
12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity
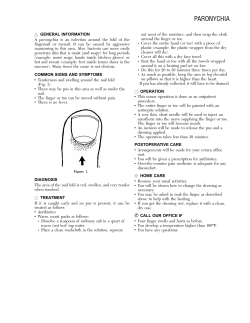
Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity 12 Angela Simon 12.1 Introduction Hammer toe and claw toe deformity is often addressed surgically. Depending on the stage of the deformity and on the dynamic and static factors, the surgical treatment should be performed via sequential procedures. The decision of how many surgical procedures will be required is done preoperatively as well as in the surgical theatre during the progression of surgically stabilizing and balancing the ray (digit and metatarsal). The definition of the deformities of lesser toes in the literature varies. In this chapter I define the digital deformities1 according to Table 12.1 (Fig. 12.1). More important for planning the surgical treatment is the knowledge of biomechanical basics in order to treat the anatomical structure. Knowledge of how to balance the tendon pathology avoids the recurrence of the deformity. 12.2 Biomechanical Basics The hinge joints have the sagittal range of motion in dorsiflexion and plantarflexion. To maintain balance, tendons normally have a combination of forces. It is important to know that only the intrinsic muscles, lumbricales and interossei, have a direct influence on plantarflexing the metatarsalphalangeal joint (MTPJ) A. Simon Klinik für Orthopädie 2, Fußzentrum Malchin, Dietrich-Bonhoeffer-Klinikum, Basedower Strasse 33, 17139 Malchin, Germany e-mail: alegna.nomis@t-online.de of the lesser toes. They blend distally into the extensor hood of the proximal phalanx (Fig. 12.2).2,3 They stay plantarly of the MTPJ axis. “The lumbricales tendons cause plantarflexion at the Metatarsophalangeal joint and dorsiflexion of the Interphalangeal joints by a sling mechanism.”2 In comparison, the tendon of the flexor digitorum longus inserts more distal at the middle phalanx. Their influence of plantarflexing the MTPJ is not direct. They plantarflex the proximal interphalangeal joint (PIPJ) and cannot neutralize the deforming forces (Fig. 12.3a).4 Imbalance of the tendons, depending on different causes, develops almost always, with the exception of special neuropathic disorders,5 weakness of the intrinsic muscles. The result is the permanent dorsiflexion of the proximal phalanx in the MTPJ and the plantarflexion in the PIPJ (Fig. 12.3b). “the flexion moment of the interossei at the MTPJ is decreased markedly because of their normal proximity to the insert center of rotation of the MTP joint on the metatarsal head”.6 The flexible deformity advances to a rigid and painful situation with callosity at the tip of the deformity (dorsal PIPJ) because of the pressure from the shoe dorsally and from the ground plantar. The severe deformity shows a permanent dorsal luxation of the proximal phalanx. “The base of the proximal phalanx is displaced onto the dorsum of the metatarsale neck along with the Table 12.1 Determining hammer toe, claw toe, and mallet toe Hammer toe Claw toe Mallet toe MTPJ Extended Extended Straight (extended) PIPJ Flexed Flexed Straight DIPJ Straight Flexed Flexed A. Saxena (ed.), International Advances in Foot and Ankle Surgery, DOI: 10.1007/978-0-85729-609-2_12, © Springer-Verlag London Limited 2012 107 108 A. Simon a Fig. 12.2 Intrinsic muscles2 a Extensor digitorum brevis Extensor digitorum longus b Flexor digitorum longus b Plantar plate Flexor digitorum brevis Long extensor Short extensor Plantar plate Long flexor Short flexor Skin Keratosis c Fig. 12.3 (a) Normal basic bony, tendinous, and capsular anatomic features in the lesser toes.3 (b) Typical deformity of the lesser toes.4 b Displaced fascial slips Dorsally dislocated MP joint Streched plantar fascial slips encircle MT neck Fig. 12.1 (a) Hammer toe. (b) Claw toe. (c) Mallet toe (third toe) Fig. 12.4 Plunger effect3 Increased ‘plunger’ effect of dorsally displaced plantar plate when plantar fascia tightens 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity a 109 b Fig. 12.5 Push-up test for a flexible hammertoe deformity (a) which reduces with plantar pressure (b)7 remnants of the plantar plate and the transverse intermetatarsale ligament”.4 The pathologic direction of tendon forces intensifies the deformity. Stainsby calls it a “plunger effect”: “The plantar plate is tethered to the contiguous deep transverse metatarsal ligament. Because of the dorsally displaced slips of the deeper layer of plantar plate, the MT head becomes depressed by a plunger mechanism”3 (Fig. 12.4). The mallet toe deformity results in a flexible or rigid contraction of the distal phalanx and is the result of a hyperactivity or contracture of the flexor digitorum longus tendon. It creates compression on the flexed tip of the toe, including the nail. A callosity and even ulcer may develop in this region. 12.3 Clinical Examination Painful callosity at the tip of the PIPJ or below the metatarsal head is often the reason for patients’ first consultation to the foot surgeon. The inspection of the axis of hip, knee, and ankle joint and the examination of muscle function is necessary to integrate or distinguish the deformity of the toes. Rotation disorders of the leg can be compensated by hyperfunction of the extrinsic muscles (extensor digitorum longus or flexor digitorum longus) and neutralize while correcting the axis of the leg if the deformity still is flexible. “Neuropathic disorders (e.g., hereditary motor–sensory neuropathy) show an imbalance preponderating the power of the extensor digitorum longus tendons, while the intrinsic Muscles – responsible to platarflex the MPTJ – are weakened.”5 After the examination, including the gait and standing bare-foot, the palpation of the foot is important to feel indurations, flexibility of every joint, tension of tendons, and painful spots. The push up test 7 (Fig. 12.5), a passive test to examine the flexibility of the MTPJ and PIPJs, is very important in deciding if a surgical release of these joints is necessary. Examination of the distal interphalangeal joint and testing the flexibility of the flexed position of the distal phalanx should be performed actively and passively. It is useful to observe the loaded foot to determine if 110 A. Simon Fig. 12.6 X-ray or hammertoe 2nd and clawtoe 3rd digits AP (a) and lateral view (b) a the deformity is flexible. Additionally, passive testing should be performed by direct palpation of the joint, and also with a flexed MTPJ. In this position the flexor digitorum longus tendon is relaxed and a flexible deformity would disappear. The active range of motion and also the isometric tests of the muscles are necessary to get the information about the dynamic balance between dorsiflexing and plantarflexing function at every joint of the lesser toes. 12.4 Radiological Information It proves useful to perform the x-ray of the whole foot in weight-bearing dorsoplantar view and exact lateral view (Fig. 12.6). In cases where the metatarsalgia is dominant, an axial view of the metatarsal heads (“sprinter/ plantar axial view”) is good additional information. 12.5 Surgical Treatment If the clinical examination has revealed that the deformity is no longer flexible, there is no chance to correct the axis and the dynamic imbalance with taping, insoles, orthoses, or stretching. The indication for a surgical treatment is the rigid and painful deformity. “Unattractive deformity that is painless is not an indication for surgical correction.”6 b The goals of the lesser toe surgery: s Correcting the axis of the toe s Stabilizing the dynamic balance between dorsi-and plantarflexion s Preserving vessels and nerves to maintain a good integrity, especially lymphatic drainage 12.5.1 Performance of the Surgical Procedure Correction of the digital deformity is the goal. The push up test is a useful and important help during the procedure. 1. Skin incision is longitudinal dorsal from distal of the PIPJ, V-shaped above the MTPJ (Fig. 12.7) to avoid a hyperdorsiflexion because of a rigid skin scar afterward. 2. Isolate the tendons of the extensor digit, longus and brevis, cutting the distal insertion of the brevis tendon, which is always located lateral of the extensor digitorum longus (EDL), inserting at the extensor hood. 3. In most cases, where the proximal phalanx does not present a total subluxation in the MTPJ, split the tendon of the EDL longitudinally (Fig.12.8a) for a later Z-plasty lengthening (Fig.12.8b). Attention: In case of a severe luxation I suggest the Stainsby 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity 111 a Fig. 12.7 Skin incision procedure with a transposition of the tendon. If deciding to perform the Stainsby procedure, at this step of the surgery procedure the EDL tendon is cut proximally without splitting (described later in this chapter). 4. Open the PIPJ, resect the collateral ligaments (Fig.12.9a), and resect the condyles (Fig. 12.9b, c) of the distal proximal phalanx to produce a little hollow in the surface. 5. Remove the cartilage of the base of the middle phalanx (Fig. 12.10a), creating a little roof. With these formations, like a positive and negative (Fig.12.10b), it is possible to avoid a rotating failure. 6. First push up test: Does the ray, the MTPJ included, stay in a right, straight position? (Fig.12.5). 7. A – Yes? Then the procedure will be finished with the temporary transarticular fixation of the ray, including the PIP fusion: s A double tip K-wire (1.4 mm diameter) drilling backward (Fig. 12.11a) from the middle phalanx out of the top of the toe, then holding the ray in the straight position drilling forward (Fig. 12.11b) the proximal end of the pin through the proximal phalanx into the distal metatarsal. The distal end of the K-wire is bent as a loop or covered with a plastic cap. s The two halves of the tendon of the ext. digitorum longus are sutured in a moderate tension as a lengthening Z-plasty (Fig. 12.12). B – No! If the ray does not stay rectus, the remaining deformity in the MTPJ (rigid dorsiflexion) has to be corrected: b Fig. 12.8 (a) Isolating and splitting the ext. digit. lg. tendon and (b) longitudinal splitting s Open the capsule of the MTPJ (Fig. 12.13); the dorsal capsule should be resected and the contracted collateral ligaments are incised. Be careful not to cut the vessels and nerves. 8. Second push up test: Does the ray, the MTPJ included, stay in a right, straight position? 9. A – Yes? Finish the procedure as shown in 7–A. B – No! Free the MTPJ plantarly; either adhesive capsule to the plantar plate or a ruptured 112 a A. Simon b c Fig. 12.9 (a) Opening the PIPJ. (b) Resecting the collateral ligaments and resection of the condyles. (c) Removal of the resected condyles plantar plate is the reason for this remaining deformity. s With a special instrument, the McGlamry elevator, carefully release this rigid tissue (Fig. 12.14a); the instrument is very sharp and the formation or the shape of the metatarsal head having a big convex structure plantarside must be known. Otherwise the cartilage or bone will be damaged. 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity a 113 b Fig. 12.10 (a) Removing cartilage of the base of the middle phalanx. (b) Formation of the surfaces as positive and negative v-shaped a b Fig. 12.11 Fixation with a K-wire. (a) Retrograde and (b) anterograde s If the plantar plate is ruptured, the current opinion in the literature is to repair the defect. Otherwise the head of the metatarsal can be dislocated again as the forces of the tendons are not in correct balance and the plunger effect will recur. s The plantar plate can be sutured from the dorsal approach, but the gap of the joint is narrow. An assistant is needed to distract the ray. With a little needle using a 2-0 suture (nonabsorbable) it might be possible to close the defect. Otherwise closure can be performed with a separate approach from plantarly: “The surgical approach for repair of an unstable second MTPJ is through a plantar incision in the first intermetatarsal space.”8 114 A. Simon a b Fig. 12.12 Lengthening suture of the ext. digit. lg. tendon Fig. 12.14 (a) The McGlamry elevator. (b) Fixation with a K-wire anterograde Fig. 12.13 Opening the capsule of the MTPJ – Carefully approach through the plantar soft tissue, preserving the vessels and nerves between the metatarsal heads at both sides. Open the sheet of the flexor tendons and separate the tendons to reach the plantar plate and visualize the rupture. “With the flexor tendons retracted, a well-defined defect in the midsubstance of the plantar plate is observed.”8 – Now you have a direct view of the cartilage of the metatarsal head. Suture with 2.0 nonabsorbable (Fig. 12.15). 10. Third push up test: Does the toe, the MTPJ included, stay in a right, straight position? 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity 115 a b Fig. 12.15 Repair of the plantar plate from the plantar approach. Courtesy of Richard Bouché, DPM 11. A – Yes? Then finish the procedure as in step 7–A. Figure 12.16 shows the preoperative situation. Keep the K-wire for 5 weeks. The removal is not painful; normally local anesthesia is not needed. Take care that the toe is fixed while extracting the K-wire with a forceps, otherwise the fusion of the PIP joint can burst. B – No! Then there are usually three kinds of disorders. The decision of surgical treatment depends on the etiology of the disorder. I. Rheumatoid arthritis (Fig. 12.17). I suggest the Stainsby procedure after steps 1–10 (without step 7A). Shorten the base of the proximal phalanx and interpose the tendon of the EDL from dorsal, through the gap of the MTPJ to plantar and fix it on the plantar plate or to the flexor tendons (if the plantar plate is damaged) (Fig. 12.18). Surgical technique of the Stainsby procedure – step by step: (a) Skin incision is made longitudinal dorsal with a v-shape above the MTPJ proximal to the distal metatarsal area (Fig. 12.17e). (b) Prepare the EDL tendons, cut the ext. digit. brevis tendon at the distal insertion, and cut the EDL tendon as proximal as possible (Fig. 12.19). Mobilize the EDL tendon until Fig. 12.16 (a) claw toe II and hallux valgus. (b) Same patient after sequential surgical procedure it is the distal insertion. Save the free portion in moistened gauze. (c) After performing the steps for the PIP fusion, usually necessary (steps 9–11, above), the base of the proximal phalanx is resected (Fig. 12.20). Now the gap at the MTPJ is larger. (d) With a mosquito-clamp the plantar plate is mobilized dorsally. If the plantar plate is damaged, mobilize (pull) the flexor tendons through this gap dorsally. The EDL tendon is interposed into the gap and fixed with a suture (vicryl 3–0) to the plantar plate or flexor tendon in a moderate, soft tension (Fig. 12.21). (e) Now continue with step 7A for finishing the surgical procedure (Fig. 12.22). (f) Sometimes it is necessary to perform a subcapital closing wedge osteotomy of the metatarsal bone for elevating and shortening the metatarsal. (See step 11B-II, below). 116 A. Simon a b c d e Fig. 12.17 (a) Rheumatory deformity of the lesser toes. (b) Lesser toe deformity; frontal view. (c) X-ray dp, rheumatory deformity of lesser toes. (d) X-ray lateral view, luxated lesser toes at rheumatory arthritis. (e) Skin incision, Stainsby procedure The result of the Stainsby procedure is an interposition arthroplasty of the MTPJ with dynamic stabilization. The advantage in rheumatoid arthritis is to preserve the metatarsal head. Sometimes it is necessary to correct all lesser toes (Fig. 12.23). II. Propulsion- or Transfer-metatarsalgia. The metatarsal bone, regarding the alignment of the length of all metatarsals, is too long (in case of a painful propulsion) or plantarized (in case of a painful weight-bearing while standing). A subcapital dorsal wedge osteotomy will elevate and 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity Fig. 12.18 Cutting the ext. digit. lg. tendon as proximal as possible Fig. 12.19 Resection of the base of the proximal phalanx 117 shorten the metatarsus. In some severe claw toe deformities it is necessary to shorten the metatarsal bone, otherwise the reposition of the subluxed ray is not possible, though the steps before have released and relaxed the deformity. In these cases, where the soft tissue is not able to tolerate a distraction for a straight position of the ray, the shortening osteotomy is successful. If the goal of the osteotomy is to elevate the metatarsal head, the direction of the bone cut should be in a correct position being sure to elevate and not plantarize the metatarsal head. If the osteotomy is too steep to the weight-bearing surface, the subcapital oblique cut from dorsal distal to proximal plantar cannot elevate the head. Shifting the metatarsal head proximal may plantarize the metatarsal head. It is difficult to bring the saw blade to a transverse position such that angulating the cut proximally will elevate the head. The complication of an oblique cut is plantarizing the head. With this failure more painful pressure is produced to the head than before surgery. This can lead to a floppy toe. Because of the difficulty with this osteotomy, it is easier and more secure to perform a second cut, less oblique, called a closing wedge osteotomy (Fig. 12.24). Fixation is performed with a cannulated screw (2.0 mm), from proximal dorsal to distal plantar, self-drilling and self-cutting (Fig.12.25). More complicated is a twist off screw, which could break off in the bone or disconnect, before reaching the final insertion. III. Flexor tendon contracture. The imbalance between flexor and extensor tendons and the weakness of the lumbricales and Interossei produce this deformity. With the transfer of the flexor digit, longus tendon a balance can be restored to avoid the pathologic dorsalflexion of the proximal phalanx. With a little transversal plantar incision below the distal interphalangeal joint the tendon is identified with a moskito clamp and cut. In the gap of the opened metatarsophalangeal joint the tendon can be harvested between the tendons of the flexor digit, brevis, laying in the middle. Pulling the distal cut flexor digit, longus tendon dorsally, the tendon is split longitudinally and both sides are bent from plantar to dorsal around the 118 Fig. 12.20 (a) Suture of the ext. digit. lg. tendon. (b) Interposition of the ext. digit. lg. tendon plantarside A. Simon a a Fig. 12.21 (a) Pin fixation after tendon interposition. (b) Interposition of the ext. digit. lg. tendon b b 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity 119 position. A small bandage, keeping the distal phalanx in the straight position is useful for 2 weeks. The flexor tenotomy procedure is very useful in diabetic patients to avoid ulcerations of the tip of the toe. Local anesthesia is not needed for neuropathic diabetic patients. Partial weight-bearing is allowed in a special shoe with a hard insole for 5 weeks, to protect the position of the pins (K-wires). K-wire removal is done after 5 weeks. Local anesthesia normally is not needed. Physiotherapy is performed after removal of the pins, taking care that the PIP-fusion should not be moved or bent. Only the MTPJ needs some exercises in dorsi- and plantarflexion. For the passive movement the toe must be stabilized at the proximal phalanx and not at the middle phalanx because of the PIP-fusion. 12.5.3.2 Rigid Deformity To correct the rigid flexion contracture of the DIPJ, it is necessary to perform a fusion in a rectus position. The dorsal skin incision should be curved like a hockey stick, protecting the region of the nail and preserving the vessels and nerves. The extensor digitorum longus tendon is transversely incised. The DIPJ is exposed by further resecting the collateral ligaments, removing cartilage of both bones, just with minimal transversal resection with a small saw blade. Cancellous bone should be exposed. Next the view to the gap on the plantar capsule is possible. The capsule should be opened and the flexor tendon is tenotomized. Fusion with a double-ended K-wire is performed as with PIPJ hammertoe surgery. Forward (antegrade) drilling of the k-wire is performed from the distal phalanx through the tip of the toe and then backward (retrograde), through the middle and proximal phalanx, holding the toe in a rectus position. Penetrating the MTPJ should be avoided (unless MTPJ deformity needs to be stabilized). The tendon of the extensor digitorum longus is sutured. The skin can be closed with resorbable or nonresorbable material. The K-wire is removed after 4 weeks. 12.5.3 Mallet Toe Deformity: Performance of the Surgical Procedure 12.6 Fig. 12.22 Schematic of the Stainsby procedure diaphysis of the proximal phalanx, preserving vessels and nerves. “The ends are sutured dorsally to eachother and to the extensor tendon in a mild tension, while the MP-Joint is fixed in 20° plantarflexion and the ankle joint in neutral position”9 (Fig. 12.26). This surgical procedure is completed as in step 7A (above). 12.5.2 Postoperative Care 12.5.3.1 Flexible Deformity The treatment usually involves a simple flexor tenotomy. Flexor digitorum longus tenotomy is a minimally invasive, percutaneous technique: Using a large gauge needle (16 or greater), insert plantarly at the joint line of the DIPJ exactly in the middle of the toe. This location avoids injuring the vessels and nerves medially and laterally. Palpating the tendon with the tip of the needle, move or carefully advance the needle 3mm to the left and right, like a windshield, holding the distal phalanx in the most extended position as possible. The sharp tip of the needle will cut the tendon. The result is the relaxed distal phalanx in rectus Author’s Experience 12.6.1 Skin Incision The v-shape above the MTPJ might avoid a contracting skin scar, which may cause recurrence of the dorsiflexion deformity of the proximal phalanx (floppy toe, nonpurchasing toe). 12.6.2 PIP-Fusion The typical, well-known Hohmann/Post procedure (proximal phalangeal head resection) did not consider removal of the cartilage at the base of the 120 a A. Simon b c Fig. 12.23 (a) Stainsby procedure performed at the right foot (see patient like in figure 12:17a, b, c, d). (b) Stainsby, same patient frontal view (right foot). (c) X-ray after removing K-wires 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity a b c d 121 Fig. 12.24 (a) First oblique cut in subcapital region. Second cut less oblique (b). Wedge removed (c). Reduction of osteotomy with McGlamry elevator (d) middle phalanx. This is an important reason why the correction of the deformity could not succeed. The fusion of the PIPJ, which is stabilizing the toe in a straight position needs the same condition for a fusion as with any other fusion of two bones. To avoid a painful nonunion it seems to be more secure to remove the cartilage of the base of the middle phalanx (Fig. 12.10). Additionally cartilage removal can prevent a rotational failure and a nonunion if the surfaces of the connecting bones have a three-dimensional formation, like a saddle roof at the middle phalanx and a v-shaped gutter at the proximal phalanx (“cup” and “cone”) (Fig. 12.27). In my opinion the peg-and-hole arthrodesis2 is quite difficult to perform because the K-wire may damage the peg; it can also fracture at osteoporotic bone. Finally after the temporary longitudinal fixation of the toe with the K-wire, be sure that the surfaces of the PIP area fits together like press fit, without any gap. On the contrary, the gap of the MTPJ should be fixed in distraction to support the release of the capsule (Fig. 12.14b). 12.6.3 MTPJ Release The recurrence of the deformity in hyperdorsiflexion of the MTPJ may happen if the MTPJ has not been released and the permanent dorsiflexion of the phalanx will continue. Every fiber of the capsule and collateral ligaments must be opened if there is a contracture of these structures. The push up test is essential. To release the plantar plate, the McGlamry elevator is very useful because of the formation of this instrument, but take care that the cartilage is not damaged with its sharp tip. Remember that the head has a large flare plantarly. 122 A. Simon 1 a 2 Fig. 12.26 Schematic of lateral view of extensor lengthening (1) and flexor transfer (2) with Girdlestone technique9 b Fig. 12.25 (a) Fixation with 2.0 cannulated screw. (b) X-ray of the closing wedge metatarsal osteotomy, II–V. ray 12.6.4 Fixation of the Ray (MTPJ Through PIP and DIPJ) Pay attention that, at the end of the procedure, the correct straight position of the toe does not produce too much distraction for the soft tissue. Otherwise the neurovascular structures may be stretched too much and may lose their function. In the worst case the toe will become necrotic. If the normal skin color and temperature does not recur after 2 h and the toe stays pale and Fig. 12.27 X-ray: bone formation for a secure PIPJ fusion cold, try to infiltrate the toe with a nitroglycerin; the arteries should vasodilate. If the toe maintains the hypoxia (Fig. 12.28a, b) after two nitroglycerin infusions, remove the K-wire to reduce the distraction. Now it is important to hold the toe straight with a bandage or soft tape, but likely the PIP fusion will not heal in a rectus position. Nevertheless it is better than producing the worst complication: a necrotic toe which has to be amputated. 12 Surgical Treatment of Hammer Toe, Claw Toe, and Mallet Toe Deformity a 123 plate is about 1 cm long. Rolling this end in the joint gap around the K-wire after drilling the K-wire, which is transarticular fixing the ray, supports to maintain the gap as an additional interposition. 12.6.6 Metatarsal Osteotomy It is useful to locate the joint line of all MTPJs with a needle. Mark it intraoperatively, into the joint gap, in the sagittal plane. If more than one ray shall be corrected, it is important to maintain the physiological alignment of the length of the metatarsal bones which helps to avoid the recurrence of a propulsion metatarsalgia. b Fig. 12.28 (a) Situation pre-op: normal perfusion; (b) post-op: hypoxia of the second toe 12.6.5 Stainsby Procedure The proximal free end of the extensor digit, longus. tendon after interposing it and suturing it to the plantar References 1. Simon A. Korrektur der Hammer-und Krallenzehenfehlstellungen: Ambulant Operieren. 2007;14:24-29. 2. Mc Glamry ED. Lesser ray deformities. In: Mc Glamry ED, Banks AS, Downey MS, eds. Comprehensive Textbook of Foot and Ankle Surgery, vol. 1. 3rd ed. Baltimore: Lippincott Williams & Wilkins; 2001:253-304. 3. Stainsby GD. Pathologic anatomy and dynamic effect of the displaced plantar plate and the importance of the integrity of the plantar plate-deep transverse metatarsal ligament tie-bar. Ann R Coll Surg Engl. 1997;79(1):58-68. 4. Hansen ST. Tendon transfers and muscle-balancing techniques. In: Hansen ST, ed. Functional Reconstruction of the Foot and Ankle. Philadelphia: Lippincott Williams & Wilkins; 2000:455-458. 5. Döderlein L. Pathomechanik des Ballenhohlfußes. In: Döderlein L, Wenz W, Schneider U, eds. Der Hohlfuß. Berlin: Springer; 2000. 6. Kitaoka HB. Realignment of lesser toe deformities. In: Kitaoka HB, ed. The Foot and Ankle. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2002:147-170. 7. Niezold D, Ferdini M. Klinische untersuchung. In: Wirth CJ, ed. Orthopädie und Orthopädiche Chirurgie. Fuß. Stuttgart: Thieme; 2002:9-19. 8. Chang TJ. Lesser digital surgery: arthroplasty, arthrodesis and flexor tendon transfer. In: Chang TJ, ed. Master Techniques in Podiatric Surgery: The Foot and Ankle. Philadelphia: Lippincott Williams & Wilkins; 2005:35-48. 9. Walsh HPJ. Kleinzehendeformitäten: transfer der beugesehne und weichteilrelease des metatarsophalangealgelenkes. In: Wülker N, Stephans M, Cracchiolo A III, eds. Operationsatlas Fuß und Sprunggelenk. Stuttgart: Enke; 1998:85-92.









© Copyright 2025