
Queries for Author Author query sheet
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:27
Author query sheet
Queries for Author
Journal: Postgraduate Medical Journal
Paper: pj72140
Title: Evaluation of the thyroid nodule
The proof of your manuscript appears on the following page(s).
Please note that this is a galley proof and the layout of the article may change before publication. Please read the manuscript
carefully, checking for accuracy, verifying the reference order and double-checking figures and tables. When reviewing your page
proof please keep in mind that a professional copyeditor edited your manuscript to comply with the style requirements of the journal.
This is not an opportunity to alter, amend or revise your paper; it is intended to be for correction purposes only.
During the preparation of your manuscript for publication, the questions listed below have arisen (the query number can also be
found in the gutter close to the text it refers to). Please attend to these matters and return the answers to these questions when you
return your corrections.
Please note, we will not be able to proceed with your article and publish it in print if these queries
have not been addressed.
Query
Reference
Query
1
Please check the legend supplied for fig 2. Please check definitions of
abbreviations.
2
Please check the page nos for ref 8.
If you are happy with the proof as it stands, please email to confirm this. Changes that do not require a copy of the proof can be sent
by email (please be as specific as possible).
Email: christinew.glenlea@btinternet.com
If you have any changes that cannot be described easily in an email, please mark them clearly on the proof and email a scan of the
changes by replying to the eProof email or by fax: +44 (0)844 443 1064.
PLEASE RESPOND WITHIN 48 HOURS
0
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:28
Review
Evaluation of the thyroid nodule
D Ghassi, A Donato
Department of Internal
Medicine, The Reading Hospital
and Medical Center, West
Reading, Philadelphia, USA
Correspondence to:
Dr D Ghassi, 10 F Downing
Square, Guilderland, NY 12084,
USA; dimpleghassi2@yahoo.
com
Received 5 June 2008
Accepted 11 December 2008
ABSTRACT
The annual incidence of thyroid cancer worldwide is 1
case per 100 000 men and 2.6 cases per 100 000
women. Most thyroid nodules are asymptomatic and are
discovered incidentally on physical examination, selfpalpation or incidentally on imaging studies performed for
unrelated reasons. Although the majority of both palpable
and non-palpable thyroid nodules are benign, ,5% may
represent thyroid cancer. Thyroid-stimulating hormone,
thyroid ultrasound and fine-needle aspiration biopsy are
key tests to guide management. Physicians caring for
patients with thyroid nodules need to develop a rational,
cost-effective approach to ordering and interpreting
imaging and diagnostic tests in the evaluation of the
thyroid nodule.
Although thyroid cancer represents under 1% of all
malignancies worldwide, it is currently one of the
most rapidly increasing malignancies in the
Western world. Thyroid nodules can be palpated
in 4–7% of patients and can be detected by imaging
in as many as 50% of the general population,1 2
with ,5% of these nodules representing cancer.
Newly available imaging modalities are identifying
these often asymptomatic and non-palpable
nodules, making it imperative that primary care
doctors understand how to interpret diagnostic
studies, understand indications for referral, and
manage the long-term survivors of thyroid cancer.
Three major endocrine societies (American
Association of Clinical Endocrinologists (AACE),
British Thyroid Association (BTA) and European
Thyroid Association (ETA)) have updated their
recommendations in the past 3 years, and their
recommendations are reviewed here. A rational,
cost-effective approach is vital to guide the primary
care doctor’s evaluation and management of this
important issue.
INCIDENCE
Approximately 275 000 new thyroid nodules are
detected annually in the USA.3 Nodules are four to
eight times more common in women and increase
in frequency with increasing age, decreased iodine
intake, and history of radiation exposure to head
and neck.4 The annual incidence of thyroid cancer
worldwide is 1 case per 100 000 men and 2.6 cases
per 100 000 women. However, Central America,
Japan and Micronesia have incidence rates two to
three times higher for unknown reasons.5
Interestingly, the incidence of thyroid cancer
diagnoses has been increasing at an alarming rate
in the Western world, from 2.7 to 7.7 per 100 000
people in the USA6 and from 2.3 to 3.5 per 100 000
people in the UK in the past 30 years.7 It has been
noted that the increase in diagnoses is predominantly driven by the increased incidence of small
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
(,1 cm) papillary thyroid cancers. Given that
mortality from thyroid cancer (0.5 per 100 000)
has not changed over this time and that there has
not been a concomitant increase in retrosternal
thyroid cancers (which would not be detected by
ultrasound surveillance),8 experts believe that
newer surveillance techniques leading to earlier
diagnosis of subclinical disease may be responsible
for this increase in cancer incidence.9 It is not clear,
however, whether the recent increase in diagnostic
CT with iodinated contrast in Western countries
has a causative role.10
HISTORY AND PHYSICAL EXAMINATION
Most thyroid nodules are asymptomatic and are
discovered incidentally on physical examination,
self-palpation or imaging studies such as carotid
ultrasound, CT or MRI of the neck performed for
unrelated reasons. History taking and examination
should focus on eliciting high-risk features for
thyroid malignancy (box 1). Male sex as well as
extremes of age (,20, .70) increase the likelihood
of malignancy. History of exposure to head and
neck radiation, either as a result of treatment of
tonsillar and thymic disease or from exposure to
nuclear fallout, is an important risk factor.3 A
family history of benign or malignant thyroid
disease, familial medullary thyroid carcinoma,
familial polyposis coli, Gardner syndrome (colon
polyposis with bone and soft tissue cancers) and
Cowden syndrome (hamartomas, fibrocystic
breast disease and breast cancer) should be
reviewed. Symptoms of airway compression, hoarseness and dysphagia often suggest local invasion.
Rate of change of any palpable thyroid mass should
be obtained. Masses that have appeared or grown
over the course of hours are usually the result of
haemorrhage into an existing nodule. However,
growth over the course of weeks is concerning for
malignancy. Symptoms of hypothyroidism and
hyperthyroidism should be elicited; however, they
are present in ,1% of patients.
Physical examination should include size, consistency (firm, cystic, rubbery) and movement
with swallowing. Fixation suggests cellular invasion secondary to malignancy. Patients with a
thyroid mass should be assessed for vocal cord
paralysis. An inspection for mucosal neuromas or
marfanoid habitus may suggest multiple endocrine
neoplasia type 2b (MEN2b). In addition to palpation of the thyroid gland, a thorough examination
of lymph nodes in the head and neck should be
performed. Indicators of thyroid malignancy
include a hard, fixed lesion, cervical lymphadenopathy, hoarseness and thyroid nodule .4 cm.
Pemburton’s sign (distension of the external
jugular veins and facial plethora or symptoms of
dyspnoea while the arms of the patient are above
1
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:28
Review
Box 1 Factors associated with increased risk of
malignancy
c
c
c
c
c
c
c
c
c
Male sex
Age ,20 or .70 years
Family history of multiple endocrine neoplasia type 2b or
medullary thyroid cancer
History of head and neck radiation
Rapid tumour growth
Firm or hard consistency
Fixed nodule
Cervical adenopathy
Hoarseness, dysphonia, dysphagia, dyspnoea or cough
the head) suggests thyroid compression of central neck
structures.6
British authorities recommend urgent referral to a thyroid
specialist for children with nodules, patients with cervical
adenopathy, unexplained airway symptoms or respiratory
problems in conjunction with a nodule or goitre, or rapidly
enlarging painless mass.1
LABORATORY EVALUATION
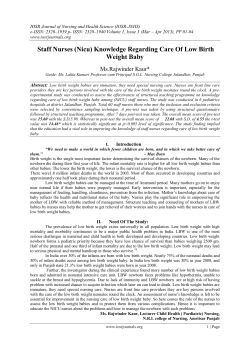
Serum thyroid-stimulating hormone (TSH) should be measured
in all patients with thyroid nodules.1 6 If it is low, concentrations of free thyroxine and free triiodothyronine should be
checked to document the severity of the hyperthyroidism (fig 1).
Suppressed TSH concentrations suggest an autonomously
functioning nodule or a toxic multinodular goitre. On the other
hand, if serum TSH is raised, serum concentrations of
thyroperoxidase antibody should be checked to diagnose
Hashimoto thyroiditis.11 Raised TSH does not exclude the need
for biopsy because ,5% of thyroid cancers are lymphomas,
which can be associated with Hashimoto thyroiditis.12
Controversy exists over the use of serum calcitonin in the
diagnostic evaluation of the thyroid nodule. AACE and BTA
guidelines do not recommend routine screening of calcitonin for
all thyroid nodules, but consider it to be useful in patients with
high suspicion of MEN2b or medullary thyroid cancer (MTC).
However, ETA in 2006 came out in favour of routine serum
calcitonin screening of all patients with thyroid nodules, citing
the high sensitivity of calcitonin for MTC, a recommendation
that has been supported by recent cost-effectiveness analyses by
Cheung et al.13 Raised calcitonin suggests MTC, although renal
failure, Hashimoto thyroiditis and hypergastrinaemia may
cause false-positive results.1 Patients diagnosed as having MTC
should be evaluated for concurrent pheochromocytoma and
hyperparathyroidism as well as screened for the RET protooncogene, with consideration of referral to a genetics counsellor.3 14 Routine assessment of thyroglobulin is not recommended
for evaluation of a thyroid nodule.15
IMAGING STUDIES
Isotope scanning
Thyroid scintigraphy is used for assessment of thyroid function
and detection of autonomously functioning thyroid tissue.
Based on the pattern of radioiodine uptake, nodules are
classified as cold (decreased uptake), hot (increased uptake in
nodule with suppression of uptake in surrounding tissue) or
warm (uptake similar to surrounding tissue). Hot nodules rarely
represent malignancy, whereas cold nodules have a malignancy
2
risk of 5–8%. As the vast majority of thyroid nodules are cold
(,85%), and only a small minority of these are malignant, the
predictive value of scintigraphy for malignancy is low.
Therefore, the AACE recommendations include thyroid scintigraphy only in cases where TSH concentrations are suppressed
(or are low-normal in areas of iodine deficiency) or where
ectopic thyroid tissue or retrosternal goitre is suspected.6 ETA
recommends scintigraphy for all patients with multinodular
goitre.
Ultrasonography
High-resolution ultrasound is extremely sensitive for detection
of thyroid nodules missed on physical examination or other
imaging techniques. In patients with a palpable thyroid nodule,
additional nodules with features requiring biopsy are detected
by ultrasound in 24%, prompting AACE to recommend
ultrasound evaluation of all palpable thyroid nodules. In
addition, ultrasound screening is recommended for all patients
at high risk of thyroid malignancy (history of familial thyroid
cancer or MEN2b or significant radiation exposure) and for
patients with multinodular goitre.6 Ultrasound evaluation is not
recommended as a screening test in patients with normal
thyroid on palpation and low risk of cancer.1 6 Along with size
determination, ultrasound can detect features of nodules that
increase the likelihood of malignancy, including hypoechogenicity, microcalcification, irregular margins and chaotic vascular
patterns, as well as extracapsular invasion and lymph node
involvement. The presence of at least two suspicious sonographic criteria reliably identifies most neoplastic lesions of the
thyroid gland.16 However, definitive differentiation between
benign and malignant lesions with current ultrasound technology is not possible. Finally, ultrasound guidance of the biopsy
can be used to decrease the rate of non-diagnostic fine-needle
aspiration biopsy (FNAB) from 16% to 4%,17 and is recommended by all three societies if an initial palpation-based FNAB
is non-diagnostic.1 6 14
Other diagnostic imaging
MRI and CT scan should not be routinely used because they are
seldom diagnostic for malignant lesions in nodular thyroid
disease. However, in cases of retrosternal goitre, where
ultrasound evaluation may be limited by anatomical factors,
MRI or CT scan may be necessary. Furthermore, CT contrast
medium contains iodine and can reduce subsequent uptake of
radioiodine, limiting the utility of scintigraphy until cleared.
Gadolinium-enhanced MRI can provide useful information
without subsequent compromise of radioiodine uptake of the
remaining thyroid tissue. Evaluation of glucose metabolism by
positron emission tomography may help to distinguish benign
from malignant nodules, but its use is limited by cost and
availability.
FNAB
FNAB is the safest, most effective and most reliable technique
available to distinguish between benign and malignant thyroid
nodules. It is a highly accurate, inexpensive outpatient
procedure and has become an integral part of evaluation of
the thyroid nodule. The diagnostic accuracy of FNAB
approaches 95% in skilled hands with experienced cytopathological support.18 Its use has reduced the number of thyroidectomies by half and the overall cost of thyroid nodule medical
care by one-quarter while doubling the yield of malignancy at
surgery.19 Use of anticoagulants and aspirin does not preclude
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:28
Review
Figure 1 Initial evaluation of a thyroid nodule. FNAB, fine-needle aspiration biopsy; MNG, multinodular goitre; T3, tri-iodothyronine; T4, thyroxine;
TPO, thyroid peroxidase; TSH, thyroid-stimulating hormone; US, ultrasonography. *Recommendation from European Thyroid Association only.
biopsy, and complications are rare. The addition of ultrasound
guidance decreases the rate of non-diagnostic FNAB from 16%
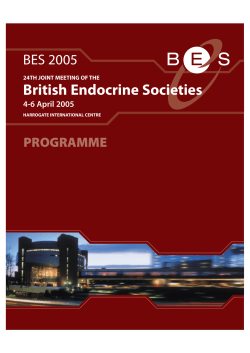
to 4%.17 Biopsy results are classified as non-diagnostic (referred
to as Thy1 by BTA), benign or non-neoplastic (Thy2), follicular
lesion/suspected follicular neoplasm (Thy3), suspicious (Thy4)
or malignant (Thy5) (fig 2).
Inadequate or non-diagnostic (AACE) or Thy1 (BTA) (4–16% of
aspirates)
This represents a lack of cellular material for an adequate
diagnosis and is usually the result of biopsy of a cystic nodule
with few or no follicular cells. Ultrasound-guided re-aspiration
from the peripheral portion of the cystic lesion should be
performed if the initial test result is non-diagnostic. Reaspiration yields satisfactory results in 50% of cases. A small
percentage (5%) of thyroid nodules remain non-diagnostic
despite good initial technique, re-biopsy and FNAB with
ultrasound guidance. In those cases, surgical excision is
recommended.6 14
Benign (AACE) or Thy2 (BTA) (70% of all aspirates)
Differential diagnoses include benign colloid nodules,
Hashimoto thyroiditis, macrofollicular adenoma, lymphocytic
thyroiditis, granulomatous thyroiditis and benign cyst.
Management options for benign nodules include observation
only with regular follow-up, suppressive thyroxine therapy,
surgery, percutaneous ethanol injection and radioactive iodine
therapy. BTA additionally advises a repeat biopsy in 3–
6 months to confirm diagnosis.14
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
Observation only with regular follow-up
Patients with benign nodules who choose conservative therapy
should be reassessed every 6–18 months for symptoms suggesting malignancy or change in size on examination. Ultrasound
re-evaluation is recommended 6–12 months after the initial
diagnosis and ‘‘regularly’’ thereafter by the AACE (grade D
recommendation- inconclusive evidence); ultrasound re-evaluation is optional in BTA guidelines.14 If the nodule size is stable,
the intervals between subsequent ultrasound evaluations can be
extended. If there is evidence of growth either clinically or by
ultrasound, repeat biopsy should be performed. In patients with
growing nodules that are benign on repeat biopsy, surgical
intervention should be considered, based on the patient’s
symptoms or preferences.
Suppressive levothyroxine therapy
Use of thyroid hormone replacement to suppress serum TSH
(below 0.3 mU) for management of thyroid nodules is
controversial. Its use is aimed at shrinking palpable thyroid
nodules and preventing the appearance of new nodules.20 A
recent meta-analysis has shown no significant difference in the
size of nodules after 6–12 months of suppressive therapy.21 As
thyroid hormone suppression induces a clinically significant
reduction in thyroid nodule volume in only a minority of
patients and is associated with hyperthyroid risks, AACE and
BTA guidelines do not recommend routine use of suppressive
levothyroxine therapy.6 14
Surgical treatment
Surgical indications for a benign thyroid nodule include
symptoms of dysphagia, dyspnoea, hoarseness, neck pressure,
hyperthyroidism from a functioning nodule and nodule growth
3
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:29
Review
Figure 2 Classification of fine-needle aspiration biopsy (FNAB) results and the recommended actions. BTA, British Thoracic Association; ETA,
European Thoracic Association; LT4, levothyroxine; PEI, percutaneous ethanol injection; RAI, radioactive iodine; TSH, thyroid-stimulating hormone; US,
ultrasound. *Recommendations from ETA only. {Recommendations from the American Association of Clinical Endocrinologists only.
{Recommendations from BTA only.
Key learning points
c
c
c
c
c
4
Thyroid nodules are palpated in 4–7% of patients and can be
detected by imaging in 50% of the general population.
Most thyroid nodules are benign and ,5% represent
malignancy.
Serum thyroid-stimulating hormone (TSH) should be measured
in all patients with thyroid nodules.
Ultrasonography is recommended in all patients with thyroid
nodules with normal or raised TSH.
Fine-needle aspiration biopsy is the most cost-effective and
accurate method for evaluating thyroid nodules.
despite benign findings on FNAB. For a solitary benign nodule,
lobectomy plus isthmectomy is sufficient. For bilateral nodules,
a near-total thyroidectomy is appropriate.
Percutaneous ethanol injection
A number of studies suggest a benefit of percutaneous ethanol
injection by ultrasound guidance in the treatment of benign,
non-functioning solid and cystic thyroid nodules. Ethanol
causes coagulative necrosis and small-vessel thrombosis.22
Prospective, randomised trials showed that percutaneous
ethanol injection is significantly superior to aspiration alone in
inducing reduction of nodule volume. A reduction of .50% of
baseline volume is obtained in almost 90% of cases.23 This
procedure requires prior documentation of benign cytology. The
rate of recurrence of cystic lesions is very low. AACE considers
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
;
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:30
Review
Key references
c
c
c
c
c
American Association of Clinical Endocrinologists and
Associazione Medici Endocrinologi. Medical guidelines for
clinical practice for the diagnosis and management of thyroid
nodules. Endocr Pract 2006;12:63–102.
Pacini F, Schlumberger M, Dralle H, et al. European consensus
for the management of patients with differentiated thyroid
carcinoma of the follicular epithelium. Eur J Endocrinol
2006;154:787–803.
Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med
2004;351:1764–71.
Gharib H, Goellner JR. Fine-needle aspiration biopsy of thyroid
nodules. Endocr Pract 1995;1:410–17.
Singer PA, Cooper DS, Daniels GH, et al. Treatment guidelines
for patients with thyroid nodules and well-differentiated
thyroid cancer. American Thyroid Association. Arch Intern
Med 1996;156:2165–72.
percutaneous ethanol injection a first-line non-surgical treatment for recurrent cystic nodules of the thyroid gland after
FNAB has ruled out a malignant lesion.6
Radioactive iodine therapy
Radioiodine can be used for treatment of a functioning (‘‘hot’’)
nodule with or without biochemical evidence of hyperthyroidism. It is contraindicated in pregnancy and lactation. The aim of
radioiodine treatment is ablation of autonomously functioning
areas to achieve euthyroidism. This treatment is successful in
85–100% of patients with hyperfunctioning thyroid nodules or
toxic multinodular goitre.24 The main side effect is hypothyroidism, occurring in 10% of patients within 5 years of
treatment. Antithyroid drugs should be withdrawn 3 weeks
before radioactive iodine treatment and should not be administered for 3–5 days after treatment.
Suspicious or indeterminate (AACE) or Thy3 and Thy 4 (BTA)
(10–20% of aspirates)
Thy3 differential diagnoses include follicular lesion/suspected
follicular neoplasms. Although some of these are tumours,
many prove to be hyperplastic nodules on excision. Thy4
represents nodules with findings suspicious, but not diagnostic,
of malignancy. Differential diagnoses include Hurthle cell
tumours and atypical papillary tumours or lymphoma.
Suspicious or indeterminate results indicate a cytology pattern
that may or may not be malignant, requiring analysis of full
histological tissue architecture to rule out malignancy.25 As
,20% of indeterminate FNAB specimens are found to be
malignant at surgical intervention, current AACE recommendations are surgical excision of all indeterminate nodules.6 BTA
suggests that these cases be reviewed by a multidisciplinary
Future research questions
c
c
c
Do newer techniques to identify thyroid nodules prolong
survival in patients screened?
Is routine serum calcitonin screening in patients undergoing
evaluation for thyroid nodule cost-effective ?
Is the recent increase in the use of CT scanning related to the
increased incidence of thyroid cancers?
team to guide further treatment, and similarly recommends
surgery for all suspected cancers.14
Malignant (AACE) or Thy5 (BTA) (5% of aspirates)
Differential diagnosis includes primary thyroid or secondary
(metastatic) cancers. The most common malignant lesion
encountered is papillary thyroid cancer. If cytological results
are positive, surgical intervention is always necessary for
surgical candidates. The extent of thyroid surgery is controversial. For most patients, especially those with differentiated
cancers .1 cm in size, familial disease, multifocal disease,
capsular invasion or lymph node involvement, near-total
thyroidectomy along with removal of lymph nodes from the
central compartment is recommended.6 Postoperative 131I
ablation is administered for high-risk patients, especially those
with gross residual disease, metastatic disease or nodal involvement. Postoperative administration of levothyroxine after
complete resection of thyroid cancer to suppress TSH concentration (,0.1 mU) has been shown to improve disease-free
survival in locally advanced papillary cancers.26
CONCLUSIONS
For patients presenting with a thyroid nodule, exclusion of
cancer is the important clinical concern. Initial evaluation
should include a serum TSH assay (to determine the functional
status of the nodule) and ultrasound (to look for other nonpalpable nodules and to determine high-risk features that
require biopsy). If serum TSH is suppressed, radionuclide
scanning should be performed. FNAB is essential for distinguishing between benign and malignant nodules. Patients with
malignant or indeterminate biopsy results should be referred for
surgery. Patients with non-diagnostic biopsy results should have
a repeat ultrasound-guided biopsy. For non-functioning, benign
nodules, no treatment is necessary, but serial follow-up should
be performed, and repeat FNAB can be considered.
MULTIPLE CHOICE QUESTIONS (ANSWERS AFTER THE
REFERENCES)
1. A 35-year-old woman undergoes routine physical examination
and her doctor notices 1.5 61 cm soft, mobile nodule on the left
thyroid lobe. What is the next diagnostic test?
A.
B.
C.
D.
2. A 45-year-old man presents to his doctor for follow-up of a 1.2
61.8 cm thyroid nodule identified incidentally on MRI of his
neck ordered for neck pain. He has no family history of thyroid
disease or MEN2b. Serum TSH = 0.0005 mU (normal 0.5-5 mU).
What is the next best test to order?
A.
B.
C.
D.
FNAB
Thyroid ultrasound
Radionuclide scintigraphy
Serum calcitonin assay
3. A 53-year-old man with normal TSH underwent FNAB of a 2
61.5 cm nodule. Pathology results were read as suspicious for
follicular neoplasm. What is the next step in management of this
patient?
A.
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140
FNAB
TSH
Thyroglobulin level
Thyroperoxidase antibodies
Wait and watch
5
pj72140
Module 1
Topics:
Postgraduate Medical Journal 6/2/09 07:55:34
Review
B. Refer for surgery
C. Radioiodine therapy
D. Levothyroxine suppression
11.
12.
13.
4. A 29-year-old woman presents to her doctor with a concern
about thyroid cancer because her friend was recently diagnosed
with a benign nodule. She denies any family history of thyroid
disease and has no history of exposure to head and neck
radiation. What screening test should be offered to her?
A.
B.
C.
D.
TSH
Ultrasound
FNAB
Physical examination
Competing interests: None.
14.
15.
16.
17.
18.
19.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
<
8.
9.
10.
6
Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management
of patients with differentiated thyroid carcinoma of the follicular epithelium.
Eur J Endocrinol 2006;154:787–803.
Singer PA, Cooper DS, Daniels GH, et al. Treatment guidelines for patients with
thyroid nodules and well-differentiated thyroid cancer. American Thyroid Association.
Arch Intern Med 1996;156:2165–72.
Lansford CD, Teknos TN. Evaluation of the thyroid nodule. Cancer Control
2006;13:89–98.
Burch HB. Evaluation and management of the solid thyroid nodule. Endocrinol Metab
Clin North Am 1995;24:663–710.
Pisani P, Parkin DM, Bray F, et al. Erratum: estimates of the worldwide mortality
from 25 cancers in 1990 (Int J Cancer 1999;83:18–29). Int J Cancer 1999;83:870–3.
American Association of Clinical Endocrinologists and Associazione Medici
Endocrinologi. Medical guidelines for clinical practice for the diagnosis and
management of thyroid nodules. Endocr Pract 2006;12:63–102.
How J, Tabah R. Explaining the increasing incidence of differentiated thyroid cancer.
CMAJ 2007;177:1383–4.
Grodski SBT, Gill A, Sywak M, et al. Increasing incidence of thyroid cancer in
retrosternal goiter. A NZ J Surg 2007;77(Suppl 1):A23–A23(21).
Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States,
1973–2002. JAMA 2006;295:2164–7.
Baker SR, Bhatti WA. The thyroid cancer epidemic: is it the dark side of the CT
revolution? Eur J Radiol 2006;60:67–9.
20.
21.
22.
23.
24.
25.
26.
Spencer CA, Takeuchi M, Kazarosyan M. Current status and performance goals for
serum thyroglobulin assays. Clin Chem 1996;42:164–73.
Pasieka JL. Hashimoto’s disease and thyroid lymphoma: role of the surgeon.
World J Surg 2000;24:966–70.
Cheung K, Roman SA, Wang TS, et al. Calcitonin measurement in the evaluation of
thyroid nodules in the United States: a cost-effectiveness and decision analysis. J Clin
Endocrinol Metab 2008;93:2173–80.
Perros P, Clarke SE, Franklyn J, et al. Introduction to the updated guidelines on the
management of thyroid cancer. Clin Med 2007;7:321–2.
Elisei R, Bottici V, Luchetti F, et al. Impact of routine measurement of serum
calcitonin on the diagnosis and outcome of medullary thyroid cancer: experience in
10,864 patients with nodular thyroid disorders. J Clin Endocrinol Metab
2004;89:163–8.
Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med 2004;351:1764–71.
Cochand-Priollet B, Guillausseau PJ, Chagnon S, et al. The diagnostic value of fineneedle aspiration biopsy under ultrasonography in nonfunctional thyroid nodules: a
prospective study comparing cytologic and histologic findings. Am J Med
1994;97:152–7.
Gharib H, Goellner JR. Fine-needle aspiration biopsy of thyroid nodules. Endocr Pract
1995;1:410–17.
Werk EE Jr, Vernon BM, Gonzalez JJ, et al. Cancer in thyroid nodules. A community
hospital survey. Arch Intern Med 1984;144:474–6.
Gharib H, Mazzaferri EL. Thyroxine suppressive therapy in patients with nodular
thyroid disease. Ann Intern Med 1998;128:386–94.
Sdano MT, Falciglia M, Welge JA, et al. Efficacy of thyroid hormone suppression for
benign thyroid nodules: meta-analysis of randomized trials. Otolaryngol Head Neck
Surg 2005;133:391–6.
Lippi F, Ferrari C, Manetti L, et al. Treatment of solitary autonomous thyroid nodules
by percutaneous ethanol injection: results of an Italian multicenter study. The
Multicenter Study Group. J Clin Endocrinol Metab 1996;81:3261–4.
Bennedbaek FN, Hegedus L. Treatment of recurrent thyroid cysts with ethanol: a
randomized double-blind controlled trial. J Clin Endocrinol Metab 2003;88:5773–7.
Meier DA, Brill DR, Becker DV, et al. Procedure guideline for therapy of thyroid
disease with (131)iodine. J Nucl Med 2002;43:856–61.
Cersosimo E, Gharib H, Suman VJ, et al. ‘‘Suspicious’’ thyroid cytologic findings:
outcome in patients without immediate surgical treatment. Mayo Clin Proc
1993;68:343–8.
Cooper DS, Specker B, Ho M, et al. Thyrotropin suppression and disease progression
in patients with differentiated thyroid cancer: results from the National Thyroid Cancer
Treatment Cooperative Registry. Thyroid 1998;8:737–44.
Answers
1 (B); 2 (C); 3 (B); 4 (D)
Postgrad Med J 2009;000:0–6. doi:10.1136/pgmj.2008.072140



















© Copyright 2025