
Heart rate is a predictor of success in the
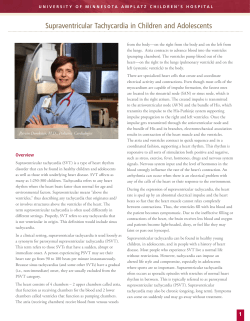
European Heart Journal (2004) 25, 1310–1317 Clinical research Heart rate is a predictor of success in the treatment of adults with symptomatic paroxysmal supraventricular tachycardia , Sergio Antonio Faraguti Piercarlo Ballo*, Daniele Bernabo Received 24 July 2003; revised 21 April 2004; accepted 13 May 2004 Available online 20 July 2004 See page 1277 for the editorial comment on this articley KEYWORDS Aims To analyse whether heart rate may affect the efficacy of adenosine, verapamil and carotid sinus massage in terminating symptomatic episodes of paroxysmal supraventricular tachycardia (PSVT) in adults. Methods and results The study population was selected among 175 adult patients, affected by symptomatic PSVT. One hundred and six of them were considered eligible for the study. Each subject received one of the following treatments: verapamil, 5 mg intravenously (IV) in 5–10 min, followed by 1–5 lg/kg/min; adenosine, 6 mg IV, followed by 12 mg IV after 2–3 min; carotid sinus massage. Adenosine and verapamil were similarly effective in terminating PSVT (74.4% vs 81.8%, P ¼ 0:45). The efficacy of carotid sinus massage was significantly lower in comparison with the other two groups (32.4%, P ¼ 0:00032 vs adenosine and P ¼ 0:000044 vs verapamil group). At logistic regression, PSVT rate showed a positive association with the percentage of sinus rhythm restoration in the group who received adenosine (P ¼ 0:0004). The probability of success in resolving the tachycardia following treatment with adenosine was >75% for heart rates over 166 beats per minute (bpm), but rapidly decreased at lower frequencies, reducing to 25% at 138 bpm. In the verapamil group, PSVT rate was negatively related to the percentage of sinus rhythm restoration (P ¼ 0:018). The probability of success in terminating PSVT following administration of verapamil was >75% for heart rates lower than 186 bpm, but tended to decrease at faster rates, reducing to 25% at 241 bpm. No significant effects of heart rate were observed in the carotid sinus massage group (P ¼ 0:17). The probability curves obtained in the adenosine and verapamil group crossed at a point corresponding to 173 bpm, which may represent a cut-off value to predict which treatment could ensure higher rate of success. Conclusions Heart rate predicts restoration of sinus rhythm in adult subjects with symptomatic episodes of PSVT treated with adenosine and verapamil. Adenosine is highly effective in PSVT characterised by fast rates, whereas the efficacy of verapamil is increased in patients with low-frequency PSVT. c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. Adenosine; Verapamil; Vagal manoeuvres; Heart rate; Supraventricular tachycardia Introduction * Corresponding author. Tel.: þ39-0187-53255/299; fax: þ39-0187533456. E-mail address: pcballo@tin.it (P. Ballo). y doi:10.1016/j.ehj.2004.07.003. Paroxysmal supraventricular tachycardia (PSVT) is a common arrhythmia which may be associated to a variety of electrophysiological abnormalities, including increased 0195-668X/$ - see front matter c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ehj.2004.05.011 Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 Department of Cardiology, S. Andrea Hospital, La Spezia, Italy Heart rate is a predictor of success in the treatment of adults with symptomatic paroxysmal supraventricular tachycardia Methods Patient selection Male or female adult subjects, affected by symptomatic PSVT, seen at our Department between 11 September, 2000 and 5 February, 2004 were retrospectively enrolled for this study. Patients were considered eligible for the study if they had (1) age P 16 years, (2) sudden onset of symptoms due to the tachycardia (subjective awareness of palpitations or rhythm irregularity or arrhythmia-related dizziness, chest discomfort, dyspnoea, asthenia, anxiety) and (3) electrocardiographic evidence of PSVT. Exclusion criteria were: haemodynamic instability (which was considered an indication for immediate electrical cardioversion), bradycardia <50 beats per minute (bpm); high-grade sinoatrial or AV block, history of sick sinus syndrome or sinus node dysfunction, heart failure (New York Heart Association class III or IV), asthma, previous implantation of pacemaker or defibrillator, use of antiarrhythmics or rate-limiting drugs within the previous 15 days, contraindications to carotid sinus massage (carotid bruit, history of previous adverse reaction to carotid sinus massage or cerebrovascular accidents in the last three months), hypersensitivity, intolerance or contraindications to verapamil or adenosine. Clinical examination and ECG All patients underwent an accurate clinical examination and a brief and targeted history. Systemic arterial pressure was determined using standard methods, with a cuff sphygmomanometer, after 3 min of supine position. Measurements were repeated every 3 min throughout the entire procedure. A 12-lead ECG was registered in each subject and electrocardiographic monitoring was maintained until completion of the therapeutic protocol. PSVT was defined as a regular tachycardia with sudden onset, QRS complexes of supraventricular origin (i.e., narrow complexes or wide complexes in the presence of aberrant conduction, previous conduction defects or suspected accessory pathways with no evidence of AV-dissociation) and abnormal non-sinus P waves. Study protocols On the basis of the general clinical evaluation, each participant in the study underwent one of the following treatments: (1) verapamil, 5 mg intravenously (IV) in 5–10 min, followed by 1–5 lg/kg/min, based on heart rate and blood pressure; (2) adenosine 6 mg IV, followed by a second dose of 12 mg IV after 2–3 min; (3) carotid sinus massage, applied twice for at least 5 s on each side. Any procedure was terminated in case of success of the treatment or if complications such as severe hypotension (systolic blood pressure <90 mmHg), bradycardia (<50 bpm), atrial fibrillation or flutter, high-degree AV-block or malignant ventricular arrhythmias occurred. Success of the treatment was defined as persistent sinus rhythm restoration, maintained for at least 3 min after the termination of PSVT. Statistical analysis Data are shown as mean values±SD for continuous variables. The comparison of normal outcomes among the three study groups was assessed using one-way analysis of variance. Dichotomous variables (i.e., gender and success in terminating PSVT) were compared with use of the v2 test. Logistic regression analysis was performed using the maximised log likelihood method, in order to evaluate the effect of PSVT rate on the success of the treatment in each group of study. Regression co-efficients, odds ratios, 95% confidence intervals (CI) and statistical significance were calculated for each treatment. The estimated probability of sinus rhythm restoration was expressed as a function of heart rate using the formula p ¼ 1 1=½expða þ b HRÞ þ 1, where p is the probability of success, expressed as a decimal between 0 and 1, exp denotes the exponential function, a and b represent the intercept and the slope of the logistic regression line in each group of study, and HR indicates heart rate. The heart rate values which corresponded to an estimated 25%, 50% and 75% probability of success were determined using the formula HR ¼ ½logitðpÞ a=b, where the expression logit (p) indicates the log odds ratio, computed as the natural logarithm of ½p=ð1 pÞ. To obtain a direct and simplified quantification of changes in the probability of success for any unitary variation in heart rate, a linear approximation was assumed for the adenosine and verapamil curves in the interval between the values of heart rate corresponding to a 25% and 75% probability of success. Linearity in this range was tested by fitting data with use of linear regression analysis, based on the least square method. Parameter estimates, Pearson’s correlation co-efficients and levels of significance of the regression lines were determined in both groups. The significance level was set at 0.05. All statistical tests were two-tailed. The SPSS software (Statistical Package for Social Sciences, Chicago, Illinois, USA) for Windows Release 11.5.0 was used to generate the statistical analyses. Results Study population One hundred and seventy-five patients met the inclusion criteria. One subject presented severe hypotension and Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 automaticity, triggered activity and re-entry circuits which develop in the atrial myocardium or in the atrioventricular (AV) junction.1–5 The general clinical approach to a subject with suspected PSVT includes a brief and targeted history and an accurate analysis of the electrocardiogram (ECG), in the attempt to differentiate PSVT from other narrow-complex tachycardias and to choose the most appropriate treatment.6;7 When no haemodynamic instability is present, vagal manoeuvres, adenosine and verapamil are usually considered as the first-line treatment of choice for PSVT,8–10 and the relative efficacy of each has been evaluated in many studies.11–16 Both adenosine and verapamil are well known to have a frequency-dependent effect on functional AV-nodal properties,17–19 and the rate-dependence of depression in AV-nodal function has been reported to play a key role in the ability of interrupting experimental pacing-induced PSVT.20 These findings suggest that the rate of the tachycardia may potentially affect the anti-arrhythmic efficacy of both drugs in spontaneous PSVT. However, whether heart rate could be a predictor of success in the treatment of PSVT in clinical practice has never been analysed. The aim of this study was to evaluate whether the rate of the tachycardia may predict the restoration of sinus rhythm in the treatment of adult subjects with symptomatic PSVT. The design of the study included two different pharmacological protocols (i.e., adenosine and verapamil) and one non-pharmacological approach (i.e., carotid sinus massage). 1311 1312 P. Ballo et al. underwent successful DC-shock. In 23 cases, PSVT was associated with type 2 second-grade AV-block (19 with conduction ratio 2:1, one with conduction ratio 4:1 and three with variable ventricular response). Twenty-two subjects were under chronic anti-arrhythmic therapy (eight of which were assuming verapamil, six propafenone, five amiodarone, two sotalol and one diltiazem). Two previously untreated patients were also excluded because one of them had spontaneously taken 300 mg of propafenone and the other 160 mg of verapamil per os at the onset of symptoms. Twenty-one subjects experienced spontaneous termination of PSVT during electrocardiographic monitoring before the beginning of the treatment. One hundred and six patients were then admitted to the study group. Thirty-nine subjects received adenosine, 33 subjects were administered verapamil and 34 underwent carotid sinus massage. The three groups were similar as regards mean age, gender distribution, arterial systolic and diastolic pressures and heart rate (Table 1). The percentages of success in terminating PSVT were significantly different among the three groups (P ¼ 0:000029). A similar efficacy of treatment was observed in the group treated with adenosine (74.4%) and among the subjects who received verapamil (81.8%, P ¼ 0:45). The percentage of PSVT interruption in the group treated with the carotid sinus massage was consistently lower in comparison with the other two groups (32.4%, P ¼ 0:00032 vs adenosine and P ¼ 0:000044 vs verapamil group). No significant complications were observed in any subject. Effect of heart rate Logistic regression (Table 2) showed a significant positive association between heart rate and the probability of Table 1 General characteristics of the three study groups Patients (males/females) Age (years) Systolic arterial pressure (mmHg) Diastolic arterial pressure (mmHg) Heart rate (bpm) Adenosine Verapamil CSM p Value 39 (13/26) 56.6±19.0 124.4±16.6 78.0±10.5 172.0±22.5 33 (10/23) 57.9±16.4 132.3±10.5 81.7±8.5 166.6±29.8 34 (13/21) 61.6±14.0 126.0±21.9 81.1±12.8 170.6±24.5 0.78 0.43 0.13 0.30 0.66 p Values were calculated using analysis of variance or v2 test. CSM, carotid sinus massage. Table 2 Effect of heart rate on the probability of sinus rhythm restoration in the three groups of study, as evaluated by logistic regression Adenosine group Verapamil group CSM group Intercept B SE p Value Odds ratio 95% CI Overall p value )11.698 8.546 3.087 0.077 )0.040 )0.023 0.028 0.019 0.018 0.006 0.033 0.204 1.081 0.961 0.978 1.023–1.141 0.926–0.997 0.944–1.012 0.0004 0.018 0.176 The co-efficients B represent the slopes of the relations between heart rate and the log odds ratio for the probability of success of the treatment in each group of study. The standard error (SE) and the statistical significance of each slope are reported in the table. Odds ratio, 95% confidence intervals (CI) and overall model significance for each study group are also shown. CSM, carotid sinus massage. Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 General features and efficacy of treatment PSVT termination in the adenosine group (Fig. 1, top panel). The maximal effect of heart rate was observed in the central portion of the curve, where the slope of the relation assumed its highest values. The estimated probability of success for the treatment with adenosine was >75% for heart rates >166 bpm, but rapidly decreased at lower frequencies, reducing to 50% at 152 bpm – corresponding to the central inflection point of the curve – and to 25% at 138 bpm. In the range between 138 and 166 bpm, the sigmoidal curve was well approximated by a linear relation (p ¼ 0:0183 HR – 2.2754; r ¼ 0:99, P < 0:0001). This corresponded to an absolute 1.8% decrease in the probability of sinus rhythm restoration for any unitary decrease in heart rate – i.e., for any reduction by one beat per minute in PSVT frequency within that interval. In the verapamil group, heart rate was negatively associated with the efficacy of the treatment in interrupting PSVT (Fig. 1, middle panel). The estimated probability of success was >75% for heart rates <186 bpm, but tended to decrease for higher values of frequency, reducing to 50% at 214 bpm and to 25% at a frequency of 241 bpm. Similarly to the adenosine curve, the S-shaped function was well fitted by a linear equation in the range between 186 and 241 bpm (p ¼ 0:0094 HR þ 2:5232; r ¼ 0:99, P < 0:0001). This corresponded to an absolute 0.9% reduction in the probability of sinus rhythm restoration for any increase by one beat per minute in PSVT rate. Although the efficacy of carotid sinus massage showed some tendency to decrease as PSVT frequency increased (Fig. 1, bottom panel), the relation to heart rate was not significant (Table 2). The comparison of the relations obtained in the adenosine and verapamil groups showed that the two curves crossed in a point which corresponded to 173.0 bpm. This represented the value of heart rate at which the two treatments would yield a similar percentage of success in PSVT termination Heart rate is a predictor of success in the treatment of adults with symptomatic paroxysmal supraventricular tachycardia Favours Adenosine Favours Verapamil Adenosine 100 Difference in the probability of success (%) Probability of success (%) 100 75 50 25 0 75 125 175 225 1313 275 50 0 -50 -100 75 Heart rate (bpm) 125 175 225 275 Heart rate (bpm) Fig. 2 Comparison of the efficacy of adenosine and verapamil according to heart rate. The plot shows the difference between the estimated probability of sinus rhythm restoration obtained by treatment with adenosine and that obtained by administration of verapamil, at different values of heart rate. At a frequency approximately equal to 173 bpm, there were no differences between the two treatments. The efficacy was better for adenosine at faster frequencies, and better for verapamil at slower frequencies (see text). Verapamil 75 50 25 0 75 125 175 225 275 Heart rate (bpm) Probability of success (%) 100 Carotid sinus massage 75 50 25 0 75 125 175 225 275 Heart rate (bpm) Fig. 1 Effect of heart rate on the probability of sinus rhythm restoration following treatment with adenosine (top panel), verapamil (middle panel) and carotid sinus massage (bottom panel). The heart rate values which corresponded to an estimated 25% and 75% probability of success are shown in each plot. In those intervals, relations were approximately linear (see text). (83.5%). Higher rates were then associated with better efficacy of adenosine, whereas lower rates were associated with better efficacy of verapamil (Fig. 2). Discussion PSVT is a common clinical condition which may be explained by various pathophysiological mechanisms. Enhanced automaticity, triggered activity or re-entry circuits which develop in the atrial myocardium or in the AV-junction may be responsible for different types of PSVT, although recent observations have suggested that other unknown mechanisms could be involved in some cases with peculiar electropharmacological responses.21 The most common arrhythmia mechanisms in PSVT are AV-intranodal re-entry, which leads to AV-nodal reciprocating tachycardia,2;5;22–26 and re-entry by an accessory AV-connection, which produces AV-reciprocating tachycardia.27;28 Atrial tachycardia is a less frequent type of PSVT which may be underlied by focal or macro re-entrant mechanisms in different regions of the atrial tissue,29–37 whereas other PSVT types are rare. Despite heterogeneity of pathogenesis, contemporary management of PSVT usually follows a general algorithm which initially includes vagal manoeuvres and administration of adenosine or verapamil.38–41 Diltiazem,42–44 b-blockers,45;46 anti-arrhythmics of class Ic47;48 and III,49–52 pharmacological associations,53;54 new selective A1 adenosine receptor agonists currently under clinical investigation55;56 and transoesophageal atrial pacing57 may also be useful in the treatment or prevention of episodes of PSVT in adults, and immediate electrical cardioversion with DC-shock is recommended in case of haemodynamically compromised patients.8;58 Digoxin is the drug of choice for supraventricular tachycardias occurring in foetuses and may be effective in the prophylaxis of recurrences in infants and children, but has a limited role in adults.59–61 Transoesophageal and/or endocavitary electrophysiology are often required to determine the exact mechanism of the arrhythmia62–64 and radiofrequency catheter ablation is generally indicated in subjects with drug-refractory arrhythmias.65–69 Adenosine and verapamil have been reported to have similar high efficacy in terminating PSVT, with a rate of success ranging from 59% to 100% for adenosine and from 73% to 98.8% for verapamil,11;13;42;70;71 according to the dose and mode of administration. Vagal manoeuvres present the advantage of being relatively simple and non-invasive, but their efficacy seems to be quite lower in comparison with pharmacological interventions, with Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 Probability of success (%) 100 1314 increase in the effective refractory period of the AVnode which occurs at fast heart rates may play a key role in determining a higher efficacy of adenosine in terminating PSVT characterised by relatively high frequencies. The efficacy of verapamil in the treatment and prophylaxis of supraventricular tachycardias is due to its ability to produce an inhibition of the inward calcium current I(Ca, L), secondary to the blockage of type L calcium channels, resulting in a rate-dependent prolongation in AV-nodal conduction time and effective refractory period and yielding a decrease in the atrial pacing rate at which AV-Wenckebach occurs.80–85 An adjunctive anti-arrhythmic mechanism of verapamil may be due to the inhibition of the rapid component of the delayed rectifier potassium current I(Kr), which produces a delay in the myocyte repolarisation process and leads to a prolongation of the action potential and effective refractory period.86–88 The rate-dependency of the pharmacological effect of verapamil is probably the result of an interaction among various factors, which may include differential effects on calcium or potassium channels, a large constant time of adaptation due to slow drug-specific association and dissociation kinetic to the calcium channel,18;84;89;90 and a modulating action by the autonomic tone.91;92 A recent study has shown that administration of verapamil in healthy adults leads to a prolongation of the atrial effective refractory period at low frequencies and to a shortening at high frequencies, suggesting a predominant effect on I(Ca, L) at fast rates and a predominant effect on I(Kr) at slow rates.93 The report that I(Kr) may play an important role in the electrophysiological properties of the AV-node94 may suggest the intriguing hypothesis that a predominant effect on the potassium channels, with subsequent increase in the effective refractory period, could exist at slow rates in the AV-nodal tissue and play some role in determining a higher efficacy of verapamil in low-frequency PSVT. The relation among rate-dependent and slowly adaptive pharmacodynamic interaction with calcium channels, differential effects on calcium and potassium channels, and potentially higher efficacy in terminating PSVT in patients with low heart frequencies in comparison with those with high frequencies should be evaluated in further studies. Limitations of the study The major limitation of this study is that the design did not include either electrophysiological study or electrocardiographic determination of PSVT types, so that the effect of different electrical patterns in affecting the relationship between heart rate and success of treatment could have not been evaluated. It is well known that different subtypes of PSVT may show unequal responsiveness to anti-arrhythmics, particularly in the case of atrial tachycardia, which does not directly involve the AV-node and tends to show variable sensitivity to nodal blocking agents such as adenosine and verapamil.95;96 However, atrial tachycardia has been reported to be relatively infrequent, accounting for only 5–15% of all PSVTs.7;97–100 Accordingly, an a posteriori analysis in our Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 percentages of PSVT termination ranging from 6% to 22% following carotid sinus massage.16;70;72–75 Our results confirm the evidence that adenosine and verapamil are similarly highly effective in terminating spontaneous episodes of PSVT in adults, whereas carotid sinus massage is able to interrupt tachycardia in a relatively low percentage of cases. However, our data also suggest that the efficacy of both adenosine and verapamil is affected by the frequency of the arrhythmia. Increasing PSVT rates were significantly associated to higher percentages of sinus rhythm restoration following treatment with adenosine (Fig. 1, top panel). In contrast, the efficacy of verapamil in restoring sinus rhythm was inversely related to the frequency of PSVT (Fig. 1, middle panel), and no significant effect of heart rate was observed in the group which had undergone carotid sinus massage (Fig. 1, bottom panel). Of note, the effect of heart rate on the efficacy of verapamil was less in comparison with that observed for adenosine, as shown by the milder steepness of the curve in the plots. However, the comparison of the relations obtained in the adenosine and verapamil groups suggested that 173 bpm could be used as the best cut-off value to predict which treatment may ensure higher probability of success in restoring sinus rhythm (Fig. 2). Heart rates over this cut-off value may be associated to higher percentages of PSVT interruption by administration of adenosine, whereas slower frequencies may be associated to better efficacy of verapamil. Heart rate is known to influence the pharmacodynamic effect of both adenosine and verapamil on the AVnode. It has been shown that the negative dromotropic effect of adenosine tends to increase when the atrial pacing cycle is progressively reduced during experimental PSVT,17 and the rate-dependent conduction slowing seems to be more pronounced for adenosine than for verapamil.19 Adenosine has been demonstrated to increase AV-nodal fatigue – i.e., the AV-nodal delay which slowly develops at fast rates – and to attenuate facilitation – i.e., the tendency of short cycles to improve subsequent nodal recovery – without directly altering AV-nodal recovery, and this may result in frequencydependent increases in the AV-nodal conduction time and effective refractory period. The substrate of this phenomenon remains to be clarified, although complex interaction among different electrophysiological and molecular mechanisms is likely to be involved. These include a direct effect on the activation of the inward rectifier potassium current I(K, Ado), which produces hyperpolarization and depression in AV-conduction,76 and an indirect effect of antagonism on catecholaminestimulated adenylate cyclase activity, which occurs through coupling with guanosine triphosphate-binding inhibitory proteins.77;78 A possible alternative ionic mechanism has also recently been proposed, involving a different adenosine-activated, time- and voltage-dependent potassium current defined Ado-I(K), which could play a key role in determining nodal depression at lower concentrations of the nucleoside and particularly at fast heart rate.79 Regardless of the exact mechanism underlying these phenomena, our hypothesis is that the enhancement in the negative dromotropic effect and the P. Ballo et al. Heart rate is a predictor of success in the treatment of adults with symptomatic paroxysmal supraventricular tachycardia Conclusions In the treatment of symptomatic episodes of PSVT in adult subjects, both adenosine and verapamil demonstrated a high rate of success in terminating the tachycardia, whereas a poor response to carotid sinus massage was observed. The rate of the tachycardia may predict the success of pharmacological treatment. The efficacy of adenosine was directly related to the frequency of the arrhythmia, so it should be considered the treatment of choice in patients with PSVT characterised by high heart rates. Conversely, the efficacy of verapamil seems to be increased in patients with low-frequency PSVT, so that it could be appropriately used as the first-line treatment in these subjects. References 1. Orejarena LA, Vidaillet HJR, DeStefano F et al. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol 1998;31:150–7. 2. Luber S, Brady WJ, Joyce T et al. Paroxysmal supraventricular tachycardia: outcome after ED care. Am J Emerg Med 2001;19:40–2. 3. Kadish A, Passman R. Mechanisms and management of paroxysmal supraventricular tachycardia. Cardiol Rev 1999;7:254–64. 4. Paparella N, Alboni P. Classification and prevalence of supraventricular tachyarrhythmia. Cardiologia 1991;36:7–10. 5. Brembilla-Perrot B, Houriez P, Beurrier D et al. Influence of age on the electrophysiological mechanism of paroxysmal supraventricular tachycardias. Int J Cardiol 2001;78:293–8. 6. Accardi AJ, Miller R, Holmes JF. Enhanced diagnosis of narrow complex tachycardias with increased electrocardiograph speed. J Emerg Med 2002;22:123–6. 7. Kalbfleisch SJ, el-Atassi R, Calkins H et al. Differentiation of paroxysmal narrow QRS complex tachycardias using the 12-lead electrocardiogram. J Am Coll Cardiol 1999;21:85–9. 8. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6: advanced cardiovascular life support: 7D: the tachycardia algorithms. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation 2000;102:I158–65. 9. Junga G, Candinas R Schweiz. Modern therapy of paroxysmal supraventricular tachycardia. Rundsch Med Prax 1999;88:273–7. 10. Paul T, Bertram H, Bokenkamp R et al. Supraventricular tachycardia in infants, children and adolescents: diagnosis, and pharmacological and interventional therapy. Paediatr Drugs 2000;2:171–81. 11. Brady Jr WJ, DeBehnke DJ, Wickman LL et al. Treatment of out-ofhospital supraventricular tachycardia: adenosine vs verapamil. Acad Emerg Med 1996;3:574–85. 12. Gil Madre J, Lazaro Rodriguez S, Sentenac Merchan G et al. Adenosine triphosphate in the treatment of supraventricular paroxysmal tachycardia: a comparison with verapamil. Rev Esp Cardiol 1995;48:55–8. 13. Davis R, Spitalnic SJ, Jagminas L. Cost-effective adenosine dosing for the treatment of PSVT. Am J Emerg Med 1999;17:633–4. 14. Lee KL, Chun HM, Liem LB et al. Effect of adenosine and verapamil in catecholamine-induced accelerated atrioventricular junctional rhythm: insights into the underlying mechanism. Pacing Clin Electrophysiol 1999;22:866–70. 15. Kirton OC, Windsor J, Wedderburn R et al. Management of paroxysmal atrioventricular nodal reentrant tachycardia in the critically ill surgical patient. Crit Care Med 1997;25:761–6. 16. Lim SH, Anantharaman V, Teo WS et al. Comparison of treatment of supraventricular tachycardia by Valsalva maneuver and carotid sinus massage. Ann Emerg Med 1998;31:30–5. 17. Lai WT, Lee CS, Wu SN. Rate-dependent properties of adenosineinduced negative dromotropism in humans. Circulation 1994;90: 1832–9. 18. Schwarzl I, Stark U, Kasper K et al. Quantification of rate-dependent effects of verapamil, diltiazem, and digoxin on atrioventricular conduction. J Pharmacol Toxicol Methods 1996;36:205–10. 19. Stark G, Sterz F, Stark U et al. Frequency-dependent effects of adenosine and verapamil on atrioventricular conduction of isolated guinea pig hearts. J Cardiovasc Pharmacol 1993;21:955–9. 20. Nayebpour M, Billette J, Amellal F et al. Effects of adenosine on rate-dependent atrioventricular nodal function. Potential roles in tachycardia termination and physiological regulation. Circulation 1993;88:2632–45. 21. Chiale PA, Franco DA, Selva HO et al. Lidocaine-sensitive atrial tachycardia: lidocaine-sensitive, rate-related, repetitive atrial tachycardia: a new arrhythmogenic syndrome. J Am Coll Cardiol 2000;36(1):1637–45. 22. Kwaku KF, Josephson ME. Typical AVNRT – an update on mechanisms and therapy. Card Electrophysiol Rev 2002;6:414–21. 23. Nawata H, Yamamoto N, Hirao K et al. Heterogeneity of anterograde fast-pathway and retrograde slow-pathway conduction patterns in patients with the fast-slow form of atrioventricular nodal reentrant tachycardia: electrophysiological and electrocardiographic considerations. J Am Coll Cardiol 1998;32:1731–40. 24. Delise P, Bonso A, Coro L et al. Pacemapping of the triangle of Koch: a simple method to reduce the risk of atrioventricular block during radiofrequency ablation of atrioventricular node reentrant tachycardia. Pacing Clin Electrophysiol 2001;24:1725–31. 25. Heinroth KM, Kattenbeck K, Stabenow I et al. Multiple AV nodal pathways in patients with AV nodal reentrant tachycardia–more common than expected. Europace 2002;4:375–82. Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 study population revealed electrographic findings suggestive for AV-nodal reciprocant tachycardia in 66 cases (62.3%), for AV-reciprocant tachycardia in 32 cases (30.2%) and for atrial tachycardia in only eight cases (7.5%). Also, the protocol of the study was designed taking into account that: (1) PSVT subtype identification by surface ECG is often difficult to perform, particularly when the tachycardia presents high frequencies, (2) electrophysiological tests are not routinely performed in clinical practice, (3) although various electrocardiographic criteria have been proposed in the attempt to distinguish different types of PSVT,100–102 about 20% of PSVT may be incorrectly classified on the basis of the surface ECG.7 The possibility that some cases of regular atrial flutter with conduction ratio 2:1 have been classified as PSVT or vice versa should also be taken into account. By design, only symptomatic episodes were included in this study, yet sub-clinical PSVT seems to be uncommon.103 This study did not analyse the potential effect of other clinical variables on the efficacy of the treatment of PSVT, such as a history positive for previous episodes of PSVT and duration of the arrhythmia. Many of the patients with PSVT often complain of previous undocumented episodes of palpitations, and it is hard to establish whether the arrhythmia is a relapse or a first episode in these cases. Also, most patients with PSVT are not able to determine the onset of the symptoms with sufficient precision, so that introducing the duration of the tachycardia as a study variable would have produced a relevant risk of biases in the analysis. In addition, it should be considered that this study was retrospective and not randomised, so that the results have to be interpreted with caution. Lastly, the effect of heart rate on the percentage of success in the treatment of PSVT using other therapeutic approaches has not been evaluated. Larger prospective trials and further studies are needed to analyse these aspects. 1315 1316 47. Reimold SC, Maisel WH, Antman EM. Propafenone for the treatment of supraventricular tachycardia and atrial fibrillation: a metaanalysis. Am J Cardiol 1998;82:66N–71N. 48. Gambhir DS, Bhargava M, Arora R et al. Electrophysiological effects and therapeutic efficacy of intravenous flecainide for termination of paroxysmal supraventricular tachycardia. Indian Heart J 1995;47: 237–43. 49. Page RL, Connolly SJ, Wilkinson WE et al. Antiarrhythmic effects of azimilide in paroxysmal supraventricular tachycardia: efficacy and dose–response. Am Heart J 2002;143:643–9. 50. Tendera M, Wnuk-Wojnar AM, Kulakowski P et al. Efficacy and safety of dofetilide in the prevention of symptomatic episodes of paroxysmal supraventricular tachycardia: a 6-month double-blind comparison with propafenone and placebo. Am Heart J 2001;142:93–8. 51. Pritchett EL, Wilkinson WE. Effect of dofetilide on survival in patients with supraventricular arrhythmias. Am Heart J 1999;138:994–7. 52. Gambhir DS, Bhargava M, Nair M et al. Comparison of electrophysiological effects and efficacy of single-dose intravenous and longterm oral amiodarone therapy in patients with AV nodal reentrant tachycardia. Indian Heart J 1996;48:133–7. 53. Price JF, Kertesz NJ, Snyder CS et al. Flecainide and sotalol: a new combination therapy for refractory supraventricular tachycardia in children <1 year of age. J Am Coll Cardiol 2002;39:517–20. 54. Alboni P, Tomasi C, Menozzi C et al. Efficacy and safety of out-ofhospital self-administered single-dose oral drug treatment in the management of infrequent, well-tolerated paroxysmal supraventricular tachycardia. J Am Coll Cardiol 2001;37:548–53. 55. Lerman BB, Ellenbogen KA, Kadish A et al. Electrophysiologic effects of a novel selective adenosine A1 agonist (CVT-510) on atrioventricular nodal conduction in humans. J Cardiovasc Pharmacol Ther 2001;6:237–45. 56. Ellenbogen KA. Randomized, double-blind, placebo-controlled study of intravenous CVT-510 in patients with PSVT undergoing an electrophysiologic study. Program and abstracts from American Heart Association Scientific Sessions 2002, November 17–20, 2002; Chicago, IL. 57. Volkmann H, Dannberg G, Heinke M et al. Termination of tachycardias by transesophageal electrical pacing. Pacing Clin Electrophysiol 1992;15:1962–6. 58. Lowenstein SR, Halperin BD, Reiter MJ. Paroxysmal supraventricular tachycardias. J Emerg Med 1996;14:39–51. 59. Pfammatter JP, Bauersfeld U. Safety issues in the treatment of paediatric supraventricular tachycardias. Drug Saf 1998;18:345–56. 60. Mathew J, Hunsberger S, Fleg J et al. Incidence, predictive factors, and prognostic significance of supraventricular tachyarrhythmias in congestive heart failure. Chest 2000;118:914–22. 61. Jaeggi E, Fouron JC, Fournier A et al. Ventriculo-atrial time interval measured on M mode echocardiography: a determining element in diagnosis, treatment, and prognosis of fetal supraventricular tachycardia. Heart 1998;79:582–7. 62. Knight BP, Ebinger M, Oral H et al. Diagnostic value of tachycardia features and pacing maneuvers during paroxysmal supraventricular tachycardia. J Am Coll Cardiol 2000;36:574–82. 63. Matsui Y, Iwasaka T, Karakawa M et al. Left ventricular systolic time intervals during paroxysmal supraventricular tachycardia: the difference between A-V nodal re-entry and A-V re-entry. J Cardiol 1992;22:679–85. 64. Knight BP, Zivin A, Souza J et al. A technique for the rapid diagnosis of atrial tachycardia in the electrophysiology laboratory. J Am Coll Cardiol 1999;33:775–81. 65. Akhtar M, Jazayeri MR, Sra J et al. Atrioventricular nodal reentry. Clinical, electrophysiological, and therapeutic considerations. Circulation 1993;88:282–95. 66. Nakagawa H, Jackman WM. Catheter ablation of macroreentrant atrial tachycardia in patients following atriotomy. Eur Heart J 2002;23:1566–8. 67. Kopf GS, Mello DM, Kenney KM et al. Intraoperative radiofrequency ablation of the atrium: effectiveness for treatment of supraventricular tachycardia in congenital heart surgery. Ann Thorac Surg 2002;74:797–804. 68. Wetzel U, Hindricks G, Schirdewahn P et al. A stepwise mapping approach for localization and ablation of ectopic right, left, and septal atrial foci using electroanatomic mapping. Eur Heart J 2002;23:1387–93. Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 26. Wu J, Zipes DP. Mechanisms underlying atrioventricular nodal conduction and the reentrant circuit of atrioventricular nodal reentrant tachycardia using optical mapping. J Cardiovasc Electrophysiol 2002;13:831–4. 27. Luria DM, Chugh SS, Munger TM et al. Electrophysiologic characteristics of diverse accessory pathway locations of antidromic reciprocating tachycardia. Am J Cardiol 2000;86:1333–8. 28. Davidson NC, Morton JB, Sanders P et al. Latent Mahaim fiber as a cause of antidromic reciprocating tachycardia: recognition and successful radiofrequency ablation. J Cardiovasc Electrophysiol 2002;13:74–8. 29. Shah DC, Haissaguerre M, Jais P et al. High-resolution mapping of tachycardia originating from the superior vena cava: evidence of electrical heterogeneity, slow conduction, and possible circus movement reentry. J Cardiovasc Electrophysiol 2002;13:388–92. 30. Matsuoka K, Kasai A, Fujii E et al. Electrophysiological features of atrial tachycardia arising from the atrioventricular annulus. Pacing Clin Electrophysiol 2002;25:440–5. 31. Katritsis D, Giazitzoglou E, Korovesis S et al. Epicardial foci of atrial arrhythmias apparently originating in the left pulmonary veins. J Cardiovasc Electrophysiol 2002;13:319–23. 32. Hegbom F, Hoff PI, Rossvoll O et al. A typical P-wave morphology in incessant atrial tachycardia originating from the right upper pulmonary vein. Scand Cardiovasc J 2000;34:277–80. 33. Ouyang F, Ernst S, Vogtmann T et al. Characterization of reentrant circuits in left atrial macroreentrant tachycardia: critical isthmus block can prevent atrial tachycardia recurrence. Circulation 2002;105(23):1934–42. 34. Markowitz SM, Brodman RF, Stein KM et al. Lesional tachycardias related to mitral valve surgery. J Am Coll Cardiol 2002;39(19): 1973–83. 35. Marrouche NF, Sippens Groenewegen A, Yang Y et al. Clinical and electrophysiological characteristics of left septal atrial tachycardia. J Am Coll Cardiol 2002;40(18):1133–9. 36. Dong J, Schreieck J, Ndrepepa G et al. Ectopic tachycardia originating from the superior vena cava. J Cardiovasc Electrophysiol 2002;13:620–4. 37. Ma G, Brady WJ, Pollack M et al. Electrocardiographic manifestations: digitalis toxicity. J Emerg Med 2001;20:145–52. 38. Blomstrom-Lundqvist C, Scheinman MM, Aliot EM et al. European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias – executive summary. A report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol 2003;42:1493–531. 39. Ferguson JD, DiMarco JP. Contemporary management of paroxysmal supraventricular tachycardia. Circulation 2003;107:1096–9. 40. Hebbar AK, Hueston WJ. Management of common arrhythmias: Part I. Supraventricular arrhythmias. Am Fam Physician 2002;65(15): 2479–86. 41. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6: advanced cardiovascular life support: section 5: pharmacology I: agents for arrhythmias. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation 2000;102:I-112–28. 42. Lim SH, Anantharaman V, Teo WS. Slow-infusion of calcium channel blockers in the emergency management of supraventricular tachycardia. Resuscitation 2002;52:167–74. 43. Gupta A, Naik A, Vora A et al. Comparison of efficacy of intravenous diltiazem and esmolol in terminating supraventricular tachycardia. J Assoc Physicians India 1999;47:969–72. 44. Dougherty AH, Jackman WM, Naccarelli GV et al. Acute conversion of paroxysmal supraventricular tachycardia with intravenous diltiazem. IV Diltiazem Study Group. Am J Cardiol 1992;70:587–92. 45. Balser JR, Martinez EA, Winters BD et al. Beta-adrenergic blockade accelerates conversion of postoperative supraventricular tachyarrhythmias. Anesthesiology 1998;89:1052–9. 46. Barbier GH, Shettigar UR, Appunn DO. Clinical rationale for the use of an ultra-short acting beta-blocker: esmolol. Int J Clin Pharmacol Ther 1995;33:212–8. P. Ballo et al. Heart rate is a predictor of success in the treatment of adults with symptomatic paroxysmal supraventricular tachycardia 86. Yue L, Feng JL, Wang Z et al. Effects of ambasilide, quinidine, flecainide and verapamil on ultra-rapid delayed rectifier potassium currents in canine atrial myocytes. Cardiovasc Res 2000;46:151–61. 87. Chouabe C, Drici MD, Romey G et al. Effects of calcium channel blockers on cloned cardiac Kþ channels IKr and IKs. Therapie 2000;55:195–202. 88. DeCoursey TE. Mechanism of Kþ channel block by verapamil and related compounds in rat alveolar epithelial cells. J Gen Physiol 1995;106:745–79. 89. Talajic M, Nattel S. Frequency-dependent effects of calcium antagonists on atrioventricular conduction and refractoriness: demonstration and characterization in anesthetized dogs. Circulation 1986;74:1156–67. 90. Stark G, Schulze-Bauer C, Stark U et al. Comparison of the frequency-dependent effects on the atrioventricular node of verapamil, amiodarone, digoxin, and diltiazem in isolated guinea pig hearts. J Cardiovasc Pharmacol 1995;25:330–5. 91. Lang J, Timour Chah Q, Charve P et al. Role of calcium in the ratedependent depression of atrioventricular nodal conduction in the dog heart under vagal influence. Int J Cardiol 1987;15:65–76. 92. Qi AZ, Tuna IC, Gornick CC et al. Potentiation of cardiac electrophysiologic effects of verapamil after autonomic blockade or cardiac transplantation. Circulation 1987;75:888–93. 93. Hassan SA, Oral H, Scharf C et al. Rate-dependent effect of verapamil on atrial refractoriness. J Am Coll Cardiol 2003;41:446–51. 94. Sato N, Tanaka H, Habuchi Y et al. Electrophysiological effects of ibutilide on the delayed rectifier K(+) current in rabbit sinoatrial and atrioventricular node cells. Eur J Pharmacol 2000;404:281–8. 95. Fujino H, Fujiseki Y, Shimada M. Electrophysiologic effects of calcium channel blockers on supraventricular tachycardia in children. J Cardiol 1989;19:307–15. 96. Bhandari AK. Atrial Tachycardia. Curr Treat Options Cardiovasc Med 1999;1:107–16. 97. Steinbeck G, Hoffmann E. ‘True’ atrial tachycardia. Eur Heart J 1998;19(Suppl E):E10–2, E48–9. 98. Simons GR, Wharton JM. Radiofrequency catheter ablation of atrial tachycardia and atrial flutter. Coron Artery Dis 1996;7:12–9. 99. Dierkes S, Vester EG, Dobran LJ et al. Adenosine in the noninvasive diagnosis of dual AV nodal conduction: use as a follow-up parameter after slow pathway ablation in AVNRT. Acta Cardiol 2001;56:103–8. 100. Maglana MP, Kam RM, Teo WS. The differential diagnosis of supraventricular tachycardia using clinical and electrocardiographic features. Ann Acad Med Singapore 2000;29:653–7. 101. Maury P, Zimmermann M, Metzger J. Distinction between atrioventricular reciprocating tachycardia and atrioventricular node reentrant tachycardia in the adult population based on P wave location. Should we reconsider the value of some ECG criteria according to gender and age? Europace 2003;5:57–64. 102. Ho YL, Lin LY, Lin JL et al. Usefulness of ST-segment elevation in lead aVR during tachycardia for determining the mechanism of narrow QRS complex tachycardia. Am J Cardiol 2003;92:1424–8. 103. Page RL, Wilkinson WE, Clair WK et al. Asymptomatic arrhythmias in patients with symptomatic paroxysmal atrial fibrillation and paroxysmal supraventricular tachycardia. Circulation 1994;89:224–7. Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 9, 2014 69. Cauchemez B, Lavergne T, Extramiana F et al. Endocavitary ablation for arrhythmias. New modalities of radiofrequency applications. New energy types. Arch Mal Coeur Vaiss 2002;95(Spec No 5): 31–9. 70. Hood MA, Smith WM. Adenosine versus verapamil in the treatment of supraventricular tachycardia: a randomized double-crossover trial. Am Heart J 1992;123:1543–9. 71. Morrison LJ, Allan R, Vermeulen M et al. Conversion rates for prehospital paroxysmal supraventricular tachycardia (PSVT) with the addition of adenosine: a before-and-after trial. Prehosp Emerg Care 2001;5:353–9. 72. Arnold RW. The human heart rate response profiles to five vagal maneuvers. Yale J Biol Med 1999;72:237–44. 73. Wen ZC, Chen SA, Tai CT et al. Electrophysiological mechanisms and determinants of vagal maneuvers for termination of paroxysmal supraventricular tachycardia. Circulation 1998;98:2716–23. 74. Mehta D, Wafa S, Ward DE et al. Relative efficacy of various physical manoeuvres in the termination of junctional tachycardia. Lancet 1988;1:1181–5. 75. Domanovits H, Laske H, Stark G et al. Adenosine for the management of patients with tachycardias – a new protocol. Eur Heart J 1994; 15:589–93. 76. Martynyuk AE, Seubert CN, Zima A et al. Contribution of I(K, ADO) to the negative dromotropic effect of adenosine. Basic Res Cardiol 2002;97:286–94. 77. Tai CT, Chen SA, Chiang CE et al. Influence of beta-adrenergic and vagal activity on the effect of exogenous adenosine on supraventricular tachycardia termination. Am J Cardiol 1997;79(15): 1628–31. 78. Chang KC, Lin YC, Chen JY et al. Interactions of esmolol and adenosine in atrioventricular nodal-dependent supraventricular tachycardia: implication for the cellular mechanisms of adenosine. Cardiology 2002;97:138–46. 79. Martynyuk AE, Zima A, Seubert CN et al. Potentiation of the negative dromotropic effect of adenosine by rapid heart rates: possible ionic mechanism. Basic Res Cardiol 2002;97:295–304. 80. Tonkin AM, Aylward PE, Joel SE et al. Verapamil in prophylaxis of paroxysmal atrioventricular nodal reentrant tachycardia. J Cardiovasc Pharmacol 1980;2:473–86. 81. Prystowsky EN. The effects of slow channel blockers and beta blockers on atrioventricular nodal conduction. J Clin Pharmacol 1988;28:6–21. 82. Tonkin AM, Shorne L. The prophylaxis of AV nodal re-entry tachycardia. Clin Exp Pharmacol Physiol Suppl 1982;6:135–43. 83. Iinuma H, Dreifus LS, Price R et al. Influence of the site of stimulation on atrioventricular nodal refractory periods and the effect of verapamil. Am J Cardiol 1986;57:1167–74. 84. Stark G, Kasper K, Schulze-Bauer C et al. How to measure AV nodal refractoriness in the presence of verapamil, amiodarone, digoxin, and diltiazem. Pacing Clin Electrophysiol 1996;19:157–64. 85. Segawa K. The relationship between refractory period and conduction time of the AV node under various cycle lengths in the canine heart. The significance of wavelength and excitable gap in reentrant tachycardia. Jpn Heart J 1996;37:373–82. 1317









© Copyright 2025