
HOW TO SURVIVE THE APPLICATION PROCESS
HOW TO SURVIVE THE
APPLICATION
PROCESS
Jeanne Maxwell, Esq.
Director of Grants Development & Compliance
Jeanne.maxwell@agr.georgia.gov
404-657-1584
and
Natalie Adan
Food Processing Manager
Natalie.adan@agr.georgia.gov
404-656-3627
Georgia Department of Agriculture
HOW TO SURVIVE THE
APPLICATION PROCESS
------------ATTENDEE INFORMATION PACKET
1. RFA Summary email
2. Grant Application Package
3. Reporting Requirements document
1. RFA – SUMMARY EMAIL
FDA – ADVANCING CONFORMANCE WITH THE VOLUNTARY NATIONAL RETAIL FOOD REGULATORY PROGRAM STANDARDS (VNRFRPS) RFA‐FD‐12‐011 (U18) DUE: MONDAY, JULY 16, 2012/JULY 9 or 10, 2012 $1,700,000 AWARD TOTAL 25‐30 AWARDS $60,000 MAXIMUM PER PROJECT‐ONE YEAR/+ FOUR MORE YEARS = $300,000 TOTAL NO COST SHARING REQUIRED Below is a listing of information we need to include within our application for this cooperative agreement/grant: 1. Project Summary – a summary of our project suitable for dissemination to the public (a statement of objectives and methods) – 30 lines maximum. 2. Project Narrative – describe the relevance of our project to the public health – 2‐3 sentences. 3. Specific Aims – this is a separate attached document – state concisely the goals of the proposed research and summarize the expected outcome(s), including the impact that the results will have; include the specific objectives – one page maximum. 4. *Research Strategy – this is the “meat” of the application – 15 pages maximum. 5. Budget Justification – this is a separate attached document – an explanation of all costs included within the Research and Related Budget spreadsheet, for all five years. 6. Budget Spreadsheet – need to complete one for each of the five years of the cooperative agreement/grant. 7. Biosketches – these are separate attached documents – in addition to the PD/PI, it may also be a good idea to include anyone who will work on the project. In fact, we may want to include a separate attachment listing information on all of the project workers. *RESEARCH STRATEGY SECTION: Usually categorized, but not required: (This information is found within the US Department of Health and Human Services SF 424 R&R Manual; p. I 110) (a) Significance (b) Innovation (c) Approach WITHIN THIS SECTION, BE SURE TO INCLUDE: Program assessment, improvement, and collaboration to accomplish the work below: The long‐term goals listed at the top of page 5 of the RFA. The six objectives listed on p. 14‐15 of the RFA. The four “outcomes” of the work listed on page 5 of the RFA. Demonstrate that capabilities can be sustained after the conclusion of the project period. Expected challenges should be documented and addressed. Develop strategies for achieving and sustaining conformance with the Retail Program Standards that can be shared and duplicated by other agencies. Show extensive cooperation and coordination with FDA Regional Offices and other FDA program offices. Identify the timeframes, personnel and other resources (e.g., supplies; training; equipment‐‐including investigational, GPS interface, communication, and laboratory) required for implementation. Include that all reporting requirements will be satisfied (mid‐year progress report; annual progress report; and final progress report). Justification for hiring new staff. Specific cost information is located on pages 12‐13 of the RFA. Indirect Cost rate is 20.23 percent ($12,138/yr; $60,690 total). Fringe Benefits rate is 52.123 percent. We need to include when we enrolled in the VNRFRPS and when we completed our self‐assessment against the Retail Program Standards as required by Standard 9. We must also show previous and subsequent years of state funding (to show that this cooperative agreement/grant is “supplementing, not replacing state funding for the program and activities”). Scoring evaluation is described on page 15 of the RFA. Please email me drafts of the Research Strategy section and any attachments in Word format; the attachments will be converted to PDFs when we submit our application. As the final due date for our application is Monday, July 16, I must submit it earlier, preferably by July 9 or 10. Please call me if you have any questions!! Jeanne 404‐657‐1584 2. GRANT APPLICATION PACKAGE
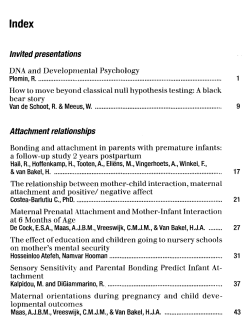
Grant Application Package
Opportunity Title:
Limited Competition: Advancing Conformance with the Vol
Offering Agency:
Food & Drug Administration
CFDA Number:
93.103
CFDA Description:
Food and Drug Administration_Research
Opportunity Number:
RFA-FD-12-011
This electronic grants application is intended to
be used to apply for the specific Federal funding
opportunity referenced here.
Competition ID:
Opportunity Open Date:
06/04/2012
Opportunity Close Date:
Agency Contact:
07/16/2012
If the Federal funding opportunity listed is not
the opportunity for which you want to apply,
close this application package by clicking on the
"Cancel" button at the top of this screen. You
will then need to locate the correct Federal
funding opportunity, download its application
and then apply.
Daniel Lukash
Grants Management Specialist
E-mail: daniel.lukash@fda.hhs.gov
Phone: 301-827-6771
This opportunity is only open to organizations, applicants who are submitting grant applications on behalf of a company, state, local or
tribal government, academia, or other type of organization.
* Application Filing Name:
Mandatory Documents
Move Form to
Complete
Move Form to
Delete
Optional Documents
R & R Subaward Budget Attachment(s) Form 5 YR 3
Move Form to
Submission List
Mandatory Documents for Submission
SF424 (R & R)
Project/Performance Site Location(s)
Research And Related Other Project Information
Research And Related Senior/Key Person Profile
Research & Related Budget
PHS 398 Cover Page Supplement
PHS 398 Research Plan
Optional Documents for Submission
PHS Cover Letter
Move Form to
Delete
Instructions
1
Enter a name for the application in the Application Filing Name field.
2
Open and complete all of the documents listed in the "Mandatory Documents" box. Complete the SF-424 form first.
- This application can be completed in its entirety offline; however, you will need to login to the Grants.gov website during the submission process.
- You can save your application at any time by clicking the "Save" button at the top of your screen.
- The "Save & Submit" button will not be functional until all required data fields in the application are completed and you clicked on the "Check Package for Errors" button and
confirmed all data required data fields are completed.
- It is recommended that the SF-424 form be the first form completed for the application package. Data entered on the SF-424 will populate data fields in other mandatory and
optional forms and the user cannot enter data in these fields.
- The forms listed in the "Mandatory Documents" box and "Optional Documents" may be predefined forms, such as SF-424, forms where a document needs to be attached,
such as the Project Narrative or a combination of both. "Mandatory Documents" are required for this application. "Optional Documents" can be used to provide additional
support for this application or may be required for specific types of grant activity. Reference the application package instructions for more information regarding "Optional
Documents".
- To open and complete a form, simply click on the form's name to select the item and then click on the => button. This will move the document to the appropriate "Documents
for Submission" box and the form will be automatically added to your application package. To view the form, scroll down the screen or select the form name and click on the
"Open Form" button to begin completing the required data fields. To remove a form/document from the "Documents for Submission" box, click the document name to select it,
and then click the <= button. This will return the form/document to the "Mandatory Documents" or "Optional Documents" box.
- All documents listed in the "Mandatory Documents" box must be moved to the "Mandatory Documents for Submission" box. When you open a required form, the fields which
must be completed are highlighted in yellow with a red border. Optional fields and completed fields are displayed in white. If you enter invalid or incomplete information in a
field, you will receive an error message.
3
Click the "Save & Submit" button to submit your application to Grants.gov.
- Once you have properly completed all required documents and attached any required or optional documentation, save the completed application by clicking on the "Save"
button.
- Click on the "Check Package for Errors" button to ensure that you have completed all required data fields. Correct any errors or if none are found, save the application
package.
- The "Save & Submit" button will become active; click on the "Save & Submit" button to begin the application submission process.
- You will be taken to the applicant login page to enter your Grants.gov username and password. Follow all onscreen instructions for submission.
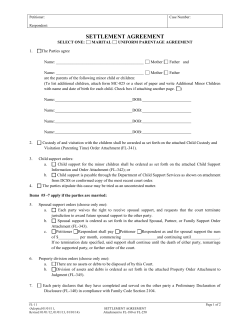
OMB Number: 4040-0001
Expiration Date: 06/30/2011
APPLICATION FOR FEDERAL ASSISTANCE
3. DATE RECEIVED BY STATE
SF 424 (R&R)
1. * TYPE OF SUBMISSION
Pre-application
State Application Identifier
4. a. Federal Identifier
Application
Changed/Corrected Application
b. Agency Routing Identifier
Applicant Identifier
2. DATE SUBMITTED
5. APPLICANT INFORMATION
* Organizational DUNS:
* Legal Name:
Department:
Division:
* Street1:
Street2:
* City:
County / Parish:
Province:
* State:
* Country:
* ZIP / Postal Code:
USA: UNITED STATES
Person to be contacted on matters involving this application
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
* Phone Number:
Fax Number:
Email:
6. * EMPLOYER IDENTIFICATION (EIN) or (TIN):
7. * TYPE OF APPLICANT:
Please select one of the following
Other (Specify):
Small Business Organization Type
Women Owned
8. * TYPE OF APPLICATION:
New
If Revision, mark appropriate box(es).
Resubmission
Renewal
Socially and Economically Disadvantaged
Continuation
A. Increase Award
Revision
B. Decrease Award
C. Increase Duration
E. Other (specify):
* Is this application being submitted to other agencies? Yes
No
9. * NAME OF FEDERAL AGENCY:
What other Agencies?
10. CATALOG OF FEDERAL DOMESTIC ASSISTANCE NUMBER: 93.103
TITLE: Food and Drug Administration_Research
Food & Drug Administration
11. * DESCRIPTIVE TITLE OF APPLICANT'S PROJECT:
12. PROPOSED PROJECT:
* Start Date
* Ending Date
* 13. CONGRESSIONAL DISTRICT OF APPLICANT
14. PROJECT DIRECTOR/PRINCIPAL INVESTIGATOR CONTACT INFORMATION
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
Position/Title:
* Organization Name:
Department:
Division:
* Street1:
Street2:
* City:
County / Parish:
* State:
* Country:
* Phone Number:
* Email:
D. Decrease Duration
Province:
USA: UNITED STATES
Fax Number:
* ZIP / Postal Code:
SF 424 (R&R)
Page 2
APPLICATION FOR FEDERAL ASSISTANCE
15. ESTIMATED PROJECT FUNDING
16. * IS APPLICATION SUBJECT TO REVIEW BY STATE EXECUTIVE
ORDER 12372 PROCESS?
a. Total Federal Funds Requested
a. YES
THIS PREAPPLICATION/APPLICATION WAS MADE
AVAILABLE TO THE STATE EXECUTIVE ORDER 12372
PROCESS FOR REVIEW ON:
b. Total Non-Federal Funds
DATE:
c. Total Federal & Non-Federal Funds
b. NO
d. Estimated Program Income
PROGRAM IS NOT COVERED BY E.O. 12372; OR
PROGRAM HAS NOT BEEN SELECTED BY STATE FOR
REVIEW
17. By signing this application, I certify (1) to the statements contained in the list of certifications* and (2) that the statements herein are
true, complete and accurate to the best of my knowledge. I also provide the required assurances * and agree to comply with any resulting
terms if I accept an award. I am aware that any false, fictitious. or fraudulent statements or claims may subject me to criminal, civil, or
administrative penalities. (U.S. Code, Title 18, Section 1001)
* I agree
* The list of certifications and assurances, or an Internet site where you may obtain this list, is contained in the announcement or agency specific instructions.
18. SFLLL or other Explanatory Documentation
Add Attachment
Delete Attachment
View Attachment
19. Authorized Representative
Prefix:
* First Name:
Middle Name:
Suffix:
* Last Name:
* Position/Title:
* Organization:
Department:
Division:
* Street1:
Street2:
* City:
County / Parish:
Province:
* State:
* Country:
USA: UNITED STATES
* Phone Number:
* ZIP / Postal Code:
Fax Number:
* Email:
* Date Signed
* Signature of Authorized Representative
Completed on submission to Grants.gov
20. Pre-application
Completed on submission to Grants.gov
Add Attachment
Delete Attachment
View Attachment
Project/Performance Site Location(s)
Project/Performance Site Primary Location
OMB Number: 4040-0010
Expiration Date: 08/31/2011
I am submitting an application as an individual, and not on behalf of a company, state,
local or tribal government, academia, or other type of organization.
Organization Name:
DUNS Number:
* Street1:
Street2:
* City:
County:
* State:
Province:
* Country:
USA: UNITED STATES
* ZIP / Postal Code:
Project/Performance Site Location 1
* Project/ Performance Site Congressional District:
I am submitting an application as an individual, and not on behalf of a company, state,
local or tribal government, academia, or other type of organization.
Organization Name:
DUNS Number:
* Street1:
Street2:
County:
* City:
* State:
Province:
* Country:
USA: UNITED STATES
* ZIP / Postal Code:
Additional Location(s)
* Project/ Performance Site Congressional District:
Add Attachment
Delete Attachment
View Attachment
RESEARCH & RELATED Other Project Information
1. * Are Human Subjects Involved?
1.a
No
Yes
If YES to Human Subjects
Is the Project Exempt from Federal regulations?
Yes
If yes, check appropriate exemption number.
If no, is the IRB review Pending?
1
Yes
No
2
3
4
5
6
No
IRB Approval Date:
Human Subject Assurance Number:
2. * Are Vertebrate Animals Used?
2.a.
Yes
No
If YES to Vertebrate Animals
Is the IACUC review Pending?
Yes
No
IACUC Approval Date:
Animal Welfare Assurance Number
3. * Is proprietary/privileged information included in the application?
Yes
4.a. * Does this project have an actual or potential impact on the environment?
No
Yes
No
4.b. If yes, please explain:
4.c. If this project has an actual or potential impact on the environment, has an exemption been authorized or an environmental assessment (EA) or
environmental impact statement (EIS) been performed?
Yes
No
4.d. If yes, please explain:
5. * Is the research performance site designated, or eligible to be designated, as a historic place?
Yes
No
6. * Does this project involve activities outside of the United States or partnerships with international collaborators?
Yes
5.a. If yes, please explain:
No
6.a. If yes, identify countries:
6.b. Optional Explanation:
7. * Project Summary/Abstract
Add Attachment
Add Attachment
8. * Project Narrative
9. Bibliography & References Cited
Add Attachment
11. Equipment
Add Attachment
Add Attachments
Delete Attachment
Add Attachment
10. Facilities & Other Resources
12. Other Attachments
Delete Attachment
Delete Attachments
Delete Attachment
View Attachments
View Attachment
View Attachment
Delete Attachment
Delete Attachment
View Attachment
View Attachment
View Attachment
OMB Number: 4040-0001
Expiration Date: 06/30/2011
RESEARCH & RELATED Senior/Key Person Profile (Expanded)
PROFILE - Project Director/Principal Investigator
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
Position/Title:
Department:
Organization Name:
Division:
* Street1:
Street2:
* City:
County/ Parish:
* State:
Province:
* Country: USA: UNITED STATES
* Zip / Postal Code:
* Phone Number:
Fax Number:
* E-Mail:
Credential, e.g., agency login:
* Project Role:
Other Project Role Category:
PD/PI
Degree Type:
Degree Year:
*Attach Biographical Sketch
Add Attachment
Delete Attachment
View Attachment
Attach Current & Pending Support
Add Attachment
Delete Attachment
View Attachment
PROFILE - Senior/Key Person 1
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
Position/Title:
Department:
Organization Name:
Division:
* Street1:
Street2:
* City:
County/ Parish:
* State:
Province:
* Country: USA: UNITED STATES
* Zip / Postal Code:
* Phone Number:
Fax Number:
* E-Mail:
Credential, e.g., agency login:
* Project Role:
Other Project Role Category:
Degree Type:
Degree Year:
*Attach Biographical Sketch
Add Attachment
Delete Attachment
View Attachment
Attach Current & Pending Support
Add Attachment
Delete Attachment
View Attachment
Delete Entry
Next Person
To ensure proper performance of this form; after adding 20 additional Senior/ Key Persons; please save your application, close the Adobe
Reader, and reopen it.
* First Name
* Last Name
Suffix
Total Number Other Personnel
Secretarial/Clerical
Undergraduate Students
Graduate Students
Post Doctoral Associates
PD/PI
Add Attachment
* Project Role
Budget Period 1
* Project Role
RESEARCH & RELATED Budget {A-B} (Funds Requested)
* Number of
Personnel
B. Other Personnel
Additional Senior Key Persons:
9. Total Funds requested for all Senior Key Persons in the attached file
8.
7.
6.
5.
4.
3.
2.
Prefix
* End Date:
Subaward/Consortium
Middle Name
* Start Date:
A. Senior/Key Person
1.
Project
Enter name of Organization:
* Budget Type:
* ORGANIZATIONAL DUNS:
* Fringe
Benefits ($)
* Fringe
Benefits ($) * Funds Requested ($)
* Funds Requested ($)
Total Salary, Wages and Fringe Benefits (A+B)
Total Other Personnel
Cal.
Acad.
Sum. * Requested
Months Months Months
Salary ($)
Total Senior/Key Person
* Requested
Salary ($)
View Attachment
Cal.
Acad. Sum.
Months Months Months
Delete Attachment
Base Salary ($)
RESEARCH & RELATED BUDGET - SECTION A & B, BUDGET PERIOD 1
OMB Number: 4040-0001
Expiration Date: 06/30/2011
Close Form
RESEARCH & RELATED BUDGET - SECTION C, D, & E, BUDGET PERIOD 1
* ORGANIZATIONAL DUNS:
* Budget Type:
Project
Subaward/Consortium
Enter name of Organization:
* Start Date:
Budget Period 1
* End Date:
C. Equipment Description
List items and dollar amount for each item exceeding $5,000
Equipment item
* Funds Requested ($)
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11. Total funds requested for all equipment listed in the attached file
Total Equipment
Additional Equipment:
Add Attachment
Delete Attachment
Funds Requested ($)
D. Travel
1.
Domestic Travel Costs ( Incl. Canada, Mexico and U.S. Possessions)
2.
Foreign Travel Costs
Total Travel Cost
Funds Requested ($)
E. Participant/Trainee Support Costs
1.
Tuition/Fees/Health Insurance
2.
Stipends
3.
Travel
4.
Subsistence
5.
Other
Number of Participants/Trainees
Total Participant/Trainee Support Costs
RESEARCH & RELATED Budget {C-E} (Funds Requested)
View Attachment
Close Form
RESEARCH & RELATED BUDGET - SECTION F-K, BUDGET PERIOD 1
* ORGANIZATIONAL DUNS:
* Budget Type:
Project
Subaward/Consortium
Enter name of Organization:
* Start Date:
Budget Period 1
* End Date:
F. Other Direct Costs
Funds Requested ($)
1. Materials and Supplies
2. Publication Costs
3. Consultant Services
4. ADP/Computer Services
5. Subawards/Consortium/Contractual Costs
6. Equipment or Facility Rental/User Fees
7. Alterations and Renovations
8.
9.
10.
Total Other Direct Costs
G. Direct Costs
Funds Requested ($)
Total Direct Costs (A thru F)
H. Indirect Costs
Indirect Cost
Rate (%)
Indirect Cost Type
Indirect Cost
Base ($)
* Funds Requested ($)
1.
2.
3.
4.
Total Indirect Costs
Cognizant Federal Agency
(Agency Name, POC Name, and POC Phone Number)
I. Total Direct and Indirect Costs
Funds Requested ($)
Total Direct and Indirect Institutional Costs (G + H)
Funds Requested ($)
J. Fee
K. * Budget Justification
Add Attachment
(Only attach one file.)
RESEARCH & RELATED Budget {F-K} (Funds Requested)
Delete Attachment
View Attachment
RESEARCH & RELATED BUDGET - Cumulative Budget
Totals ($)
Section A, Senior/Key Person
Section B, Other Personnel
Total Number Other Personnel
Total Salary, Wages and Fringe Benefits (A+B)
Section C, Equipment
Section D, Travel
1. Domestic
2. Foreign
Section E, Participant/Trainee Support Costs
1. Tuition/Fees/Health Insurance
2. Stipends
3. Travel
4. Subsistence
5. Other
6. Number of Participants/Trainees
Section F, Other Direct Costs
1. Materials and Supplies
2. Publication Costs
3. Consultant Services
4. ADP/Computer Services
5. Subawards/Consortium/Contractual Costs
6. Equipment or Facility Rental/User Fees
7. Alterations and Renovations
8. Other 1
9. Other 2
10. Other 3
Section G, Direct Costs (A thru F)
Section H, Indirect Costs
Section I, Total Direct and Indirect Costs (G + H)
Section J, Fee
PHS 398 Cover Page Supplement
1. Project Director / Principal Investigator (PD/PI)
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
2. Human Subjects
Clinical Trial?
No
Yes
* Agency-Defined Phase III Clinical Trial?
No
Yes
3. Applicant Organization Contact
Person to be contacted on matters involving this application
* First Name:
Prefix:
Middle Name:
* Last Name:
Suffix:
* Phone Number:
Fax Number:
Email:
* Title:
* Street1:
Street2:
* City:
County/Parish:
* State:
Province:
* Country:
USA: UNITED STATES
* Zip / Postal Code:
OMB Number: 0925-0001
PHS 398 Cover Page Supplement
4. Human Embryonic Stem Cells
* Does the proposed project involve human embryonic stem cells?
No
Yes
If the proposed project involves human embryonic stem cells, list below the registration number of the
specific cell line(s) from the following list: http://stemcells.nih.gov/research/registry/. Or, if a specific
stem cell line cannot be referenced at this time, please check the box indicating that one from the
registry will be used:
Cell Line(s):
Specific stem cell line cannot be referenced at this time. One from the registry will be used.
OMB Number: 0925-0001
PHS 398 Research Plan
1. Application Type:
From SF 424 (R&R) Cover Page. The response provided on that page, regarding the type of application being submitted, is repeated for your
reference, as you attach the appropriate sections of the Research Plan.
*Type of Application:
New
Resubmission
Renewal
Continuation
Revision
2. Research Plan Attachments:
Please attach applicable sections of the research plan, below.
1. Introduction to Application
Add Attachment
Delete Attachment
View Attachment
2. Specific Aims
Add Attachment
Delete Attachment
View Attachment
3. *Research Strategy
Add Attachment
Delete Attachment
View Attachment
4. Inclusion Enrollment Report
Add Attachment
Delete Attachment
View Attachment
5. Progress Report Publication List
Add Attachment
Delete Attachment
View Attachment
6. Protection of Human Subjects
Add Attachment
Delete Attachment
View Attachment
7. Inclusion of Women and Minorities
Add Attachment
Delete Attachment
View Attachment
8. Targeted/Planned Enrollment Table
Add Attachment
Delete Attachment
View Attachment
9. Inclusion of Children
Add Attachment
Delete Attachment
View Attachment
10. Vertebrate Animals
Add Attachment
Delete Attachment
View Attachment
11. Select Agent Research
Add Attachment
Delete Attachment
View Attachment
12. Multiple PD/PI Leadership Plan
Add Attachment
Delete Attachment
View Attachment
13. Consortium/Contractual Arrangements
Add Attachment
Delete Attachment
View Attachment
14. Letters of Support
Add Attachment
Delete Attachment
View Attachment
15. Resource Sharing Plan(s)
Add Attachment
Delete Attachment
View Attachment
(for RESUBMISSION or REVISION only)
Human Subjects Sections
Other Research Plan Sections
16. Appendix
Add Attachments
Remove Attachments
View Attachments
Close Form
Next
Print Page
About
PHS 398 Checklist
OMB Number: 0925-0001
1. Application Type:
From SF 424 (R&R) Cover Page. The responses provided on the R&R cover page are repeated here for your reference, as you answer
the questions that are specific to the PHS398.
* Type of Application:
New
Resubmission
Renewal
Continuation
Revision
Federal Identifier:
2. Change of Investigator / Change of Institution Questions
Change of principal investigator / program director
Name of former principal investigator / program director:
Prefix:
* First Name:
Middle Name:
* Last Name:
Suffix:
Change of Grantee Institution
* Name of former institution:
3. Inventions and Patents
* Inventions and Patents:
Yes
(For renewal applications only)
No
If the answer is "Yes" then please answer the following:
* Previously Reported:
Yes
No
4. * Program Income
Is program income anticipated during the periods for which the grant support is requested?
Yes
No
If you checked "yes" above (indicating that program income is anticipated), then use the format below to reflect the amount and
source(s). Otherwise, leave this section blank.
*Budget Period
*Anticipated Amount ($)
*Source(s)
5. * Disclosure Permission Statement
If this application does not result in an award, is the Government permitted to disclose the title of your proposed project, and the name,
address, telephone number and e-mail address of the official signing for the applicant organization, to organizations that may be
interested in contacting you for further information (e.g., possible collaborations, investment)?
Yes
No
PHS Cover Letter
OMB Numbers: 0925-0001
0925-0002
*Mandatory Cover Letter Filename:
Add Cover Letter File
Delete Cover Letter File
View Cover Letter File
3. REPORTING REQUIREMENTS
VOLUNTARY NATIONAL RETAIL FOOD REGULATORY PROGRAM STANDARDS RFA‐FD‐12‐011 ‐ $70,000 x 5 Years 9/10/12 – 6/30/2017 REPORTING REQUIREMENTS – Funding Source #2850 REPORT UPDATED 2/19/13 The required mid‐year/yearly/final progress and financial reports, with their due dates, are listed below. I will send you reminder emails approximately three to four weeks before each due date. All reports are to be emailed to me for review; the revised reports will be sent to FDA from my office. Please contact me if you have any questions (extension 2603). YEAR 1 – September 10, 2012 – June 30, 2013 WE MUST PROVIDE DETAILED RESPONSES TO THE TWO WEAKNESSES (SEE BELOW) IDENTIFIED IN OUR SUMMARY STATEMENT, TO BE INCLUDED WITH OUR MID‐YEAR REPORT: The rationale and design to meet the goals and project milestones of the cooperative agreement: Strengths: The program enrolled in the VNRFRPS in 2001 and now has a renewed commitment. The proposal included plans to hire, train, and standardize a Retail Standards Manager to oversee the VNRFRPS implantation and conformance. The current Retail Food Regulation will be rewritten to the 2013 version of the FDA Model Food Code. The program has Standardized Retail Field staff. The program plans to overhaul outmoded Field Inspection Manual with written policies, operating procedures, and MOU’s required by the Retail Standards. Plans to apply the new Integration System for Manufactured Foods with a new inspection form and electronic inspection software to retail risk based inspections. The applicant has already performed a self‐assessment to gauge their current compliance with the VNRFRPS. The application shows a strong recommitment to the Retail Standards. The agency will utilize some of the existing Manufactured Foods Program structure. Some of the background agency assessment has already been conducted. Weaknesses: In recent years, the program’s involvement in the VNRFRPS has been delayed due to personnel changes and lack of available funding. Demonstrates that capabilities that can be sustained after the conclusion of the project period. Expected challenges should be documented and addressed: Strengths: There is a renewed commitment by the department for personnel, resources and funding. Sustainability is built into the project strategy. This funding will allow time and resources for updating written policies and procedures for consistency. Challenges were identified and explained. Weaknesses: The proposal did not provide details on sustaining the program. There is a commitment to continue to sustain the development and implementation of the Retail Program Standards beyond the conclusion of the project period; however, how this will be accomplished is unclear. Sustainability was mentioned, but no details were provided. March 12, 2013 – Mid‐Year Progress Report ‐ Contains a description of project activities covering a six‐month period (9/2012 – 3/12/13) and responses to Summary Statement weaknesses. Please see attached pages for specific categories to include in mid‐year progress report. [JM will email report to Dan Lukash with cc to Technical Advisor and Wendy Campbell.] May 1, 2013 – Non‐Competing Continuation Progress Report – PHS‐2590 (due 60 days prior to the start of the next budget period). May 13, 2013 – Annual Progress Report‐‐Contains a description of project activities covering the entire year (9/2012 – 5/13/2013). NOTE: FDA reviews our yearly progress before approving funds for the next year; therefore, these reports are due earlier than when the year officially ends in order to award our additional funds in a timely manner. Please see attached pages for specific categories to include in annual progress report. May 13, 2013 – Annual Financial Statement – SF‐425; an original and two copies must be submitted to FDA. [May 1, 2013 – Request for Carryover Funds] ‐ If amount is below 25 percent of federal funding yearly total, just include request within the Annual Financial Statement. If amount exceeds 25 percent of federal funds, must submit formal request to Dan Lukash, including how balance occurred, the plan for the money, etc. Allow 30 days for formal request. YEAR 2 – July 1, 2013 – June 30, 2014 January 1, 2014 – Mid‐Year Progress Report ‐ Contains a description of project activities covering a six‐month period (7/1/2013 – 12/31/13). May 1, 2014 – Non‐Competing Continuation Progress Report – PHS‐2590 May 1, 2014 – Annual Progress Report‐‐Contains a description of project activities covering the entire year (7/1/2013 – 5/1/2014). May 1, 2014 – Annual Financial Statement – SF‐425 [May 1, 2014 – Request for Carryover Funds] YEAR 3 – July 1, 2014 – June 30, 2015 January 1, 2015 – Mid‐Year Progress Report ‐ Contains a description of project activities covering a six‐month period (7/1/2014 – 12/31/14). May 1, 2015 – Non‐Competing Continuation Progress Report – PHS‐2590 May 1, 2015 – Annual Progress Report‐‐Contains a description of project activities covering the entire year (7/1/2014 – 5/1/2015). May 1, 2015 – Annual Financial Statement – SF‐425 [May 1, 2015 – Request for Carryover Funds] YEAR 4 – July 1, 2015 – June 30, 2016 January 1, 2016 – Mid‐Year Progress Report ‐ Contains a description of project activities covering a six‐month period (7/1/2015 – 12/31/15). May 1, 2016 – Non‐Competing Continuation Progress Report – PHS‐2590 May 1, 2016 – Annual Progress Report‐‐Contains a description of project activities covering the entire year (7/1/2015 – 5/1/2016). May 1, 2016 – Annual Financial Statement – SF‐425 [May 1, 2016 – Request for Carryover Funds] YEAR 5 – July 1, 2016 – June 30, 2017 January 1, 2017 – Mid‐Year Progress Report‐‐Contains a description of project activities covering a six‐month period (7/1/16 – 12/31/16). September 30, 2017 – Final Program Progress Report (due 90 days after full project is completed). September 30, 2017– Final Financial Statement; Financial Status Report and Invention Statement. Information to Include within Mid‐Year Progress Reports (THERE IS A SAMPLE PROGRESS REPORT FORM SENT FROM FDA, located at the end of this document.) 1. Detailed progress report on whether we are meeting the project milestones detailed in the cooperative agreement and in the proposal. 2. Status report on the hiring and training of food program personnel. 3. Status report on the operational readiness of any equipment, supplies, software and other purchases using cooperative agreement funds. 4. Certification of current appropriation funding levels for the retail food regulatory program. 5. An updated strategic plan that accurately reflects when specific objectives and tasks have been, or will be, completed and/or implemented and when new objectives and tasks are identified to advance conformance with the Retail Program Standards. The strategic plan should include timeframes, responsible personnel, and other required resources. 6. Description of program improvements in achieving conformance with the Retail Program Standards and promoting more effective control of foodborne illness risk. 7. Cooperative agreement project point of contact (including mailing address, telephone number, and email address) and designation of key personnel working on project. 8. Estimated unobligated balance, funds expended, and funds remaining on this project. 9. Any pending issues, concerns, or challenges encountered in accomplishing the planned work. Provide corrective actions and proposed solutions. Identify any additional support that can be provided by FDA. YEAR 5 – Information to Include within Final Progress Report: Full written documentation of the project and summaries of accomplishments and goals, as described in the grant application. The documentation must be in a form and contain sufficient detail so that other state, local, and tribal governments could reproduce the final project. The report should also detail the strategy to continue advancing conformance with the Retail Program Standards (current and future versions). PLEASE REMEMBER: 1. Keep grant information re facilities, work, training, etc., separate from food contract. 2. Share strategies, documents, etc., with FBI. 3. Participate in committee meetings, presentations, promotion of new strategies, etc. 4. Submit our Funding Certification Letter. 1. Date submitted
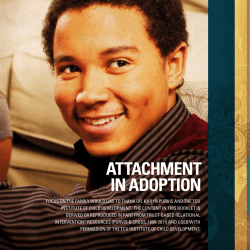
Progress Report
2. Grant No.
3. Project Period
4. Budget Period
5. Dates covered by this report
6. Project Title
7. Grantee Name and Address
8. P.I Name, phone and e-mail
Mid‐year progress reports must contain the elements below as applicable to their proposal and award, but are not limited to, the following:
1. Detailed progress report on the grantee meeting the project milestones identified in the proposal.
2. Status report on the hiring and training of food program personnel.
3. Status report on the operational readiness of equipment, supplies, software, and other purchases
using cooperative agreement funds.
4. Certification of current appropriation funding levels for the retail food regulatory program.
5. A strategic plan that accurately reflects when specific objectives and tasks have been, or will be,
completed and/or implemented and when new objectives and tasks are identified to advance
conformance with the Retail Program Standards. The strategic plan should include timeframes,
responsible personnel, and other required resources.
6. Description of program improvements in achieving conformance with the Retail Program Standards
and promoting more effective control of foodborne illness risk factors in.
7. Cooperative agreement project point of contact (including mailing address, telephone number, and
email address) and designation of key personnel working on project.
8. Estimated unobligated balance, funds expanded, and funds remaining on this project.
9. Any pending issues, concerns, or challenges encountered in accomplishing the planned work.
Provide corrective actions and proposed solutions. Identify any additional support that can be provided
by FDA.
CONTACT INFORMATION Dan Lukash Grants Management Specialist FDA Office of Acquisition Support and Grants 301‐827‐6771 Daniel.Lukash@fda.hhs.gov Wendy Campbell Project Officer FDA, Office of Regulatory Affairs 615‐310‐0483 Wendy.Campbell@fda.hhs.gov Linda Collins, Lead Technical Advisor Retail Food Program Specialist FDA 214‐253‐4945 Linda.Collins@fda.hhs.gov Dan Redditt Southeast Region Retail Food Technical Advisor FDA 404‐253‐1265 Daniel.Redditt@fda.hhs.gov Chris Smith Georgia Retail Food Specialist FDA 404‐253‐1274 Chris.Smith@fda.hhs.gov






© Copyright 2025