
IVUS-OCT QUANTIFICATIONS: WHAT TO MEASURE AND HOW TO DO IT?
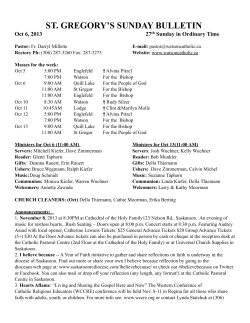
IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA N. 1• 2011 IVUS-OCT QUANTIFICATIONS: WHAT TO MEASURE AND HOW TO DO IT? Vasile Sirbu, Giuseppe Musumeci Cardiovascular Department, Cardiologia 2, Diagnostica Interventistica, Ospedali Riuniti di Bergamo Invasive coronary angiography has been the gold standard during the past 50 years for establishing the presence, location, and severity of epicardial coronary artery lesions. It has the great merit in bringing back the atherosclerotic pathology to one single parameter easy to be managed: the severity of stenosis. OCT, and IVUS are invasive intracoronary imaging techniques. Both use the delay time of echoes, IVUS directly ultrasound echo, and OCT indirectly-optical echo using the technique known as interferometry. IVUS has good penetration in tissue allowing the visualization of the so called “far field”, OCT has high luminal resolution, and permits to analyze in detail the “near field” (Figure 1). The combination of these techniques brings complementary information. Both of them allow data quantification, and reporting in a standard accepted way. Measurements in OCT and IVUS can be divided in qualitative, and quantitative, can be performed pre procedure, post stent implantation, and in follow-up to assess the vessel response to either stent implantation or medicamentous treatment. The analysis of the intracoronary images starts with the quality screening. During this initial process frames with poor quality are excluded from further analysis. The reason to exclude a frame from OCT analysis are: a large arc of the image is out of the screen or a side branch occupied >45° of the cross-section, this usually happens when large diameter vessels (>4 mm) are present in the scanned segment. Poor image quality can be caused also by residual blood or artifacts. Large vessels, and blood presence is not affecting the quality of IVUS scan. Motion artifacts can decrease the accuracy of measurements. Some of them are common in both OCT and IVUS, and others are unique in OCT imaging systems(1). No uniform rotational distortion “NURD” - focal image loss or shape distortion, and “sew-up” artifact the result of rapid artery or imaging wire movement in 1 frame’s imaging formation, leading to single point misalignment of the lumen border are common for both IVUS and OCT. Artifacts specific for OCT are more numerous. Some of them like “saturation artifact” signals with amplitudes that exceed the dynamic range of the data acquisition system produced by reflected light or “bubble artifact” attenuation of the signal along a region of the vessel wall caused by small air bubbles in the sheath of the ImageWireTM, “sunflower effect” or “merry-go-round artifact” caused by eccentricity of the ImageWire in the vessel lumen does not affect grossly the image interpretation or quantifications. Others like “fold-over” artifact- the consequence of the “phase wrapping” along the Fourier transformation when structure signals are reflected from outside the system’s field of view or NURD requires frame removal from subsequent analysis (Figure 2). No consensus agreement is present in the literature regarding the “ideal” interval of OCT analysis. It can be performed at different intervals along the scanned segment, ranging approximately from 0.06 mm up to 1 mm. Continuous assessment of every frame is not recommended because cardiac dynamics introduces forward and backward longitudinal displacement of the image wire, a phenomenon that can cause the “persistence” of Corresponding author: Dott. Vasile Sirbu Cardiovascular Department - Cardiologia 2 - Diagnostica Interventistica - Ospedali Riuniti di Bergamo Largo Barozzi, 1 - 24128 Bergamo (BG) - Italy Tel. +39.035.266455 - Fax +39.035.400491 - Cell. +39.320.7722456 - E-mail: dr_sarbu@yahoo.com 39 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA N. 1• 2011 B A C D Figure 1. Very late stent thrombosis. Corresponding angiographic (A), IVUS long-view reconstruction (B), OCT cross-sectional images (C, D) obtained after thrombus aspiration. IVUS has good tissue penetration and allows visualization of the positively remodeled vessel, OCT has high luminal resolution and permits to analyse in detail the presense of coverage, stent apposition and thrombus classification. A B C D E Figure 2. Most common artifacts in OCT. A: out of screen”; B: blood contamination; C: “fold-over” artifact; D: “bubble” artifact; E: “saturation” artifact. Residual blood attenuates the OCT signal. Saturation artifact occurs when light reflected from a highly specular surface, such as stent struts, produces signals with amplitudes that exceed the dynamic range of the data acquisition system. Fold-over artifact is more specific to the new generation of FD-OCT. It is the consequence of the “phase wrapping” or “alias” along the Fourier transformation when structure signals are reflected from outside the system’s field of view. Bubble artifact occurs when small air bubbles are formed in the sheath of the ImageWireTM (LightLab Imaging, Inc. - Westford, MA, USA), and it can attenuate the signal along a region of the vessel wall. the previous frame image in the current frame. Conversely, large intervals are to be avoided since strut coverage or malapposition may occur in clusters. Shorter intervals were adopted by our group to improve the sensitivity of the method, and minimize the variability of strut-level response(2). Both in IVUS, and in OCT analysis can be performed on frame, segment or vessel level. On the frame level vessel morphology and stent vessel interaction can be analyzed. 40 Vessel morphology allows detection of the amount, and the characteristics of the pathology. The criteria for plaque characterization in both systems are based on signal interpretation, and are present for 10 years for IVUS, and recently published for OCT(3,4). A higher sensitivity and specificity of OCT for tissue characterization of coronary plaques compared to integrated backscatter IVUS, and conventional IVUS for fibrous, calcium, and lipid pool has been reported(5) (Figure 3). Still, IVUS is more IVUS-OCT QUANTIFICATIONS: WHAT TO MEASURE AND HOW A B C D E F G H I J TO DO IT? Figure 3. Coronary plaques seen by OCT. A: normal vessel wall is characterized by a layered architecture, comprising high backscattering or signal-rich intima (thin), a media that frequently has low backscattering or is signal-poor, and a heterogeneous and sometimes highly backscattering adventitia. With OCT, the internal elastic membrane (IEM) is defined as the border between the intima and media and the external elastic membrane (EEM) is defined as the border between the media and the adventitia). OCT measurement of intimal thickness, which is the early phase of coronary atherosclerosis, is well correlated to histological examination; B: atheroma from 6 to 13 o’clock with homogeneous signal backscattering; C: microvessels that supply blood to atheroma (arrow); D: fibrous plaque has high backscattering and a homogeneous OCT signal (arrow); E: fibrocalcific plaque calcific at 1-3 o’clock: fibrous tissue and calcium characterized as a signal-poor that has a sharply delineated border; F: thick cap fibroatheroma and, a thick cap (>65 µm) (arrow) with signal attenuation due to necrotic core behind characterized by a fast optical signal dropoff and little backscattering within the lesion; G: thin cap fibroatheroma, a delineated necrotic core with an overlying fibrous cap with thickness less than 65 µm and signal attenuation behind due to necrotic core. The bright points of signal enhancement suspect colonies of phoamy cells. Multiple studies demonstrate these lesions are more commonly found at the culprit site in patients with ACS and AMI; H: ruptured thin cap fibroatheroma identified by a presence of fibrous cap discontinuity and(red arrow) a cavity formation within (asterix), thrombus deposition on top (white arrow); I, J: thrombus identified as abnormal mass protruding into the lumen, with signal backscattering and various degrees of attenuation. White thrombi were characterized by signal rich and low-backscattering projections protruding into the lumen (arrows). Sometimes them may be sufficiently large to obscure the underlying rupture site or luminal defect (J). able to quantify plaque volumes, and phenomenon of positive vessel remodeling (Figure 4). A correlation between the presence of positive vessel remodeling in IVUS, and higher number of TCFA in OCT in the examined vessel was found(6). Information about preprocedure plaque type can have prognostic implications. OCT, and IVUS can visualize features related to the culprit lesion such as plaque rupture, and subsequent thrombosis(7,8). Identification of the high-risk plaque for distal embolization remains a challenge during coronary interventions, and tissue characterization might give unique information in this scenario. The amount of lipid content is correlated to the “no reflow phenomenon” in acute coronary syndrome (ACS)(9). Information about calcium content, and distribution can help in planning plaque preparation, and debulking techniques(10). Pathology studies performed the late 1990s have changed the primary focus for heart attack prevention from coronary stenosis to coronary vulnerable plaquethin cap fiboatheroma (TCFA), and TCFA rupture. A hypothesis that measurements of plaque volume or composition may provide indices that would serve as useful surrogates for subsequent clinical events was proposed(11). Recently softwares performing spectral analysis of ultrasound backscattered data were implemented into conventional IVUS systems. These software facilitate the interpretation tissue components, and allow quantification of the morphological findings like the percent of necrotic core, lipid burden, and calcium extent in the examined vessel (Figure 5). Some limitations of IVUS tissue characterization should be acknowledged: the plaque components identified by each system vary, and a uni41 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA N. 1• 2011 A B C D Figure 4. IVUS calculations. IVUS has good tissue penetration and allows visualisation of external vessel border and thus permits quantification of plaque volume. A: long view reconstruction of a stented coronary in follow-up with evidence of sever positive remodeling that accompanies only the stent and not the rest of the vessel (arrow); B: distal reference segment showing a calcific plaque from 6 to 8 o’clock (arrow); C: stented segment with quantifications of extenal elastic membrane (arrow), stent and lumen CSAs; D: proximal reference segment showing a fibrotic plaque from 3 to 7 o’clock (arrow). form color codification is lacking, and thrombus is not recognized by the encoding algorithms. Two different approaches are present in determination of the lesion responsible for acute coronary events, TCFA: IVUS uses the amount of necrotic core, and plaque volume, and OCT uses the cap thickness (Figure 6). In intravascular imaging a ruptured plaque is identified by a presence of fibrous cap discontinuity, and a cavity formation within(12). Serial examination of vessel morphology, evaluating the progression/regression of specific atheroma features under lipid-lowering therapy, demonstrated significantly increase in fibrous-cap thickness by OCT follow-up(13), and reduced amount of necrotic core, and plaque volume, using IVUS(14). Thrombus is frequently identified in target lesions, and depending on its composition is classified on white, and red with respective optical characteristics in OCT. Red thrombi have OCT appearance as high-backscattering protrusions inside the lumen, with signal-free shadowing. White thrombi were characterized by signal rich, 42 and low-backscattering projections protruding into the lumen(15). Thrombus can also be visualized in IVUS if appropriate enhancement techniques are applied, but no classification on thrombus type is present (Figure 7). Both systems are valuable in detecting the morphometric characteristics of the vessel as minimum vessel diameters, and areas, reference segments, stenosis quantification. (Figure 4, 5). The parameters regarding post stent implantation evaluation are apposition to the vessel wall, the minimum, and maximum stent diameters, and areas as well as derived indexes as stent expansion, and simmetricity. The incomplete stent apposition (ISA) can be evaluated by calculating the fraction of the lumen area outside the stent cross-section area (CSA). A number of derived morphometric measurements are usually presented: the minimum stent CSA divided by the average of reference lumen CSA ratio is usually calculated as a parameter of stent expansion, while the minimum stent diameter divided by maximum stent diameter as a parameter of stent simmetricity. While during BMS era it was impor- IVUS-OCT QUANTIFICATIONS: WHAT tant to maximize the final result due to the important late-loss, nowadays, while using DES, concerns regarding stent thrombosis has focused attention on optimal stent deployment(16,17). Using OCT, a more detailed evaluation of the vessel TO MEASURE AND HOW TO DO IT? response to injury after implantation like tissue protrusion, edge dissection, residual reference segment stenosis“geographic miss”, and residual thrombus (Figure 9). Metal stent struts are opaque, and act for light as a mirror, thus only the luminal surface of individual struts is Figure 5. IVUS tissue characterization softwares. The software uses post processing of the backscattered radio frequency IVUS signal in order to characterize plaque composition. The iMap by iLab System Software (Boston Scientific Corp) does tissue characterization based on pattern recognition and integrated backscattered ultrasound signals. Values are calculated as average power of the backscattered signal using a fast Fourier transformation. 43 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA A C N. 1• 2011 B D E Figure 6. Thin Cap Fibro Atheroma in OCT. A: evidence of TCFA with cap thickness of 60 µm (arrow); B: TFCA erosion with evidence of discontinuity of thin cap and connection of the cavity with lumen of the vessel (arrow); C: distal and proximal (E) reference segments. The site with the largest lumen proximal to a stenosis but within the same segment (usually within 10 mm of the stenosis with no major intervening branches). Reference segments with large CSAs; D: segment containing TCFA with intermediate narrowing of lumen area and stenosis of 30%. visualized by OCT. The opacity of metal struts causes a shadow that obscures deeper structures within the vessel wall(18). Strut apposition to vessel wall was classified in protruding, where the strut boundary is located above the level of the luminal surface, and embedded, where the strut boundary is below the level of the luminal surface(1). ISA-separation of the stent strut from the lumen border by a distance greater than the width of the stent strut according to each stent specification, plus a compensation factor of 20 µm to correct for “strut blooming” 44 according to some authors or resolution of the current OCT technology to the others(19,20). In case of data analysis by independent core laboratory, a blinding of the operator to the treatment assignment is usually performed. To allow this the OCT calculations are stored in an integrated database system, and corrected for strut (polymer) thickness of different stent types after the data analysis is completed(21). A relatively high proportion of malapposed struts after stent deployment were reported in regions of stent overlap, and severe calcified lesions(22). IVUS-OCT QUANTIFICATIONS: WHAT TO MEASURE A B C D E F AND HOW TO DO IT? Figure 7. IVUS and OCT visualisation of stented coronary artery. Corresponding IVUS (A-C) and OCT (D-F) cross-sections of a stented coronary artery in follow-up. OCT has a higher capacity in evaluating the thin coverage (D vs A); both techniques are able to detect large degrees of stent malapposition but IVUS has the possibility to evaluate the EEM (B vs E); large amount of thrombus can be equally detected by IVUS, and OCT when special enhansement procedures (blood removal by contrast medium) (C vs F). Tissue protrusion is defined as a tissue prolapse between stent struts extending inside a circular arc connecting adjacent struts(23). During primary percutaneous coronary interventions (PCI) thrombus is easily visualized by OCT, and can protrude in-between or overly stent struts. The classification of the dissection is equal for IVUS, and OCT, and is divided into: intimal, medial, adventitial. To quantify the severity of a dissection its depth, circumferential extent, length, size of residual lumen (CSA) is quantified(3). Although small degrees of dissection, tissue protrusion, and incomplete stent apposition following stent deployment (24) are more frequent findings in OCT than in IVUS the clinical significance of these non flow obstructing defects is not known (Figure 7). The quantification or grading of these findings may be important to predict lesion outcomes after PCI. Differences in the chronology, and morphology of biological processes among species raised significant challenges to translating pre clinical results to humans(25), and resulted in the need for the in vivo imaging surrogate endpoints. Longitudinal studies (pre/post intervention vs. follow-up) can potentially be used to evaluate the response of the artery to treatment strategies. For these studies, serial examinations are usually required by performing imaging at baseline, and in follow-up. The OCT, and IVUS datasets are then registered using landmarks such as the stent edges, and side branches, distance from coronary ostia if available(23). Following registration, the data are then compared, using qualitative or quantitative measurements. The optimal time for assessing stent coverage in followup is to be defined according to stent type. In BMS tissue with homogeneous optical characteristics was observed 45 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA A B C D N. 1• 2011 Figure 8. Automated contour detection algorithm for coronary OCT. A: frame level calculation with determination of lumen and stent CSAs, diameter stenosis, and NIH areas in FU; B: same frame strut level analysis that allows to determine NIH value at each strut. Once strut identified the standard OCT software export to a exel file - “CSV file” and precise position of each strut, each strut level NIH, the arc between each struts, and the number of analyzed struts per frame is available for reporting; C: frame level calculation of malapposition distance, and areas. D: same frame with calculation at “strut level”. The software allows reporting the number, arc, and distance of malapposition. six months after stent implantation, while during an extended period of time (≥5 yrs), OCT presented signal patterns of atherosclerotic progression(26). While analyzing vessel response to drug eluting or bioabsorbable stents the presence/absence of polymer, its degradation 46 kinetics, and/or drug elution kinetics must be taken in consideration in establishing the time point for imaging follow-up(27,28). The parameters that usually are reported in follow-up intravascular imaging stent studies are: external elastic IVUS-OCT QUANTIFICATIONS: WHAT membrane (EEM), stent, and lumen cross-sectional area (CSA), plaque plus media CSA (counted as EEM minus TO MEASURE AND HOW TO DO IT? lumen), neointimal hyperplasia (NIH) (calculated as the difference between stent, and lumen), percent NIH vol- A B C D E F G H Figure 9. Stent vessel interaction post PCI. A: edge strut malapposition (arrow); B: edge plaque dissection (arrow); C: intraluminal protrusion of soft plaque material (asterix); D: intraluminal protrusion of calcific plaque and stent underexpansion (arrow); E: embolization of plaque matherial to stent struts at the ostium of side branch (arrow); F: 360° stent malapposition due to underexpansion; G: stent underexpansion due to severe vessel wall pathology (Ca); H: stent overexpansion and media rupture (arrow). A B C D E Figure 10. Stent strut classification by intracoronary Optical Coherence Tomography (OCT). A: covered embedded strut; B: protruding/covered strut; C: malapposed covered strut; D: well apposed uncovered strut; E: malapposed strut uncovered struts. A B C D Figure 11. Abnormal intraluminal tissue (AIT) Classification. A: floating flap; B: related to neointimal proliferation; C: related to uncovered strut; D: related to malapposed strut. 47 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA ume obstruction (computed as NIH divided by stent volume). The detection of late malapposition requires the comparison of post-intervention, and follow-up images. Stent malapposition (defined as blood speckle behind stent struts) is categorized as persistent -visible at post-procedure, and follow-up, resolved -visible only at post-procedure, and late acquired -visible only at followup. ISA due to positive vessel remodeling was demonstrated as a substrate for DES late stent thrombosis (LST), but no data on post intervention IVUS were available in the study(29). By using serial OCT, Ozaki demonstrated that ISA observed at follow-up in SES is more frequently derived from post intervention persistent ISA without neointimal growth, rather than acquired ISA due to vascular remodeling(30). Unlike BMS which develop circumferential coverage easily measured by IVUS, and angiography, the smaller amount of neointimal growth after DES implantation is largely under the limit of resolution of these imaging techniques(31). Due to higher resolution OCT allows the so called “strut level” analysis. A semi automated stent contour algorithm applies 360 radial chords for detailed quantification of NIH thickness at every degree of the A N. 1• 2011 cross section (Figure 8). Its ability to appropriately identify uncovered, and covered stent struts was demonstrated by Murata et al. based on analysis of 3,000 struts(32). Close degree of correlation between OCT, and scanning electron microscopy (SEM) in detection of strut coverage was recently reported(33). This capability has been used to evaluate the response to stent implantation in series of prospective randomized clinical trials(27,28). Struts are normally classified in types based upon the coverage value of strut-intimal thickness (SIT): struts covered by tissue have positive SIT values, while uncovered or malapposed struts have negative SIT. Depending on tissure coverage, and apposition we classified the struts in four types: covered by tissue where the strut boundary is below the luminal surface are defined as embedded covered struts; those covered by tissue where the boundary is above the lumen are defined as protruding covered struts; those not covered by tissue but abutting the vessel wall are classified as uncovered apposed struts; and those not covered by tissue, and not abutting the vessel wall are classified as uncovered, and malapposed struts(19,22) (Figure 10). The number of struts without coverage is counted for each frame analyzed, and the total number, and percentage struts, and B Figure 12. Tissue coverage in follow-up. A: tissue with non homogeneous characteristics of the backscattering, a clear delimitation can be seen between the light characteristics (not homogeneous and with light attenuation) of the tissue covering the stent, and the tissue of the vessel behind stent struts ( homogeneous, and with more bright appearance); B: no difference in optic characteristics between the tissue covering stent struts, and tissue behind stent strut with bright, and homogeneous apperarance. 48 IVUS-OCT QUANTIFICATIONS: WHAT frames with uncovered struts are recorded. The stent length lacking neointimal coverage or having malapposed struts is counted as maximum length (in consecutive frames), and total length (in cumulative frames). The length of the phenomenon in mm is calculated by the pullback rate (mm/s) times the frame rate (s)(1). Derived from direct measurements indexes regarding uniformity of stent coverage can be calculated: neointimal unevenness score (NUS)-calculated by dividing the maximum neointimal thickness to the average neointimal thickness in each analyzed frame, and RUTTS-proportion of frames with >30% uncovered struts per frame. These indexes have been associated to the presence of subclinical thrombus (NUS), and to late stent thrombosis in preclinical studies (RUTTS)(34,35). Measurements for strut apposition, and strut coverage are highly reproducible at the core laboratory (36). DES OCT assessment at different time points demonstrated a significant rate of uncovered stent struts at early, and late follow-up, ranging from 15% at 3 months to 5% at 2 years, and high degree of heterogeneity. Despite the fact that neointimal coverage in DES may progress overtime, previous long-term OCT studies have shown that uncovered stent struts decreased but not disappear from 6 to 12 months(37). The distinction between fibrin clot, and neointimal hyperplasia is not always possible. A more descriptive term of abnormal intraluminal tissue (AIT) defined as TO MEASURE AND HOW TO DO IT? any irregular mass protruding beyond the stent strut into the lumen was adopted by us for qualitative assessment. In order to avoid misclassification of small image artifacts, only AIT >0.25 mm diameter should be included. AIT can be further classified in 4 categories according to its relationship with strut coverage, apposition, presence of underlying NIH, and it’s amount (27) (Figure 11). The described frequency of this phenomenon is much higher than the reported incidence of clinical stent thrombosis. Several OCT studies shown that the presence of subclinical OCT evidence of intracoronary thrombus has not been associated with thrombotic clinical events(34). Neither IVUS nor OCT has tissue characterization software regarding stent coverage since stent struts represent an important artifact. Even with 10 fold higher resolution OCT is not able to discriminate between the natures of tissue coverage, be it fibrin, endothelium, thrombus or neointima. The significance of the tissue characteristics such as reflectivity, and texture is unknown, and densitometry analysis may be a promising method to overcome this limitation(33) (Figure 12). The relationship between all these OCT morphometric findings, and subsequent clinical events has to be determined in a larger number of patients, and with additional years of clinical follow-up. The routine clinical use of OCT will require further clinical trials to validate the technology, establish standard definitions/measurements, and to test its safety, and utility in improving clinical outcomes. References 1. Bezerra HG, Costa MA, Guagliumi G, et al. Intracoronary optical coherence tomography: a comprehensive review clinical and research applications. JACC Cardiovasc Interv 2009;2:1035-46. 2. Mehanna EA, Attizzani GF, Kyono H, et al. Coronary stent assessment by optical coherence tomography. Int J Cardiovasc Imaging. In press. 3. Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2001;37:1478-92. 4. Prati F, Regar E, Mintz GS, et al. Expert’s OCT Review Document. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur Heart J 2010;31:401-15. 5. Yabushita H, Bouma BE, Houser SL, et al. Characterization of human atherosclerosis by optical coherence tomography. Circulation 2002;106:1640-5. 6. Yamada R, Okura H, Kume T, et al. Relationship between arterial and fibrous cap remodeling: a serial three-vessel intravascular ultrasound and optical coherence tomography study. Circ Cardiovasc Interv 2010 Oct;3(5):484-90. Epub 2010 Aug 24. 7. Kubo T, Imanishi T, Takarada S, et al. Assessment of culprit lesion morphology in acute myocardial infarction: ability of optical coherence 49 IL GIORNALE ITALIANO DI CARDIOLOGIA INVASIVA tomography compared with intravascular ultrasound and coronary angioscopy. J Am Coll Cardiol 2007;50:933-9. 8. Ando H, Amano T, Matsubara T, et al. Comparison of Tissue Characteristics Between Acute Coronary Syndrome and Stable Angina Pectoris. Circ J 2010 Dec 14. [Epub ahead of print]. 9. Tanaka A, Imanishi T, Kitabata H, et al. Lipid-rich plaque and myocardial perfusion after successful stenting in patients with non-STsegment elevation acute coronary syndrome: an optical coherence tomography study. Eur Heart J 2009 Jun;30:1348-55. 10. Boccuzzi GG, Di Maggio L, Massara C, et al. Intravascular ultrasound-guided rotational atherectomy for heavily calcified renal artery stenosis. J Cardiovasc Med (Hagerstown) 2010 Feb 24. 11. Kragel AH, Reddy SG, Wittes JT, et al. Morphometric analysis of the composition of atherosclerotic plaques in the four major epicardial coronary arteries in acute myocardial infarction and in sudden coronary death. Circulation 1989;80:1747-56. 12. Jang IK, Tearney GJ, MacNeill B, et al. In vivo characterization of coronary atherosclerotic plaque by use of optical coherence tomography. Circulation 2005;111:1551-5. 13. Takarada S, Imanishi T, Kubo T, et al. Effect of statin therapy on coronary fibrous-cap thickness in patients with acute coronary syndrome: Assessment by optical coherence tomography study. Atherosclerosis 2009;202:491-7. 14. Hong MK, Park DW, Lee CW, et al. Effects of statin treatments on coronary plaques assessed by volumetric virtual histology intravascular ultrasound analysis. JACC Cardiovasc Interv 2009;2:679-88. 15. Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary arterial thrombus by optical coherence tomography. Am J Cardiol 2006;97:1713-7. 16. Regar E, Lemos PA, Saia F, et al. Incidence of thrombotic stent occlusion during the first three months after sirolimus-eluting stent implantation in 500 consecutive patients. Am J Cardiol 2004;15;93:1271-5. 17. Holmes DR Jr, Kereiakes DJ, Garg S, et al. Stent thrombosis. J Am Coll Cardiol 2010;56:1357-65. 18. Sawada T, Shite J, Negi N, et al. Factors that influence measurements and accurate evaluation of stent apposition by optical coherence tomography assessment using a phantom model. Circ J 2009;73:1841-7. 19. Guagliumi G, Sirbu V. Optical coherence tomography: high resolution intravascular imaging to evaluate vascular healing after coronary stenting. Catheter Cardiovasc Interv 2008;72:237-47. 20. Kim JS, Fan C, Choi D, et al. Different patterns of neointimal coverage between acute coronary syndrome and stable angina after various types of drug-eluting stents implantation; 9-month follow-up optical coherence tomography study. Int J Cardiol 2011 Feb 3;146(3):341-6. Epub 2009 Aug 25. 21. Tanigawa J, Barlis P, Dimopoulos K, et al. Optical coherence tomography to assess malapposition in overlapping drug-eluting stents. Eurointervention 2008;3:580-3. 22. Guagliumi G, Sirbu V, Bezerra H, et al. Strut coverage and vessel wall response to zotarolimus-eluting and bare-metal stents implanted in patients with ST-segment elevation myocardial infarction: the OCTAMI 50 N. 1• 2011 (Optical Coherence Tomography in Acute Myocardial Infarction) Study. JACC Cardiovasc Interv 2010;3:680-7. 23. Bouma BE, Tearney GJ, Yabushita H, et al. Evaluation of intracoronary stenting by intravascular optical coherence tomography. Heart 2003;89;317-20. 24. Kubo T, Imanishi T, Kitabata H, et al. Comparison of vascular response after sirolimus-eluting stent implantation between patients with unstable and stable angina pectoris: a serial optical coherence tomography study. JACC Cardiovasc Imaging 2008;1:475-84. 25. Serruys PW, Ormiston JA, Sianos G, et al. Actinomycin-eluting stent for coronary revascularization: a randomized feasibility and safety study: the ACTION trial. J Am Coll Cardiol 2004;44:1363-7. 26. Takano M, Yamamoto M, Inami S, et al. Appearance of lipid-laden intima and neovascularization after implantation of bare-metal stents extended late-phase observation by intracoronary optical coherence tomography. J Am Coll Cardiol 2010;55:26-32. 27. Barlis P, Regar E, Serruys PW, et al. An optical coherence tomography study of a biodegradable vs. durable polymer-coated limus-eluting stent: a LEADERS trial sub-study. Eur Heart J 2010;31:165-76. 28. Guagliumi G, Sirbu V, Musumeci G, et al. Strut coverage and vessel wall response to a new-generation paclitaxel-eluting stent with an ultrathin biodegradable abluminal polymer: Optical Coherence Tomography Drug-Eluting Stent Investigation (OCTDESI). Circ Cardiovasc Interv 2010;3:367-75. 29. Cook S, Wenaweser P, Togni M, et al. Incomplete stent apposition and very late stent thrombosis after drug-eluting stent implantation. Circulation 2007;115:2426-34. 30. Ozaki Y, Okumura M, Ismail TF, et al. The fate of incomplete stent apposition with drug-eluting stents: an optical coherence tomographybased natural history study. Eur Heart J 2010;31:1470-6. 31. Matsumoto D, Shite J, Shinke T, et al. Neointimal coverage of sirolimus-eluting stents at 6-month follow-up: evaluated by optical coherence tomography. Eur Heart J 2007;28:961-7. 32. Murata A, Wallace-Bradley D, Tellez A, et al. Accuracy of optical coherence tomography in the evaluation of neointimal coverage after stent implantation. JACC Cardiovasc Imaging 2010;3:76-84. 33. Templin C, Meyer M, Müller MF, et al. Coronary optical frequency domain imaging (OFDI) for in vivo evaluation of stent healing: comparison with light and electron microscopy. Eur Heart J 2010;31:1792-801. 34. Otake H, Shite J, Ako J, et al. Local determinants of thrombus formation following sirolimus-eluting stent implantation assessed by optical coherence tomography. JACC Cardiovasc Interv 2009;2:459-66. 35. Finn AV, Joner M, Nakazawa G, et al. Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization. Circulation 2007;115:2435-41. 36. Gonzalo N, García-García HM, Serruys PW, et al. Reproducibility of quantitative optical coherence tomography for stent analysis. Eurointervention 2009;5:224-32. 37. Katoh H, Shite J, Shinke T, et al. Delayed neointimalization on sirolimus-eluting stents: 6-month and 12-month follow up by optical coherence tomography. Circ J 2009;73:1033-7.










© Copyright 2025