
Student Orientation Manual 2014 Edition
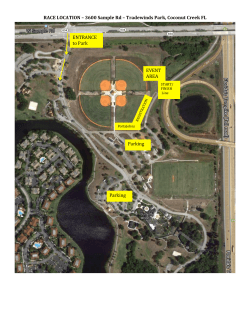
Student Orientation Manual 2014 Edition Updated 2/2014 Welcome to Fairfield Medical Center! We hope you find your student experience with us to be both beneficial to your personal and professional growth, as well as enjoyable! Part of our responsibility to you is to ensure your safety and that of our patient’s and staff before you actually start your student experience. In order to do so, we have put together this Reference Guide for you to review. Again, welcome to Fairfield Medical Center! We look forward to meeting you and having the opportunity to build a personal and professional relationship with you! Thank you and welcome! Becky DeVoss, RN Clinical Education Coordinator Learning & Development 740-687-8496 rebeccas@fmchealth.org Table of Contents Requirements Application …………………………………………………………. Orientation post test ……………………………………………….. Liability …………………………………………………………….. Confidentiality ……………………………………………………… TB test ………………………………………………………………. Background check …………………………………………………. Immunizations ……………………………………………………… CPR …………………………………………………………………. FMC Badge …………………………………………………………. Clinical Documentation ……………………………………………. Glucose Meters …………………………………………………….. Page 4 4 4 4 4 4 4 4 4 5 5 General Information Telephone numbers ……………………………………………….5 Absences ……………………………………………………………. 5 Cafeteria ……………………………………………………………. 5 Classrooms …………………………………………………………. 6 Lost and Found …………………………………………………….. 6 Dress Code ………………………………………………………….. 6 Housekeeping ………………………………………………………. 6 Parking ……………………………………………………………… 6,16 Personal Property ………………………………………………….. 6 Personal Phone calls ……………………………………………….. 6 Smoking …………………………………………………………….. 6 Solicitation …………………………………………………………... 7 Orientation to Standards and Guidelines Emergency Code …………………………………………………….. 7-10 Patient Identifiers ……………………………………………………. 10 Infection Control ……………………………………………………... 10 Blood Borne Pathogens ………………………………………………. 11 Infectious Waste ……………………………………………………… 11 Hazardous Spill/Code orange ………………………………………… 11 Hazardous Communication Plan ……………………………………. 12 Universal Protocol ……………………………………………………. 12 Interruption Plan ……………………………………………………… 12 Equipment Management ……………………………………………… 13 Center Police …………………………………………………………... 13 Safety Program ………………………………………………………… 13 Customer Service ……………………………………………………… 13 Event Reporting ………………………………………………………... 14&15 Falls ……………………………………………………………………. 15 Patient Rights …………………………………………………………….15 Confidentiality ……………………………………………………………15 Table of Abbreviations ……………………………………………………16 Parking Policy …………………………………………………………….17 Appendix Appendix A ……………………………………………………………….Application Appendix B ………………………………………………………………..Liability/Waiver and Confidentiality Statement Appendix C ………………………………………………………………..Immunization Form Appendix D ……………………………………………………………… Background Check Appendix E ……………………………………………………………… Orientation Test 3 REQUIREMENTS Student Please complete the application and orientation post test included with this manual. Also, the notice of privacy, liability statement and confidentiality statement must be signed and returned. The immunization and background check forms must be completed submitted prior to clinical rotation. Application If you are in a Clinical Rotation or a Health Tech program, you will turn this in to your instructor. Otherwise, please send completed application directly to: Learning & Development Attn: Becky DeVoss 401 N Ewing St Lancaster, Ohio 43130 rebeccas@fmchealth Your application must be submitted 3 weeks prior to your clinical rotation/internship or shadowing experience to allow for time to process and develop a clinical site for your rotation. Liability Confidentiality These must be signed and turned in with the application Post-test Please review the Orientation Manual included and complete the post-test. If you are in a Clinical Rotation or a Health Tech program, you will turn this into your instructor. Otherwise, please send your completed post-test directly to Learning & Development. FMC Badge All paperwork must be received and your student file complete before a badge will be issued. Stop by Human Resources between the hours of 7:00am-4:00pm to pick-up an ID badge. A non-photo “Student” badge will be given to anyone shadowing. For all others, your picture will be taken and used in providing you a FMC ID badge. The badge is to be worn while here at FMC. There is a cost of $25.00 for any lost, damaged, or unreturned badge. TB Test You need to be able to submit evidence of a two step negative TB Test. If you are in a school program, they should provide this testing and have it on record. Have the school provide evidence of compliance. If you have not received a TB test they may be obtained from your private physician or the health department. CPR If you will be involved with any direct patient care, you will need to verify that you have a current CPR certification. FMC offers CPR classes. Please contact Learning and Development at 740-687-8491 to register. Parking Tag If your student experience will require you to be at FMC more than 8 hours, you will need to stop in Human Resources between the hours of 7:00am-4:00pm to pick-up a parking tag. You will need your license plate number. 10 Panel Drug students will need to provide evident of a negative 10 panel drug screen Screen Not required of those that are Shadowing 4 Immunizations All students will need to provide proof that they are current on all immunization prior to clinical rotation. This includes: A 2-step TB skin test and then annual thereafter. We also require documentation of the MMR vaccine, Varicella and Hepatitis B, or lab work indicating immunity to these diseases. If your college does not have a copy you may contact your high school for a copy. If these are not up to date you may go to your family physician or to the health department for these vaccinations. Background Federal background checks will be completed and turned in with application for all students this does not include those who are shadowing.) If you have not had a background check completed by your college/university it may be obtained through: Fairfield County Sherriff’s Department 108 N. High Street Lancaster, Ohio 43130 The cost is $30.00 and payment is by cash or check – NO debit or credit card Flu Vaccines Students must provide proof of the Flu vaccine for the current year. If student has deemed not to have the flu shot administered said student will need to wear a mask. Additional training may be requested by your instructor based on the location of your experience. Please contact the instructor directly to schedule any of the following courses. Clinical Documentation This class is required of any student who will be involved with charting. All the paperwork required for these classes will be given to you on the day of your class. There are three different classes, depending on the department: HSM- All Surgery departments. HED- ICU, PCU, 3rd, 4th, 5th, 6 South, 6 North, Respiratory HEC - Emergency Room Glucose Meters Nursing students (RN, LPN, NA)with direct patient contact will need to show competency in the use of a Glucose meter. Testing will occur in the department by your preceptor or by your class instructor. You will find the necessary paperwork in this manual 5 General Information IMPORTANT TELEPHONE NUMBERS Fairfield Medical Center: 740-687-8000 Fairfield Medical Center Police: 740-687-8019 ABSENCES If you are sick, or will have to be absent for any reason, please notify your instructor and/or supervisor in advance. CAFETERIA You are welcome to eat in the Center cafeteria and you will receive a discount when wearing your FMC ID badge. The cafeteria is open for lunch from 10:30 am until 1:30 pm and serves dinner from 4:30 pm until 6:30 pm. Please try to avoid the rush hour between 11:30 am -12:30 pm. This facility is open at other times for coffee and snacks, but cannot be used as a “study hall” for long periods of time during the day. CLASSROOMS Classrooms will be provided for students with the understanding that chairs, tables and equipment will be returned to their proper places at the end of the class period. Please remember that conferences and other classes are taking place in the area most of the time and your cooperation in keeping the atmosphere quiet and conducive to study will be appreciated. Professional conduct should extend to the classroom area, as well as patient care areas. LOST AND FOUND Fairfield Medical Center is not responsible for lost articles. Articles found on the Center premises that are not Center property should be submitted to the Patient Representative. Students who lose personal articles on the Center premises should contact Patient Representative. DRESS CODE Please adhere to the uniform or dress requirements for your particular clinical training program. In general, uniforms should be kept neat and clean. Recreational clothing and blue jeans are prohibited while on duty in Fairfield Medical Center. Name badges will be issued by the Human Resources Department and are to be worn at all times on duty. If lost, replacement badges will cost $25.00. You are required to turn in your name badge to your clinical instructor or to Human Resources upon completion of this student experience. Earrings are permitted to be worn only in your ears, and limited to two per ear. Tattoos should not be visible under any circumstances unless for a medical reason such as being a diabetic. See personal appearance policy below. 6 HOUSEKEEPING Please do your best to keep the Center as clean and neat as possible; free of clutter and litter, which helps to eliminate germs. You will want to follow good housekeeping rules throughout your health care career. The best time to start is now while you are a student. PARKING All students are required to park in the designated student parking. If student is found parking in employee lots – a ticket from the hospital police will be issued. Three (3) parking violations will result in the student being asked to leave the clinical site. (Map is included to denote student parking area.) There will be a charge of $40.00 per semester for each student. Failure to pay for the parking will result in loss of clinical hours. PERSONAL PROPERTY The Center is not responsible for lost or stolen articles. Please limit the amount of money and other valuables you bring to the Medical Center. Ensure that these items are either with you or properly secured at all times. Lockers are available per request and coat racks are located in each department. PERSONAL PHONE CALLS Though it is impossible to completely eliminate all emergency telephone calls, please limit the use of the telephone to important matters that cannot be handled otherwise. Use of cell phones or texting in clinical areas is prohibited during your student experience. SMOKING Effective July 1, 2006, Fairfield Medical Center became a smoke-free campus. You are not permitted to use tobacco products, of any kind, on the premise while on or off duty. SOLICITATION AND DISTRIBUTION Employees and Non-employees are not permitted to solicit or distribute materials on Center premises at any time. Students cannot solicit or distribute any materials to other students or employees on work time. Examples: Avon, Pampered Chef. STUDENT RECORDS Each student will maintain their own hour/daily records. It will not be the responsibility of the “Center” to maintain those for the student or intern. 7 Orientation to Standards and Guidelines The content below is information that you need to know as required by The Joint Commission, the Occupational Safety and Health Administration (OSHA) and Fairfield Medical Center. The Joint Commission - The Joint Commission accredits and certifies nearly 15,000 health care organizations and programs in the United States. Joint Commission accreditation and certification is recognized nationwide as a symbol of quality that reflects an organization’s commitment to meeting certain performance standards. OSHA - OSHA's mission is to assure the safety and health of America's workers by setting and enforcing standards; providing training, outreach, and education; establishing partnerships; and encouraging continual improvement in workplace safety and health Emergency Codes The following codes are listed on the back of your identification badge. Code Red - Fire Remember: Close all doors and windows Leave all lights ON Do not use elevators Follow instructions from the manager or supervisor. If you need to use a fire extinguisher remember PASS – Pull the pin, Aim, Squeeze and Sweep. Code Adam – Missing Child In the event of a missing or abducted child or infant you will notify the Center’s Switchboard Operator and alert Center Police. The Center Police Officer will be in charge of the situation. Staff will be directed to check and guard stairwells, elevators, and all entrances to departments and the facility. Staff will watch for persons not appropriate for their area and observe if they could be hiding an abducted infant. Remember to remain calm. Code Brown – Missing Adult Patient An adult patient is missing from your unit. You will begin an immediate search of your department and the Center. Notify the Center’s Switchboard, Center Police, House Supervisor, 8 Manager, the attending physician, and the patient’s residence. Note a time frame when the patient was last seen. Code Green – External Disaster/ Code Yellow – Internal Disaster External disaster means that the event is occurring outside of the facility. Internal means that we have multiple victims of a related disaster within our building. If you hear Level One overhead this means that there is a disaster in progress but the victims hae not arrived at FMC. You will need to take direction from the manager of the unit you have been assigned to or from your instructor. Level 2 means that the victims of the disaster have started arriving in the ED. Again, follow the instructions of the manager of the unit or your instructor. Code Gray – Severe Weather When Fairfield County is affected by severe weather – the Center Police will determine if a Code Grey needs to be put into effect. If you hear a Code Grey Option One announced – this means that a Tornado or high wind “WATCH” has been issued by the National Weather Service for our area. During a Code Grey Option One you will need to follow the instructions of the manager on the unit. You will help remove objects from the patient’s window sills, make sure that you know where the flashlights are and begin closing the blinds and drapes in the patient rooms. When Option Two has been called – it denotes that a tornado has been sighted or that we have a high wind WARNING in our area. You will need to assist the unit staff in closing the blinds and drapes in the patient rooms, close all doors, including the smoke barrier doors. If asked by the manager of the unit – evacuate patients to an area that has been chosen by the manager. Code Blue – Adult Medical Emergency Code blue is called when a person is unresponsive and does not have a pulse or is breathing. If you witness or find a patient/person who is unresponsive, without a pulse and breathing you should call for help and start CPR. Code Pink – Infant/Child Medical Emergency Code pink is called when an infant or child is not breathing and has no pulse. You will need to establish unresponsiveness, call for help and start. Code Violet – Violent / Combative Person 9 Code Violet is used when a person has lost control and immediate assistance is needed in order to manage their aggressive behavior. If you encounter a person who has lost control – notify the manager of the unit. They will evaluate the patient and decide the course of treatment Code Silver – Hostage Situation or person with a weapon If you encounter a person who has a weapon or you have been taken hostage – never argue with the person, do not panic, do what you are told, always face the person and do not try to be a hero. If you hear a Code Silver announced – follow the direction of your instructor or the manager of the unit. You may be asked to assist in closing doors, assisting patients, visitors and staff. Do not use the elevators and do not transport any patients at this time. Code Black – Bomb / Bomb Threat If you would receive a phone call that threatens a bomb do the following: 1. 2. 3. 4. 5. 6. Remain calm. Speak in a normal tone. Keep the caller on the line. Listen for distinguishing voice characteristics. Listen for background noise. Obtain assistance from the manager and/or instructor You may also be asked to assist with looking for unusual objects that may potentially be a bomb. Patient Identifiers One of the most important tasks that you will do on a daily basis is identifying your patient. At Fairfield Medical Center we use the: 1. Patient name 2. Patient’s Date of Birth Do not use the patient’s room number Always have a document to compare the date of birth and the patient’s name Infection Control Universal precautions is treating ALL patients as if their blood and body fluids were potentially infectious regardless of known infectious disease. Hand washing is the single most important procedure in Infection Control. 10 . The protection you use to prevent exposure- gloves, masks, gowns, aprons, eye protection are called Personal Protective Equipment (PPE) To prevent the event of a needle stick you would not recap needles. If you were to be stuck by a contaminated needle you would, report this to your instructor and manager of the department; fill out an incident report, and complete the post exposure management kit of lab testing. You will report to the Emergency Room and any cost associated will be the responsibility of the student. Blood Borne Pathogens Examples of blood borne pathogens are Malaria, Hepatitis, HIV, Syphilis. You can prevent contact with a blood borne pathogen by treating all blood and body fluids as if they are potentially infectious. Use gloves, masks and gowns. Always wash your hands Infectious Waste Infectious wastes are spread by blood, air, and contact If you have infectious wastes that are disposable, put in a red biohazard bag Hazardous Material Spill Code Orange Hazardous materials are chemical substances which, if released or misused, can pose a threat to the environment, life or health. . Chemical exposure may cause or contribute to many serious health effects such as heart dysfunction, kidney, lung, and brain damage, sterility, cancer, burns and rashes. Some chemicals may also be safety hazards and have the potential to cause fires and explosions and other serious accidents. The most common types of hazardous spills at Fairfield Medical Center are: Chemo therapy agents Blood and body fluids Chemicals Radioative ALL employees should know the location, content, and use of any spill kit in their department. The spill kit will be used when the spill is larger than 1 cubic foot or more in volume. 11 Hazardous Communication Program In order to identify hazardous products on the units you are assigned, check for the warning labels on the container. You can also look for the material safety data sheet which is located on the intranet or in the Orange and White manual located on the units. Universal Protocol It is important in any procedure that is performed at Fairfield Medical Center that 3 processes are checked prior to the start of the procedure. 1. Verify that you have the correct procedure, the right patient and the correct site 2. Make sure that the patient has gone through a pre-procedure verification process a. must be completed prior to the procedure – you are verifying that you have all the proper documents, related information and equipment 3. A time out is conducted before the procedure. a. completed immediately before starting the procedure b. it includes: anesthesia, surgeon, circulating nurse or nurse attending procedure or any other active participants. Interruption Plan – Power & Telephones 1. Power Failure In the event of a power failure, the Center’s generators will automatically start within10seconds.Hallway lights are equipped with emergency power as well as red outlets, which include light switches. Nursing floors have emergency power in each of the patient rooms, as identified by the red wall plate covering. 2. Telephones If the Center encounters a telephone outage – cell phones are available on each of the units Do not transmit cellular phones in the following areas: Surgery – behind the line Cardiac services ICU ED PACU Cardiac Rehab PCU You can find department cell phone numbers in the Emergency and Disaster Manual on your unit 12 Equipment Management All equipment that is utilized for patient care must have a Bio Med or Plant Engineering sticker on it and must have been checked with in the past 12 months. If a piece of equipment fails while you are using it, do the following: 1. 2. 3. Remove from use immediately! Inform your Manager / Supervisor. Place a tag on the piece of equipment noting that it is broken or does not work. Center Police The Center has police officers on duty 24 hours a day who are responsible for safeguarding individuals while they are on the Center premises, as well as for providing security of the buildings and grounds. If an unsafe situation exists, employees are encouraged to call the Center Police at 8019 immediately. In addition, the officers are available to escort employees to their cars in the parking lot. Safety Program If you encounter a safety issue, report this to your instructor and manager of the unit. Customer Relations It is everyone’s responsibility in the Center to provide great service to our customers. This means using “good manners” at all times. Always take a person where they need to go – do not point and give directions. If someone looks lost, ask if they need assistance Answer call lights immediately Ask patients, “Is there anything more I can do for you, I have time.” If you encounter a patient or family member who has a complaint – contact your instructor, manager of the unit and Patient Representative at ext. 8555 or (740) 687-8555. AIDET Acknowledge—Acknowledge the patient by name. Make eye contact. Ask: "Is there anything I can do for you?" Introduce—Introduce yourself, your skill set, your professional certification, and experience. 13 Duration—Give an accurate time expectation for tests, physician arrival, and tray delivery. Explanation—Explain step by step what will happen, answer questions, and leave a phone number where you can be reached. Thank—Thank the patient for choosing your hospital, and for their communication and cooperation. Thank the family for assistance and being there to support the patient Event Reports (formerly known as incident reports) ALL incidents that occur on Center property involving patients, visitors, and employees must be reported. Three different incident reports are available, depending on the situation. An incident report should never be filed in the patient record or photocopied. All information must be factual. The incident report is to be completed by the individual at the time of the incident! 1. Computer Event Report Form (Open Microsoft Word, click File>New>FMC Forms) The Event Report Form is used to report incidents involving: Employees Physicians Allied Health Staff Volunteers Students Visitors When an employee has an incident or is injured on the job, follow these steps: 1. 2. 3. 4. 5. Report incident to Manager/Supervisor. Complete the incident report. If medical attention is needed- seek treatment in Employee Health. The Emergency Department is for emergencies only and must be authorized by calling the Manager or House Supervisor on duty. The Manager/Supervisor will complete an investigation into the incident. Management will send the completed form to Employee Health within 48 hours of the incident. When a visitor has an incident or is injured, follow these steps: 1. 2. Offer immediate First Aid and call the House Supervisor or your Manager. The Incident Report should be completed by the person who witnessed or found the visitor 14 2. Patient Event Report Form (Tan Color Form*) (Note: Patient Incident Reports may also be completed on the AS 400, under QA Incident Report) You would fill out a patient incident report when an incident occurs that is not within the norm for patient, such as: When a patient falls Performing the wrong procedure on a patient Performing the procedure on the wrong patient This form must be completed immediately after the incident and care of the patient. It should be reviewed by your instructor before submission to the nurse manager. 3. Medication Event Report Form (Salmon Color) Whenever a medication incident or potential medication incident occurs, even if the error does not reach the patient. Be sure to fill out the form as completely as possible. Turn into your instructor for review and then to the manager of the unit. Falls Program You will know if a patient is at High Risk for Falling when you see a yellow dot on patient’s chart and on name card on patient’s door; High Fall Risk label at head of bed below patient’s name; Yellow wrist band on the patient. Patient Rights and Responsibilities All patients and family members need to know where the patient rights and responsibilities are located. It is you responsibility as a healthcare provider to assist them. There are patient rights brochures on each unit. Confidentiality / HIPAA All students and employees have the legal and ethical responsibility to keep all information about patients and their families confidential and private. Patient information may only be discussed with other healthcare providers who need that information in order to do their job. Safety Issues If you note a safety issue at Fairfield Medical Center you should call the safety hotline at 687-8988 15 TABLE OF DANGEROUS ABBREVIATIONS & SYMBOLS The following list of abbreviations and symbols has compiled by the Pharmacy and Therapeutics Committee due to their potential for error. Please do not use these dangerous abbreviations or symbols. Abbreviation/Symbol MgSO4 Intended Meaning Magnesium sulfate Misinterpretation Morphine sulfate Correction Use “magnesium sulfate” or “mag sulfate” Magnesium sulfate Use “morphine” or “morphine sulfate” Magnesium sulfate Use “morphine” or “morphine sulfate” mg Use “mcg” Read as a 0 or 4 “unit” has no causing 10-fold acceptable overdose, 4U seen as abbreviation. Use “40” or 4u seen as “44” “unit” Misread as IV Use “international (intravenous) units” or “units” Misread as “U” or “00” Use “ml” MSO4 Morphine sulfate MS Morphine sulfate ug U or u Microgram Unit IU International units cc Cubic centimeter Zero after decimal point (1.0) 1mg Misread as 10mg if decimal point is not seen No zero before decimal point (.5mg) 0.5mg Misread as 5mg if the decimal point is not seen QD, qd Daily QOD, qod Every other day. Misread as QID or QOD Misread as QD or QID Do not use terminal zeros for doses expressed in whole numbers Always use zero, before a decimal point when the dose is less than a whole number Use “daily” Use “every other day” 16 FAIRFIELD MEDICAL CENTER Subject: Parking Regulations Students must park in the student lot located on South Ewing street across from Anchor Hocking. This is for day shift. Evening shift students will parking in the J lot. Parking in the garage is completely prohibited. Students are not to use the Valet parking. Tickets will be issued to those that do. – Greater than 2 tickets for any reason will result in removal of student from their clinical at Fairfield Medical Center 17 FAIRFIELD MEDICAL CENTER Subject: Personal Appearance EMPLOYEE HANDBOOK HUMAN RESOURCES POLICY & PROCEDURES Supersedes: June 20, 2011 Effective: August 1, 2011 Page 1 of 2 POLICY It is the policy of Fairfield Medical Center (FMC) that each employee’s dress, grooming, and personal hygiene should be appropriate to the work situation and in a professional manner that inspires confidence and trust among patients and visitors and presents a professional, positive and consistent image to those we serve. PURPOSE This policy is the Center-wide Personal Appearance policy. Minimally, each department will adhere to these standards and may require a more restrictive dress code based on operational, infection control, and safety needs. More restrictive requirements must be reviewed and approved by Human Resources and will be communicated, interpreted, and enforced by the manager. Employees in the Patient Services Division should refer to the Patient Services Dress Code Policy for further details. PROCEDURE I. Employees are expected to present a professional, businesslike image to customers and the public at all times. Clothing must be clean, neatly pressed, in good repair, properly fitted, not revealing and appropriate for the type of work performed. Acceptable personal appearance is an ongoing requirement of employment with the Center. Radical departures from professional dress or personal grooming and hygiene standards will not be permitted unless authorized by the appropriate Chief Officer or the department requesting the variance. II. All employees are required to wear their Center ID badges facing forward while working. III. Any employees who work in an office setting, and/or have regular contact with the public must comply with the following personal appearance standards: A. Employees are expected to dress in a manner that is acceptable to the established standards of the Center and requirements of their department. Employees should not wear suggestive attire including backless tops, tank tops or spaghetti straps, jeans, sports clothing, shorts, sandals, flip flops, slippers, T-shirts, novelty buttons, non-approved hats, sleeveless shirts, blouses or dresses unless worn with a jacket or sweater and similar items of casual attire that do not present a professional appearance. B. All employees are required to be well groomed, practice appropriate personal hygiene and use good judgment in dressing appropriately for their position, within the requirements of this policy. C. Hair should be clean, combed, and neatly trimmed or arranged. Unkempt hair is not permissible, regardless of length. Sideburns, moustaches, and beards should be neatly trimmed. D. Tattoos (except for medical alerts) and body piercings, other than two earrings per ear, cannot be visible. FAIRFIELD MEDICAL CENTER Subject: Personal Appearance EMPLOYEE HANDBOOK HUMAN RESOURCES POLICY & PROCEDURES Supersedes: June 20, 2011 Effective: August 1, 2011 Page 2 of 2 E. Artificial nails are not to be worn by employees performing clinical tasks. Natural fingernail tips are to be kept less than ¼ an inch long by employees performing direct clinical tasks. Nail polish, if permitted and worn, should be free of chips. F. Employees attending training classes at the Center must wear business casual attire (No backless tops, tank tops or spaghetti straps, jeans, sports clothing, shorts, sandals, flip flops, slippers, T-shirts, sleeveless shirts, blouses or dresses unless worn with a jacket or sweater). IV. Employees who do not regularly meet the public should follow basic requirements of safety and comfort, but must still be as neat and professional as working conditions permit. V. Certain employees may be required to meet special dress, grooming and hygiene standards, such as wearing uniforms or scrubs, depending on the nature of their job. These requirements are specified by individual department policies. A. Specifically, for Patient Services, there is a color requirement in uniforms for four main reasons: patient satisfaction, patient safety, hospital image, and professionalism. These requirements are in place for the purpose of improving safety, quality, and patient satisfaction; other employees may not be dressed in like manner. 18 1. RNs – navy scrub pants, scrub top, and lab jacket (as needed). 2. Clinical Nurse Leaders – white pants, scrub top, lab jacket (as needed), & shoes. 3. Clinical Coordinators – navy pants, white shirt, white lab jacket (as needed), & white shoes. B. Couriers and other employees that work outside may wear hats (FMC Logo only) outside FMC facilities and in their vehicles to protect themselves from temperature extremes and from sun exposure. VII. At the Center’s administrative discretion, employees may be permitted to dress in a more casual fashion than is normally required. On these occasions, employees are still expected to present a neat appearance and are not permitted to wear ripped or disheveled clothing, athletic wear, or similarly inappropriate clothing. Human Resources will give advance notification of what type of casual wear, e.g. hospital T-shirts or college sweatshirts, may be worn and the times that such clothing will be permitted. VII. Any employee who does not conform to the standards of this policy will be sent home and required to change clothes that meet the acceptable established guidelines of this policy. Hourly employees will not be compensated for any work time missed because of failure to comply with this policy. Violations of this policy may also result in disciplinary action up to and including termination for repeated failure to follow the policy. 19 Student Verification Agreement Student Name______________________________________ School____________________________________________ I, ________________________(representative from school) do consent and verify that __________________________(Student’s name)has received the following: (Please check all that apply) _____ Criminal background check _____ Current TB test(within the current year) _____ Immunizations to include; MMR, Varicella and Hepatitis _____ 5 Panel drug screen _____ Flu Vaccine _____ Current CPR Card , if applicable That his or her record meets the Fairfield Medical Center permissible standards. Fairfield Medical Center honors the partnerships and maintains that integrity with all programs and students who use the Fairfield Medical Center facilities. Signature on this record substanciates that the school/college/university maintains current and accurate records of the above. That FMC may contact an individual institution and request copies of the records. **If the school program cannot verify that this student has received the above then the student must provide Fairfield Medical Center with a copy of those items required for their application Signature ____________________ (Representative from school) Title _______________ Date_________ 20 TO BE SIGNED BY EACH STUDENT AS A CONDITION OF PARTICIAPTION IN ANY STUDENT/INTERN/SHADOW EXPERIENCE CONFIDENTIALITY STATEMENT I understand that as a student completing my internship/shadowing experience at Fairfield Medical Center, I may be exposed to confidential information regarding patients and financial information produced by or held by Fairfield Medical Center. During the term of my visit with Fairfield Medical Center and any related activities, or any time thereafter, I shall not directly or indirectly, make or cause to be made, any disclosure or other use not authorized by Fairfield Medical Center of any confidential information acquired during the course of my experience at Fairfield Medical Center unless such information is or becomes otherwise legally available to the public. For purposes of this agreement, the term “confidential information” means any business, medical or financial information not generally known to the public at large regarding the business and operations of Fairfield Medical Center and its patients, employees and physicians. Any breach of confidential information by me shall constitute grounds for immediate termination from my internship/shadowing experience at Fairfield Medical Center and can further be grounds for any legal action taken by the offended parties. WAIVER OF LIABILITY/RELEASE WITH ASSUMPTION OF RISK AND INDEMNIFICATION In exchange for the agreement of the Hospital to permit participation in any student/intern/shadow experience, I hereby voluntarily assume the risk of injury and waive, release, and agree to hold harmless and indemnify the Hospital, its employees and agents from any and all liability, arising from negligence or otherwise, and all damages in any way resulting from participation in any student/intern/ shadow experience at the Hospital, including but not limited to bodily, personal, or mental injury. The undersigned, has read the above carefully, understand its significance, and voluntarily agree to all of its terms. NOTICE OF PRIVACY PRACTICES ACKNOWLEDGEMENT By signing below, I acknowledge that I am in receipt of Fairfield Medical Center’s Notice of Privacy Practices. Date: ______________________ ____________________________________ Student Signature ____________________________________ Student Name (printed) If student is under 18 years of age, the student’s parent or guardian must also sign this statement: Date: _______________________ ____________________________________ Parent Signature ___________________________________ Parent Name (printed) Student Application- Fairfield Medical Center 21 PERSONAL Student Name _______________________________ Phone # ________________________ Address____________________________________ Cell # __________________________ City/State/Zip ________________________________ Email __________________________ If under 18 yrs of age, please check _______ Please complete: REQUEST # Hrs _________ Clinical Rotation______ Shadowing_______ Internship________ Department(s)_______________________________Dates_____________________ Have you made contact w/this department? Y N Dept. Contact Name ___________________ Are you currently employed/volunteer or have you ever been employed/volunteered at SCHOOL FMC Fairfield Medical Center or any of its affiliate in any capacity? Y N If yes, date____________________ and department School Name __________________________________ __________________________________ Instructor _____________________________________ Instructor Email_________________________________ Phone____________________________ Program Graduation Date____________ In consideration of of myStudy_______________________________ student experience at Fairfield Medical Center, I agree to Expected conform to the rules and regulations of this facility. I understand that my experience can be terminated at any time and for any reason, at the option of either the facility, the school or myself. I understand that this student experience does not enter me into an agreement of employment with this facility. I hereby affirm that the information provided on this application (and accompanying resume, if any) is true and complete. I understand that any false or misleading representations or omissions may disqualify me from this student experience and further disqualify me from consideration for employment. I hereby authorize persons, school, and employers named in this application (resume, if any) to provide this facility with any relevant information regarding my student experience, and I release all such persons from any liability regarding the provision or use of such information. Signature ______________________________________________ Date _____________________________ My typed name above shall have the same force and effect as my written signature. Your signature verifies that you have read and understood all that is contained In this packet and hereby agree to adhere to the standards Email to Becky DeVoss at rebeccas@fmchealth.org or by mail to: Becky DeVoss, Staff Development Fairfield Medical Center 401 North Ewing Street Lancaster, Ohio 43130 Fairfield Medical Center 22 Student Orientation Post Test Name: _______________________ School: ____________________ Date: _______________ For questions 1-10 write the letter which matches the proper emergency code. 1. ____ Code Red 2. ____ Code Blue 3. ____ Code Black 4. ____ Code Green 5. ____Code Orange 6. ____Code Violet 7. ____Code Silver 8. ____Code Grey 9. ____Code Brown 10. ____Code Adam A. Stay Away – Violence of hazard B. Missing Adult C. Large influx of patients, Emergency plan activated D. Fire E. Medical Emergency F. Child Abduction G. Severe weather H. Person with weapon I. Combative person J. Bomb Threat 11.If there is an emergency in the hospital what number would you dial? _____________ 12.What do the initials PASS mean? P ___________________________________________________ A___________________________________________________ S___________________________________________________ S___________________________________________________ 13. As part of the hospitals commitment to the “Patient’s First” ethic, you must respect a patient’s religious and cultural belief’s or practices unless safety or medical necessity dictates otherwise? True ___ False___ 14. The type of event report that is used for visitors is? __________________________________ 15. What is an example of a blood borne pathogen? ____________________________________ 16. What color denotes that the patient is at high risk for falling? _________________________ 17. List 3 dangerous abbreviations. _________________, ________________, _______________ 18. We have the responsibility to report any suspected signs of abuse. No individual reporting abuse shall be criminally liable for any report required or authorized by law unless it can be proven that a false report was made and that the person knew that the report was false. True__________ False__________ 19. It is the responsibility of any employee or student to keep all information about our patients and their families confidential. True _________ False______________ 20. Who is responsible for providing customer service for our patients and their families? a. Physicians b. Nurses c. No One d. Every One 23 21. What are Universal Precautions? _________________________________________________________ 22. If you have lost your coat at Fairfield Medical Center who would you go see to help locate it. ____________________________________________________________________________________ 23. You are allowed to wear jeans and sandals at Fairfield Medical Center? True_________ False ________ 24. As a student you are allowed to park in the parking garage. True ______ False________ 25. Are students allowed to use their cell phones on units that have patients? Yes____ No _____ 26. You are allowed to smoke in the bathrooms at Fairfield Medical Center? Yes ______No _______ 27. As a student, selling Avon while you are on duty is considered solicitation. Yes _____ No _______ 28. What is the number to call the Center Police? ________________________________________ 29. What is the Safety Hotline Number? ________________________________________________ 30. A piece of equipment that you are using breaks. You should tell your instructor, manager of the unit, mark it as broken and take it out of service. Yes______ No _______ 31. In the event of a power failure the generators start up in how many seconds. ___________ 32. _____________________ is the single most important procedure in Infection Control. 33. The two patient identifiers we use here at Fairfield Medical Center. ________________________ ________________________________________ 34. Tattoos may be seen by our patients? No ____ Yes_____ 35. How many piercings are you allowed to have when you work at Fairfield Medical Center. ________ 36. What does TJC stand for? ____________ ________________________ _______________________ 37. Personal Protective Equipment includes: select as many as apply ____ Goggles ____ Gloves ____ Gowns ____ Masks 38. – 40 I have read the student manual and will comply with the rules and regulations set forth. Non -compliance may lead to dismissal from the Center. _______________________________ Signature ______________________ Date Signature ______________________ Date__________________ 24 FAIRFIELD MEDICAL CENTER STUDENT SECURITY REQUEST FORM (If Applicable) Last Name First Name School/College/University Medical Field Middle Initial FOR CLINICAL EDUCATION COORDINATOR TO FILL OUT Security Access required for the following Applications ( Student Coordinator will approve and submit request) Systems Network Login CPOE Single Sign-On Portal Other_____________ Clinical Documentation Inpatient Documentation (HED) HSM - surgery Other _________________________________________- Clinical Education Coordinator ___________________________________Date________________________ SYSTEMS ACCESS SECURITY AGREEMENT(If Applicable) I, __________________________________________________ have read, understood, and will comply with the following: 25 (Last name, First name, Middle initial) I am the only person authorized to use my password(s) and user ID(s). I will not disclose my password(s) or user ID(s) to anyone. I will not attempt to learn another person’s password(s)/user ID(s). I will not attempt to access information by using a password(s) or user ID(s) other than my own. I will retrieve or attempt to retrieve from the computer system only medical data that is directly related to the treatment of patients with whom I have a clinical relationship or those patients for whom I have been asked to provide a consultation or for approved educational or research purposes. I agree to maintain the confidentiality of all such patient data. I will access patient data only as required by my employment or medical staff responsibilities or for approved educational or research purposes. It is my responsibility to logout of the system. I will not, under any circumstances, leave a computer terminal to which I have logged in unattended. If I have reason to believe that the confidentiality of any of my password(s)/user ID(s) has been compromised, I will contact the Systems Department immediately so that my password(s)/user ID(s) can be deleted and a new password(s)/user ID(s) assigned to me. I will immediately report any known or suspected breach of the confidentiality of the system or records/data obtained from it to the Medical Information Services manager. I understand that my password(s)/user ID(s) will be deleted from the system when I am no longer employed or have privileges at this institution or when my job duties do not require access to the medical record database. I will immediately report any such status change to the Systems Department. I understand my access will be automatically deactivated after 90 days of non-use. I understand that medical records confidentiality is required by law, and that there are statutes specifically mandating the confidentiality of, among other areas, mental health, HIV, and drug and alcohol-related treatment records. I understand that any fraudulent application, violation of confidentiality or any violation of the above provisions may result in disciplinary action from termination of access to the system or appropriate medical staff or University disciplinary measures up to and including termination of my employment with the University or the hospital. I understand that the Systems department maintains an audit trail of accesses to patient information that records the user, date, and patient identification of all accesses to electronic medical records. I understand that my access rights are subject to periodic review, revision and annual renewal. NEW FOR 2012: I will not attempt to connect any personal laptop, PC, or hand-held devices to the private hospital wired or wireless networks. I will not attempt to alter any security software, filters, policy, or configuration on any hospital devices. I will not load, install, or remove any software on a hospital device or on the Common Desktop without assistance or approval from the FMC Systems department. (This includes screensavers and Internet toolbars). I understand that I am absolutely liable for all activity that takes place under my credentials. I understand that if I do not accept these restrictions of access I may be denied access or have access terminated to relevant computer systems and networks. Applicant Printed Name_____________________________________________________________________________________ Office/Department/Unit: _______________________ Title/Position:__________________________ Telephone Number: _____________________ For Students: Start Date______ __End Date________ Physician Preceptor______________________ E-Mail Address: _____________________________ ________________________________________ Signature _________________ Date Supervisor or Office Manager of Person Approving Issuance of this Account: Name___________________________________ ________________________________________ Signature Position______________________________ Telephone Number_________________________ __________________ Date SYSTEMS ACCESS SECURITY AGREEMENT 26









© Copyright 2025