
Document 15810
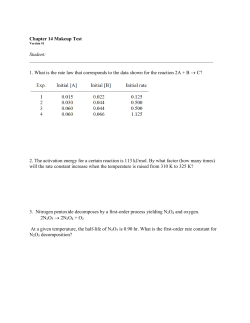
T E R S Accuracy of Blood Glucose Meters in Pregnant Subjects With Diabetes I t is essential for pregnant women with diabetes to maintain a blood glucose level as near to normal as possible to improve perinatal outcome (1,2). Selfmonitoring of capillary blood glucose is an important component of the management of blood glucose (3). However, a report on four glucose meters cast doubts on the accuracy of these devices in pregnant women with diabetes (4). We evaluated the accuracy and precision of the MediSense Precision QID, a new glucose meter based on electrochemical biosensor technology. A total of 50 pregnant subjects with diabetes participated in our study. Their gestational ages ranged from 4 to 38 weeks. Of the subjects, 3,17, and 30 were in their 1st, 2nd, and 3rd trimesters, respectively. A total of 6 subjects had IDDM, 5 had NIDDM, and 39 had gestational diabetes. Analytical accuracy was assessed by comparing capillary blood glucose values between the Precision QID and a laboratory method (the YSI glucose analyzer). Two tests were performed with the Precision QID and the YSI glucose analyzer on each subject. Precision was determined by calculating the mean of all coefficients of variation (CVs) between the duplicate measurements. We found the accuracy of the Precision QID comparable with that of the laboratory method; an error grid analysis (5) of the 100 results is shown in Fig. 1. Of the Precision QID results, 94 and 100% agreed within 15 and 20%, respectively, of the laboratory method values. Linear regression analysis of the data showed the following: correlation coefficient (r) 0.98, slope 1.03, intercept 1.0 mg/dl, Sy.x 8.2 mg/dl. The mean absolute bias was 6.6%. The mean CV of paired replicates was 3.5%, indicating good precision with the Precision QID. It was suggested (4) that lower hematocrit levels and metabolic and physiological changes of pregnancy may interfere with the accuracy of glucose reflectance meters; the levels of free fatty acids, ketones, triglycerides, and cholesterol are increased in blood during pregnancy. Our data established that the Pre- cision QID is accurate and precise for monitoring glycemic control in pregnant subjects with diabetes. The hematocrits of the subjects in this study ranged from 30 to 47%, which is within the operating specifications of the Precision QID. The Precision QID test strip has a unique third electrode specifically for canceling the effects of interferences from drugs and endogenous substances in the blood (6). This additional electrode may contribute to the accuracy of the Precision QID results in pregnant subjects. In addition to accuracy, a glucose meter for pregnant women who need frequent self-monitoring of blood glucose should be easy to use and maintain. The Precision QID meets this expectation. It requires only a small drop of blood (5 /ml) and 20 s for a test, with no test-strip holder or optical window to clean. Besides the small sample-volume requirement, the Precision QID has a unique operating feature that allows the user to apply another drop of blood within 30 s to the same test strip if the first drop does not start the test. Thus, it maximizes accuracy and the success rate of testing and minimizes wastage of test strips due to insufficient specimens. PATRICIA STENGER, RN, CDE MARY ELLEN ALLEN, RN ouu - LISA LISIUS, RN, CDE X 500- 400 - - x E in © a 3 a o § 300- / , / / A/ A / AA y/ A A A / c on a- / ' From the Eastern Maine Medical Center, Diabetes Center, Bangor, Maine. Address correspondence to Patricia Stenger, RN, CDE, Eastern Maine Medical Center, Diabetes Center, 431 State St., Suite 4, Bangor, ME 04401. / A A xX/ / X / / / 'XX /A X X / X / Acknowledgment—This study was supported in part by a grant from MediSense. B References X B /X / /-/ y 200 - .2 AS/ D D 100A / r r / 00 100 By A / 1 200 300 400 YSI Mean Glucose, mg/dL Figure 1—Error grid analysis oj 100 glucose results. 268 E 500 600 1. Karlsson K, Kjellmer I: The outcome of diabetic pregnancies in relation to the mother's blood sugar level. Am] Obstet Gynecol 112:213-220,1972 2. Fuhrmann K, Reiher H, Semmler K, Fischer F, Fischer M, Glochner E: Prevention of congenital malformations in infants in insulin dependent diabetic mothers. Diabetes Care 6:219-222, 1983 3. American Diabetes Association: Consensus statement on self-monitoring of blood glucose. Diabetes Care 18:47-52, 1995 4. Harkness LJ, Ashwood ER, Parsons S, Lenke RR: Comparison of the accuracy of glucose reflectance meters in pregnant in- DIABETES CARE, VOLUME 19, NUMBER 3 , MARCH 1996 Letters sulin-dependcnt diabetics. Obstet Gynecol 77:181-185, 1991 'x Clarke WL, Cox D, Gonder-Frederick LA, Carter W, Pohl SL: Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care 10:622-628, 1987 b. Ng RH, Martin L, Halpin M, Bernstein R, Fischer J, Taylor E, Schroder S: Clinical performance of a new test strip with the MediSense blood glucose sensor. Clin Chem 41 :S181, 1995 Sex Differences in Plasma Glucose Thresholds for Counterregulatory Hormone Release and Hypoglycemia Symptom Perception S ex has recently been identified as a relevant factor in blood glucose (BG) thresholds for cognitive-motor dysfunction in adult IDDM patients (1,2) and counterregulatory hormone secretion in nondiabetic adults (3,4). These studies suggest that males may be more sensitive to low BG, both in terms of counterregulatory hormone secretion and cognitivemotor functioning. We attempted to replicate and extend these findings. We reanalyzed data from a previous insulin infusion study (5-7), comparing the BG thresholds for counterregulatory hormone release and symptom perception in adult IDDM subjects. Of the adults with IDDM, 19 men and 22 women were compared. Men and women did not differ in terms of age (33.2 ± 6.6 vs. 34.5 ± 9.2 years [means ± SD], NS), duration of disease (11.2 ± 10.9 vs. 14.2 ± 11.3 years, NS), daily insulin (.59 vs. .64 U/kg, NS), or HbAi (12.2 ± 3 . 6 vs. 11.3 ±2.3,NS). Intermediate and long-acting insulins were discontinued 48 h before testing, and overnight euglycemia was maintained at —5.6 mmol/1 with a previously described open-loop insulin infusion algorithm (8,9). At 0800, the subjects were connected to the Biostator glucosecontrolled insulin infusion system (Miles, lilkhart, IN) for continuous glucose monitoring and insulin (human regular, Lilly, DIABETES CARK, VOLUME 19, NUMBER 3 , MARCH Indianapolis, IN) infusion at the rate of 40 jLtmol • kg" 1 • h ~ \ The insulin infusion was continued for 120 min. Plasma was sampled every 10 min for the determination of plasma glucose, epinephrine, and glucagon. Plasma glucose was determined with a glucose oxidase method (Beckman glucose analyzer, Fulton, CA). Plasma glucagon was determined by radioimmunoassay (10), and plasma epinephrine concentration was determined by a single-isotope derivative method (11). Immediately before the 10min blood draws, subjects rated (0 = none, 6 = extreme) five autonomic symptoms (trembling, pounding heart, sweaty, cold hands, tense/frustrated) and five neuroglycopenic symptoms (difficulty concentrating, confusion, blurred vision, slurred speech, numb lips). Using the criteria of other published studies, the plasma glucose threshold level was defined as that at which there was an unequivocal sustained increase in circulating epinephrine and glucagon or an increase in symptom ratings above baseline level (3,6). For example, if the plasma epinephrine fluctuated between 10 and 20 pmol/1 and epinephrine rose to 81 pmol/1 at 70 min and to 96 pmol/1 at 80 min and sustained this elevation, the plasma glucose level at 70 min would be identified as the threshold for epinephrine release. This was done by two examiners who were blind to the subject's sex. No plasma glucose thresholds were found for hormones or symptoms for three women and two men, i.e., they did not counterregulate and were therefore not included in the data analysis. Once BG thresholds for each hormone and each symptom cluster were identified for each subject, data were divided according to sex and analyzed with analysis of variance. Relative to the women, the men's plasma glucose levels were significantly higher for plasma epinephrine release (3.2 ± 0.56 vs. 2.8 ± 0.49 mmol/1, P •• • 0.030) and plasma glucagon release (2.9 ± 0.69 vs. 2.5 ± 0.39 mmol/1, P = = 0.04). However, there were no significant differences between the men's and the women's plasma glucose levels for initial perception of either autonomic (2.9 :•: 0.7 vs. 3.0 ± 0.6 mmol/1) or neuroglycopenic symptoms (3.0 ± 0.7 vs. 3.1 :+: 0.8 mmol/1; Fig. 1). These data are the only available data on diabetic patients that confirm previous studies with nondiabetic subjects demonstrating that men with IDDM respond with epinephrine and glucagon at a higher plasma glucose level than do women. This sex difference cannot be explained in terms of differential metabolic control, since we found no difference in HbAj. Also, it cannot be explained by a differential rate of BG fall, since women's BG tended to fall faster (0.07 mmol • T ' • min [ ) than men's (,0.0'5 mmol • I" 1 • min" 1 , NS). Whether differential counterregulatory and cognitive responses are centrally or peripherally mediated is yet to be clarified. The present data do not suggest that sex affects BG thresholds for the perception of either autonomic or neuroglycopenic symptoms. Clinically, this may reflect an inherent danger for men. It is possible that men may experience hypoglycemia counterregulation and cognitive- mM 3.5 •<.O4 3 2.5 2 1.5 1 0.5 0 Epinephrine Glucagon Figure 1—Sex differences in blood glucose thresholds. 1996 Autonom Sx Neuroglycop Sx men; ^ g , women. 269





















© Copyright 2025