
Welcome to SPRC’s Research to Practice Webinar on Understanding Nonsuicidal Self-Injury in
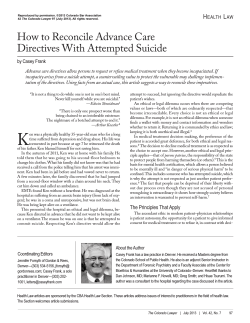
Welcome to SPRC’s Research to Practice Webinar on Understanding Nonsuicidal Self-Injury in Suicide Prevention You are muted and will not hear anything until the moderator begins the session. If you are experiencing technical difficulties, please call 307-GET-WEB1 (307-438-9321) or email webinar@sprc.org Expand control panel Raise hand Call-in for audio Enter question during Q&A Understanding Nonsuicidal Self-Injury in Suicide Prevention Morton M. Silverman, M.D. Suicide Prevention Resource Center Barent Walsh, Ph.D. The Bridge of Central Massachusetts 4 Nonsuicidal Self-Injury: An Introduction and Perspective Morton M. Silverman, M.D. Senior Advisor Suicide Prevention Resource Center Newton, MA SPRC R2P Webinar July 27, 2010 A Perspective Terms in the Literature: • Self-Harming Behaviors (SHB) • Self-Mutilative Behaviors (SMB) • Self-Injurious Behaviors (SIB) SIB = refers to a broad class of behaviors in which an individual directly and deliberately causes harm to him/herself Self-Injurious Behaviors (SIB) 2 Types of SIB: • Nonsuicidal Self-Injury (NSSI) • Suicide Attempts (SA) NSSI = direct, deliberate destruction of one’s own body tissue in the absence of intent to die SA = direct efforts to intentionally end one’s own life Associations and Correlations, but not Necessarily Causations • There are theoretical, methodological, and clinical differences among various forms of SIB • However - these behaviors are related, interactive, and can co-occur within individuals • Hence - these behaviors may well lie along a continuum of self-harming behaviors Some Similar Risk Correlates • • • • • Emotional regulation skills Problem-solving skills Communication problems Impulsivity Unstable interpersonal relationships The Relationships between NSSI and Suicide Attempts (SA) • NSSI is a risk factor for subsequent suicidal behaviors • NSSI is similar to suicidal ideation in conferring increased risk for SA • NSSI can be mistaken for SA - and vice versa • Some individuals report both NSSI and SA • NSSI and SA commonly co-occur - especially in adolescents Relevance to Joiner’s Theory • Joiner’s Theory suggests that habituation to fear and physical pain, such as that associated with suicidality, increases the desire and the capability to engage in lethal self-injurious behaviors • Hence….repeated episodes of NSSI may increase the risk for subsequent SAs and death by suicide Joiner TE (2005). Why People Die by Suicide. MA: Harvard University Press Implications for Suicide Prevention • The prevention of SIB (NSSI and SA) addresses similar psychological, emotional, cognitive, and interpersonal factors • Plus…..by preventing NSSI, the expected outcome would be a reduction in subsequent suicidality Goals of This Webinar • What is NSSI? - similarities/differences to SA • How is NSSI a risk factor for suicide? • How do you intervene with NSSI? • How do you prevent NSSI in high schools? • How do you evaluate prevention outcomes? Understanding Nonsuicidal SelfInjury in Suicide Prevention Barent Walsh, Ph.D. Executive Director The Bridge of Central Massachusetts, Inc. 4 Mann Street Worcester, MA 01602 Phone: 508-755-0333 email: barryw@thebridgecm.org Thanks to: • Jennifer Muehlenkamp, PhD, University of Wisconsin-Eau Claire • Candice Porter, MSW, Screening for Mental Health -- for their contributions to the High School Prevention Program And to: • Morton Silverman, M.D. • Tiffany Kim & Xan Young, Suicide Prevention Resource Center -- for their contributions to this presentation… Differentiating Suicide from NSSI Suicidal Behavior NSSI Prevalence In U.S., 10 deaths by suicide per 100,000 in population Unclear; estimates from 400 to 1400 per 100,000 Intent Permanently end psychological pain; terminate consciousness Temporarily modify emotional distress; effect change in others Lethality of Method High lethality: gunshot, hanging, O.D., jumping, ingesting poison Low lethality: cutting, self-hitting, burning, picking, abrading Differentiating Suicide from NSSI Suicidal Behavior NSSI Cutting as a method for suicide vs. NSSI Almost no one dies by cutting: All ages: .2% of suicides die by cutting; For 15-24 year olds: .6%; For 25-34 year olds: 1.5% Cutting is the most common NSSI method almost universally in both community & clinical samples Frequency Low rate behavior even in severely mentally ill persons Frequently high rate: scores of episodes per person Number of methods Repeat attempters generally employ one method, often overdose In both community & clinical samples, most use multiple methods; e.g. Whitlock (2008) 78% Differentiating Suicide from NSSI Suicidal Behavior Ideation Suicidal ideation predominates; less positive Reasons for Living and Attraction to Life (Muehlenkamp 2010) NSSI Suicidal ideation infrequent; concerning when present; more positive RFL and AL Cognition & Affect Helplessness and hopelessness predominate; poor problem solving Helplessness and hopelessness less likely as long as NSSI “works”; more intact problem solving Aftermath Immediate relief; reduction in negative affect Continued despair; often high lethality Differentiating Suicide from NSSI Reaction of others Suicidal Behavior NSSI Most others express concern and support; move towards protection Ongoing NSSI may be condemned, judged negatively; therapyinterfering behaviors are common (aka counter-transference) Restriction of means? Often an important preventive intervention Often ill-advised, counterproductive Cautionary Notes: SelfInjury vs. Suicidal Behavior • While self-injury is generally not about ending one’s life, NSSI is a risk factor for suicidal behavior. • It is important to emphasize that while the behaviors are distinct, both can occur within the same individual. The Relationship between Suicide Attempts & NSSI • NSSI is associated with Suicide Attempt Risk when the following are present: - Higher levels of suicidal ideation Severity of depression Diagnosis of Borderline Personality Disorder Impulsivity Greater levels of negative affect Apathy & hopelessness Self-derogation/lack of self-acceptance Brausch & Gutierrez (2009); Muehlenkamp (2010) Relationship Between NSSI and Suicide Attempts What to Watch For… • Severity and duration of NSSI • NSSI becoming less effective in reducing emotional distress • Worsening mental health symptoms Protective Factors • Family connectedness, support • Peer social support Brausch & Gutierrez (2009) Muehlenkamp (2010) More on the Relationship between Suicide Attempts and NSSI Klonsky (2010) reported in a recent study of 428 high school students: • NSSI - 6% • Suicide Ideation - 17% • Attempted Suicide - 3% Rates of attempted suicide among those who had: • NSSI • Suicide Ideation 27% 18% Relationship to Attempted Suicide Adolescent inpatients (n = 171) • • • • • • Suicide Ideation NSSI Borderline Personality Emotion Dysregulation Impulsivity Loneliness Klonsky (2010) .55 .50 .39 .34 .11 .09 Conclusion re: Suicide and NSSI NSSI is substantially different from suicide, yet NSSI is a strong risk factor for suicide • Good clinical practice suggests: - Understand, manage, & treat differentially - Carefully cross-monitor; assess interdependently - Intervene early with NSSI to prevent emergence of suicidality NSSI Demographics in the U.S. • In community samples, a range of 6 to 25 % of youth report self-injuring at least once • In clinical samples, more females report NSSI than males; In community samples, no gender difference • Age of onset for the majority is 13 to 15 • NSSI may be more common among Caucasians & GLBTQ youth (Nixon & Heath, 2008) • Females may be more likely to cut or pick; Males may prefer self-hitting, punching walls (community sample, Whitlock 2008) More U.S. Demographics • Data from the 2007 Massachusetts Youth Risk Behavior Survey (YRBS) indicated that 17% of high school students and 16% of middle school students reported having self-injured during the past year. • Also, a recent study from Cornell and Princeton Universities, using a sample of almost 3000 students, found that 17% indicated having self-injured (Whitlock et al. 2006b). -- And in a follow-up study involving 8 colleges and more than 11,000 students, Whitlock (2008) found that 15.3% reported some NSSI lifetime; 29.4% reported more than 10 episodes Therefore…. Given the increased prevalence of NSSI in the general population… And its role as a risk factor for subsequent suicidality…. We developed a self-injury prevention program for high school staff and students Program Components • • • • • • Signs of Self-Injury DVD (SOSI) Self-assessment form for students Lesson plan and discussion guidelines for teachers Lecture for staff training Guidelines for planning a parent training Templates for educational and communication materials for staff, parents, and students • Self-Injurious Thoughts and Behaviors Interview (SITBI) assessment forms for school clinicians (Nock et al. 2007) Program Goals • Decrease NSSI by teaching students more adaptive coping skills • Decrease self-injury by educating students and the school community about risk factors, clinical implications, and outcomes associated with selfinjury. • Encourage help-seeking among students – either for themselves or on behalf of a friend. • Help school staff make the key distinction between self-injury and suicide. Program Goals (continued) • Engage parents and school staff as partners in prevention - teach them to identify and respond to signs of self-injury. • Encourage schools to develop a school protocol for responding to self-injury that is strategic, compassionate, and effective. EDUCATION about Self-Injury DVD (2 chapters) Discussion Guide •Emphasizes NSSI is treatable Provides basic NSSI info •Models appropriate responses Provides discussion guidelines •Encourages help seeking BEHAVIOR • Acknowledge (the signs) • Care (express concern) • Tell (a trusted adult) RISK ASSESSMENT • Student assessment tool • Clinician assessment tool (SITBI) •Referral to Treatment as needed “Signs of Self-Injury” DVD • The 29 minute DVD is the main teaching tool. • Includes 2 chapters - 1 for students and 1 for staff. • Student chapter includes: - 3 dramatizations of students responding to NSSI with a friend and with a school guidance counselor - 2 demonstrate help-seeking behavior; 1 reviews how to avoid social contagion - a personal testimonial from a person who has recovered from self-injury (not an actor) • The DVD uses teen actors who model appropriate support and help-seeking behaviors (ACT message). The “Signs of Self-Injury: ACT® to Prevent Self-Injury Prevention Program” The DVD employs the Acronym ACT > Acknowledge that your friend has a problem and that self-injury is serious. > Care enough to let your friend know you want to help. > Tell a trusted adult about the self-injury. Implementing the Program for Students The program for students takes about 60 minutes. Some schools choose to employ 2 class periods or over 2 days. The steps include: • • • • • Introduction (5 minutes) DVD (18 Minutes) Discussion (20-30 minutes) Student Self-Assessment (10 minutes) Help-Seeking; Students complete a Response Card which allows them to request to speak with someone after the program (5 minutes) DVD Program Continued Staff chapter includes: • clinical information about NSSI • response guidelines, recommending the use of a “low key dispassionate demeanor” • A DVD chapter in which a guidance counselor demonstrates appropriate responses • Interviews with NSSI experts and school personnel who have dealt with NSSI in their schools • Guidelines for preventing social contagion of NSSI Implementing the Program For Staff Staff training takes about 1 – 1.5 hours. It includes: • Introduction; what SOSI is, who it targets; Reviewing myths vs. facts of NSSI • Viewing both chapters of the DVD, staff version & student version (29 minutes) • Reviewing the teaching points of the video • Developing a staff team to respond to NSSI • Reviewing a school protocol for handling students who disclose NSSI • Reviewing school and community health resources • Identify a point person that training participants can contact regarding future questions SOSI Outcome Data • 5 Schools; 282 students total • Pre-Assessment, Program, Post-Assessment • Assessment Tools - SITBI for NSSI thoughts, behaviors New Instrument that measures: - Knowledge of NSSI (11 items; = .93) - Attitudes • Discomfort with NSSI ( = .83) • Avoidance of peer NSSI ( = .77) • Approach/Helping Desires ( = .85) - Help-seeking behaviors Muehlenkamp et al. (2009) Outcomes for SOSI Program Evaluation 9 8 7 6 5 PRE 4 3 2 POST p < .001 p < .001 p < .08 1 0 Knowledge Discomfort Avoidance Help Desire NSSI Act SOSI Outcomes Conclusions • Improved attitudes in students towards acceptance & helping • No iatrogenic effects reported • Help seeking behaviors increased (but not significantly) • Feasibility Data = Very positive from school staff • NSSI acts declined (but not significantly) • Program has initial promise; more research needed For the full report, see: Muehlenkamp, J.J., Walsh, B.W. & McDade, M. (2009). Preventing non-suicidal self-injury in adolescents. Journal of Youth and Adolescence, 39, 306-314. For More Information on the SOSI Prevention Program Candice Porter at Screening for Mental Health, Wellesley, MA. E-mail: cporter@MENTALHEALTHSCREENING.ORG Phone: 781-239-0071 For questions and feedback regarding the webinar, please contact: Xan Young Project Director, Training Institute Suicide Prevention Resource Center, EDC xyoung@edc.org Tiffany Kim Project Coordinator, Training Institute Suicide Prevention Resource Center, EDC tkim@edc.org General References re: NSSI Alderman, T. (1997). The scarred soul: Understanding and ending self-inflicted violence. Oakland, CA: New Harbinger Press. Beck, J.S. (1995). Cognitive therapy, basics and beyond. New York: Guilford Press. Bohus, M., Limberger, M., et al. (2000). Pain perception during self-reported distress and calmness in patients with borderline personality disorder and self-mutilating behavior, Psychiatry Research, 95, 251-260. Foa, E.B., Keane, T.M. & Friedman, M.J. (Eds.). (2000). Effective treatments for PTSD. New York: Guilford Press. Gratz, K.L. & Chapman, A.L. (2009). Freedom from self-harm: Overcoming selfinjury with skills from DBT and other treatments. Oakland, CA: New Harbinger. Hayes, S.C., Follette, V.M. & Linehan, M.M. (Eds). (2004). Mindfulness and acceptance. New York: Guilford Press. Hollander, M. (2008). Helping teens who cut. New York: Guilford. Hyman, J. (1999). Women living with self-injury. Philadelphia: Temple University Press. General References re: NSSI Joiner. T. (2007). Why people die by suicide. Cambridge, MA: Harvard University Press. Joiner, T. (2010). Myths about suicide. Cambridge, MA: Harvard University Press. Keuthen, N.J., Stein, D.J. & Christenson, G.A. (2001). Help for hair pullers, Understanding and coping with trichotillomania. Oakland, CA: Harbinger Publications. Kettlewell, C. (1999). Skin game: A Cutter’s Memoir. New York: St. Martin’s Press. Klonsky, D. E. (2007). The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review, 27, 226-239. Linehan, M.M. (1993a). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford Press. Linehan, M.M. (1993b). Skills training manual for treating borderline personality disorder. Guilford. Miller, A.L., Rathus, J.H., & Linehan, M.M. (2007). Dialectical behavior therapy with suicidal adolescents. Guilford. General References re: NSSI Muehlenkamp, J. J. (2006). Empirically supported treatments and general therapy guidelines for non-suicidal self-injury. Journal of Mental Health Counseling, 28, 166-185. Nhat Hanh, T. (1975). The miracle of mindfulness. Boston, MA: Beacon Press. Nixon, M.K. & Heath, N.L. (2008). Self-injury in youth. New York: Routledge. Nock, M.K., Holmberg, E.B., Photos, V.I. & Michel, B.D. (2007). The SelfInjurious Thoughts and Behaviors Interview. Psychological Assessment, 19 (3), 309-317. Nock, M.K. & Kessler, R.C. (2006). Prevalence of and risk factors for suicide attempts versus suicide gestures: Analysis of the National Comorbidity study. Journal of Abnormal Psychology, 115(3), 616-623. Nock, M. K. & Prinstein, M. J. (2004). A functional approach to the assessment of self-mutilative behavior. Journal of Consulting and Clinical Psychology, 72(5), 885-890. Segal, Z.V., Williams, J.M.G. & Teasdale, J.D. (2002). Mindfulness-based cognitive therapy for depression. New York: Guilford. Shneidman, E.S. (1985). Definition of suicide. New York: John Wiley & Sons. General References re: NSSI Walsh, B. & Doerfler, L. (2009). Residential treatment of self-injury. In Nock, M. (Editor). Understanding non-suicidal self-injury: Origins, assessment, and treatment. Washington, DC: American Psychological Association. Walsh, Barent (2007). Clinical assessment of self-injury: A practical guide. Journal of Clinical Psychology: In Session, 63, 1057-1068. Walsh, B. (2006). Treating self-injury: A practical guide. New York: Guilford. Walsh, B. & Rosen, P. (1985). Self-mutilation and contagion: An empirical test. American Journal of Psychiatry, 142, 119-120. Walsh, B. & Rosen, P. (1988). Self-mutilation: Theory, research and treatment. New York: Guilford Press. Whitlock, J., Eckenrode, J., & Silverman, D. (2006b). Self-injurious behaviors in a college population. Pediatrics, 117(6), 1939-1948. Whitlock, J. L., Powers, J. L., & Eckenrode, J. (2006a). The virtual cutting edge: The internet and adolescent self-injury. Developmental Psychology, 42(3), 1-11. References re: the Relationship Between Suicide and NSSI & Demographics of NSSI Berman, A.L., Jobes, D.A. & Silverman, M.M. (2006). Adolescent suicide: Assessment and Intervention (2nd ed.) Washington, DC: American Psychological Association Brausch, A. M. & Gutierrez, P. M. (2009). Differences in non-suicidal self-injury an suicide attempts in adolescents. Journal of Youth and Adolescents, 39 (3), 233-242. Centers for Disease Control and Prevention (2009). Web-based Injury Statistics Query and Reporting System (WISQARS). Available from www.cdc.gov/ncipc/wisqars/default.htm. Heath, N. L. et al. (2008). Self-injury today: Review of population and clinical studies of adolescents. In M.K. Nixon & N.L. Heath (eds.). Self-injury in youth: The essential guide to assessment and intervention. New York: Routledge. Klonsky, E.D. (2010). The Relationship Between Non-Suicidal Self-Injury and Attempted Suicide in Three Samples. Panel session at the Annual meeting of the American Association of Suicidology, Orlando, FL. References re: the Relationship Between Suicide and NSSI & Demographics of NSSI Klonsky, E.D. & Muehlenkamp, J.J. (2007). Non-suicidal self-injury: A research review for the practitioner. Journal of Clinical Psychology/ In session, 63, 1045-1056. Massachusetts Department of Elementary and Secondary Education (2008). Health and risk behaviors of Massachusetts youth: The report. available at: http://www.doe.mass.edu/cnp/hprograms/yrbs Muehlenkamp, J.J. & Kerr, P.L. (February 2010). Untangling a complex web: How non-suicidal self-injury and suicide attempts differ. The Prevention Researcher, Volume 17(1), 8-10. Muehlenkamp, J.J. & Gutierrez, P.M. (2007). Risk for suicide attempts among adolescents who engage in non-suicidal self-injury. Archives of Suicide Research, 11, 69-82. Muehlenkamp, J.J. (April 2010). Evidence-based approaches to nonsuicidal self-injury. Day long pre-conference workshop with Barent Walsh. Annual meeting of the American Association of Suicidology, Orlando, FL. References re: the Relationship Between Suicide and NSSI & Demographics of NSSI Nock, M.K., Joiner, T.E., Gordon, K.H., Lloyd-Richardson, E. & Prinstein, M. (2006). Nonsuicidal self-injury among adolescents: Diagnostic correlates and relation to suicide attempts. Psychiatry Research, 144, 65-72. Rodham, K. & Hawton, K. (2009). Epidemiology and phenomenology of nonsuicidal self-injury. In Nock, M.K. Understanding non-suicidal selfinjury: Origins, Assessment, and Treatment. Washington, DC: American Psychological Association. Skegg, K. (2005). Self-harm. Lancet, 366, 1471-1483. Walsh, B.W. (2006). Treating self-injury: A practical guide. New York: Guilford Press. Whitlock, J., Eckenrode, J., & Silverman, D. (2006b). Self-injurious behaviors in a college population. Pediatrics, 117(6), 1939-1948.





© Copyright 2025