
Diffusing Capacity: How to Get It Right
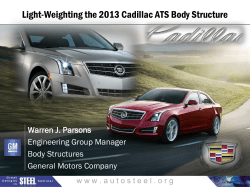
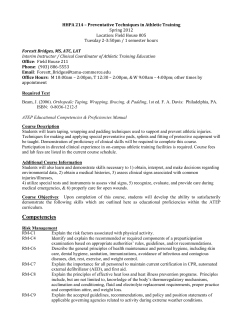
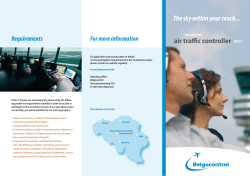
Diffusing Capacity: How to Get It Right Robert L Jensen PhD and Robert O Crapo MD Introduction Calculating Diffusing Capacity Measuring Diffusing Capacity Calibrating the Equipment Optimizing the Test Procedure Summary The carbon monoxide diffusing capacity test (DLCO) is a commonly performed pulmonary function test that requires technical expertise and attention to detail to get acceptable results. With the advent of automated devices and powerful computer programs, DLCO measurement has rapidly gained wide clinical acceptance. But there are many subtle aspects to performing the test that can diminish its accuracy and repeatability. The clinician must ensure: that the DLCO instrument is correctly calibrated; that inhalation is least 90% of the largest previously measured vital capacity; that the patient executes a quick, smooth inhalation within 2 seconds; that the breath-hold is 9 –11 seconds; that the breath-hold is without straining (no Valsalva or Mu¨ller maneuvers); that exhalation is quick and smooth; that a representative gas sample is obtained from the correct portion of the exhalation; and that at least 5 minutes elapse between DLCO tests. At least 2 but no more than 5 DLCO tests should be conducted, and testing is complete when 2 tests are within 10% or 3 DLCO units (mL CO/min/mm Hg) of each other. The reported DLCO value is the average of the first 2 tests that meet the reproducibility criteria, but if 5 tests are performed and no 2 meet the reproducibility criteria, the reported value is the average of the 2 tests with the highest inspiratory volumes. These quality controls will help laboratories achieve consistent high DLCO accuracy. Key words: diffusing capacity, DLCO, carbon monoxide, pulmonary function tests. [Respir Care 2003;48(8):777–782. © 2003 Daedalus Enterprises] Introduction The efficiency of the lung in transporting oxygen from the alveoli across the alveolar-capillary membrane and into hemoglobin within the red blood cells can be assessed by Robert L Jensen PhD and Robert O Crapo MD are affiliated with the Pulmonary Division, LDS Hospital, and the University of Utah, Salt Lake City, Utah. Dr Jensen presented a version of this report at the 18th Annual New Horizons Symposium, Pulmonary Function Testing in 2002: Updates and Answers, October 6, 2002, at the American Association for Respiratory Care’s 48th Internaitonal Respiratory Congress in Tampa, Florida. Correspondence: Robert L Jensen PhD, Pulmonary Division, LDS Hospital, 8th Avenue and C Street, Salt Lake City UT 84143. E-mail: ldrjens1@ihc.com. RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8 the carbon monoxide diffusing capacity test (DLCO).1,2 This is because carbon monoxide (CO) follows the same diffusion pathway as oxygen, and its uptake is relatively easy to measure. Like oxygen molecules, CO molecules move from the alveolar space across the lung membrane, into the plasma, into the red blood cells, and finally bind onto the hemoglobin molecules at the same sites as do oxygen molecules (Figure 1). The only major differences between CO and oxygen behavior are (1) the solubility of the gases in intercellular fluids and plasma and (2) how strongly these gas molecules adhere to the hemoglobin binding sites.3 Calculating Diffusing Capacity The single-breath DLCO test has been made widely available by manufacturers that have automated and comput- 777 DIFFUSING CAPACITY: HOW Fig. 1. The gas diffusion pathway is similar for carbon monoxide (CO) and oxygen (O2). Hb ⫽ hemoglobin. erized the procedure. All commercial systems conduct the test during a single-breath maneuver. A tracer gas (helium, neon, or methane) is also used to measure the initial dilution of the inhaled CO and to estimate alveolar volume. The fundamental equation to calculate DLCO is: DLCO ⫽ ˙ CO V PACO ⫺ Pc CO (1) ˙ CO is the rate of disappearance of CO; PACO is in which V the alveolar concentration of CO, which is determined from measuring the exhaled gas after the anatomical dead space (trachea and upper airways) has been cleared; and Pc CO is the partial pressure of CO in the blood. We can assume Pc CO is essentially zero, except in smokers and individuals exposed to CO. With this assumption the final equation then becomes: DLCO ⫽ ˙ CO V PACO (2) In North America the unit for DLCO is mL CO/min/mm Hg. The Syste`me Internationale unit is mmol/min/kPa, and in Europe the test is called the CO transfer factor. The following equation converts between the 2 units: DLCO ⫽ 2.986 ⫻ TLCO(SI) (3) Measuring Diffusing Capacity The basic measurement procedure is straightforward. The subject inhales a test gas containing 0.3% CO and a tracer (usually 0.3% CH4, 0.5% Ne, or 1–5% He), and a measurement is made of the exhaled concentrations of CO and the tracer after a breath-hold of about 10 seconds. The single-breath DLCO is not the only way to measure CO transport across the lung membrane. The intra-breath 778 TO GET IT RIGHT method, the steady state, and rebreathing methods can also measure CO transport. However, the single-breath DLCO has been extensively studied within healthy subjects, reference equations have been derived, and automated devices are commercially available; therefore, the singlebreath DLCO is at present the only method finding clinical utility. Further development is required before other DLCO methods will have similar clinical acceptance. The American Thoracic Society (ATS) has adopted standardized testing procedures and equipment recommendations for the single-breath DLCO.4 Standardization of testing procedures and equipment ensures that the test is performed consistently. These standards allow comparison of measurements from different pulmonary function laboratories. Several small studies have found that differences between measurements made with the same individual in several different laboratories can vary as much as 50%.5 Most the differences can be explained by procedural problems that, when addressed, reduce the differences. In measuring DLCO the first thing to recognize is that there are interactions: (1) between the subject and the testing device (eg, equipment placed in front of the patient’s face, mouthpieces), (2) between the technician and the subject, and (3) between the technician and the testing device. The condition of the subject is critical to the test. Several patient factors can affect the results. The subject should not have had any of the following: a meal within 2 hours of the test; recent strenuous exercise; ongoing or recent respiratory infection; or a blood alcohol level. The subject should already have had spirometry (to measure forced vital capacity or slow vital capacity), should be fully cooperative and able to follow instructions, and should be seated for the test session. Clear explanation of the testing procedure prior to the test is essential to obtaining good results. Demonstrating the maneuver to the patient, with a mouthpiece, can overcome some training and language problems.4 The standard procedure is to test the patient while he or she is seated in a stationary chair. The test should always be done with nose clips and the mouthpiece and valves placed at a comfortable level and position for the patient.4 Most devices have a screen display of patient breathing patterns prior to performing the test. During the “prebreath-hold” phase the patient is instructed to exhale completely (though this is not a forced maneuver), at which point valves are activated and the patient is instructed to inhale the test gas fully, in ⱕ 2 seconds, and hold the breath. It is very important that the patient rest against a closed glottis or the valve and not strain to pull in (Mu¨ller maneuver) or apply pressure by bearing down (Valsalva maneuver). The Mu¨ller maneuver will recruit blood to the lung and cause an inaccurately high DLCO reading, and the Valsalva maneuver will decrease the volume of blood in the lung and cause an inaccurately low DLCO reading. The RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8 DIFFUSING CAPACITY: HOW breath-hold period is about 10 seconds: the ATS standard is 9 –11 seconds.4 Most DLCO measuring devices display or indicate the end of the breath-hold period, and the patient is coached to exhale fully when the valves open or the time interval is completed. The ATS standard waiting period between consecutive DLCO maneuvers is 5 min, which ensures that all the test gas has washed out of the lungs. Even though the test seems simple, the results are affected by several factors, the most important of which are: 1. Inspired volume 2. Calibration 3. Sufficient washout volume 4. Representativeness of the sampled gas The inspired volume is critical to the test. Imagine if a subject only inhaled enough test gas to fill the anatomical dead space. No CO diffusion would occur and the effective DLCO measurement would be zero, since CO can only diffuse into the blood when it reaches the alveolar region. Even if the test gas enters the alveolar region, if the lung is not fully inflated, CO uptake will be inappropriately reduced because of incomplete membrane expansion. Thus, the inhalation must be at least 90% of the patient’s largest measured vital capacity, to ensure sufficient inhaled volume. This is why it is necessary to measure the patient’s vital capacity prior to the DLCO test. If the inspiratory volume is ⬍ 90% of the vital capacity the DLCO measurement will be inaccurately low and the patient might be misinterpreted as having below-normal DLCO. The way to obtain a good vital capacity measurement is the same as for all good quality spirometry. Obtain the following for each spirometry effort: 1. Full inspiration to total lung capacity 2. Quick forced expiration, without hesitation 3. Minimum of 6 seconds of exhalation 4. At least 3 acceptable trials 5. The reproducibility of the 2 best tests should be ⫾ 200 mL for both forced vital capacity and forced expiratory volume in the first second There are many excellent guides and books about spirometry testing. Every effort should be made to meet the ATS standards in the ATS manual of procedures.6 Though no laboratory can have all patients meet the ATS standards, even in laboratories that see numerous very sick patients the ATS standards can be met ⬎ 85% of the time. Calibrating the Equipment Calibration is always critical. It is the essential element in good quality control and accurate measurements. The ATS standards recommend that DLCO systems be calibrated daily, and twice daily in busy laboratories. Fortunately, the manufacturers have almost uniformly instrumented DLCO systems to perform gas calibrations just prior to each DLCO test. This reduces problems associated with RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8 TO GET IT RIGHT normal drift in the gas analyzer outputs, which greatly influence test results. However, the flow sensors and/or volume sensors are not recalibrated prior to each DLCO test and need to be recalibrated daily or twice daily. The volume measurement systems should be calibrated using a 3-L syringe that is in good condition and has had its accuracy certified by the factory or some other reputable source at some regular interval (1 or 2 y). Barometric pressure and temperature are also important. The DLCO calculations use barometric pressure measurements, so they should be accurate on average. The barometric pressure should be set to the normal average barometric pressure at your laboratory. Weather-related changes in barometric pressure will not greatly affect DLCO measurements. Temperature on the other hand is very important. Each 1° C of mismeasurement introduces a 0.67% error in the DLCO. That may not seem like much, but normal temperature variations in a laboratory can be up to 10° C per day and could introduce up to 7% error in the DLCO if not included in the DLCO calculations. Use a good electronic thermometer and consistently enter the temperature into the DLCO instrument to increase your DLCO accuracy. Confidence in volume measurements allows you to make correct judgments about the adequacy of inspired volumes. If these systems are not correctly volume-calibrated, a number of problems may occur: 1. The inspiratory volume can be erroneous, which can lead to incorrectly accepting or rejecting a maneuver based on the 90%-of-vital-capacity criteria 2. If inspiratory volume is mismeasured, then alveolar volume will be incorrect 3. DLCO may be incorrectly calculated 4. Valves may not open or close at the correct volumes or times One problem occasionally encountered is that the volume calibration for the DLCO system is done when the system is in a spirometry mode or configuration, after which the system is changed to a DLCO mode that may require adding valves or tubing to be placed near the flowsensor. Those changes in the physical configuration can alter the volume calibration characteristics. A simple check of the DLCO volume calibration can be done with a 3-L syringe DLCO test. First set up the system to do the test for a normal patient. Next attach a 3-L syringe to the mouthpiece. When the syringe is completely emptied, start the DLCO inhalation maneuver. Withdraw the full 3 L into the syringe, wait approximately 10 seconds, and then discharge the syringe back into the device. The measured inspiratory volume should be 3 L multiplied by the correction factor converting ambient-temperatureand-pressure-dry (ATPD) to body-temperature-and-pressure-saturated (BTPS). This factor is typically around 1.10, making the measured inspiratory volume around 3.33 L. 779 DIFFUSING CAPACITY: HOW TO GET IT RIGHT Fig. 3. Ideal tracing of a single-breath DLCO test. In the initial phase the inhaled volume and gas concentrations rise. The plateau of the curve represents the breath-hold phase. In the exhalation phase lung volume decreases sharply (%VC ⫽ percent of vital capacity), whereas carbon monoxide concentration ([CO]) decreases more gradually, and the tracer decreases and then reaches a plateau. Fig. 2. A DLCO simulator designed to test the accuracy of DLCO measurement instruments. The simulator produces known volumes of precision gases that simulate human breath. The device can reliably simulate the same value to within fractions of a DLCO unit (mm CO/min/mm Hg). (Courtesy Hans Rudolph Inc, Kansas City, Missouri) The measured DLCO should be zero, since no CO diffusion can occur in the syringe. A new device has become available for testing DLCO instruments (Figure 2).7 It uses precision syringes in conjunction with precision mixed gases to simulate volumes and gas concentrations that would be measured from a human subject. A software calculator records the values the instrument measures and reports differences for each aspect of the DLCO measurement, including gas concentrations, volumes, and final DLCO calculations. If the DLCO measurement device does not report the target DLCO, the problem can be easily identified as a volume, carbon monoxide, or tracer measurement failure. Optimizing the Test Procedure The washout volume is the volume of gas that must leave the lungs so that all remaining gas exiting the lungs is gas from the alveolar gas-exchanging regions and not 780 from the trachea and upper airways, where no gas exchange occurs. The ATS standards recommend a minimum washout volume of 750 mL.4 Some instruments use rapid gas analyzers that display the gas concentration curves and allow the user to adjust the washout volume. For those types of instruments the washout volume is adjusted so the tracer concentration reaches a plateau and the CO concentration indicates alveolar gas (Figure 3). Obtaining a representative sample of the alveolar gas is key to obtaining a representative DLCO measurement. When rapid gas analyzers are used and the graphical output of these is displayed for review, determining if the gas samples are from the correct part of the exhaled gas volume is made simple by visually inspecting the curves. Somewhere between 0.75 and 1.5 L of gas should be used for the gas analysis. When curves are not available, we can only assume that the washout and sample volumes are appropriate and that the correct gas concentration measurements were made (Figure 4). Achieving good control of the technical aspects of the DLCO test is the first step toward getting excellent results. Applying quality control procedures to your laboratory will help ensure that your results are consistently excellent. Quality control for the DLCO test includes (1) immediate appraisal of the test and (2) reproducibility of multiple test maneuvers. Immediate appraisal includes: 1. Inhalation to at least 90% of the largest previously measured vital capacity 2. Quick, smooth inhalation within 2 seconds 3. Breath-hold of 9 –11 seconds 4. Hold the breath without straining (no Valsalva or Mu¨ ller maneuvers) 5. Quick smooth exhalation 6. Check the washout and sample volumes if the device allows 7. Wait at least 5 min between DLCO tests RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8 DIFFUSING CAPACITY: HOW TO GET IT RIGHT Fig. 4. An actual DLCO tracing, showing the instrument’s automated selection for the washout volume (discard) and the sample volume (collection). The upper panel shows the first trial and lower panel shows the second trial. Note the differences in washout volumes (Trial 1 ⫽ 1.21 L, Trial 2 ⫽1.66 L) and collection volumes (Trial 1 ⫽ 0.87 L, Trial 2 ⫽ 0.75 L); these values are determined from the part of the curve that decreases after the plateau. Correct setting of the washout and collection volumes will produce different values for each test. RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8 781 DIFFUSING CAPACITY: HOW These quality control measures ensure that each individual test is performed well. Following these guidelines can help identify methodological problems that might lead to erroneous DLCO values. When problems are identified, an individual test can be discarded rather than sent for interpretation. Reproducibility is the second aspect: 1. Perform at least 2 but no more than 5 DLCO tests 2. Testing is complete when 2 tests are within 10% or 3 DLCO units (mL CO/min/mm Hg) of each other 3. The reported DLCO value is the average of the first 2 tests that meet the reproducibility criteria. However, if 5 tests are performed and no two meet the reproducibility criteria, the reported value is the average of the 2 tests with the highest inspiratory volumes. Following these simple quality control procedures will reduce noise in your data, ensure that your DLCO values are accurate, allow better diagnosis with the DLCO values, and allow better assessment of DLCO trends or changes when patients return for follow-up tests. The choice of reference values for DLCO is made by the individual laboratory.8 However, several surveys have found that a large number of laboratories were using the reference values that were the factory defaults when they purchased the device. Each laboratory’s staff should review with their medical director their choice of reference equations and should document their choice. See Crapo and Jensen’s review of reference equations in this issue of RESPIRATORY CARE.9 There is no way to describe the complex understanding that each pulmonary technician has of the equipment, laboratory, and individual characteristics of each patient being tested. To obtain consistently representative results, be alert for peculiarities in the testing, abnormally high or low 782 TO GET IT RIGHT gas concentrations, or suspicious attributes or breathing patterns, and always consider if the results seem to fit the clinical impressions for the subject. Summary The clinician must pay careful attention to calibration and the test procedure to maximize the consistency and value of DLCO results. REFERENCES 1. Comroe JH Jr. Pulmonary diffusing capacity for carbon monoxide (DLCO). Am Rev Repir Dis 1975;111(2):225–228. 2. Krogh M. The diffusion of gases through the lungs of man. J Physiol 1914;49:271–300. 3. Forster RE, Fowler D, Bates V, Van Lingen B. The absorption of carbon monoxide by the lungs during breathholding. J Clin Invest 1954;33:1135–1145. 4. American Thoracic Society. Single-breath carbon monoxide diffusing capacity (transfer factor): recommendations for a standard technique—1995 update. Am J Respir Crit Care Med 1995;152(6 Pt 1):2185–2198. 5. Wanger J, Irvin C. Comparability of pulmonary function results from 13 laboratories in a metropolitan area. Respir Care 1991;36(12): 1375–1382. 6. Wanger J. Editor-in Chief. Pulmonary function laboratory management and procedure manual. A project of the American Thoracic Society. 1998. Available at http://www.thoracic.org/education/labmanual.asp (accessed 6/11/03). 7. Glissmeyer EW, Jensen RL, Crapo RO, Greenway LW. Initial testing with a carbon monoxide diffusing capacity simulator (abstract). J Investig Med 1999;47:37A. 8. American Thoracic Society. Lung function testing: selection of reference values and interpretative strategies. Am Rev Respir Dis 1991; 144(5):1202–1218. 9. Crapo RO, Jensen RL. Standards and interpretive issues in lung function testing. Respir Care 2003;48(8):764–772. RESPIRATORY CARE • AUGUST 2003 VOL 48 NO 8







© Copyright 2025