
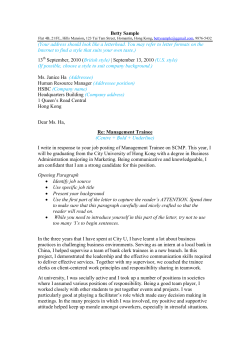
Hepatitis C Enrollment Form
Hepatitis C Enrollment Form FaxReferral Referral 877-552-2907 Phone: 888-345-1678 Fax To:To: 877-552-2907 Phone: 888-345-1678 Email Referral To: To: customerservicefax@caremark.com E-mail Referral customerservicefax@caremark.com 6 Simple steps to submitting a referral 11 PATIENT INFORMATION 22 PRESCRIBER INFORMATION Prescriber’s Name: (Complete the following or include demographic sheet) Patient Name: State License #: Address: DEA #: City, State, Zip: Group or Hospital: Primary Phone: Home Alternate Phone: Home DOB: Gender: Cell Cell Male Work Address: Work City, State Zip: Female E-mail: Last Four of SS #: NPI #: Phone: Fax: Contact Person: Phone: Primary Language: 3 INSURANCE INFORMATION Please fax copy of prescription and insurance cards with this form, if available (front and back) 4 DIAGNOSIS AND CLINICAL INFORMATION Diagnosis (ICD-9 or ICD-10): 070.54 Chronic Hepatitis C Needs by Date:__________ Ship to: 070.51 Acute Hepatitis C Patient 050.5 Liver Transplant Office 042 HIV Other:___________ Other:_____________ ICD-10 Code & Description:_____________________________________________________________________________________________________ Patient Evaluation: Height: ____________________________in/cm HCV Genotype: Is patient: 1a Naïve 1b 1 2 Partial Responder 3 Weight: ____________________________kg/lbs 4 5 Non-Responder Last Date of Therapy: Allergies:____________________________ 6 Relapser Product Names: Is patient currently on Hepatitis C Virus (HCV) therapy? Yes If Yes, Therapy Start Date: No Product Names:________________________________________________________________ Specialty Pharmacy to coordinate injection training/home health nurse visit as necessary. Yes No PRESCRIPTION INFORMATION 5 MEDICATION PEGASYS PEGINTRON DOSE/STRENGTH 180 ug/0.5 ml ProClick Autoinjector Other REDIPEN® 120 mcg 150 mcg Other RIBAVIRIN 200mg tablets RIBA-PAK 600/600mg 400/400mg 200 mg caps VICTRELIS™ (boceprevir) 200mg capsules 600/400mg 200/400mg DIRECTIONS QUANTITY REFILLS Inject 180ug subcutaneously once a week as directed Inject __ mcg subcutaneously weekly Other: Take __ tabs/caps oral qam and __ tabs/caps qpm to equal a total of ____ mg/day . Take ___ mg oral qam and ___ qpm to equal a total of ___ mg/day Take 800 mg orally three times daily every 7-9 hours with food. Begin after week 4 of pegylated interferon therapy. 28 day supply Sovaldi (sofosbuvir) 400 mg tabs Take one 400mg tablet orally once a day 28 day supply Olysio (simeprevir) 150 mg capsule Take one 150mg capsule orally once a day 28 day supply Maximum12wks Take orally once daily. 28 day supply Maximum 8wks Maximum12wks Sofosbuvir/ ledipasvir Fixed-dose combination tablet of 90 mg of ledipasvir/400 mg of sofosbuvir Patient is interested in patient support programs 6 STAMP SIGNATURE NOT ALLOWED X DISPENSE AS WRITTEN Ancillary supplies and kits provided as needed for administration X (Date) PRODUCT SUBSTITUTION PERMITTED (Date) IMPORTANT NOTICE: This facsimile transmission is intended to be delivered only to the named addressee and may contain material that is confidential, privileged, proprietary or exempt from disclosure under applicable law. If it is received by anyone other than the named addressee, the recipient should immediately notify the sender at the address and telephone number set forth herein and obtain instructions as to disposal of the transmitted material. In no event should such material be read or retained by anyone other than the named addressee, except by express authority of the sender to the named addressee. Hepatitis C 022514




















© Copyright 2025