapies should be evaluated early-stage to mid-stage during development of clinical programs. It is likely that in the future, combinations of agents will be used to prevent or treat difficult mucositis problems like those seen in patients receiving concomitant chemotherapy and radiotherapy for head and neck cancer or lung cancer or in patients receiving high-dose chemotherapy with allogeneic stem cell transplantation. The 2040 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 TABLE 3 Agents with Evidence Insufficient to Support a Guideline Agent Oral Amifostine Azelastine Chamomile Chlorhexidine Clarithromycin Clindamycin Coatings for surface, mucoadherent (various) Cyanoacrylate-based tissue adhesives Cytokines and growth factorsa Granulocyte–colony-stimulating factor Granulocyte-macrophage–colony-stimulating factor Gelclair Immunoglobulin Nonsteroidal antiinflammatory drugs Pilocarpine Polaprezinc PTA Povidone iodine Prostaglandin E2 analogue Prostaglandin inhibitor Silver nitrate Sodium alginate Steroids Tetrachlorodecaoxide Traumeel S Tretinoin cream (0.1%) Gastrointestinal Amifostine Butyric acid Glutamine Misoprostol Use Reference(s) Prevention Prevention Prevention and treatment Prevention Antonadou et al., 2001127; Komaki et al., 2002124 Osaki et al., 1994138 Carl and Emrich, 1991139; Fidler et al., 1996140 Prevention Therapy Pain management Pain management Prevention and treatment Prevention and treatment Treatment Prevention Treatment Prevention and treatment Prevention Treatment Prevention Prevention and treatment Treatment Treatment Treatment Treatment Treatment Treatment Treatment Treatment Treatment Treatment Treatment McGaw and Belch, 1985141; Ferretti et al., 1990142; Rutkauskas and Davis, 1993143; Epstein et al., 1992144; Dodd et al., 199657 Yuen et al., 2001145 Donnelly et al., 1993146 Ishii et al., 1990147; LeVeque et al., 1992148; Oguchi et al., 1998149; Redding and Haveman, 1999150; Yamamura et al., 1999151 Kutcher, 2001152; Perez et al., 2000153; Narang, 2001154 Crawford et al., 1999155; Schneider et al., 1999156; Mascarin et al., 1999157; Karthaus et al., 1998158 Makkonen et al., 2000159; Tejedor et al., 2000160; Crawford et al., 1999155; Wagner et al., 1999161; Chi et al., 1995162; Bez et al., 1999163; Saarilahti et al., 2001164; Hejna et al., 2001165; Sprinzl et al., 2001166; van der Lelie et al., 2001167; Cartee et al., 1995168 Smith, 2001169; Innocenti et al., 2002170 Schedler et al., 1994171; Schedler et al., 1997172; Mose et al., 1997173 Pillsbury et al., 1986174; Rymes et al., 1996175; Tanner et al., 1981176 Warde et al., 2002177; Awidi et al., 2001178 Masayuki et al., 2002179 Bondi et al., 199760,b Rahn et al., 1997180; Adamietz et al., 1998181 Matejka et al., 1990182; Porteder et al., 1988183; Pretnar et al., 1989184; Labar et al., 1993185; Hanson et al., 1997186 Pillsbury et al., 1986174; Tanner et al., 1981176 Maciejewski et al., 1991187 Oshitani et al., 1990188 Leborgne et al., 1998189; Barrett, 1990190; Wolff et al., 1998191 Malik et al., 1997192 Oberbaum, 1998193; Oberbaum et al., 2001194 Cohen et al., 1997195 Kligerman et al., 1992198; Mitsuhashi et al., 1993199; Montana et al., 1992200 Vernia et al., 2000201 Daniele et al., 2001202; Savarese et al., 2000203; Decker-Baumann et al., 1999204 Khan et al., 2000205 PTA: polymyxin E, tobrymycin, and amphotericin. a For more information on cytokines and growth factors, see Discussion. b These investigators found that PTA was statistically significantly superior to a rinse containing diphenhydramine and local anesthetic, but they expressed doubt that the clinical effect would be significant. incidence of mucositis in children receiving anticancer therapy has been widely reported. Furthermore, studies of antimucositis agents in the pediatric population are rare. The panel encourages clinical development programs to begin testing promising agents in children with cancer who are at risk of alimentary tract mucositis, and clinical investigators are encouraged to publish rates of mucositis from anticancer therapies in a fashion similar to those published for adults (see the accompanying article in this issue9). Finally, the field of mucositis research needs to develop a scoring system or classification system to determine the mucotoxic potential of anticancer regimens. The panel encourages investigators reporting studies of newer anticancer strategies to report mucositis rates of these treatment modalities using standardized methods. Lumping all grades of mucositis together prevents supportive care experts from learning the mucotoxic potential of newer treatments. This classification system is needed for use in clinical trials of newer agents Clinical Practice Guidelines for Mucositis/Rubenstein et al. that can prevent or treat this significant side effect of anticancer therapy and for making comparisons among trials of promising agents. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. Sonis ST, Oster G, Fuchs H, et al. Oral mucositis and the clinical and economic outcomes of hematopoietic stem-cell transplantation. J Clin Oncol. 2001;19:2201–2205. Bellm LA, Epstein JB, Rose-Ped A, Martin P, Fuchs HJ. Patient reports of complications of bone marrow transplantation. Support Care Cancer. 2000;8:33–39. Sonis J, Doukas D, Klinkman M, Reed B, Ruffin MT. Applicability of clinical trial results to primary care. JAMA. 1998; 280:1746. Somerfield M, Padberg J, Pfister D, et al. ASCO clinical practice guidelines: process, progress, pitfalls, and prospects. Classic Papers Current Comments. 2000;4:881– 886. Sackett DL. Rules of evidence and clinical recommendations on the use of antithrombotic agents. Chest. 1989;95(2 Suppl):2S– 4S. Cook DJ, Guyatt GH, Laupacis A, Sackett DL. Rules of evidence and clinical recommendations on the use of antithrombotic agents. Chest. 1992;102(4 Suppl):305S–311S. Hadorn D, Baker D, Hodges J, Hicks N. Rating the quality of evidence for clinical practice guidelines. J Clin Epidemiol. 1996;49:749 –754. Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelines following guidelines? The methodological quality of clinical practice guidelines in the peer-reviewed medical literature. JAMA. 1999;281:1900 –1905. Sonis ST, Elting LS, Keefe D, et al. Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer. 2004;100(Suppl):1995–2025. Keefe DM, Brealey J, Goland GJ, Cummins AG. Chemotherapy for cancer causes apoptosis that precedes hypoplasia in crypts of the small intestine in humans. Gut. 2000;47:632– 637. Keefe DM. The effect of cytotoxic chemotherapy on the mucosa of the small intestine [Ph.D. dissertation]. Adelaide: University of Adelaide, 1998. Carratu R, Secondulfo M, de Magistris L, et al. Assessment of small intestinal damage in patients treated with pelvic radiotherapy. Oncol Rep. 1998;5:635– 639. Hovdenak N, Fajardo L, Hauer-Jensen M. Acute radiation proctitis: a sequential clinicopathologic study during pelvic radiotherapy. J Radiat Oncol Biol Phys. 2000;48:1111–1117. Ikuno N, Soda H, Watanabe M, Oka M. Irinotecan (CPT-11) and characteristic mucosal changes in the mouse ileum and cecum. J Natl Cancer Inst. 1995;87:1876 –1883. Sonis ST, Peterson DE, McGuire DB, Williams DA. Prevention of mucositis in cancer patients. J Natl Cancer Inst Monogr. 2001;29:1–2. Ruescher T, Sodeifi A, Scrivani S, Kaban L, Sonis ST. The impact of mucositis on alpha hemolytic streptococcal infection in patients undergoing autologous bone marrow transplantation for hematological malignancies. Cancer. 1998;82: 2275–2281. Popescu RA, Norman A, Ross PJ, Parikh B, Cunningham D. Adjuvant or palliative chemotherapy for colorectal cancer in patients 70 years or older. J Clin Oncol. 1999;17:2412–2418. Meta-Analysis Group in Cancer. Toxicity of fluorouracil in patients with advanced colorectal cancer: effect of admin- 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 2041 istration schedule and prognostic factors. Meta-Analysis Group in Cancer. J Clin Oncol. 1998;16:3537–3541. Wardley AM, Jayson GC, Swindell R, et al. Prospective evaluation of oral mucositis in patients receiving myeloablative conditioning regimens and haemopoietic progenitor rescue. Br J Haematol. 2000;110:292–299. Trotti A, Byhardt R, Stetz J, et al. Common Toxicity Criteria: Version 2.0. An improved reference for grading the acute effects of cancer treatment: impact on radiotherapy. Int J Radiat Oncol Biol Phys. 2000;47:13– 47. Epstein JB, Emerton S, Kolbinson DA, et al. Quality of life and oral function following radiotherapy for head and neck cancer. Head Neck. 1999;21:1–11. Solomon CS, Shaikh AB, Arendorf TM. An efficacious oral health care protocol for immunocompromised patients. Spec Care Dentist. 1995;15:228 –233. Bonnaure-Mallet M, Bunetel L, Tricot-Doleux S, Guerin J, Bergeron C, LeGall E. Oral complications during treatment of malignant diseases in childhood: effects of tooth brushing. Eur J Cancer. 1998;34:1588 –1591. Beck S. Impact of a systematic oral care protocol on stomatitis after chemotherapy. Cancer Nurs. 1979;2:185–199. Beck S. Mucositis. In: Yarbro C, Frogge M, Goodman M, editors. Cancer symptom management. Sudbury, MA: Jones & Bartlett, 1999:328 –343. Christman N, Kirchhoff K, Oakley M. Concrete objective information. In: Bulecheck G, McCloskey J, editors. Nursing interventions: essential nursing treatments (2nd edition). Philadelphia: WB Saunders, 1992:140 –180. Graham K, Pecoraro D, Ventura M, Meyer C. Reducing the incidence of stomatitis using a quality assessment and improvement approach. Cancer Nurs. 1993;16:117–122. Larson P, Miaskowski C, MacPhail L, et al. The PRO-SELF Mouth Aware Program: an effective approach for reducing chemotherapy-related mucositis. Cancer Nurs. 1998;21:263– 268. Yeager K, Webster J, Crain M, Kasow J, McGuire D. Implementation of an oral care standard for leukemia and transplantation patients. Cancer Nurs. 2000;23:40 – 47. Borowski B, Benhamou E, Pico J, Laplanche A, Margainaud J, Hayat M. Prevention of oral mucositis in patients treated with high-dose chemotherapy and bone marrow transplantation: a randomized controlled trial comparing two protocols of dental care. Eur J Cancer B Oral Oncol. 1994;30B:93– 97. Dudjak L. Mouth care for mucositis due to radiation therapy. Cancer Nurs. 1987;10:131–140. Kenny S. Effect of two oral care protocols on the incidence of stomatitis in hematology patients. Cancer Nurs. 1990;13: 345–353. McGuire D, Owen D, Peterson D. Nursing interventions for acute oral pain and mucositis. Oncol Nurs Forum. 1998;25: 341. Levy-Polack MP, Sebelli P, Polack NL. Incidence of oral complications and application of a preventive protocol in children with acute leukemia. Spec Care Dentist. 1998;18: 189 –193. Cheng KK, Molassiotis A, Chang AM, Wai WC, Cheung SS. Evaluation of an oral care protocol intervention in the prevention of chemotherapy-induced oral mucositis in paediatric cancer patients. Eur J Cancer. 2001;37:2056 –2063. Dando S. Cancer patients’ and health care professionals’ perceptions of the need for oral health education. Br Dent Nurs J. 1995;54:18 –19. 2042 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 37. Adams A. Qualified nurses lack adequate knowledge related to oral health, resulting in inadequate care of patients on medical wards. J Adv Nurs. 1996;24:552–560. 38. Mueller B, Millheim E, Farrington E, Brusko C, Wiser T. Mucositis management practices for hospitalized patients: national survey. J Pain Symptom Manage. 1995;10:510 –520. 39. Zakrzewska J, Leeson R, Mcluskey M, Vickers M. The development of patient information leaflets. Care of the mouth after radiotherapy. Gerodontology. 1997;14:48 –53. 40. Fulton JS, Middleton GJ, McPhail JT. Management of oral complications. Semin Oncol Nurs. 2002;18:28 –35. 41. Chapman CR, Hill HF. Prolonged morphine self-administration and addiction liability. Evaluation of two theories in a bone marrow transplant unit. Cancer. 1989;63:1636 –1644. 42. Dunbar PJ, Buckley P, Gavrin JR, Sanders JE, Chapman CR. Use of patient-controlled analgesia for pain control for children receiving bone marrow transplant. J Pain Symptom Manage. 1995;10:604 – 611. 43. Hill HF, Coda BA, Mackie AM, Iverson K. Patient-controlled analgesic infusions: alfentanil versus morphine. Pain. 1992; 49:301–310. 44. Hill HF, Mackie AM, Coda BA, Iverson K, Chapman CR. Patient-controlled analgesic administration. A comparison of steady-state morphine infusions with bolus doses. Cancer. 1991;67:873– 882. 45. Mackie AM, Coda BC, Hill HF. Adolescents use patientcontrolled analgesia effectively for relief from prolonged oropharyngeal mucositis pain. Pain. 1991;46:265–269. 46. Pillitteri LC, Clark RE. Comparison of a patient-controlled analgesia system with continuous infusion for administration of diamorphine for mucositis. Bone Marrow Transplant. 1998;22:495– 498. 47. Zucker TP, Flesche CW, Germing U, et al. Patient-controlled versus staff-controlled analgesia with pethidine after allogeneic bone marrow transplantation. Pain. 1998;75:305–312. 48. Collins JJ, Geake J, Grier HE, et al. Patient-controlled analgesia for mucositis pain in children: a three-period crossover study comparing morphine and hydromorphone. J Pediatr. 1996;129:722–728. 49. Coda BA, O’Sullivan B, Donaldson G, Bohl S, Chapman CR, Shen DD. Comparative efficacy of patient-controlled administration of morphine, hydromorphone, or sufentanil for the treatment of oral mucositis pain following bone marrow transplantation. Pain. 1997;72:333–346. 50. World Health Organization. Cancer pain relief (2nd edition). Geneva: World Health Organization, 1996. 51. Jacox A, Carr D, Payne R, et. al. Management of cancer pain. Clinical practice guideline no. 9. Rockville, MD: Agency for Healthcare Policy and Research, Public Health Service, U.S. Department of Health and Human Services, 1994. 52. Krajnik M, Zylicz Z, Finlay I, Luczak J, van Sorge AA. Potential uses of topical opioids in palliative care—report of 6 cases. Pain. 1999;80:121–125. 53. Carnel SB, Blakeslee DB, Oswald SG, Barnes M. Treatment of radiation- and chemotherapy-induced stomatitis. Otolaryngol Head Neck Surg. 1990;102:326 –330. 54. Rothwell BR, Spektor WS. Palliation of radiation-related mucositis. Spec Care Dentist. 1990;10:21–25. 55. Spijkervet FK, Van Saene HK, Van Saene JJ, et al. Effect of selective elimination of the oral flora on mucositis in irradiated head and neck cancer patients. J Surg Oncol. 1991; 46:167–173. 56. Sedal-Turhal N, Erdal S, Karacay S. Efficacy of treatment to 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. relieve mucositis-induced discomfort. Support Care Cancer. 2000;8:55–58. Dodd MJ, Larson PJ, Dibble SL, et al. Randomized clinical trial of chlorhexidine versus placebo for prevention of oral mucositis in patients receiving chemotherapy. Oncol Nurs Forum. 1996;23:921–927. Dodd MJ, Dibble SL, Miaskowski C, et al. Randomized clinical trial of the effectiveness of 3 commonly used mouthwashes to treat chemotherapy-induced mucositis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:39 – 47. Dall’Oppio L. [Prevention of oral mucositis]. 1997. Bondi E, Baroni C, Prete A, et al. Local antimicrobial therapy of oral mucositis in paediatric patients undergoing bone marrow transplantation. Oral Oncol. 1997;33:322–326. Coetzee MJ, Boshoff B, Goedhals L, Pienaar FD. Formula C—popular, cheap and readily available relief for radiation and cancer chemotherapy mucositis. S Afr Med J. 1997;87: 80 – 81. Perch SJ, Machtay M, Markiewicz DA, Kligerman MM. Decreased acute toxicity by using midline mucosa-sparing blocks during radiation therapy for carcinoma of the oral cavity, oropharynx, and nasopharynx. Radiology. 1995;197: 863– 866. Ship JA, Eisbruch A, D’Hondt E, Jones RE. Parotid sparing study in head and neck cancer patients receiving bilateral radiation therapy: one-year results. J Dent Res. 1997;76:807– 813. Kim JH, Chu FC, Lakshmi V, Houde R. Benzydamine HCl, a new agent for the treatment of radiation mucositis of the oropharynx. Am J Clin Oncol. 1986;9:132–134. Prada A, Chiesa F. Effects of benzydamine on the oral mucositis during antineoplastic radiotherapy and/or intra-arterial chemotherapy. Int J Tissue React. 1987;9:115–119. Epstein JB. Oral and maxillofacial cancer pain. Spec Care Dentist. 1986;6:223–227. Epstein JB. Oral and pharyngeal candidiasis. Topical agents for management and prevention. Postgrad Med. 1989;85: 257–258, 263–265, 268 –269. Epstein JB, Silverman S Jr., Paggiarino DA, et al. Benzydamine HCl for prophylaxis of radiation-induced oral mucositis: results from a multicenter, randomized, double-blind, placebo-controlled clinical trial. Cancer. 2001;92:875– 885. Foote RL, Loprinzi CL, Frank AR, et al. Randomized trial of a chlorhexidine mouthwash for alleviation of radiation-induced mucositis. J Clin Oncol. 1994;12:2630 –2633. Samaranayake LP, Robertson AG, MacFarlane TW, et al. The effect of chlorhexidine and benzydamine mouthwashes on mucositis induced by therapeutic irradiation. Clin Radiol. 1988;39:291–294. Spijkervet FK, van Saene HK, Panders AK, et al. Effect of chlorhexidine rinsing on the oropharyngeal ecology in patients with head and neck cancer who have irradiation mucositis. Oral Surg Oral Med Oral Pathol. 1989;67:154 –161. Mahood DJ, Dose AM, Loprinzi CL, et al. Inhibition of fluorouracil-induced stomatitis by oral cryotherapy. J Clin Oncol. 1991;9:449 – 452. Cascinu S, Fedeli A, Fedeli SL, Catalano G. Oral cooling (cryotherapy), an effective treatment for the prevention of 5-fluorouracil-induced stomatitis. Eur J Cancer B Oral Oncol. 1994;30B:234 –236. Rocke LK, Loprinzi CL, Lee JK, et al. A randomized clinical trial of two different durations of oral cryotherapy for prevention of 5-fluorouracil-related stomatitis. Cancer. 1993;72: 2234 –2238. Clinical Practice Guidelines for Mucositis/Rubenstein et al. 75. Loprinzi CL, Wender DB, Veeder MH, et al. Inhibition of 5-fluorouracil-induced ocular irritation by ocular ice packs. Cancer. 1994;74:945–948. 76. Edelman MJ, Gandara DR, Perez EA, et al. Phase I trial of edatrexate plus carboplatin in advanced solid tumors: amelioration of dose-limiting mucositis by ice chip cryotherapy. Invest New Drugs. 1998;16:69 –75. 77. Gandara DR, Edelman MJ, Crowley JJ, Lau DH, Livingston RB. Phase II trial of edatrexate plus carboplatin in metastatic non-small-cell lung cancer: a Southwest Oncology Group study. Cancer Chemother Pharmacol. 1997;41:75–78. 78. Dreicer R, Propert KJ, Kuzel T, Kirkwood JM, O’Dwyer PJ, Loehrer PJ. A Phase II trial of edatrexate in patients with advanced renal cell carcinoma. An Eastern Cooperative Oncology Group study. Am J Clin Oncol. 1997;20:251–253. 79. Anderson H, Scarffe JH, Sutton RN, Hickmott E, Brigden D, Burke C. Oral acyclovir prophylaxis against herpes simplex virus in non-Hodgkin lymphoma and acute lymphoblastic leukaemia patients receiving remission induction chemotherapy. A randomised double blind, placebo controlled trial. Br J Cancer. 1984;50:45– 49. 80. Saral R, Ambinder RF, Burns WH, et al. Acyclovir prophylaxis against herpes simplex virus infection in patients with leukemia. A randomized, double-blind, placebo-controlled study. Ann Intern Med. 1983;99:773–776. 81. Okuno SH, Foote RL, Loprinzi CL, et al. A randomized trial of a nonabsorbable antibiotic lozenge given to alleviate radiation-induced mucositis. Cancer. 1997;79:2193–2199. 82. Okuno SH, Woodhouse CO, Loprinzi CL, et al. Phase III controlled evaluation of glutamine for decreasing stomatitis in patients receiving fluorouracil (5-FU)-based chemotherapy. Am J Clin Oncol. 1999;22:258 –261. 83. Bianco J, Appelbaum F, Nemunaitis J, et al. Phase I–II trial of pentoxifylline for the prevention of transplant-related toxicities following bone marrow transplantation. Blood. 1991; 78:1205–1211. 84. Stockschlader M, Kalhs P, Peters S, et al. Intravenous pentoxifylline failed to prevent transplant-related toxicities in allogeneic bone marrow transplant recipients. Bone Marrow Transplant. 1993;12:357–362. 85. Ferra C, de Sanjose S, Lastra C, et al. Pentoxifylline, ciprofloxacin, and prednisone failed to prevent transplant-related toxicities in bone marrow transplant recipients and were associated with an increased incidence of infectious complications. Bone Marrow Transplant. 1997;20:1075–1080. 86. Van der Jagt R, Pari G, McDiarmid S, Boisvert D, Huebsch L. Effect of pentoxifylline on regimen related toxicity in patients undergoing allogeneic or autologous bone marrow transplantation. Bone Marrow Transplant. 1994;13:203–207. 87. Attal M, Huguet F, Rubie H, et al. Prevention of regimenrelated toxicities after bone marrow transplantation by pentoxifylline: a prospective, randomized trial. Blood. 1993;82: 732–736. 88. Clift RA, Bianco JA, Appelbaum FR, et al. A randomized controlled trial of pentoxifylline for the prevention of regimen-related toxicities in patients undergoing allogeneic marrow transplantation. Blood. 1993;82:2025–2030. 89. Barasch A, Peterson DE, Tanzer JM, et al. Helium-neon laser effects on conditioning-induced oral mucositis in bone marrow transplantation patients. Cancer. 1995;76:2550 –2556. 90. Cowen D, Tardieu C, Schubert MM, et al. Low energy helium-neon laser in the prevention of oral mucositis in patients undergoing bone marrow transplant: results of a dou- 2043 ble blind randomized trial. Int J Radiat Oncol Biol Phys. 1997;38:697–703. 91. Kilic D, Egehan I, Ozenirler S, Dursun A. Double-blinded, randomized, placebo-controlled study to evaluate the effectiveness of sulphasalazine in preventing acute gastrointestinal complications due to radiotherapy. Radiother Oncol. 2000;57:125–129. 92. Martenson JA, Bollinger JW, Sloan JA, et al. Sucralfate in the prevention of treatment-induced diarrhea in patients receiving pelvic radiation therapy: a North Central Cancer Treatment Group Phase III double-blind placebo-controlled trial. J Clin Oncol. 2000;18:1239 –1245. 93. Kneebone A, Mameghan H, Bolin T, et al. The effect of oral sucralfate on the acute proctitis associated with prostate radiotherapy: a double-blind, randomized trial. Int J Radiat Oncol Biol Phys. 2001;51:628 – 635. 94. O’Brien PC, Franklin CI, Poulsen MG, Joseph DJ, Spry NS, Denham JW. Acute symptoms, not rectally administered sucralfate, predict for late radiation proctitis: longer term follow-up of a Phase III trial—Trans-Tasman Radiation Oncology Group. Int J Radiat Oncol Biol Phys. 2002;54:442– 449. 95. Baughan CA, Canney PA, Buchanan RB, Pickering RM. A randomized trial to assess the efficacy of 5-aminosalicylic acid for the prevention of radiation enteritis. Clin Oncol (R Coll Radiol). 1993;5:19 –24. 96. Resbeut M, Marteau P, Cowen D, et al. A randomized double blind placebo controlled multicenter study of mesalazine for the prevention of acute radiation enteritis. Radiother Oncol. 1997;44:59 – 63. 97. Martenson JA Jr., Hyland G, Moertel CG, et al. Olsalazine is contraindicated during pelvic radiation therapy: results of a double-blind, randomized clinical trial. Int J Radiat Oncol Biol Phys. 1996;35:299 –303. 98. Kochhar R, Patel F, Dhar A, et al. Radiation-induced proctosigmoiditis. Prospective, randomized, double-blind controlled trial of oral sulfasalazine plus rectal steroids versus rectal sucralfate. Dig Dis Sci. 1991;36:103–107. 99. Kochhar R, Sriram PV, Sharma SC, Goel RC, Patel F. Natural history of late radiation proctosigmoiditis treated with topical sucralfate suspension. Dig Dis Sci. 1999;44:973–978. 100. Leuchter RS, Petrilli ES, Dwyer RM, Hacker NF, Castaldo TW, Lagasse LD. Nd:YAG laser therapy of rectosigmoid bleeding due to radiation injury. Obstet Gynecol. 1982;59(6 Suppl):65S– 67S. 101. Taylor JG, DiSario JA, Buchi KN. Argon laser therapy for hemorrhagic radiation proctitis: long-term results. Gastrointest Endosc. 1993;39:641– 644. 102. Fantin AC, Binek J, Suter WR, Meyenberger C. Argon beam coagulation for treatment of symptomatic radiation-induced proctitis. Gastrointest Endosc. 1999;49:515–518. 103. Tam W, Moore J, Schoeman M. Treatment of radiation proctitis with argon plasma coagulation. Endoscopy. 2000; 32:667– 672. 104. Jensen DM, Machicado GA, Cheng S, Jensen ME, Jutabha R. A randomized prospective study of endoscopic bipolar electrocoagulation and heater probe treatment of chronic rectal bleeding from radiation telangiectasia. Gastrointest Endosc. 1997;45:20 –25. 105. Rubinstein E, Ibsen T, Rasmussen RB, Reimer E, Sorensen BL. Formalin treatment of radiation-induced hemorrhagic proctitis. Am J Gastroenterol. 1986;81:44 – 45. 106. Mayer R, Klemen H, Quehenberger F, et al. Hyperbaric oxygen—an effective tool to treat radiation morbidity in prostate cancer. Radiother Oncol. 2001;61:151–156. 2044 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 107. Woo TC, Joseph D, Oxer H. Hyperbaric oxygen treatment for radiation proctitis. Int J Radiat Oncol Biol Phys. 1997;38: 619 – 622. 108. Counter S, Froese D, Hart M. Prospective evaluation of formalin therapy for radiation proctitis. Am J Surg. 1999;177: 396 –398. 109. Saclarides TJ, King DG, Franklin JL, Doolas A. Formalin instillation for refractory radiation-induced hemorrhagic proctitis. Report of 16 patients. Dis Colon Rectum. 1996;39: 196 –199. 110. Charneau J, Bouachour G, Person B, Burtin P, Ronceray J, Boyer J. Severe hemorrhagic radiation proctitis advancing to gradual cessation with hyperbaric oxygen. Dig Dis Sci. 1991; 36:373–375. 111. Barbatzas C, Spencer GM, Thorpe SM, Sargeant LR, Bown SG, Carbatzas C. Nd:YAG laser treatment for bleeding from radiation proctitis. Endoscopy. 1996;28:497–500. 112. Kaassis M, Oberti E, Burtin P, Boyer J. Argon plasma coagulation for the treatment of hemorrhagic radiation proctitis. Endoscopy. 2000;32:673– 676. 113. Sartori S, Trevisani L, Nielsen I, Tassinari D, Abbasciano V. Misoprostol and omeprazole in the prevention of chemotherapy-induced acute gastroduodenal mucosal injury. A randomized, placebo-controlled pilot study. Cancer. 1996; 78:1477–1482. 114. Sartori S, Trevisani L, Nielsen I, Tassinari D, Panzini I, Abbasciano V. Randomized trial of omeprazole or ranitidine versus placebo in the prevention of chemotherapy-induced gastroduodenal injury. J Clin Oncol. 2000;18:463– 467. 115. Gebbia V, Carreca I, Testa A, et al. Subcutaneous octreotide versus oral loperamide in the treatment of diarrhea following chemotherapy. Anticancer Drugs. 1993;4:443– 445. 116. Cascinu S, Fedeli A, Fedeli SL, Catalano G. Octreotide versus loperamide in the treatment of fluorouracil-induced diarrhea: a randomized trial. J Clin Oncol. 1993;11:148 –151. 117. Goumas P, Naxakis S, Christopoulou A, Chrysanthopoulos C, Nikolopoulou VV, Kalofonos HP. Octreotide acetate in the treatment of fluorouracil-induced diarrhea. Oncologist. 1998;3:50 –53. 118. Cascinu S, Fedeli A, Fedeli SL, Catalano G. Control of chemotherapy-induced diarrhea with octreotide. A randomized trial with placebo in patients receiving cisplatin. Oncology. 1994;51:70 –73. 119. Zidan J, Haim N, Beny A, Stein M, Gez E, Kuten A. Octreotide in the treatment of severe chemotherapy-induced diarrhea. Ann Oncol. 2001;12:227–229. 120. Barbounis V, Koumakis G, Vassilomanolakis M, Demiri M, Efremidis AP. Control of irinotecan-induced diarrhea by octreotide after loperamide failure. Support Care Cancer. 2001;9:258 –260. 121. Wang J, Zheng H, Sung CC, Hauer-Jensen M. The synthetic somatostatin analogue, octreotide, ameliorates acute and delayed intestinal radiation injury. Int J Radiat Oncol Biol Phys. 1999;45:1289 –1296. 122. Wang J, Zheng H, Hauer-Jensen M. Influence of short-term octreotide administration on chronic tissue injury, transforming growth factor beta (TGF-beta) overexpression, and collagen accumulation in irradiated rat intestine. J Pharmacol Exp Ther. 2001;297:35– 42. 123. Komaki R, Seiferheld W, Ettinger D, Lee JS, Movsas B, Sause W. Randomized Phase II chemotherapy and radiotherapy trial for patients with locally advanced inoperable nonsmall-cell lung cancer: long-term follow-up of RTOG 92-04. Int J Radiat Oncol Biol Phys. 2002;53:548 –557. 124. Komaki R, Lee JS, Kaplan B, et al. Randomized Phase III study of chemoradiation with or without amifostine for patients with favorable performance status inoperable Stage II–III non-small cell lung cancer: preliminary results. Semin Radiat Oncol. 2002;12(1 Suppl 1):46 – 49. 125. Bourhis J, De Crevoisier R, Abdulkarim B, et al. A randomized study of very accelerated radiotherapy with and without amifostine in head and neck squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2000;46:1105–1108. 126. Koukourakis M, Kyrias G, Kakolyris S, et al. Subcutaneous administration of amifostine during fractionated radiotherapy: a randomized Phase II study. J Clin Oncol. 2000;18: 2226 –2233. 127. Antonadou D, Coliarakis N, Synodinou M, et al. Randomized Phase III trial of radiation treatment ⫹/⫺ amifostine in patients with advanced-stage lung cancer. Int J Radiat Oncol Biol Phys. 2001;51:915–922. 128. Brizel D, Wasserman T, Henke M, et al. Phase III randomized trial of amifostine as a radioprotector in head and neck cancer. J Clin Oncol. 2000;18:3339 –3345. 129. Leong SS, Tan EH, Fong KW, et al. Randomized doubleblind trial of combined modality treatment with or without amifostine in unresectable Stage III non-small-cell lung cancer. J Clin Oncol. 2003;21:1767–1774. 130. Liu T, Liu Y, He S, Zhang Z, Kligerman MM. Use of radiation with or without WR-2721 in advanced rectal cancer. Cancer. 1992;69:2820 –2825. 131. Anne PR. Phase II trial of subcutaneous amifostine in patients undergoing radiation therapy for head and neck cancer. Semin Oncol. 2002;29(6 Suppl 19):80 – 83. 132. Human Genome Sciences. Results of Phase 2 repifermin clinical trial demonstrate safety and efficacy in patients with cancer-therapy-induced mucositis [press release]. Rockville, MD: Human Genome Sciences, 2003. 133. Brizel D, Le Q, Rosenthal D, et al. Phase 2 study of recombinant human keratinocyte growth factor (rHUKGF) in head and neck cancer treated with standard (SRT) or hyperfractionated irradiation (HRT) and concurrent chemotherapy (CT). In: Proceedings of the 44th Annual Meeting of the American Society for Therapeutic Radiology and Oncology. Fairfax, VA: American Society for Therapeutic Radiology and Oncology, 2002. 134. Spielberger R, Emmanouilides C, Stiff P, et al. Use of recombinant human keratinocyte growth factor (RHuKGF) can reduce severe oral mucositis in patients with hematologic malignancies undergoing autologous, peripheral blood progenitor cell transplantation [abstract 3642]. Presented at the Annual Meeting of the American Society for Clinical Oncology, Chicago, IL, May 31–June 3, 2003. Available from URL: http://www.asco.org/ac/1,1003,_12-002627-00_19-002. 000005m00.asp 135. Peterson D, Petit R. Phase III study: AES-14 in chemotherapy patients at risk for mucositis [abstract 2917]. Prog Proc Am Soc Clin Oncol. 2003;22:725. 136. Giles F, Miller CB, Hurd DD, et al. A Phase III, randomized, double-blind, placebo-controlled, multinational trial of iseganan for the prevention of oral mucositis in patients receiving stomatotoxic chemotherapy (PROMPT-CT trial). Leuk Lymphoma. 2003;44:1165–1172. 137. Goldberg SL, Pineiro L, Schuster MW, et al. Identification of transplant conditioning regimens of high mucositis potential [abstract 1468]. Prog Proc Am Soc Clin Oncol. 2002;21: 368a. Clinical Practice Guidelines for Mucositis/Rubenstein et al. 138. Osaki T, Ueta E, Yoneda K, Hirota J, Yamamoto T. Prophylaxis of oral mucositis associated with chemoradiotherapy for oral carcinoma by azelastine hydrochloride (Azelastine) with other antioxidants. Head Neck. 1994;16:331–339. 139. Carl W, Emrich LS. Management of oral mucositis during local radiation and systemic chemotherapy: a study of 98 patients. J Prosthet Dent. 1991;66:361–369. 140. Fidler P, Loprinzi CL, O’Fallon JR, et al. Prospective evaluation of a chamomile mouthwash for prevention of 5-FUinduced oral mucositis. Cancer. 1996;77:522–525. 141. McGaw WT, Belch A. Oral complications of acute leukemia: prophylactic impact of a chlorhexidine mouth rinse regimen. Oral Surg Oral Med Oral Pathol. 1985;60:275–280. 142. Ferretti GA, Raybould TP, Brown AT, et al. Chlorhexidine prophylaxis for chemotherapy- and radiotherapy-induced stomatitis: a randomized double-blind trial. Oral Surg Oral Med Oral Pathol. 1990;69:331–338. 143. Rutkauskas JS, Davis JW. Effects of chlorhexidine during immunosuppressive chemotherapy. A preliminary report. Oral Surg Oral Med Oral Pathol. 1993;76:441– 448. 144. Epstein JB, Vickars L, Spinelli J, Reece D. Efficacy of chlorhexidine and nystatin rinses in prevention of oral complications in leukemia and bone marrow transplantation. Oral Surg Oral Med Oral Pathol. 1992;73:682– 689. 145. Yuen KY, Woo PC, Tai JW, Lie AK, Luk J, Liang R. Effects of clarithromycin on oral mucositis in bone marrow transplant recipients. Haematologica. 2001;86:554 –555. 146. Donnelly JP, Muus P, Horrevorts AM, Sauerwein RW, De Pauw BE. Failure of clindamycin to influence the course of severe oromucositis associated with streptococcal bacteraemia in allogeneic bone marrow transplant recipients. Scand J Infect Dis. 1993;25:43–50. 147. Ishii J, Nakanishi K, Shimada K. [Treatment of radiostomatitis with Salcoat]. Gan No Rinsho. 1990;36:66 –70. 148. LeVeque FG, Parzuchowski JB, Farinacci GC, et al. Clinical evaluation of MGI 209, an anesthetic, film-forming agent for relief from painful oral ulcers associated with chemotherapy. J Clin Oncol. 1992;10:1963–1968. 149. Oguchi M, Shikama N, Sasaki S, et al. Mucosa-adhesive water-soluble polymer film for treatment of acute radiationinduced oral mucositis. Int J Radiat Oncol Biol Phys. 1998; 40:1033–1037. 150. Redding SW, Haveman CW. Treating the discomfort of oral ulceration resulting from cancer chemotherapy. Compend Contin Educ Dent. 1999;20:389 –392, 394, 396. 151. Yamamura K, Yotsuyanagi T, Okamoto T, Nabeshima T. Pain relief of oral ulcer by dibucaine-film. Pain. 1999;83: 625– 626. 152. Kutcher M. Evaluating the efficacy of 2-octyl cyanoacrylate bioadhesive for treatment of oral ulcerations. Compend Contin Educ Dent Suppl. 2001;(32):12–16. 153. Perez M, Fernandez I, Marquez D, Bretana RM. Use of N-butyl-2-cyanoacrylate in oral surgery: biological and clinical evaluation. Artif Organs. 2000;24:241–243. 154. Narang U. Cyanoacrylate medical adhesives—a new era Colgate ORABASE Soothe.N.Seal liquid protectant for canker sore relief. Compend Contin Educ Dent Suppl. 2001;(32):7– 11. 155. Crawford J, Tomita DK, Mazanet R, Glaspy J, Ozer H. Reduction of oral mucositis by filgrastim (r-metHuG-CSF) in patients receiving chemotherapy. Cytokines Cell Mol Ther. 1999;5:187–193. 156. Schneider SB, Nishimura RD, Zimmerman RP, et al. Filgrastim (r-metHuG-CSF) and its potential use in the reduction 2045 of radiation-induced oropharyngeal mucositis: an interim look at a randomized, double-blind, placebo-controlled trial. Cytokines Cell Mol Ther. 1999;5:175–180. 157. Mascarin M, Franchin G, Minatel E, et al. The effect of granulocyte colony-stimulating factor on oral mucositis in head and neck cancer patients treated with hyperfractionated radiotherapy. Oral Oncol. 1999;35:203–208. 158. Karthaus M, Rosenthal C, Huebner G, et al. Effect of topical oral G-CSF on oral mucositis: a randomised placebo-controlled trial. Bone Marrow Transplant. 1998;22:781–785. 159. Makkonen TA, Minn H, Jekunen A, Vilja P, Tuominen J, Joensuu H. Granulocyte macrophage-colony stimulating factor (GM-CSF) and sucralfate in prevention of radiationinduced mucositis: a prospective randomized study. Int J Radiat Oncol Biol Phys. 2000;46:525–534. 160. Tejedor M, Valerdi JJ, Arias F, et al. Hyperfractionated radiotherapy concomitant with cisplatin and granulocyte colony-stimulating factor (filgrastim) for laryngeal carcinoma. Cytokines Cell Mol Ther. 2000;6:35–39. 161. Wagner W, Alfrink M, Haus U, Matt J. Treatment of irradiation-induced mucositis with growth factors (rhGM-CSF) in patients with head and neck cancer. Anticancer Res. 1999; 19:799 – 803. 162. Chi KH, Chen CH, Chan WK, et al. Effect of granulocytemacrophage colony-stimulating factor on oral mucositis in head and neck cancer patients after cisplatin, fluorouracil, and leucovorin chemotherapy. J Clin Oncol. 1995;13:2620 – 2628. 163. Bez C, Demarosi F, Sardella A, et al. GM-CSF mouth rinses in the treatment of severe oral mucositis: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:311–315. 164. Saarilahti K, Kajanti M, Joensuu T, Kouri M, Joensuu H. Comparison of granulocyte-macrophage colony-stimulating factor and sucralfate mouthwashes in the prevention of radiation-induced mucositis: a double-blind prospective randomized Phase III study. Int J Radiat Oncol Biol Phys. 2002;54:479 – 485. 165. Hejna M, Kostler WJ, Raderer M, et al. Decrease of duration and symptoms in chemotherapy-induced oral mucositis by topical GM-CSF: results of a prospective randomised trial. Eur J Cancer. 2001;37:1994 –2002. 166. Sprinzl GM, Galvan O, de Vries A, et al. Local application of granulocyte-macrophage colony stimulating factor (GMCSF) for the treatment of oral mucositis. Eur J Cancer. 2001; 37:2003–2009. 167. van der Lelie H, Thomas BL, van Oers RH, et al. Effect of locally applied GM-CSF on oral mucositis after stem cell transplantation: a prospective placebo-controlled doubleblind study. Ann Hematol. 2001;80:150 –154. 168. Cartee L, Petros WP, Rosner GL, et al. Evaluation of GM-CSF mouthwash for prevention of chemotherapy-induced mucositis: a randomized, double-blind, dose-ranging study. Cytokine. 1995;7:471– 477. 169. Smith T. Gelclair: managing the symptoms of oral mucositis. Hosp Med. 2001;62:623– 626. 170. Innocenti M, Moscatelli G, Lopez S. Efficacy of Gelclair in reducing pain in palliative care patients with oral lesions: preliminary findings from an open pilot study. J Pain Symptom Manage. 2002;24:456 – 457. 171. Schedler M, Feidt H, Niewaldt M. La¨bt sich die radiogene mucositis mit immunoglobulin behandein? [Can radiotherapy-induced mucositis be treated with immunoglobulins?] Zentralbl Hals Ohren Heikunde Kopf Halschirurg. 1990;139: 3– 4. 2046 CANCER Supplement May 1, 2004 / Volume 100 / Number 9 172. Schedler M, Bost P, Federspil P, Pautler M, Schatzle W. Die behandlung der strahleninduzierten mukositis bei kopf-/halstumoren mit intramuskular verabriechtem polyvalenten immunoglobulin. [Therapy of X-ray–induced mucositis in head and neck cancers with intramuscularly applied polyvalent immunoglobulins.] Tumordiagn Ther. 1994;15:184–191. 173. Mose S, Adamietz IA, Saran F, et al. Can prophylactic application of immunoglobulin decrease radiotherapy-induced oral mucositis? Am J Clin Oncol. 1997;20:407– 411. 174. Pillsbury HC III, Webster WP, Rosenman J. Prostaglandin inhibitor and radiotherapy in advanced head and neck cancers. Arch Otolaryngol Head Neck Surg. 1986;112:552–553. 175. Rymes N, Glick L, Holmes JA. Topical mesalazine in the treatment of chemotherapy and radiotherapy-induced oral mucositis. Bone Marrow Transplant. 1996;18:484. 176. Tanner NS, Stamford IF, Bennett A. Plasma prostaglandins in mucositis due to radiotherapy and chemotherapy for head and neck cancer. Br J Cancer. 1981;43:767–771. 177. Warde P, O’Sullivan B, Aslanidis J, et al. A Phase III placebocontrolled trial of oral pilocarpine in patients undergoing radiotherapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2002;54:9 –13. 178. Awidi A, Homsi U, Kakail RI, et al. Double-blind, placebocontrolled cross-over study of oral pilocarpine for the prevention of chemotherapy-induced oral mucositis in adult patients with cancer. Eur J Cancer. 2001;37:2010 –2014. 179. Masayuki F, Norihiko K, Keita T, et al. [Efficacy and safety of polaprezinc as a preventive drug for radiation-induced stomatitis]. Nippon Igaku Hoshasen Gakkai Zasshi. 2002;62: 144 –150. 180. Rahn R, Adamietz IA, Boettcher HD, Schaefer V, Reimer K, Fleischer W. Povidone-iodine to prevent mucositis in patients during antineoplastic radiochemotherapy. Dermatology. 1997;195 Suppl 2:57– 61. 181. Adamietz IA, Rahn R, Bottcher HD, Schafer V, Reimer K, Fleischer W. Prophylaxis with povidone-iodine against induction of oral mucositis by radiochemotherapy. Support Care Cancer. 1998;6:373–377. 182. Matejka M, Nell A, Kment G, et al. Local benefit of prostaglandin E2 in radiochemotherapy-induced oral mucositis. Br J Oral Maxillofac Surg. 1990;28:89 –91. 183. Porteder H, Rausch E, Kment G, Watzek G, Matejka M, Sinzinger H. Local prostaglandin E2 in patients with oral malignancies undergoing chemo- and radiotherapy. J Craniomaxillofac Surg. 1988;16:371–374. 184. Pretnar J, Glazar D, Mlakar U, Modic M. Prostaglandin E2 in the treatment of oral mucositis due to radiochemotherapy in patients with haematological malignancies. Bone Marrow Transplant. 1989;4 Suppl 3:106. 185. Labar B, Mrsic M, Pavletic Z, et al. Prostaglandin E2 for prophylaxis of oral mucositis following BMT. Bone Marrow Transplant. 1993;11:379 –382. 186. Hanson W, Reddy S, Simon S, Mihalo W, Tova Y. Protection from radiation-induced oral mucositis by a mouth rinse containing the prostaglandin E1 analog, misoprostol: a placebo controlled double blind trial. In: Honn K, editor. Eicosanoids and other bioactive lipids in cancer, inflammation, and radiation injury. New York: Plenum Press, 1997:811– 818. 187. Maciejewski B, Zajusz A, Pilecki B, et al. Acute mucositis in the stimulated oral mucosa of patients during radiotherapy for head and neck cancer. Radiother Oncol. 1991;22:7–11. 188. Oshitani T, Okada K, Kushima T, et al. [Clinical evaluation of sodium alginate on oral mucositis associated with radiotherapy]. Nippon Gan Chiryo Gakkai Shi. 1990;25:1129–1137. 189. Leborgne JH, Leborgne F, Zubizarreta E, Ortega B, Mezzera J. Corticosteroids and radiation mucositis in head and neck cancer. A double-blind placebo-controlled randomized trial. Radiother Oncol. 1998;47:145–148. 190. Barrett AP. Dexamethasone as an adjunct in oropharyngeal obstruction in a patient with leukemia. Oral Surg Oral Med Oral Pathol. 1990;70:741–743. 191. Wolff JE, Hauch H, Kuhl J, Egeler RM, Jurgens H. Dexamethasone increases hepatotoxicity of MTX in children with brain tumors. Anticancer Res. 1998;18:2895–2899. 192. Malik IA, Moid I, Haq S, Sabih M. A double-blind, placebocontrolled, randomized trial to evaluate the role of tetrachlorodecaoxide in the management of chemotherapy-induced oral mucositis. J Pain Symptom Manage. 1997;14:82– 87. 193. Oberbaum M. Experimental treatment of chemotherapyinduced stomatitis, using a homeopathic-complex remedy: a preliminary study. Biomed Ther. 1998;16:261–265. 194. Oberbaum M, Yaniv I, Ben-Gal Y, et al. A randomized, controlled clinical trial of the homeopathic medication TRAUMEEL S in the treatment of chemotherapy-induced stomatitis in children undergoing stem cell transplantation. Cancer. 2001;92:684 – 690. 195. Cohen G, Elad S, Or R, Galili D, Garfunkel AA. The use of tretinoin as oral mucositis prophylaxis in bone marrow transplantation patients: a preliminary study. Oral Dis. 1997;3:243–246. 196. Lopez I, Goudou C, Ribrag V, Sauvage C, Hazebroucq G, Dreyfus F. [Treatment of mucositis with vitamin E during administration of neutropenic antineoplastic agents]. Ann Med Interne (Paris). 1994;145:405– 408. 197. Wadleigh RG, Redman RS, Graham ML, Krasnow SH, Anderson A, Cohen MH. Vitamin E in the treatment of chemotherapy-induced mucositis. Am J Med. 1992;92:481– 484. 198. Kligerman MM, Liu T, Liu Y, Scheffler B, He S, Zhang Z. Interim analysis of a randomized trial of radiation therapy of rectal cancer with/without WR-2721. Int J Radiat Oncol Biol Phys. 1992;22:799 – 802. 199. Mitsuhashi N, Takahashi I, Takahashi M, Hayakawa K, Niibe H. Clinical study of radioprotective effects of amifostine (YM-08310, WR-2721) on long-term outcome for patients with cervical cancer. Int J Radiat Oncol Biol Phys. 1993;26: 407– 411. 200. Montana GS, Anscher MS, Mansbach CM II, et al. Topical application of WR-2721 to prevent radiation-induced proctosigmoiditis. A Phase I/II trial. Cancer. 1992;69:2826 –2830. 201. Vernia P, Fracasso PL, Casale V, et al. Topical butyrate for acute radiation proctitis: randomised, crossover trial. Lancet. 2000;356:1232–1235. 202. Daniele B, Perrone F, Gallo C, et al. Oral glutamine in the prevention of fluorouracil induced intestinal toxicity: a double blind, placebo controlled, randomised trial. Gut. 2001; 48:28 –33. 203. Savarese D, Al-Zoubi A, Boucher J. Glutamine for irinotecan diarrhea. J Clin Oncol. 2000;18:450 – 451. 204. Decker-Baumann C, Buhl K, Frohmuller S, von Herbay A, Dueck M, Schlag PM. Reduction of chemotherapy-induced side-effects by parenteral glutamine supplementation in patients with metastatic colorectal cancer. Eur J Cancer. 1999; 35:202–207. 205. Khan AM, Birk JW, Anderson JC, et al. A prospective randomized placebo-controlled double-blinded pilot study of misoprostol rectal suppositories in the prevention of acute and chronic radiation proctitis symptoms in prostate cancer patients. Am J Gastroenterol. 2000;95:1961–1966.






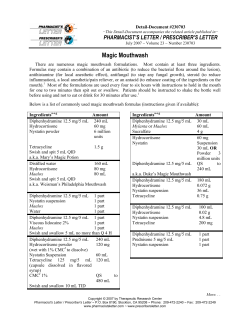





© Copyright 2025