
NEWS ANAESTHESIA INSIDE THIS ISSUE:
ANAESTHESIA The Newsletter of the Association of Anaesthetists of Great Britain and Ireland NEWS ISSN 0959-2962 No. 328 NOVEMBER 2014 INSIDE THIS ISSUE: Social media networks as a learning platform – the anaesthesia trainees’ perspective What's new in regional anaesthesia? Still bleeding after all these years X-Porte – The World’s First Ultrasound Kiosk Editorial Contents Social22 1 22/09/2014 15:43 03Editorial 04 What's new in regional anaesthesia? 04 08 Social media networks as a learning platform – the anaesthesia trainees’ perspective One look and the difference is clear: C X-Porte delivers a type of image clarity never before seen in point-of-care ultrasound systems. 07 Museum, Library and Archives Committee Report M Y CM X-Porte’s Extreme Definition Imaging (XDI) was specifically created to meet the challenge of unwanted phantom echoes from side-lobe beams. Using XDI proprietary beamforming technology, visual clutter is substantially reduced while significantly enhancing clarity. • Onboard Education: Watch 3D learning animations concurrently with live scans for real-time comparisons and guidance. • Fully customisable: Multi-gesture touch-screen interface. Sealed to facilitate cleaning and infection control. • Industry-leading five-year warranty. Learn more about X-Porte today by downloading our X-Porte iPad app. Or, better still, request a demonstration to experience X-Porte yourself. Email us at ukresponse@sonosite.com www.sonosite.co.uk/products/x-porte MY CY CMY K The production schedule for Anaesthesia News requires us to write these introductions six weeks or so before publication. So I am writing this from Annual Congress in Harrogate. And what a Congress it is proving to be! Over 800 delegates, a fantastic ‘buzz’, lots of great talks, workshops, poster and abstract presentations and our keynote lectures. In addition, over 30 (hard core) cyclists have raised money for charity by riding here from Bristol and London and receiving pledges of over £13,000 for two charities (Lifebox and CTC). If, like me, you are humbled by their fantastic efforts please consider giving – it’s not too late: http://www.aagbi.org/about-us/aagbi-fundraising/ cycle-for-guy/chosen-charities For many members, the AAGBI meetings are the jewels in the crown of our activities. Even before Annual Congress started the scientific programme for WSM London in January was published. A particular delight at recent meetings has been the increase in the number of abstract submissions; many are from trainees and some are from medical students. As an aside can I remind members that the AAGBI offers medical students funding for undergraduate electives that exposes them to anaesthesia or intensive care. The next round is now open and the closing date for applications is 5 January 2015, so please let any students passing through your department know. We are particularly keen to support those who wish to travel to the developing world. Visit http://www.aagbi.org/undergraduate-awards for further details. This month’s Anaesthesia News contains two articles on social media and one on the value of sending trainees to the developing world. We publish many articles on the developing world and this one is particularly interesting as it reports just how beneficial such programmes can be to both parties. Finally, Nigel Bedforth and colleagues have written about the future for regional anaesthesia. Of course, it is not just enthusiasts who undertake blocks. However, those developing new ideas, techniques, equipment and drugs continue to advance this area. We thought such an update and future gazing would help to set the scene for the rest of us. FUJIFILM SonoSite, Inc. the SonoSite logo and other trademarks not owned by third parties are registered and unregistered trademarks of FUJIFILM SonoSite, Inc. in various jurisdictions. All other trademarks are the property of their respective owners. ©2014 FUJIFILM SonoSite, Inc. All rights reserved. Our Association continues to grow with an ever-increasing range of activities and services for its members. See you in London in January? 08 10 News from the European Society of Anaesthesiology 11 Cadaveric training courses: a realistic environment to learn anaesthetic technical skills? 13 Ultrasound technology 11 15 Still bleeding after all these years… 17 Anaesthetic training in underdeveloped countries: what is the role of junior trainees? 15 19 Social media in anaesthesia - uniting the trainees 24 Your Letters 27 Anaesthesia Digested 28 Particles 17 The Association of Anaesthetists of Great Britain and Ireland 21 Portland Place, London W1B 1PY Telephone: 020 7631 1650 Fax: 020 7631 4352 Email: anaenews@aagbi.org Website: www.aagbi.org Anaesthesia News Chair Editorial Board: Nancy Redfern Editors: Phil Bewley and Sally El-Ghazali (GAT), Nancy Redfern, Richard Griffiths, Sean Tighe, Tom Woodcock, Mike Nathanson, Rachel Collis, Upma Misra and Felicity Plaat Address for all correspondence, advertising or submissions: Email: anaenews@aagbi.org Website: www.aagbi.org/publications/anaesthesia-news Editorial Assistant: Rona Gloag Email: anaenews@aagbi.org Design: Chris Steer AAGBI Website & Publications Officer Telephone: 020 7631 8803 Email: chris@aagbi.org Printing: Portland Print Copyright 2014 The Association of Anaesthetists of Great Britain and Ireland Mike Nathanson AAGBI Council Member Anaesthesia News November 2014 • Issue 328 The Association cannot be responsible for the statements or views of the contributors. No part of this newsletter may be reproduced without prior permission. Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements. 3 What’s in regional anaesthesia? In this article we discuss some recent developments in regional anaesthesia including innovation in imaging technology, needle position detection and drug development. New approaches Strain and shear wave elastography Ultrasound imaging has allowed regional anaesthetists to rely less on traditional anatomical landmarks and develop new innovative approaches to nerves. These include ‘body wall’ blocks such as the transversus abdominis plane,1,2 sub-sartorial canal3 and thoracic wall blocks.4 The development of some of these is ongoing and their efficacy and place in clinical practice yet to be fully determined. Ultrasound also allows targeting of small nerves and delivery of highly accurate, low volume blocks, for example blocks around the ankle5 or shoulder.6 Ultrasound is now being used to develop motor sparing sensory blockade around the knee; this may prove to be a useful approach following knee surgery.7 The elasticity of a material describes its ability to return to its original shape after being stretched. In the body, stiffer tissues will deform less than softer tissues following application of a force. Ultrasound can be used to image or measure tissue elasticity following application of a force by, for example, pressure from the transducer or following injection of a fluid. Local anaesthetic tissue displacement is represented by colour changes on screen. Shear waves created by ultrasound can be used to detect tissues with differing hardness, and may provide extra information when differentiating nerves from other tissues.14 Elastography in regional anaesthesia has not yet been shown to have definite advantages over standard imaging in patients, so we await further studies. 3D ultrasound scanning Three-dimensional ultrasound imaging provides the user with a view of a whole volume of interest rather than the standard narrow slice. The image can be displayed as a whole volume rendered image (rather like a hologram) or in a multiplanar view, where a series of slices are displayed simultaneously (usually orthogonal - three planes at right angles to each other). Ultrasound machines can now provide 3D imaging in real time; also termed four-dimensional imaging. Despite these developments, 4D imaging has not yet been incorporated into common practice, with clinical experience limited to a number of reports including the popliteal fossa,8 interscalene catheter placement9 and radial nerve blockade.10 This is because the machines are expensive, the probes unwieldy and the resulting images are somewhat complex and difficult to interpret. The potential advantages of 4D ultrasound imaging are improved visibility of structures to reduce needle overshoot11 and improved visualisation of local anaesthetic spread, catheter position and the needle tip to nerve relationship. Time will tell if these potential advantages translate into clinical practice. Fusion scanning This produces improved accuracy for ultrasound-guided biopsy procedures and has the potential to facilitate certain regional anaesthetic techniques. These would include deep techniques or those where bony structures may impede ultrasound penetration such as lumbar plexus and paravertebral blockade or interventional pain procedures such as spinal injections and coeliac plexus blocks. The two images have to be accurately aligned to avoid a target registration error. This can either be done using external markers (frames), fixed points on the bony skeleton or using organ surfaces as markers or vascular structures to align image volumes. The pre-procedural MRI or CT scan and the ultrasound scan should be performed in the same position and as close together in time as practical to minimise alignment errors.15 Radiologists are increasingly using this technology to target biopsies in major organs (for example breast, prostate and liver) and for musculoskeletal injections such as the sacroiliac joint. There is limited experience of this new technique in anaesthesia but the potential to use the ever-increasing number of MRI and CT studies, that many patients have, to aid in regional anaesthesia and pain procedures is an exciting prospect. Very high frequency scanning Ultrasound transducers have now been developed which produce ultrasound at frequencies up to 50 MHz. Frequencies this high produce short wavelengths and images with a resolution capable of discerning features as small as 40 µm (compared with standard ultrasound which will discern features of approximately 200 µm). This technology gives us the opportunity to obtain much higher detail in our images, for example allowing us to visualise nerve architecture in fine detail and produce better understanding and control of the needle tip to nerve interaction (Figure 2). The challenge will be to produce pictures with enough tissue penetration to be clinically useful. Magnetic resonance imaging and x-ray computed tomography (MRI and CT) have excellent spatial resolution and soft tissue recognition but are impractical for real-time needling due to the radiation, magnetic field, equipment size and need for immobility of the subject. Ultrasound is suitable for real time imaging, but is limited by the depth of structures to image, the presence of bone and need for needle angulation away from the probe. Fusion imaging uses pre-procedural MRI or CT and fuses this into the same screen as the live ultrasound images (Figure 1). Encapsulating agents One of the ultimate advances in regional anaesthesia would be the development of a local anaesthetic agent with an ultra-long action. This could be applied to target nerves in very low concentrations, to achieve prolonged analgesia without motor blockade. This would see an end to the requirement for either a large single-shot dose of local anaesthetic or for postoperative perineural local anaesthetic infusion. Encapsulating agents are biodegradable and can carry local anaesthetics and slowly release them to produce a prolonged period of action. Two such agents are liposomes and microspheres constructed from hydrophobic substances such as polylactic and polyglycolic acids. Liposomes seem to have the lowest toxicity and a liposomal bound local anaesthetic preparation has gained FDA approval, so we should now expect to see development of the evidence base.16 Microsphere-coated mesh Recently, mesh coated with polylactide co-glycolic acid microspheres containing bupivacaine out-performed single-shot bupivacaine given at the time of surgical insult in a rat model. This may prove to be a useful way of delivering the slow release local anaesthetic to the tissues.17 Needle technology Recent needle developments include needle guidance systems. One example is the Ultrasonix GPSTM guidance system (Ultrasonix Medical Corporation, High Wycombe, UK). Sensors mounted in the needle tip communicate positional information to sensors mounted in the transducer. The needle position is superimposed on the ultrasound image to provide the operator with improved information regarding orientation of the needle to the transducer. Another such system is the eGuide Freehand Navigation system (eZono AG, Jena, Germany) that uses magnetism to detect the position of the needle in relation to the transducer and plot the needle trajectory on-screen (Figure 3). There is currently little proof of benefit of these systems in regional anaesthesia,18 but they may have particular use in facilitating training. Robotics Robotic technology is being used successfully in some surgical specialties. A robotic system has recently been applied to regional anaesthesia. Workers have successfully placed needles in phantoms and, more recently, 13 patients underwent popliteal sciatic nerve blocks.12,13 We await further investigation to show the advantages, if any, over the standard technique. The astronomical price involved means that the benefits of any robotic technique would have to be substantial! 4 Figure 1 A fusion image of ultrasound and MRI scan at the level of iliac crest; the ultrasound image is impaired due to overlying bony cover and depth, but by using the MRI image, which provides excellent resolution of psoas muscle and lumbosacral plexus, it should be possible, with needle guidance, to place the needle in the appropriate site for a lumbar plexus block (figure courtesy of T Bentsen MD, Aarhus, Denmark) Anaesthesia News November 2014 • Issue 328 Figure 2 Figure 3 A high frequency scan of the median nerve at the wrist; note the increased resolution of the nerve architecture; also note the limited depth of the picture (picture taken following ethical approval with MS550D transducer with 55 MHz peak and 40 MHz centre frequency, Vevo 2100 preclinical ultrasound system, courtesy of Fujifilm VisualSonics, Sonosite Ltd, London, UK) A needle guidance system during an out-of-plane needle approach to a target; the green target box turns green as the needle tip enters the plane of the ultrasound beam and becomes visible as a hyperechoic dot (figure courtesy of eZono AG, Jena, Germany) Anaesthesia News November 2014 • Issue 328 5 26th Anaesthesia, Critical Care and Pain Update Val d’Isere, 2-5 February 2015 Centre de Congrés Multidisciplinary meeting Lectures | Workshops Joint and Satellite sessions Short paper competition Guest speakers The introduction of ultrasound to regional anaesthesia has seen an unprecedented surge in enthusiasm and delivery of these techniques. Innovation still abounds, and these authors wait with some excitement to see how the next generation of drugs, ultrasound equipment and needles will improve regional anaesthesia delivery to the further benefit of our patients. N. Bedforth and K. Mohammed Rafi Queen’s Medical Centre, Nottingham, UK B. Nicholls Musgrove Park Hospital, Taunton, UK References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 6 Tran TMN, Ivanusic JJ, Hebbard P, Barrington MJ. Determination of spread of injectate after ultrasound-guided transversus abdominis plane block: a cadaveric study. British Journal of Anaesthesia 2009; 102: 123–7. Heil JW, Ilfeld BM, Loland VJ, Sandhu NS, Mariano ER. Ultrasound-guided transversus abdominis plane catheters and ambulatory perineural infusions for outpatient inguinal hernia repair. Regional Anesthesia and Pain Medicine 2010; 35: 556–8. Jenstrup MT, Jaeger P, Lund J, et al. Effects of Adductor-Canal-Blockade on pain and ambulation after total knee arthroplasty: a randomized study. Acta Anaesthesiologica Scandinavica 2012; 56: 357–64. Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013; 68: 1107–13. Redborg KE, Sites BD, Chinn CD, et al. Ultrasound improves the success rate of a sural nerve block at the ankle. Regional Anesthesia and Pain Medicine 2009; 34: 24–8. Maybin J, Townsley P, Bedforth N, Allan A. Ultrasound guided supraclavicular nerve blockade: first technical description and the relevance for shoulder surgery under regional anaesthesia. Anaesthesia 2011; 66: 1053–5. Egeler C, Jayakumar A, Ford S. Motor-sparing knee block - description of a new technique. Anaesthesia 2013; 68: 542–3. Feinglass NG, Clendenen SR, Torp KD, Wang RD, Castello R, Greengrass RA. Real-time three-dimensional ultrasound for continuous popliteal blockade: a case report and image description. Anesthesia and Analgesia 2007; 105: 272–4. Clendenen SR, Riutort KT, Feinglass NG, Greengrass RA, Brull SJ. Real-time three-dimensional ultrasound for continuous interscalene brachial plexus blockade. Journal of Anesthesia 2009; 23: 466–8. Foxall GL, Hardman JG, Bedforth NM. Three-dimensional, multiplanar, ultrasound-guided, radial nerve block. Regional Anesthesia and Pain Medicine 2007; 32: 516–21. French JLH, Raine-Fenning NJ, Hardman JG, Bedforth NM. Pitfalls of ultrasound guided vascular access: the use of three/four-dimensional ultrasound. Anaesthesia 2008; 63: 806–13. Morse J, Terrasini N, Wehbe M, et al. Comparison of success rates, learning curves, and inter-subject performance variability of robot-assisted and manual ultrasound-guided nerve block needle guidance in simulation. British Journal of Anaesthesia 2014; 112: 1092-7. Hemmerling TM, Taddei R, Wehbe M, Cyr S, Zaouter C, Morse J. Technical communication: First robotic ultrasound-guided nerve blocks in humans using the Magellan system. Anesthesia and Analgesia 2013; 116: 491–4. Munirama S, McLeod G. Novel applications in ultrasound technology for regional anesthesia. Current Anesthesiology Reports 2013; 3: 230–5. Rasoulian A, Abolmaesumi P, Mousavi P. Feature-based multibody rigid registration of CT and ultrasound images of lumbar spine. Medical Physics 2012; 39: 3154–66. Weiniger CF, Golovanevski L, Domb AJ, Ickowicz D. Extended release formulations for local anaesthetic agents. Anaesthesia 2012; 67: 906–16. Ohri R, Wang JC-F, Pham L, et al. Prolonged amelioration of experimental postoperative pain by bupivacaine released from microsphere-coated hernia mesh. Regional Anesthesia and Pain Medicine 2014; 39: 97–107. Brinkmann S, Vaghadia H, Sawka A, Tang R. Methodological considerations of ultrasound-guided spinal anesthesia using the Ultrasonix GPS™ needle tracking system. Canadian Journal of Anaesthesia 2013; 60: 407–8. www.doctorsupdates.com education in a perfect location doctorsupdates TM Conclusions Advanced Airways Techniques May 2015 This course has been running for many years and continues to develop. It is aimed at anaesthetists who wish to develop advanced airways management knowledge, skills and strategy planning to deal with a variety of clinical scenarios. Key features that make this course of high education value includes tutor:delegate ratio of mostly 1:1; experienced consultants as tutors; use of cadavers, animal and manikin models; and a mixture of hands-on practice and discussion on case management. No previous experience of advanced airways techniques is required. Course Fee: £325 Full details and online registration available at http://www.cuschieri.dundee.ac.uk/ Cuschieri Skills Centre – University of Dundee Ninewells Hospital and Medical School, Dundee, Tayside, DD1 9SY Scotland Tel: +44(0)1382 383400 Fax: +44(0)1382 646042 Anaesthesia News November 2014 • Issue 328 Museum, Library and Archives Committee Report The growth in visitors to the Heritage Centre continues. Visits by individuals are up by 18% on the previous year and visits by groups are up by 260%. The groups comprised three school/students groups, eight adult groups, one adult group from overseas and one adult specialist group from industry (Intersurgical). Three new volunteers were also welcomed into our existing volunteer group: Mrs Hilary Riches (granddaughter of Charles King, founder of the Heritage Centre), Hannah Brayford (medical student with an interest in a career in anaesthesia) and Richard Birks (past president). This year we have managed to secure ‘The Joseph Clover manuscript’ which has attracted international attention from Australia. Clover was an early pioneer of anaesthesia; he designed equipment to deliver anaesthetics, improved techniques and pioneered monitoring during anaesthesia. Earlier this year, a couple of members of the Heritage Committee visited and inspected the graves of John Snow and Joseph Clover in Brompton Cemetery and can report that, apart from minor works, the memorials are in good order. We have also received some very nice donations of books and equipment from Frenchay Hospital, Great Ormond Street Hospital and from the executors of Edith Gilchrist. The AAGBI is very grateful for these objects and will take great care in preserving them for future generations. A very big challenge that we face over the next four years is the launch and continuation of the World War 1 exhibition. The conflict, which devastated Europe for over 4 years, was arguably a pivotal event in the development of the specialty of clinical anaesthesia. Securing funding for the World War 1 project and making it accessible to non-AAGBI members will mark out the next four years. We will increase our outreach to a nonspecialist audience via an education pack, specific events and themes to the exhibitions, such as The Somme, Boyle against Marshall and the treatment of shock. We want to raise awareness of the advances made in anaesthesia as a result of World War 1 and to show that later conflicts have had the same effect. Over the next year we have various challenges and priorities. There are IT challenges, as it is important for us that we manage to transfer as Anaesthesia News November 2014 • Issue 328 Anaesthesia News November 2014 • Issue 328 much of the audio and video archive to a digital format. Completing an inventory of our objects that are kept in a remote out-store and working to make them available to people through social media, temporary exhibitions and our website will form an important part of our work. We will continue to prepare our database, AdLib, for the release of a new software package. This will involve data cleaning, keeping in touch with the software developers and being aware of how it is developing. We’ll also be increasing our use of social media. The series of World War 1 exhibitions will be promoted and developed and we’ll be working with an education consultant to explore ways of working with schools, colleges and universities. We will work to support the development of the Anaesthesia Heritage Centre and will consider the provision of more tablets to make the history of anaesthesia more accessible and to make more information available electronically. We hope that the work of maintaining the heritage of anaesthesia remains relevant to the core activities of the AAGBI. We aim to support members and educate the public about the rich history of our specialty, promoting the knowledge and training of anaesthetists and we will continue to make the most of our collections within a limited space. www.aagbi.org/education/heritage-centre Dr Richard Griffiths Chair of the Museum, Library and Archives Committee Trish Willis Heritage and Records Manager 77 Social media networks as a learning platform – the anaesthesia trainees’ perspective Social22 Facebook is just a decade old yet social media networks (SMN) have rapidly established themselves as household names. Medical institutions have also become involved. The General Medical Council (GMC), the Royal College of Anaesthetists (RCoA) and the AAGBI boast Facebook and Twitter accounts. Anaesthetists have always prided themselves on being leaders in medical education. The AAGBI1 and the RCoA2 have introduced e-learning platforms which are very popular. Other enthusiasts have taken this further using SMN to provide an accessible and interactive learning environment.3 It has been assumed that SMN must be the way forward for medical education, but this is without consulting potential users. We explored the views of anaesthesia trainees on using social media as a learning platform, how much they use SMN currently and what obstacles or concerns they have which may prevent their engagement. 22/09/2014 15:43 C M Y CM MY CY CMY K A questionnaire with two distinct aims was sent to all anaesthetic registrars in the Northern School of Anaesthesia. First, we wished to establish how prevalent social media use was among the registrars and how they accessed their social media. Second, we wanted to explore their thoughts regarding the use of social media as a learning platform, what role it could play and to establish any concerns and reservations. A total of 25 responses were received (response rate 37%). This number of respondents was considered adequate for the purposes of a focus group. The overwhelming majority (92%) stated that they regularly used social media and nearly all (96%) used a Facebook account. The second most common network of choice was Twitter (16%). Forty-six percent were signed up to a single social network, 33% were signed up to two, and 17% were signed up to more than two. Most (65%) primarily accessed their social media using their mobile devices (mobile phone 52%, tablet 13%), the remainder opting for conventional computer systems. Almost all (92%) currently used online learning resources with the majority (80%) regarding them as useful to varying degrees. 8 1 formal guidance regarding the use of social media by doctors and what may constitute inappropriate usage.7 Information governance, patient confidentiality and data protection are at the forefront of many NHS Trusts’ corporate reasoning driving strict internet access policies. It may well be that the perceived rewards from a social media learning resource could be overshadowed by the grim warnings Trusts have made regarding potential breaches. It can be seen how some registrars would just feel that it is more trouble than it is worth! benefit, although most users commented on the ease of access to educational material through social media, its portability and the speed of publishing. A similar proportion voiced concerns regarding privacy (50%), with 17% opting to post using pseudonyms. A third voiced concerns regarding mixing their work and private lives, and commented on tactics they used to separate the two (e.g. excluding senior clinicians from their networks, avoiding discussing real cases, adjusting privacy settings, not divulging work locations and anonymising posts). In keeping with modern trends, most of our respondents accessed their social media with mobile devices rather then traditional computers. This enables users to circumnavigate tight Trust internet policies, and the rapidly advancing technology and increasing ease with which social media can be accessed would suggest significant potential for use as a learning platform. However, the enthusiasm for such a resource was lukewarm. Pushing the boundaries of medical education into the realms of social media has introduced more than just the expected technological and ethical challenges. It has also resulted in a blurring of the intersection between personal and work lives, creating a dilemma for many. It seems that active users engage with a variety of different networks on a regular basis, and most are cautious with what they post. Many use a network where no login credentials are required (YouTube), hence avoiding divulging any private information and users have employed a number of strategies to deal with commonly arising concerns. Mixing work with social activity Of the small majority (52%) that wanted a social media resource, equal proportions considered potential roles for group discussions, notifications, one-to-one advice, and for exam studying. Interestingly almost half (48%) said that they would not use social media in this context. Most commented that they felt it was risky and did not feel they wanted to mix work with social media. Furthermore, when asked if they would like a social media learning resource, the same proportion (48%) responded that they would not. The most common concern (52%) was about privacy issues, with the rest concerned about lack of accessibility or usefulness. Several surveys and studies have been conducted to estimate SMN use among medical professionals, some suggesting that up to 90% of doctors may use social media platforms for personal use, and 65% for professional purposes alone.4 Our results confirm this ubiquity. Other studies have examined the content of individual profiles and accounts, with some disquieting findings.5,6 These studies raise numerous concerns regarding inappropriate content, unprofessional conduct, ethical breaches, violations of patient privacy and conflicts of interest. It is therefore not surprising that the GMC recently issued Anaesthesia News November 2014 • Issue 328 Our results suggest that privacy seemed to be the biggest concern for anaesthetic registrars, and the idea that both work colleagues and personal friends could see and participate in the same virtual space can be quite unappealing. What one might want to share with family and friends may not be something you wish work colleagues to know. Some things may even be inappropriate.5 While most social media networks have filtering options allowing content to be visible and accessible only by certain groups of people, these are often not well known or understood by users. When faced with this dilemma, it can be seen why most would opt for avoidance. In an era of increasing shift work and more non-clinical work, it can also be extremely difficult to maintain an adequate and healthy work-life balance. In this environment, the desire to avoid mixing work with social activity may be another factor. Available evidence also shows that with advancing medical experience, many clinicians attempt to keep clear boundaries between work and personal lives.6 The above results do pose a question. There are several SMN e-Learning resources in existence. They are popular – GasClass has over 1000 registered followers – and are presumably used by a similar cohort to the one we surveyed. How do those who are engaged in the process deal with the concerns raised above? Another survey was undertaken to look at this. The administrators of GasClass kindly allowed us to survey their members at the end of their winter term. We found that, after Twitter, the most commonly used network for educational purposes was YouTube (58%) and 21% did not use any other network. Active users almost exclusively used mobile devices or a tablet (92%) for accessing social media. Usage was similar with most users (50%) engaged with social media for 1–2 hours a day. Peer group discussion was reported as the main Anaesthesia News November 2014 • Issue 328 As is often the case, more work needs to be done in this area. Both surveys raise some interesting questions, especially about privacy. The further work we have done shows that using the right network, with the right controls may increase participation greatly. Ultimately any e-learning resource should take into account the needs, opinions and concerns of the intended audience. This would enable medical education to be delivered in a way that maximises support and encourages active engagement. Majid Saleem ST6 – Anaesthesia Naveed Kara ST8 – Otolaryngology James Cook University Hospital, Middlesbrough, UK References 1. 2. 3. 4. 5. 6. 7. Learn@AAGBI. http://www.learnataagbi.org E-Learning Anaesthesia (e-LA). http://www.e-LA.org.uk Doran M, Williamson S, Whitehead I. Welcome to Gasclass – An online discussion for anaesthetists. Anaesthesia News 2013; 306: 12. Modahl M, Tompsett L, Moorhead T. Doctors, patients & social media. QuantiaMD, 2011. http://www.quantiamd.com/q-qcp/ doctorspatientsocialmedia.pdf Bosslet GT, Torke AM, Hickman SE, et al. The patient-doctor relationship and online social networks: results of a national survey. Journal of General Internal Medicine 2011; 26: 1168-74. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. Journal of General Internal Medicine 2008; 23: 954–7. http://www.gmc-uk.org/publications/21833.asp 9 Cadaveric News from the European Society of Anaesthesiology The notable news from the ESA is that the annual congress in 2016 will be held in London (28 May–31 May). The meeting is the ‘jewel in the crown’ of ESA activities. This year there were more than 5000 delegates and around 10% were from the UK and Ireland. As the national society of the host country, the AAGBI will form part of the National Organising Committee. The majority of the scientific programme is developed by the ESA’s Scientific Committee; however the host country society has the opportunity to recommend local speakers for one or two sessions. In addition the AAGBI will help with organising social events and the opening ceremony. Members of the AAGBI based in the UK and Ireland have a good track record of supporting ESA activities including the annual congress, the European exam (EDAIC), research networks and guideline production. Many of these roles require an application to join the relevant committee, all of which are reviewed by the Nominations Committee (the only ESA committee directly elected by ESA members at the Annual Meeting). The by-laws for the ESA for election to the ESA Council allow support by the relevant national society, and for the UK and Ireland this is the AAGBI. However, for many other posts a similar letter of support from the national society can be useful to demonstrate credibility, relevant experience and links to a wide audience. While certainly not essential, candidates for posts are advised to consider obtaining such support. Often your colleagues from other countries will be doing the same. The AAGBI is happy to offer support to members in good standing and by including a brief CV with your request the AAGBI’s letter to the ESA can be drafted to draw attention to relevant facts. Please consider applying for these posts when they are advertised on the ESA website or in the e-newsletter, and if you seek AAGBI support please contact the Honorary Secretary of the Association (honsecretary@aagbi.org). For general advice or any other information about the ESA please contact me at mike.nathanson@nuh.nhs.uk Mike Nathanson Council Member, AAGBI and Council Member, ESA 10 GAT ASM ABSTRACT SUBMISSION MANCHESTER 2015 GAT Oral and Poster Prizes Trainee anaesthetists are invited to submit an abstract for oral or poster presentation at the GAT ASM. The authors of the six highest-scoring abstracts in the preliminary review will be invited to present their work orally and will be eligible for the Oral Presentation Prize. A cash prize will be awarded to the winner. training courses onment a realistic envir to learn anaesthetic ? technical skills h us, it w s ay w al is le op pe on ticing ‘The moral burden of prac lications Atul Gawande, Comp ’ n. e ok sp un rt pa t but for the mos Case Presentation Prize Trainees are asked to submit an abstract of an interesting case that they have been involved in, and which has learning points that may aid other anaesthetists in their management of similar cases. The three best submissions as judged in the preliminary review will be invited to present their work orally at the ASM and the audience asked to vote for their favourite. A cash prize will be awarded to the winner. Poster Competition The remaining successful authors will be invited to present a poster. Entries will be allocated into one of the following three categories depending on the grade of the presenting author: Foundation Year Trainees; ACCS/Core Trainees; ST3+ Doctors. A cash prize and a certificate will be awarded to the winner in each category. The judges also reserve the right to award discretionary certificates. Medical Students Poster Prize Medical students are invited to submit an abstract for poster presentation on a theme related to Anaesthesia/Pain/ITU. A cash prize will be awarded to the winner. Prize The Anaesthesia History Prize The Association of Anaesthetists and the History of Anaesthesia Society will award a cash prize for an original essay on a topic related to the history of anaesthesia, intensive care or pain management written by a trainee member of the Association. A £500 cash prize and an engraved medal will be awarded for the best entry, and the winner will be invited to present their paper at the ASM. CLOSING DATE FOR SUBMISSIONS: MONDAY 19 JANUARY 2015 For full details and to apply please go to the GAT ASM website www.gatasm.org/content/oral-poster-prizes If you have any additional queries, please contact the AAGBI Secretariat on 020 7631 1650 (option 3) or email gat@aagbi.org Anaesthesia News November 2014 • Issue 328 We can all remember the nerve-wracking experience of performing a procedure such as venous cannulation or central neuraxial blockade for the first time on a patient. Trying to appear confident and competent when you don’t know what it will actually feel like to perform, even though you have read about it and observed it. Add to this is a sense of responsibility to the patients, all of whom deserve the best possible care, and a feeling of anxiousness that as a novice performing the procedure you may not be providing this. In addition to the ethical dilemma of ‘practicing’ on patients, trainees are required to learn a greater number of techniques in fewer hours, for increasingly complex patients. Acquiring the technical skills required to become an anaesthetist can prove challenging. The ‘see one, do one, teach one’ philosophy is no longer acceptable. A recent review1 of the ethical and legal difficulties associated with medical training involving patients noted that the learner has a responsibility to fulfil the preparatory requirements for the skill being learned, to gain the necessary knowledge in the classroom and the manual dexterity in skills labs and simulations, before gaining experience with patients. Anaesthesia News November 2014 • Issue 328 The medical education community has responded to this by developing increasingly sophisticated part task simulators to take the place of the patient. This allows healthcare professionals to begin to learn technical skills such as cannulation and central neuraxial blockade. On trauma and resuscitation courses, animal models are also used as surrogates on which to practice procedures such as chest drains and surgical cricothyroidotomy. These simulated patients allow the novice to experience a technique for the first time without practising on a patient. Even more ‘real’ is the use of cadavers to teach practical procedures. Changes to the Human Tissue Act in 2004 (England/Wales/ Northern Ireland) and the Anatomy Act (Scotland) in 2006 made it possible to perform surgical procedures on cadavers. The surgical specialties were the first to explore the opportunities this change in the law afforded for medical training; however anaesthesia has now also started to utilise cadavers as a teaching resource. Over recent months I have attended two training courses which have used a combination of part task simulation and cadavers to teach anaesthetic practical procedures. 11 Advertorial The first, a thoracic epidural course at the Newcastle Surgical Training Centre (http://nstcsurg.org/), catered for a mixture of participants, with all grades of trainee and consultants present. Part task simulators and fresh frozen cadavers were used to give novices the opportunity to undertake the whole procedure several times in a low pressure, low risk environment. More senior trainees and consultants had the chance to practice less commonly used techniques on a cadaver rather than a patient, such as the paramedian approach and tunnelling of catheters, increasing confidence to use these skills in clinical practice. The second was an advanced airway course, for senior trainees and consultants, at the Cuschieri Skills Centre, Dundee (http://www. cuschieri.dundee.ac.uk/). NAP4 made strong recommendations regarding improvements in airway training including the teaching of advanced and emergency airway techniques.2 This course teaches these airway skills using a mixture of part task simulators, animal models and cadavers to simulate patients. The cadavers used during this course were Thiel embalmed, a type of soft-fix tissue preservation, which retains more lifelike tissue colour and flexibility compared to other methods of preservation. Certainly during fibreoptic intubation, while concentrating on the screen, the lifelike colour and feel of the tissues meant the experience of performing the procedure seemed ‘real’. We also practiced front of neck access on the cadavers using needle cricothyroidotomy followed by jet ventilation using the rise and fall of the chest to confirm success. As the Thiel cadavers are an expensive resource and the more invasive surgical cricothryroidotomy would have required each participant to have sole access to a cadaver, animal models (porcine larynx) were used to practice this technique instead. This course provided a valuable opportunity to practice emergency airway procedures, which it is vital all anaesthetists are competent to perform, but which we rarely use on patients. The high ratio of equipment and trainers to candidates meant there was lots of time to practice and consolidate all the technical skills taught. Thiel embalming Thiel embalming was first described in the 1990s by Professor Thiel of the University of Graz, Austria, and was introduced to the UK in 2009 by the Centre for Anatomy and Human Identification, University of Dundee (http://cahid.dundee.ac.uk). This preservation method involves an initial perfusion of the cadaver followed by three months submersion in an embalming fluid based on water, glycol and various salts. This method costs more than formalin based preservation techniques but this is balanced by the large number of procedures that can be performed on each cadaver, as they can be stored at room temperature and re-used over a period of years.3 The lifelike retention of tissue flexibility and quality is thought to be due to disruption of the muscle fibres by the boric acid component of Thiel embalming, while the muscles themselves remain intact within their fibrous sheaths. The superiority of Thiel embalming over other methods has been confirmed for several surgical procedures.4 most training courses in USGRA use live models for scanning with needling practiced on phantoms, the steepest learning curve for most involves the skill in putting these two aspects together. Cadavers can offer a realistic model on which to combine scanning and needling. Research would suggest that Thiel embalming offers some benefits over fresh cadavers in the positioning of limbs, ease of visualisation of both anatomy and needle and in the lifelike ‘pop’ sensation when fascial layers are punctured.6,7 Clearly the competence to perform a practical technique also requires an understanding of when the technique is required and how to manage the team involved as well as any complications which may occur. Both the courses I attended had adequate time allotted for scenario discussions around the equally important human factor aspects of both central neuraxial procedures and difficult airway training. Sarah Gibb ST7 Northern School of Anaesthesia Declaration of interest The GAT Committee were given a complimentary registration to the Dundee Advanced Airways Course. Permission to print the photographs illustrating this article was given by Roos Eisma, Operational Manager and Scientific Officer, CAHID. References 1. Iqbal R, Rhys Hooper C. Ethico-legal considerations of teaching. Continuing Education in Anaesthesia, Critical Care and Pain 2013; 13: 203–7. 2. Major complications of airway management in the United Kingdom. The 4th National Audit Project of the Royal College of Anaesthetists and Difficult Airway Society. Report and findings, March 2011. http://www.rcoa.ac.uk/nap4 (accessed 04/09/2014) 3. Eisma R., Mahendran S, Majumdar S, Smith D, Soames RW. A comparison of Thiel and formalin embalmed cadavers for thyroid surgery training. The Surgeon, 2011; 9: 142–6. 4. Benkhadra M, Bouchot A, Gérard J, et al. Flexibility of Thiel’s embalmed cadavers: The explanation is probably in the muscles. Surgical and Radiological Anatomy 2011; 33: 365–8. 5. Raju PKBC. et al. Thiel cadavers: A further step in teaching airway skills. Poster Presentation. Difficult Airway Society 2013. 6. Benkhadra M, Faust A, Ladoire S, et al. Comparison of fresh and Thiel’s embalmed cadavers according to suitability for ultrasound-guided regional anaesthesia of the cervical region. Surgical and Radiological Anatomy 2009; 31: 531–5. 7. Macleod G, Eisma R, Schwab A, Corner G, Soames R, Cochran S. An evaluation of Thiel-embalmed cadavers for ultrasound-based regional anaesthesia training and research. Ultrasound 2010; 18: 125–9. The Dundee group’s pilot study to evaluate the use of Thiel embalmed cadavers during airway training demonstrated that the cadavers were rated superior to manikins for direct laryngoscopy, insertion of supraglottic airway device, videolaryngoscopy, fibreoptic intubation and cricothyroid puncture. Thiel embalmed cadavers also do not have the strong smell associated with formalin preservation making it more acceptable to participants.5 12 ULTRASOUND TECHNOLOGY; A REVELATION FOR REGIONAL ANAESTHESIA AND CHRONIC PAIN MANAGEMENT Point-of-care ultrasound technology has come a long way in the last decade, from the early systems with tiny screens producing a grainy image, through to modern state-of-the-art instruments with outstanding resolution; the development of ultrasound technology has been nothing short of phenomenal. As a result, the popularity of using point-of-care ultrasound to guide regional anaesthesia continues to grow and, like many in the UK, the anaesthesia department at Morriston Hospital, Swansea, has turned to this technique for routine hand surgical lists. Interest in point-of-care ultrasound began with the acquisition of some very basic instruments to meet NICE guidelines for central venous access, however, it was soon clear that these systems would also be ideal for performing nerve blocks, and could potentially revolutionise both regional anaesthesia and chronic pain management. Using ultrasound for the hand lists alone has introduced massive financial savings, recovering the cost of the ultrasound instrument several times over. Where general anaesthesia requires a dedicated consultant anaesthetist for each theatre list, ultrasound-guided regional blocks can be handled safely and effectively by just one anaesthetist covering two theatres, allowing as many as eight patients to be treated in an afternoon. The system has been in use for seven years now, with a success rate close to 100%, allowing more than 90% of hand surgical procedures to be carried out as day-case patients, maximising throughput efficiency and helping to reduce waiting times. Patients appreciate regional anaesthesia too; those unsuitable for general anaesthetic can still be treated, and time to discharge is much faster. Surgery while the patient is awake also makes it easier for the surgeon to explain the treatment, showing them what is happening. Most patients engage with the process and find it fascinating. Today, the hospital has access to a wide range of ultrasound systems – SonoSite’s iLook®, MicroMaxx®, M-Turbo®, S-Nerve™ and the recently launched X-Porte® – and is benefitting from increasingly advanced technology in even more applications where precise needle placement is essential. Another example at Morriston is in replacing fluoroscopy imaging with ultrasound guidance in the management of spinal chronic pain interventions. While fluoroscopy outlines the bony structures, allowing the anaesthetist to establish whether the needle is in an optimal Cadavers are also being used to teach the practical skills required to perform ultrasound guided regional anaesthesia (USGRA). Although Anaesthesia News November 2014 • Issue 328 ANAESTHESIOLOGY Anaesthesia News November 2014 • Issue 328 or suboptimal position, ultrasound has the advantage of also visualising soft tissue structures, adding an extra dimension to the accuracy of the procedure. Fluoroscopy may require several attempts to position the needle accurately, whereas with ultrasound it is possible to identify the target and correctly place the needle first time, which is far easier for a patient to tolerate. From a practical perspective, medical staff are no longer repeatedly exposed to radiation which, although very low level, requires a heavy protective gown to be worn. Ultrasound also offers cost savings – there is no need for an expensive X-ray suite or the services of a radiographer, and fewer staff are required – and increased flexibility. Often, patients are unable to adopt the position necessary to perform an X-ray-guided injection, or lie still on the table. With ultrasound, there is the flexibility to adapt procedures to the needs of the individual patient, while still maintaining accuracy of injection. Dr Christian Egeler Consultant Anaesthetist, Morriston Hospital, Swansea Affordable ultrasound: No running costs with the SonoSite standard 5 year warranty Such precision is applicable to all other chronic pain interventions, offering the possibility of new treatment approaches. As a further advantage, ultrasound enables the anaesthetist to see the spread of the injectate. In many cases, this additional accuracy enables the drug dosages to be reduced, reducing the risk of side effects and increasing the cost-effectiveness of the procedure. While further studies are necessary, from experience, ultrasound certainly seems to enhance the safety of injection, opening up new possibilities and improving patient experience. Overall, it has transformed regional anaesthesia and chronic pain interventions, proving a cost-saving modality in modern anaesthesia. For more information about FUJIFILM SonoSite products, please contact: FUJIFILM SonoSite Ltd Tel: +44 (0)1462 341151 Email: ukresponse@sonosite.com www.sonosite.co.uk 13 Still bleeding after all these years… 14th Obstetric Anaesthesia Symposium 9th December 2014 Lumley Castle, Co.Durham Maternal Critical Care: a view point Dr A Vercueil – London Training for Obstetric Emergencies Dr N Hayes – Dublin Anaesthesia for the Developing Brain Dr T Girard- Switzerland Top Tips for Optimising Labour Analgesia: the best in evidence based practice Dr G Stocks - London Haemodynamic Monitoring of the Pregnant Mother Dr S Armstrong – Surrey NAP5 – Awareness in Obstetric Anaesthesia Dr N Lucas - London Uterotonics in Prevention and Treatment of PPH Dr T Girard - Switzerland The Invasive Placenta: Regional Policy for Screening and Management Professor S Robson - Newcastle How (not) to Publish a Paper Dr R Russell – Editor in Chief IJOA Decision Making for Obstetric Emergencies: can the Obstetrician make it better for the anaesthetist Mr K Hinshaw - Sunderland Fees: Consultants £150 Staff Grades £100 Trainees £50 Midwives £40 ANAESTHESIA NEWS 5 CPD Points Applied for Course Organisers Dr U Misra Consultant Anaesthetist & J Williams Anaesthetic Secretary Sunderland Royal Hospital Tel No: 0191 5656256 Ext 42447 Email: janice.williams@chsft.nhs.uk The AAGBI Bleeding, Clotting and Haemorrhage seminar celebrates its 10th anniversary this December with a special two-day meeting in London. It has evolved into one of the most established and popular seminars run by the AAGBI, having been attended by over 1000 delegates since its inception. Anaesthesia News now reaches over 10,500 anaesthetists every month and is a great way of advertising your course, meeting, seminar or product. Anaesthesia News is the official magazine of the Association of Anaesthetists of Great Britain & Ireland. The inaugural seminar was fully booked two months before the event and ongoing popularity has dictated a move to a larger venue to accommodate demand. From the outset, Ravi has always been able to attract a host of national and international experts to speak on key aspects of haemorrhage management. Anaesthetists take a lead role in almost all major haemorrhage management across a wide variety of hospital settings. All anaesthetists are expected to manage bleeding patients appropriately - be it in elective or emergency surgery, trauma, obstetrics or in critical care. Current knowledge of development and best practice is essential to ensure that our patients receive optimal care. In the words of Richard Dutton (Executive Director of the American Society of Anesthesiologists Quality Institute, anaesthesiologist at Baltimore Shock Trauma Centre and a regular speaker) the Bleeding, Clotting and Haemorrhage seminar ‘has significantly advanced the practice of resuscitation; as well as the awareness of trauma as a disease that is amenable to a systematic, scientific, multi-disciplinary approach. The concepts of early recognition of life-threatening hemorrhagic shock, a 'damage control’ approach to surgery, deliberate hypotension, early (and diverse) coagulation testing, and timely support with plasma and platelets were all early scientific topics at this meeting’. For further information on advertising Tel: 020 7631 8803 or email Chris Steer: chris@aagbi.org Dr Les Gemmell 21 Portland Place, London W1B 1PY Evolution Significant advancements have been made in understanding the pathophysiology of major haemorrhage, development of tissue damage associated coagulopathy in trauma and the role of platelets and fibrinogen in haemostasis. A host of novel pharmacological options and new blood component therapies have been introduced into clinical care - some with more success than others. Near patient testing has become more widely established and accepted beyond the cardiac theatre to guide blood component therapy optimally. CALL NOW FOR A MEDIA PACK Immediate Past Honorary Secretary The long running organiser is Dr Ravishankar Rao Baikady, a consultant anaesthetist at the Royal Marsden Hospital in London, with an interest in anaesthesia for major cancer surgery and preoperative assessment. While working as a senior registrar at St George’s Hospital in 2003, he was part of a group who published research on the role of recombinant Factor 7 (Novoseven) in fixation of pelvic fractures.1 During this time he identified that there was a great degree of confusion among clinicians regarding management of major haemorrhage. In his own words, ‘the most striking element was a lack of ownership and poor communication between clinicians - anaesthetists, transfusion practitioners, haematologists and surgeons’. The seminar was designed to collate expert opinion from a variety of backgrounds and efficiently update anaesthetists with recent developments on the management of major haemorrhage. Transfusion practice and the management of major haemorrhage have evolved substantially over the last ten years. Clinical practice now involves widespread use of major haemorrhage protocols, 1:1 red cell to plasma ratios and near patient coagulation testing with TEG or ROTEM to guide component therapy. Establishment of local, national and international guidelines and multidisciplinary hospital transfusion committees have fostered a much better understanding between anaesthetists, surgeons, haematologists and the blood bank, helping to facilitate a more coordinated and efficient process. www.aagbi.org/publications 14 Origins Anaesthesia News November 2014 • Issue 328 Anaesthesia News November 2014 • Issue 328 This year’s event promises to excel, with a host of international experts speaking on a variety of themes relevant to all anaesthetists. The first day includes updates on current research in haemostasis, coagulopathy monitoring and point of care testing and the role of red blood cells; finishing with a session on current controversies in haemorrhage management. The second day explores best practice in trauma, subspecialty haemorrhage management and drugs in haemostasis. It promises to be a truly comprehensive account of current knowledge, delivered by excellent speakers from across the globe. Secrets of a successful seminar The AAGBI is always interested in hearing from clinicians who are keen to establish new seminars. Ravi’s advice is to ‘identify a topic which is not well understood or where research is informing rapid developments in practice. Choice of topics and speakers is key. I always believed in a mix of international and national speakers, there is lot to learn from practice in other countries’. The evidence suggests that his approach can be very successful and he deserves great credit. Again, the words of Richard Dutton: ‘it has been my great pleasure to be a participant in the meeting over the years. I cannot say enough about Ravi's skills as a creator, organiser and convener’. The future It is likely that developments will continue to evolve in this field and there is an undoubted requirement for a forum at which anaesthetists can acquire current knowledge. Improvements in understanding the pathophysiology associated with major haemorrhage are likely to lead novel pharmacological targets. ‘Patient Blood Management’ is a multi-faceted WHO concept from 2011 which is yet to be fully integrated into British hospitals but one which dovetails with many of the Enhanced Recovery themes.2 Conclusions The AAGBI Bleeding, Clotting and Haemorrhage seminar continues to thrive. It is an excellent opportunity to hear experts speak on a topic which pervades all aspects of anaesthesia. Places for December will go fast, better sign up now! Dr Jonny Price ST6 Anaesthesia and Intensive Care Medicine, London GAT Elected Committee Member Acknowledgements With thanks to Ravishankar Rao Baikady and Richard Dutton for their contributions. References 1. Raobaikady R, Redman J, Ball JA, Maloney G, Grounds RM. Use of activated recombinant coagulation factor VII in patients undergoing reconstruction surgery for traumatic fracture of pelvis or pelvis and acetabulum: A double-blind, randomized, placebo-controlled trial. British Journal of Anaesthesia 2005; 94: 586–91. 2. Spahn DR, Theusinger OM, Hofmann A. Patient blood management is a win-win: A wake-up call. British Journal of Anaesthesia 2012; 108: 889–92. 15 Anaesthetic training in underdeveloped countries: what is the role of junior trainees? The view of the UK trainee On completion of my basic anaesthetic training in the London Deanery I had an opportunity to experience anaesthesia in Zambia as part of the MMed Anaesthesia Programme at the University Teaching Hospital, Lusaka. This teaches Zambian doctors to become specialist anaesthetists. I had no idea what to expect or how I would fit in to the programme, so I attended a faculty meeting in London and spoke to Professor Kinnear, the head of the MMED Anaesthesia Programme. My brief was to help the UK consultant faculty deliver basic science teaching to the Zambian trainees and provide UK style MCQ/viva practice. My secondary objective was to ascertain if other UK trainees would benefit from this role as part of a larger, more formalised training programme. I also expected to learn from the first cohort of anaesthetic trainees and experience anaesthesia in unfamiliar surroundings. My primary FRCA gave me the perfect grounding in basic science knowledge and exam skills to help the UK consultant faculty cover important elements of the syllabus and provide a more junior perspective to the teaching programme. Teaching helped me to embed my basic sciences knowledge. Due to the intermittent visits of the UK consultants, local students were not able to have regular exam viva practice. I spent time practising mock viva and MCQs with them. This was well received and allowed the MMED students to gauge the standard of clinical knowledge of a UK trainee at a similar level of experience. It was evident that Zambian and UK trainees have similar anxieties regarding training and exams. I also learned about anaesthesia using limited resources in unfamiliar surroundings. There were some stark differences in practice, such as the almost universal non-availability of capnography, but I put this to good use by explaining how capnography works and the huge benefits that UK practice has gained from its consistent use. Lack of monitoring allowed me to recognise that safe anaesthesia can still be delivered without the plethora of anaesthetic devices we employ in the UK. I put into practice theory about anaesthetic devices/drugs that I had only seen images of and read about in books. For example, using halothane and draw over vaporisers, and coping with antiquated anaesthetic machines. Holding and using equipment and applying somewhat turgid learning about physical properties is priceless in my view. With the pace of technological change in UK based anaesthetics, equipment that was in use only 10 years ago is now historic for junior UK trainees. 16 A surprising aspect of my experience was my increased appreciation of the role of managers in the NHS, having seen the clinicians at UTH hospital deal with complex organisational issues as well as their clinical work on a daily basis. A hospital like UTH run on a limited budget also illustrated to me how to save money and stop the unnecessary waste that is commonplace in UK hospitals, a lesson I now try to apply in my own practice. As a junior in UK training there is no opportunity to gain insight into the running costs of a department and to realise that all members of the team are responsible for driving down costs. This attachment is a worthwhile partnership between an overseas training programme and UK trainees. It provides a platform for colearning, discovery of differing practice, and allows UK trainees to gain new skills that would be impossible to obtain in a UK training programme. This experience has been invaluable for my continuing anaesthetic career. I look forward to becoming more involved in the programme in the future and hope my experience will serve as a model for improved training for both Zambian and UK junior anaesthetists. Natasha Clunies-Ross ST3 Anaesthetic Trainee, KKS Deanery, St Richards Hospital, Chichester The view of the Zambian trainee For the first time since the Zambia Anaesthesia MMed programme began, we had a junior trainee from the UK who was here for one month, rather than the more normal two weeks. This made a huge difference. I was the first trainee to meet Natasha on her arrival, and I was asked by my Head of Department, to show her around the hospital. She did not take long to adjust to her new surroundings and engage with delivery of the programme. She told me that she had just completed her primary FRCA exam, and had a strong desire to teach. I remember she asked some probing questions the very first day I was with her. My fellow trainees and I usually have discussions in the evening and Natasha quickly offered to stay late to help our discussion group. We found this so humbling that someone would give up part of their leisure time and make a sacrifice for us. Natasha helped us with difficult topics and concepts that we found hard to understand, especially the basic sciences where most of our weaknesses lie. The value of these extracurricular teaching sessions Anaesthesia News November 2014 • Issue 328 was immense and we would like to acknowledge her efforts. All the Zambian trainees thought she equipped us well for our exam. It was unfortunate that she had to leave before we took our exams in June. However, she laid the foundations of our knowledge and helped boost our confidence in facing the viva exam. Besides helping us to prepare for the exams, Natasha helped us with clinical cases and we learned some clinical skills from her. We got to share many experiences, and it was encouraging to note that many of our needs and concerns were familiar. Personally I see no disadvantages to having a junior UK trainee who has completed their primary FRCA exams coming over for a month in addition to the visiting consultant lecturers, because they will impart knowledge to the MMed trainees in their own way. We are looking forward to having another junior trainee with a teaching spirit like Natasha CluniesRoss. Jane Kabwe MMed Year 3 student, University Teaching Hospital, Lusaka The view of the Head of Programme The Zambia MMed Anaesthesia Programme was identified as a priority project by the Zambian Permanent Secretary for Health in 2009, when it was realised that the country required trained physician anaesthetists to address its high anaesthetic mortality rate. Postgraduate training was already available in several hospital specialties such as surgery, orthopaedics, O&G and Paediatrics, offered by the University of Zambia School of Medicine as a 4 year Master of Medicine (MMed) programme. It was decided that this should also be the format for postgraduate anaesthetic training, but the greatest barrier was a complete absence of a curriculum, faculty or any infrastructure support for a postgraduate programme. For this reason the UK was approached to initiate and embed a programme, with the aim of developing local capacity so that it could become selfsustaining over time. The Zambia MMed Programme is now in its third year, and has evolved a ‘hybrid’ overseas faculty model consisting of a long term UK consultant, a 6-month senior UK trainee fellow, several shortterm UK consultants, and ad hoc junior UK trainees. The challenging nature of the clinical environment has dictated that faculty should be experienced, competent and independent before embarking on the Anaesthesia News November 2014 • Issue 328 role, which meant that the exact role of the junior trainee was unclear at first. However, a few pioneering core trainees have begun to define the very important part that they have to play, and Natasha and Jane’s accounts describe the symbiosis of international peer co-learning. Jane has given a humble view of how the Zambian trainees benefited hugely from learning the academic aspects of anaesthesia from their UK counterpart, a paradigm completely foreign to them. Besides the teaching, what Natasha also brought was the example of a fully matured professional, confident of her own role in the care and safety of patients, and the responsibility to advocate for patients. Zambia lacks this tradition and the local trainees will certainly benefit from the modelling of inter-professional behaviours by their UK peers to help them to build their own professional identities. However, what Jane has failed to describe is the huge clinical experience she and her co-trainees have accumulated from having to cope with complex cases almost from day one of their training. On a normal day they have to share a porter who acts as an itinerant assistant, they have to reuse odd bits of disposable equipment, learn to make do with the drugs available to them on that day, and work with equipment that is in various stages of falling apart. This takes enormous resilience, innovation, patience, and often a good sense of humour. They also frequently deal with surgeons unused to challenge from anaesthetists, and have had to develop effective negotiating skills in the face of conflict. Surely NHS trainees will benefit from learning these rare traits? Having started from a position of uncertainty about the role of junior UK trainees in the challenging environment of UTH, I now have no doubt of their value. They undoubtedly have as much to learn as they have to teach, provided they start out with the right preparation. To achieve maximum benefit it is important for the trainee to define the boundaries of their clinical practice (which may be different to the UK) since they may be faced with situations beyond their competence. For optimal learning they should also have access to adequate supervision for clinical, educational and pastoral support. And they should have clear objectives for their visit. If these basic elements can be provided, the trainee will come away having experienced and supported something of immense educational value. John Kinnear Head of Programme, Zambia MMed Anaesthesia; Consultant in Anaesthetics and Critical Care Medicine, Southend Hospital 17 The Anaesthesia Heritage Centre invites you to a series of new exhibitions: ANAESTHESIA HERITAGE CENTRE A Silver Lining Through the Dark Clouds Shining*: The Development of Anaesthesia During the First World War * A line from Keep the Home-Fires Burning by Ivor Novello The Anaesthesia Heritage Centre is producing a series of four temporary exhibitions honouring the work of the doctors who gave anaesthesia and pain relief to wounded people during the First World War. * The four exhibitions, each lasting a year, will explore the development of anaesthesia and pain relief and how the status of anaesthesia changed during this time. g n i t i n U Social media e h t in anaesthesia ra inees t The first exhibition in 2014-2015 will look at Geoffrey Marshall versus Henry Boyle: who really developed the Boyle machine? s bringing back the wounded British soldier ©IWM (Q 721) courtesy of the Imperial War Museum • The first specialist military anaesthetic posts were created. • An understanding developed of how to anaesthetise wounded soldiers suffering from shock. • The Boyle anaesthetic machine was developed which is still in use today.e Visitor information: The Anaesthesia Heritage Centre, AAGBI Foundation, 21 Portland Place, London W1B 1PY. Open Monday to Friday 10am until 4pm (last admission 3.30pm). Appointments are recommended: email heritage@aagbi.org or phone 020 7631 8865. Admission is free. Group visits for up to 20 people can be arranged at a small cost per person. Registered as a charity in England & Wales no. 293575 and in Scotland no. SC040697 Did you know that during the First World War Oral history interviews linking past to present are also featured. These living histories highlight how treating wounded people in wartime has led to developments in pain relief and anaesthesia. Geoffrey Marshall Marshall’s apparatus Boyle’s apparatus Henry Boyle Visit www.aagbi.org/heritage for further information TRAVEL GRANTS/ IRC FUNDING Social media, once the province of youth, has now been used increasingly to communicate and distribute information in the workplace. For example, the AAGBI and the RCoA both have Facebook and Twitter accounts and my own department utilises WhatsApp as a means of instant departmental communication. The immediacy and connectivity make them excellent tools, but can they be utilised more effectively amongst the trainee body to effect change? SAS Simulation Training Thursday 26 February 2015 or Thursday 12 March 2015 In my Deanery there are 17 different hospitals spread across a reasonably large geographical area. Therefore trainees are dispersed and often not in touch with each other or aware of training issues or opportunities others have discovered. This problem came to my attention when I was on maternity leave and I found the process of negotiating my return to work as a less than full time (LTFT) trainee difficult and somewhat stressful. In a climate where LTFT training is increasingly desired, its implementation at a grass roots level can be variable and understandably difficult while service provision assumes everyone works full time. The International Relations Committee (IRC) offers travel grants to members who are seeking funding to work, or to deliver educational training courses or conferences, in low and middle-income countries. Please note that grants will not normally be considered for attendance at congresses or meetings of learned societies. Exceptionally, they may be granted for extension of travel in association with such a post or meeting. Applicants should indicate their level of experience and expected benefits to be gained from their visits, over and above the educational value to the applicants themselves. For further information and an application form please visit our website: http://www.aagbi.org/international/irc-fundingtravel-grants or email secretariat@aagbi.org or telephone 020 7631 1650 (option 3) Closing date: 02 January 2015 Venue: Centre For Clinical Practice Chelsea and Westminster Hospital 369 Fulham Road | London | SW10 9NH 2 x one day training courses Delegate registration fees: £240 per candidate Spaces are limited. To book please contact: simulation@chelwest.nhs.uk This course is specially designed for the needs of SAS anaesthetists. The content will be based on Anaesthesia Crisis Resource Management (ACRM). This course aims to train anaesthetists to avoid and deal with crisis situations. The main focus is on teamwork and human factors. Useful practical points will also be covered. The setting is a simulated theatre using an advanced simulation manikin with realistic physical and physiological signs. (CPD points applied for) I decided to set up a closed Facebook group for LTFT trainees in my Deanery to share experiences and information. The group has the privacy designation of 'secret' which means that its existence and content is known only to those who are invited to join. The Deanery was able to confirm the number of LTFT trainees but not their details; however, given the relatively small numbers, the identities of these trainees was easy to obtain via word of mouth. Very quickly all the LTFT trainees in the Deanery were members. The forum has become a safe place to discuss our experiences of working LTFT and to share information about working conditions on different clinical sites. It is used on an almost daily basis. It became clear that there were aspects of working LTFT that were causing unhappiness and concerns over training. These were issues Anaesthesia News November 2014 • Issue 328 about which the training committee were largely unaware. Working as a cohesive group, Dr Jacqueline McCarthy, a fellow trainee and active member of the Facebook group, carried out a survey of all the LTFT trainees in our Deanery, and presented the training committee with data representative of the experiences of all LTFT trainees in anaesthetic training posts. Using social media as a platform to facilitate change has had a large impact on those trainees working LTFT in our Deanery. The forum has facilitated information sharing, valuable data collection and peer support for a group of trainees that can often feel isolated and separate from the rest of the trainee body. In a climate of budget cuts, recruitment difficulties and the European Working Time Directive, sustainability of LTFT training appears under threat. We feel that by uniting as a group and engaging with the training committee we can work together to maintain and improve our training. Miriam Stephens ST5 Anaesthesia Royal Alexandra Hospital, Paisley Jacqueline McCarthy ST5 Anaesthesia Western Infirmary, Glasgow 19 NIAA National Institute of Academic Anaesthesia JOINT NIAA AND RCS MEETING: In September 2014, the AAGBI launched Lifeboxes for Rio. A two year fundraising campaign aiming to raise funding for 600 Lifebox pulse oximeters, one for each British athlete attending the next Olympic and Paralympic Games in Rio de Janeiro (5 - 21 August 2016). That’s £96,000 to save thousands of lives around the world in countries where patients are at risk of death from oxygen starvation during surgery. Join the campaign and become a Lifeboxes for Rio fundraiser The AAGBI wants to involve its members all over the UK and Ireland in the Lifeboxes for Rio fundraising campaign. There are lots of ways to take part: Bake, bike ride, run or walk – or devise your own fundraising concept. www.aagbi.org/about-us/aagbi-fundraising AAGBI Foundation: Registered as a charity in England & Wales no. 293575 and in Scotland no. SC040697 Lifebox: Registered as a charity in England & Wales (1143018) Perioperative Clinical Research: Opportunities for surgical and anaesthetic collaboration Wednesday, 4 March 2015 at The Royal College of Surgeons of England, 35–43 Lincoln’s Inn Fields, London WC2A 3PE SESSIONS INCLUDE ■ ■ ■ Funders’ market place, HTA, EME and i4i Exemplar initiatives from surgery and anaesthesia Dragons’ Den: four presentations. Submit yours to dabrahams@rcseng.ac.uk SPEAKERS INCLUDE ■ ■ Professor Dion Morton Professor Mike Grocott CPD POINTS WILL BE AWARDED ‘Explore new collaborative research opportunities for surgeons and anaesthetists focusing on developments in perioperative care and enhanced recovery.’ Book your free place now: http://bit.ly/1qH7cho REGIONAL ANAESTHESIA UK G N I T E E M C I F I T ESIA H T N S E E A I N A C L S L IONA G A E R U F O N S E I N A LENGING THE BOUNDAR CHAL 15 0 2 y a M 5 1 & Fri D R O OXF n Hall Thurs 14 w o T d r Oxfo S P O H S K R WO E S R U O C REFRESHER N O I T I T E P M POSTER CO R E N N I D E C CONFEREN This is your opportunity to tell us: - what you like - what you would like us to do differently - what you don’t like C M Y CM MY CY CMY K - help shape our future strategy We last ran a survey in 2011: the results have been acted on to ensure the AAGBI delivers the services that meet your needs: - Last time, 86% of you said that you wanted the AAGBI to provide online facilities to help support your revalidation CPD - we have created Learn@AAGBI, the new online learning and CPD zone. - You told us you valued the AAGBI’s patient safety guidelines – we continue to update our guidelines and in September 2014 will be launching the new AAGBI Guidelines App. - 84% of you had attended an AAGBI meeting; we have provided bigger and better conferences offering top quality education with record attendance figures at Annual Congress 2013 and WSM London 2014 - 40% of you said you used Facebook – so we have developed the AAGBI Facebook page and we continue to grow our followers. - 91% said that they thought the AAGBI membership offers value for money – we want to make sure that we are still continuing to do so... FOR MORE DETAILS, REGISTRATION OR ABSTRACT FORM, GO TO www.ra-uk.org Tell us how we can do even better! UNDERGRADUATE ELECTIVE FUNDING UP TO £750 Medical students in Great Britain and Ireland are eligible to apply to the AAGBI Foundation for funding towards a medical student elective period taking place between April and September 2015. A further round of funding will be advertised in the Spring for electives taking place from October 2015 onwards. Preference will be given to those applicants who can show the relevance of their intended elective to anaesthesia, intensive care or pain relief. Applicants may wish to note that a key focus of the AAGBI is support for projects in the developing world. For further information and to apply please visit our website: www.aagbi.org/undergraduate-awards email secretariat@aagbi.org or telephone 020 7631 1650 (option 3) Closing date: 05 January 2015 for consideration at the February 2015 Research & Grants Committee meeting Should anaesthetists spend all their time giving anaesthetics? I read William Harrop-Griffiths’ President’s Report with my usual interest.1 A few years ago, at the time that anaesthetic practitioners were being introduced, a senior manager remarked to me that this appeared an excellent idea and that anaesthetists would surely welcome the opportunity to concentrate their expertise on more interesting and demanding cases. I replied that I did not entirely agree. For my part I needed the ‘simple’ cases as a counterbalance to ‘interesting and demanding’ ones and that if I spent all my time on the latter I would end up feeling frazzled and burnt out. I pointed out that ‘simple’ cases only appeared so because of our high standard of training, and that anaesthetists themselves were prone to forget this. I also said that there was satisfaction in managing such lists with expedition which contributed to keeping waiting lists low. I do not disagree with the substance of Dr Harrop-Griffiths’ argument, and appreciate he does not propose we entirely give up anaesthetising fit patients for minor procedures, however I hope managers do not construe this as an opportunity to reduce consultant numbers! Dr John R. May ‘Pinewood’, Daviot Muir, Inverness Reference 1. Harrop-Griffiths W. President’s report. Anaesthesia News 2014; 325: 5-6. Dear Editor, The Wylie Medal will be awarded to the most meritorious essay on this year’s topic related to anaesthesia Safety in numbers written by an undergraduate medical student at a university in Great Britain or Ireland. THE WYLIE MEDAL UNDERGRADUATE ESSAY PRIZE 2015 Prizes of £500, £250 and £150 will be awarded to the best three submissions. I read with interest Dr Inas Ahmed’s article on her jury summons.1 She implies that no doctor would be employed if they had been detained at Her Majesty’s Pleasure. From personal experience I can recount that this is not so. In the 1980s I was very active as an anti-nuclear Christian peace activist and spent several short sentences in prison for non-violent protests. I continued very contentedly in my work as a consultant anaesthetist without any harassment. My colleagues were either bemused, amused or perhaps quietly respectful of my stand. I was always able to change my on-call duty without detriment to patient care. A.J. Cronin’s classic novel The Citadel portrayed the ruthless punishment of those doctors who dared to step out of line. It is a great novel but in my experience my colleagues were better. I was also very privileged to be able to write a description in the BMJ2 of the appalling unhealthy prison conditions (at the time) in Pentonville Prison and add my small voice to the need for prison reform. SEND YOUR LETTERS TO: The Editor, Anaesthesia News at anaenews.editor@aagbi.org Please see instructions for authors on the AAGBI website Dear Editor, Dear Editor, Allaying a patient’s fears pre-operatively is one of the key roles of the pre-operative visit, and Dr Scott-Brown's approach and use of technology is to be commended.1 The photograph of induction shows that routine pre-oxygenation is also practiced. Having experienced an anaesthetic a few years ago, I now take a slightly different approach to that pictured. Dr Kaye is correct that any doctor escorting a patient on a helicopter transfer should have the necessary training.1 But they may need advice if they are receiving an air transfer, or the aircraft is collecting a patient that doesn't need a doctor to escort them. Lying relatively flat on a trolley, with a person standing above your head is a little unusual. To find a mask placed over your face, held in a gloved hand, which partly obscures your view, and then for that person to lean over your head whilst stretching for the cannula, can be a little disconcerting. To the anxious patient it could induce a feeling of panic. Standing in front of the patient who is in a semi-sitting position, allows the anaesthetist to maintain eye contact with the patient. The patient is then offered the mask and circuit and, if tolerated, asked to hold the mask on their face themselves. When pre-oxygenated, the anaesthetist can watch and talk to the patient during induction, even feeling the pulse (though I betray my age here), before stepping into the usual position for intubation. Dr Sarah McLean ST3 Anaesthesia Dr Kenneth Barker Consultant Anaesthetist Raigmore Hospital, Inverness However, I doubt I will be getting a jury summons any time in the future. Dr Ray Towey Volunteer Consultant Anaesthetist, St Mary’s Hospital Lacor, Gulu, Uganda The overall winner will receive the Wylie Medal in memory of the late Dr W Derek Wylie, President of the Association 1980-82. For further information and to apply please visit our website: www.aagbi.org/undergraduate-awards or email secretariat@aagbi.org or telephone 020 7631 1650 (option 3) your Letters Dear Editor References Reference 1. Scott-Brown S. Your anaesthetic. Everything you ever wanted to know about your anaesthetic but were too afraid to ask. Anaesthesia News 2014; 322: 23-5. I am involved in motorsport medicine and as a Chief Medical Officer have liaised with several air ambulances on what rally medics should do. The product of that liaison is a page of ‘Advice for Marshals’ that is included in a major rally's Operations Manual. The most important point is that no-one should approach the aircraft until signalled to do so by the aircrew, and only from the sides, never from the rear, due to the danger from the main rotor, lowest at the front, and the tail rotor. Dr John Davies Consultant Anaesthetist Royal Lancaster Infirmary Reference 1. Kaye C. Patient transportation by helicopter. Anaesthesia News 2014; 322: 32. For the latest news and event information follow @AAGBI on Twitter 1. Ahmed I. Jury summons: an anaesthetist’s reflection on the legal system. Anaesthesia News 2014; 324: 6-7. 2. Towey RM. The state of the prisons. BMJ 1984; 288: 482. Closing date: 05 January 2015 24 Anaesthesia News November 2014 • Issue 328 Anaesthesia News November 2014 • Issue 328 25 Digested WORLD AIRWAY MANAGEMENT MEETING November 2014 Hypersensitivity associated with sugammadex administration: a systematic review Tsur A, Kalansky A. BOOKING NOW OPEN FOR THE WORLD’S LARGEST AIRWAY MEETING 12-14 NOVEMBER 2015 Booking is now open for next year’s biggest world airway management meeting in Dublin. This is a joint meeting of the Difficult Airway Society & The Society for Airway Management. • Scientific programme • Workshops • Industry exhibition • Poster competition • Keynote speakers • Social events Plus, much much more! JOINT MEETING OF THE DIFFICULT AIRWAY SOCIETY & THE SOCIETY FOR AIRWAY MANAGEMENT www.wamm2015.com DUBLIN TO MARK THE 20TH ANNIVERSARY OF THE DIFFICULT AIRWAY SOCIETY & THE SOCIETY FOR AIRWAY MANAGEMENT Sugammadex is a drug that somehow I have never got around to using. Our anaesthetic colleagues in the USA also do not use it because it has not yet been approved by the FDA due to concerns about hypersensitivity reactions. This review by Tsur and Kalansky should at least help them inform their deliberations. The authors gathered evidence of early hypersensitity reactions with sugammadex from a wide variety of sources, including regulatory bodies and the manufacturer. There is good evidence that the reported reactions are actually due to sugammadex rather than other anaesthetic drugs or combinations of drugs. All patients included in the review survived, but there some limitations with the reported data. It only included articles written in English so some reports of hypersensitivity, particularly recent cases in the Japanese literature, were excluded. Also, as a relatively new drug, it is difficult to estimate a reliable frequency of allergic reactions without more data on patient usage. Perhaps much of the drug that has been sold is kept for emergency use, so that sales figures may not directly reflect patient administration to date. Sugammadex is an innovative drug with novel advantages, but I would personally struggle to make a case for anything other than exceptional use. This review helps to quantify one of its major perceived disadvantages and informs risk-benefit assessment. The effects of intra-operative dexmedetomidine on postoperative pain, side-effects and recovery in colorectal surgery Cheung, CW Qiu Q, Ying ACL, Choi SW, Law WL, Irwin MG. Dexmedetomidine seems to be another drug that I would struggle to make a good case for using routinely. Although there is a good theoretical basis for use in a wide variety of applications in anaesthesia and critical care, supporting evidence for clinical benefit has generally been unconvincing. In this article the authors performed a randomised controlled study on the addition of dexmedetomidine to a COX-2 inhibitor and PCA postoperative analgesic regime for colorectal surgery, theorising that a reduction in use of opioids with dexmedetomidine should reduce the incidence of opioid-related side-effects and expedite recovery. Unfortunately, although a reduction in pain scores was seen in the dexmedetomidine group, there was no demonstrable reduction in opioid consumption, opioid-related complications or hospital stay. It thus fails to confirm the opioid-sparing effect reported in other studies, and it was insufficiently powered to detect side-effect differences between groups for either opioids or dexmetetomidine. The authors discuss possible confounding factors in this and other studies that may help to explain some of the results. Which supraglottic airway will serve my patient best? Kristensen, MS, Teoh WH, Asai, T. If, like me, you are puzzled about the sheer variety and claims for perceived advantages of different supraglottic airway devices (SADs), then this editorial, which considers evidence from no less than three previous meta-analyses will help you understand why. They tackle the minefield of device testing and the type of evidence needed before considering use in patients, SADs for airway rescue and the limitations of studies that have used simulated airways to evaluate SADs. They also discuss the responsibilities and moral obligations of manufacturers to produce devices fit for purpose. Despite the large number of papers already published, there still seems to be major deficiencies in the available data, making the question posed by the title difficult to answer. Like all good editorials, it highlights the limitations of existing data and gives useful suggestions about directions for future research. BJ Jenkins Editor, Anaesthesia N.B. the articles referred to can be found either in a print issue or on Early View (ePub ahead of print) Anaesthesia News November 2014 • Issue 328 27 Particles Brown CH, Azman AS, Gottschalk A, Mears SC, Sieber FE Neuman MD, Rosenbaum PR, Ludwig JM, Zubizarreta JR, Silber JH Watson MJ, Walker E, Rowell S, et al. Sedation depth during spinal anaesthesia and survival in elderly patients undergoing hip fracture repair Anaesthesia technique, mortality and length of stay after hip fracture surgery Femoral nerve block for pain relief in hip fracture: a dose finding study JAMA 2014; 311: 2508–17 Anaesthesia 2014; 69: 683–6 Introduction There are over 300,000 hip fractures in the USA per year. Regional anaesthesia for hip fracture surgery may reduce postoperative complications. This study aimed to compare regional and general anaesthesia techniques with regard to 30-day mortality and length of hospital stay. Background Hip fracture is a common orthopaedic emergency, with approximately 77,000 people admitted to hospital in the UK with fractured hips each year.1 Effective analgesia options for patients with hip fracture include femoral nerve block.2 This study attempted to establish the minimal effective dose of levobupivacaine that would provide analgesia to 50% and 95% of patients with a hip fracture, when injected around the femoral nerve using ultrasound guidance. Anesthesia & Analgesia 2014; 118: 977–80 Background Several studies have previously reported an association between low intraoperative bispectral index (BIS) values and increased mortality.1-4 However, this finding was not confirmed as only a few randomised trials of BIS-targeted anaesthesia were previously reported. It is uncertain as to whether low BIS values can be considered as a marker of poor prognosis or whether mortality can be reduced with targeted anaesthetic management based on BIS monitoring. The original randomised trial was performed between 2005 and 2008 and showed a 50% reduction in postoperative delirium5 among patients undergoing surgical repair of hip fracture under spinal anaesthesia who had light versus deep sedation. A later follow-up survival analysis was conducted among the same patients with the suggestion that light sedation may reduce 1-year as well as long-term mortality compared with deep sedation. Methods 114 patients aged >65 were admitted following hip fracture to the Johns Hopkins Bayview Hospital and underwent surgical repair under spinal anaesthesia. Patients were randomised to light intra-operative sedation (BIS>80) or deep intra-operative sedation (BIS approximately 50) by using a propofol or midazolam infusion. Outcomes measured were 1-year mortality as a primary outcome and overall mortality as a secondary outcome in all patients and those with serious comorbidities. Results There was no significant difference in the 1-year mortality between the groups. However 1-year mortality was reduced in patients with a Charlson comorbidity score >4 who had light sedation (22.2%) compared with the deep sedation group (43.6%; HR, 0.43; 95%CI, 0.19-0.97; p=0.04) during spinal anaesthesia. Time to death was also noted to be 4.47 times longer in the light sedation group than in the deep sedation group. 1-year mortality was also reduced in patients with a Nottingham score >4 who had light sedation compared with the deep sedation group (HR, 0.44; 95 CI, 0.21-0.96; p=0.04), and time to death was again longer after light sedation compared to deep sedation (RT, 4.37; 95% CI, 1.16-16.41; p=0.03). Discussion The trial demonstrated that 1-year mortality was reduced in patients with high comorbidity scores who were randomised to light sedation compared with those randomised to deep sedation. The results support the suggestion that light sedation may have a role in reducing mortality, particularly among patients with comorbidities undergoing surgical hip repair under spinal anaesthesia. The results are limited because of the small sample size, unclear cause of death and limitation to a specific surgery. Further research on reduced mortality following light sedation during spinal anaesthesia is needed. Methods A matched, retrospective cohort study was undertaken using data collected from general acute care hospitals in New York State between July 1st 2004 and December 31st 2011. Inclusion criteria were >50 years old, having sustained a hip fracture and the principal procedure of ORIF, hemiarthroplasty or total hip replacement. For patients with multiple hip fracture admissions, the first admission was the index. Patients were matched in relation to the distance they lived from hospitals that specialised in regional or general anesthesia. There was also a secondary analysis included within hospital matches and across hospital matching. The primary outcome was 30-day mortality. In-patient length of stay was a secondary outcome. The hypothesis was that regional anaesthesia would be associated with improved outcomes versus general anaesthesia. Results 98,064 patients were identified for inclusion, 41,335 had missing data (those with missing data were more likely to be from an area of greater poverty and lower educational achievement). Of the remaining 56,729, 15,904 (28%) had regional anaesthesia and 40,825 (72%) had general anesthesia. Those receiving regional anaesthesia were older and had more chronic lung disease. Overall 3032 (5.3%) people died. Mortality was 5.3% for regional anaesthesia and 5.4% for general anaesthesia. The mean length of in-patient stay was 6 days in the regional anesthesia group and 6.3 days in the general anaesthesia group (p <0.001) Discussion There was no reduction in 30-day mortality from the use of regional anaesthesia compared with general anaesthesia. Regional anaesthesia was associated with a slightly shorter length of hospital stay which was possibly related to a lower rate of complications. The authors injected 30 ml levobupivacaine 0.10% w/v in the first participant. A reduction in pain score of ≥20 points with impaired cold sensation was defined as effective. Subsequently, depending on whether the injection was effective or ineffective, the levobupivacaine concentration injected into the next patient was reduced or increased by 0.025% w/v, respectively. If cold and pain measurements conflicted, the response was deemed ‘equivocal’ and the next dose given at the same concentration. After recruitment of 17 patients, the ‘stepdown’ was reduced to 0.005% w/v, to make calculation of the ED50 and ED95 more efficient. The authors used regression analysis to estimate the levobupivacaine concentrations that would be effective in 50% and 95% of patients.3,4 Results Data from 36/40 patients was analysed and estimated the ED50 and ED95 to be 0.026 (CI, 0.023–0.028) and 0.036 (0.027–0.047) % w/v, respectively. Discussion This study found that 30 ml of levobupivacaine at a concentration of 0.05% w/v reduced rest pain by ≥20/100 points in patients with neck of femur fractures, a concentration one-tenth to one-fifth of that typically used in clinical practice. Christina McCarroll and Camilla Waugh ST4 Northern Deanery Lucy Powell CT1 Anaesthesia, Sunderland Royal Hospital References 1. National Institute for Health and Clinical Care Excellence. Hip Fracture: the Management of Hip Fracture in Adults. CG124 London: NICE, 2011. 2. Parker MJ, Griffiths R, Appadu BN. Nerve blocks (subcostal, lateral cutaneous, femoral, triple, psoas) for hip fractures. Cochrane Database of Systematic Reviews 2002; 1: CD001159. 3. Dixon WJ. The up-and-down method for small samples. Journal of the American Statistical Association 1965; 60: 967–78. 4. Brownlee KA, Hodges JH, Rosenblatt M. The up-and-down method with small samples. Journal of the American Statistical Association 1953; 48: 262–77. References Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one1. year mortality after noncardiac surgery. Anesthesia & Analgesia 2005; 100: 4–10. 2. Lindholm ML, Träff S, Granath F, et al. Mortality within 2 years after surgery in relation to low intraoperative bispectral index values and preexisting malignant disease. Anesthesia & Analgesia 2009; 108: 508–12. 3. Leslie K, Myles PS, Forbes A, Chan MT. The effect of bispectral index monitoring on long-term survival in the B-aware trial. Anesthesia & Analgesia 2010; 110: 816–22. 4. Kertai MD, Pal N, Palanca BJ, et al. Association of perioperative risk factors and cumulative duration of low bispectral index with intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology 2010; 112: 1116–27. 5. Seiber FE, Zakriya KJ, Gottschalk A, et al. Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair. Mayo Clinic Proceedings 2010; 85: 18–26. Anaesthesia News November 2014 • Issue 328 Participants were taken to theatre recovery, where a further pain score was recorded and sensation to cold on the middle third of the anterior thigh tested and compared with the contralateral thigh. Femoral nerve block was then performed by one of the authors, a consultant anaesthetist, using ultrasound and a Tuohy needle. A catheter was threaded through the needle after injection of 30 ml levobupivacaine around the femoral nerve had raised the fascia iliaca. Pain and cold measurements were repeated 30 min after levobupivacaine injection, when 20 ml levobupivacaine 0.25% w/v was injected through the catheter if the pain score exceeded 30/100. Although this is a large observational study, the data are from just one US state and the conclusions may not be applicable in other situations. Mohamed Eid ST5 Anaesthesia, Royal Victoria Infirmary 28 Method Forty consecutive competent patients with a hip fracture and a resting pain score of ≥50/100 before surgical fixation were included. Patients with local anaesthetic toxicity, neurological conditions or lower limb amputation were excluded. Anaesthesia News November 2014 • Issue 328 29 EDINBURGH EETING ANNUAL SCIENTIFIC M MANCHESTER SCOTLAND MANCHESTER , UNI VERSITY OF RENOLD BUILDING Y LEAVE NOW! BOOK YOUR STUD 17-19 JUNE 2015 cludinglectures, nalprogrammein • Greateducatio andworkshops ing arn dle ce ase problemb nualDinner&Dan tsincludingtheAn • Funsocialeven itiesincluding tun por top men evelop sandprizes • Professionald antinterview,poster mentoring,consult ingof mwithlivestream roo aby &b ent • Par s conferencelecture www.gatasm.org AC2015advert.indd 1 Learn@AAGBI NEW TY FUNCTIONALI Reflect on educational videos from Annual Congress 2014 and other recent events with Learn@AAGBI The template is easy to use allowing you to reflect on the conference as a whole or on individual lectures. Step-by-step guide on how to reflect using the site: Step 1. Go to www.aagbi.org/education Step 2. Click on the ‘Learn@AAGBI’ box Step 3. Log in note: you will need your AAGBI membership number and password Step 4. From the search page select AAGBI conferences/seminars Step 5. From the list select the video that you wish to reflect on Step 6. After watching the whole video, open the reflective learning form and complete it Step 7. If you are happy with what you have written, click on ‘Submit form’, or if you would like to add more later on, click ‘save draft’. This will upload into the ‘My CPD Area’ as either ‘draft’ or a completed ‘Submitted Reflective Note’. Go to www.aagbi.org/education and use Learn@AAGBI for your reflections at our meetings, and for your ongoing CPD and exam preparation. 30/07/2014 14:26 A AGBI TOPICS INCLUDE: Anaesthetists in training Clinical anaesthesia Clinical measurement/equipment P P A S E IN L E ID U G Contractual/job planning Elderly anaesthesia Ethics and law Haematology Human factors Independent practice Irish anaesthetists Obstetric anaesthesia Regular updates Resuscitation and trauma SAS anaesthesia Wellbeing FREE GBI A A R O F RS MEMBE Checklist for t anaesthetic equipmen ol Reflective learning to DOWNLOAD THE APP TODAY FOR APPLE AND ANDROID DEVICES www.aagbi.org/guidelines-app


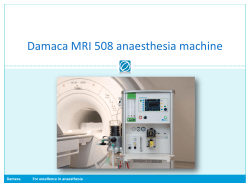







© Copyright 2025