
Maternal nutrition: Effects on health in the next generation Review Article
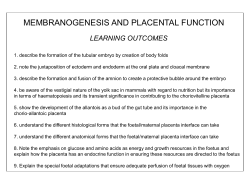
Review Article Indian J Med Res 130, November 2009, pp 593-599 Maternal nutrition: Effects on health in the next generation Caroline Fall MRC Epidemiology Resource Centre, University of Southampton, Southampton General Hospital Southampton, UK Received April 24, 2009 Nearly 20 years ago, it was discovered that low birthweight was associated with an increased risk of adult diabetes and cardiovascular disease (CVD). This led to the hypothesis that exposure to undernutrition in early life increases an individual’s vulnerability to these disorders, by ‘programming’ permanent metabolic changes. Implicit in the programming hypothesis is that improving the nutrition of girls and women could prevent common chronic diseases in future generations. Research in India has shown that low birthweight children have increased CVD risk factors, and a unique birth cohort in Delhi has shown that low infant weight, and rapid childhood weight gain, increase the risk of type 2 diabetes. Progress has been made in understanding the role of specific nutrients in the maternal diet. In the Pune Maternal Nutrition Study, low maternal vitamin B12 status predicted increased adiposity and insulin resistance in the children, especially if the mother was folate replete. It is not only maternal undernutrition that causes problems; gestational diabetes, a form of foetal overnutrition (glucose excess), is associated with increased adiposity and insulin resistance in the children, highlighting the adverse effects of the ‘double burden’ of malnutrition in developing countries, where undernutrition and overnutrition co-exist. Recent intervention studies in several developing countries have shown that CVD risk factors in the offspring can be improved by supplementing undernourished mothers during pregnancy. Results differ according to the population, the intervention and the post-natal environment. Ongoing studies in India and elsewhere seek to understand the long-term effects of nutrition in early life, and how best to translate this knowledge into policies to improve health in future generations. Key words Low birth weight - foetal growth - maternal nutritional status - underweight Introduction was because of better childhood living conditions brought about by social reforms. In 1977, Forsdahl2 discovered a geographical correlation in Norway between heart disease mortality in 1964-1967 and infant mortality rates 70 years earlier. He suggested that growing up in poverty caused ‘permanent damage’ perhaps due to a ‘nutritional deficit’, which resulted in ‘life-long vulnerability’ to an affluent adult lifestyle and high fat intakes. The concept that longevity is influenced by events in early life is not new. In 1934, Kermack et al 1 showed that death rates in Europe from 1751 to 1930 fell with each successive year-of-birth cohort. They rejected one possible explanation, that ‘a more healthy race of children was born in each successive decade’, and thought that it 593 594 INDIAN J MED RES, NOVEMBER 2009 Studies by Barker & Osmond3,4 in the UK, a decade later, focused on pre-natal factors. Differences around the UK in neonatal mortality (a marker for low birthweight) in 1921-1925 predicted death rates from stroke and heart disease in 1968-19783. The discovery of birth records dating from 1911 in the county of Hertfordshire made it possible to show that low birthweight and weight at one year were associated with an increased risk of death from cardiovascular disease4. There was an approximate doubling of mortality from the highest to the lowest extremes of birthweight. Based on these findings, they put forward the controversial hypothesis that poor foetal and early post-natal nutrition was a cause of adult cardiovascular disease. He was convinced that falling mortality rates in the western world were because mothers, and therefore foetuses and babies, were better nourished, with each succeeding generation. Since then, studies around the world have shown that lower birthweight is associated with an increased risk of a wide range of health problems in adult life, including type 2 diabetes5, metabolic syndrome6, chronic lung disease7, osteoporosis8 and mental illness9. There is also a wealth of data showing that poor intrauterine and infant growth and nutrition are associated with reduced capacity in adult life, including reduced stature, lower physical work capacity, impaired cognitive function and educational attainment, and (for women) an increased risk of low birthweight in the next generation10. These studies have led to a new branch of scientific research: the developmental origins of health and disease (DOHaD). or ‘programmed’ because they occur during critical periods of early development. The mechanisms by which this could occur11-15 include simple growth failure, leading to impaired organ size and structure, for example, reduced numbers of pancreatic beta cells, renal nephrons or brain neurones, and altered arterial structure. These include altered endocrine settings, for example, reduced insulin secretion and sensitivity, and upregulation of the HPA axis and sympathetic nervous system. At a cellular level, these include altered epigenetic characteristics – changes to the proteins and other molecules attached to DNA which control gene expression. Each of these changes can lead directly to adult cardiovascular disease, or render the individual more susceptible to the effects of environmental stressors such as obesity arising in later life. The programming hypothesis is supported by numerous examples of nutritional programming in experimental animals. In rats, maternal protein restriction in pregnancy leads to higher blood pressure16, impaired glucose tolerance17, insulin resistance18,19, and altered hepatic architecture and function20 in the adult offspring. Animal experiments allow more sophisticated study of the mechanisms of programming at tissue and cellular levels. For example, insulin resistance and The foetal programming hypothesis Obviously, it is not low birthweight of itself that causes these problems, but what low birthweight represents: foetal undernutrition and impaired development11 (Fig. 1). The foetus depends on the transfer of nutrients from the mother, and adapts to inadequate nutrition in several ways: prioritization of brain growth at the expense of other tissues such as the abdominal organs, altered secretion and sensitivity to the foetal growth hormones insulin and insulinlike growth factor-1 (IGF-I), and upregulation of the hypothalamo-pituitary-adrenal (HPA) ‘stress’ axis. The foetus sacrifices tissues that require high-quality building blocks, like muscle or bone, and instead lays down less demanding tissue, like fat. Although occurring in response to a transient phenomenon (foetal undernutrition), these changes can become permanent Fig. 1. The foetal programming hypothesis; flow diagram illustrating proposed effects of intra-uterine nutrition on the foetus, and long-term effects on metabolism and disease risk. Source: Ref. 23. FALL: DEVELOPMENTAL ORIGINS OF HEALTH & DISEASE 595 impaired glucose tolerance in adult offspring of proteindeprived rats results from reduced gene expression for enzymes in the insulin-signalling pathway18. Raised blood pressure in the offspring of protein-deprived rats has been linked to epigenetic changes that can be prevented by supplementing the mother with folate21. cholesterol concentrations and subscapular/triceps skinfold ratios, and after adjusting for 8-year weight, higher systolic blood pressure and insulin resistance22. These risk factors were highest in children who were born small but became the biggest (heaviest, tallest and most adipose) at 8 years. Associations of cardiovascular disease and its risk factors with different body proportions at birth may reflect undernutrition during critical periods in gestation for the development of tissues and organ systems11. Male and female foetuses have different growth priorities, and adapt differently to undernutrition, reflected in sex differences in associations with neonatal body proportions11. The hyperplastic development of many tissues continues in early infancy, and undernutrition during infancy is probably equally important3. Another clear example of the disadvantages being small in early life and becoming obese as an adult came from a study of young adults in New Delhi, who were measured at birth and every 6 months until the age of 21 yr23. Mean birthweight was only 2.9 kg. As children, many of the cohort were underweight-forage [53% at the age of 2 yr, using National Center for Health Statistics (NCHS) standards]. When they were re-traced at 26-32 yr, 40 per cent were overweight (BMI >25 kg/m2) and 10 per cent were obese (BMI >30 kg/m2). Four per cent already had type 2 diabetes and 15 per cent had impaired glucose tolerance (IGT) (pre-diabetes). After adjusting for adult BMI, plasma glucose concentrations and insulin resistance were inversely related to birthweight, and IGT and diabetes were associated with lower weight and BMI at the age of 1 yr. In contrast, the childhood growth of those who developed IGT or diabetes was characterised by accelerated BMI gain relative to the rest of the cohort (Fig. 2). From being below the cohort mean for BMI at 2 years they were well above the mean at 30 years. The highest prevalence of IGT and diabetes was in men and Research in the Indian scenario Indian researchers have made a major contribution to the DOHaD field and towards its translation into improved human health. A study of CVD risk factors in Indian children was the first in a developing country to examine associations between size at birth and later risk22. Among 4 yr old children born in the KEM Hospital, Pune, lower birthweight was associated with higher plasma glucose concentrations after an oral glucose load. When the children were re-studied at 8 years, those of lower birthweight had higher LDL- Age (yr) Age (yr) Fig. 2. Data from the New Delhi birth cohort. Mean sex-specific SD scores for height (left) and BMI (right) at every age from birth to 21 yr, and when studied at 26-32 yr, for subjects who developed IGT or diabetes. Mean SD scores are indicated by the solid line, and 95 per cent CI’s by dotted lines. The mean SD score for the whole cohort is zero. [Reprinted with permission from the Massachusetts Medical Society (The New England Journal of Medicine 2004; 350 : 865-75)]. 596 INDIAN J MED RES, NOVEMBER 2009 women who had low BMI SD scores in infancy but high SD scores at 12 years or later. There are a number of possible reasons why weight gain in childhood, on a background of foetal restriction, might cause disease. Low birthweight babies tend to catch-up (compensatory growth), and the rapidity of post-natal growth may simply indicate the severity of growth retardation at birth. Alternatively the process of catch-up may be disadvantageous in itself. It may impose excess demand on other tissues which are not capable of compensatory hyperplasia, such as the pancreas. It may alter body composition; animals can gain excessive fat if they are placed on a high plane of nutrition after a period of early postnatal undernutrition24. McCance suggested that good nutrition at this stage emphasises the development of tissues like fat, which maintain the capacity for growth throughout life, but cannot recover tissues such as muscle, which develop earlier and lose the capacity for cell division24. Another possibility is that the hormones driving catch-up growth have adverse cardiovascular and metabolic effects25. The Pune Maternal Nutrition Study has given insight into foetal development in Indian populations. This is a prospective population-based observational study of rural Indian women and their offsprings26,27. The mothers were short and thin (mean pre-pregnant height and BMI: 152 cm and 18.1 kg/m2) and the mean full term birthweight was only 2.7 kg. Detailed anthropometry of the newborns showed that their body composition differed from white Caucasian babies born in the UK27. They were lighter by almost 2 standard deviations, and lean tissues such as muscle (mid-upperarm circumference) and abdominal viscera (abdominal circumference) showed a similar deficit. Truncal fat (subscapular skinfolds), however, was relatively ‘spared’ (-0.5 SD). Thus, although extremely small and thin, the babies were relatively adipose. A similar pattern has been confirmed in urban Indian populations28. The aetiology of the muscle-thin but adipose ‘thinfat’ phenotype of Indian newborns is unknown. The adiposity is related to maternal adiposity and lipid, glucose and insulin concentrations, but the low lean mass is unexplained. The phenotype may be ‘adaptive’ and carry survival advantage; for example, in the face of a nutritional deficit, muscle growth may be sacrificed, and fat laid down preferentially as a substrate for brain growth and/or immune function. Its consequences for later health are unknown; however it echoes the well-described adult Indian phenotype (lower muscle mass, higher percentage body fat, and greater tendency to central adiposity than white Caucasians) that is strongly associated with type 2 diabetes29. The findings highlight the fact that birthweight provides only a crude summary of foetal growth and fails to describe potentially important differences in the development of specific tissues. Studies in India have also highlighted problems associated with maternal diabetes, which causes extreme high rather than extreme low birthweight. In a recent study of contemporary women giving birth in Mysore30, the prevalence of gestational diabetes was high (6%) despite a low average maternal age and BMI. As expected, babies born to diabetic mothers were heavier (mean birthweight 3339 g) than babies of mothers with normal glucose tolerance (2956 g). When studied at the age of 5 yr, they were more adipose and had higher insulin concentrations, than children of nondiabetic mothers30. The role of nutrition Foetal growth depends on the uptake of nutrients, which occurs at the end of a complex materno-foetal supply line31. This includes intake, i.e., the mother’s appetite, diet and absorption. The nutrients arriving at the placenta, and how they are transferred to the foetus, depend on maternal metabolism: her endocrine status, her partitioning of nutrients between storage, utilization or circulation, and her cardiovascular adaptations to pregnancy, such as plasma volume expansion which increases uterine blood flow. These are influenced by maternal nutrition in ways that are poorly understood. The link between maternal and foetal nutrition is thus indirect and explains why the full impact of maternal diet on foetal growth remains unclear. Foetal growth can be readily restricted in experimental animals by reducing maternal intakes of energy and protein during pregnancy31. Energy and protein deficiency in the mother is also associated with intrauterine growth retardation in humans, size at birth is strongly related to maternal body mass index, and during acute famine birthweight falls by several hundred grams32,33. However, randomised clinical trials (RCTs) of energy and/or protein supplements have shown only small effects on birthweight34. There is evidence that supplementing undernourished mothers with micronutrients, or improving the diet quality, increases foetal growth. The Pune Maternal Nutrition Study showed that mothers with higher intakes of FALL: DEVELOPMENTAL ORIGINS OF HEALTH & DISEASE micronutrient-rich foods like green leafy vegetables, fruit and milk had babies that were larger in all body dimensions26. Several recent RCTs have also shown increased newborn size after maternal micronutrient supplementation, although the increase was small35,36. Foetal growth is related to maternal height and birthweight. This suggests that undernutrition of the mother during her own foetal life and childhood growth limits the growth of her foetus. Effects of the mother’s current nutritional status are therefore influenced by her own past nutrition and that of earlier generations. A relatively un-researched time is the periconceptional period. Before the mother even knows she is pregnant, and before placentation occurs, sufficient nutrients must be present in the embryo’s immediate environment. The importance of periconceptional nutrition has been demonstrated by the reduction in neural tube defects with pre-conceptional folate supplementation37. In experimental animals, peri-conceptional undernutrition alters the allocation of cells in the blastocyst and permanently changes the foetal growth trajectory. Later effects in the offspring include pre-term delivery and adult hypertension38,39. Several micronutrients, especially those involved in 1-carbon metabolism (such as folic acid and vitamin B12) act as co-factors or molecular donors for epigenetic processes such as DNA methylation, which modulate gene expression, and therefore cellular proliferation and apoptosis, during foetal development. Genomewide demethylation occurs just after fertilization, followed by re-methylation at different stages of embryonic development40. Epigenetic changes induced at this time may become permanent and heritable, determining outcomes in later life and in the next generation. Maternal diet, and especially folate and vitamin B12 intakes influences these processes. For example, the phenomenon in rats by which maternal protein restriction leads to hypertension in the offspring, and its prevention by maternal folate supplementation, have been linked to the de-methylation (by protein restriction) and re-methylation (by folate) of specific genes41. 597 surveys and famine studies. For example, the Dutch Famine studies have shown that maternal exposure to famine in late gestation was associated with glucose intolerance and insulin resistance in the offspring42. The current focus on developmental origins of health and disease has led to the setting up of new prospective studies in which detailed information on maternal nutrition in pregnancy has been collected. One of these, the Pune Maternal Nutrition Study, has shown that low maternal calcium intake is associated with lower bone mineral content in the children43. This may be a simple example of inadequate ‘building blocks’ for the tissue concerned. The same study has also provided evidence of the importance of 1-carbon metabolism in programming processes. Vitamin B12 deficiency in the mother, especially if she was folate replete, was associated with increased body fat and insulin resistance in the children (Fig. 3)44. We are now beginning to see the DOHaD hypothesis tested in intervention studies, by following up the children of undernourished women who took part in randomized controlled trials of nutritional supplementation in pregnancy. A follow up study of adults born during the INCAP trial in Guatemala, in which villages were randomized to receive Atole45 (a high-energy, high-protein drink) or Fresco (lower energy, no protein) found higher HDL-cholesterol and lower triglyceride concentrations in those whose mothers had Atole45. Among adolescents in India, whose pregnant mothers received food-based energy and protein supplements as part of a package of public health interventions, insulin resistance and arterial stiffness were reduced compared to controls46. Systolic Maternal nutritional status and disease risk in the offspring If the foetal programming hypothesis is right, and maternal nutrition has important effects on adult health, correlations would be expected between measures of maternal nutrition and disease in the offspring. Until recently, the only data to test this were from old dietary Fig. 3. Insulin resistance (HOMA) in children aged 6 yr from the Pune Maternal Nutrition Study, in relation to maternal vitamin B12 (18 wk) and erythrocyte folate (28 wk). [Reprinted with permission from Springer (Diabetologia 2008; 51 : 29-38)]. 598 INDIAN J MED RES, NOVEMBER 2009 blood pressure was lower (-2.5 mmHg) in 2-yr old Nepali children whose mothers received multiple micronutrients in pregnancy rather than standard iron/ folate tablets47. However, there were negative findings in a trial of high-energy biscuits in the Gambia48. The intervention reduced the incidence of low birthweight by 40 per cent and halved perinatal mortality, but at follow up there was difference in blood pressure between children born to women who received the intervention during pregnancy compared to women who received it during lactation. There are many good reasons for improving the diets of undernourished mothers. The Gambia supplement produced an impressive reduction in perinatal mortality, and in Guatemala, early-life exposure to Atole improved childhood growth and adult economic productivity49. Clearly, at present, there is inadequate evidence that such interventions improve adult health in the offspring. The findings from these trials suggest that there may be beneficial effects on some cardiovascular risk factors, that these are complex, and differ according to the population, the intervention and the post-natal environment. Given the need for much deeper understanding, it is to be hoped that the investigators will follow up their subjects further to determine the full extent of any effects, and that other trials of enhanced materno-foetal nutrition will add data to the currently meagre evidence-base on this important issue. Acknowledgment The work reported in this review was supported by the Medical Research Council, UK, the Wellcome Trust, UK, the British Heart Foundation and the Parthenon Trust. References 1. Kermack WO, McKendrick AG, McKinlay PL. Death rates in Great Britain and Sweden; some general regularities and their significance. Lancet 1934; i : 698-703. 2. Forsdahl A. Are poor living conditions in childhood and adolescence an important risk factor for arteriosclerotic disease? Br J Prev Soc Med 1977; 31 : 91-5. 3. Barker DJP, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet 1986; i : 1077-81. 4. Barker DJP, Osmond C, Winter PDW, Margetts B, Simmonds SJ. Weight in infancy and death from ischaemic heart disease. Lancet 1989; ii : 577-80. 5. EARLYREAD Collaboration. Birthweight and risk of type 2 diabetes: a quantitative systematic review of published evidence. JAMA 2008; 300 : 2885-97. 6. Ramadhani MK, Grobbee DE, Bots ML, Castro Cabezas M, Vos LE, Oren A, et al. Lower birthweight predicts metabolic syndrome in young adults: the Atherosclerosis Risk in Young Adults (ARYA) study. Atherosclerosis 2006; 184 : 21-7. 7. Barker DJP, Godfrey KM, Fall CHD, Osmond C, Winter PD, Shaheen S. The relation of birthweight and childhood respiratory infection to adult lung function and death from chronic obstructive airways disease. BMJ 1991; 303 : 671-5. 8. Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, Hanson M. Developmental origins of osteoporotic fracture. Osteoporosis Int 2006; 17 : 337-47. 9. Landon J, Davison M, Breier B. The developmental environment: influences on subsequent cognitive function and behaviour. In: Gluckman P, Hanson M, editors. Developmental origins of health and disease. Cambridge: Cambridge University Press; 2006. p. 370-8. 10. Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al and the Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: consequences for adult health and human capital. Lancet 2008; 371 : 340-57. 11. Barker DJP. Mothers, babies and health in later life. London: Churchill Livingstone; 1998. 12. Lucas A. Programming by early nutrition in man. Ciba Foundation Symposium No. 156, Chichester, UK: John Woley and Sons; 1991. p. 38-50. 13. Waterland RA, Garza C. Potential mechanisms of metabolic imprinting that lead to chronic disease. Am J Clin Nutr 1999; 69 : 179-97. 14. Nafee TM, Farrell WE, Carroll WD, Fryer AA, Ismail KMK. Epigenetic control of fetal gene expression. Br J Obstet Gyncol 2008; 115 : 158-68. 15. Fall CHD. Fetal and maternal nutrition. In: Stanner S, editor. Cardiovascular disease: Diet, nutrition and emerging risk factors. Oxford, UK: British Nutrition Foundation Task Force. Blackwell Publishing; 2005. 16. Langley SC, Jackson AA. Increased systolic blood pressure in adult rats induced by fetal exposure to maternal low protein diets. Clin Sci 1994; 86 : 217-22. 17. Ozanne SE, Hales CN. The long-term consequences of intrauterine protein malnutrition for glucose metabolism. Proc Nutr Soc 1999; 58 : 615-9. 18. Ozanne SE, Dorling MW, Wang CL, Nave BT. Impaired PI 3-kinase activation in adipocytes from early growth-restricted rats. Am J Physiol 2001; 280 : E534-9. 19.Vickers MH, Breier BH, Cutfield WS, Hofman PL, Gluckman PD. Fetal origins of hyperphagia, obesity, and hypertension and postnatal amplification by hypercaloric nutrition. Am J Physiol Endocrinol Metab 2000; 279 : E83-7. 20. Hales CN, Desai M, Ozanne SE, Crowther NJ. Fishing in the stream of diabetes: from measuring insulin to the control of fetal organogenesis. Biochem Soc Trans 1996; 24 : 341-50. 21. Torrens C, Brawley L, Anthony FW, Dance CS, Dunn R, Jackson AA, et al. Folate supplementation during pregnancy improves offspring cardiovascular dysfunction induced by protein restriction. Hypertension 2006; 47 : 982-7. 22. Bavdekar A, Yajnik CS, Fall CHD, Bapat S, Pandit AN, Deshpande V, et al. The insulin resistance syndrome (IRS) in eight-year-old Indian children: small at birth, big at 8 years or both? Diabetes 2000; 48 : 2422-9. FALL: DEVELOPMENTAL ORIGINS OF HEALTH & DISEASE 23. Bhargava SK, Sachdev HPS, Fall CHD, Osmond C, Lakshmy R, Barker DJP, et al. Relation of serial changes in childhood body mass index to impaired glucose tolerance in young adulthood. N Engl J Med 2004; 350 : 865-75. 24. McCance RA. Food, growth and time. Lancet 1962; ii : 621-6. 25. Lever AF, Harrap SB. Essential hypertension: a disorder of growth with origins in childhood? J Hyperten 1992; 10 : 101-20. 26. Rao S, Yajnik CS, Kanade A, Fall CHD, Margetts BM, Jackson AA, et al. Intake of micronutrient-rich foods in rural Indian mothers is associated with the size of their babies at birth; the Pune Maternal Nutrition Study. J Nutr 2001; 131 : 1217-4. 27. Yajnik CS, Fall CHD, Coyaji KJ, Hirve SS, Rao S, Barker DJP, et al. Neonatal anthropometry: the thin-fat Indian baby; the Pune Maternal Nutrition Study. Int J Obesity 2003; 27 : 173-80. 28. Krishnaveni GV, Hill JC, Veena SR, Leary SD, Saperia J, Chachyamma KJ, et al. Truncal adiposity is present at birth and in early childhood in South Indian children. Indian Pediatr 2005; 42 : 527-38. 29. Yajnik CS. Obesity epidemic in India: intra-utrine origins? Proc Nutr Soc 2004; 63 : 1-10. 30. Krishnaveni GV, Hill JC, Leary S, Veena SR, Saperia J, Saroja A, et al. Anthropometry, glucose tolerance and insulin concentrations in Indian children: relationships to maternal glucose and insulin concentrations during pregnancy. Diabetes Care 2005; 28 : 2919-25. 31. Harding JE. The nutritional basis of the fetal origins of adult disease. Int J Epidemiol 2001; 30 : 15-25. 32. Leary S, Fall CHD, Osmond C, Lovel H, Campbell D, Eriksson J, et al. Geographical variation in relationships between parental body size and offspring phenotype at birth. Acta Obstet Scand 2006; 85 : 1066-79. 33. Susser M, Stein Z. Timing in prenatal nutrition: a reprise of the Dutch Famine Study. Nutr Rev 1994; 52 : 84-94. 34. Kramer MS. Balanced protein/energy supplementation in pregnancy. In: The Cochrane Library, Issue 3. 2001 Oxford: Update software. 35. Haider BA, Bhutta ZA. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst Rev(4), CD004905, 2006. 36. Bhutta Z, Ahmad T, Black RE, Cousens S, Dewey K, Giugliani E, et al and the Maternal and Child Undernutrition Study Group. What works? Interventions to affect maternal and child undernutrition and survival globally. Lancet 2008; 371 : 417-40. 37. Lumley J, Watson L, Watson M, Bower C. Periconceptional supplementation with folate and/or multivitamins for preventing neural tube defects. Cochrane Database Syst Rev 2001; 3 : CD001056. 599 38. Bloomfield F, Oliver M, Harding JE.The late effect of fetal growth patterns. Arch Dis Child Fetal Neonatal Ed 2006; 91 : 299-304. 39. Watkins AJ, Wilkins A, Cunningham C, Perry VH, Seet MJ, Osmond C, et al. Low protein diet fed exclusively during mouse oocyte maturation leads to behavioural and cardiovascular abnormalities in the offspring. J Physiol 2008; 586 : 2231-44. 40. Godfrey KM, Lillycrop KA. Epigenetic mechanisms and the mismatch concept of the developmental origins of health and disease. Ped Res 2007; 61 : 5R-9R. 41. Lillycrop KA, Phillips ES, Jackson AA, Hanson MA, Burdge GC. Dietary protein restriction of pregnant rats induces, and folic acid supplementation prevents, epigenetic modification of hepatic gene expression in the offspring. Br J Nutr 2005; 135 : 1382-6. 42. Ravelli ACJ, van der Meulen JHP, Michels RPJ, Osmond C, Barker DJP, Hales CN, et al. Glucose tolerance in adults after prenatal exposure to famine. Lancet 1998; 351 : 173-7. 43. Ganpule A, Yajnik CS, Fall CHD, Rao S, Fisher DJ, Kanade A, et al. Bone mass in Indian children; relationships to maternal nutritional status and diet during pregnancy; the Pune Maternal Nutrition Study. J Clin Endocrinol Metab 2006; 91 : 29943001. 44. Yajnik CS, Deshpande SS, Jackson AA, Refsum H, Rao S, Fisher DJ, et al. Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: The Pune Maternal Nutrition Study. Diabetologia 2008; 51 : 29-38. 45. Stein AD, Wang M, Ramirez-Zea M, Flores R, Grajeda R, Melgar P, et al. Exposure to a nutrition supplementation intervention in early childhood and risk factors for cardiovascular disease in adulthood: evidence from Guatemala. Am J Epidemiol 2006; 164 : 1160-70. 46. Kinra S, Sarma KVR, Ghafoorunissa, Mendu VVR, Ravikumar R, Mohan V, et al. Effect of integration of supplemental nutrition with public health programmes in pregnancy and early childhood on cardiovascular risk in rural Indian adolescents: long term follow-up of Hyderabad nutrition trial. BMJ 2008; 337 : 1-10. 47. Vaidya A, Saville N, Shrestha BP, Costello AM, Manandhar DS, Osrin D. Effects of a maternal multiple micronutrient supplement on children’s weight and size at 2 years of age in Nepal; follow-up of a double blind randomised controlled trial. Lancet 2008; 371 : 452-4. 48. Hawkesworth S, Prentice A, Fulford A, Moore S. Maternal protein-energy supplementation does not affect adolescent blood pressure in the Gambia. Int J Epidemiol 2009; 38 : 119-27. 49. Hoddinot J, Maluccia JA, Behrman JR, Flores R, Martorell R. Effect of a nutrition intervention in early childhood on economic productivity in Guatemalan adults. Lancet 2008; 371 : 411-6. Reprint requests: Prof. Caroline HD, MRC Epidemiology Resource Centre, University of Southampton, Southampton General Hospital Tremona Road, Southampton, UK SO16 6YD e-mail: chdf@mrc.soton.ac.uk













© Copyright 2025