
Common Dermatologic Presentations: The Red Face THE RED FACE
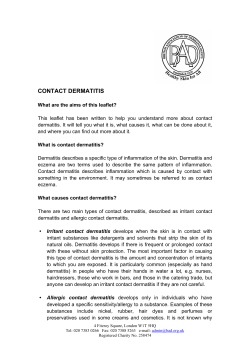
THE RED FACE Common Dermatologic Presentations: The Red Face Sharon Barthelette, MD, Laura Rosenzweig, BA, Kimberly A. Cayce, MD, Gloria F. Graham, MD, and Steven R. Feldman, MD, PhD Abstract • Objective: To review common dermatologic causes of the “red face.” • Methods: Qualitative assessment of the literature. • Results: Patients with dermatologic problems frequently present in the primary care setting. The most common causes of “red face” are rosacea, acne, actinic keratoses, seborrheic dermatitis, and atopic dermatitis. In cases without complicating factors, the primary care physician can make a clinical diagnosis and initiate treatment. If the diagnosis is in question or the patient has many complicating factors, a referral to a dermatologist or other specialist may be indicated. • Conclusion: Prompt recognition and understanding of common causes of red face will prevent costly diagnostic studies and direct essential therapy. C utaneous disease is frequently encountered in primary care. In a chart review study of 570 patients who presented to their primary care physician, 36.5% had at least one skin problem, and in more than half of those with skin disease, their skin condition was the chief complaint [1]. The presenting complaint of a “red face” may suggest a wide range of skin diseases. The more common include rosacea, acne vulgaris, and various forms of dermatitis. In most cases, a thorough history and physical should be sufficient to make a diagnosis and to select appropriate initial therapy. Prompt recognition and understanding of these common conditions will prevent costly diagnostic studies and direct essential therapy. If the diagnosis is in question or the patient has many complicating factors, a referral to a dermatologist or other specialist may be indicated. This article discusses the clinical presentation, diagnosis, and treatment of common skin diseases that present as red face. use of over-the-counter anti-acne washes. He is otherwise healthy and is not taking any medications. Physical examination reveals pustules and open comedones on the forehead, cheeks, and chin. There are no cysts or nodules present. This patient has a mild form of acne vulgaris. Acne affects almost 80% of people at some point between the ages of 11 and 30 years [2]. Acne often occurs on the face, chest, and back (and occasionally the buttocks) and appears as comedones (comedonal acne) (Figure 1a), papulopustules (papulopustular acne) (Figure 1b), or nodules (nodular acne and acne conglobata) (Figure 1c). The severity of acne is determined by the number of papules, pustules, and nodules present; however, factors such as psychosocial impact and previous response to therapy also are considered [3]. Mild acne consists of few papules and pustules but no nodules, while numerous papules, pustules, and nodules constitute severe disease [3]. Acne conglobata, which usually spares the face, is the most severe form and is characterized by burrowing and interconnecting abscesses and scars, leading to pronounced disfigurement. Acne is caused by pilosebaceous gland inflammation and follicular plugging and usually develops during puberty, when elevated levels of circulating androgens enhance pilosebaceous gland activity. However, acne does not necessarily remit with the end of puberty, and it may present beyond the mid-twenties. Acne tends to be more severe in men and has been associated with XYY syndrome [4]. The occurrence of acne appears to have a genetic component in that the majority of patients with nodular acne have a parent with severe acne [5]. Differential Diagnosis Several red face conditions must be distinguished from acne. Rosacea may present with papules and pustules but is typified Case 1—Acne A 14-year-old boy presents to his primary care physician with a complaint of a “red face with bumps for the past half year.” He has noticed some improvement following 36 JCOM January 2004 Vol. 11, No. 1 From the Department of Dermatology, University of Texas Health Science Center at San Antonio, San Antonio, TX (Dr. Barthelette); and the Center for Dermatology Research, Wake Forest University School of Medicine, WinstonSalem, NC (Ms. Rosenzweig and Drs. Cayce, Graham, and Feldman). www.turner-white.com CLINICAL REVIEW A B C Figure 1. (A) Comedonal acne, (B) papulopustular acne, and (C) nodular acne. A B C Figure 2. Presentation of rosacea. (A) Persistent erythema seen in rosacea, (B) papulopustular rosacea, and (C) rhinophyma. Figure 3. Perioral dermatitis. Figure 4. Contact dermatitis. by facial flushing and telangiectasias, and comedones are not present. In perioral dermatitis, micropapulopustules characteristically are concentrated around the mouth. Infectious folliculitis, whether gram-positive or gram-negative, may sometimes be confused with acne. The clinician should suspect gram-negative folliculitis in acne patients on prolonged antibiotics whose acne suddenly worsens. The follicular papules and pustules seen in eosinophilic pustular folliculitis are pruritic and are generally more extensive, involving the face, neck, www.turner-white.com Figure 5. Actinic keratoses. trunk, and proximal extremities. Acne excorie, small eroded lesions that have been picked at, may occur alone or in conjunction with acne, making the acne appear much worse. Etiology and Pathogenesis The occurrence of acne results from a number of interacting factors. During adolescence and young adulthood, androgens stimulate the sebaceous glands to produce more sebum. Abnormal desquamation of the epithelial cells leads to Vol. 11, No. 1 January 2004 JCOM 37 THE RED FACE Figure 6. Seborrheic dermatitis. Figure 7. Atopic dermatitis. Figure 9. Ulerythema ophryogenes. A B Figure 8. Tinea faciei. Figure 10. Dermatomyositis. C Figure 11. (A) Acute, (B) subacute, and (C) chronic forms of cutaneous lupus erythematosus. obstruction of the sebaceous follicle, which appears clinically as noninflammatory open comedones (blackheads) and closed comedones (whiteheads). As the amount of sebum within the blocked follicle increases, the sebum leaks across the follicular wall into the dermis. The presence of sebum within the dermis induces the skin inflammation visible as papules, pustules, and nodules. Within the blocked ducts, the skin bacteria Propionibacterium acnes proliferate and produce large amounts of free fatty acids. The inflammatory 38 JCOM January 2004 Vol. 11, No. 1 process is augmented by chemotactic factors (activation of the classic and alternative complement pathways results in the formation of C5a and production of low-molecularweight, serum-independent neutrophil chemotactic factors) and proinflammatory mediators (lysosomal enzymes and reactive oxygen species) [6,7]. When taking the history of a new patient, the clinician should ask about cofactors in the occurrence of acne. Patients may be using acne-promoting medications such as lithium, www.turner-white.com CLINICAL REVIEW hydantoins, androgens, and glucocorticoids. Some comedogenic cosmetics may contribute to the occurrence of acne. Patients should opt for water-based cosmetics. Contrary to urban folklore, there is no substantial evidence that acne is caused by certain foods such as chocolate or fried foods. Patients with acne may develop their own home remedies that involve harsh abrasives. These cleaning techniques will aggravate the acne and should be avoided. Additionally, pressure from propping the face on the hands and occlusion from leaning on the telephone can be aggravating to the acne lesions. These directly irritating factors are termed “acne mechanica” and often are overlooked by the patient [8]. Treatment Because adolescents and adults with acne can experience low self-esteem, depression, and social isolation, it is important to treat acne promptly and aggressively. Medical therapy of acne is determined by severity of the disease. A report from the Global Alliance to Improve the Outcomes of Acne included guidelines for acne therapy [9]. Mild disease. First-line therapy for treating mild acne with comedones and little inflammation is tretinoin, a topical retinoid. Tretinoin is a vitamin A derivative that both unseats existing comedones and retards the creation of new ones by increasing the rate of cell turnover and decreasing cell adhesion [10]. Side effects of tretinoin include dryness and erythema. Patients with sensitive skin may benefit from the milder cream formulation (0.025% cream) as opposed to the gel variety (0.01% gel). A microencapsulated tretinoin 0.1% gel has been developed that may be less irritating. If these formulations are intolerable, patients may use tretinoin less frequently (3 times a week) and slowly increase the frequency of application to once per day. Patients should be educated about increased photosensitivity while on vitamin-A– derived therapy and should be advised to limit sun exposure and wear sunscreen. An alternative topical retinoid is tazarotene gel, which was proven in a multicenter, doubleblind, vehicle-controlled study to be safe and effective for mild to moderate acne [11]. Adapalene (gel or solution) is a naphthoic acid agent with action similar to tretinoin but is gentler on the skin [12]. Topical antimicrobial therapy can be added when there is an increased inflammatory component in the acne presentation. Clindamycin and erythromycin topicals are primarily used and are equally effective [13]. These agents inhibit the proliferation and activity of P. acnes and mildly decrease inflammatory response. They are available in a variety of forms, including lotions, solutions, gels, creams, and medicated pads. Benzoyl peroxide is a topical antibacterial agent that also is available in a variety of formulations (cleanser, gel, cream, lotion, solution, pads) and concentrations (2.5%, www.turner-white.com 5%, 10%) and can be applied once or twice daily. Weaker concentrations are available over the counter. When initiating topical antibacterial therapy, clinicians should advise patients that initially their skin may become mildly red and scaly but this side affect will likely abate with continued use. Contact allergy may occur in 1% to 2% of patients; signs of allergic reaction should prompt discontinuation of the therapy [13]. Benzoyl peroxide should not be applied concurrently with topical tretinoin because it will oxidize the tretinoin, rendering it ineffective; benzoyl peroxide may be used in the morning, with tretinoin applied at night. This interaction is not an issue with other retinoids such as adapalene and tazarotene. Benzoyl peroxide has been combined with topical erythromycin in an effective formulation. Another topical alternative is azelaic acid 20%, which has comedolytic and antimicrobial properties [14] as well as a skin lightening effect that is useful in alleviating postinflammatory hyperpigmentation. Moderate disease. In moderate acne or failed topical regimens, oral antibiotics in addition to the topical retinoids are appropriate. Frequently used oral antibiotics include tetracycline, doxycycline, minocycline, trimethoprim-sulfamethoxazole, and erythromycin. Oral tetracycline (initially 500 mg twice daily) is an affordable, effective treatment modality. Tetracycline must be taken on an empty stomach to be effective, while doxycycline and minocycline, which are derivatives of tetracycline, can be taken with food. Adverse effects of doxycycline include gastrointestinal upset and increased photosensitivity. Antibiotic resistance is less likely to develop with minocycline than with other antibiotics [15]. However, the use of minocycline is limited by its higher cost and potential adverse effects, which include reversible central nervous system disturbances (ataxia and vertigo), mucocutaneous pigmentary changes, and the rare development of drug-induced hepatotoxicity and systemic lupus erythematosus [16,17]. Tetracycline, doxycycline, and minocycline should not be used in children or pregnant women due to their capacity to stain developing teeth yellow. Erythromycin can be used in pregnancy, and it can be taken with food; however, it may cause significant gastrointestinal upset. Trimethoprimsulfamethoxazole may be used in erythromycin- and tetracycline-resistant acne but should be avoided in patients allergic to sulfonamides. Once the desired effect of the antibiotics has been achieved, the dosage should be gradually tapered over several months to maintain control. Patients should be instructed to increase their dosage to the original starting dose if an acne flare occurs while tapering. Female patients may benefit from the use of oral contraceptive pills that contain both estrogens and antiandrogens [18]. Estrogens can improve acne by decreasing sebum production and diminishing androgen effects (by blocking Vol. 11, No. 1 January 2004 JCOM 39 THE RED FACE testosterone-receptor sites and lowering free testosterone and dehydroepiandrosterone-sulfate levels). They are particularly beneficial in patients whose acne appears to flare at certain times in the menstrual cycle. Patients with signs of polycystic ovarian disease, including hirsutism, acne, and obesity, also will benefit from hormonal therapy. The first low-dose oral contraceptive to receive an indication for acne treatment by the Food and Drug Administration (FDA) was norgestimate/ ethinyl estradiol. Drospirenone/ethinyl estradiol also is effective in treating acne. This agent is unique in that it contains drospirenone, a derivative of 17α-spironolactone, which is a potassium-sparing diuretic with antiandrogenic properties. A trial of spironolactone may be attempted in female patients when other therapies have failed and pregnancy will be avoided during the treatment period. This drug, usually initiated at 25 mg daily, blocks androgen receptors and inhibits 5α-reductase activity. More potent antiandrogenic drugs have been used in Europe with overwhelming success [18]; however, these agents are not available in the United States. Hormonal agents can be used with topical and oral acne therapies. Severe disease. For severe or recalcitrant cases of acne, referral should be made to a dermatologist for oral isotretinoin therapy. Isotretinoin is indicated for patients in whom topical therapies and oral antibiotics have failed, especially in the setting of severe nodular or scarring acne. Patients may need isotretinoin therapy for up to 5 months, and repeat courses of drug therapy may be necessary for recurrences. Prior to beginning isotretinoin therapy, 2 negative pregnancy tests must be performed on any woman of reproductive age, regardless of response to questions about sexual activity. Oral isotretinoin is a highly teratogenic drug that can result in fetal central nervous system anomalies, facial dysmorphia, and ear, eye, and cardiovascular abnormalities [19]. Sexually active women should use 2 contraceptive methods from 1 month before beginning isotretinoin therapy until 1 month after completing the therapy. Urine pregnancy tests also should be performed at monthly visits. Adverse effects of isotretinoin are common and include cheilitis, blepharoconjunctivitis, epistaxis, and photosensitivity. Less frequent side effects include decreased night vision, headache, and hair loss. Myalgias and arthralgias are common in patients undergoing isotretinoin therapy, but myalgias and arthralgias also are associated with untreated acne conglobata and acne fulminans [20]. Approximately 10% of patients with isotretinoin-related musculoskeletal pains develop asymptomatic bony growths of the spine [19]. A rare adverse effect of isotretinoin use is pseudotumor cerebri. Isotretinoin therapy also has been associated with elevated triglycerides, dyslipidemias, and liver function test abnormality. For this reason, measurements of lipid levels and 40 JCOM January 2004 Vol. 11, No. 1 liver function should be performed prior to and during isotretinoin therapy. Patients must be seen monthly for the duration of isotretinoin therapy for clinical evaluation, laboratory work review, and medication refills. The relationship between depression and isotretinoin therapy has been widely debated. The FDA’s Adverse Event Reporting System database lists 37 reports of suicide, 110 reports of hospitalization for depression, suicidal ideation, or suicide attempt, and 284 reports of depression without hospitalization in patients receiving isotretinoin between 1982 and 2000 [21]. However, no molecular link between depression and isotretinoin has been identified, and there does not seem to be a causal relationship between suicide and isotretinoin therapy [22]. Nevertheless, clinicians who prescribe isotretinoin should continually monitor for signs of depression and stop the medication promptly if depressive symptoms occur. Typically, comedonal and papulopustular acne can be managed by a primary care provider. Cases resistant to topical keratolytics and an adequate course of oral antibiotics (continuous, full-dose therapy for at least 1 year) should be referred to a dermatologist [23,24]. Patients with nodular acne should be referred to a dermatologist in a more timely manner to help avoid permanent physical and psychologic consequences. Case 2—Rosacea A 45-year-old white woman presents with complaints of 2 years of facial flushing. She reports that the flushing intensifies when she drinks tea and coffee. She experienced mild acne as an adolescent. She is in good health and takes no medicines other than a once-a-day vitamin. Her mother experienced similar facial reddening when she was in her forties. Physical examination of the patient reveals an erythematous face with clusters of papules and pustules on the chin and cheeks. This patient has rosacea, a condition that affects 13 to 14 million Americans [25,26]. The age of onset of rosacea is between 30 and 50 years. It is most common in persons of Celtic origin and has a 3:1 female predominance. A history of acne vulgaris may be present, but it is not necessary for the development of rosacea. Patients with rosacea present with flushing or persistent erythema (Figure 2a), telangiectasias, and clusters of papules and pustules (Figure 2b). Secondary features of rosacea include a burning or stinging sensation, elevated red plaques, or rough, scaly patches. Women are more likely to be symptomatic on the chin and cheeks, while men often show signs of rosacea on the nose [27]. Chronic disease may result in a bulbous appearance of the nose, termed “rhinophyma” (Figure 2c). Ocular symptoms occur in many patients with rosacea and occasionally present www.turner-white.com CLINICAL REVIEW without facial skin signs. The signs of ocular rosacea include conjunctival injection, eyelid margin irritation, and telangiectasias. The patient with ocular rosacea may report stinging, foreign body sensation, and tearing [28,29]. tional stress. Many people may associate the findings of rosacea with chronic alcoholism. Although alcohol may be a trigger for flares of rosacea, the signs of rosacea are not secondary to long-term alcohol abuse. Differential Diagnosis A variety of diseases may present with signs and symptoms similar to those in rosacea. Lupus erythematosus may be considered in the differential diagnosis; however, lupus erythematosus is less likely to have the pustules of rosacea and presents with the classic malar rash in approximately half of patients. Rosacea may be differentiated from acne vulgaris by the absence of comedones in rosacea. Seborrheic dermatitis also should be considered, but its distribution includes the scalp, glabella, and nasolabial and mesiolabial folds. Seborrheic dermatitis is characterized by the presence of greasy scales that are noticeably absent in rosacea. One “do not miss” diagnosis is carcinoid syndrome secondary to a malignant tumor presenting with paroxysmal flushing. Pustules and papules are not present in carcinoid syndrome. If carcinoid syndrome is suspected due to the presence of weight loss, diarrhea, blood pressure lability, or shortness of breath, a referral to an internist should be made promptly. Treatment Rosacea is not a curable disease, and the goal of therapy should be adequate control and alleviation of the symptoms. Clinicians can be of great help to patients by educating them about rosacea triggers. Rosacea patients should be advised to avoid hot drinks and foods, temperature extremes, and other rosacea stimuli. Mild disease is controlled via topical therapies, while more severe disease may require systemic therapy. Additionally, patients with ocular manifestations of rosacea may require referral to an ophthalmologist. Topical antibiotic medications are typically chosen first as therapy for mild to moderate rosacea. The FDA has approved metronidazole 0.75% (gel, cream, lotion) and metronidazole 1% (cream) for treatment of rosacea [35]. A study by Jorizzo et al showed equal efficacy of once- and twice-daily application of metronidazole 1% cream [36]. Patients with dry skin may better tolerate the cream formulations. Azelaic acid 20% cream applied twice daily for patients with papulopustular rosacea demonstrated a comparable response to treatment with 0.75% metronidazole [37]. Azelaic acid also is available in a 15% gel. Sulfacetamide is another useful topical agent, but it should not be prescribed to patients with sulfa allergies. Other secondline agents include clindamycin 1% solution, gel, or lotion and erythromycin 2% solution. Patients also may benefit from benzoyl peroxide 2.5%, gradually increasing to 5% and 10% concentrations. However, the drying nature of this product may make its use intolerable. In patients with papular and pustular lesions that do not respond to standard therapies, tretinoin cream (0.025%, 0.05%, 0.1%) may be applied. However, it must be used with caution as tretinoin may exacerbate the underlying inflammation and lead to worsening erythema and angiogenesis [38]. Those with concomitant acne vulgaris could benefit. Patients should start with the lowest concentration, applying it 2 to 3 times per week at night and gradually increasing the potency and frequency of use. Topical corticosteroids should be avoided in the treatment of rosacea. Although corticosteroids may initially alleviate the inflammation, chronically they will thin the skin and worsen its appearance. In fact, corticosteroid use on the face can induce erythema and pustule and papule formation, resulting in the so called steroid rosacea. Systemic treatment is preferred if topical treatment fails or if severe disease is seen on initial presentation. Oral antibiotics also are indicated for initial therapy of ocular rosacea. First-line agents include oral tetracycline, minocycline, and doxycycline. Oral trimethoprim-sulfamethoxazole and metronidazole are appropriate second-line treatment options. Etiology and Pathogenesis Despite the great number of studies examining the pathogenesis of rosacea, the precise etiology is still uncertain. The contributions of bacterial infections, mite infestations, and abnormal vasodilatory changes have been widely debated. The increased incidence of Helicobacter pylori positivity in patients with rosacea has led researchers to postulate an association between Helicobacter infection and skin disease [30]. However, a cause-and-effect relationship has not been firmly established. The hypothesized role of Demodex mites in the development of rosacea was supported by evidence of a higher prevalence and density of mites in the follicles of rosacea-affected patients compared with nonaffected patients [31]. However, tetracycline therapy for 1 month did not significantly decrease mite counts, although rosacea symptoms improved [32]. Abnormal vasodilation patterns have been identified in patients with rosacea. In one study, patients with rosacea had impaired venous blood flow from the face to the brain through the emissary veins, resulting in vasodilation of facial blood conduits [33]. The heightened vascular response to environmental stimuli as well as longstanding facial vasodilation is thought to result in the skin changes evident in rosacea. Flares of rosacea are provoked by a variety of stimuli [34]. Environmental factors, such as sun exposure or extreme cold, commonly prompt rosacea flares. Rosacea also may be aggravated by certain medications (ie, corticosteroids, niacin, nifedipine, nitroglycerin), spicy foods, hot drinks, and emowww.turner-white.com Vol. 11, No. 1 January 2004 JCOM 41 THE RED FACE A condition related to rosacea is perioral dermatitis. This disease occurs most commonly in women, often with a slightly earlier age of onset (age 16 to 45 years) than rosacea. It is not usually as chronic as rosacea. The lesions are similar in appearance to those in rosacea but are limited to the area surrounding the mouth (Figure 3). Occasionally, the periorbital areas, glabella, and forehead also are involved. The treatment of perioral dermatitis is similar to that of rosacea. Referral to a dermatologist should be considered for refractory or complicated disease. A dermatologist can prescribe isotretinoin for severe rosacea that is unresponsive to standard therapies. Patients with recalcitrant telangiectasias may benefit from pulsed-dye laser therapy [39]. The primary care physician should consider referring patients with rhinophyma for surgical intervention since this condition often does not respond to topical or oral medications. Options available for surgical treatment of rosacea include cryosurgery, dermabrasion, electrosurgery, or lasers. Case 3—Contact Dermatitis A 25-year-old white woman presents with complaints of facial itching and redness. She reports that the rash appeared overnight 5 days ago. She has no known allergies and is not taking any medications. She has been taking an over-the-counter antihistamine that she says moderately alleviates her pruritus. On physical examination, her face and neck are erythematous with scattered vesicles. The rash spares the periorbital and perioral regions. She also has increased redness of her palms. She reports no new animal or plant exposures. She denies using cosmetics. When asked about any recent travel, she reports a day trip to the beach almost a week ago. Further questioning reveals that she applied a friend’s sunscreen to her face at that time. This patient has a classic case of contact dermatitis, likely caused by sunscreen use. Contact dermatitis can present in a variety of forms depending on the location and duration of exposure. In acute eruptions, macular erythema, papules, vesicles, and bullae are seen (Figure 4). However, in chronic contact dermatitis, patients present with lichenified (thickened) skin with fissuring and crusting. When contact dermatitis affects the periorbital region (often seen in airborne allergens), the eyelids can become severely edematous. Common culprits found in contact dermatitis involving the area around the mouth include lipstick, chapstick (especially with sunscreens), toothpaste, bubblegum, and some foods. Differential Diagnosis Given the varied presentations of contact dermatitis, the differential diagnosis is broad. Leading the list of possibilities are atopic dermatitis and tinea infection. Taking a good pa42 JCOM January 2004 Vol. 11, No. 1 tient history is key. In a patient who has a region of eczematous skin, contact dermatitis should be foremost on the list of possible diagnoses. A thorough exposure history should be obtained with particular attention to exposures taking place around the time the patient noticed the rash. The clinician should ask about new cleaning products, cosmetics, topical medications, sunscreen, pets, or plants as well as about recreational activities and work conditions that may be the cause of the dermatitis. Persons at risk for occupational exposures include those working in the health care, agriculture, recreational, and maintenance industries. Skin disease is the second most common occupational illness in the United States, accounting for 41,800 cases and 11.5% of work-related illness [40]. The 2 forms of contact dermatitis, nonallergic irritant dermatitis and allergic dermatitis, cannot be differentiated based on physical examination alone. Not only do these 2 entities produce similar physical findings, but there also is significant overlap between the inflammatory mediators involved in their pathogenesis. In addition, there are many agents that can produce both allergic and nonallergic dermatitis. Nonallergic irritant variety dermatitis may involve single or chronic exposure to an agent that is directly toxic to the skin. Irritant dermatitis may occur within hours of the exposure to a strong agent or after several exposures to a weaker irritant. Responsible agents in irritant contact dermatitis include cleaning agents, abrasives, organic solvents, detergents, soaps, desiccant powders, plants, animal enzymes, soils, dusts, and water. Patch tests can be helpful in patients for whom the causative agent of the dermatitis cannot be identified. Patch testing is only useful in identifying causative agents of the allergic variety of contact dermatitis. The commercially available T.R.U.E. allergen patch test identifies allergies to 23 common agents, including fragrances, preservatives, metals, rubber compounds, and adhesives. The patch test should be performed by an individual who is familiar with the technique. In this test, chemicals are applied to a patch that is then taped to the patient’s back. The patient returns after 48 hours to have the reactions graded. The patch is then reapplied and read after another 48 hours as some reactions may be delayed. However, the agents identified may or may not be the causative agent of the dermatitis, and the T.R.U.E. allergen patch test does not include all the thousands of agents that are potential allergens. Etiology and Pathogenesis Allergic contact dermatitis is an immunologic phenomenon involving cell-mediated or delayed hypersensitivity reactions (type 4 hypersensitivity). In allergic contact dermatitis, the individual must first be sensitized to the antigen. During sensitization, the antigen is engulfed and processed by the www.turner-white.com CLINICAL REVIEW Langerhans’ cell so it can be expressed on the cell’s surface. Through dermal lymphatics, the Langerhans’ cell then migrates to the regional lymph nodes and presents the antigen to T lymphocytes. This interaction is followed by the production of cytokines and the proliferation of T lymphocytes that are specific for the antigen [41]. Repeat antigen challenges will result in the appearance of a rash in 24 to 48 hours after the exposure. However, the signs of allergic contact dermatitis can develop as quickly as 8 to 10 hours and as late as 4 to 7 days following exposure. Common agents in allergic contact dermatitis include poison ivy or oak, nickel, rubber compounds, cosmetics, and medications [42]. If sensitization occurs to one member of an antigen family, cross-reactivity can occur from exposure to other family members. For example, if patients are sensitive to benzocaine, they also must avoid cross-reactive agents such as anesthetics (procaine), hair dyes (p-phenylenediamine), sunscreens (p-aminobenzoic acid), and textile dyes (aniline dye) [43]. Treatment Therapy for contact dermatitis is multidimensional. First and foremost, the patient should be advised to avoid the agent causing the dermatitis. Although this method for preventing the dermatitis may sound simple, complete avoidance may be unacceptable or impossible for the patient to achieve. In this situation, patients should take steps to protect themselves through barriers (ie, gloves). Commercially available compounds such as bentoquatam applied prior to exposure to poison ivy may lessen the occurrence of contact dermatitis. Mild dermatitis can be treated with topical steroids, and antihistamines (ie, hydroxyzine, diphenhydramine, loratadine, or cetirizine) are key for decreasing the associated pruritus. Patients with severe generalized contact dermatitis may benefit from an intramuscular triamcinolone injection or a prednisone taper. Wet compresses with aluminum acetate may be beneficial in the case of weeping and itching skin. In addition, oatmeal baths are useful for moisturizing the itchy, dry skin. Case 4—Actinic Keratosis A 78-year-old male presents for evaluation of areas of flaky, red areas on his forehead. He is a farmer and has spent decades in the bright southern sun without using any protective clothing or sunscreen. Examination of the patient reveals an elderly white man with multiple erythematous, scaly plaques on his forehead and cheeks. This patient has actinic (solar) keratoses. These lesions are reddish brown, rough, scaly papules and plaques with associated telangiectasias that appear in sun-exposed body regions (Figure 5). They are most common in older, fairskinned individuals. There is an increased risk for the develwww.turner-white.com opment of actinic keratoses in patients who are immunosuppressed [44]. Patients with certain genetic abnormalities, such as albinism, Bloom syndrome, xeroderma pigmentosum, and Cockayne’s syndrome are predisposed to developing actinic keratosis. The major clinical significance of actinic keratoses is that over time they may develop into squamous cell cancer. Differential Diagnosis A number of conditions can be mistaken for actinic keratoses. The most important diagnoses not to miss include squamous cell carcinoma and superficial basal cell carcinoma. If the diagnosis is uncertain based on clinical examination alone, a biopsy should be performed. Typically, skin cancers are more firm than actinic keratoses. Squamous cell carcinomas (SCCs) are often friable and bleed with slight trauma and, unlike the usually asymptomatic actinic keratoses, SCCs may be painful or itch. Basal cell carcinomas (BCCs) may present in several different forms, but the most common type is a pearly, translucent papule with telangiectasias. BCCs are also more likely to ulcerate and bleed than actinic keratoses. Seborrheic keratoses, which also are more common in older populations, are benign growths that must be distinguished from actinic keratoses. Erythema typically surrounds the base of actinic keratoses but not seborrheic keratoses. In addition, the hyperkeratosis of seborrheic keratoses is smooth and sometimes soft, unlike the hard, irregular hyperkeratosis of actinic keratoses. Verruca vulgaris also should be considered in the differential diagnosis of actinic keratoses. Etiology and Pathogenesis The chief risk factor for the development of actinic keratosis is ultraviolet (UV) B radiation. UVA radiation alone (and in combination with psoralen, radiographs, and radioactive isotypes) also is associated with their appearance. Due to chronic UV exposure, some patients may have a persistently red face (chronic actinic damage) and not necessarily the presence of actinic keratoses. In actinic keratoses, the UV radiation induces thymidine dimer formation, resulting in mutations in replicating DNA [45]. Mutations of the telomerase gene and tumor suppressor gene p53 are seen in actinic keratosis. Telomerase is involved in indicating the number of divisions a cell can undergo. When this gene is mutated, the cell and its descendants become immortal. The tumor suppressor gene p53 is important in cell-directed death of damaged cells. Without the product of this gene, severely damaged cells continue to proliferate. Ultimately, these mutations lead to neoplastic transformation of the skin cells. Studies estimate that the risk of developing squamous cell cancer from any given actinic keratosis is between 0.075% and 0.096% per year [46]. Although the presence of a single lesion may not result in a significant risk of cancer, patients with Vol. 11, No. 1 January 2004 JCOM 43 THE RED FACE years of photodamage usually present with numerous actinic keratoses. Accordingly, squamous cell cancer would be projected to develop at a rate of 10.2% in 20 years in an individual with the average number 7.7 actinic keratoses [47]. HIV-positive patients (83% in AIDS patients) develop seborrheic dermatitis (as opposed to 1% to 3% of immunocompetent adults), and the severity of disease is correlated with declining T cell immunity [53,54]. Treatment Actinic keratoses are commonly treated with cryosurgery using liquid nitrogen. The freezing that results from liquid nitrogen therapy results in the sloughing of the photodamaged cells of the epidermis. Cryosurgery is performed in the office without anesthetic and results in moderate posttreatment swelling, discomfort, and blistering. Patients with multiple actinic keratoses may benefit from therapy with topical agents such as fluorouracil and imiquimod. These topical agents must be applied daily for a period of 2 to 4 weeks and may result in significant erythema, scaling, and inflammation. Fluorouracil is available as 5%, 1%, and 0.5% fluorouracil cream formulations. Imiquimod is an immuneresponse modifier that up-regulates interferon production. Imiquimod has been approved for the treatment of genital warts, and recent studies have shown it to be safe and effective for the treatment of actinic keratoses [48–50]. Differential Diagnosis Seborrheic dermatitis can be confused with other skin diseases such as atopic dermatitis, fungal infection, rosacea, or psoriasis. If a questionable case of seborrheic dermatitis fails to respond to standard topical therapy, another disease entity may be present. Patients with seborrhea often have additional skin diseases such as acne and rosacea. It may be prudent to refer these individuals to a dermatologist for evaluation and possible oral isotretinoin therapy. Case 5—Seborrheic Dermatitis A 20-year-old man presents with complaints of itching and redness under his beard for many years. He also has dandruff and an itchy scalp that improves mildly with use of zinc pyrithione shampoo. Physical examination reveals a young man with yellow scales overlying a greasy erythematous scalp. There also is erythema with mild scaling in his beard. The occurrence of greasy, red skin with overlying yellow-red scale should suggest seborrheic dermatitis (Figure 6). Seborrheic dermatitis is distributed in areas of active sebaceous glands; the scalp (dandruff), eyebrows, beard, forehead, nasolabial fold, glabella, retroauricular region, concha of ear and ear canal, axilla, groin, sternum, submammary areas, and umbilicus are commonly involved. Seborrheic dermatitis may be first encountered in the infant as “cradle cap” that usually remits after the first few months of infancy. It reappears in adolescence with the onset of puberty and is common throughout young adulthood. Seborrheic dermatitis is rare among middle-age individuals but becomes common again in later life. In adults, seborrheic dermatitis is a chronic condition cycling between exacerbations and remissions. The winter climate tends to worsen the disease. The effect of sunlight on seborrheic dermatitis is controversial. One study suggests a beneficial effect of sun exposure [51], while another reports that psoralen plus UVA light (PUVA) therapy induces seborrheic dermatitis [52]. Up to 42% of 44 JCOM January 2004 Vol. 11, No. 1 Etiology and Pathogenesis Malassezia yeasts are normal skin colonizers that are thought to play a role in the development of seborrheic dermatitis. The Malassezia yeasts appear on the skin with the onset of puberty, thriving on the concurrent increase in lipid material. Yeast lipase activity results in the production of arachidonic acid, a potent inflammatory mediator produced by P. acnes in the pathogenesis of acne [55]. These theories about the fungal role in seborrheic dermatitis are supported by studies reporting the successful treatment of the disease with azole drugs [56–59]. Treatment Topical agents are the first-line treatment of seborrheic dermatitis. In adults, scalp seborrhea may be treated with overthe-counter shampoos containing selenium sulfide and zinc. Sulfur forms hydrogen sulfide when it interacts with keratinocytes, producing a keratolytic effect that reduces dandruff [60]. Zinc pyrithione has keratolytic as well as antifungal activity [61]. Topical coal tar, propylene glycol, terbinafine, and lithium succinate also have been shown to successfully treat seborrheic dermatitis [62–67]. Corticosteroids also are beneficial, but chronic use is limited because of the possibility of skin atrophy. Topical azoles (ketoconazole, bifonazole, miconazole) are available in numerous formulations for the treatment of seborrheic dermatitis. Other successful topical medications include sodium sulfacetamide, ciclopirox, tacrolimus, and pimecrolimus [68–71]. If seborrheic dermatitis cannot be controlled with topical agents, oral medications can be used. Agents such as oral ketoconazole (200 mg daily for 4 weeks), itraconazole (200 mg daily for 7 days), and terbinafine (250 mg daily for 4 weeks) have been used in the treatment of widespread seborrheic dermatitis [72–74]. Oral isotretinoin is useful in the treatment of seborrhea as it reduces the production of sebum and has anti-inflammatory properties [75]. www.turner-white.com CLINICAL REVIEW Case 6—Atopic Dermatitis A 5-month-old infant is brought to the pediatric office for an itchy red face for the past month. Upon examination, the infant has erythematous cheeks with oozing and crusting. Additionally, there is mild erythema in the diaper area. Atopic dermatitis (eczema) is a disease marked by severe pruritus and is largely a disease of infants and children. It affects at least 10% of children at some point within their childhood [76]. Although most children will outgrow this disease by adulthood, some will suffer from it throughout their life. In infantile atopic dermatitis, the head, diaper area, and extensor surfaces exhibit a papulovesicular rash with oozing and crusting. Chronically, the itch–scratch cycle results in lichenified, scaling skin. Adults and children often have this lichenified skin on the face, neck, upper chest, hands, and antecubital and popliteal fossa (Figure 7). The infraorbital areas are often dark and have increased skin folds (Dennie-Morgan lines). Chronic rubbing of the eyes may result in loss of hair in the lateral third of the eyebrow. Perifollicular hyperkeratosis on the extensor surfaces of the extremities (keratosis pilaris) and fish-scale–like hyperkeratosis of the arms and shins (ichthyosis vulgaris) are associated findings in patients with atopic dermatitis, especially in patients with dark skin. The criteria for diagnosis of atopic dermatitis are outlined in the Table. Differential Diagnosis Although the diagnosis of atopic dermatitis in children may seem relatively straightforward, it is important to consider other disease entities that may present with similar examination findings and are found in children with recurrent illnesses, developmental abnormalities, or organomegaly [77]. Young males with recurrent infections, thrombocytopenia manifested by bleeding tendencies, and eczema should be evaluated for Wiskott-Aldrich syndrome. Another presentation of atopic dermatitis is in Netherton syndrome, a severe autosomal recessive skin disorder characterized by congenital erythroderma, hair-shaft abnormalities, and high levels of immunoglobulin (Ig) E. Differential diagnoses for atopic dermatitis are many, including contact dermatitis, seborrheic dermatitis, psoriasis, scabies, and drug reactions. It is important to consider the complete clinical picture when treating the patient. Etiology and Pathogenesis Atopic dermatitis is part of a family of diseases that also includes allergic rhinitis, xerosis, and asthma. This constellation of disease is referred to as “atopy.” Individuals may suffer from one or more atopic diseases, and they often have family members who have atopic dermatitis, asthma, or www.turner-white.com Table. Criteria for Diagnosis of Atopic Dermatitis Major features (must have 3 or more) Pruritus Typical morphology and distribution Flexural lichenification in adults Facial and extensor involvement in infants and children Dermatitis (chronically or chronically relapsing) Personal or family history of atopy (asthma, allergic rhinitis, atopic dermatitis) Minor features (must have 3 or more) Cataracts (anterior-subcapsular) Cheilitis Conjunctivitis (recurrent) Eczema (perifollicular accentuation) Facial pallor/facial erythema Food intolerance Hand dermatitis (nonallergic, irritant) Ichthyosis Elevated immunoglobulin E Immediate (type 1) skin test reactivity Cutaneous infections (Staphylococcus aureus, herpes simplex) Infraorbital fold (Dennie-Morgan lines) Itching when sweating Keratoconus Keratosis pilaris Nipple dermatitis Orbital darkening Palmar hyperlinearity Pityriasis alba White dermographism Wool intolerance Xerosis Note: 3 or more major features plus 3 or more minor features must be present to make a diagnosis of atopic dermatitis. Data from Hanifin JM, Lobitz WC Jr. Newer concepts of atopic dermatitis. Arch Dermatol 1977;113:663–70; and Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol (Stockh) 1980;92(Suppl):44–47. allergic rhinitis, which supports a strong genetic component of atopy. In a study of siblings with atopic dermatitis, 69% had at least one parent with atopic dermatitis [78]. Twinbased concordance studies have provided further data to support a genetic linkage theory of atopy [79]. Multiple gene loci have been identified as sites of polymorphisms linked to atopic disease [80,81]. Environmental factors also are thought to be critical in the expression of atopic dermatitis. The house dust mite (Dermatophagoides farinae) has been associated [82,83]. Numerous studies have examined the lifetime prevalence of atopic Vol. 11, No. 1 January 2004 JCOM 45 THE RED FACE dermatitis, with actual percentages varying greatly between geographic locations sampled and the time period during which surveys were conducted [84]. It appears from these studies that developed countries have a higher incidence of atopy than their more rural neighbors. The “hygiene hypothesis” has been developed to explain the greater incidence of atopic dermatitis in higher socioeconomic classes and industrialized countries [85]. This theory suggests that the unhygienic atmosphere (early infections, larger households) in rural environments provides early exposure to allergens that protects the individual from developing atopy. Early exposure to pets (within the first 2 years of life) seems to be protective against developing atopic dermatitis, although one study found a greater incidence in those with guinea pigs [86,87]. While the complex interaction between genetics and environment is certainly at the root of atopic dermatitis, the causal effects of environmental factors are not yet completely understood. Atopic dermatitis appears to result from immune dysregulation, neural dysfunction, and a defective skin barrier. Atopic dermatitis is associated with elevated T-lymphocyte activation, hyperstimulatory Langerhans’ cells, abnormal cell-mediated immunity, and overproduction of IgE [88]. Patients with atopic dermatitis have been shown to have alterations in the levels and distribution of neuropeptides. This abnormality is thought to contribute to the hallmark of atopic dermatitis: itch [89,90]. Patients with atopic dermatitis also have elevated sphingomyelin deacylase, resulting in lower ceramide levels and a reduction in hydration of the skin and its barrier function [91]. The weakened epidermal layer is then more vulnerable to irritants and allergens. Together, defective immunity and a weak epidermal barrier in atopic dermatitis often result in superinfection with pathogens such as Staphylococcus aureus. Superinfection with the herpes virus may result in eczema herpeticum marked by fever, malaise, and painful, disseminated, erosive lesions. Treatment Treatment of atopic dermatitis is similar to that of contact dermatitis. Foremost in therapy of atopic dermatitis is the limitation of exposure to the exacerbating factor. These factors include excessive bathing, dry environments, harsh detergents, and emotional stress. Often, patients with atopic dermatitis and coexisting allergic hypersensitivity will show improvement in their dermatitis with elimination of the offending antigens. This may include thorough housecleaning to eliminate dust and mites or avoiding certain foods. Antihistamines are useful in combating the itch of atopic dermatitis. The tricyclic antidepressant doxepin is a potent H1 blocker and also is useful in alleviating itch; however, it should be used with caution as toxic doses can cause fatal heart arrhythmias. In order to combat the dryness that 46 JCOM January 2004 Vol. 11, No. 1 amplifies the itch, patients should cleanse with moisturizing soaps and oatmeal baths. Ointments and thick creams should be applied after bathing to lock in moisture. Topical corticosteroids are the traditional therapy of atopic dermatitis. For mild dermatitis, low-potency topical corticosteroids such as 1% hydrocortisone are useful. In more severe disease, it may be necessary to use mediumpotency corticosteroids (eg, triamcinolone 0.1%). In acute flares, high-potency steroids can be used for a short time but should not be used on the face. In the most severe flares, a brief, systemic prednisone taper may rarely be indicated along with the institution of aggressive topical therapy. However, it is best to avoid systemic steroids if possible as many patients flare and develop more severe dermatitis [92]. Many patients with severe dermatitis may be secondarily infected by S. aureus. A short course of antistaphylococcal antibiotic (cephalexin) may be indicated if infection is suspected or if patients are proven nasal carriers of S. aureus. The patient with severe atopic dermatitis unresponsive to conventional medications may be referred to a dermatologist for treatment with other drugs or UV light therapy. PUVA therapy and UVA/UVB phototherapy have been used for treating severe atopic dermatitis. Topical or oral cyclosporine is an effective therapy for severe atopic dermatitis [93,94]. Oral cyclosporine is limited by the need to measure blood pressure and serum creatinine every 2 weeks for 3 months and then monthly. Topical tacrolimus is an effective and safe alternative to corticosteroids for the treatment of atopic dermatitis in both children and adults [95–97]. Tacrolimus is an immunomodulator whose advantage over corticosteroids is that it does not cause skin atrophy, a useful property in the treatment of facial dermatitis. Initially, the patient may experience some burning, stinging, or erythema with the application of tacrolimus; however, these adverse effects resolve over time. Topical tacrolimus is prepared in 0.1% and 0.03% concentrations. Pimecrolimus, available as 1% cream, is an alternative immunomodulator approved by the FDA for atopic dermatitis. Less Common Red Face Diagnoses Tinea faciei, although not very common and often misdiagnosed, presents as an easily treatable cause of red face. The lesions are scaly, erythematous, annular plaques that may have pustules along the border (Figure 8). Fungal culture or potassium hydroxide examination confirms the diagnosis, and topical antifungals yield successful results. Ulerythema ophryogenes (keratoses pilaris atrophicans faciei) is a chronic condition that manifests shortly after birth and is characterized by follicular papules with surrounding erythematous halos (Figure 9). Initially, the disorder targets the lateral aspects of the eyebrows, but progression to the cheeks and forehead is not uncommon. Gradual loss of the www.turner-white.com CLINICAL REVIEW eyebrow hair is seen, which may eventually involve the entire eyebrow. Keratosis pilaris of the extensor aspects of the arms is often seen, and an association with atopic dermatitis has been reported [98]. In addition, several congenital abnormalities (ie, Noonan’s syndrome and Cornelia de Lange’s syndrome, Rubinstein—Taybi syndrome) have been linked [99–102]. The systemic diseases lupus erythematosus and dermatomyositis can present with a red face. Dermatomyositis classically presents on the face with periorbital confluent, macular, violaceous (heliotrope) erythema, although a more generalized “red face” may be seen (Figure 10). Other hallmark cutaneous features include violaceous papules (Gottron’s papules) and symmetric confluent macular violaceous erythema (Gottron’s sign) overlying the interphalangeal and/or metacarpophalangeal joints, symmetric confluent macular violaceous erythema overlying the dorsal aspect of the fingers up to the arms and neck (shawl sign) and anterior neck and upper chest (V sign), periungual telangiectasias, and bilaterally symmetric confluent hyperkeratosis along the ulnar aspect of the thumb and radial aspect of the fingers (mechanic’s hand lesion) [103]. Although skin disease is usually the first sign of dermatomyositis, muscle weakness (proximal myositis) soon follows, and other organ systems (ie, cardiac, pulmonary, gastrointestinal) also may be involved. Lupus erythematosus–specific skin disease can be divided into acute cutaneous lupus erythematosus (ACLE), subacute cutaneous lupus erythematosus (SCLE), and chronic cutaneous lupus erythematosus (CCLE). ACLE typically presents with confluent, symmetric, erythema over the malar eminences and bridge of the nose, sparing the nasolabial folds (butterfly rash) (Figure 11a). Erythematous macules and/or papules that evolve into hyperkeratotic papulosquamous or annular/polycyclic plaques, predominantly in sunexposed areas, generally occur with SCLE (Figure 11b). The typical presentation in CCLE includes sharply demarcated, coin-shaped (discoid) erythematous plaques with prominent, adherent scale and central atrophy primarily affecting the face, scalp, ears, V area of the neck, and extensor aspects of the arms (Figure 11c) [104]. The risk of systemic lupus erythematosus is greatest with ACLE (72%) and least with CCLE (14%) [105]. Systemic manifestations may involve renal, cardiac, pulmonary, neurologic, hematologic, immunologic, and musculoskeletal systems. In either of these systemic disorders involving the skin, the role of a dermatologist is beneficial and referral should be made promptly once the diagnosis is suspected. Corresponding author: Steven R. Feldman, MD, PhD, Professor, Departments of Dermatology and Pathology, Wake Forest University School of Medicine, Medical Center Blvd., Winston-Salem, NC 27157, sfeldman@wfubmc.edu. www.turner-white.com Financial disclosures: None. Author contributions: conception and design, KAC, SRF; drafting of the article, SB, LR; critical revision of the article for important intellectual content, KAC, GFG, SRF; collection and assembly of data, SB, LR, KAC. References 1. Lowell BA, Froelich CW, Federman DG, Kirsner RS. Dermatology in primary care: Prevalence and patient disposition. J Am Acad Dermatol 2001;45:250–5. 2. Kraning K, Odland G. Prevalence, morbidity, and cost of dermatologic diseases. J Invest Dermatol 1979;73(5 Pt 2): 395–401. 3. Pochi PE, Shalita AR, Strauss JS, et al. Report of the Consensus Conference on Acne Classification. Washington, DC, March 24 and 25, 1990. J Am Acad Dermatol 1991;24:495–500. 4. Voorhees JJ, Hayes E, Wilkins J, Harrell ER. The XYY chromosomal complement and nodulocystic acne. Ann Intern Med 1970;73:271–6. 5. Herane MI, Ando I. Acne in infancy and acne genetics. Dermatology 2003;206:24–8. 6. Vowels BR, Yang S, Leyden JJ. Induction of proinflammatory cytokines by a soluble factor of Propionibacterium acnes: implications for chronic inflammatory acne. Infect Immun 1995;63:3158–65. 7. Jain A, Sangal L, Basal E, et al. Anti-inflammatory effects of erythromycin and tetracycline on Propionibacterium acnes induced production of chemotactic factors and reactive oxygen species by human neutrophils. Dermatol Online J 2002;8:2. 8. Mills OH Jr, Kligman A. Acne mechanica. Arch Dermatol 1975;111:481–3. 9 Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol 2003;49(1 Suppl):S1–37. 10. Leyden JJ, Marples RR, Mills OH, Kligman AM. Tretinoin and antibiotic therapy in acne vulgaris. South Med J 1974;67:20–5. 11. Shalita AR, Chalker DK, Griffith RF, et al. Tazarotene gel is safe and effective in the treatment of acne vulgaris: a multicenter, double-blind, vehicle-controlled study. Cutis 1999;63:349–54. 12. Shalita A, Weiss JS, Chalker DK, et al. A comparison of the efficacy and safety of adapalene gel 0.1% and tretinoin gel 0.025% in the treatment of acne vulgaris: a multicenter trial. J Am Acad Dermatol 1996;34:482–5. 13. Usatine RP, Quan MA. Pearls in the management of acne: an advanced approach. Prim Care 2000;27:289–308. 14. Cunliffe WJ, Holland KT. Clinical and laboratory studies on treatment with 20% azelaic acid cream for acne. Acta Derm Venereol Suppl (Stockh) 1989;143:31–4. 15. Cooper AJ. Systematic review of Propionibacterium acnes resistance to systemic antibiotics. Med J Aust 1998;169:259–61. 16. Gough A, Chapman S, Wagstaff K, Emery P, Elias E. Minocycline induced autoimmune hepatitis and systemic lupus erythematosus-like syndrome. BMJ 1996;312:169–72. 17. Sturkenboom MC, Meier CR, Jick H, Stricker BH. Minocycline and lupuslike syndrome in acne patients. Arch Intern Med 1999;159:493–7. Vol. 11, No. 1 January 2004 JCOM 47 THE RED FACE 18. Zouboulis CC, Piquero-Martin J. Update and future of systemic acne treatment. Dermatology 2003;206:37–53. 19. Lammer EJ, Chen DT, Hoar RM, et al. Retinoic acid embryopathy. N Engl J Med 1985;313:837–41. 20. Knitzer RH, Needleman BW. Musculoskeletal syndromes associated with acne. Semin Arthritis Rheum 1991;20:247–55. 21. Wysowski DK, Pitts M, Beitz J. An analysis of reports of depression and suicide in patients treated with isotretinoin. J Am Acad Dermatol 2001;45:515–9. 22. Jacobs DG, Deutsch NL, Brewer M. Suicide, depression, and isotretinoin: is there a causal link? J Am Acad Dermatol 2001;45:S168–75. 23. Margolis CF, Ramundo ML. Acne management. Primary care physician or dermatologist? Postgrad Med 1987;82:139–46. 24. Hill VA, Wong E, Hart CJ. General practitioner referral guidelines for dermatology: do they improve the quality of referrals? Clin Exp Dermatol 2000;25:371–6. 25. Landow K. Unraveling the mystery of rosacea. Keys to getting the red out. Postgrad Med 2002;112:51–8, 82. 26. Del Rosso JQ. A status report on the medical management of rosacea: focus on topical therapies. Cutis 2002;70:271–5. 27. Ferri’s clinical advisor: instant diagnosis and treatment. St. Louis: Mosby; 2003. 28. Quarterman MJ, Johnson DW, Abele DC, et al. Ocular rosacea. Signs, symptoms, and tear studies before and after treatment with doxycycline. Arch Dermatol 1997;133:49–54. 29. Akpek EK, Merchant A, Pinar V, Foster CS. Ocular rosacea: patient characteristics and follow-up. Ophthalmology 1997; 104:1863–7. 30. Rebora A, Drago F, Parodi A. May Helicobacter pylori be important for dermatologists? Dermatology 1995;191:6–8. 31. Georgala S, Katoulis AC, Kylafis GD, et al. Increased density of Demodex folliculorum and evidence of delayed hypersensitivity reaction in subjects with papulopustular rosacea. J Eur Acad Dermatol Venereol 2001;15:441–4. 32. Bonnar E, Eustace P, Powell FC. The Demodex mite population in rosacea. J Am Acad Dermatol 1993;28:443–8. 33. Brinnel H, Friedel J, Caputa M, et al. Rosacea: disturbed defense against brain overheating. Arch Dermatol Res 1989; 281:66–72. 34. Blount BW, Pelletier AL. Rosacea: a common, yet commonly overlooked, condition. Am Fam Physician 2002;66:435–40. 35. Bleicher PA, Charles JH, Sober AJ. Topical metronidazole therapy for rosacea. Arch Dermatol 1987;123:609–14. 36. Jorizzo JL, Lebwohl M, Tobey RE. The efficacy of metronidazole 1% cream once daily compared with metronidazole 1% cream twice daily and their vehicles in rosacea: a doubleblind clinical trial. J Am Acad Dermatol 1998;39:502–4. 37. Maddin S. A comparison of topical azelaic acid 20% cream and topical metronidazole 0.75% cream in the treatment of patients with papulopustular rosacea. J Am Acad Dermatol 1999;40(6 Pt 1):961–5. 38. Katsambas AD, Nicolaidou E. Acne, perioral dermatitis, flushing, and rosacea: unapproved treatments or indications. Clin Dermatol 2000;18:171–6. 39. Landow K. Unraveling the mystery of rosacea. Keys to getting the red out. Postgrad Med 2002;112:51–8. 48 JCOM January 2004 Vol. 11, No. 1 40. Cherry N, Meyer JD, Adisesh A, et al. Surveillance of occupational skin disease: EPIDERM and OPRA. Br J Dermatol 2000;142:1128–34. 41. Belsito DV. Mechanisms of allergic contact dermatitis. Immunol Allergy Clin N Am 1989;9:579–95. 42. Lookingbill DP, Marks JG Jr. Principles of dermatology. 3rd ed. Philadelphia: WB Saunders Co; 2000:152–6. 43. Belsito DV. The diagnostic evaluation, treatment, and prevention of allergic contact dermatitis in the new millennium. J Allergy Clin Immunol 2000;105:409–20. 44. Price ML, Tidman MJ, Fagg NL, et al. Distinctive epidermal atypia in immunosuppression-associated cutaneous malignancy. Histopathology 1988;13:89–94. 45. Cockerell CJ. Pathology and pathobiology of the actinic (solar) keratosis. Br J Dermatol 2003;149 (Suppl):S34–6. 46. Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet 1988; 243:795–7. 47. Dodson JM, DeSpain J, Hewitt JE, Clark DP. Malignant transformation of actinic keratoses and the controversy over treatment. A patient-oriented perspective. Arch Dermatol 1991;127:1029–31. 48. Persaud AN, Shamuelova E, Sherer D, et al. Clinical effect of imiquimod 5% cream in the treatment of actinic keratosis. J Am Acad Dermatol 2002;47:553–6. 49. Salasche SJ, Levine N, Morrison L. Cycle therapy of actinic keratoses of the face and scalp with 5% topical imiquimod cream: An open-label trial. J Am Acad Dermatol 2002;47:571–7. 50. Stockfleth E, Meyer T, Benninghoff B, et al. A randomized, double-blind, vehicle-controlled study to assess 5% imiquimod cream for the treatment of multiple actinic keratoses. Arch Dermatol 2002;138:1498–502. 51. Berg M. Epidemiological studies of the influence of sunlight on the skin. Photodermatol 1989;6:80–4. 52. Tegner E. Seborrhoeic dermatitis of the face induced by PUVA treatment. Acta Derm Venereol 1983;63:335–9. 53. Mathes BM, Douglass MC. Seborrheic dermatitis in patients with acquired immunodeficiency syndrome. J Am Acad Dermatol 1985;13:947–51. 54. Garman ME, Tyring SK. The cutaneous manifestations of HIV infection. Dermatol Clin 2002;20:193–208. 55. Greaves MW, Camp RD. Prostaglandins, leukotrienes, phospholipase, platelet activating factor, and cytokines: an integrated approach to inflammation of human skin. Arch Dermatol Res 1988;280 (Suppl):S33–41. 56. Faergemann J. Seborrhoeic dermatitis and Pityrosporum orbiculare: treatment of seborrhoeic dermatitis of the scalp with miconazole-hydrocortisone (Daktacort), miconazole and hydrocortisone. Br J Dermatol 1986;114:695–700. 57. Segal R, David M, Ingber A, et al. Treatment with bifonazole shampoo for seborrhea and seborrheic dermatitis: a randomized, double-blind study. Acta Derm Venereol 1992;72:454–5. 58. Carr MM, Pryce DM, Ive FA. Treatment of seborrhoeic dermatitis with ketoconazole: I. Response of seborrhoeic dermatitis of the scalp to topical ketoconazole. Br J Dermatol 1987;116:213–6. 59. Shiri J, Amachai B. Treatment of seborrheic dermatitis of the www.turner-white.com CLINICAL REVIEW 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. scalp and dandruff with a shampoo containing 1% bifonazole (Agispor shampoo). J Dermatol Treatment 1998;9:95–6. Lin AN, Reimer RJ, Carter DM. Sulfur revisited. J Am Acad Dermatol 1988;18:553–8. Gupta AK, Bluhm R, Cooper EA, et al. Seborrheic dermatitis. Dermatol Clin 2003;21:401–12. Garcia RL, Miller JD, Miller WN. Occlusive tar extract therapy for recalcitrant psoriasis and seborrheic dermatitis of the scalp. Cutis 1978;22:90–1. Olansky S. Whole coal tar shampoo: a therapeutic hair repair system. Cutis 1980;25:99–104. Cuelenaere C, De Bersaques J, Kint A. Use of topical lithium succinate in the treatment of seborrhoeic dermatitis. Dermatology 1992;184:194–7. Boyle J, Burton JL, Faergemann J. Use of topical lithium succinate for seborrhoeic dermatitis. Br Med J (Clin Res Ed) 1986;292:28. Faergemann J. Propylene glycol in the treatment of seborrheic dermatitis of the scalp: a double-blind study. Cutis 1988;42:69–71. A double-blind, placebo-controlled, multicenter trial of lithium succinate ointment in the treatment of seborrheic dermatitis. Efalith Multicenter Trial Group. J Am Acad Dermatol 1992;26:452–7. Dupuy P, Maurette C, Amoric JC, Chosidow O. Randomized, placebo-controlled, double-blind study on clinical efficacy of ciclopiroxolamine 1% cream in facial seborrhoeic dermatitis. Br J Dermatol 2001;144:1033–7. Ling MR. Topical tacrolimus and pimecrolimus: future directions. Semin Cutan Med Surg 2001;20:268–74. Vardy D, Zvulunov A, Tchetov T, et al. Adouble blind, placebocontrolled trial of ciclopiroxolamine 1% shampoo for treatment of scalp seborrheic dermatitis. J Dermatol Treatment 2000;11: 73–7. Johnson BA, Nunley JR. Treatment of seborrheic dermatitis. Am Fam Physician 2000;61:2703–4. Ford GP, Farr PM, Ive FA, Shuster S. The response of seborrhoeic dermatitis to ketoconazole. Br J Dermatol 1984;111: 603–7. Scaparro E, Quadri G, Virno G, et al. Evaluation of the efficacy and tolerability of oral terbinafine (Daskil) in patients with seborrhoeic dermatitis. A multicentre, randomized, investigator-blinded, placebo-controlled trial. Br J Dermatol 2001;144:854–7. Caputo R, Barbareschi M. Itraconazole: new horizons. G Ital Dermatol Venereol 2002;137:1–7. Orfanos CE, Zouboulis CC. Oral retinoids in the treatment of seborrhoea and acne. Dermatology 1998;196:140–7. Leung DY. Atopic dermatitis: new insights and opportunities for therapeutic intervention. J Allergy Clin Immunol 2000;105:860–76. Fleischer AB Jr, Feldman S, editors. 20 common problems in dermatology. New York: McGraw Hill, Health Professions Division; 2000. Bradley M, Kockum I, Soderhall C, et al. Characterization by phenotype of families with atopic dermatitis. Acta Derm Venereol 2000;80:106–10. www.turner-white.com 79. Kang K, Stevens SR. Pathophysiology of atopic dermatitis. Clin Dermatol 2003;21:116–21. 80. Lee YA, Wahn U, Kehrt R, et al. A major susceptibility locus for atopic dermatitis maps to chromosome 3q21. Nat Genet 2000;26:470–3. 81. Bradley M, Soderhall C, Luthman H, et al. Susceptibility loci for atopic dermatitis on chromosomes 3, 13, 15, 17 and 18 in a Swedish population. Hum Mol Genet 2002;11:1539–48. 82. Matsuoka H, Maki N, Yoshida S, et al. A mouse model of the atopic eczema/dermatitis syndrome by repeated application of a crude extract of house-dust mite Dermatophagoides farinae. Allergy 2003;58:139–45. 83. Pajno GB, Peroni DG, Barberio G, Pietrobelli A, Boner AL. Predictive features for persistence of atopic dermatitis in children. Pediatr Allergy Immunol 2003;14:292–5. 84. Worldwide variations in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet 1998;351:1225–32. 85. Strachan DP. Hay fever, hygiene, and household size. BMJ 1989;299:1259–60. 86. Zirngibl A, Franke K, Gehring U, et al. Exposure to pets and atopic dermatitis during the first two years of life. A cohort study. Pediatr Allergy Immunol 2002;13:394–401. 87. Schafer T, Heinrich J, Wjst M, et al. Indoor risk factors for atopic eczema in school children from East Germany. Environ Res 1999;81:151–8. 88. Cooper KD. Atopic dermatitis: recent trends in pathogenesis and therapy. J Invest Dermatol 1994;102:128–37. 89. Giannetti A. Neuropeptides in atopic dermatitis. Curr Probl Dermatol 1999;28:51–5. 90. Scholzen T, Armstrong CA, Bunnett NW, et al. Neuropeptides in the skin: interactions between the neuroendocrine and the skin immune systems. Exp Dermatol 1998;7:81–96. 91. Hara J, Higuchi K, Okamoto R, et al. High expression of sphingomylenin deacylase is an important determinant of ceramide deficiency leading to barrier disruption in atopic dermatitis. J Invest Dermatol 2000;115:406–13. 92. David TJ. Recent developments in the treatment of childhood atopic eczema. J R Coll Physicians Lond 1991;25:95–101. 93. de Prost Y, Bodemer C, Teillac D. Double-blind randomization placebo-controlled trial of local cyclosporine in atopic dermatitis. Arch Dermatol 1989;125:570. 94. van Joost T, Stolz E, Heule F. Efficacy of low-dose cyclosporine in severe atopic skin disease. Arch Dermatol 1987; 123:166–7. 95. Ruzicka T, Bieber T, Schopf E, et al. A short-term trial of tacrolimus ointment for atopic dermatitis. European Tacrolimus Multicenter Atopic Dermatitis Study Group. N Engl J Med 1997;337:816–21. 96. Reitamo S, Van Leent EJ, Ho V, et al. Efficacy and safety of tacrolimus ointment compared with that of hydrocortisone acetate ointment in children with atopic dermatitis. J Allergy Clin Immunol 2002;109:539–46. 97. Reitamo S, Rustin M, Ruzicka T, et al. Efficacy and safety of tacrolimus ointment compared with that of hydrocortisone butyrate ointment in adult patients with atopic dermatitis. Vol. 11, No. 1 January 2004 JCOM 49 THE RED FACE J Allergy Clin Immunol 2002;109:547–55. 98. Mertens RL. Ulerythema ophryogenes and atopy. Arch Dermatol 1968;97:662–3. 99. Snell JA, Mallory SB. Ulerythema ophryogenes in Noonan syndrome. Pediatr Dermatol 1990;7:77–8. 100. Pierini DO, Pierini AM. Keratosis pilaris atrophicans faciei (ulerythema ophryogenes): a cutaneous marker in the Noonan syndrome. Br J Dermatol 1979;100:409–16. 101. Florez A, Fernandez-Redondo V, Toribio J. Ulerythema ophryogenes in Cornelia de Lange syndrome. Pediatr Dermatol 2002;19:42–5. 102. Gomez Centeno P, Roson E, Peteiro C, et al. Rubinstein-Taybi syndrome and ulerythema ophryogenes in a 9-year-old boy. Pediatr Dermatol 1999;16:134–6. 103. Sontheimer RD, Costner M. Dermatomyositis. In: Freedberg IM, Eisen AZ, Wolff K, editors. Fitzpatrick’s dermatology in general medicine. 5th ed. New York: McGraw Hill; 1999. 104. Costner M, Sontheimer R. Lupus erythematosus. In: Freedberg IM, Eisen AZ, Wolff K, editors. Fitzpatrick’s dermatology in general medicine. 5th ed. New York: McGraw Hill; 1999. 105. Watanabe T, Tsuchida T. Classification of lupus erythematosus based upon cutaneous manifestations. Dermatological, systemic and laboratory findings in 191 patients. Dermatology 1995;190:277–83. Copyright 2004 by Turner White Communications Inc., Wayne, PA. All rights reserved. 50 JCOM January 2004 Vol. 11, No. 1 www.turner-white.com









© Copyright 2025