
Owner Operator Application
Owner Operator Application Any Individual wishing to conduct business with Express Courier as an Owner Operator must meet DOT standards. Information solicited will be used to determine eligibility and will not be used for any purposes prohibited by law. SSN: Name: Birth Date: First Middle Last Address: Home Phone: City Fax: Zip State Zip Email: Previous Address: City How long at this address: State Do you have computer access at home? Yes No Do you have the legal right to work in the United States? Yes No Have you ever had an agreement with Express Courier as an Owner Operator? Yes No If yes, indicate dates: Have you ever been an Employee of Express Courier? Yes If yes, indicate dates: No Company Location: Position: _ Reason for leaving: Are you now under contract of Employment? Yes No How long since termination of your last Owner-Operator agreement or last employment? How did you hear about this opportunity? Date you can start: Type of Vehicle: In the past 3 years, have you ever knowingly used any narcotics, amphetamines, or barbiturates, other than those prescribed by a physician? If yes, explain: *Have you ever been convicted of a criminal offense including either a felony or misdemeanor charge? Yes No If Yes, please provide the following information for each charge: Charge: City: County: State: Date of Arrest: Date of Final Disposition: Charge: City: Date of Arrest: Court where case was handled: County: State: Court where case was handled: Date of Final Disposition: Page 1 of 43 *Are you currently charged with committing a criminal offense including either a felony or misdemeanor charges? Yes No Charge: ___________________________________________________ County: __________________________________________ City: _____________________________ State: ______________ Court where case was handled: ___________________________ Date of Arrest: _______________________________ Date of Final Disposition: ________________________________ Describe the Final Disposition: ___________________________________________________________________________________ Owner Operator contracts require flexibility in scheduling. Please list the days and hours, you are generally available for service: Monday: Tuesday: Wednesday: Thursday: Friday: Saturday: Sunday: From: _____________ _____________ _____________ _____________ _____________ _____________ _____________ To: _____________ _____________ _____________ _____________ _____________ _____________ _____________ Accident Record For the Past 3 Years or More Date of Accident: ___________________________ Nature of Accident: ________________________________________________ Number of Fatalities: ________________________ Number of Injuries: ________________________________________________ Date of Accident: ___________________________ Nature of Accident: ________________________________________________ Number of Fatalities: ________________________ Number of Injuries: ________________________________________________ Date of Accident: ___________________________ Nature of Accident: ________________________________________________ Number of Fatalities: ________________________ Number of Injuries: ________________________________________________ Traffic Convictions and Forfeitures for the past 3 years (Other than parking violations) Date of Violation: __________________________ Location: ___________________________ Charge: _______________________ Penalty: ___________________________________________________________________________________________________ Date of Violation: __________________________ Location: ___________________________ Charge: ______________________ Penalty: ___________________________________________________________________________________________________ Date of Violation: __________________________ Location: ___________________________ Charge: _______________________ Penalty: ___________________________________________________________________________________________________ Education: Grade School: 8 High High School: 0 College: 0 Name of last school attended: ____________________________________________ City/State: _____________________________ Experience and Qualifications Driver License Number: ______________________________________ State of Issue: _______________________________ Type: ______________ Expiration Date: ___________________ Name as it appears on License: ___________________________ Driver License Number: ______________________________________ State of Issue: _______________________________ Type: ______________ Expiration Date: ___________________ Name as it appears on License: ___________________________ Driver License Number: ______________________________________ State of Issue: _______________________________ Type: ______________ Expiration Date: ___________________ Name as it appears on License: ___________________________ 1.) Have you ever been denied a license, permit or privilege to operate a motor vehicle? Yes 2.) Has any license, permit or privilege ever been suspended or revoked? Yes No No If you answered yes to either 1 or 2, please explain: ____________________________________________________________________________________________________________________ Page 2 of 43 List special courses or training that will help you as a driver: Which Safe Driving awards do you hold and from whom? Previous Employment or Owner Operator History All Owner-Operator applicants to drive commercial motor vehicles weighing at least 10,000 lbs must provide the following information on all previous employers or entities with which the applicant contracted during the past 3 years. Applicants to drive commercial motor vehicle with a gross combination weight rating 26,001 lbs or more shall also provide an additional 7 years information on those previous employers or entities for whom the applicant operated such vehicle. Entity Name: Address: Phone Number: Contact Person: City State Salary/Wage: Zip Position: Reason for leaving: Contract/Employment Start Date: Contract/Employment Termination Date: Entity Name: Address: Phone Number: Contact Person: City State Salary/Wage: Zip Position: Reason for leaving: Contract/Employment Start Date: Contract/Employment Termination Date: Entity Name: Address: Phone Number: Contact Person: City Salary/Wage: State Zip Position: Reason for leaving: Contract/Employment Start Date: Contract/Employment Termination Date: Page 3 of 43 To Be Read and Signed by Applicant By affixing my signature below, I understand and agree that as part of the procedure for processing this application, the Company may investigate all facts and statements presented here. This inquiry may include information as to my character, general reputation, and prior work habits, whichever may be applicable. My signature below releases from liability all persons and/or organizations supplying or collecting such information. I hereby authorize a representative of the Company to inquire as to my record with any and all of my former employers or companies I have previously contracted with. I further understand and agree that any false statements or answers made by me on this application or supplement thereto, will be grounds for the company to dissolve any agreements. I understand and agree that my contract and compensation can be dissolved, with or without cause, and with or without notice, at any time, at my option or the option of the Company, and that no manager or supervisor other than the President of the Company or his duly authorized representative has any authority to enter into any other agreement for any specified period of time, or to make any agreement contrary to the foregoing. Date Owner-Operator’s Signature NOTICE In compliance with the Department of Transportation, and before entering into an agreement with Express Courier, you may be required to have physical examination by a licensed physician. The cost of the physical is solely the responsibility of the Owner- Operator. Included in the examination is a hearing test, vision test, a comprehensive medical and occupational history questionnaire, vital signs, height, weight, a general physical examination and a urine drug screen. Additionally, if you are offered a run or route, which requires the ability to lift, you may be administered relevant tests. Results of the physical will be submitted under confidential cover to a Company representative. Where test results indicate the presence of illicit drugs and/or undeclared pharmaceutical and/or alcoholic substances, or other conditions, which the Department of Transportation has deemed to be unacceptable, the offer of a contract must be rescinded without penalty to the Company. By affixing your signature below, you can certify that you have been advised, via this notice, of the test which may be conducted and that you voluntarily agree to submit to such testing, if required, following an offer of a contract. Furthermore, you will authorize release of the test results to the responsible agent of our Company, and acknowledge that you understand and agree to all conditions state above. Date Owner-Operator’s Signature Page 4 of 43 Owner-Operator Qualifications Prior to orientation acceptance, all new Owner Operator applicants must provide a current Motor Vehicle Report from the state in which the applicant’s driver’s license was issued. In addition, Motor Vehicle Reports will be checked annually on all Owner Operators under contract. Any applicant or driver whose record has any of the following characteristics in the last 5 years does not meet the requirements and will be declined or their contract will be terminated. Driving under the influence Driving while impaired Driving while in possession of alcohol or drugs Driving with a suspended or revoked license Vehicular manslaughter Vehicular homicide Vehicular assault A felony in which a vehicle is used Reckless driving Hit and run Eluding a police officer Refusal to submit to a blood, urine, or breathalyzer test Speeding exceeding 100 mph (or speeding in excess of 25 mph over the limit) Speed contest / drag racing More than two at-fault accidents, or four moving violations Other violations and accidents on MVR will be reviewed by Express compliance for acceptability I have read and understand the above OO Qualifications requirements. Owner Operator’s Signature: Date: Page 5 of 43 Branch: Branch Operator # ___ ___________ ___________ ___ Owner O _ ____ _______ ____________ ___________ ___________ ________ ___ ___________ ___________ ___________ Name: __ Firrst Mid ddle Last ____________ _ _________ ____________ ___________ ______ ____ ____________ ____________ ___ ____ ______ Address:: __________ City State Zip Number: _____ ___________ ______ Startt Date: _____ ___________ _____ Phone N ___________ License Numb ber: _______ ___________ ____________ ____ State: _ ________ Exxpiration Date e: _________ ____ Driver’s L ____________ ___________ __ Birth Date e: _________ ___________ ___________ SSN: __ Vehicle Information n ___________ ________ Ve ehicle Model: ___________ _ ___________ ___________ Make: ______ _______ Yea ar: _________ ____ Vehicle M ____________ ____________ ____ Color: _ ___________ ___________ ___________ ___________ ___ VIN: ____ ____________ _ State: ____ ___________ _______ Exp ___________ ____________ Tag: _______ piration Date: ___________ ____ License T Insurance Informattion ___________ ___________ ____________ ___________ ____________ ___________ ___________ e Carrier: ____ bile Insurance Automob ____ ___________ ______ ____ ____________ ____________ ____________ _ _________ ____________ ____ ______ ___ Address:: __________ City State Zip _____ Policy _____ ___________ Number: _____ ___________ y Number: ___ ___________ ____________ ____________ Phone N __________ Expiration Da ___________ ___ ate: ________ ___________ ___________ Effective Date: ______ ___________ ___________ Name: ______ ___________ ________ ____________ __ Phone Num mber: ______ ___________ Agent’s N ___________ ___________ Address: ____ ____________ ___________ ____________ ___________ ___________ ___________ Agent’s A ____ ____________ ____________ Amount: ____ ____________ ___________ _________ Property P Dam mage Amount:: __________ ____ Liability A ST BE FAXED S FORM MUS UIRED: THIS EHICLE LICENSE, VE D TO CORPO ORATE WITH A COPY OF F DRIVER’S L ****REQU F INSURANC RATION, AND PROOF OF BER, CE INCLUDIN NG INSURAN NCE COMPAN NY NAME, POLICY NUMB REGISTR VE A TION DATE, LIABILITY AMOUNTS, ED. EHICLE(S) COVERED, C A AND NAME(S)) OF INSURE EXPIRAT Page 6 of 43 PE ERSONAL L DATA R RECORD Branch BRANCH H __________ _______ R # _________ ________ OWNER OPERATOR CONTRAC CTOR INFOR RMATION NAM ME ADDR RESS CIT TY STATE S ZIP TELEPH HONE CEL LL PHO ONE EMA AIL ADDR RESS EMERGENCY Y CONTACT INFORMATIO ON NAM ME ADDR RESS CIT TY STATE ZIIP TELEP PHONE CELL P PHONE DATE NOTES 1.______ __________ _________ ____________ ____________ ___________ ___________ ____________ ____________ ___________ ____ 2.______ __________ _________ ____________ ____________ ___________ ___________ ____________ ____________ ___________ ____ 3.______ __________ _________ ____________ ____________ ___________ ___________ ____________ ____________ ___________ ____ 4.______ __________ _________ ____________ ____________ ___________ ___________ ____________ ____________ ___________ ____ Page 7 of 43 NOTICE – BACKGROUND INVESTIGATION AUTHORIZATION In connection with your application and/or employment with (_______________________________) (Employer) this notice is provided to inform you that a “consumer report” and/or “investigative consumer report”, as defined by the Fair Credit Reporting Act, may be obtained from a consumer reporting agency for employment purposes. These types of reports may include information as to your character, general reputation, personal characteristics and mode of living, whichever are applicable. The report may also contain information about you relating to criminal history, credit history, driving and/or motor vehicle records, social security verification, verification of your education or employment history or other background checks. They may involve interviews with sources such as your neighbors, friends or associates. Reports may be obtained any time after receipt of this authorization and if hired, throughout the course of your employment, as permitted by law. You have the right, upon written request made within a reasonable amount time after the receipt of this notice, to request disclosure of the nature and scope of any investigative consumer report to Confirm Choice, 4205 Hillsboro Pike, Suite 200, Nashville, TN 37215, toll free number 1-888-925-0114. For information about Confirm Choice’s privacy practices, see www.confirmchoice.com. The scope of this notice and authorization is not limited to the present and, if hired, will continue and allow Employer to conduct future screenings for retention, promotion or reassignment, unless revoked by you in writing. Employer also reserves the right to share such reports with a third-party for whom you will be placed to work as a representative of Employer, if applicable. Acknowledgement and Authorization By signing below you acknowledge receipt of a copy of the A Summary of Your Rights under the Fair Reporting Act and certify that you have read this notice and authorization as well as the summary. You hereby authorize, without reservation, the obtaining of a “consumer report” and/or “investigative consumer report” at any time after receipt of this authorization and during the course of your employment, to the extent permitted by law. You also confirm your understanding and provide consent for this report to be shared with a third-party for whom you may be placed to work as a representative of Employer, if applicable. Minnesota & Oklahoma applicants or employees only: Under state law you have a right to receive a copy of your consumer report, free of charge, if one is requested by Employer. By checking “yes”, a copy will be provided to you at the address you provide on this notice. I would like to receive a copy of my consumer report: (___) Yes (___) No New York applicants or employees only: Under state law you have the right to inspect and receive a copy of any investigative consumer report requested by Employer by contacting Confirm Choice directly. You also acknowledge receipt of a copy of Article 23-A of the New York Correction Law by signing this notice. Washington State applicants or employees only: Under state law you have a right to request a copy of the Washington Fair Credit Reporting Act’s disclosures to consumers (RCW 19.182.070) by contacting Confirm Choice directly. California, Maine applicants or employees only: Under state law you have a right to receive a copy of your investigative consumer report and/or consumer credit report, free of charge, if one is requested by Employer. By checking “yes” a copy will be provided to you at the address you provide on this Notice. I would like to receive a copy of my consumer report: (___) Yes (___) No _____________________ Social Security Number* Signature Today’s Date Print Full Name __________________________________________________ Other names you have used ___________________________________________ Date of Birth* Driver’s License Number & State Issued Name as it appears on Driver’s License Current Address City State Zip Previous Address 1: ___________________________________________________________________________________ Previous Address 2: ___________________________________________________________________________________ * This information will be used for employment-related background screening purposes only and no other purpose. 3/19/13 ___________ __ ________ Date n: Express Co ourier Attention are that consu umer and mo otor vehicle re eports may be I am awa e obtained ass part of Exprress Courier IInternational’ss evaluation of o my Operator agreement execu ution. The re ports p may be procured byy Express Cou mpany Owner-O urier Internatiional or its in surance com ntative(s), and d may include e personal in nformation ob d, an represen btained from sstate motor vvehicle deparrtments, my driving record ment of my insurability for th he insurance program, p or other o assessm consum mer reports. ng this letter, I hereby provide my auth horization for Express Cou Be signin urier Intl. or th heir insurance e company re epresentative(s) to s additional report re aluate procure ssuch informattion and reports, as well as about m me from time--to-time as de eemed approp priate, to eva ability or for other o permissiible purposes s. my insura Sincerelyy, ___________ ___________ ________ ________ Operator’s Sig gnature Owner-O _____ ____________ ___________ __ Owne er-Operator # Branch ___________ ___________ ________ ________ Branch ________ __ ________ ___________ ___________ ____________ ____________ ____________ _______ ___ ____________ _________ Name ass it appears on Drriver’s License n Driver’s Lice ense e Number Sttate Issuing Liicense ____________ ________ ___________ ___________ _ __________ ___ _______ ___________ __________ Date of B Birth Gender Social Se ecurity Numb ber Page 9 of 43 COMPANY PROPERTY RECEIPT Owner-Operator # Name Date_ My signature below acknowledges that I, _, will be provided for my use while serving as an Owner-Operator on behalf of Express Courier, Inc., or will lease from the company the following items: (A) cooler, (B) vehicle sign, (C) pager, (D) communication device, (E) Spill Kit The following items have been provided to me by Express Courier, Inc. and I understand I will be charged a reasonable fee for their use. In the event that my contract is terminated for any reason, I will promptly return all items. A) COOLER (1) Thermos Cooler - Replacement Cost $50.00 B) TRUCK SIGNS (2) Truck Signs. I understand it is ICC policy to display these signs while performing delivery services for the company. Replacement cost $10.00 each. C) PAGER (1) Pager - Replacement Cost $100.00 D) COMMUNICATION DEVICE (1) Phone – Replacement Cost $200.00 Phone No. Serial No. E) Spill Kit (1) AC Adapter Cost $43.25 (1) Belt Clip Cost $10.81 (1) $8.00 IT IS HEREBY UNDERSTOOD AND AGREED UPON THAT REIMBURSEMENT FOR LOST OR DAMAGED ITEMS MAY BE DEDUCTED FROM MY FINAL COMMISSION CHECK AT THE COSTS DESIGNATED ABOVE. SIGNATURE SIGNATURE (OWNER-OPERATOR) (EXPRESS COURIER MANAGEMENT) DATE DATE Page 10 of 43 Owner Operator Scanner Inventory Control Form Location Name: O/O Name: Date: O/O Number: I, , acknowledge receipt of the following said equipment and agree to a deduction from my weekly settlement for the associated costs. I understand that I am solely responsible for the equipment and will be held accountable should it be lost, stolen or broken beyond repair. Further, I understand that should termination of contract occur, I will be expected to immediately return said equipment. If I neglect to return the equipment, the amount necessary to replace the equipment will be due within ten (10) days of the contract termination date. I hereby consent to Express Courier International, Inc. deducting from any settlement commissions due me the value of any equipment I do not return, the cost of repair of the damaged equipment, or the cost associated with the repair of any damaged equipment. If I do not reimburse ECI in full for the said equipment, I understand that I will be responsible for any legal fees incurred by ECI in an effort to seek reimbursement. If scanner is damaged due to abuse or negligence a $25 handling fee will be deducted for shipping and handling. Scanner Unit Unit Number SIM Number Serial Number Replacement Cost $ 1,881.89 Stylus Cost $ 5.00 Holster Cost $ 32.50 Car Charger $ 74.00 Wall Charger $ 82.00 ***Commissions are calculated on four-week average of scan deliveries*** OO Signature: Date: ECI Representative Signature: Date: Page 11 of 43 Dispatch Notification Form Owner-Operator Number: Owner-Operator Name: Monday Tuesday Wednesday Thursday Friday Saturday Sunday Type of Vehicle: What part of town do you sign on in? Page 12 of 43 POLICY AND PROCEDURES FOR OWNER-OPERATORS The company has various types of runs or services, which may be offered to you on a regular basis. Our dispatchers determine who is available to handle a given run based on the availability of owner-operators. When a run is offered to you, you have the right under your contract with us to refuse the run. If you choose to do so, you must notify dispatch immediately so that the run can be offered to another owner-operator. The company does not set service hours for owner-operators. As a owner-operator, you have the flexibility of setting your own service hours and are a master of your own time. At the same time, however, the Company knows when runs are available and what our customer’ time requirements are. Therefore, to maximize your income and to assist in facilitating run assignments, it is advisable that you work with dispatch to determine the hours you will be available for service each day or each week. If you intend to take an extended period of non-service for any reason, it is requested that you provide dispatch with a minimum of five (5) days notice of this activity so that we can make arrangements with other owner-operators. I have read, understand, and agree to comply with the above Policy and Procedures. Owner-Operator’s Signature Date Page 13 of 43 Anti-Harassment Policy Express Courier International, Inc. is committed to providing all owner-operators the opportunity to pursue excellence and profitability in their professional driving careers. As a condition to a continual contractual relationship, Express Courier International, Inc. expects owner-operators, doing business on behalf of ECI and their customers, to conduct themselves in a professional manner at all times. This can only be achieved when there is a mutual respect for all individuals with whom owner- operators may come into contact with daily. Express Courier International, Inc. has a zero tolerance policy regarding any form of harassment. Comments, words, jokes, suggestive gestures or actions made to any individual, or that may be overheard or seen by them based on an individual’s sex, race, ethnicity, age, religion, veteran status or any other legally protected characteristic will not be tolerated. Any form of harassment (both overt and subtle) is a form of misconduct that demeans another person and undermines the integrity of the business relationship established between ECI and the owner-operators and customers. Thus, it is strictly prohibited. This policy is applicable to all owner-operators at all times they are in performance of their duties on behalf of ECI. I have read and understand the above Anti-Harassment Policy. Owner-Operator’s Signature Date Page 14 of 43 CONFIDENTIALITY STATEMENT CONFIDENTIALITY REQUIREMENTS - PROTECTING THE PRIVACY OF PATIENTS’ HEALTH INFORMATION 1. INFORMATION REQUIRED TO BE PROTECTED The privacy of all medical records and other individually identifiable health information must be protected at all times. Information relating to a patient’s health care history, diagnosis, treatment, or evaluation shall be considered individually identifiable health information. Confidentiality of their health information must be maintained at all times, and may only be disclosed with the express written consent of the patient. Non-individually identifiable health information (e.g. health information that cannot be linked to a specific patient) is not included with in the definition of protected health information. 2. BOUNDARIES ON HEALTH INFORMATION USE AND RELEASE An individual’s health information can be used for health purposes only. a. Protect individually identifiable health information. Express Courier shall not publish or otherwise make generally available any information or data that identifies a patient for purposes other than treatment, payment or other health care operations, without his or her express written consent. This does not restrict the internal use of such information or data that is required in the Express Courier also maintains physical, electronic and procedural safe guards to protect safeguards and expect to make ongoing improvements to maintain and enhance our level of security for individually identifiable health information. b. Ensure that health information is not used for non-health purposes. Patient information can be used or disclosed only for purposes of health care treatment, payment, and operations. Health information cannot be used for purposes not related to health care without explicit authorization from the patient. For example, Express Courier may not access the personal health information obtained by an Express Courier affiliate for any purpose other than to perform the services for which we were engaged, unless Express Courier first obtains the explicit authorization of the patient. c. Maintain health information in a manner to protect confidentiality. All individually identifiable health information shall be maintained by Express Courier in a confidential manner which prevents unauthorized or inadvertent disclosure to third parties. For example, Express Courier may share confidential information with a third party under contract or affiliated with Express Courier for the same purpose of performing the services which we were engaged, providing that the information shall remain confidential at all times and shall be shared with only those persons that have authority to receive such information. PENALTIES FOR MISUSE OF PERSONAL HEALTH INFORMATION There are serious penalties for violation of the confidentiality of health information. Please be advised of the following: State Penalties. Various state laws impose criminal and civil penalties on individuals who misuse or disclose individually identifiable health information without explicit consent by the patient. b. Federal Penalties. HIPAA (Health Insurance Portability and Accountability Act) is a piece of federal legislation that directly addresses the protection of confidential health information. This law is being phased in over a two-year period. Once effective, HIPAA will provided civil money penalties up to $25,000 per person, per year for violations of patient confidentiality. HIPAA also provides for federal criminal penalties. c. Express Courier’s Penalties. Any owner-operator who violated the privacy and confidentiality of patient health information, though disclosure or otherwise, may be subject to contract termination with Express Courier International, Inc. a. I understand and agree that in the performance of my duties as an Owner-Operator of Express Courier International, Inc., I must hold medical information in confidence. Further, I understand that intentional or involuntary violation of customer confidentiality may result in punitive action including possible fine or imprisonment. Owner-Operator’s Signature Date Page 15 of 43 ENVIRONMENTAL, HEALTH AND SAFETY INFORMATION DRY ICE HANDLING This information is being provided to make you aware of a potentially hazardous condition that exists when handling DRY ICE, or SOLID CARBON DIOXIDE. Please ensure that all personnel who may come into contact with this substance read this information sheet. There are two hazards associated with handling dry ice: Carbon Dioxide intoxication and frozen tissue. CARBON DIOXIDE INTOXICATION When concentrations of Carbon Dioxide in air reach approximately 10 times normal, the typical symptoms of Carbon Dioxide intoxication include headaches, drowsiness, and perspiration. Higher levels can add tremors, visual disturbances, and finally unconsciousness. At much higher concentrations, Carbon Dioxide displaces the oxygen percentage below the levels necessary to support life. To minimize this hazard, ventilate indoor areas to avoid hazardous Carbon Dioxide concentrations. Carbon Dioxide is a heave gas and will remain in low spots without assisted ventilation. Employees should avoid lowering their heads into dry ice chests or in areas immediately adjacent to or in the proximity of materials packaged with dry ice. Carbon Dioxide will displace the oxygen in these containers and you could pass out. When transporting any amount of dry ice, be sure that the heating and air conditioner controls are set to the “Normal” or “Vent” positions and roll down a window an inch or so. Avoid using the “Maximum” A/C setting, which will entrap the Carbon Dioxide and elevate concentrations to dangerous levels. FROZEN TISSUE Direct contact of skin or eyes with dry ice causes the tissue to instantly freeze and be damaged. Damage to eyes cannot be repaired. Protective gloves (suitable for work with cryogens) and safety eyewear/face shields are recommended when working with cold liquid, solid, or vapor. Be sure that you have some heave gloves in case you need to handle the dry ice. In the event of accidental contact, immediately report the incident to your driver supervisor. To help ensure your safety, the following measures have been instituted: Your work area where the dry ice is stored will be periodically monitored for levels of Carbon Dioxide. It must also be monitored if the amount of dry ice stored is increased. Your vehicle will be periodically monitored while you drive your route. If you are called upon to transport larger amounts of dry ice than the routine amount, notify ECI so that your vehicle can be monitored. Procedures for packaging Dry Ice for Air shipments Under no circumstances are you to pack more then FOUR LBS of dry ice to ONE Styrofoam receptacle without written permission by the air carrier. Under no circumstances are you to pack more than ONE Styrofoam receptacle within one sealed box. Your dry ice placards are to be placed on each end of the outside box with no more than 4lbs. written in the space provided. I have read/reviewed the process for handling dry ice and have been given the opportunity to ask questions. understand my responsibilities as an owner-operator when handling dry ice. Owner-Operator’s Signature I Date Page 16 of 43 OWNER-OPERATOR AGREEMENT Express Courier International, Inc. (“CARRIER”), an authorized motor carrier, and (“OWNER-OPERATOR”), in consideration of the covenants and agreements contained herein and pursuant to the federal leasing regulations under 49 C.F.R. Part 376, enter into this Owner Operator Agreement (“Agreement”) on BBBBBBBBBBBBBBBBBBBBBBBBB 1. PROVISION OF SERVICES AND EQUIPMENT. During the term of this Agreement, OWNER-OPERATOR shall provide CARRIER transportation related services and the use of the equipment set forth below or in an appendix (the “Equipment”). OWNER-OPERATOR represents and warrants that OWNER-OPERATOR has title to or is authorized to contract the Equipment and services to CARRIER. Upon initiation of this Agreement with the OWNER-OPERATOR, CARRIER shall furnish to OWNER- OPERATOR a verification form for Equipment to be contracted, which shall constitute the receipt required by 49 C.F.R.§ 376.11(b). Upon termination of this Agreement, OWNER-OPERATOR shall execute a similar form terminating the availability of the Equipment; provided, however, that the Agreement and CARRIER’s obligations thereunder shall expire upon the written notice of termination regardless of whether OWNER-OPERATOR submits the form terminating the availability of the equipment as required by this provision. Year Make Serial No. Unit # 2. DURATION OF AGREEMENT AND TERMINATION. This Agreement shall begin on the date set forth above. Either party may terminate this Agreement for any reason by giving three (3) day’s written notice to that effect to the other party either personally, by mail, or by fax machine at the address or fax number shown at the end of this Agreement. The ability of either party to terminate this Agreement shall in no way be interpreted as an at-will employment provision and shall not otherwise affect OWNER-OPERATOR’s status as an independent contractor under this Agreement. The effective date and time of termination shall be as set forth in the written notice or the verification form for Equipment issued by OWNER-OPERATOR, whichever date is earlier. OWNER-OPERATOR shall, upon the termination of this Agreement, remove all CARRIER identification from the Equipment and return it to CARRIER, via hand delivery or certified mail, together with all of CARRIER’s property, paperwork, load securement equipment and freight, to CARRIER’s nearest terminal. If OWNER-OPERATOR fails to return CARRIER’s property or freight to CARRIER or remove and return all CARRIER identification from the Equipment upon termination of this Agreement, OWNER-OPERATOR shall pay CARRIER, all collections costs incurred by CARRIER, including reasonable attorney fees, and CARRIER may pursue all other remedies allowed by law or authorized in the Agreement against OWNER-OPERATOR. 3. COMPENSATION. It is expressly understood and agreed that OWNER-OPERATOR’s compensation shall be as set forth in Appendix A, and such compensation shall constitute the total compensation for everything furnished, provided, or done by OWNER-OPERATOR in connection with this Agreement, including driver’s services. Although CARRIER shall use reasonable efforts to make shipments available to OWNER-OPERATOR for transportation during the term of this Agreement, OWNER- OPERATOR acknowledges and agrees that CARRIER does not guarantee any specific number of shipments or amount of revenue to OWNER-OPERATOR during the term of this Agreement. 4. SETTLEMENT PERIOD. At any time during which OWNER-OPERATOR participates in CARRIER’s Administrative Services program as set forth in Section 3(c) to Appendix A, CARRIER shall settle with OWNEROPERATOR with respect to services provided under this Agreement within fifteen (15) calendar days of OWNEROPERATOR’s completion of the services at issue, conditioned upon OWNER-OPERATOR’s submission of properly completed logs if and as required by the U.S. Department of Transportation (“DOT”). If OWNER-OPERATOR does not participate in CARRIER’s Administrative Charge program as set forth in Section 3(c) to Appendix A, CARRIER shall settle with OWNER-OPERATOR with respect to services provided under this Agreement within fifteen (15) calendar days after OWNER-OPERATOR’s submission, in proper form, of those documents necessary for CARRIER to secure payment from its customers, including the signed freight bill, delivery receipt or bill of lading, proof of accessorial services and properly completed logs i f a n d as required by the U.S. Department of Transportation (“DOT”). Upon request of OWNER-OPERATOR, CARRIER shall provide OWNER-OPERATOR with a copy of the documents necessary to calculate the compensation paid to CARRIER by CARRIER’s customers for shipments handled by OWNER-OPERATOR. OWNER-OPERATOR may examine CARRIER’s tariffs, or other contracts or documents, if any, from which charges and rates are computed; provided, however, only that information that would Page 17 of 43 appear on a rated freight bill need be disclosed by CARRIER. CARRIER shall have the right to review all of OWNEROPERATOR’s documents and records relating to the use of the Equipment and the services provided under this Agreement, and OWNER-OPERATOR agrees to provide CARRIER with access to such documents and records upon reasonable notice. OWNER-OPERATOR must give CARRIER written notice of any dispute regarding amounts paid or not paid by CARRIER, which notice must be received by CARRIER within ninety (90) days of payment by CARRIER of the settlement giving rise to the dispute. The written notice must be sent to CARRIER’s Compliance Department at PO Box 290279, Nashville, TN 37229-0279 in order to be effective. FAILURE TO PROVIDE NOTICE AS REQUIRED HEREIN WITHIN THE TIMEFRAME REQUIRED HEREIN WILL RESULT IN WAIVER OF ANY CLAIM OWNER-OPERATOR MAY HAVE WITH RESPECT TO ANY SUCH PAYMENT OR FAILURE TO PAY. With respect to final settlement upon termination of this Agreement, the failure on the part of OWNER-OPERATOR to remove and return to CARRIER all identification devices of CARRIER or a letter certifying their removal shall entitle CARRIER to withhold any payments owed to OWNER-OPERATOR, until such obligation is met. 5. CHARGE BACK. CARRIER shall charge back to OWNER-OPERATOR at the time of payment or settlement, any liability or expense CARRIER has incurred or paid that, under this Agreement or any addendum to this Agreement, OWNER-OPERATOR is obligated to bear. Such expenses shall be deducted from the amount of OWNEROPERATOR’s compensation and shall include those expenses set forth in Appendix A of this Agreement. The amount of each item to be charged back to OWNER- OPERATOR shall be disclosed in Appendix A or elsewhere in this Agreement or any addendum thereto. CARRIER shall provide OWNER-OPERATOR written itemization and documentation of all charge backs where such documentation is necessary to verify the validity of the charge. 6. INSURANCE. The respective obligations of the parties shall be as set forth in Appendix B. CARRIER shall maintain public liability, property damage and cargo insurance in such amounts as are required by the DOT and applicable state regulatory agencies. CARRIER shall maintain insurance coverage for the protection of the public pursuant to 49 U.S.C. § 13906. CARRIER’s possession of legally required insurance shall in no way restrict CARRIER’s right of indemnification from OWNER- OPERATOR as provided under this Agreement. 7. COMPLIANCE WITH PERTINENT LAWS AND REGULATIONS BY OWNER-OPERATOR. (a) Drivers. OWNER-OPERATOR shall provide competent drivers who meet CARRIER’s minimum driver qualification standards and all of the requirements of the DOT, including but not limited to, familiarity and compliance with state and federal motor carrier safety laws and regulations. Where required by law, OWNER-OPERATOR and OWNER-OPERATOR’s drivers shall obtain and maintain commercial driver licenses. Any and all licenses, commercial or otherwise required to perform the services hereunder, must remain valid so long as OWNER-OPERATOR and/or OWNER-OPERATOR’s drivers continue to perform services pursuant to this Agreement. The parties agree that CARRIER shall have the right to disqualify any driver provided by OWNER-OPERATOR in the event that the driver is found to be unsafe, unqualified pursuant to federal or state law, in violation of CARRIER's minimum qualification standards, unprofessional, or in violation of any policies of CARRIER or CARRIER’s customers. Upon a driver’s disqualification by CARRIER, OWNER-OPERATOR shall be obligated to furnish another competent, reliable and qualified driver that meets the minimum qualification standards established by CARRIER. (b) Paperwork Requirements. OWNER-OPERATOR shall submit to CARRIER, on a timely basis, all driver logs and supporting documents (including original toll receipts for CARRIER’s reproduction), physical examination certificates, accident reports, and any other required data, documents or reports. As required by 49 C.F.R. § 376.12(i), CARRIER will keep the original of this Agreement with a copy to be maintained by OWNER-OPERATOR, and a second copy to be carried in the Equipment during the term of this Agreement. (c) Shipping Documents. OWNER-OPERATOR agrees that all bills of lading, waybills, freight bills, manifests, or other papers identifying the property carried on the Equipment shall be those of CARRIER, or as authorized by CARRIER, and shall indicate that the property transported is under the responsibility of CARRIER or a carrier with which the Equipment has been subcontracted. (d) Drug and Alcohol Testing. OWNER-OPERATOR and, in the event OWNER-OPERATOR is not the sole operator of the Equipment, OWNER-OPERATOR’s drivers, shall comply with CARRIER’s Drug and Alcohol Policy, including participation in CARRIER’s random drug and alcohol testing program, and any addendums or revisions thereto. Timing and frequency of screens may vary depending on the customers served by OWNER-OPERATOR. Likewise, OWNER-OPERATOR will submit to a background check as required by various customers of CARRIER. (e) Safe Operations. OWNER-OPERATOR agrees to operate the Equipment in a safe and prudent manner at all times so as to avoid endangering the public, the driver, and/or the property being Page 18 of 43 transported and in accordance with the laws of the various jurisdictions in which the Equipment will be operated and pursuant to the operating authorities of CARRIER, and in accordance with all rules related to traffic safety, highway protection and road requirements. Moreover, OWNER-OPERATOR agrees that all drivers and/or workers employed by OWNER-OPERATOR will comply with the terms of this Agreement, including the requirement of safe operations, while operating the Equipment on behalf of OWNER-OPERATOR. OWNER-OPERATOR agrees that any driver utilized by OWNER-OPERATOR will comply with CARRIER’s policies and procedures and any subsequent revisions thereto, which will be provided by CARRIER. 8. OPERATIONAL EXPENSES. (a) Operating Expenses. OWNER-OPERATOR shall, at its sole cost and expense, provide all the Equipment ready to operate and fully roadworthy, including the necessary licenses, permits, cab cards, state base plates and shall furnish all necessary oil, fuel, tires, and other parts, supplies and equipment necessary or required for the safe and efficient operation and maintenance of the Equipment, including repairs for the operation of such Equipment. OWNER-OPERATOR shall pay all expenses incident to the operation of the Equipment, including, but not limited to, empty mileage, lumper expenses, highway use taxes, weight taxes, state property or indefinite situs taxes, fuel taxes, registration fees, ferry and toll charges, and detention and accessorial charges not collected by CARRIER because of OWNEROPERATOR’s failure to provide the required documentation. (b) Maintenance and Inspection. OWNER-OPERATOR, at its sole cost and expense, shall maintain the Equipment in safe condition and in complete compliance with all laws and regulations of the states in which OWNER-OPERATOR operates and, as applicable, the DOT. In order to ensure compliance with all applicable DOT regulations, OWNER-OPERATOR shall, at its sole cost and expense, make the Equipment available for inspection by CARRIER upon reasonable request by CARRIER. OWNER-OPERATOR shall, at its sole cost and expense, have the Equipment inspected annually, as required by 49 C.F.R. § 396.17, at CARRIER's maintenance facility or at another maintenance facility which CARRIER may, in its sole discretion, authorize. OWNER-OPERATOR shall, as directed by CARRIER, forward to CARRIER all inspection, maintenance and repair records for the Equipment. (c) Fines. OWNER-OPERATOR or its drivers (as professional drivers engaged in a separate and distinct profession) agree to pay all fines, including but not limited to parking and traffic fines and penalties, imposed for violation of any law or regulation by the state or any locality in which OWNER-OPERATOR operates, the DOT, where such violation results, at least partially, from the acts or omissions of OWNEROPERATOR. 9. UNIFORMS. In order to perform the services provided for under this Agreement, it will be necessary for OWNER- OPERATOR to enter upon the premises of customers of CARRIER. In order to gain access to such facilities, help ensure the safety and security of such facilities, CARRIER’s customers may require OWNEROPERATOR to wear a uniform and/or a photo identification badge, which badge may indicate that the OWNEROPERATOR is “leased to” CARRIER, or may otherwise bear CARRIER’s or the customer’s name or logo. Such uniform and/or photo identification badge shall be removed while not performing services pursuant to this Agreement. The OWNER-OPERATOR shall have the option of purchasing shirts or caps with the Express Courier logo on it from CARRIER or from another source. If OWNER-OPERATOR elects to purchase any part of the uniform from CARRIER, OWNER-OPERATOR’s purchases shall be deducted from the OWNER-OPERATOR’s settlement(s). 10. COMMUNICATION EQUIPMENT. Given the time sensitive nature of CARRIER’s business, all OWNEROPERATORS must have a communication device which interface’s with the CARRIER’s operating system. The OWNER-OPERATOR may purchase its own equipment; however, it must be demonstrated to the satisfaction of CARRIER that the device has coverage in the area to be served and provides the functionality needed prior to entering this Agreement. The OWNER-OPERATOR also has the option to rent the equipment from the CARRIER on a weekly basis. The cost (as stated in Appendix A) shall be charged back to OWNER-OPERATOR. 11. CARGO CLAIMS. OWNER-OPERATOR shall immediately report all cargo claims, including all shortages, overages or other exceptions to the cargo, to CARRIER. CARRIER reserves the right to investigate all paid cargo claims, including but not limited to, delays, shortages, mis-deliveries, and claims related to lost, damaged or contaminated loads, arising out of, or in connection with, OWNER-OPERATOR's services to determine if OWNEROPERATOR's actions or omissions resulted in, or contributed to, the cargo claim. If it is determined, in the sole discretion of CARRIER, that OWNER-OPERATOR's actions or omissions resulted in, or contributed to, the cargo claim, then CARRIER shall: a) charge back OWNER-OPERATOR for the first $250 of the cargo claim in the event that OWNER-OPERATOR has elected to participate in CARRIER’s cargo liability limiter program (which election can be made in Appendix A;or, b) charge back to OWNER-OPERATOR the full amount of any such claim in the event OWNER- OPERATOR has not elected not elected to participate in CARRIER’s cargo liability limiter program. Page 19 of 43 Before deducting any cargo claim from OWNER-OPERATOR’s compensation, CARRIER shall provide OWNEROPERATOR with a written explanation and itemization for each such claim. 12. ACCIDENTS AND CLAIMS. OWNER-OPERATOR shall immediately report any accident or potential claim to CARRIER involving operations under this Agreement. OWNER-OPERATOR and its drivers shall cooperate fully with CARRIER with respect to any legal action, regulatory hearing or other similar proceeding arising from the operation of the Equipment, the relationship created by this Agreement or the services performed hereunder. OWNEROPERATOR shall, upon CARRIER’s request and at OWNER-OPERATOR’s sole expense, provide written reports or affidavits, attend hearings and trials and assist in securing evidence or obtaining the attendance of witnesses. OWNER-OPERATOR shall provide CARRIER with any assistance as may be necessary for CARRIER or CARRIER’s representatives or insurers to investigate, settle or litigate any accident, claim or potential claim by or against CARRIER. 13. HOLD HARMLESS. Except to the extent that CARRIER is able to recover for OWNER-OPERATOR’s acts or omissions under the insurance policies maintained by OWNER-OPERATOR hereunder, OWNER-OPERATOR agrees to defend, indemnify and hold harmless CARRIER from any direct, indirect and consequential loss, damage, fine, expense, including reasonable attorney’s fees, action, claim for injury to persons, including death, and damage to property which CARRIER may incur arising out of or in connection with the operation of the Equipment, OWNEROPERATOR’s obligations under this Agreement, or any breach by OWNER-OPERATOR of the terms of this Agreement. This provision shall remain in full force and effect both during and after the termination of this Agreement. The foregoing notwithstanding, in the event that OWNER-OPERATOR participates in CARRIER’s Auto Liability Indemnity program and maintains insurance complying with all requirements of such program as set forth in Appendix B: (i) OWNER- OPERATOR shall have no liability to CARRIER for loss or damage in excess of the full policy limits of OWNER- OPERATOR’s auto liability insurance; and (ii) CARRIER will hold harmless and indemnify OWNEROPERATOR, from any and all claims brought by third parties relating to or arising from any accident actually covered by OWNER-OPERATOR’s automobile liability insurance, including claims by CARRIER’s insurers. 14. CARRIER RESPONSIBILITIES. (a) Exclusive Possession and Responsibility. The Equipment shall be for CARRIER’s exclusive possession, control, and use for the duration of this Agreement. As such, and as required by federal law, the OWNER-OPERATOR shall not operate the Equipment for any other motor carrier without prior written consent from CARRIER. CARRIER shall assume complete responsibility for the operation of the Equipment for the duration of this Agreement. This subparagraph is set forth solely to conform to DOT regulations and shall not be used for any other purposes, including any attempt to classify OWNER-OPERATOR as an employee of CARRIER. Nothing in the provisions required by 49 C.F.R. § 376.12(c)(1) is intended to affect whether OWNER-OPERATOR or its drivers are an independent contractor or an employee of CARRIER. An independent contractor relationship may exist when a carrier complies with 49 U.S.C. § 14102 and attendant administrative requirements. The foregoing notwithstanding, OWNER-OPERATOR may haul on behalf of other motor carriers during the term of this Agreement, provided that OWNER-OPERATOR obtains CARRIER’s written permission to enter into a trip lease, and provided further that OWNER- OPERATOR removes all identification from the Equipment identifying CARRIER prior to beginning operations on behalf of any other carrier. (b) Identification of Equipment. CARRIER shall identify the Equipment in accordance with the requirements of the DOT and appropriate state regulatory agencies. CARRIER shall have the right to place and maintain on the Equipment CARRIER’s name and any lettering, advertisement, slogans or designs as CARRIER may choose. OWNER-OPERATOR shall remove such identification at the termination of this Agreement or while operating such Equipment for any purpose other than conducting CARRIER’s business. At its discretion, OWNER-OPERATOR may have the identification permanently painted on the Equipment. OWNER-OPERATOR further agrees to keep the Equipment in clean appearance and identified as described herein, at its sole cost and expense. CARRIER agrees that OWNER-OPERATOR may display OWNER-OPERATOR’s name and address on the Equipment where required by applicable state law. Page 20 of 43 (c) Owner-Operator Not Employee Of Carrier. It is expressly understood and agreed that OWNEROPERATOR is an independent contractor for the Equipment and driver services provided pursuant to this Agreement. OWNER-OPERATOR shall not be considered, whether under the provisions of this Agreement or otherwise, as having the status of an employee of CARRIER for any purpose whatsoever, including but not limited to, federal, state or local tax purposes, and OWNER-OPERATOR shall not be entitled to participate in any plans, arrangements or distributions the CARRIER may make in connection with any pension, stock, bonus, profit sharing or similar benefits for CARRIER’s employees. Moreover, OWNER-OPERATOR is not covered by unemployment insurance or workers’ compensation provided by CARRIER, and OWNER-OPERATOR has no right to nor will OWNER-OPERATOR seek benefits or any form of payment from or through CARRIER under state unemployment coverage or workers’ compensation. OWNER-OPERATOR agrees to defend, indemnify and hold CARRIER harmless for any claims, suits, or actions, including reasonable attorney’s fees in protecting CARRIER’s interests, brought by employees, any union, the public, or state or federal agencies, arising out of the operation of the Equipment or the providing of driver services under this Agreement. CARRIER is concerned only with the result achieved, and not the method used; therefore, OWNER- OPERATOR is free to select his/her own routes, as well as the sequence of deliveries so long as applicable customer requirements are met. OWNER-OPERATOR has the express right to accept or reject any assignment(s) from CARRIER and may advertise is/her services to other competitive companies. OWNER-OPERATOR also agrees to provide necessary documentation and apply for certification of its independent contractor status where mandated by applicable state law. OWNER- OPERATOR hereby assumes full control and responsibility for the selection, training, hiring, setting of grooming and dress standards, disciplining, discharging, setting of hours, wages and salaries, providing for unemployment insurance, state and federal taxes, fringe benefits, workers’ compensation, adjustment of grievances, all acts and omissions, and all other matters relating to or arising out of OWNER-OPERATOR’s employment or use of drivers and laborers, and any and all other employees or agents of OWNER-OPERATOR that OWNEROPERATOR may provide or use to perform any aspect of this Agreement. OWNER- OPERATOR shall be solely responsible for complying with any and all state and federal laws, rules and regulations that may be applicable to the terms and conditions of employment of OWNER-OPERATOR’s employees or applicants for employment, including, without limitation, compliance with the Federal Fair Credit Reporting Act; verification of immigration and naturalization status; proof of proper taxpayer identification number; proof of highway use tax being currently paid when the OWNER- OPERATOR purchases its license; proof of payment of income; unemployment; Medicare and other state and federal payroll taxes; and, other required withholdings for OWNER-OPERATOR’s employees. OWNER-OPERATOR further expressly acknowledges, understands, and agrees that OWNER-OPERATOR is responsible for the payment of estimated Social Security taxes, along with state and federal income taxes, and that such Social Security tax is higher than the Social Security tax that OWNER-OPERATOR would pay if he or she were an employee of CARRIER, and that the services performed by OWNER- OPERATOR for CARRIER, pursuant to this Agreement, is not work covered by the unemployment laws of any state, including Georgia. OWNER-OPERATOR’s performance of these responsibilities shall be considered proof of its status as an independent contractor in fact. Proof of such control and responsibility shall be submitted by OWNER-OPERATOR to CARRIER as required by CARRIER and may include, but not be limited to, proof of highway use tax being currently paid, proof of income tax being currently paid, and proof of payment of payroll tax for OWNER-OPERATOR’s drivers. For the purposes of this section, the term OWNER-OPERATOR refers to the owner of the Equipment as well as drivers that may be operating the Equipment on behalf of the owner. As required by law, CARRIER agrees to file information tax returns (Form 1099) on behalf of OWNER-OPERATOR if OWNER-OPERATOR is paid more than the statutory amount in compensation during a calendar year. Page 21 of 43 15. BREACH. Notwithstanding anything to the contrary in this Agreement, this Agreement may be terminated, at any time, by either party in the event of a material breach by the other of any term or obligation contained in this Agreement. In the event of a breach and when practicable, written notice shall be served upon the breaching party, notifying such party of the breach and the termination of the Agreement and reason therefore. If, in CARRIER’s judgment, OWNER-OPERATOR has subjected CARRIER to liability because of OWNEROPERATOR’s acts or omissions, CARRIER may take possession of the shipment entrusted to OWNER-OPERATOR and complete performance. In such event, OWNER-OPERATOR shall waive any recourse against CARRIER for such action and OWNER-OPERATOR shall reimburse CARRIER for all direct or indirect costs, expenses, or damages, including attorney’s fees, incurred by CARRIER as a result of CARRIER’s taking possession of the shipment and completing performance. 16. OWNER-OPERATOR NOT REQUIRED TO PURCHASE PRODUCTS, EQUIPMENT, OR SERVICES FROM CARRIER. OWNER-OPERATOR is not required to purchase or rent any products, equipment, or services from CARRIER as a condition of entering into this Agreement. In the event OWNER-OPERATOR elects to purchase or rent equipment from CARRIER or from any third party, for which the purchase or rental contract gives CARRIER the right to make deductions from OWNER- OPERATOR’s settlement, then the parties mutually agree to attach and incorporate each such contract, specifying all terms thereof, to this Agreement as a separate addendum. 17. PASSENGER AUTHORIZATION. In accordance with customer requirements regarding security, OWNER-OPERATOR shall not allow any passengers to ride in the Equipment unless authorized in writing by CARRIER as required by law. Before passenger authorization will be given by CARRIER, OWNER-OPERATOR (or its driver) and the passenger requesting authorization shall submit a fully executed Passenger Authorization and Release of Liability form to CARRIER for prior approval. 18. LOADING AND UNLOADING. In the event the shipper or consignee does not assume loading and unloading responsibilities, OWNER-OPERATOR shall be responsible for the loading or unloading of property transported on behalf of CARRIER at OWNER-OPERATOR’s expense unless otherwise specified in Appendix A. 19. CONFIDENTIALITY. OWNER-OPERATOR hereby recognizes and acknowledges that any list of CARRIER’s customers, as it may exist now or from time to time, is a valuable, special and unique asset of the business of CARRIER. OWNER-OPERATOR agrees, during and after the term of this Agreement, not to disclose the list of CARRIER’s customers or any part thereof to any person, firm, corporation, association, or other entity for any reason or purpose whatsoever without CARRIER’s prior written consent. OWNER-OPERATOR agrees to preserve as “Confidential Matters”, all trade secrets, know how and information relating to CARRIER’s business, forms, processes, developments, sales and promotional systems, prices and operations, which information may be obtained from tariffs, contracts, freight bills, letters, reports, disclosures, reproductions, books, records, or other contractors, and other sources of any kind resulting from this Agreement. OWNER-OPERATOR agrees to regard such Confidential Matters as the sole property of CARRIER, and shall not publish, disclose or disseminate the same to others without the written consent of CARRIER. In the event of any breach or threatened breach by OWNEROPERATOR of the provisions of this paragraph, CARRIER shall be entitled to an injunction, restraining OWNEROPERATOR from disclosing, in whole or in part, the list of CARRIER’s customers, and all other Confidential Matters. OWNER-OPERATOR agrees that CARRIER will be irreparably damaged in the event of any breach of this provision by OWNER-OPERATOR. Accordingly, in addition to any other legal or equitable remedies that may be available to CARRIER, OWNER-OPERATOR agrees that CARRIER will be able to seek and obtain immediate injunctive relief in the form of a temporary restraining order without notice, preliminary injunction, or permanent injunction against OWNER-OPERATOR to enforce this confidentiality provision. CARRIER shall not be required to post any bond or other security and shall not be required to demonstrate any actual injury or damage to obtain injunctive relief from the courts. Nothing hereunder shall be construed as prohibiting CARRIER from pursuing any remedies available to CARRIER at law or in equity for such breach, including the recovery of monetary damages from OWNER- OPERATOR. 20. BENEFIT AND ASSIGNMENT. This Agreement shall be binding upon and inure to the benefit of the parties to this Agreement and their respective successors. OWNER-OPERATOR may not assign or subcontract all or a portion of its obligations to another party without the prior written consent of OWNER-OPERATOR. 21. NOTICE. All notice provisions of this Agreement shall be in writing delivered personally, by postage prepaid, first class mail, or by facsimile machine to the addresses or fax number shown at the end of this Agreement. 22. NON-WAIVER. The failure or refusal of either party to insist upon the strict performance of any provision of this Agreement, or to exercise any right in any one or more instances or circumstances shall not be construed as a waiver or relinquishment of such provision or right, nor shall such failure or refusal be deemed a customary practice contrary to such provision or right. Page 22 of 43 23. SEVERABILITY. If any Agreement or its appendices is deemed invalid for any reason whatsoever, the Agreement shall be void only as to such provision, and this Agreement shall remain otherwise binding between the parties. Any provision voided by operation of the foregoing shall be replaced with provisions which shall be as close as the parties’ original intent as permitted under applicable law. 24. GOVERNING LAW AND CHOICE OF FORUM. This Agreement is to be governed by the laws of the United States and of the State of Tennessee, without regard to any choice of law rules, and CARRIER and OWNER-OPERATOR hereby consent to the jurisdiction of the state and federal courts of Tennessee. 25. COMPLETE AGREEMENT. This Agreement, including any Appendices attached, constitutes the sole, entire, and existing agreement between the parties herein, and supersedes all prior agreements and undertakings, oral and written, expressed or implied, or practices, between the parties, and expresses all obligations and restrictions imposed on each of the respective parties during its term, except those specifically modified or changed by mutual written agreement between CARRIER and OWNER-OPERATOR. IN WITNESS WHEREOF, CARRIER and OWNER-OPERATOR hereby sign this Agreement as of the date stated above. CARRIER: Express Courier International, Inc. Owner-Operator Address: 238 Bedford Way Address: Franklin City TN State 37064 Zip City Fax: Fax: By: Phone: State Zip Cell Phone: Printed Name Email: FEIN or SSN: By: Printed Name: Page 23 of 43 RECEIPT FOR AVAILABILITY OF CONTRACTED VEHICLE(S) Contracted from OWNER-OPERATOR the vehicle or vehicles described in this Agreement. Equipment inspected at 20 at : o’clock By: .M. on _, (CARRIER Representative) Printed Name Page 24 of 43 Appendix A OWNER-OPERATOR’s Compensation (Percentage of Revenue) 1. SHARE OF REVENUE. Unless otherwise agreed to in writing between the parties, CARRIER shall pay OWNEROPERATOR a share of the revenue which will be based upon the vehicle size used with exceptions as noted: 2. a) For hauling of loads tendered by CARRIER: The percentage of Adjusted Gross Revenue set forth in the Commission Percentage Table attached hereto as Appendix C shall by paid for pickups and deliveries accomplished by OWNER-OPERATOR with Equipment pursuant to this Agreement. b) The foregoing notwithstanding, the Parties understand and agree that in certain circumstances CARRIER may enter into special pricing arrangements with its customers pursuant to which it would be inequitable between the Parties to pay OWNER-OPERATOR the rates contained in Appendix C. In those situations, CARRIER and OWNER-OPERATOR will enter into a signed Settlement Addendum prior to dispatch of the relevant movement that will govern the rate to be paid for the moves referenced in such Settlement Addendum. Any such Settlement Addendum shall be considered a part of this Agreement and shall continue in effect for all loads between the points stated therein unless revised in writing by a subsequent Settlement Addendum or terminated by written agreement of the Parties. c) Adjusted Gross Revenue. AGR shall mean all revenue received by CARRIER from the shippers, consignees, or other carriers for commodities hauled by OWNER-OPERATOR under this Agreement, including fuel-related or other surcharges, reduced by: (1) any and all expenses attributed to accessorial services paid to a third party or to OWNER-OPERATOR by CARRIER; (b) the amount paid to any third party by CARRIER in relation to movement of the load, including without limitation, amounts paid to other contractors as a pro-rata payment for their participation in the movement of a load; (c) any amount paid by CARRIER to interline or augmenting carriers; (d) any warehouse or storage charges; (e) any revenue received by CARRIER as an excess value or insurance charge on high value shipments; (f) all incentives, discounts or commissions given to CARRIER’s customers or other third parties. d) Fuel Surcharges. CARRIER shall pay OWNER-OPERATOR fuel surcharges listed in the CARRIER’S “Fuel Surcharge Program” which is hereby incorporated by reference as an addendum to this Agreement e) Accessorial Service Charges. OWNER-OPERATOR shall be paid a percentage of all delivery related expenses and collected accessorial service charges, including detention, loading/unloading, equipment order not used, reconsignment and diversion, repositioning, layover, and stop-off charges. The payment percent will be based on the current Commission Percentage Table for vehicle sizes as set forth in Appendix C. PAY-CARD. Payment from CARRIER to OWNER-OPERATOR will be made via a Pay-Card whereby payment is “loaded” onto a pay-card issued to OWNER-OPERATOR by a third party vendor (“Vendor”). Use of the Pay-Card to receive payment is mandatory and by entering into this Agreement, OWNER-OPERATOR consents to receiving payments via the Pay-Card issued by the Vendor. There are fees related to the use of the Pay-Card, but those fees are neither paid nor owed to CARRIER. The Vendor offers one free transaction immediately following loading of a payment onto the Pay-Card, and OWNER-OPERATOR can take advantage of the free transaction in order to transfer funds from the card to a traditional bank account in order to avoid paying additional fees to the Vendor. Vendor requires that OWNER-OPERATOR sign a Pay-Card Consent Form, and may also require that OWNER-OPERATOR sign a Cardholder Agreement. Page 25 of 43 3. CHARGE BACK ITEMS. The following items shall be charged back and deducted from OWNER-OPERATOR’s compensation: a) Fixed Chargebacks. ONE TIME CHARGE BACK ITEMS AS NEEDED OR REQUESTED Identification Badge (All OWNER-OPERATORs are responsible for obtaining at least one badge from CARRIER or an alternative source. OWNER-OPERATORs electing the administrative charge below are entitled to replacement badges at no additional cost.) COST $6.50 (per badge) C.O.D. Charges (Customer payments collected and retained by OWNER-OPERATOR) Fines and Penalties Uniforms (Initial if Electing ) Actual Actual Actual Blood Spill Clean-Up Kits Actual Coolers Actual Handy Map Actual Cargo Claim (if OWNER-OPERATOR does not participate in cargo liability limiter program) Actual Cargo Claim (if OWNER-OPERATOR participates in CARRIER’s cargo liability limiter program) First $250 OWNER-OPERATOR agrees that CARRIER may charge back to OWNER-OPERATOR any other expenses or cost incurred by CARRIER for which OWNER-OPERATOR is responsible for under this Agreement or as otherwise agreed to by the parties. OWNER-OPERATOR hereby waives any objection to any charge back item unless OWNER-OPERATOR notifies CARRIER of OWNEROPERATOR’s disagreement with such charge back within thirty (30) days of the charge back. b) Tiered Chargebacks. The following items will likewise be charged back each week, with the amount of the chargeback determined by the OWNER-OPERATOR’s average weekly gross commission in the month preceding such chargeback. As such, at the beginning of the month, OWNER-OPERATOR will be assigned to a tier, based on the process set forth herein, and any chargebacks from the chart below made during such month will be for the amount set forth in the applicable tier. For purposes of determining the average weekly gross commission for the preceding month, CARRIER will add the total gross commission (i.e., pre-chargeback commission) of the OWNER-OPERATOR for all payments made by CARRIER during the preceding calendar month, and divide that total by the number of payments made by CARRIER during the preceding calendar month. That total will be compared against the chart below to determine the applicable tier. For new OWNER-OPERATORs for which there is no established payment history, CARRIER will, in its sole discretion, assign the OWNER-OPERATOR to a tier during OWNEROPERATOR’s first month of operation. If, after the first calendar month of operation (whether a partial or full month), it turns out the OWNER-OPERATOR was assigned to the wrong tier, CARRIER shall pay a refund any overpayment, or OWNER-OPERATOR will reimburse CARRIER for any underpayment, as applicable. Page 26 of 43 Item Tier 1 Tier 2 Tier 3 Tier 4 Occupational Accident Insurance $1,000,000 Coverage (See Appendix B for details and to elect) $14.50 $27.50 $27.50 $27.50 Cargo Liability Limiter Program Per Driver (See Appendix B for details) (Initial if Electing ) $4.00 $4.50 $5.00 $5.50 Auto Liability Indemnity Per Driver (See Appendix B for details) (Initial if Electing ) $4.50 $5.00 $6.50 $7.00 $5.50 $17.00 $21.00 $24.00 $3.50 $5.00 $5.00 $5.00 $13.50 $19.00 $19.00 $19.00 3.25% of gross weekly compensation 3.25% of gross weekly compensation 2.00% of gross weekly compensation 1.15% of gross weekly compensation Scanner (Initial if Electing Per Unit Pager (Initial if Electing Per Unit Nextel (Initial if Electing Per Unit Administrative Services (Initial if Electing )* ) _) ) *Maximum Charge is $45.00 per week. Tier Average Gross Commission (per week) Range 1 $0.00-$249.99 2 $250.00-$499.99 3 $500.00-$799.99 4 $800.00 and up c) Administrative Services. OWNER-OPERATOR has the option, by electing above, of receiving certain administrative services from CARRIER. Those services include provision of manifests, facilitation of drug screens, facilitation of customer and/or government required background checks, obtaining an annual motor vehicle report (“MVR”) in accordance with customer requirements, facilitation of customer required training (e.g., biohazard and HIPPA), facilitating procurement of TSA required threat assessments, route optimization, and ID badges. At any time during which OWNER-OPERATOR participates in this Administrative Services program, CARRIER shall settle with OWNER-OPERATOR with respect to services provided under this Agreement within fifteen (15) calendar days of OWNER-OPERATOR’s completion of the services at issue, conditioned upon OWNER-OPERATOR’s submission of properly completed logs if and as required by the U.S. Department of Transportation (“DOT”). If OWNEROPERATOR does not participate in CARRIER’s Administrative Charge program CARRIER shall settle with OWNER-OPERATOR with respect to services provided under this Agreement within fifteen (15) calendar days after OWNER-OPERATOR’s submission, in proper form, of those documents necessary for CARRIER to secure payment from its customers, including the signed freight bill, delivery receipt or bill of lading, proof of accessorial services and properly completed logs as required by the U.S. Department of Transportation (“DOT”). The provisions of this Section shall govern in the event of any inconsistency or dispute with the provisions of the Agreement governing settlement period. If OWNER-OPERATOR is not electing to receive Administrative Services from CARRIER, then OWNER-OPERATOR is responsible for the following: Page 27 of 43 i. ii. iii. iv. v. vi. vii. OWNER-OPERATOR must supply route sheets and manifests in order to document daily pick-ups and deliveries as required by CARRIER’s customers. OWNER-OPERATOR must ensure that it and all of its drivers submit to a drug screen (at least 10 panels) from a vendor approved by CARRIER and provide the results to CARRIER. This 10 panel minimum screen is in addition to, and not a substitute for, any drug screen required by applicable motor carrier safety regulations (which require screening of drivers holding commercial driver licenses). OWNER-OPERATOR must provide, annually, a criminal background check of state, federal, and local databases going back at least 10 years. OWNER-OPERATOR must provide an annual MVR that is not more than a month old and that includes a minimum years of history. In addition to this OWNER-OPERATOR must provide additional MVR as required.(Customer, vendor or safety requirement applies here.) OWNER-OPERATOR must obtain training with respect to HIPPA and Biohazard training from customer approved sources, and provide proof of acceptable completion of such training to CARRIER. OWNER-OPERATOR must obtain either a Transportation Worker Identification Credential (“TWIC”), Hazardous Material Endorsement to a commercial driver license, or other TSA-approval alternative Security Threat Assessment (“STA”) credential and provide proof of such credential to CARRIER. OWNER-OPERATOR must route its own stops. The undersigned parties agree to THIS APPENDIX as the latest date set forth below. CARRIER: OWNER-OPERATOR: By: By: Printed Name Printed Name Date: Date: Page 28 of 43 Appendix B INSURANCE It shall be CARRIER’s responsibility, pursuant to federal and state law, to provide public liability and property damage insurance for the Equipment at all times while the Equipment is being operated on behalf of CARRIER. However, CARRIER’s possession of such insurance shall in no way affect CARRIER’s rights of indemnification against OWNER-OPERATOR as provided for in this Agreement. OWNER-OPERATOR shall maintain, at its sole cost and expense, the following minimum insurance coverages in support of its indemnity of CARRIER during the term of this Agreement and, if applicable, pay CARRIER to assume its liability under the parameters as set forth in paragraph 1(a) and (b). below. 1. AUTO LIABILITY. a. OWNER-OPERATOR shall procure, carry and maintain auto liability insurance, which shall provide coverage to OWNER-OPERATOR for bodily injury or death to any person in a minimum amount of $100,000 or $300,000 minimum for any single occurrence or for damages to property in any single occurrence of $100,000 or a combined single limit of no less than $300,000. Although CARRIER shall have primary responsibility to provide insurance for the protection of the public, OWNER-OPERATOR’s coverage shall be primary vis-à-vis CARRIER and shall show CARRIER as an additional insured of such coverage. OWNER-OPERATOR’s policy shall not contain any policy exclusions reasonably likely to exclude coverage for OWNER-OPERATOR’s operations pursuant to this Agreement, including, but not limited to, exclusions for business use. b. OWNER-OPERATOR shall also pay, via settlement deduction, for participation in CARRIER’s Auto Liability Indemnity (“ALI”) program. This charge shall be for limitation of damages that OWNEROPERATOR may otherwise be responsible to CARRIER for in excess of the coverage otherwise payable under OWNER-OPERATOR’s above-described auto liability insurance coverage. Charges for the ALI program are set forth in Appendix A. c. As an alternative to providing a certificate of auto liability insurance evidencing the coverage set forth in section (a) above, and participation in the ALI program, OWNER-OPERATOR may provide CARRIER a certificate of insurance evidencing commercial auto liability coverage in the amount of $1,000,000 combined single limit, showing CARRIER as an additional insured of such coverage. Although CARRIER shall have primary responsibility to provide insurance for the protection of the public, OWNEROPERATOR’s coverage shall be primary vis-à-vis CARRIER. 2. WORKERS’ COMPENSATION/OCCUPATIONAL ACCIDENT INSURANCE. OWNER-OPERATOR shall provide workers’ compensation insurance coverage for all its employees, agents and anyone driving the Equipment in amount not less than statutory limits required by applicable state law. Other than in the state of CA, CO, MA, NC, NJ, NV, or NY, if OWNER-OPERATOR is the sole owner and the sole and exclusive operator of the vehicle that is driven exclusively by OWNER-OPERATOR under this Agreement, then OWNER-OPERATOR may, as an alternative to obtaining workers’ compensation coverage, obtain an occupational accident insurance policy that is acceptable to CARRIER or participate in an occupational accident program facilitated by CARRIER for a weekly charge, per driver, as set forth in Appendix A. If OWNER-OPERATOR is otherwise is entitled to obtain and rely upon occupational accident coverage as set forth above, OWNER-OPERATOR must obtain a policy with limits of at least $1,000,000. If OWNER-OPERATOR is based and/or resides in North Carolina, and if CARRIER consents, OWNER-OPERATOR can elect to be covered by CARRIER’s workers’ compensation insurance coverage, the mutually agreed cost of which will be charged back to OWNER-OPERATOR. 3. CARGO INSURANCE. In addition to the insurance coverages required under this Agreement, it is OWNEROPERATOR’s responsibility to procure cargo insurance in amounts acceptable to CARRIER (no less than $100,000 per vehicle with a deductible amount no greater than $250 per vehicle) or participate in CARRIER’s cargo liability limiter program for a charge as set forth in Appendix A, pursuant to which OWNER-OPERATOR’s cargo liability to CARRIER is limited to the first $250 per claim. Page 29 of 43 4. ACCEPTABILITY OF COVERAGE. OWNER-OPERATOR shall furnish to CARRIER written certificates obtained from OWNER-OPERATOR’s insurance carrier showing that all insurance coverages required above have been procured from and A.M. Best “B” rated company, are being properly maintained, and the premiums therefore are paid, specifying the name of the insurance carrier, the policy number, the expiration date, naming CARRIER as an additional insured (or for cargo coverage - loss payee), and further showing that written notice of cancellation or modification of the policy shall be given to CARRIER at least thirty (30) days prior to such cancellation or modification. OWNER-OPERATOR agrees to defend, indemnify and hold harmless CARRIER from any direct, indirect and consequential loss, damage, fine, expense, including reasonable attorney fees, actions, claim for injury to persons, including death, and damage to property which CARRIER may incur arising out of or in connection with, OWNER-OPERATOR’s failure to maintain the insurance coverages required by this Agreement. In addition, OWNER-OPERATOR, on behalf of its insurer, expressly waives all subrogation rights against CARRIER, and, in the event of a subrogation action brought by OWNER-OPERATOR’s insurer, OWNEROPERATOR agrees to defend, indemnify and hold harmless CARRIER from such claim. OWNER-OPERATOR may, at OWNER-OPERATOR’s notion, authorize CARRIER to facilitate, on OWNER-OPERATOR’s behalf, the payment of insurance coverages via coverages pre-approved by CARRIER in accordance with the requirements of this Agreement. OWNER-OPERATOR will be charged back for all CARRIER’s expense and cost of such facilitation. In addition, upon failure herein, CARRIER is authorized but not required to obtain such insurance at its expense and charge OWNER-OPERATOR all cost incurred by CARRIER in obtaining and facilitating payment for such coverage on OWNER-OPERATOR’s behalf. OWNER-OPERATOR recognizes that CARRIER is not in the business of providing or selling insurance, and any insurance coverage requested by OWNER-OPERATOR from CARRIER is subject to all of the terms, conditions and exclusions of the actual policy issued by the insurance underwriter. For policy(s) facilitated by CARRIER, CARRIER shall ensure that OWNER-OPERATOR is provided with a certificate of insurance (showing the name of the insurer, the cost of insurance, the deductibles (if any), the policy number, the type of insurance, and the effective dates of the insurance) for each insurance policy under which the OWNER-OPERATOR selects coverage from the insurance underwriter, and CARRIER shall provide OWNER-OPERATOR with a copy of each policy upon request by OWNER-OPERATOR. CARRIER: EXPRESS COURIER INTERNATIONAL, INC. OWNER-OPERATOR: By: By: Printed Name Printed Name Fax: Title Fax: Address: Address: 238 Bedford Way City: City: Franklin State: TN Zip: 37064 State: Zip: Phone: Cell Phone: FEIN or SSN: Email: Page 30 of 43 COVERAGE ADMINISTERED BY ECI BY DEDUCTION OWNER-OPERATOR hereby requests CARRIER, through the insurance broker with pre-approved insurance programs, to obtain for OWNER-OPERATOR the insurance coverages marked with OWNER-OPERATOR’s initials below. In the event OWNEROPERATOR elects such coverage, the following shall be considered the certificate of insurance which CARRIER is obligated to provide to OWNER-OPERATOR. Workers’ Compensation: [or occupational accident if OWNER-OPERATOR is sole owner and operator of the vehicle] Insurance Co.: Policy No.: Coverage Dates: Amount of Coverage: $_ Current Cost to OWNER-OPERATOR: $ per unit of Equipment per month Deductible for which OWNER-OPERATOR is liable: $ per occurrence Occupational Accident Coverage: Insurance Co.: Policy No.: Coverage Dates: Amount of Coverage: $_ Current Cost to OWNER-OPERATOR: $ per unit of Equipment per month Deductible for which OWNER-OPERATOR is liable: $ per occurrence Minimum Coverage: Statutory [Minimum coverage for occupational accident based on CARRIER facilitated program as minimum benefit limits] Owner-Operator’s Signature Print Name Date Page 31 of 43 Appendix C COMMISSION PERCENTAGE TABLE 70% of AGR 14ft or Larger Box Truck 65% of AGR Extended Cargo Vans (2-3 ft extensions) 60% of AGR Cargo Vans and Covered Full-Size Pickup Trucks (must hold two 4’x4’x4’ skids or equivalent) 55% of AGR Minivans or Covered Small Pickup Trucks 50% of AGR Cars 45% of AGR Pickup Trucks without Topper - (contractors have 30 days to secure a Topper) Page 32 of 43 Hepatitis B Vaccine Notice Form Facility Location: I understand that due to my occupational exposure to blood or other potentially infectious materials (OPIM), I may be at risk of acquiring hepatitis B virus (HBV) infection. I understand that without the vaccine, I am at risk of acquiring hepatitis B, a serous disease. I understand that as an owner operator it is my responsibility to pay the cost of the vaccination. By signing below, I acknowledge my receipt and review of this notice. Owner Operator’s Name (Print) Owner Operator’s Signature Date Page 33 of 43 Web Training Instructions Instructions for viewing the HighQ online training seminar Medical Courier Training are listed below. This is an audio and video program that you must follow along with the training manual. Begin by clicking on the link below: https://www.323.livemeeting.com/cc/highqllc/view • • • Your Name: Recording ID: Recording Key: 1. 2. 3. 4. Your full name dotc bbp Click on View Recording. Type in your email address and the name of your company. Once again click on View Recording. There will be two formats to choose from. Click on View beside Microsoft Live Office Replay. (Note: You will need to use Microsoft Internet Explorer for your browser. Some browsers do not support these programs.) This will take you through the seminar letting you stop, pause and replay if necessary. At the end of the training the HighQ testing page will appear on your screen. If you are not taken directly to this testing page, please contact us at start@highqllc.com. You can also log on directly to the test at http://www.highqllc.com/QuizMed.html. Upon completion of your quiz, type in your full name and company then click Send. It is recommended that you print a copy of your quiz results for your own records. If your results don’t email properly, you can fax them to HighQ Training at 1-888-371-0863. Keep your certificate of completion for your permanent records. If you have any questions or problems logging on, please email HighQ Training at start@highqllc.com or call 724-749-4710, extension #4. Thank you, HighQ Training Page 34 of 43 INDEPENDENT CONTRACTOR OCCUPATIONAL ACCIDENT ENROLLMENT FORM Express Courier International, Inc. INSURED PERSON INFORMATION: Last Name CERTIFICATION First Name M.I. Street City State Zip Contact Telephone Number(s) Date of Birth Social Security Number Email address Beneficiary Last Name First Name M.I. Beneficiary Address or Relationship Check box to have death benefits paid to my Estate Start Date Check One: Full time: Driver Number or Part time: Location/Terminal: Gallagher Transportation Services I certify that all information in this Enrollment Form and other enrollment documents is true and correct to the best of my knowledge. I hereby request occupational accident coverage under the insurance program (“Occupational Accident Program”) developed by Gallagher Transportation Services (“Gallagher”). I verify that I am the independent contractor/driver named on this Enrollment Form who is under contract to the facilitating motor carrier on the date of this Enrollment Form. I verify that I am also an independent contractor/driver under contract to the facilitating motor carrier and understand that I am covered only while under contract with the facilitating motor carrier. I have designated the noted beneficiary in the event of my death. I certify that I am under the age of 75 as of the date set forth below my signature. I understand and acknowledge that Arthur J. Gallagher Risk Management Services, Inc. (“AJG”) is the insurance agent with limited authority to procure the insurance coverage referenced in this Enrollment Form. I also acknowledge that I have not sought or received insurance advice from Gallagher or AJG on the referenced insurance coverage as it applies to me and/or my business needs. I further understand and acknowledge that compensation for the services described above is part of the cost of the insurance coverage and not separately charged to me. In accordance with my independent contractor operating agreement, and as an addendum thereto, I authorize the facilitating motor carrier to periodically deduct my insurance costs. If such settlements (or other monies due me) are not sufficient to cover the insurance costs, I will remit by certified check or money order the outstanding insurance cost to Gallagher Transportation Services, 2345 Grand Boulevard, Suite 400, Kansas City, MO 64108 within a ten (10) day period. Otherwise, I understand the insurance underwriters may cancel this insurance coverage in accordance with policy terms and conditions. I also understand coverage will not automatically be reinstated if cancellation is processed. I have read, understand and agree to the terms and conditions on the reverse side of this Enrollment Form. I agree that a photographic, facsimile or electronically signed copy of the authorization is as valid as the original. By signing below, I acknowledge that I may receive my Occupational Accident Confirmation of Coverage electronically in lieu of it being mailed to my residence. If I would prefer to receive a paper copy, I will contact Gallagher Transportation Services at 800.279.7500 and request a copy. Arthur J. Gallagher Risk Management Services, Inc. Administrative Office: 2345 Grand Blvd., Suite 400 Kansas City, MO 64108 (800) 279-7500 (816) 329-0891 (Fax) Occ.Acc Enrollment Form Edition 01.01.2011-Electronic Transportationword/PolicyForms/T4OccAccEnrollmentFormElectronic01.10.2011.doc Signed: Date: Page 1 of 2 TERMS AND CONDITIONS - Please read carefully It is further understood and agreed: 1. Not Statutory Workers’ Compensation & Employers’ Liability: This coverage is NOT a statutory Workers’ Compensation and Employers’ Liability policy, and the benefits under this coverage do not necessarily equal the benefits which an individual might be eligible for under statutory Workers’ Compensation. However, you agree that in the event of an occupational accident, you will look to the occupational accident coverage described herein in lieu of seeking Workers’ Compensation coverage. 2. Assignment of Benefits: In the event benefits are paid from the statutory Workers’ Compensation and Employers’ Liability Policy of the facilitating motor carrier or any similar policy becomes liable for such benefits, the benefits which an Insured Person is entitled to under this policy will be automatically assigned to the facilitating motor carrier. In such event, you agree to the immediate assignment to the facilitating motor carrier of all benefits which you receive or would otherwise be payable to you or any third party under the Occupational Accident Program. 3. Cost and Consent to Cost Change: You understand that the insurance cost shown may include taxes, fees and administrative expenses which you accept and acknowledge as part of the insurance cost. The insurance underwriters reserve the right to change the rate by giving written notice to you. 4. Evidence of Coverage: Your state of principal operations could require you to purchase Statutory Workers’ Compensation, otherwise, the facilitating motor carrier will accept coverage under the Occupational Accident Program. If you do not participate in the Occupational Accident Program, you are required to have on file a certificate of insurance for Statutory Workers’ Compensation or when allowed by law, an Occupational Accident Certificate. Your insurance agent should provide this information to the facilitating motor carrier. You will be enrolled in the facilitated occupational accident program until you provide proof of appropriate coverage. At that time you will receive an adjustment in any costs charged to you. 5. Termination: In the event your independent contractor operating agreement with the facilitating motor carrier is terminated for any reason by either party, the occupational accident coverage will be cancelled effective the date of the contract termination or the earliest date thereafter allowed by law. You should make arrangements to replace coverage immediately. 6. Terms & Conditions: Coverage will be subject to all policy terms, conditions and exclusions as detailed in the Evidence of Insurance. The Insured Person must be under age 75 to enroll in the Occupational Accident Program. 7. Authorization of Settlement Deduction: You authorize the facilitating motor carrier to deduct from your settlement checks, funds, accruals or other compensation, on a periodic basis (e.g. weekly or monthly) in amounts sufficient to pay the insurance costs and hereby instruct it to forward such funds to Gallagher by the 15th of each month. Your cost (as described in “Cost and Consent to Cost Change”) will be deducted from your settlement check. If your settlement check is not enough to cover your insurance cost, you will be asked to forward a check or money order made payable to Gallagher Transportation Services, 2345 Grand Boulevard, Suite 400, Kansas City, MO 64108 immediately, or the coverage will be cancelled, in accordance with policy terms and conditions. 8. Effective Date: Coverage shall become effective on the date your Enrollment Form is accepted by Gallagher. PLEASE READ ALL INFORMATION CAREFULLY BEFORE SIGNING THE APPLICATION ON THE REVERSE SIDE Gallagher Transportation Services Arthur J. Gallagher & Co. Risk Management Services, Inc. Administrative Office: 2345 Grand Blvd., Suite 400 Kansas City, MO 64108 (800) 279-7500 (816) 329-0891 (Fax) Please fax all applications to Gallagher Transportation at (816) 329-0891 Occ.Acc Enrollment Form Edition 01.01.2011 Transportationword/PolicyForms/T4OccAccEnrollmentFormElectronic01.10.2011.doc Page 2 of 2 PAY CARD CONSENT FORM Please complete the following consent Form to sign up for your Pay Card account. Print Name: ______________________ __________________________ __________________________ First Middle Last Home Address: ________________________ ________________________ __________ ___________________ Street City State Zip Code The fees listed below will be deducted from your Pay Card balance for each transaction after your first transaction each settlement load. You may withdraw your pay in full by going to a teller at a participating bank for a cash disbursement. If it is your first transaction after your pay has been loaded to your Card, then the following fees will not apply. TRANSACTION TYPE Cash Disbursement at Teller at Participating Banks Cash Disbursement - Domestic Cash Disbursement – International ATM ATM Withdrawal - Domestic ATM Withdrawal – International ATM Decline Fee - Domestic ATM Decline Fee – International ATM Balance Inquiry - Domestic ATM Balance Inquiry - International POS POS Purchase – Domestic POS Purchase - International POS Purchase with Cashback - Domestic POS Purchase with Cashback – International POS Balance Inquiry - Domestic POS Balance Inquiry - International POS Refund - Domestic POS Refund - International POS Decline Fee - Domestic POS Decline Fee - International OTHER Direct Deposit - Automatic $0.50 Direct Deposit - Manual $0.75 Comchek Draft Fee $3.00 Invalid Claim Fee $50.00 Replacement Card Fee $2.00 Text Messaging (service available soon) $N/A Using PIN Signing $N/A $N/A $5.00 $8.00 $1.75 $5.00 $1.75 $5.00 $1.75 $5.00 N/A N/A N/A N/A N/A N/A $0.50 $5.00 $0.50 $5.00 $0.50 $5.00 $0.50 $5.00 $0.50 $5.00 $0.00 $0.00 N/A N/A N/A N/A $0.00 $0.00 $0.00 $0.00 Comdata will notify you of any changes in these Comdata Fees. ATM owners outside of Comdata’s surcharge free ATM n etwork and other place s where you use your Card may charge fees (even for a balance inquiry without completing a funds tra nsfer) that will be ded ucted from your Card balance. Page 37 of 43 If you use your Card ou tside the United States, or if you obtain funds (or make a purchase) in a currency other than US Dollars (the currency in which your Card is issued), then the a mount deducted from your funds will be converted into US Dollars by the card network. The card network will charge a Cross-Border Fee of 0.8% and Currency Conversion Fee of 0.2 % (for a tot al fee of 1 % of the tra nsaction amount) to be included in the transaction am ount. This card network cross border and currency conversion charge is independent of and in addition to any international fee indicated in the Comdata Fees above. You will not earn interest on your funds. BY SIGNING BEL OW, I CONSENT TO RECEIVE MY COMMISSIONS BY ELECTRONIC TRANSFER TO MY PAY CARD. I ACKNOWLEDGE THAT I HAVE RECEIVED A COPY OF THE CARDHOLDER AGREEMENT, AND I HAVE READ, UNDERSTAND AND A GREE TO ALL OF T HE TERMS IN T HE CARDHOLDER AGREEMENT. I ALS O UNDERSTAND AND AGREE TO THE FEES THAT I WILL INCUR USING THE PAY CARD. Print Name: Sign Name: Contractor Number: Date: Page 38 of 43 W-9 Request for Taxpayer Identification Number and Certification Form (Rev. October 2007) Print or type See Specific Instructions on page 2. Department of the Treasury Internal Revenue Service Give form to the requester. Do not send to the IRS. Name (as shown on your income tax return) Business name, if different from above Check appropriate box: Individual/Sole proprietor Corporation Partnership Limited liability company. Enter the tax classification (D=disregarded entity, C=corporation, P=partnership) Other (see instructions) � Address (number, street, and apt. or suite no.) � Exempt payee Requester’s name and address (optional) City, state, and ZIP code List account number(s) here (optional) Part I Taxpayer Identification Number (TIN) Enter your TIN in the appropriate box. The TIN provided must match the name given on Line 1 to avoid backup withholding. For individuals, this is your social security number (SSN). However, for a resident alien, sole proprietor, or disregarded entity, see the Part I instructions on page 3. For other entities, it is your employer identification number (EIN). If you do not have a number, see How to get a TIN on page 3. Social security number Note. If the account is in more than one name, see the chart on page 4 for guidelines on whose number to enter. Employer identification number Part II or Certification Under penalties of perjury, I certify that: 1. The number shown on this form is my correct taxpayer identification number (or I am waiting for a number to be issued to me), and 2. I am not subject to backup withholding because: (a) I am exempt from backup withholding, or (b) I have not been notified by the Internal Revenue Service (IRS) that I am subject to backup withholding as a result of a failure to report all interest or dividends, or (c) the IRS has notified me that I am no longer subject to backup withholding, and 3. I am a U.S. citizen or other U.S. person (defined below). Certification instructions. You must cross out item 2 above if you have been notified by the IRS that you are currently subject to backup withholding because you have failed to report all interest and dividends on your tax return. For real estate transactions, item 2 does not apply. For mortgage interest paid, acquisition or abandonment of secured property, cancellation of debt, contributions to an individual retirement arrangement (IRA), and generally, payments other than interest and dividends, you are not required to sign the Certification, but you must provide your correct TIN. See the instructions on page 4. Sign Here Signature of U.S. person � Date � General Instructions Section references are to the Internal Revenue Code unless otherwise noted. Purpose of Form A person who is required to file an information return with the IRS must obtain your correct taxpayer identification number (TIN) to report, for example, income paid to you, real estate transactions, mortgage interest you paid, acquisition or abandonment of secured property, cancellation of debt, or contributions you made to an IRA. Use Form W-9 only if you are a U.S. person (including a resident alien), to provide your correct TIN to the person requesting it (the requester) and, when applicable, to: 1. Certify that the TIN you are giving is correct (or you are waiting for a number to be issued), 2. Certify that you are not subject to backup withholding, or 3. Claim exemption from backup withholding if you are a U.S. exempt payee. If applicable, you are also certifying that as a U.S. person, your allocable share of any partnership income from a U.S. trade or business is not subject to the withholding tax on foreign partners’ share of effectively connected income. Note. If a requester gives you a form other than Form W-9 to request your TIN, you must use the requester’s form if it is substantially similar to this Form W-9. Definition of a U.S. person. For federal tax purposes, you are considered a U.S. person if you are: ● An individual who is a U.S. citizen or U.S. resident alien, ● A partnership, corporation, company, or association created or organized in the United States or under the laws of the United States, ● An estate (other than a foreign estate), or ● A domestic trust (as defined in Regulations section 301.7701-7). Special rules for partnerships. Partnerships that conduct a trade or business in the United States are generally required to pay a withholding tax on any foreign partners’ share of income from such business. Further, in certain cases where a Form W-9 has not been received, a partnership is required to presume that a partner is a foreign person, and pay the withholding tax. Therefore, if you are a U.S. person that is a partner in a partnership conducting a trade or business in the United States, provide Form W-9 to the partnership to establish your U.S. status and avoid withholding on your share of partnership income. The person who gives Form W-9 to the partnership for purposes of establishing its U.S. status and avoiding withholding on its allocable share of net income from the partnership conducting a trade or business in the United States is in the following cases: ● The U.S. owner of a disregarded entity and not the entity, Cat. No. 10231X Form W-9 (Rev. 10-2007) Page 39 of 43 Form W-9 (Rev. 10-2007) ● The U.S. grantor or other owner of a grantor trust and not the trust, and ● The U.S. trust (other than a grantor trust) and not the beneficiaries of the trust. Foreign person. If you are a foreign person, do not use Form W-9. Instead, use the appropriate Form W-8 (see Publication 515, Withholding of Tax on Nonresident Aliens and Foreign Entities). Nonresident alien who becomes a resident alien. Generally, only a nonresident alien individual may use the terms of a tax treaty to reduce or eliminate U.S. tax on certain types of income. However, most tax treaties contain a provision known as a “saving clause.” Exceptions specified in the saving clause may permit an exemption from tax to continue for certain types of income even after the payee has otherwise become a U.S. resident alien for tax purposes. If you are a U.S. resident alien who is relying on an exception contained in the saving clause of a tax treaty to claim an exemption from U.S. tax on certain types of income, you must attach a statement to Form W-9 that specifies the following five items: 1. The treaty country. Generally, this must be the same treaty under which you claimed exemption from tax as a nonresident alien. 2. The treaty article addressing the income. 3. The article number (or location) in the tax treaty that contains the saving clause and its exceptions. 4. The type and amount of income that qualifies for the exemption from tax. 5. Sufficient facts to justify the exemption from tax under the terms of the treaty article. Example. Article 20 of the U.S.-China income tax treaty allows an exemption from tax for scholarship income received by a Chinese student temporarily present in the United States. Under U.S. law, this student will become a resident alien for tax purposes if his or her stay in the United States exceeds 5 calendar years. However, paragraph 2 of the first Protocol to the U.S.-China treaty (dated April 30, 1984) allows the provisions of Article 20 to continue to apply even after the Chinese student becomes a resident alien of the United States. A Chinese student who qualifies for this exception (under paragraph 2 of the first protocol) and is relying on this exception to claim an exemption from tax on his or her scholarship or fellowship income would attach to Form W-9 a statement that includes the information described above to support that exemption. If you are a nonresident alien or a foreign entity not subject to backup withholding, give the requester the appropriate completed Form W-8. What is backup withholding? Persons making certain payments to you must under certain conditions withhold and pay to the IRS 28% of such payments. This is called “backup withholding.” Payments that may be subject to backup withholding include interest, tax-exempt interest, dividends, broker and barter exchange transactions, rents, royalties, nonemployee pay, and certain payments from fishing boat operators. Real estate transactions are not subject to backup withholding. You will not be subject to backup withholding on payments you receive if you give the requester your correct TIN, make the proper certifications, and report all your taxable interest and dividends on your tax return. Payments you receive will be subject to backup withholding if: 1. You do not furnish your TIN to the requester, 2. You do not certify your TIN when required (see the Part II instructions on page 3 for details), 3. The IRS tells the requester that you furnished an incorrect TIN, Page 2 4. The IRS tells you that you are subject to backup withholding because you did not report all your interest and dividends on your tax return (for reportable interest and dividends only), or 5. You do not certify to the requester that you are not subject to backup withholding under 4 above (for reportable interest and dividend accounts opened after 1983 only). Certain payees and payments are exempt from backup withholding. See the instructions below and the separate Instructions for the Requester of Form W-9. Also see Special rules for partnerships on page 1. Penalties Failure to furnish TIN. If you fail to furnish your correct TIN to a requester, you are subject to a penalty of $50 for each such failure unless your failure is due to reasonable cause and not to willful neglect. Civil penalty for false information with respect to withholding. If you make a false statement with no reasonable basis that results in no backup withholding, you are subject to a $500 penalty. Criminal penalty for falsifying information. Willfully falsifying certifications or affirmations may subject you to criminal penalties including fines and/or imprisonment. Misuse of TINs. If the requester discloses or uses TINs in violation of federal law, the requester may be subject to civil and criminal penalties. Specific Instructions Name If you are an individual, you must generally enter the name shown on your income tax return. However, if you have changed your last name, for instance, due to marriage without informing the Social Security Administration of the name change, enter your first name, the last name shown on your social security card, and your new last name. If the account is in joint names, list first, and then circle, the name of the person or entity whose number you entered in Part I of the form. Sole proprietor. Enter your individual name as shown on your income tax return on the “Name” line. You may enter your business, trade, or “doing business as (DBA)” name on the “Business name” line. Limited liability company (LLC). Check the “Limited liability company” box only and enter the appropriate code for the tax classification (“D” for disregarded entity, “C” for corporation, “P” for partnership) in the space provided. For a single-member LLC (including a foreign LLC with a domestic owner) that is disregarded as an entity separate from its owner under Regulations section 301.7701-3, enter the owner’s name on the “Name” line. Enter the LLC’s name on the “Business name” line. For an LLC classified as a partnership or a corporation, enter the LLC’s name on the “Name” line and any business, trade, or DBA name on the “Business name” line. Other entities. Enter your business name as shown on required federal tax documents on the “Name” line. This name should match the name shown on the charter or other legal document creating the entity. You may enter any business, trade, or DBA name on the “Business name” line. Note. You are requested to check the appropriate box for your status (individual/sole proprietor, corporation, etc.). Exempt Payee If you are exempt from backup withholding, enter your name as described above and check the appropriate box for your status, then check the “Exempt payee” box in the line following the business name, sign and date the form. Page 40 of 43 Page Form W-9 (Rev. 10-2007) Generally, individuals (including sole proprietors) are not exempt from backup withholding. Corporations are exempt from backup withholding for certain payments, such as interest and dividends. Note. If you are exempt from backup withholding, you should still complete this form to avoid possible erroneous backup withholding. The following payees are exempt from backup withholding: 3 Part I. Taxpayer Identification Number (TIN) The chart below shows types of payments that may be exempt from backup withholding. The chart applies to the exempt payees listed above, 1 through 15. Enter your TIN in the appropriate box. If you are a resident alien and you do not have and are not eligible to get an SSN, your TIN is your IRS individual taxpayer identification number (ITIN). Enter it in the social security number box. If you do not have an ITIN, see How to get a TIN below. If you are a sole proprietor and you have an EIN, you may enter either your SSN or EIN. However, the IRS prefers that you use your SSN. If you are a single-member LLC that is disregarded as an entity separate from its owner (see Limited liability company (LLC) on page 2), enter the owner’s SSN (or EIN, if the owner has one). Do not enter the disregarded entity’s EIN. If the LLC is classified as a corporation or partnership, enter the entity’s EIN. Note. See the chart on page 4 for further clarification of name and TIN combinations. How to get a TIN. If you do not have a TIN, apply for one immediately. To apply for an SSN, get Form SS-5, Application for a Social Security Card, from your local Social Security Administration office or get this form online at www.ssa.gov. You may also get this form by calling 1-800-772-1213. Use Form W-7, Application for IRS Individual Taxpayer Identification Number, to apply for an ITIN, or Form SS-4, Application for Employer Identification Number, to apply for an EIN. You can apply for an EIN online by accessing the IRS website at www.irs.gov/businesses and clicking on Employer Identification Number (EIN) under Starting a Business. You can get Forms W-7 and SS-4 from the IRS by visiting www.irs.gov or by calling 1-800-TAX-FORM (1-800-829-3676). If you are asked to complete Form W-9 but do not have a TIN, write “Applied For” in the space for the TIN, sign and date the form, and give it to the requester. For interest and dividend payments, and certain payments made with respect to readily tradable instruments, generally you will have 60 days to get a TIN and give it to the requester before you are subject to backup withholding on payments. The 60-day rule does not apply to other types of payments. You will be subject to backup withholding on all such payments until you provide your TIN to the requester. Note. Entering “Applied For” means that you have already applied for a TIN or that you intend to apply for one soon. Caution: A disregarded domestic entity that has a foreign owner must use the appropriate Form W-8. IF the payment is for . . . THEN the payment is exempt for . . . Part II. Certification Interest and dividend payments All exempt payees except for 9 Broker transactions Exempt payees 1 through 13. Also, a person registered under the Investment Advisers Act of 1940 who regularly acts as a broker Barter exchange transactions and patronage dividends Exempt payees 1 through 5 Payments over $600 required to be reported and direct 1 sales over $5,000 Generally, exempt payees 2 1 through 7 1. An organization exempt from tax under section 501(a), any IRA, or a custodial account under section 403(b)(7) if the account satisfies the requirements of section 401(f)(2), 2. The United States or any of its agencies or instrumentalities, 3. A state, the District of Columbia, a possession of the United States, or any of their political subdivisions or instrumentalities, 4. A foreign government or any of its political subdivisions, agencies, or instrumentalities, or 5. An international organization or any of its agencies or instrumentalities. Other payees that may be exempt from backup withholding include: 6. A corporation, 7. A foreign central bank of issue, 8. A dealer in securities or commodities required to register in the United States, the District of Columbia, or a possession of the United States, 9. A futures commission merchant registered with the Commodity Futures Trading Commission, 10. A real estate investment trust, 11. An entity registered at all times during the tax year under the Investment Company Act of 1940, 12. A common trust fund operated by a bank under section 584(a), 13. A financial institution, 14. A middleman known in the investment community as a nominee or custodian, or 15. A trust exempt from tax under section 664 or described in section 4947. 1 2 See Form 1099-MISC, Miscellaneous Income, and its instructions. However, the following payments made to a corporation (including gross proceeds paid to an attorney under section 6045(f), even if the attorney is a corporation) and reportable on Form 1099-MISC are not exempt from backup withholding: medical and health care payments, attorneys’ fees, and payments for services paid by a federal executive agency. To establish to the withholding agent that you are a U.S. person, or resident alien, sign Form W-9. You may be requested to sign by the withholding agent even if items 1, 4, and 5 below indicate otherwise. For a joint account, only the person whose TIN is shown in Part I should sign (when required). Exempt payees, see Exempt Payee on page 2. Signature requirements. Complete the certification as indicated in 1 through 5 below. 1. Interest, dividend, and barter exchange accounts opened before 1984 and broker accounts considered active during 1983. You must give your correct TIN, but you do not have to sign the certification. 2. Interest, dividend, broker, and barter exchange accounts opened after 1983 and broker accounts considered inactive during 1983. You must sign the certification or backup withholding will apply. If you are subject to backup withholding and you are merely providing your correct TIN to the requester, you must cross out item 2 in the certification before signing the form. Page 41 of 43 Form W-9 (Rev. 10-2007) Page 3. Real estate transactions. You must sign the certification. You may cross out item 2 of the certification. 4. Other payments. You must give your correct TIN, but you do not have to sign the certification unless you have been notified that you have previously given an incorrect TIN. “Other payments” include payments made in the course of the requester’s trade or business for rents, royalties, goods (other than bills for merchandise), medical and health care services (including payments to corporations), payments to a nonemployee for services, payments to certain fishing boat crew members and fishermen, and gross proceeds paid to attorneys (including payments to corporations). 5. Mortgage interest paid by you, acquisition or abandonment of secured property, cancellation of debt, qualified tuition program payments (under section 529), IRA, Coverdell ESA, Archer MSA or HSA contributions or distributions, and pension distributions. You must give your correct TIN, but you do not have to sign the certification. What Name and Number To Give the Requester For this type of account: 1. Individual 2. Two or more individuals (joint account) 3. Custodian account of a minor (Uniform Gift to Minors Act) 4. a. The usual revocable savings trust (grantor is also trustee) b. So-called trust account that is not a legal or valid trust under state law 5. Sole proprietorship or disregarded entity owned by an individual Give name and SSN of: The individual The actual owner of the account or, if combined funds, the first 1 individual on the account 2 The minor The grantor-trustee The actual owner The owner 1 2 3 4 1 3 Give name and EIN of: For this type of account: 6. Disregarded entity not owned by an individual 7. A valid trust, estate, or pension trust 8. Corporate or LLC electing corporate status on Form 8832 9. Association, club, religious, charitable, educational, or other tax-exempt organization 10. Partnership or multi-member LLC 11. A broker or registered nominee 12. Account with the Department of Agriculture in the name of a public entity (such as a state or local government, school district, or prison) that receives agricultural program payments 1 The owner 4 Legal entity The corporation The organization 4 Secure Your Tax Records from Identity Theft Identity theft occurs when someone uses your personal information such as your name, social security number (SSN), or other identifying information, without your permission, to commit fraud or other crimes. An identity thief may use your SSN to get a job or may file a tax return using your SSN to receive a refund. To reduce your risk: ● Protect your SSN, ● Ensure your employer is protecting your SSN, and ● Be careful when choosing a tax preparer. Call the IRS at 1-800-829-1040 if you think your identity has been used inappropriately for tax purposes. Victims of identity theft who are experiencing economic harm or a system problem, or are seeking help in resolving tax problems that have not been resolved through normal channels, may be eligible for Taxpayer Advocate Service (TAS) assistance. You can reach TAS by calling the TAS toll-free case intake line at 1-877-777-4778 or TTY/TDD 1-800-829-4059. Protect yourself from suspicious emails or phishing schemes. Phishing is the creation and use of email and websites designed to mimic legitimate business emails and websites. The most common act is sending an email to a user falsely claiming to be an established legitimate enterprise in an attempt to scam the user into surrendering private information that will be used for identity theft. The IRS does not initiate contacts with taxpayers via emails. Also, the IRS does not request personal detailed information through email or ask taxpayers for the PIN numbers, passwords, or similar secret access information for their credit card, bank, or other financial accounts. If you receive an unsolicited email claiming to be from the IRS, forward this message to phishing@irs.gov. You may also report misuse of the IRS name, logo, or other IRS personal property to the Treasury Inspector General for Tax Administration at 1-800-366-4484. You can forward suspicious emails to the Federal Trade Commission at: spam@uce.gov or contact them at www.consumer.gov/idtheft or 1-877-IDTHEFT(438-4338). Visit the IRS website at www.irs.gov to learn more about identity theft and how to reduce your risk. The partnership The broker or nominee The public entity List first and circle the name of the person whose number you furnish. If only one person on a joint account has an SSN, that person’s number must be furnished. Circle the minor’s name and furnish the minor’s SSN. You must show your individual name and you may also enter your business or “DBA” name on the second name line. You may use either your SSN or EIN (if you have one), but the IRS encourages you to use your SSN. List first and circle the name of the trust, estate, or pension trust. (Do not furnish the TIN of the personal representative or trustee unless the legal entity itself is not designated in the account title.) Also see Special rules for partnerships on page 1. Note. If no name is circled when more than one name is listed, the number will be considered to be that of the first name listed. Privacy Act Notice Section 6109 of the Internal Revenue Code requires you to provide your correct TIN to persons who must file information returns with the IRS to report interest, dividends, and certain other income paid to you, mortgage interest you paid, the acquisition or abandonment of secured property, cancellation of debt, or contributions you made to an IRA, or Archer MSA or HSA. The IRS uses the numbers for identification purposes and to help verify the accuracy of your tax return. The IRS may also provide this information to the Department of Justice for civil and criminal litigation, and to cities, states, the District of Columbia, and U.S. possessions to carry out their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. You must provide your TIN whether or not you are required to file a tax return. Payers must generally withhold 28% of taxable interest, dividend, and certain other payments to a payee who does not give a TIN to a payer. Certain penalties may also apply. Page 42 of 43 Ow wner Operrator App plication S Submiss sion Page e Once yo ou have com mpleted the Owner Operator Applica ation and ha ave reviewe ed the Owne er Operator Agreement, may sellect the ema ail button below to subm mit this applic cation to Exxpress. Plea ase review a all informatio on provided make any correctio ons necessa ary before submitting this applica ation. You also have the option of printing applicatiion for your own records s. Email Form Print Form




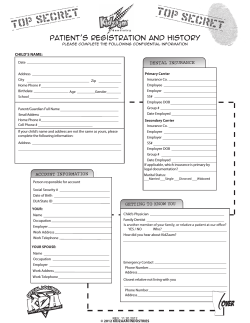





© Copyright 2025