
Downloaded from by guest on June 9, 2014 ajcn.nutrition.org
/3-Carotene
Hannes
and cancer
B St#{228}helin, K Fred
ABSTRACT
Basel
In 197 1-1973
Study
carotene
started
and
their
l2-y
observation
families
(lung cancer
malignancies
were
Low
intake
risk.
examination
antioxidant
553
men
Eric
L#{252}din
of the
vitamins
of2974
men.
in 1977-79.
(1973-85)
and
Electric
A subsample
During
the
died,
204
bronchus
cancer,
stomach
with the 2421 survivors.
carotene
(< 0.23 mol/L)
plasma
lung
study
J C/in Nuir
which
cancer
model).
carotene
is known
associated
with
(all
to reflect
ach
cancer,
physiologic
cancer-risk,
variation,
vitamin
A, plasma
fact
contains,
car-
mortality
and
vitamin
incidence
of carotene
other
could
substances
biological
of
be as-
plasma
cancer
incidence.
a large
which
effects.
analyzing
and
follow-ups
prospective
in 1980
and
might
Additional
cv-
concentrations
study
1985
l2-y mortality
from
of the 7-y mortality
an inverse
subsequent
begun
between
cancer
variations
allowed
cancer
and
was among
relationship
lung
physiological
levels
many
studies
Study,
levels
surveys
to the
of
in
1959,
at the third evaluation
(BS III) in 197 1-1973
all plasma
in 2974 participants
ofthe
follow-up
exam.
Subsequent
ofthe
7- and
The analysis
stom-
however,
compounds
Basel
epidemiological
related
risk ofbronchus
cancer
was confirmed
(6-9).
Food rich in antioxidant
corn-
from
The
first
was
low
idence
comes
the
that
for the observed
measured
vitamins
cancer
lung cancer,
The
antioxidant
199 l;53:265S-9S.
/3-Carotene,
among
of carotene
be responsible
onstrate
KEY WORDS
intake
cancer.
pounds
Higher
risks
and retinol
increased
(5) was
the
sociated
with an increased
later on by several
studies
of cancer
The relative
risk
was significantly
cancer
(Cox’s
< 0.0 1) ifboth
carotene
is in our
Am
and
Study
in which
and
death
serum
(6).
in carotene
evaluation
carotene
In the present
levels,
age, and sex as well as a 7- and
plasma
carotene
are presented.
the
other causes
(10).
the first to dem-
12-y
influence
mortality
levels
paper
oflife
the
style,
in relation
to
Introduction
Study
Migration
cancer
studies
incidence
promote,
most
and
or retard
obvious
eating
the
suggest
and
Quality
cancer
between
and
occurring
differences
environmental
prevent
differences
habits.
naturally
that
factors
formation.
nations
composition
fore not surprising
that
nutrients
thought
to affect profoundly
the
Among
widely.
The
initiate,
are specific
varies
in
on
the
food
factors.
vitamins
Less effort
was
and
in the past
to look
It is there-
protective
Among
factors
(3).
the mechanisms
thought
to influence
free radical
formation
is of particular
damage
DNA,
structural
proteins,
and
lead
free
radicals
to toxic
products
(4). The
interest.
enzymes,
body’s
carcinogenesis,
Free radicals
can
and membranes,
rotenoids.
affecting
pected
heavily
On the other
differentiation
to play
Am J C/in Nutr
a role
hand,
and
in cancer
l99l;53:265S-9S.
on
defense
antioxidant
system
vitamins
development
and
chronic
Printed
and
vitamins
against
and
other
micronutrients
have
long
diseases.
in USA.
The
been
casus-
Western
© 1991 American
methods
was
started
of Basel
to participate.
The
and in 1971-1973
in extensive
clinical
of a study
mediately
of this
after
or later
size,
1959
(4858
study
of the
phar-
laboratory
all plasma
reevaluated
males,
(BS III:3528
were
major
i age
39 ±
1 1 y)
was
repeated
in
males, 48 ± 10 y).
invited
to participate
analyses.
As a unique
vitamins
were
in all participants.
in 2974 men.
of married
probands
were
as a prospective
examination
the subjects
and
venipuncture
set was available
A subsample
1925
in
( 1 1 ). Employees
of death
At the BS III examination
in the
feature
measured
im-
A complete
data
with
children,
and
born
Basel
Family
Study
(12)
in 1977-1979.
This allowed
an estimate
ofthe
predictive
power
ofa single plasma
vitamin
determination
in 3 1 3 men as well as
the evaluation
of the influence
of age and sex.
Clinic, Kantonsspital,
University
of Basel, Inand Molecular
Biology, University
of Berne and
Unit for Biostatistics,
F Hoffmann-La
Roche Ltd. Basel, Switzerland.
2 Address
reprint requests to HB St#{228}helin,Kantonsspital
Basel, CH4031 Basel, Switzerland.
I
depends
and
companies
1965-1968
for protective
Nevertheless,
increasing
evidence
suggests
that certain
and antioxidant
compounds
may act as preventive
or
Study
causes
volunteered
and food
composition
are
occurrence
of cancer
( 1 , 2).
spent
Basel
major
maceutical
Cancer,
like other
chronic
diseases
such as atherosclerosis,
is
not caused
by a single factor, but is a multifactorial
event. Hence,
much
emphasis
has been placed
on the search
for risk factors
for cancer.
population
From
the Geriatric
stitute of Biochemistry
Society
for Clinical
Nutrition
2655
Downloaded from ajcn.nutrition.org by guest on June 9, 2014
low.
otene
at the third
the major
elevated
(P
< 0.05)
for lung
were noted
for all cancer
(P
were
Eichholzer,
the Basel Study
68, stomach
cancer
20; colon
cancer
1 7, all other
99). We found
significantly
lower
mean
carotene
compared
with low
<
Monika
in the plasma
reinvestigated
period
for all cancer,
0.01)
ofsubjects
P
in 1959,
were measured
levels
Gey,
prevention:
STAHELIN
2665
TABLE
I
Basel Study
197 1 - I 973: intercorrelation
Vitamin
Carotene
VitaminA
Vitamin E
Vitamin
C
r
S
The
= P
paper
ofthe
deaths)
and 1985 (with
ofall but eight subjects
death
certificates
certificate
Cancer
death
(lCD
162. n
I 7), and
=
The
the
after
blood
24-mo
Seasonal
rection
results
intervals
from
The
morning
lung
153,
and
state).
in the
a-carotene.
Carotene
after
adjusting
and
age and
and
is based
for cholesterol
on the comparison
and
on the estimation
triglycerides
ofrelative
risk comparing
the
levels.
was
in lung
The
hazard
vitamins
coefficient
for car-
0.45.
102 cancer
more
often
2 gives
lower
levels
the
previously
(6), carotene
stomach
lower in stomach
in all cancer
(P
vitamin
<
cancer
0.01).
cancer
A and
(P
<
for
(P
0.01).
<
result
only
was significantly
(P
<
vitamin
0.05);
0.0 1 ). Among
C were
vitamin
sig-
C was
The individual
cancer
risk may be estimated
more conclusively
by calculating
relative
risks. For this purpose
the cancer incidence
in subjects
with values
in quartile
1 was compared
to the mci-
Results
2.0
0.
P/zisiologic
variation
olpiasma
carotene
1.8
..a
....
..
.. .........
thPrcnt6
......D.........
Carotenes
correlate
weakly
but significantly
lesterol
in fasting
subjects
(r = 0.23), but not
The
car-
the 204 cancer
plasma
only
low
adjusting
survivors
2) influenced
and
carotene
ob-
for carotene
(Table
cholesterol
cancer
with
values
is calculated
to the 2421
were
an additional
due to cancer.
in subjects
the mean
C. Significance
Compared
antioxidants
deaths
S-y from
1980-85
totaling
in 204 deaths
Table
As reported
other
in quartile
of antioxidant
correlation
period
occurred
A and
for
originally
incidence
on the average
nificantly
also lower
subjects
vitamin
proportional
had
marginally.
of means
death
intake
The
7-y follow-up
smoking.
was
as well as smoking
below
quartile
1 with subjects
with higher
relative
risk was estimated
using
Cox’s
regression
model
(13. 14).
the
vitamins
Adjusting
subjects
6 y later. Similar
proportions
third quartile.
Hence,
a single
measurements
concentration.
age and
lower
analysis
two
cohort.
and cancer
Cancer
Basel
for cholesterol.
statistical
0.062
0.391
0.722
-0.056
long-term
in our
for the
otene
cases
-20%
reflects
Carotene
place
a tentative
corgave no different
contains
-0.059
0.391
0.502
-0.074
one-halfofthe
served;
during
the following
102 cancer
deaths
occurred,
(I I). During
in a fasting
about
carotene
During
took
/3-Lipoproteins
in the lowest
quartile
for the second
and
measurement
otene
58.6%).
measured
sampling
in 1971-1973
/3-carotene
standardized
previously
that
1 were still
were found
37).
=
Triglycerides
0.234
0.254
0.561
-0.046
and
death
below.
as analyzed
-80%
The
Tuesday
presented
the
were
were observed.
Nevertheless,
variation
in a logistic
model
the one
carotene
area
(every
variations
ofseasonal
vital status
is based on
rate
153, n
triglycerides
as described
Cholesterol
revealed
1971-1973.
(autopsy
in 197 1-1973.
C
men.
in 1980(268
If possible,
15 1 +
and
period
from
down
into cancer
of the
151, n = 20), colon(ICD
(lCD
sampling
sampling
at weekly
broken
(lCD
cholesterol,
for 2974
deaths).
The
the analysis
result
and lipids*
0.175
-0.018
0.021
coefficients
revision).
vitamins,
Vitamin
was completed
by the autopsy
gastrointestinal
vitamins,
shortly
8th
AL
adjustment
ofcarotene
levels
1.6
with plasma
chowith triglycerides.
for cholesterol
is advisable
1.4
to
1.2
ensure
comparability
ficients
in different
observed
likewise
a small
in our
groups.
groups
influence
are
The
given
as shown
correlation
coef-
1. Age has
1 where results
in Table
in Figure
I
the
Basel
Family
Study
are
given.
Females
have
506P.cc.nb$.
Q...
0
from
Fmas
1.0
0.8
higher
0.6
carotene
concentrations
despite
levels. Ofparticular
importance
levels
significantly.
levels.
Nonsmoking
tration
of 0.38
(- 18%. P
(-27%,
P
<
<
Smokers
have
survivors
Mmol/L,
had
while
0.01). A similar
0.5) and lung
1973
examination
participating
(BS
III)
at the
consistently
a median
smokers
difference
cancer.
Carotene
levels depend
on
plasma
levels for all antioxidants
subgroup
their lower plasma
cholesterol
is smoking.
It influences
carotene
had
Basel
carotene
a median
was observed
carotene
0.4
5th
P.rCOnt4S
0.2
concenof 0.31
0
1’O
20
30
40
50
60
for all deaths
Ag.
dietary
habits.
determined
with
lower
A comparison
of
during
the 1971-
determinations
Family
made
Study
in the
(1977-1979)
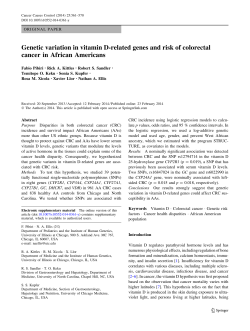
FIG I . Carotene
plasma values in parents and children:
distribution
ofcarotene
in 1998 participants
ofthe Basel Family Study (1977-1979).
Broken lines represent
values from females, solid lines represent
values
from males (506 fathers, 509 mothers,
SOS sons, and 478 daughters).
Downloaded from ajcn.nutrition.org by guest on June 9, 2014
n
F
on the data
cohort
(lCD
was further
68). stomach
=
correlation
a total of 553
was ascertained;
was checked
antioxidant
0.214
0.340
concentrates
follow-up
carotene,
Vitamin
0.00 1: Pearson
<
present
A mortality
the
A
-0.03
0. 1
>
of plasma
ET
CAROTENE
TABLE
Plasma
2
values
at BS III of carotene
and vitamins
AND
A and C for survivors
2675
CANCER
and cancer
groups*
l2-y mortality
Survivors
(n = 2421)
Carotene
Carotene
Vitamin
Vitamin
*
(zmol/L)
(tmol/L).
A (imol/L)II
C (zmol/L)
± SEM:
.
0.436
0.428
2.81
52.76
All P values
± 0.005
± 0.005
±
±
calculated
0.01
0.44
considering
Bronchus
cancer
(n = 68)
Stomach
(n
0.295
0.297
2.77
52.38
0.281
0.274
2.60
42.86
smoking
±
±
±
±
0.025t
0.026t
0.07
3.68
follow-up
=
cancer
20)
Gastrointestinal
cancer
(n = 37)
0.O4lt
0.035t
0.08
4.88t
0.365
0.362
2.79
45.90
±
±
±
±
±
±
±
±
All cancer
(n = 204)
0.046
0.047
0.09
3.57
0.344
0.342
2.81
47.61
0.Ol6t
0.017t
0.04
l.78t
±
±
±
±
and age.
t P < 0.01.
tP<0.0S.
§ Adjusted to cholesterol.
II Adjusted
among
carotene
also
for
Table
subjects
with
(quartile
1) was
smoking,
age,
higher
0.23
and
risk
ofdeath
all cancer
associated
Low
carotene
low
with
and
carotene
< 0.05)
(RR
P
0.05
<
(P
oflow
risks (RR)
died within
unchanged
as of low
carotene
for
results
in bronchus
and
risk
be caused
this question
we analyzed
in
cancer).
(P
<
0.01).
the
RR
1 .8,
P
in all cancer
effect of carotene
phenomenon.
To
risks
ofthe
carotene
(quintile
small
numbers
in the estimates.
carotene
No of
subjects
6
All values
adjusted
for smoking,
may
It is noteworthy
for plasma
the
same
significantly
higher
ERR 2.2 1 ; I .03-4.74
and
for all cancer
in Basel
(RR
95%
con-
1 .5 1 ; 1.01-
poor
status
burgh,
‘--20%
than
in Finland,
and Italy, and
loss in frozen
lower
can be characterized
in
ofwhich
were analyzed
(4, 6, 8, 16, 1 7). The
has a relative
ofcarotene,
Basel
semialpine
Switzerland
60% lower than in France
(18). Considering
samples,
it may be estimated
to be 35-60%
in Washington
County
(6,
pop-
as low as in Edin-
17), Hawaii,
and
the
storage
lower
London
Area (19).
in our
tioned
probably
and
and its interaction
Follow-up
same
in Basal
the samples
ulation
than
instability
4), although
essentially
had
0.04).
=
laboratory
retinol
some
A
cancer
0.03]
in the
cancer
low
values
Low vitamin
A
2.45 Mmol/L)
Low /3-carotene
and low vitamin
P
P
(lung
average
(<
(CI),
give
Discussion
produced
Bronchus
cancer
Lowcarotene
(< 0.23 Mmol/L)
All cancer
Lowcarotene
for bronchus
interval
95% CI,
study
population
to other cohorts,
the relative
limits
risks
fidence
The male
comparison
and
cancer
1 for carotene
by subclinical
above
3
risks and 95% confidence
bronchus
in quintile
relative
2.27,
risk of subjects
in quintile
3 was set to 1 . Figure
a certain
dose-dependent
effect;
however,
high
5) do not appear
to be strikingly
superior
to
TABLE
Relative
and
Subjects
low vitamin
quintiles.
The
2 demonstrates
values
(quintile
have
all cancer
result.
0.01).
<
that
were calculated
after the
the first 2 y. The effect of
A more important
question
is whether
is related
to a threshold
or a dose-dependent
answer
The
carotene
could
value
was adjusted
had a significantly
elevated
levels
cutoff
model
cholesterol.
a significantly
remained
as well
2.47,
cancer
retinol
Thus
the relative
of subjects
who
The
The
with low carotene
the combination
A was
cancer.
exclusion
from
values.
zmol/L.
plasma
3 show that subjects
higher
For
and triglycerides.
In contrast,
vitamins
A, C, and E are clearly
higher
study
population
compared
with the populations
menabove.
The low carotene
status
among
our population
explains
all cancer
the strong
death
with vitamin
Relative
observed.
inverse
The
relationship
relative
with
poor
lung
carotene
cancer
status
A
risk
95% Confidence
interval
P
68
37
l2y
7 y
1.76*
2.26
1.07-2.87
0.98-5.25
0.026
0.06
204
102
204
102
204
12y
7y
12 y
7 y
12 y
1.29
1.46
1.37
1.94
2.42
0.91-1.84
0.88-2.44
0.92-2.02
1.22-3.07
1.57-3.72
0.157
0.15
0.126
0.01
0.01
age, and lipids.
Downloaded from ajcn.nutrition.org by guest on June 9, 2014
dence
to cholesterol
268S
STAHELIN
m$k Ro
ET
AL
Our results leave no doubt
that low carotene
with an increased
risk for bronchus
cancer
5.
7
death.
Several
other
An overview
4.
Carotene
7
found
vitamin
similar
results
A correlate
in affluent
western
:
may
than
act independently
from
free radical
scavenging
:
:
plasma
results
value
suggest
,
4.
tant
has
that
low
values
adjusting
societies
oflow
carotene
that vitamin
A
carotene
through
other mechanisms
(eg, growth
factors,
etc). Hence,
as lower limit for carotene
that about one-third
ofthe
unfavorably
to note
(2 1-23).
et al (24).
weakly
(Table
l)(25).
The synergistic
effect
low vitamin
A in our population
suggests
Study
:
-
and
have
by Ziegler
only
and
3,
2
studies
is given
status is associated
and overall
cancer
has to be defined.
population
ofthe
(< 0.30
for
cholesterol
the
relationship
mol/L).
did
a
Our
Basel
It is impornot
change
the
&
0
__________________________________________
0
1
2
observed
3
4
from
5
QuIntlis Rang.
association.
lung
amount
associated
overall
cancer
may
between
strongly
and
carotene-containing
cancer.
encourage
a higher
supplements
intake
mortality
be independent
of lipoproteins
as carotene
carrier,
with a relative
risk below
1 (Fig
data
against
Thus
and
higher
2 and
of dietary
as a preventive
of the
values
were
Fig 3). Our
carotenoids
measure
13
References
of the Basel
Basel Study
cancer,
is more
Age and
carotene
common
lipoprotein
higher
lower
levels
intake
than
The
higher
nogenic
effect
of
/3-carotene
low
since
may
effect
in Switzerland
seem
in smokers
smoking
a lowering
may explain
the fact
death,
with its leading
levels
concentration.
likely
that
Study
population
population
cancer
their
suggest,
increase
values
the
carotene
levels
with
thus
the
concentrations
reflect
other
The
studies,
or have
enhance
the
increased
remains
most
are lower.
requirements
may
However,
(10).
in determining
in females
lipid
in agreement
(1 7, 18, 20) and
of smoking.
in general
less important
plasma
that in the
cause lung
relative
independent
carcirisk
of
smoking.
msk do
5.
4.
3,
1’
2
7
7
______________________________________________
1
.
7
-r
--
4.
S
-
s
#{163}
4.
4
5
0
0
1
2
Onth.
3
R
FIG 3. Comparison
of relative risk in different carotene
quintiles
for
all cancer (n = 204). Above average carotene
values have distinctly
lower
risks than below average carotene
concentrations.
1. Doll R, Peto R. The causes of cancer.
quantitative
estimates
of
avoidable
risks ofcancer
in the United States today. JNCI 198 l;66:
1 19 1-308.
2. Committee
on Diet, Nutrition
and Cancer. Diet, nutrition
and cancer. Progr Food Nutr Sci 1985;9:283-341.
3. Bertram IS, Kolonel LN, Meyskens
FL. Rationale
and strategies for
chemoprevention
of cancer in humans.
Cancer Res l987;47:30l231.
4. Gey KF. On the antioxidant
hypothesis
with regard to arteriosclerosis.
Bibl Nutr Dicta l986;37:53-9
1.
5. Shekelle RB, Lepper M, Liu S. et al. Dietary vitamin A and risk of
cancer in the Western
Electric Study. Lancet l98l;2:l
185-90.
6. Stahelin MB, R#{246}seI
F, Buess F, et al. Cancer, vitamins,
and plasma
lipids: Prospective
Basel Study. JNCI l984;73: 1463-8.
7. Menkes
MS. Comstock
OW, Vuilleumier
IP, et al. Serum betacarotene,
vitamins
A and F, selenium
and the risk of lung cancer.
N Engl I Med 1986;3l5:l250-4.
8. Nomura
AMI, Stemmermann
ON, Heilbrun
1K, et al. Serum vitamin levels and the risk ofcancer
ofspecific
sites in men of Japanese
ancestry
in Hawaii. Cancer Res l985;45:2369-72.
9. Ziegler RG, Mason Ti, Stemhagen
A, et al. Carotenoid
intake, vegetables, and the risk oflung cancer among white men in New Jersey.
Am I Epidemiol
1986;l23:1080-93.
10. St#{228}helinHB, Thurneysen
I, Buess E, et al. Mortality
and causes of
death in the 20-years
follow-up
of the Basel Study. Schweiz
Med
Wochenschr
1988;l 18:1039-47.
1 1. Widmer
LK, St#{228}helin
HB, Nissen C, et al. Bawl Study: venous and
arterial disease, ooronary heart disease in a working population.
Bern,
Switzerland:
Hans Huber,
1981.
12. St#{228}helinHB, Bruppacher
R. The influence
of the family on risk
factors in children
and adolescents.
The Basel Family Study. In:
St#{228}helin
MB, Spahr A, Schweizer
W, eds. Cardiovascular
risk factors
in children.
Bern: Huber 1985:88-159.
13. Kalbfleisch
ID, Prentice
RL. The statistical
analysis of failure time
data. New York: Wiley, 1980.
14. BMDP statistical software. Berkeley: University
ofCalifornia,
1983.
15. Wald NJ, Boreham
I, Hayward
IL, et al. Plasma retinol, beta-carotene and vitamin
F levels in relation
to the future risk of breast
cancer. Br I Cancer
1984;49:321-4.
Downloaded from ajcn.nutrition.org by guest on June 9, 2014
FIG 2. Comparison
of relative risk in different carotene
quintiles
for
bronchus
cancer (n = 68). Risks are expressed
in relation
to the third
quintile,
in which the risk has been set to 1.00. Above average carotene
values have distinctly
lower risks than below average carotene
concentrations.
Confidence
intervals
are wide because of the small number
in
each quintile.
cancer
CAROTENE
16. Peleg I, Heyden
5, Knowles
M, et al. Serum retinol and risk of
subsequent
cancer: extension
of the Evans County,
Georgia Study.
INCI l984;73:1455-8.
17. Comstock
OW, Menkes MS. Schober
SF. Serum levels of retinol,
beta-carotene,
and alpha-tocopherol
among older subjects.
Am I
Epidemiol l988;l27:l 14-23.
I 8. Lemoine
AC, Le Devehat
C, Herberth
B, et al. Vitamin
status in
three groups of French adults. Ann Nutr Metab l986;30(suppl
1):
1-94.
19. Wald N, Boreham
I, Bailey A. Serum retinol and subsequent
risk
20.
ofcancer.
BrI Cancer
1986:54:957-61.
Chow CK, Thacker
RR, Changehit
C, et al. Lower level of vitamin
C and carotenes
in plasma of cigarette
smokers.
Am I Clin Nutr
l986;5:305-l 2.
AND
CANCER
2695
21. Connett
IF, Kuller LH, Kjelsberg
MO, et al. Relationship
between
carotenoids
and cancer. The multiple
risk factor intervention
trial
(MRFIT)
study. Cancer
1989;64: 126-34.
22.
Paganini-Hill
beta-carotene,
l987;79:443-8.
A, Chao
and the
A, Ross RK, Henderson
BE. Vitamin
A,
risk of cancer:
a prospective
study. JNCI
23. Colditz
GA, Branch
LG, Lipnick
Ri, ci al. Increased
green and
yellow vegetable intake and lowered cancer deaths in an elderly population. Am I Clin Nutr l985;4l:32-6.
24. Ziegler RG. Vegetables,
fruits, and carotenoids
Am I Clin Nutr l99l;53(suppl):25lS-9S.
25.
Olsen IA. Serum levels of vitamin
of nutritional
status. JNCI l984;73:
and the risk of cancer.
A and carotenoids
1439-44.
as reflectors
Downloaded from ajcn.nutrition.org by guest on June 9, 2014





















© Copyright 2025