
How To Fully Protect the Kidney in a Severe Model... Progressive Nephropathy: A Multidrug Approach
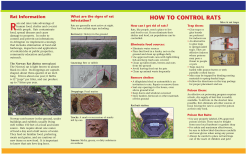
J Am Soc Nephrol 13: 2898–2908, 2002 How To Fully Protect the Kidney in a Severe Model of Progressive Nephropathy: A Multidrug Approach CARLA ZOJA,* DANIELA CORNA,* DAVIDE CAMOZZI,* DARIO CATTANEO,* DANIELA ROTTOLI,* CRISTIAN BATANI,* CRISTINA ZANCHI,* MAURO ABBATE,* and GIUSEPPE REMUZZI*† *Mario Negri Institute for Pharmacological Research, Bergamo, Italy; and †Unit of Nephrology and Dialysis, Azienda Ospedaliera, Ospedali Riuniti di Bergamo, Bergamo, Italy. Abstract. The current therapy for chronic proteinuric nephropathies is angiotensin-converting enzyme inhibitors (ACEi), which slow, but may not halt, the progression of disease, and which may be not effective to the same degree in all patients. In accelerated passive Heymann nephritis (PHN), this study assessed the effect of combining ACEi with angiotensin II receptor antagonist (AIIRA) and with statin that, besides lowering cholesterol, influences inflammatory and fibrogenic processes. Uninephrectomized PHN rats were divided into four groups (n ⫽ 10 each) and daily given oral doses of the following: vehicle; 40 mg/L lisinopril; 100 mg/L lisinopril plus L-158,809; 0.3 mg/kg lisinopril plus L-158,809 plus cerivastatin. Treatments started at 2 mo when rats had massive proteinuria and signs of renal injury and lasted until 10 mo. Increases in BP were equally lowered by treatments. ACEi kept proteinuria at levels comparable to pretreatment and numerically lower than vehicle. The addition of AIIRA to lisin- opril was more effective, being proteinuria reduced below pretreatment values and significantly lower than vehicle. When cerivastatin was added on top of ACE inhibition and AIIR blockade, urinary protein regressed to normal values and renal failure was prevented. Renal ACE activity was increased threefold in PHN, it was inhibited by more than 60% after ACEi, and decreased below control values with triple therapy. Cerivastatin inhibited ACE activity by 30%. Glomerulosclerosis, tubular damage and interstitial inflammation were ameliorated by ACEi alone or combined with AIIRA, and prevented by addition of statin. TGF-1 mRNA upregulation in PHN kidney was partially reduced after ACEi or combined with AIIRA and almost normalized after adding statin. Cerivastatin inhibited TGF-1 gene upregulation by 25%. These data suggest a possible future strategy to induce remission of proteinuria, lessen renal injury, and protect from loss of function in those patients who do not fully respond to ACEi therapy. Proteinuria is a major determinant of progression in both experimental and human nephropathies. High levels of urinary proteins, which reflect excess protein trafficking through the glomerulus, are associated with a faster course of disease (1,2). Experimental observations suggested mechanisms whereby enhanced tubular reabsorption of proteins contributes substantially to promote interstitial inflammatory and fibrogenic reactions that evolve to renal scarring. Overloading of proximal tubular cells in culture with plasma proteins enhanced the production of proinflammatory substances such as endothelin-1, monocyte chemoattractant protein-1 (MCP-1), and RANTES (3–5). Transforming growth factor  (TGF-) was also upregulated in proximal tubular cells on protein challenge (6). Mediators were released preferentially into the basolateral cell medium in a fashion that in the kidney would incite interstitial inflammation and fibrosis. Angiotensin (Ang) converting enzyme inhibitors (ACEi), which reduce protein trafficking and its long-term toxicity, offer superior protection against renal damage. In virtually all experimental models of chronic proteinuric nephropathy, ACEi limit proteinuria and renal injury when treatment starts soon after insult (7–9). By contrast, a delayed administration may not be sufficient to reduce proteinuria and to slow the progression of the disease (10,11). Thus in diabetic rats, ACEi normalized proteinuria and protected against renal structural changes when treatment was started early in the course of the disease (23 wk), but not at the time when proteinuria was higher (32 wk) (12). In the accelerated model of passive Heymann nephritis (PHN), lisinopril limited proteinuria and renal injury if given since 7 d after disease induction, whereas it failed, even at a very high dose, if given since 4 mo (10,13). Similar considerations apply to the clinical setting (14). In proteinuric patients, ACEi slow, but do not invariably halt, progressive nephropathy (15,16). Thus, treatments that synergize with ACEi in further limiting proteinuria and/or limiting interstitial injury have been proposed. The combination of ACEi and AngII type 1 receptor antagonist (AIIRA) has been suggested as a way to maximize renin angiotensin system (RAS) blockade at different levels: reduction of AII availability for binding to angiotensin type I (AT1) receptor and direct inhibition of AII binding to AT1 (17,18). The rationale for the Received May 22, 2002. Accepted August 2, 2002. Correspondence to Dr. Carla Zoja, ‘Mario Negri’ Institute for Pharmacological Research, Via Gavazzeni, 11, 24125 Bergamo, Italy. Phone: 39-0-35-319-888; Fax: 39-035-319-331; E-mail: zoja@marionegri.it 1046-6673/1312-2898 Journal of the American Society of Nephrology Copyright © 2002 by the American Society of Nephrology DOI: 10.1097/01.ASN.0000034912.55186.EC J Am Soc Nephrol 13: 2898–2908, 2002 Angiotensin II Blockade Plus Statin Prevent Progressive Nephropathy combination therapy rests on the evidence that long-term ACEi treatment results in the accumulation of AngI, which may escape ACE inhibition and generate AII that through AT1 receptor causes deleterious effects to the kidney, such as vasoconstriction, inflammation, and fibrosis (19,20). Studies have shown in fact that in the presence of ACE inhibition, AII may be produced by alternative pathways, including chymase (17). Angiotensin receptor blockers could overcome these shortcomings of ACEi by directly antagonizing the AT1 receptor. In addition, the blockade of AT1 receptor in the presence of elevated AII levels can result in the stimulation of the angiotensin subtype 2 (AT2) receptor, which seems to counteract the vasoconstrictor and proliferative action of AT1 (17). Of interest is the evidence that combining an ACE inhibitor and an AIIRA reduced plasma and kidney AII levels more than these agents did alone, providing a potential mechanism for their synergism in reducing proteinuria and BP (21). So far, experimental and clinical studies on combination therapy with ACEi and AIIRA are few and the results are conflicting. In diabetic transgenic (mRen-2)27 rats, low-dose perindopril plus valsartan gave more benefit on the kidney versus monotherapy (22). In rats with renal mass reduction, ACEi plus AIIRA resulted in greater renal protection (23), but not in a study when the doses were adjusted to maintain BP control comparable to single drugs (24). In rats with adriamycin nephrosis, addition of AIIRA failed to overcome resistance to ACE inhibition (11). In a small study in patients with IgA nephropathy, ACEi plus AIIRA was at least additive in decreasing proteinuria, in contrast to no effect when the dose of either drug was doubled (25). Among type 2 diabetic patients with microalbuminuria, the combined drugs also afforded greater reductions in BP and albuminuria (26). In a study of 23 patients with nondiabetic chronic nephropathies at comparable BP control, combined therapy with halved doses of ACEi and AIIRA decreased proteinuria better than full doses alone (27). However, AIIRA added on top of maximal ACE inhibition was not superior to ACEi alone in decreasing proteinuria in 16 patients with various chronic renal diseases (28). Statins have pleiotropic properties that complement their cholesterol-lowering effects and may provide additional benefit in combination therapy. By interfering with prenylation of Ras and Rho family small GTP-binding proteins, they block the activation of mitogen-activated protein kinase signaling pathways and transcription factors including NF-B and AP-1 (29 –31), which regulate the expression of inflammatory, vasoactive, and fibrogenic genes critical to renal disease progression. Combining ACEi with a statin had more renal protective effect than single therapy in rats with puromycin-induced nephrotic syndrome (32) as well as in rats subjected to 5/6 nephrectomy (33). We have recently documented that in severe passive Heymann nephritis (PHN) resistant to ACEi alone, combination of lisinopril with simvastatin given from month 4 to 10 of disease prevented proteinuria from worsening and also limited tubulointerstitial damage (10). In the present study, we assessed whether a multidrug approach with ACEi, AIIRA, and statin could even reverse proteinuria and renal disease progression in rats with accelerated 2899 PHN treated in the phase of overt proteinuria. Renal TGF-1 expression was also evaluated. Materials and Methods Experimental Design Male Sprague-Dawley rats (Charles River Italia s.p.a., Calco, Italy) with initial body weights of 300 to 350 g were used in this study. Animal care and treatment were conducted in accordance with the institutional guidelines that are in compliance with national (Decreto Legislativo n.116, Gazzetta Ufficiale suppl 40, 18 febbraio 1992, Circolare n.8, Gazzetta Ufficiale 14 luglio 1994) and international laws and policies (EEC Council Directive 86/609, OJL358 –1, December 1987; Guide for the Care and Use of Laboratory Animals, U.S. National Research Council, 1996). All animals were housed in a room in which the temperature was kept constant on a 12-h dark/12-h light cycle and allowed free access to standard diet containing 20% protein by weight and tap water. Passive Heymann nephritis (PHN) was induced in non-anesthetized rats by a single intravenous injection of 0.4 ml/100 g body wt of rabbit anti-Fx1A antibody. Unilateral nephrectomy at day 7, when animals were proteinuric, was performed to accelerate the onset of renal histologic damage (34). Two months later, rats were divided into five groups and daily treated up to 10 mo as follows: vehicle (group 1, n ⫽ 10); 40 mg/L lisinopril (AstraZeneca; Basiglio, Milan, Italy) in the drinking water (group 2, n ⫽ 10); 40 mg/L lisinopril plus 100 mg/L L-158,809 (Merck & Co., Inc., Rahway, NJ) (group 3, n ⫽ 10); 40 mg/L lisinopril plus 100 mg/L L-158,809 plus 0.3 mg/kg cerivastatin (group 4, n ⫽ 10); 0.3 mg/kg cerivastatin (Bayer AG, Wuppertal, Germany) (group 5, n ⫽ 10). Doses of lisinopril, L-158,809, and cerivastatin were chosen on the basis of previously published studies (8,35). A group of normal rats followed up to 10 mo served as control (group 6, n ⫽ 6). In addition, five PHN rats together with four age-matched normal rats were sacrified 2 mo after disease induction for renal histologic evaluation. Systolic BP and urinary protein excretion were measured every 2 mo. Serum creatinine was evaluated at baseline and at months 2 (before treatment), 4, 8, and 10. Serum levels of cholesterol, triglycerides, aspartate transaminase (AST), and alanine aminotransferase (ALT) were assessed at the end of the study. At month 10, rats were anesthetized and kidneys were removed for measurement of ACE activity, histology and immunohistochemistry, and total RNA preparation to assess TGF-1 mRNA by Northern blot analysis. Systolic BP (SBP) was recorded in conscious rats by tail plethysmography (IITC Life Science, Woodland Hills, CA). Twenty-four– hour urine samples were collected using metabolic cages, and proteinuria was determined by modified Coomassie blue G dye-binding assay for proteins with BSA as standard. Blood was collected from the tail vein of anesthetized animals. Serum was obtained after whole blood clotting and kept frozen at ⫺20°C until assayed. Creatinine was measured by alkaline picrate method. Serum cholesterol, triglycerides, and transaminase levels were measured using an autoanalyzer (CX5, Beckman Instruments Inc., Fullerton, CA). Measurement of ACE Activity Renal tissue was homogenized in distilled water and centrifuged at 12,000 ⫻ g for 10 min at 4°C. The resulting supernatant was used for ACE activity determination by a spectrophotometric method (Sigma). ACE activity was expressed as relative units per milligram protein of tissue. Renal Histology The removed kidneys were fixed for 6 h in Dubosq-Brazil, dehydrated in alcohol, and embedded in paraffin. Kidney samples were 2900 Journal of the American Society of Nephrology J Am Soc Nephrol 13: 2898–2908, 2002 sectioned at 3-m intervals, and the sections were stained with Masson’s trichrome, hematoxylin and eosin, and periodic acid-Schiff reagent (PAS stain). Tubular (atrophy, casts, and dilatation) and interstitial changes (fibrosis and inflammation) were graded from 0 to 4⫹ (0, no changes; 1⫹, changes affecting ⬍25% of the sample; 2⫹, changes affecting 25 to 50% of the sample; 3⫹, changes affecting 50 to 75% of the sample; 4⫹, changes affecting 75 to 100% of the sample). At least 100 glomeruli were examined for each animal, and the extent of glomerular damage was expressed as the percentage of glomeruli presenting sclerotic lesions. All renal biopsies were analyzed by the same pathologist who was unaware of the nature of the experimental groups. Immunohistochemical Analyses Mouse monoclonal antibodies were used for the immunohistochemical detection of ED-1 antigen present in rat monocytes and Table 1. Time course of body weight (g) in PHN ratsa Groups PHN ⫹ vehicle PHN ⫹ ACEi PHN ⫹ ACEi ⫹ AIIRA PHN ⫹ ACEi ⫹ AIIRA ⫹ cerivastatin PHN ⫹ cerivastatin Control 0 mo 2 mo (before treatment) 4 mo 6 mo 8 mo 10 mo 305 ⫾ 5 (n ⫽ 10) 315 ⫾ 3 (n ⫽ 10) 323 ⫾ 10 (n ⫽ 10) 307 ⫾ 6 (n ⫽ 10) 304 ⫾ 4 (n ⫽ 10) 324 ⫾ 7 (n ⫽ 6) 532 ⫾ 12 (n ⫽ 10) 538 ⫾ 15 (n ⫽ 10) 506 ⫾ 17 (n ⫽ 10) 519 ⫾ 13 (n ⫽ 10) 542 ⫾ 23 (n ⫽ 10) 562 ⫾ 23 (n ⫽ 6) 598 ⫾ 14 (n ⫽ 10) 592 ⫾ 17 (n ⫽ 10) 538 ⫾ 24b (n ⫽ 10) 526 ⫾ 24bdf (n ⫽ 8) 589 ⫾ 25 (n ⫽ 10) 631 ⫾ 22 (n ⫽ 6) 634 ⫾ 15 (n ⫽ 10) 626 ⫾ 21 (n ⫽ 10) 571 ⫾ 31b (n ⫽ 10) 569 ⫾ 21ce (n ⫽ 7) 623 ⫾ 27 (n ⫽ 9) 682 ⫾ 23 (n ⫽ 6) 657 ⫾ 17 (n ⫽ 9) 636 ⫾ 25 (n ⫽ 10) 603 ⫾ 35 (n ⫽ 10) 586 ⫾ 21cd (n ⫽ 7) 654 ⫾ 28 (n ⫽ 9) 708 ⫾ 24 (n ⫽ 6) 661 ⫾ 30 (n ⫽ 8) 666 ⫾ 26 (n ⫽ 10) 678 ⫾ 32 (n ⫽ 9) 618 ⫾ 24c (n ⫽ 7) 689 ⫾ 28 (n ⫽ 8) 758 ⫾ 29 (n ⫽ 6) a Values are expressed as mean ⫾ SE. PHN, passive Heymann nephritis; ACEi, angiotensin-converting enzyme inhibitor; AIIRA, angiotensin II receptor antagonist. b P ⬍ 0.05 versus control. c P ⬍ 0.01 versus control. d P ⬍ 0.05 versus vehicle. e P ⬍ 0.01 versus vehicle. f P ⬍ 0.05 versus lisinopril. Table 2. Time course of systolic blood pressure (mmHg) in PHN rats Groups PHN ⫹ vehicle PHN ⫹ ACEi PHN ⫹ ACEi ⫹ AIIRA PHN ⫹ ACEi ⫹ AIIRA ⫹ cerivastatin PHN ⫹ cerivastatin Control Values are expressed as mean ⫾ SE. P ⬍ 0.05 versus control. c P ⬍ 0.01 versus control. d P ⬍ 0.05 versus vehicle and cerivastatin. e P ⬍ 0.01 versus vehicle and cerivastatin. f P ⬍ 0.01 versus lisinopril. g P ⬍ 0.05 versus vehicle. a b 0 mo 2 mo (before treatment) 4 mo 6 mo 8 mo 10 mo 122 ⫾ 3 (n ⫽ 10) 121 ⫾ 2 (n ⫽ 10) 118 ⫾ 2 (n ⫽ 10) 122 ⫾ 2 (n ⫽ 10) 122 ⫾ 3 (n ⫽ 10) 116 ⫾ 4 (n ⫽ 6) 127 ⫾ 2 (n ⫽ 10) 130 ⫾ 3 (n ⫽ 10) 129 ⫾ 3 (n ⫽ 10) 130 ⫾ 2 (n ⫽ 10) 129 ⫾ 2 (n ⫽ 10) 121 ⫾ 2 (n ⫽ 6) 133 ⫾ 3c (n ⫽ 10) 93 ⫾ 2ce (n ⫽ 10) 91 ⫾ 3ce (n ⫽ 10) 83 ⫾ 1cef (n ⫽ 8) 123 ⫾ 2g (n ⫽ 10) 122 ⫾ 1 (n ⫽ 6) 144 ⫾ 3c (n ⫽ 10) 94 ⫾ 3ce (n ⫽ 10) 87 ⫾ 3ce (n ⫽ 10) 85 ⫾ 2ce (n ⫽ 7) 137 ⫾ 4b (n ⫽ 9) 122 ⫾ 4 (n ⫽ 6) 148 ⫾ 4c (n ⫽ 9) 85 ⫾ 2ce (n ⫽ 10) 86 ⫾ 3ce (n ⫽ 10) 85 ⫾ 2ce (n ⫽ 7) 135 ⫾ 2cg (n ⫽ 9) 121 ⫾ 2 (n ⫽ 6) 152 ⫾ 5c (n ⫽ 8) 90 ⫾ 4ce (n ⫽ 10) 90 ⫾ 3ce (n ⫽ 9) 85 ⫾ 2ce (n ⫽ 7) 137 ⫾ 3cg (n ⫽ 8) 120 ⫾ 2 (n ⫽ 6) J Am Soc Nephrol 13: 2898–2908, 2002 Angiotensin II Blockade Plus Statin Prevent Progressive Nephropathy 2901 Table 3. Time course of urinary protein excretion (mg/d) in PHN ratsa Groups PHN ⫹ vehicle PHN ⫹ ACEi PHN ⫹ ACEi ⫹ AIIRA PHN ⫹ ACEi ⫹ AIIRA ⫹ cerivastatin PHN ⫹ cerivastatin Control 0 mo 2 mo (before treatment) 4 mo 6 mo 8 mo 10 mo 20 ⫾ 1.9 (n ⫽ 10) 21 ⫾ 1.2 (n ⫽ 10) 20 ⫾ 1.5 (n ⫽ 10) 23 ⫾ 0.7 (n ⫽ 10) 17 ⫾ 1.3 (n ⫽ 10) 21 ⫾ 2.2 (n ⫽ 6) 425 ⫾ 69c (n ⫽ 10) 408 ⫾ 64c (n ⫽ 10) 406 ⫾ 51c (n ⫽ 10) 439 ⫾ 54c (n ⫽ 10) 406 ⫾ 71c (n ⫽ 10) 28 ⫾ 7 (n ⫽ 6) 625 ⫾ 94c (n ⫽ 10) 274 ⫾ 86cd (n ⫽ 10) 127 ⫾ 28ce (n ⫽ 10) 55 ⫾ 14efg (n ⫽ 8) 474 ⫾ 58ce (n ⫽ 10) 32 ⫾ 6 (n ⫽ 6) 653 ⫾ 80c (n ⫽ 10) 352 ⫾ 123c (n ⫽ 10) 129 ⫾ 44ce (n ⫽ 10) 59 ⫾ 22efg (n ⫽ 7) 632 ⫾ 75c (n ⫽ 10) 40 ⫾ 9 (n ⫽ 6) 700 ⫾ 70c (n ⫽ 9) 344 ⫾ 117 (n ⫽ 10) 187 ⫾ 75e (n ⫽ 10) 76 ⫾ 29ef (n ⫽ 7) 711 ⫾ 87c (n ⫽ 9) 49 ⫾ 9 (n ⫽ 6) 697 ⫾ 47c (n ⫽ 8) 381 ⫾ 131 (n ⫽ 10) 272 ⫾ 86be (n ⫽ 9) 92 ⫾ 20efh (n ⫽ 7) 752 ⫾ 78c (n ⫽ 8) 88 ⫾ 26 (n ⫽ 6) Values are expressed as mean ⫾ SE. P ⬍ 0.05 versus control. c P ⬍ 0.01 versus control. d P ⬍ 0.05 versus vehicle. e P ⬍ 0.01 versus vehicle. f P ⬍ 0.01 versus cerivastatin. g P ⬍ 0.05 versus lisinopril, lisinopril ⫹ L158,809. h P ⬍ 0.05 versus lisinopril⫹L158,809. a b Table 4. Time course of serum creatinine (mg/dl) in PHN ratsa Groups PHN ⫹ vehicle PHN ⫹ ACEi PHN ⫹ ACEi ⫹ AIIRA PHN ⫹ ACEi ⫹ AIIRA ⫹ cerivastatin PHN ⫹ cerivastatin Control 0 mo 2 mo (before treatment) 4 mo 8 mo 10 mo 0.60 ⫾ 0.03 (n ⫽ 10) 0.59 ⫾ 0.02 (n ⫽ 10) 0.59 ⫾ 0.02 (n ⫽ 10) 0.57 ⫾ 0.02 (n ⫽ 10) 0.55 ⫾ 0.02 (n ⫽ 10) 0.57 ⫾ 0.02 (n ⫽ 6) 0.81 ⫾ 0.02c (n ⫽ 10) 0.86 ⫾ 0.03c (n ⫽ 10) 0.82 ⫾ 0.02c (n ⫽ 10) 0.84 ⫾ 0.03c (n ⫽ 10) 0.81 ⫾ 0.04c (n ⫽ 10) 0.64 ⫾ 0.01 (n ⫽ 6) 1.10 ⫾ 0.03c (n ⫽ 10) 0.86 ⫾ 0.02cd (n ⫽ 10) 0.82 ⫾ 0.03cd (n ⫽ 10) 0.79 ⫾ 0.03cef (n ⫽ 8) 1.12 ⫾ 0.03c (n ⫽ 10) 0.61 ⫾ 0.03 (n ⫽ 6) 1.22 ⫾ 0.10c (n ⫽ 9) 0.95 ⫾ 0.05c (n ⫽ 10) 0.87 ⫾ 0.06bdf (n ⫽ 10) 0.79 ⫾ 0.03cef (n ⫽ 7) 1.12 ⫾ 0.12c (n ⫽ 9) 0.63 ⫾ 0.04 (n ⫽ 6) 2.03 ⫾ 0.67c (n ⫽ 8) 1.06 ⫾ 0.06c (n ⫽ 10) 0.95 ⫾ 0.07bd (n ⫽ 9) 0.86 ⫾ 0.03bef (n ⫽ 7) 1.27 ⫾ 0.08c (n ⫽ 8) 0.74 ⫾ 0.03 (n ⫽ 6) Values are expressed as mean ⫾ SE. P ⬍ 0.05 versus control. c P ⬍ 0.01 versus control. d P ⬍ 0.05 versus vehicle and cerivastatin. e P ⬍ 0.01 versus vehicle and cerivastatin. f P ⬍ 0.05 versus lisinopril. a b macrophages (Chemicon, Temecula, CA) and rat CD8⫹ cell surface glycoprotein on T-suppressor cells (OX8; PharMingen, Los Angeles, CA). ED-1 antigen was stained on paraffin sections using an alkaline phosphatase-Fast Red technique. CD8 staining was analyzed by indirect immunofluorescence technique. Fragments of renal tissues were frozen in liquid nitrogen and cut at 3 m using a Mikrom 500 O cryostat (Walldorf, Germany). The sections were blocked with 1% PBS/BSA, incubated overnight at 4°C with the primary antibody (W3/25, 40 g/ml; OX6, 5 g/ml), washed with PBS, and then incubated with Cy3-conjugated donkey anti-mouse IgG antibodies (5 g/ml in PBS; Jackson ImmunoResearch Laboratories, West Grove, PA) for 1 h at room temperature. For each marker, positive cells were counted in at least ten randomly selected high-power microscopic fields (⫻400) per each animal. 2902 Journal of the American Society of Nephrology J Am Soc Nephrol 13: 2898–2908, 2002 Table 5. Serum lipid profile and serum transaminase levels in PHN ratsa Groups PHN ⫹ vehicle PHN ⫹ ACEi PHN ⫹ ACEi ⫹ AIIRA PHN ⫹ ACEi ⫹ AIIRA ⫹ cerivastatin PHN ⫹ cerivastatin Control Serum Cholesterol (mg/dl) Serum Triglycerides (mg/dl) ALT (IU/L) AST (IU/L) 154 ⫾ 15b (n ⫽ 8) 94 ⫾ 16c (n ⫽ 10) 91 ⫾ 16d (n ⫽ 9) 65 ⫾ 5d (n ⫽ 7) 161 ⫾ 18b (n ⫽ 8) 67 ⫾ 4 (n ⫽ 6) 367 ⫾ 25b (n ⫽ 8) 241 ⫾ 68c (n ⫽ 10) 163 ⫾ 35d (n ⫽ 9) 153 ⫾ 45d (n ⫽ 7) 392 ⫾ 44b (n ⫽ 8) 186 ⫾ 21 (n ⫽ 6) 35 ⫾ 7 (n ⫽ 8) 34 ⫾ 5 (n ⫽ 10) 46 ⫾ 4 (n ⫽ 9) 44 ⫾ 3 (n ⫽ 7) 37 ⫾ 4 (n ⫽ 8) 51 ⫾ 5 (n ⫽ 6) 76 ⫾ 12 (n ⫽ 8) 79 ⫾ 13 (n ⫽ 10) 77 ⫾ 14 (n ⫽ 9) 81 ⫾ 8 (n ⫽ 7) 54 ⫾ 3 (n ⫽ 8) 70 ⫾ 3 (n ⫽ 6) Values are expressed as mean ⫾ SE. P ⬍ 0.01 versus control. c P ⬍ 0.05 versus vehicle. d P ⬍ 0.01 versus vehicle. a b was labeled with ␣-32P dCTP by random-primed method. Hybridization was performed overnight in 0.25 mol/L Na2HPO4, pH 7.2, 7% SDS. Filters were washed twice for 30 min with 20 mmol/L Na2HPO4, pH 7.2, 5% SDS and two times for 10 min with 20 mmol/L Na2HPO4, pH 7.2, 1% SDS at 65°C. Membranes were subsequently probed with a glyceraldehyde-3-phosphate dehydrogenase (GAPDH) cDNA, taken as internal standard of equal loading of the samples on the membrane. TGF- mRNA optical density was normalized to that of the constituently released GAPDH gene expression. Statistical Analyses Data of all the animals until death were included in the statistical analyses. Results were expressed as mean ⫾ SEM and analyzed using the nonparametric Mann Whitney test or Kruskal-Wallis test for multiple comparisons as appropriate. The statistical significance level was defined as P ⬍ 0.05. Results Systemic Parameters Figure 1. ACE activity in kidney homogenate from passive Heymann nephritis (PHN) rats given vehicle (n ⫽ 8), cerivastatin (n ⫽ 8), angiotensin-converting enzyme inhibitors (ACEi) (n ⫽ 10), ACEi plus angiotensin II (AngII) receptor antagonist (AIIRA) plus cerivastatin (n ⫽ 7), and in control rats (n ⫽ 6). Data are mean ⫾ SE. °P ⬍ 0.05, °°P ⬍ 0.01 versus control; *P ⬍ 0.05, **P ⬍ 0.01 versus vehicle. Northern Blot Analyses Total RNA was isolated from whole kidney tissue by the guanidium isothiocyanate/cesium chloride procedure. Twenty micrograms of total RNA were then fractionated on 1.6% agarose gel and blotted onto synthetic membranes (Zeta-probe; Biorad, Richmond, CA). A 0.45 kb EcoRI/HindIII fragment of human TGF-1 cDNA from plasmid pUC18 was used to detect 2.5 kb transcript. The probe By the end of the study, two rats with PHN died in the vehicle group (months 6.5 and 9), one in the group given lisinopril plus L-158,809 (month 8.5), three in the group given lisinopril plus L-158,809 plus cerivastatin (months 2.5, 3, and 5.5), two in the group on cerivastatin alone (months 7 and 9). All rats on lisinopril alone and controls were alive at 10 mo. Food intake was comparable in PHN and control groups for the entire study period. As shown in Table 1, rats with PHN gained weight along the study; however, body weight was numerically lower than controls, with a statistical significance being observed for rats given ACEi plus AIIRA plus statin. Rats with PHN exhibited an increase in SBP with respect to controls (Table 2). Treatment with the ACEi alone or in combination with AIIRA or with AIIRA plus cerivastatin maintained SBP at values lower than those of vehicle group, and even of controls. In rats on cerivastatin alone, SBP was lower J Am Soc Nephrol 13: 2898–2908, 2002 Angiotensin II Blockade Plus Statin Prevent Progressive Nephropathy 2903 than in vehicle rats, which is consistent with the antihypertensive effect previously described for statins and attributed to drug interaction with endothelial function or AII receptors (36). Renal Parameters In rats with PHN, mean values of proteinuria exceeded 400 mg/d in all groups before treatment (Table 3). Administration of lisinopril maintained over time urinary protein excretion at values comparable to those measured before treatment and numerically, although not significantly, lower than vehicle. When lisinopril was combined with the AIIRA L-158,809, more marked antiproteinuric effect was evident, with proteinuria values being consistently reduced with respect to pretreatment and significantly different from vehicle at all time points considered. Remarkably, proteinuria was further lowered to control levels when animals were treated with the triple therapy of ACEi plus AIIRA plus cerivastatin. In PHN rats given cerivastatin, proteinuria values were lower than those measured in vehicle group at 4 mo, thereafter they became comparable. Renal function, as evaluated by serum creatinine levels, was progressively impaired in PHN rats given vehicle (Table 4). In rats treated with lisinopril, mean value of serum creatinine was numerically lower than in rats given vehicle. A difference in serum creatinine was achieved when lisinopril was combined with L-158,809 and even to a more significant extent when all three drugs were administered together. Treatment with cerivastatin did not improve renal function. Serum Cholesterol and Triglycerides In PHN rats given vehicle, serum cholesterol and triglyceride levels were increased with respect to controls (Table 5). Lisinopril alone or combined with L-158,809 significantly reduced hypercholesterolemia and hypertriglyceridemia. More remarkably, cholesterol and triglycerides in the group given the triple therapy accounted for values within the control range. Administration of cerivastatin alone had no effect. Serum Transaminase Levels In PHN rats, serum transaminase levels were not modified by treatments (Table 5). Renal ACE Activity ACE activity in renal homogenate from PHN rats was elevated as compared with controls (Figure 1). In response to lisinopril treatment renal ACE activity was inhibited by more than 60%. The addition of cerivastatin to ACEi plus AIIRA led to a further striking reduction in ACE activity, which decreased below control values. Treatment with cerivastatin alone resulted in a 30% inhibition of ACE activity. Renal Histology Rats with PHN exhibited glomerular and tubulointerstitial changes 2 mo after disease induction (Figure 2). At 10 mo in PHN rats given vehicle, on average 60% of glomeruli were affected by sclerotic changes (Figures 2 and 3). Figure 2. Renal morphologic parameters evaluated at month 2 in PHN (n ⫽ 5, first column) and control rats (n ⫽ 4, second column) and at month 10 in PHN rats given vehicle (n ⫽ 8), cerivastatin (n ⫽ 8), ACEi (n ⫽ 10), ACEi plus AIIRA (n ⫽ 9), ACEi plus AIIRA plus cerivastatin (n ⫽ 7), and in control rats (n ⫽ 6). Data are mean ⫾ SE. §P ⬍ 0.01 versus control (month 2); *P ⬍ 0.05, **P ⬍ 0.01 versus vehicle; °P ⬍ 0.05, FP ⬍ 0.01 versus cerivastatin; ⫹P ⬍ 0.01 versus ACEi; #P ⬍ 0.05 versus ACEi, ACEi⫹AIIRA, ⌬P ⬍ 0.05 versus PHN at month 2 . Tubulointerstitial damage consisted of interstitial fibrosis and inflammation associated with tubular atrophy and eosinophilic casts in the tubular lumen. Lisinopril alone or combined with L-158,809 significantly protected PHN rats from glomerulosclerosis, tubular damage, and interstitial inflammation, with respect to vehicle-rats. In rats given the triple therapy, complete renoprotection was achieved, so that glomerular and tubular morphology was comparable to age-matched normal controls. Actually, renal injury documented in PHN at 2 mo was reversed by the multidrug therapy. Treatment with cerivastatin had only a mild protective effect on renal damage. 2904 Journal of the American Society of Nephrology J Am Soc Nephrol 13: 2898–2908, 2002 Figure 3. Light micrographs of sections of kidney cortex showing effects of drug treatments on renal structural changes in PHN. (A) PHN⫹vehicle, (B) PHN⫹cerivastatin, (C) PHN⫹lisinopril, (D) PHN⫹lisinopril⫹L-158,809, (E) PHN⫹lisinopril⫹L-158,809⫹cerivastatin, (F) age-matched control rats. Magnification, ⫻100. Renal Expression of TGF- mRNA Figure 4. ED-1–positive monocytes/macrophages and CD-8 –positive T cells infiltrating the interstitium of rats with PHN (n ⫽ 8) and the effect of cerivastatin (n ⫽ 8), ACEi (n ⫽ 10), ACEi⫹AIIRA (n ⫽ 9), ACEi⫹AIIRA⫹cerivastatin (n ⫽ 7). Data are mean ⫾ SE. HPF, high power field; *P ⬍ 0.05, **P ⬍ 0.01 versus vehicle; °P ⬍ 0.05, #P ⬍ 0.01 versus ACEi, ACEi⫹AIIRA, and cerivastatin. Inflammatory Cell Infiltrates in Renal Interstitium A massive infiltration of ED-1–positive monocytes/macrophages (Figure 4) and CD-8 –positive T cells (Figures 4 and 5) was present in the renal interstitium of PHN rats given vehicle, as evaluated at month 10. Lisinopril alone or combined with L-158,809 limited the number of infiltrating cells. The degree of cell infiltrates was decreased further by the combined administration of ACE inhibitor plus AIIRA plus statin. A tendency toward less accumulation of ED-1–positive cells was observed in the renal interstitium of rats treated with cerivastatin in respect to vehicle rats, although statistical significance was not reached. Upregulation of TGF-1 mRNA was observed in the kidney of PHN rats given vehicle (Figure 6). Densitometric analyses of the autoradiographic signals showed a 4.8-fold increase in TGF-1 transcript levels with respect to age-matched controls. TGF-1 gene overexpression was partially reduced after the administration of lisinopril alone or combined with L-158,809 (34 to 38% inhibition in respect to vehicle), but a statistical significance was not achieved. By contrast, the TGF-1 signal appeared significantly reduced after lisinopril plus L-158,809 plus cerivastatin treatment. In the rats given cerivastatin TGF1, gene upregulation was inhibited by 25% with respect to vehicle. Discussion Results from this study demonstrate that in a severe model of proteinuric nephropathy, which partly resembles advanced phases of human disease, regression of proteinuria and complete protection of the kidney can be achieved by combined administration of ACEi, AIIRA, and statin. The current therapy for chronic proteinuric nephropathies is ACEi that limit proteinuria and reduce GFR decline and risk of end-stage renal disease more effectively than other antihypertensive treatments (14,37,38). Full remission of proteinuria, however, is seldom obtained, and ACEi may be not effective to the same degree in all individuals, particularly when therapy is started late. For nonresponders, treatment procedure to remission and/or regression must include a multimodal strategy (14,39). Here, we documented that lisinopril given from 2 to 10 J Am Soc Nephrol 13: 2898–2908, 2002 Angiotensin II Blockade Plus Statin Prevent Progressive Nephropathy 2905 Figure 5. Representative photomicrographs of sections of kidney cortex stained for detection of CD-8 –positive T cells, obtained at 10 mo from PHN rats given vehicle (A), cerivastatin (B), lisinopril (C), lisinopril⫹L-158,809 (D), or lisinopril⫹L-158,809⫹cerivastatin (E) and from age-matched control rats (F). Magnification, ⫻200. mo after disease induction to PHN rats with heavy proteinuria kept urinary protein excretion at levels that were both comparable to pretreatment and numerically, albeit not significantly, lower than those of rats given no drug. Renal function ameliorated after ACEi but not to a significant extent. By contrast, the addition of AIIRA therapy to lisinopril resulted in greater antiproteinuric effect, being urinary protein excretion consistently reduced with respect to pretreatment values and significantly lower than vehicle rats at any time points considered. Thus, blocking the receptor binding in concomitance with the formation of AII further increased the antiproteinuric effect of the ACEi alone and further protected against renal function deterioration. When cerivastatin was added on top of ACE inhibition and AT1 blockade, proteinuria regressed toward normal values and renal failure was prevented. Cerivastatin alone had effects on proteinuria only in the early phase of treatment and partially decreased serum creatinine levels. The mechanism(s) by which ACEi plus AIIRA, and to a greater extent the addition of statin, lowered proteinuria in PHN animals below the pretreatment levels, can be related to the combined drugs’ actions on the glomerular filtration barrier function. As suggested by several studies, both ACEi and AIIRA reduce membrane pore dimensions and improve glomerular size-selectivity in experimental and human proteinuric nephropathies (40 – 43). There is also evidence that ACEi preserved heparan sulfate proteoglycans in the glomerular basement membrane (GBM) of rats with adriamycin nephropathy (44). In the PHN model, we documented that the early treatment with lisinopril preserved the frequency of epithelial slits and prevented the associated loss of hydraulic permeability of the GBM (45). Moreover, in the same model, blocking AII synthesis or activity preserved the expression of nephrin, the slit diaphragm protein in the podocytes (46). On the other hand, preliminary data in 5/6 nephrectomized rats fed a high-cholesterol diet indicate that statins have the capability to preserve anionic sites in the GBM (Suzuki T, personal communication), that may account for the maximal antiproteinuric effect achieved by adding cerivastatin to ACEi and AIIRA. Data of a similar BP control among PHN rats receiving either lisinopril or the combined therapies would weaken the role for the BP lowering action in the superior protective effects of the multidrug therapy. In fact, recent data have shown that in PHN the early treatment with the antihypertensive drug lacidipine, at variance with lisinopril, failed to limit proteinuria and renal damage, despite similar degree of BP reduction (47). Cerivastatin alone did not modify hypercholesterolemia of PHN, a finding also described in other rat models, including puromycin aminonucleoside nephrosis (48), mesangial proliferative nephritis (49), and AngII–induced renal injury (31). However, addition of cerivastatin to AngII blocking agents lowered serum cholesterol to normal levels in parallel to and as a likely consequence of the strong antiproteinuric effect of triple therapy (10). An interesting finding of the current study is that the addition of cerivastatin on the background of ACE inhibition resulted in a dramatic decrease of renal ACE activity. Actually, ACE activity was increased in the kidney of PHN rats and could be inhibited by more than 60% after lisinopril. Adding cerivastatin to ACEi plus AIIRA led to a further striking 2906 Journal of the American Society of Nephrology Figure 6. (Top) Renal expression of TGF- mRNA assessed at month 10 in age-matched control rats (n ⫽ 6) and in PHN rats given vehicle (n ⫽ 8), cerivastatin (n ⫽ 8), ACEi (n ⫽ 10), ACEi⫹AIIRA (n ⫽ 9), ACEi⫹AIIRA⫹cerivastatin (n ⫽ 7). Northern blot experiments were performed using total RNA from whole kidney tissue of either separate or pooled samples for each group. Results shown are representative of pooled samples for each group. (Bottom) Densitometric analysis of the autoradiographic signals for TGF-. Results shown are mean ⫾ SE of separate animals for each group. The optical density of the autoradiographic signals was quantitated and calculated as the ratio of TGF- to GAPDH mRNA. Results expressed as fold increase over control (represented as 1) in densitometric arbitrary units. °P ⬍ 0.01 versus control; *P ⬍ 0.05 versus other PHN groups. J Am Soc Nephrol 13: 2898–2908, 2002 reduced AT1 receptor density in isolated platelets (52). It is tempting to speculate that cerivastatin combined with lisinopril and L-158,809, along with the possible effect of improving the permselectivity of the glomerular barrier (as we stated above) may contribute to achieve full inhibition of RAS, thereby preventing local AngII generation and its deleterious effects (19,20). Increased intrarenal synthesis of AII has been measured in experimental renal disease (53,54) and might contribute together with excess protein traffic in promoting tubulointerstitial inflammation and fibrosis (1). In this respect, AngII immunoreactive material was detected in tubular cells after subtotal nephrectomy in rats at sites of upregulation of TGF- and type IV collagen mRNA (54). In vitro and in vivo studies have consistently documented that statins modulate intracellular signaling pathways responsible for inflammation and fibrosis (29 –31). We have recently reported that in severe PHN the beneficial effect of combined therapy of lisinopril and simvastatin against injury could be attributed, at least in part, to further inhibition of MCP-1– dependent interstitial inflammation by simvastatin (10). Here, we extended our observations to TGF-, the crucial mediator of fibrosis for which expression was also found to be reduced by lovastatin in glomeruli of diabetic rats (55). Upregulation of TGF- mRNA of PHN kidney was inhibited by 25% after cerivastatin and almost normalized after combined administration of ACEi plus AIIRA plus statin therapy. The finding that renal structural integrity was fully preserved by triple therapy clearly indicates that simultaneous blocking of pathways of injury, including proteinuria, AII, and TGF-, eventually translates into both full prevention of progressive parenchymal injury and preservation of renal function. Our data cannot clearly unravel a hierarchy of protective mechanisms or establish which combination(s) of factors was most affected by the multidrug treatment. However, maximization of the antiproteinuric action, presumably by mechanisms at the glomerular level, appears to play an important role to achieve protection, possibly in combination with the inhibitory effect on secondary pathways, leading to inflammatory and immune cell accumulation and fibrosis. In conclusion, our data suggest a possible future strategy to induce remission of proteinuria as well as to lessen renal injury and protect from loss of function in those patients who do not fully respond to ACEi therapy. Acknowledgments reduction in ACE activity below control values. Notably, treatment with cerivastatin alone resulted in a 30% inhibition of ACE activity. These data are in agreement with the observation of an inhibitory effect of statins on ACE activity in a different experimental setting, cardiac hypertrophy induced by hemodynamic overload in rats (50). That statins can directly interfere with RAS is also suggested by findings that atorvastatin downregulated AT1 receptor mRNA expression either in cultured vascular smooth muscle cells exposed to AngII or in aortic segments of spontaneously hypertensive rats (51). Moreover, in hypercholesterolemic patients, statin treatment effectively We thank Dr. Marcella Pagnoncelli for animal care assistance. We are also indebted to Drs. Flavio Gaspari and Roberta Donadelli for helpful collaboration. Cerivastatin was provided by Dr. Hilmar Bischoff, Bayer AG, Wuppertal, Germany. Lisinopril was kindly provided by AstraZeneca, Basiglio, Milan, Italy, and L-158,809 by Merck & Co., Inc., Rahway, NJ. Part of this study has been presented at the 34th Annual Meeting of the American Society of Nephrology, San Francisco, CA, October 13–17, 2001. References 1. Remuzzi G, Bertani T: Pathophysiology of progressive nephropathies. N Engl J Med 339: 1448 –1456, 1998 J Am Soc Nephrol 13: 2898–2908, 2002 Angiotensin II Blockade Plus Statin Prevent Progressive Nephropathy 2. Remuzzi G: Nephropathic nature of proteinuria. Curr Opin Nephrol Hyperten 8: 655– 663, 1999 3. Zoja C, Morigi M, Figliuzzi M, Bruzzi I, Oldroyd S, Benigni A, Ronco P, Remuzzi G: Proximal tubular cell synthesis and secretion of endothelin-1 on challenge with albumin and other proteins. Am J Kidney Dis 26: 934 –941, 1995 4. Wang Y, Chen J, Chen L, Tay YC, Rangan GK, Harris DC: Induction of monocyte chemoattractant protein-1 in proximal tubule cells by urinary protein. J Am Soc Nephrol 8: 1537–1545, 1997 5. Zoja C, Donadelli R, Colleoni S, Figliuzzi M, Bonazzola S, Morigi M, Remuzzi G: Protein overload stimulates RANTES production by proximal tubular cells depending on NF-kB activation. Kidney Int 53: 1608 –1615, 1998 6. Yard BA, Chorianopoulos E, Herr D, van der Woude FJ: Regulation of endothelin-1 and transforming growth factor-beta1 production in cultured proximal tubular cells by albumin and heparan sulphate glycosaminoglycans. Nephrol Dial Transplant 16: 1769 –1775, 2001 7. Zatz R, Dunn BR, Meyer TW, Anderson S, Rennke HG, Brenner BM: Prevention of diabetic glomerulopathy by pharmacological amelioration of glomerular capillary hypertension. J Clin Invest 77: 1925–1930, 1986 8. Zoja C, Donadelli R, Corna D, Testa D, Facchinetti D, Maffi R, Luzzana E, Colosio V, Bertani T, Remuzzi G: The renoprotective properties of angiotensin-converting enzyme inhibitors in a chronic model of membranous nephropathy are solely due to the inhibition of angiotensin II: Evidence based on comparative studies with a receptor antagonist. Am J Kidney Dis 29: 254 –264, 1997 9. Abbate M, Zoja C, Rottoli D, Corna D, Perico N, Bertani T, Remuzzi G: Antiproteinuric therapy while preventing the abnormal protein traffic in proximal tubule abrogates protein and complement-dependent interstitial inflammation in experimental renal disease. J Am Soc Nephrol 10: 804 – 813, 1999 10. Zoja C, Corna D, Rottoli D, Cattaneo D, Zanchi C, Tomasoni S, Abbate M, Remuzzi G: Effect of combining ACE inhibitor and statin in severe experimental nephropathy. Kidney Int 61: 1635– 1645, 2002 11. Bos H, Henning RH, de Boer E, Tiebosch ATMG, de Jong PE, de Zeeuw D, Navis GJ: Addition of AT1 blocker fails to overcome resistance to ACE inhibition in adriamycin nephrosis. Kidney Int 61: 473– 480, 2002 12. Perico N, Amuchastegui SC, Colosio V, Sonzogni G, Bertani T, Remuzzi G: Evidence that an angiotensin-converting enzyme inhibitor has a different effect on glomerular injury according to the different phase of the disease at which the treatment is started. J Am Soc Nephrol 5: 1139 –1146, 1994 13. Donadelli R, Abbate M, Zanchi C, Corna D, Tomasoni S, Benigni A, Remuzzi G, Zoja C: Protein traffic activates NF-kB gene signaling and promotes MCP-1-dependent interstitial inflammation. Am J Kidney Dis 36: 1226 –1241, 2000 14. Ruggenenti P, Schieppati A, Remuzzi G: Progression, remission, regression of chronic renal diseases. Lancet 357: 1601–1608, 2001 15. Bos H, Andersen S, Rossing P, de Zeeuw D, Parving H-H, de Jong PE, Navis GJ: Role of patient factors in therapy resistance to antiproteinuric intervention in nondiabetic and diabetic nephropathy. Kidney Int 57(Suppl 75): S32–S37, 2000 16. Shiigai T, Shichiri M: Late escape from the antiproteinuric effect of ACE inhibitors in nondiabetic renal disease. Am J Kidney Dis 37: 477– 483, 2001 2907 17. Taal MW, Brenner BM: Renoprotective benefits of RAS inhibition: From ACEI to angiotensin II antagonists. Kidney Int 57: 1803–1817, 2000 18. Hilgers KF, Mann JFE: ACE inhibitors versus AT1 receptor antagonists in patients with chronic renal disease. J Am Soc Nephrol 13: 1100 –1108, 2002 19. Klahr S, Morrissey J: Angiotensin II and gene expression in the kidney. Am J Kidney Dis 31: 171–176, 1998 20. Ruiz-Ortega M, Lorenzo O, Suzuki Y, Ruperez M, Egido J: Proinflammatory actions of angiotensins. Curr Opin Nephrol Hypertens 10: 321–329, 2001 21. Komine N, Khang S, Wead LM, Blantz RC, Gabbai FB: Effect of combining an ACE inhibitor and an angiotensin II receptor blocker on plasma and kidney tissue angiotensin II levels. Am J Kidney Dis 39: 159 –164, 2002 22. Wilkinson-Berka JL, Gibbs NJ, Cooper ME, Skinner SL, Kelly DJ: Renoprotective and anti-hypertensive effects of combined valsartan and perindopril in progressive diabetic nephropathy in the transgenic (mRen-2)27 rat. Nephrol Dial Transplant 16: 1343–1349, 2001 23. Cao Z, Cooper ME, Wu LL, Cox AJ, Jandeleit-Dahm K, Kelly DJ, Gilbert RE: Blockade of the renin-angiotensin and endothelin systems on progressive renal injury. Hypertension 36: 561–568, 2000 24. Ots M, Mackenzie HS, Troy JL, Rennke HG, Brenner BM: Effects of combination therapy with Enalapril and Losartan on the rate of progression of renal injury in rats with 5/6 renal mass ablation. J Am Soc Nephrol 9: 224 –230, 1998 25. Russo D, Minutolo R, Pisani A, Esposito R, Signoriello G, Andreucci M, Balletta MM: Coadministration of losartan and enalapril exerts additive antiproteinuric effect in IgA nephropathy. Am J Kidney Dis 38: 18 –25, 2001 26. Mogensen CE, Neldam S, Tikkanen I, Oren S, Viskoper R, Watts RW, Cooper ME: Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: The Candesartan and Lisinopril Microalbuminuria (CALM) study. BMJ 321: 1440 –1444, 2000 27. Perticucci E, Campbell R, Perna A, Ferrari S, Cattaneo D, Ruggenenti P, Koleva NZ, Aros C, Remuzzi G: ACE inhibitors (ACEi), angiotensin II antagonists (ATA) or their combination: How to best renoprotect patients with non diabetic chronic nephropathies [Abstract]? J Am Soc Nephrol 12: 82A, 2001 28. Agarwal R: Add-on angiotensin receptor blockade with maximized ACE inhibition. Kidney Int 59: 2282–2289, 2001 29. Oda H, Keane WF: Recent advances in statins and the kidney. Kidney Int 56: S2–S5, 1999 30. Kim SI, Kim HJ, Han DC, Lee HB: Effect of lovastatin on small GTP binding proteins and on TGF-b1 and fibronectin expression. Kidney Int 58: S88 –S92, 2000 31. Park JK, Muller DN, Mervaala EM, Dechend R, Fiebeler A, Schmidt F, Bieringer M, Schafer O, Lindschau C, Schneider W, Ganten D, Luft FC, Haller H: Cerivastatin prevents angiotensin II-induced renal injury independent of blood pressure and cholesterol-lowering effects. Kidney Int 58: 1420 –1430, 2000 32. Brouhard BH, Takamori H, Satoh S, Inman S, Cressman M, Irwin K, Berkley V, Stowe N: The combination of lovastatin and enalapril in a model of progressive renal disease. Pediatr Nephrol 4: 436 – 440, 1994 33. Lee SK, Jin SY, Han DC, Hwang SD, Lee HB: Effects of delayed treatment with enalapril and/or lovastatin on the progres- 2908 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. Journal of the American Society of Nephrology sion of glomerulosclerosis in 5/6 nephrectomized rats. Nephrol Dial Transplant 8: 1338 –1343, 1993 Benigni A, Corna D, Maffi R, Benedetti G, Zoja C, Remuzzi G: Renoprotective effect of contemporary blocking of angiotensin II and endothelin-1 in rats with membranous nephropathy. Kidney Int 54: 353–359, 1998 Bauersachs J, Galuppo P, Fraccarollo D, Christ M, Ertl G: Improvement of left ventricular remodeling and function by hydroxymethylglutaryl coenzyme A reductase inhibition with cerivastatin in rats with heart failure after myocardial infarction. Circulation 104: 982–985, 2001 Borghi C, Veronesi M, Prandin MG, Dormi A, Ambrosioni E: Statins and blood pressure regulation. Curr Hypertens Rep 3: 281–288, 2001 The Gisen Group: Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet 349: 1857–1863, 1997 Taal MW, Brenner BM: Evolving strategies for renoprotection: Nondiabetic chronic renal disease. Curr Opin Nephrol Hypertens 10: 523–531, 2001 Ruggenenti P, Brenner BM, Remuzzi G: Remission achieved in chronic nephropathy by a multidrug approach targeted at urinary protein excretion. Nephron 88: 254 –259, 2001 Remuzzi A, Puntorieri S., Battaglia C, Bertani T, Remuzzi G: Angiotensin converting enzyme inhibition ameliorates glomerular filtration of macromolecules and water and lessens glomerular injury in the rat. J Clin Invest 85: 541–549, 1990 Remuzzi A, Perico N, Amuchastegui CS, Malanchini B, Mazerska M, Battaglia C, Bertani T, Remuzzi G: Short- and long-term effect of angiotensin II receptor blockade in rats with experimental diabetes. J Am Soc Nephrol 4: 40 – 49, 1993 Remuzzi A, Perico N, Sangalli F, Vendramin G, Moriggi M, Ruggenenti P, Remuzzi G: ACE inhibition and ANG II receptor blockade improve glomerular size-selectivity in IgA nephropathy. Am J Physiol 276: F457–F466, 1999 Ruggenenti P, Mosconi L, Vendramin G, Moriggi M, Remuzzi A, Sangalli F, Remuzzi G: ACE inhibition improves glomerular size selectivity in patients with idiopathic membranous nephropathy and persistent nephrotic syndrome. Am J Kidney Dis 35: 381–391, 2000 Wapstra FH, Navis GJ, van Goor H, van den Born J, Berden JHM, de Jong PE, de Zeeuw D: ACE inhibition preserves heparan sulfate proteoglycans in the glomerular basement membrane of rats with established adriamycin nephropathy. Exp Nephrol 9: 21–27, 2001 J Am Soc Nephrol 13: 2898–2908, 2002 45. Remuzzi A, Monaci N, Bonassi ME, Corna D, Zoja C, Mohammed EI, Remuzzi G: Angiotensin-converting enzyme inhibition prevents loss of glomerular hydraulic permeability in passive Heymann nephritis. Lab Invest 79: 1501–1510, 1999 46. Benigni A, Tomasoni S, Gagliardini E, Zoja C, Grunkemeyer JA, Kalluri R, Remuzzi G: Blocking angiotensin II synthesis/activity preserves glomerular nephrin in rats with severe nephrosis. J Am Soc Nephrol 12: 941–948, 2001 47. Benigni A, Gagliardini E, Remuzzi A, Corna D, Remuzzi G: Angiotensin-converting enzyme inhibition prevents glomerulartubule disconnection and atrophy in passive Heymann nephritis, an effect not observed with a calcium antagonist. Am J Pathol 159: 1743–1750, 2001 48. Moritomo Y, Hirano T, Ebara T, Kurokawa M, Naito H, Furukawa S, Nagano S: Fluvastatin, a new inhibitor of 3-hydroxy3-methylglutaryl coenzyme A reductase, suppresses very lowdensity lipoprotein secretion in puromycin aminonucleosidenephrotic rats. Nephron 67: 218 –225, 1994 49. Yoshimura A, Inui K, Nemoto T, Uda S, Sugenoya Y, Watanabe S, Yokota N, Taira T, Iwasaki S, Ideura T: Simvastatin suppresses glomerular cell proliferation and macrophage infiltration in rats with mesangial proliferative nephritis. J Am Soc Nephrol 9: 2027–2039, 1998 50. Luo J-D, Zhang W-W, Zhang G-P, Guan J-X, Chen X: Simvastatin inhibits cardiac hypertrophy and angiotensin-converting enzyme activity in rats with aortic stenosis. Clin Exp Pharmacol Physiol 26: 903–908, 1999 51. Wassmann S, Laufs U, Baumer AT, Muller K, Konkol C, Sauer H, Bohm M, Nickenig G: Inhibition of geranylgeranylation reduces angiotensin II-mediated free radical production in vascular smooth muscle cells: involvement of angiotensin AT1 receptor expression and Rac1 GTPase. Mol Pharmacol 59: 646 – 654, 2001 52. Nickenig G, Baumer AT, Temur Y, Kebben D, Jockenhovel F, Bohm M: Statin-sensitive dysregulated AT1 receptor function and density in hypercholesterolemic men. Circulation 100: 2131–2134, 1999 53. Guan S, Fox J, Mitchell KD, Navar LG: Angiotensin and angiotensin converting enzyme tissue levels in two-kidney, one clip hypertensive rats. Hypertension 20: 763–767, 1992 54. Gilbert RE, Wu LL, Kelly DJ, Cox A, Wilkinson-Berka JL, Johnston CI, Cooper ME: Pathological expression of renin and angiotensin II in the renal tubule after subtotal nephrectomy. Am J Pathol 155: 429 – 440, 1999 55. Kim SI, Han DC, Lee HB: Lovastatin inhibits transforming growth factor-b1 expression in diabetic rat glomeruli and cultured rat mesangial cells. J Am Soc Nephrol 11: 80 – 87, 2000 See related editorial, “The Next Treatments of Chronic Kidney Disease: If We Find Them, Can We Test Them,” on pages 3024 –3026.









© Copyright 2025