
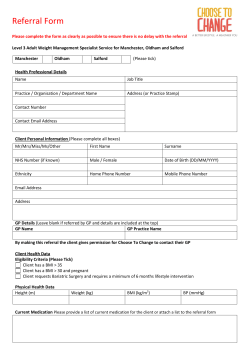
Original Article Differences in prescribed Kt/V and delivered haemodialysis
NDT Advance Access published June 19, 2013 Nephrol Dial Transplant (2013) 0: 1–5 doi: 10.1093/ndt/gft237 Original Article Differences in prescribed Kt/V and delivered haemodialysis dose—why obesity makes a difference to survival for haemodialysis patients when using a ‘one size fits all’ Kt/V target London Medical School, London NW3 2QG, UK Keywords: anthropomorphic Watson, body composition, Kt/V, multi-frequency bioimpedance, muscle fat, obesity Correspondence and offprint requests to: Andrew Davenport; E-mail: andrewdavenport@nhs.uk the Watson-based urea volume of distribution for the obese patients (BMI > 35; spKt/V 1.63 ± 0.48 versus 1.41 ± 0.35 and BMI 30–35; 1.65 ± 0.3 versus 1.46 ± 0.26, both P < 0.01). Conclusions. Prescribing dialysis or quantifying on-line clearance based on the anthropomorphically derived Watson equation leads to underestimation of the delivered dose to obese patients, due to changes in underlying body composition. As such, when using a ‘one size fits all’ target Kt/V, obese patients have an advantage over patients with normal BMI, in that they will receive a greater delivered dose of dialysis, and this may potentially explain the paradoxical survival advantage of the morbidly obese haemodialysis patient. A B S T R AC T Background. Morbid obesity is reported to be a survival factor for haemodialysis patients compared with those with a normal body mass index (BMI), yet morbid obesity (BMI >35) is a mortality risk factor for obese patients in the general population. Traditionally, haemodialysis dosing is prescribed to achieve a target Kt/V corrected for total body water (TBW). As obese patients typically have increased body fat, which contains less water than muscle, then obese patients may have lower levels of body water than their slimmer counterparts, and as such delivered Kt/V could be greater than that estimated using standard anthropomorphic equations, and so increased dialysis dose may help explain the increased survival reported for obese patients. Methods. We compared multi-frequency bioelectrical impedance analysis (MF-BIA) measurements of TBW in healthy haemodialysis outpatients, and compared TBW with that calculated from the Watson equation derived from anthropomorphic measurements. Results. Three hundred and sixty-three adult patients, mean age 58.1 ± 16.7 years, 60.9% male and 29.9% diabetic were studied. MF-BIA-measured body composition showed that as BMI increased from <20 to >35, the percentage skeletal muscle mass fell from 42.8 ± 4.9 to 29.2 ± 5.5% (P < 0.01) whereas the % fat mass increased from 24.5 ± 11.6 to 46.7 ± 6.8% (P < 0.01). As such, TBW measured by MF-BIA was significantly lower from that predicted by the Watson equation at higher BMIs (BMI > 35; 38.9 ± 6.8 versus 44.7 ± 6.9 L, P < 0.01 and BMI = 30–35; 37.2 ± 7.5 versus 41.9 ± 7.3 L, P < 0.01), and as such the delivered Kt/V using MF-BIA was much greater than that using © The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. INTRODUCTION Mortality risk progressively increases with chronic kidney disease staging [1], and intuitively treatment with a greater amount of dialysis might be expected to improve patient survival. The National Cooperative Dialysis Study (NCDS) showed that those patients treated by thrice weekly haemodialysis with higher time-averaged urea concentrations were more likely to become unwell, and defined a threshold adequacy, based on urea clearance [2]. Urea clearance was expressed as Kt/V, where K is the dialyser urea clearance, t is the duration of the dialysis session and V is the volume of urea distribution [3]. Later studies showed a relationship between carbamylated haemoglobin [4] and Kt/V [5]. Subsequent observational studies reported improved patient survival rates with Kt/V > 1.0 [6, 7], and by consensus dialysis sessional Kt/V targets were increased to 1.2 [8]. The Haemodialysis study (HEMO study) 1 Downloaded from http://ndt.oxfordjournals.org/ by guest on October 1, 2014 UCL Center for Nephrology, Royal Free Hospital, University College Andrew Davenport Wilcoxon rank-sum pair test for paired values with Bonferroni correction for multiple analyses where appropriate and by ANOVA with Tukey post-hoc correction. Statistical analysis used Graph Pad Prism version 6.0 (Graph Pad, San Diego, CA, USA) and SPSS version 17 (University Chicago, USA). Statistical significance was taken at or below the 5% level. R E S U LT S We studied 363 adult patients, mean age 58.1 ± 16.7 years, 60.9% male, 28.9% diabetic and dialysis vintage 51 (20–83) months. Major racial groups were 51.5% Caucasoid, 37.8% south Saharan African or Afro-Caribbean and 34.2% Asian. Post-dialysis weight 70 ± 16.0 kg, body mass index (BMI) 25.8 ± 5.4 kg/m2, dialysis session time 3.94 ± 0.5 h with preand post-dialysis serum urea 19.8 ± 6.0 and 5.3 ± 2.3 mmol/L, respectively, with a urea reduction ratio 73.3 ± 7.1%. Pre-dialysis haemoglobin 11.4 ± 1.5 g/L, albumin 40.9 ± 3.9 g/L, median C-reactive protein 4 (2–11) mg/L and glucose 5.9 (4.8–8.4) mmol/L. TBW, measured by MF-BIA post-dialysis was 35.2 ± 7.5 L and did not differ from that estimated from Watson (36.6 ± 7.0 L), but single-pool Kt/V was statistically different for that using MF-BIA 1.65 ± 0.41 compared with that using the Watson equation, 1.56 ± 0.32, P < 0.001. MFBIA skeletal muscle mass was 26.3 ± 6.2 kg, fat mass 23.0 ± 12.0 kg, giving a percentage body skeletal muscle content of 37.6 ± 6.9% and fat content of 31.4 ± 13.0%. Patients were divided according to BMI into five groups, those with a BMI 19 or lower, 20–25, 25–30, 30–35 and >35.0. There was no difference in ethnic distribution between the groups, although there were differences in sex distribution and diabetes with BMI (Table 1). TBW was significantly greater when calculated by the Watson equation compared with that measured by MF-BIA for those patients with the greater BMIs (Figure 1). The pre-dialysis serum urea was lower in those patients with the smallest BMI compared with the highest quintile, whereas the urea reduction ratio was higher for the lowest quintile BMI compared with the highest (Table 1). Comparing single-pool Kt/V measured by the Daugirdas equation [23], and that recalculated using MF-BIA, then Kt/V was greater with the Daugirdas equation for those patients with the lowest BMIs, and lower for those with the highest BMIs (Figure 2). The percentage ultrafiltration to MF-BIA measured TBW was greater for the highest BMI groups (Table 1). Although there was a trend for patients with a lower BMI having shorter dialysis sessions, this was not significant when correcting for multiple analyses (Table 1). Body composition, in terms of muscle and fat differed between the BMI quintiles, with reducing muscle mass and increasing fat as BMI increased (Figure 3). M AT E R I A L S A N D M E T H O D S Multi-frequency bioimpedance measurements were made post dialysis in 361 healthy haemodialysis outpatients attending their mid-week dialysis session (InBody 720 Body Composition Analysis, Biospace, Seoul, South Korea) [17], using direct segmental MF-BIA with tetrapolar 8-point tactile electrodes [18], in a standardized manner [19]. Patients with cardiac pacemakers, implantable defibrillators, amputees and those unable to stand on the bioimpedance machine were excluded from study. Fresenius F4000H or 5000H dialysis machines (Fresenius Bad Homburg, Germany) were used with polysulfone high-flux dialysers (Nipro Corporation, Osaka, Japan) [20], with ultrapure quality dialysis water and low-molecular-weight heparin (Tinzaparin, Leo Laboratories, Princes Risborough, UK) [21]. Pre- and post-dialysis dialysis blood samples were taken in a standardized fashion measured with a standard laboratory auto-analyser (Roche Integra, Roche diagnostics, Lewes, UK) and haemoglobin (XE-2100 Sysmex Corporation, Kobe, Japan). Kt/V was calculated using the Daugirdas equation [22]. Body composition was derived from multi-frequency bioelectrical impedance assessments (MF-BIA) [15, 23]. Using TBW measured post dialysis by MF-BIA, Kt/V was recalculated [24] assuming the Watson formula for TBW [25]. Ethical approval was granted by the local ethical committee as part of UK National Health Service audit and clinical service development. Statistical analysis Results are expressed as mean ± standard deviation, or median and inter-quartile range, or percentage. Statistical analysis was by χ 2 analysis, corrected for small numbers by Yates’ correction, students’ t-test for parametric and the Mann–Whitney U-test for nonparametric data, Student’s pair t-test and DISCUSSION Although the NCDS study helped to define a lower limit for dialysis dosing, based on urea clearance [2, 3], subsequent 2 A. Davenport Downloaded from http://ndt.oxfordjournals.org/ by guest on October 1, 2014 ORIGINAL ARTICLE [9], the second randomized controlled trial to investigate the effect of Kt/V on patient outcomes, reported that higher doses did not improve overall patient survival. However, on subgroup analysis, women who had been established on haemodialysis for more than 3 years did benefit from higher Kt/V targets. This led to suggestions that using an estimate of body water resulted in underdosing of some patient groups on one hand and potentially delivering greater doses to others [10]. Whereas for the general population, morbid obesity is associated with increased mortality [11], several observational studies have reported that survival is increased for the morbidly obese haemodialysis patients [12, 13]. This apparent paradox may be due to changes in body composition, as fat contains less water than muscle, and the standard equations used to calculate body water may not reflect these differences. Multi-frequency bioelectrical impedance assessments (MFBIA) can be used to both measure body water [14] and also body composition in dialysis patients [15, 16]. To determine whether obese patients receive a proportionally higher dialysis dose when the same Kt/V target is used, we compared total body water (TBW) estimation by anthropomorphic equations and that measured by MF-BIA. Table 1. Patients divided according to body mass index (kg/m2) ≤20 20–25 25–30 30–35 >35.0 n 38 141 120 42 22 Male 16 90 81 28 10 Female 22 52 41 14 12 diabetic 2 38 31 20 13 Not diabetic 36 103 89 22 9 Caucasoid 12 51 50 19 10 African 10 39 36 11 8 Asian 16 49 33 9 4 Pre urea (mmol/L) 17.2 ± 5.5 20.0 ± 6.7 19.8 ± 5.0 20.4 ± 5.8 21.7 ± 5.7* URR (%) 75.2 ± 8.6 74.5 ± 6.3 73.0 ± 6.6 71.1 ± 6.5 78.7 ± 9.8* UF/TBW% 2.4 (1.4–3.2) 3.1 (1.9–4.0) 3.4 (2.3–5.0) 4.9 (2.8–6.5) 4.6 (3.5–7.7)* Session time (h) 3.8 ± 0.62 3.89 ± 0.46 4.0 ± 0.46 3.97 ± 0.55 4.12 ± 0.57 Comparison of sex, diabetes and racial origin, Sub Sahara African-AfroCaribbean (African). χ analysis. Pre-dialysis serum urea (Pre-urea). URR, urea reduction ratio. Dialysis session time in hours. Males versus females P = 0.035, diabetes versus no diabetes P < 0.001. Ultrafiltration volume (UF) to total body water (TBW). Results expressed as mean ± SD or median (inter-quartile range). *P < 0.05 BMI < 20 versus BMI > 35. 2 ORIGINAL ARTICLE Downloaded from http://ndt.oxfordjournals.org/ by guest on October 1, 2014 BMI F I G U R E 2 : Kt/V calculated by the Daugirdas equation [22] com- pared with that using total body water measured by multifrequency bioelectrical impedance analysis (MF-BIA) in patient cohort divided into body mass index (BMI) kg/m2 groups. *P < 0.05 versus MF-BIA after correction for multiple analyses. F I G U R E 1 : Total body water (TBW) calculated by Watson equation [23] compared with TBW measured by multi-frequency bioelectrical impedance analysis (MF-BIA) in patient cohort divided into body mass index (BMI) kg/m2 groups. *P < 0.05 versus MF-BIA after correction for multiple analyses. the volume of urea distribution, then V will be overestimated in the morbidly obese patient due to the relative increase in fat mass and reduction in muscle, due to the lower water content of adipose tissue. In addition, to achieve a pre-determined target, it is most likely that dialysis session time will be increased for the obese patient, so they additionally benefit both from increased clearance of time-dependent solutes, such as phosphate [28], and also control of sodium balance and overhydration. This is supported by our study with both a trend in terms of dialysis session time and an increasing proportion of ultrafiltration to TBW with increasing BMI. As such, this improved delivery of a higher dose of dialysis for the obese patient could potentially explain the apparent paradox of an apparent survival advantage for the morbidly obese (BMI > 35) haemodialysis patient compared with those with prospective studies failed to show that increasing the delivered dialysis dose based on Kt/V prescription increased patient survival [9]. This could be due to many confounders, including residual renal function, the time to accumulate uraemic toxins to cause morbidity and mortality [26], and the effects of intradialytic weight gains and extracellular volume control [27]. In addition, the mean Kt/V values in the HEMO study were not too dissimilar between the groups at 1.16 versus 1.32, so another potential confounder could have been that patients with higher BMIs had an underestimate of the actual dose delivered, and those with lower BMIs an overestimate, so that the groups were not as separated as initially thought. When dialysis is prescribed according to Kt/V, or measured by on-line clearance using the Watson equation to estimate 3 Obesity and delivered dialysis dose obesity with increased body fat content, by containing less water than muscle, paradoxically has become a survival advantage for haemodialysis patients using current treatment target paradigms. C O N F L I C T O F I N T E R E S T S TAT E M E N T The author has no conflict of interest. The data contained in this paper have not been previously published in whole or part form, or by abstract. F I G U R E 3 : Changes in body composition as percentage of muscle REFERENCES 1. Chronic Kidney Disease Prognosis ConsortiumMatsushita K, van der Velde M, Astor BC et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative metaanalysis. Lancet 2010; 375: 2073–2081 2. Lowrie EG, Laird NM, Parker TF et al. Effect of the haemodialysis prescription of patient morbidity: report from the National Cooperative Dialysis Study. N Engl J Med 1981; 305: 1176–1181 3. Gotch FA, Sargent JA. A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 1985; 28: 526–534 4. Davenport A, Jones SR, Goel S et al. Differentiation of acute from chronic renal impairment by detection of carbamylated haemoglobin. Lancet 1993; 341: 1614–1617 5. Davenport A, Jones S, Goel S et al. Carbamylated hemoglobin: a potential marker for the adequacy of haemodialysis therapy in end-stage renal failure. Kidney Int 1996; 50: 1344–1351 6. Parker TF, 3rd, Husni L, Huang W et al. Survival of haemodialysis patients in the United States is improved with a greater quantity of dialysis. Am J Kidney Dis 1994; 23: 670–680 7. Held PJ, Port FK, Wolfe RA et al. The dose of haemodialysis and patient mortality. Kidney Int 1996; 50: 550–556 8. Morbidity and mortality of dialysis: an NIH Consensus Statement Online. Ann Intern Med 1993; 11: 1–33 9. Eknoyan G, Beck GJ, Cheung AK et al. Haemodialysis (HEMO) Study Group. Effect of dialysis dose and membrane flux in maintenance haemodialysis. N Engl J Med 2002; 347: 2010–2019 10. Spalding EM, Chandna SM, Davenport A et al. Kt/V underestimates the haemodialysis dose in women and small men. Kidney Int 2008; 74: 348–355 11. Kral JG. Morbid obesity and related health risks. Ann Intern Med 1985; 103(6 (Pt 2)): 1043–1047 12. Leavey SF, McCullough K, Hecking E et al. Body mass index and mortality in ‘healthier’ as compared with ‘sicker’ haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 2001; 16: 2386–2394 13. Jialin W, Yi Z, Weijie Y. Relationship between body mass index and mortality in hemodialysis patients: a meta-analysis. Nephron Clin Pract 2012; 121: c102–c111 14. Papakrivopoulou E, Booth J, Pinney J et al. Comparison of volume status in asymptomatic haemodialysis and peritoneal dialysis outpatients. Nephron Extra 2012; 2: 48–54 15. Fürstenberg A, Davenport A. Comparison of multifrequency bioelectrical impedance analysis and dual-energy X-ray normal BMI, whereas the morbidly obese patient in the general population has increased risk of mortality. The Watson equation, which is advocated as the standard for calculating TBW, and recommended by many clinical guideline committees [29], was derived from studies in the 1950s and 1960s. Since then, body composition has changed in many economically developed countries, with a trend to increased obesity. Our data support earlier smaller anthropomorphic studies [30] and the more recent analysis from the HEMO study [31], which reported that the Watson equation overestimates TBW in haemodialysis patients, and these differences in expected and delivered dialysis dose would help to explain the reports of increased survival reported in overweight patients [32], More recently, some groups have used alternative scales, such as body surface area rather than urea volume distribution to adjust dialysis dose for body size [33]. Normalizing Kt/V to body surface area rather than Watson-derived TBW, lowered the dose of dialysis delivered to women compared with men in the HEMO [33]. Subsequent re-analysis of the HEMO study group using dialysis dose corrected for body surface area (BSA) recently reporting different dose–mortality relationships, which were substantially different from those using the original volume-based dosing regimen, reporting an increased survival for haemodialysis patients up to a Kt/V of 1.6 [34]. Morbidly obese patients were however excluded from the HEMO study, and our data would suggest that although correction for BSA may well be an improvement on the Watson-derived urea volume, any adjustment for BSA assumes a fixed relationship with body composition [35], which may well no longer hold given the current epidemic of obesity in the developed world. Our data show that when prescribing or delivering haemodialysis to a pre-determined target or on-line Kt/V, the actual dose of dialysis delivered to the obese patient will be greater than that predicted by using anthropomorphically derived equations of TBW, and conversely reducing the dose of dialysis to the patient with a low BMI. Thus, to achieve current, one size fits all, Kt/V targets the morbidly obese patient potentially benefits from not only greater small solute clearances, but also from longer session times, with improved clearance of timedependent solutes and reduced risk of overhydration. As such 4 A. Davenport Downloaded from http://ndt.oxfordjournals.org/ by guest on October 1, 2014 ORIGINAL ARTICLE mass and fat mass according to body mass index (BMI) kg/m2 groups. *P < 0.05 versus MF-BIA after correction for multiple analyses compared to the two lowest BMI quintile. 16. 17. 18. 19. 20. 22. 24. 25. Received for publication: 3.2.2013; Accepted in revised form: 19.4.2013 5 Obesity and delivered dialysis dose ORIGINAL ARTICLE 23. Downloaded from http://ndt.oxfordjournals.org/ by guest on October 1, 2014 21. 26. Davenport A, Farrington K. Dialysis dose in acute kidney injury and chronic dialysis. Lancet 2010; 375: 705–706 27. Davenport A. How best to improve survival in haemodialysis patients: solute clearance or volume control? Kidney Int 2011; 80: 1018–1020 28. Davenport A, Gardner C, Delaney M. Do differences in dialysis prescription impact on KDOQI bone mineral targets? The Pan Thames Renal Audit. Blood Purif 2010; 30: 111–117 29. NKF KDOQI Guidelines: Clinical Practice Guidelines and Clinical Practice Recommendations 2006 Updates Hemodialysis Adequacy. http://www.kidney.org/professionals/KDOQI/guideline_ upHD_PD_VA/hd_guide2.htm (March 2013, date last accessed) 30. Kloppenburg WD, Stegeman CA, de Jong PE et al. Anthropometry-based equations overestimate the urea distribution volume in haemodialysis patients. Kidney Int 2001; 59: 1165–1174 31. Daugirdas JT, Greene T, Depner TA et al. Hemodialysis (HEMO) Study Group. Anthropometrically estimated total body water volumes are larger than modeled urea volume in chronic hemodialysis patients: effects of age, race, and gender. Kidney Int 2003; 64: 1108–1119 32. Lowrie EG, Li Z, Ofsthun N et al. Body size, dialysis dose and death risk relationships among hemodialysis patients. Kidney Int 2002; 62: 1891–1897 33. Daugirdas JT, Greene T, Chertow GM et al. Can rescaling dose of dialysis to body surface area in the HEMO Study explain the different responses to dose in women versus men? Clin J Am Soc Nephrol 2010; 5: 1628–1636 34. Ramirez SP, Kapke A, Port FK et al. Dialysis dose scaled to body surface area and size-adjusted, sex-specific patient mortality. Clin J Am Soc Nephrol 2012; 7: 1977–1987 35. Dubois D, Dubois EF. A formula to estimate the approximate surface area if the height and weight be known. Arch Intern Med 1916; 863: 17 absorptiometry assessments in outpatient haemodialysis patients. Am J Kidney Dis 2010; 57: 123–129 Fürstenberg A, Davenport A. Assessment of body composition in peritoneal dialysis patients using bioelectrical impedance and dualenergy x-ray absorptiometry. Am J Nephrol 2011; 33: 150–156 Booth J, Pinney J, Davenport A. The effect of vascular access modality on changes in fluid content in the arms as determined by multifrequency bioimpedance. Nephrol Dial Transplant 2011; 26: 227–231 Sartorio A, Malovolti M, Agosti F et al. Body water distribution in severe obesity and its assessment from eight polar bioelectrical impedance analysis. Eur J Clin Nutr 2005; 59: 155–160 Booth J, Pinney J, Davenport A. N-terminal proBNP—marker of cardiac dysfunction, fluid overload, or malnutrition in haemodialysis patients? Clin J Am Soc Nephrol 2010; 5: 1036–1040 Vernon K, Peasegood J, Riddell A et al. Dialyzers designed to increase internal filtration do not result in significantly increased platelet activation and thrombin generation. Nephron Clin Pract 2011; 117: c403–408 Davenport A. Low-molecular-weight heparin as an alternative anticoagulant to unfractionated heparin for routine outpatient haemodialysis treatments. Nephrology (Carlton) 2009; 14: 455–461 Daugirdas JT. Second generation logarithmic estimates of singlepool variable volume Kt/V: an analysis of error. J Am Soc Nephrol 1993; 4: 1205–1213 Campos AC, Chen M, Meguid MM. Comparisons of body composition derived from anthropometric and bioelectrical impedance methods. J Am Coll Nutr 1989; 8: 484–489 Lindley EJ, Chamney PW, Wuepper A et al. A comparison of methods for determining urea distribution volume for routine use in on-line monitoring of haemodialysis adequacy. Nephrol Dial Transplant 2009; 24: 211–216 Watson PE, Watson ID, Batt R. Total body water volume for adult males and females estimated from simple anthropometric measurements. Am J Clin Nutr 1980; 33: 27–39










© Copyright 2025