
On This Page
On This Page Travel Notices in Effect Safety and Security Abroad Preparing for Your Trip to Belize Other Diseases Found in Mexico and Central America Staying Healthy During Your Trip After You Return Home Travel Notices in Effect Update: Dengue, Tropical and Subtropical Regions Updated: September 19, 2007 Update: 2007 Measles and Mumps Outbreaks Updated: May 17, 2007 Safety and Security Abroad Registration of Traveler Emergency Contact and Itinerary Information Updated: June 18, 2007 Transportation Security Administration U.S. Department of State Page | 1 Preparing for Your Trip to Belize Before visiting Belize, you may need to get the following vaccinations and medications for vaccinepreventable diseases and other diseases you might be at risk for at your destination: (Note: Your doctor or health-care provider will determine what you will need, depending on factors such as your health and immunization history, areas of the country you will be visiting, and planned activities.) To have the most benefit, see a health-care provider at least 4–6 weeks before your trip to allow time for your vaccines to take effect and to start taking medicine to prevent malaria, if you need it. Even if you have less than 4 weeks before you leave, you should still see a health-care provider for needed vaccines, anti-malaria drugs and other medications and information about how to protect yourself from illness and injury while traveling. CDC recommends that you see a health-care provider who specializes in Travel Medicine. Find a travel medicine clinic near you. If you have a medical condition, you should also share your travel plans with any doctors you are currently seeing for other medical reasons. If your travel plans will take you to more than one country during a single trip, be sure to let your health-care provider know so that you can receive the appropriate vaccinations and information for all of your destinations. Long-term travelers, such as those who plan to work or study abroad, may also need additional vaccinations as required by their employer or school. Although yellow fever is not a disease risk in Belize, the government requires travelers arriving from countries where yellow fever is present to present proof of yellow fever vaccination. If you will be traveling to one of these countries where yellow fever is present before arriving in Belize, this requirement must be taken into consideration. Be sure your routine vaccinations are up-to-date. Check the links below to see which vaccinations adults and children should get. Routine vaccines, as they are often called, such as for influenza, chickenpox (or varicella), polio, measles/mumps/rubella (MMR), and diphtheria/pertussis/tetanus (DPT) are given at all stages of life; see the childhood and adolescent immunization schedule and routine adult immunization schedule. Routine vaccines are recommended even if you do not travel. Although childhood diseases, such as measles, rarely occur in the United States, they are still common in many parts of the world. A traveler who is not vaccinated would be at risk for infection. Page | 2 Vaccine-Preventable Diseases Vaccination or Disease Recommendations or Requirements for Vaccine-Preventable Diseases Recommended if you are not up-to-date with routine shots such as, measles/mumps/rubella (MMR) vaccine, diphtheria/pertussis/tetanus (DPT) vaccine, etc. Recommended for all unvaccinated people traveling to or working in countries with an Hepatitis A or intermediate or high level of hepatitis A virus infection (see map) where exposure might immune globulin occur through food or water. Cases of travel-related hepatitis A can also occur in travelers to (IG) developing countries with "standard" tourist itineraries, accommodations, and food consumption behaviors. Recommended for all unvaccinated persons traveling to or working in countries with intermediate to high levels of endemic HBV transmission (see map) and who might be Hepatitis B exposed to blood or body fluids, have sexual contact with the local population, or be exposed through medical treatment, such as for an accident, and for all adults requesting protection from HBV infection. Recommended for all unvaccinated people traveling to or working in Mexico and Central Typhoid America, especially if visiting smaller cities, villages, or rural areas and staying with friends or relatives where exposure might occur through food or water. Recommended for travelers spending a lot of time outdoors, especially in rural areas, Rabies involved in activities such as bicycling, camping, hiking, or work. Also, children are considered at higher risk because they tend to play with animals and may not report bites. Routine Malaria Drugs to Prevent Malaria (Antimalarial drugs) If you will be visiting a malaria risk area in Belize, chloroquine is the recommended antimalarial drug. Malaria risk area in Belize: All, except no risk in Belize City A Special Note about Antimalarial Drugs You should purchase your antimalarial drugs before travel. Drugs purchased overseas may not be manufactured according to United States standards and may not be effective. They also may be dangerous, contain counterfeit medications or contaminants, or be combinations of drugs that are not safe to use. Halofantrine (marketed as Halfan) is widely used overseas to treat malaria. CDC recommends that you do NOT use halofantrine because of serious heart-related side effects, including deaths. You should avoid using antimalarial drugs that are not recommended unless you have been diagnosed with life-threatening malaria and no other options are immediately available. For detailed information about these antimalarial drugs, see Information for the Public: Prescription Drugs for Malaria. Page | 3 More Information About Malaria Malaria is always a serious disease and may be a deadly illness. Humans get malaria from the bite of a mosquito infected with the parasite. Prevent this serious disease by seeing your health-care provider for a prescription antimalarial drug and by protecting yourself against mosquito bites (see below). Travelers to malaria risk-areas in Belize, including infants, children, and former residents of Belize, should take one of the following antimalarial drugs listed above. Symptoms Malaria symptoms may include fever chills sweats headache body aches nausea and vomiting fatigue Malaria symptoms will occur at least 7 to 9 days after being bitten by an infected mosquito. Fever in the first week of travel in a malaria-risk area is unlikely to be malaria; however, you should see a doctor right away if you develop a fever during your trip. Malaria may cause anemia and jaundice. Malaria infections with Plasmodium falciparum, if not promptly treated, may cause kidney failure, coma, and death. Despite using the protective measures outlined above, travelers may still develop malaria up to a year after returning from a malarious area. You should see a doctor immediately if you develop a fever anytime during the year following your return and tell the physician of your travel. Items to Bring With You Medicines you may need: The prescription medicines you take every day. Make sure you have enough to last during your trip. Keep them in their original prescription bottles and always in your carry-on luggage. Be sure to follow security guidelines, if the medicines are liquids. Antimalarial drugs, if traveling to a malaria-risk area in Belize and prescribed by your doctor. Medicine for diarrhea, usually over-the-counter. Note: Some drugs available by prescription in the US are illegal in other countries. Check the US Department of State Consular Information Sheets for the country(s) you intend to visit or the embassy or consulate for that country(s). If your medication is not allowed in the country you will be visiting, ask your health-care provider to write a letter on office stationery stating the medication has been prescribed for you. Page | 4 Other items you may need: Iodine tablets and portable water filters to purify water if bottled water is not available. See Preventing Cryptosporidiosis: A Guide to Water Filters and Bottled Water and Safe Food and Water for more detailed information. Sunblock and sunglasses for protection from harmful effects of UV sun rays. See Skin Cancer Questions and Answers for more information. Antibacterial hand wipes or alcohol-based hand sanitizer containing at least 60% alcohol. To prevent insect/mosquito bites, bring: o Lightweight long-sleeved shirts, long pants, and a hat to wear outside, whenever possible. o Flying-insect spray to help clear rooms of mosquitoes. The product should contain a pyrethroid insecticide; these insecticides quickly kill flying insects, including mosquitoes. o Bed nets treated with permethrin, if you will not be sleeping in an air-conditioned or wellscreened room and will be in malaria-risk areas. For use and purchasing information, see Insecticide Treated Bed Nets on the CDC malaria site. Overseas, permethrin or another insecticide, deltamethrin, may be purchased to treat bed nets and clothes. See other suggested over-the-counter medications and first aid items for a travelers' health kit. Note: Check the Air Travel section of the Transportation Security Administration website for the latest information about airport screening procedures and prohibited items. Other Diseases Found in Mexico and Central America Risk can vary between countries within this region and also within a country; the quality of in-country surveillance also varies. The following are disease risks that might affect travelers; this is not a complete list of diseases that can be present. Environmental conditions may also change, and up to date information about risk by regions within a country may also not always be available. Dengue epidemics have affected most countries in Central America in the past 5 years. Filariasis, leishmaniasis, onchocerciasis (River blindness), and American trypanosomiasis (Chagas' disease) are diseases carried by insects that also occur in this region, mostly in rural areas. Risk to the usual traveler is low. Myiasis (botfly) is endemic in Central America. Protecting yourself against insect bites (see below) will help to prevent these diseases. Gnathostomiasis (roundworms) has increased in Mexico, with many cases being reported from the Acapulco area, infection has been reported in travelers. Humans become infected by eating undercooked fish or poultry, or reportedly by drinking contaminated water. Page | 5 Foci of active transmission of leishmaniasis (predominantly cutaneous) are present in all countries in Central America. West Nile virus has been found in Mexico and may spread in Central America. Diarrhea in travelers is common and may be caused by bacteria, viruses, and parasites. Diarrhea caused by enterotoxigenic E. coli predominates, but other bacteria and protozoa (including Giardia, Cryptosporidia, and Entamoeba histolytica) can also cause diarrhea. Cases of hantavirus pulmonary syndrome have been reported from Panama. Outbreaks of leptospirosis have occurred in travelers to the area (including whitewater rafters in Costa Rica and U.S. troops training in Panama). Sporadic cases and outbreaks of coccidioidomycosis and histoplasmosis have occurred in travelers to Central America. Risky activities include disturbing soil and entering caves and abandoned mines. Cutaneous larva migrans occurs in visitors, especially those visiting beaches. For more information, see the Geographic Distribution of Potential Health Hazards to Travelers and Goals and Limitations in determining actual disease risks by destination Staying Healthy During Your Trip Prevent Insect Bites Many diseases, like malaria and dengue, are spread through insect bites. One of the best protections is to prevent insect bites by: Using insect repellent (bug spray) with 30%-50% DEET. Picaridin, available in 7% and 15% concentrations, needs more frequent application. There is less information available on how effective picaridin is at protecting against all of the types of mosquitoes that transmit malaria. Wearing long-sleeved shirts, long pants, and a hat outdoors. Remaining indoors in a screened or air-conditioned area during the peak biting period for malaria (dusk and dawn). Sleeping in beds covered by nets treated with permethrin, if not sleeping in an air-conditioned or wellscreened room. Spraying rooms with products effective against flying insects, such as those containing pyrethroid. For detailed information about insect repellent use, see Insect and Arthropod Protection. Page | 6 Be Careful about Food and Water Diseases from food and water are the leading cause of illness in travelers. Follow these tips for safe eating and drinking: Wash your hands often with soap and water, especially before eating. If soap and water are not available, use an alcohol-based hand gel (with at least 60% alcohol). Drink only bottled or boiled water, or carbonated (bubbly) drinks in cans or bottles. Avoid tap water, fountain drinks, and ice cubes. If this is not possible, learn how to make water safer to drink. Do not eat food purchased from street vendors. Make sure food is fully cooked. Avoid dairy products, unless you know they have been pasteurized. Diseases from food and water often cause vomiting and diarrhea. Make sure to bring diarrhea medicine with you so that you can treat mild cases yourself. Avoid Injuries Car crashes are a leading cause of injury among travelers. Protect yourself from these injuries by: Not drinking and driving. Wearing your seat belt and using car seats or booster seats in the backseat for children. Following local traffic laws. Wearing helmets when you ride bikes, motorcycles, and motor bikes. Not getting on an overloaded bus or mini-bus. Hiring a local driver, when possible. Avoiding night driving. Other Health Tips To avoid animal bites and serious diseases (including rabies and plague) do not handle or pet animals, especially dogs and cats, If you are bitten or scratched, wash the wound immediately with soap and water and seek medical attention to determine if mediation or anti-rabies vaccine is needed. To avoid infections such as HIV and viral hepatitis do not share needles for tattoos, body piercing, or injections. To reduce the risk of HIV and other sexually transmitted diseases always use latex condoms. To prevent fungal and parasitic infections, keep feet clean and dry, and do not go barefoot, especially on beaches where animals may have defecated. Page | 7 After You Return Home If you are not feeling well, you should get medical attention and mention that you have recently traveled. If you have visited a malaria-risk area, continue taking your chloroquine for 4 weeks after leaving the risk area. Malaria is always a serious disease and may be a deadly illness. If you become ill with a fever or flu-like illness either while traveling in a malaria-risk area or after you return home (for up to 1 year), you should seek immediate medical attention and should tell the physician your travel history. Important Note: This document is not a complete medical guide for travelers to this region. Consult with your doctor for specific information related to your needs and your medical history; recommendations may differ for pregnant women, young children, and persons who have chronic medical conditions. Map Disclaimer - The boundaries and names shown and the designations used on maps do not imply the expression of any opinion whatsoever on the part of the Centers for Disease Control and Prevention concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Approximate border lines for which there may not yet be full agreement are generally marked. Page Located on the Web at http://wwwn.cdc.gov/travel/destinationBelize.aspx Page | 8 Outbreak Notice Update: Dengue, Tropical and Subtropical Regions This information is current as of today, January 29, 2008 at 12:23 Updated: September 19, 2007 Dengue has become one of the most common viral diseases transmitted to humans by the bite of infected mosquitoes (usually Aedes aegypti); it is the most common cause of fever in travelers returned from the Caribbean, Central America, and South Central Asia.* Symptoms of dengue include fever, severe headache, retro-orbital eye pain (pain behind the eye), joint and muscle pain, and rash. Dengue can produce a range of illness from mild to severe, as well as fatal hemorrhagic fever. Travelers are at risk for dengue infection if they travel to or reside in areas where dengue virus is transmitted; the preventive measures outlined below can reduce their risk. Dengue Risk Areas The range of areas where dengue is located has rapidly expanded in recent years. Today it includes many tropical countries in Southeast Asia, the Indian Subcontinent, the South Pacific, the Caribbean, South and Central America, northeastern Australia, and Africa. See the Distribution of dengue maps for areas where it is present most of the time. Risk of infection is related to mosquito exposure, which can vary with the season. The mosquitoes that transmit dengue breed in man-made and natural containers, which are especially common in and around houses; therefore, dengue is common where many houses are clustered. Currently, an outbreak of dengue is being reported in French Polynesia and Palau in the South Pacific. Singapore is also experiencing an increase in dengue cases this year. As of June 30, 2007, the outbreak of dengue in Paraguay was reported to be subsiding. Other areas in South and Central America and the Caribbean, such as Brazil, Guadeloupe, Martinique, Mexico, Nicaragua, and Puerto Rico, are experiencing an increase in dengue cases in 2007. Prevention Measures for Travelers No vaccine is available to prevent dengue, and there is no specific treatment other than therapeutic support. Travelers can reduce their risk by protecting themselves from mosquito bites: Use insect repellent containing DEET or Picaridin on exposed skin. DEET concentrations of 30% to 50% are effective for several hours. Picaridin, available in 7% and 15% concentrations, must be applied more frequently. When using sunscreen, apply it before insect repellent. o DEET formulations as high as 50% are recommended for both adults and children over 2 months of age. Protect infants less than 2 months of age by using a carrier draped with mosquito netting with an elastic edge for a tight fit. Wear loose, long pants and long-sleeved shirts when outdoors. Indoors, spray insecticide where the Aedes mosquito likes to linger: closets, behind curtains, and under beds. If practical, empty or cover containers containing water. Air conditioned, screened rooms furnished with mosquito nets provide further protection. Page | 9 Empty or cover containers that can collect water (e.g., uncovered barrels, flower vases, or cisterns), because mosquitoes that transmit dengue breed in standing water. Aedes mosquitoes, the principal mosquito vector, usually are active at dusk and dawn, but may feed at any time during the day, especially indoors, in shady areas, or when the weather is cloudy. Unlike malaria, dengue is often transmitted in urban as well as in rural areas. Additional Information Proper diagnosis of dengue is important; many other diseases may mimic dengue and health-care providers should consider dengue, malaria, and (in South Asia and countries bordering the Indian Ocean), chikungunya in the differential diagnosis of patients who have fever and a history of travel to tropical areas during the 2 weeks before symptom onset. See Dengue and Dengue Hemorrhagic Fever: Information for HealthCare Practitioners for information regarding reporting dengue cases and instructions for specimen shipping. Serum samples obtained for viral identification and serologic diagnosis can be sent through state or territorial health departments to CDC's Dengue Branch, Division of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne and Enteric Diseases, 1324 Calle Cañada, San Juan, Puerto Rico 00920-3860; telephone, 787-706-2399; fax, 787-706-2496. For more information about dengue and protection measures, see the following links: Dengue Fever in CDC Health Information for International Travel 2008 Insect and Arthropod Protection Questions and Answers: Insect Repellent Use and Safety Overview of dengue from CDC Division of Vector-Borne Infectious Diseases For more information about dengue in travelers, see Travel-Associated Dengue—United States, 2005 [MMWR 2006, 55 (25)]. Travel-Associated Dengue Infections—United States, 2001-2004 [MMWR 2005, 54 (22)] For more information about recent dengue outbreaks, see Pan American Health Organization http://www.paho.org/english/ad/dpc/cd/dengue.htm South East Asia-Region/WHO (SEARO) http://www.searo.who.int/EN/Section10/Section332_1098.htm * Freedman DO, Weld LH, Kozarsky PE, Fisk T, Robins R, von Sonnenburg F, et al.; for the GeoSentinel Surveillance Network. Spectrum of disease and relation to place of exposure among ill returned travelers. N Engl J Med 2006;354:119-130 Page Located on the Web at http://wwwn.cdc.gov/travel/contentDengueTropicalSubTropical.aspx Page | 10 Dengue Fever Description Dengue fever and dengue hemorrhagic fever (DHF) are viral diseases transmitted by Aedes mosquitoes, usually Aedes aegypti. The four dengue viruses (DEN-1 through DEN-4) are immunologically related, but do not provide cross-protective immunity against each other. Occurrence Dengue, a disease found in most tropical and subtropical areas of the world, has become the most common arboviral disease of humans. More than 2.5 billion persons now live in areas where dengue infections can be locally acquired (1). Reported attack rates for disease during epidemics range from 1 per hundred to 1 per thousand of the population (2). However, because persons with milder illness may not seek medical attention and subsequently be reported, the actual number of infections in a population may be 5 to 10 times greater than the number reported. Epidemics caused by all four virus serotypes have become progressively more frequent and larger in the past 25 years. As of 2005, dengue fever is endemic in most tropical countries of the South Pacific, Asia, the Caribbean, the Americas, and Africa (see Maps 4-1, 4-2). Additionally, most tropical urban centers in these regions have multiple dengue virus serotypes co-circulating (hyperendemicity), which is associated with increased dengue transmission and the appearance of DHF. Future dengue incidence in specific locales cannot be predicted accurately, but a high level of dengue transmission is anticipated in all tropical areas of the world for the indefinite future. The incidence of the severe disease, DHF, has increased dramatically in Southeast Asia, the South Pacific, and the American tropics in the past 25 years, with major epidemics occurring in many countries every 3-5 years. The first major epidemic in the Americas occurred in Cuba in 1981, and a second occurred in Venezuela in 19891990 (3,4). Since then, outbreaks and rates of endemic, confirmed DHF have occurred in most tropical American countries. After an absence of 35 years, several locally acquired cases of dengue fever occurred in southern Texas in 1980 associated with epidemic dengue in adjacent states in Mexico (5). In the last decade, such dengue cases have been identified in Texas every 1 to 5 years. The most recent cases in 2005 included the first locally acquired DHF case in the continental United States (6). After an absence of 56 years, a limited outbreak of dengue fever occurred in Hawaii in 2001, associated with imported cases arriving from areas with epidemic dengue in the South Pacific (7). Page | 11 MAP 4-01 Distribution of dengue, Western Hemisphere. Risk for Travelers The principal mosquito vector, Ae. aegypti, is most frequently found in or near human habitations and prefers to feed on humans during the daytime. It has two peak periods of biting activity: in the morning for several hours after daybreak and in the late afternoon for several hours before dark. Nevertheless, the mosquito may feed at any time during the day, especially indoors, in shady areas, or when it is overcast. Mosquito breeding sites include artificial water containers such as discarded tires, uncovered water storage barrels, buckets, flower vases or pots, cans, and cisterns. Cases of dengue fever and DHF are confirmed every year in travelers returning to the United States after visits to tropical and subtropical areas (8). Studies of military and relief workers placed the estimated risk for travelers returning from dengue-endemic areas near one illness per thousand travelers (9, 10). This estimate may overstate the danger for tourists who may have less contact with the vector when they stay only a few days in air-conditioned hotels with well-kept grounds, or when they participate in outdoor recreational activities where the vector mosquito may be absent (such as sunbathing or playing golf in the middle of the day). A recent study of tourists visiting Hawaii during a dengue outbreak in 2001 failed to identify serologic evidence of dengue infection among over 3,000 travelers; however, this study was limited by the fact that only persons sick enough to seek medical attention received dengue testing (11). As a result, milder dengue infections that did not require medical attention might have been missed. Moreover, travelers who stay in the homes of friends and relatives in locations with intense disease transmission may have a higher risk of illness. Therefore, travelers to endemic and epidemic areas should take precautions to avoid mosquito bites (see Chapter 2). Page | 12 Current data suggest that co-circulation of all four dengue strains in the same geographic region, virus genotype, and host factors such as immune status (i.e., having had a previous dengue infection), age, and genetic background are the most important risk factors for developing DHF (12). In Asia, where a high proportion of the population has experienced a dengue infection early in life, DHF is observed most commonly in infants and children younger than 15 years of age who are experiencing a second dengue infection. In the Americas and the Pacific, where primary infection at a young age is less common, DHF is typically observed in older children and adults. Therefore, international travelers from nonendemic areas (such as the United States) are generally at low risk for DHF. There is little information in published reports about the consequences of dengue infection for pregnant women. No convincing evidence demonstrating an association between dengue infection during pregnancy and congenital malformations has been reported. However, if the mother is ill with dengue at the time of delivery, the child can be born with dengue infection or can acquire dengue through the delivery process itself, and then develop the manifestations of dengue fever or DHF (13). Passive transplacental transfer of maternal anti-dengue antibodies acquired from a previous maternal infection can also place infants at greater risk of DHF with their first dengue infection, but these maternal antibodies are cleared by 9-12 months of age (14,15). Transfusion-related dengue infection is a theoretical possibility (16). MAP 4-02 Distribution of dengue, Eastern Hemisphere. Clinical Presentation Dengue fever is characterized by sudden onset after an incubation period of 3-14 days (most commonly 4-7 days) of high fevers, severe frontal headache, and joint and muscle pain. Many patients have nausea, vomiting, and a maculopapular rash, which appears 3-5 days after onset of fever and can spread from the torso to the arms, legs, and face. The disease is usually self-limited, although convalescence can be Page | 13 prolonged. Most patients report a nonspecific viral syndrome or a flu-like illness. Asymptomatic infections are also common. Although these patients do not experience symptoms at the time of the acute infection, the immunity that results increases the risk for DHF during a subsequent infection. Approximately 1% of patients with dengue infection progress to DHF. As the patient’s fever resolves, usually 3-5 days following the onset of fever, patients may develop leaky capillaries, which allow serum proteins and fluid to accumulate in the pleural and abdominal cavities. Thrombocytopenia and hemorrhagic manifestations, which can range from microscopic hematuria or increased menstrual flow to hemetemesis, are part of the syndrome. Neutropenia, elevated liver enzymes, and disseminated intravascular coagulation are also common. The case-fatality ratio for DHF averages about 5% worldwide, but can be kept below 1% with proper clinical management. Dengue shock syndrome is the progression of DHF to a hypotensive state. Despite the name, the progression of DHF to DSS is primarily due to capillary leakage rather the hemorrhaging (12). Physicians should consider dengue in the differential diagnosis of all patients who have fever and a history of travel to a tropical area within 2 weeks of onset of symptoms. Commercial tests are available for serologic diagnosis, but their results must be interpreted with care. Sensitivity and specificity of kits may vary among manufacturers, laboratories, and over time. In combination with a compatible travel history and symptom profile, anti-dengue IgM positivity suggests a recent dengue infection, but IgG positivity may only indicate infection at an indeterminate time in the past. Both anti-dengue IgM and IgG antibodies cross-react with anti-West Nile, -yellow fever, -Japanese encephalitis, and -other flavivirus anti-bodies; therefore, prior infection or vaccination with another flavivirus may also result in positive anti-dengue antibody results. If testing at CDC is requested, acute- and convalescent-phase serum samples (collected 0-5 days and 6-30 days from fever onset, respectively) should be obtained and sent through state or territorial health department laboratories to CDC’s Dengue Branch, Division of Vector-Borne Infectious Diseases (DVBID), National Center for Infectious Diseases, 1324 Calle Cañada, San Juan, Puerto Rico 00920-3860. Serum samples should be accompanied by clinical and epidemiologic information, including the date of disease onset, the date of collection of the sample, and a detailed recent travel history. For additional information, the Dengue Branch can be contacted by telephone 1-787-706-2399; fax 1-787-706-2496; e-mail hseda@cdc.gov; or the DVBID website at http://www.cdc.gov/ncidod/dvbid/dengue/index.htm. Prevention No vaccine is available. Travelers should be advised that they can reduce their risk of acquiring dengue by remaining in well-screened or air-conditioned areas when possible, wearing clothing that adequately covers the arms and legs, and applying insect repellent to both skin and clothing. The most effective repellents are those containing N,N-diethylmetatoluamide (DEET) (see Chapter 2). Treatment Acetaminophen products are recommended for managing fever. Acetylsalicyclic acid (aspirin) and nonsteroidal anti-inflammatory agents (such as ibuprofen) should be avoided because of their anticoagulant properties. Salicylates (e.g., aspirin) should be especially avoided in children due to the association with Reye syndrome. Patients should be encouraged to rest and take fluids. Warning signs of progression to severe disease include abrupt change from fever to hypothermia, severe abdominal pain, prolonged vomiting, and altered mental status (e.g., irritability, confusion, lethargy). Prompt treatment of DHF with intravenous fluid can improve patient outcomes. In such cases, hospitalization with close monitoring of vital signs, fluid balance, and hematologic parameters is indicated, as well as additional supportive measures (12). Page | 14 References 1. Gubler DJ. The global emergence/resurgence of arboviral diseases as public health problems. Arch Med Res. 2002;33:330-42. 2. Pan American Health Organization. 2005: Number of reported cases of dengue & dengue hemorrhagic fever (DHF), Region of the Americas (by country and subregion). Available at: http://wwwn.cdc.gov/travel/forward.aspx?t=http://www.paho.org/English/AD/DPC/CD/dengue -cases-2005.htm. Accessed 12 July 2006. 3. Kouri GP, Guzman MG, Bravo JR, Triana C. Dengue haemorrhagic fever/dengue shock syndrome: lessons from the Cuban epidemic, 1981. Bull World Health Organ. 1989;67:375-80. 4. Pan American Health Organization. Dengue hemorrhagic fever in Venezuela. Epidemiol Bull. 1990;11:7-9. 5. CDC. Dengue–Texas. MMWR Morbid Mortal Wkly Rep. 1980;29:451. 6. Lacayo M, Taylor R, Duran H, Abell A, et al. Outbreak investigation of dengue—Texas, 2005 (Latebreaker). Presented at 54th Annual Meeting: American Society of Tropical Medicine and Hygiene. Washington, DC, December 11-15, 2005. 7. Effler PV, Pang L, Kitsutani P, Vorndam V, Nakata M, Ayers T, et al., and Hawaii Dengue Outbreak Investigation Team. Dengue Fever, Hawaii, 2001–2002. Emerg Infect Dis. 2005;11:5:742-749. 8. CDC. Travel-associated dengue —United States, 2005. MMWR Morbid Mortal Wkly Rep. 2006;55:22:700-2. 9. Trofa AF, DeFraites RF, Smoak BL, Kanesathasan N, King AD, Burrous JM, et al. Dengue fever in US military per-sonnel in Haiti. JAMA. 1997;277:1546-8. 10. O’Leary DR, Rigau-Pérez JG, Hayes EB, Vorndam AV, Clark GG, Gubler DJ. Assessment of Dengue risk in relief workers in Puerto Rico after Hurricane Georges. Am J Trop Med Hyg. 2002;66:35-39. 11. Smith CE, Tom Tammy, Sasaki J, Ayers T, Effler PV. Dengue risk among visitors to Hawaii during an outbreak. Emerg Infect Dis. 2005;11:750-66. 12. Rigau-Pérez JG, Clark GC, Gubler DJ, Reiter P, Sanders EJ, Vorndam AV. Dengue and dengue haemorrhagic fever. Lancet. 1998;352:971-7. 13. García-Rivera EJ, Rigau-Pérez JG. Dengue virus. In: Scott GB, Hutto SC, eds. Diagnosis of congenital and perinatal infections: a concise guide. Totowa, NJ: Humana Press, 2005:189-99. 14. Kliks SC, Nimmanitya S, Nisalak A, Burke DS. Evidence that maternal dengue antibodies are important in the development of dengue hemorrhagic fever in infants. Am J Trop Med Hyg. 1988;38:411–9. 15. Fernandez R, Rodriguez T, Borbonet F, Vasquez S, Guzman M, Kouri G. Estudio de la relacion dengue-embarazo en un grupo de madres cubanas. Rev Cubana Med Trop. 1994;46:76–8. 16. Beatty ME, Biggerstaff B, Rigau J, Petersen L. Estimated risk of transmission of dengue virus through blood transfusion in Puerto Rico (#126). At 5th International Conference on Emerging Infectious Diseases. Atlanta, GA. March 19-22, 2006. MARK E BEATTY, GARY G CLARK Page Located on the Web at http://wwwn.cdc.gov/travel/yellowBookCh4-DengueFever.aspx Page | 15 Outbreak Notice Update: 2007 Measles and Mumps Outbreaks This information is current as of today, January 29, 2008 at 12:25 Updated: May 17, 2007 Measles and mumps remain common diseases in many parts of the world. For US travelers, the risk for exposure to measles and mumps can be high, and both diseases can be prevented by the MMR (measles, mumps, rubella) vaccine. Worldwide, more than 20 million people get sick with measles each year; of these cases, 345,000 are fatal. Measles cases occur in all regions of the world: Southeast Asia (14 million cases), Africa (3.5 million cases), Eastern Mediterranean (2 million cases), Western Pacific (1 million cases), Europe (170,000 cases) and the Americas (<1,000 cases). Mumps is endemic in all regions of the world, including in many developed countries. Currently, numerous measles outbreaks are ongoing worldwide, including an outbreak in Japan in the Western Pacific Region, that has resulted in imported cases into the U.S. However, in 2007, the majority of US import-associated cases have been linked to India. Recent cases of mumps have been reported in Nova Scotia, New Brunswick, Prince Edward Island, and Ontario, Canada . The large outbreak of mumps that occurred in the United Kingdom in 2005-6 has waned, although mumps remains endemic there. Recommendations for travelers All travelers should be fully immunized and keep a copy of their immunization records with them as they travel. Children o 12 months or older should receive 2 doses of MMR vaccine separated by at least 28 days, with the first dose administered on or after the first birthday. o 6–11 months of age, if they must travel outside the US, should receive single-antigen measles vaccine before departure if it is available, or MMR if single-antigen measles vaccine is not available. (Note: MMR given before 12 months of age should not be counted as part of the series. Children who receive MMR before age 12 months will need 2 more doses of MMR, the first of which should be administered at 12 months of age.) Adolescents and Adults o who have received 2 doses of live measles- or mumps-containing vaccine are generally considered immune to measles and mumps. o are also considered immune to measles and mumps if they have had the diagnosis documented by a physician, laboratory evidence of immunity, or were born before 1957. o who cannot be considered immune based on the above criteria should receive 2 doses of MMR vaccine, separated by at least 28 days. Page | 16 Information about Measles Measles is a serious disease. Some people who become sick with measles also get an ear infection (7%-9%), diarrhea (8%), or a serious lung infection, such as pneumonia (1%-6%). One of 1,500 people with measles develops inflammation of the brain. In the United States in recent years, approximately 1-3 of every 1,000 people with measles have died . Measles can cause especially severe disease in people who are malnourished or immunosuppressed (i.e., HIV infection, leukemia, lymphoma, or generalized malignancy) or in persons receiving certain drugs or radiation therapies. Information about Mumps Mumps is an infection of the salivary glands caused by a virus. It spreads through direct contact with respiratory droplets or saliva from an infected person. Early symptoms include fever, headache, and muscle aches; fewer than half of infected people may have the characteristic swelling of the glands close to the jaw. Mumps infection can lead to meningitis, inflammation of the testicles or ovaries, inflammation of the pancreas, and deafness, which may be permanent. Information about the Vaccine The MMR vaccine also provides protection against rubella (German measles). Rubella is caused by a virus that is spread through droplet transmission. It can cause a rash, mild fever, and arthritis (mostly in women). If a woman gets rubella while she is pregnant, she could have a miscarriage or her baby could be born with serious birth defects, such as deafness, cataracts, or mental retardation. Since the introduction of vaccines containing measles, rubella, or mumps vaccine viruses—and later the combined measles-mumps-rubella (MMR) vaccine—in the United States, the numbers of reported cases of measles, mumps, and rubella, and of birth defects caused by rubella infection (congenital rubella syndrome) have decreased substantially. However, routine surveillance and vaccination remain necessary because of the continuing possibility that these diseases may be introduced from other countries. For more information, see the following links: Lancet 2007; 369:191-200 General Information on Outbreaks of Mumps in Canada MMR vaccine (MMWR Recommendations and Reports, May 22, 1998) Measles, mumps, and rubella (National Immunization Program website) Measles outbreaks in Europe (Eurosurveillance website) Measles (Health Information for International Travel) Mumps (Health Information for International Travel) Rubella (Health Information for International Travel) Page Located on the Web at http://wwwn.cdc.gov/travel/contentMeaslesMumpsOutbreaks.aspx Page | 17 Hepatitis, Viral, Type A Description Hepatitis A is a viral infection of the liver caused by hepatitis A virus (HAV). HAV infection may be asymptomatic or its clinical manifestations may range in severity from a mild illness lasting 1-2 weeks to a severely disabling disease lasting several months. Clinical manifestations of hepatitis A often include fever, malaise, anorexia, nausea, and abdominal discomfort, followed within a few days by jaundice (1). Occurrence HAV is shed in the feces of persons with HAV infection. Transmission can occur through direct person-toperson contact; through exposure to contaminated water, ice, or shellfish harvested from sewagecontaminated water; or from fruits, vegetables, or other foods that are eaten uncooked and that were contaminated during harvesting or subsequent handling. HAV infection is common (high or intermediate endemicity) throughout the developing world, where infections most frequently are acquired during early childhood and usually are asymptomatic or mild. In developed countries, HAV infection is less common (low endemicity), but communitywide outbreaks still occur in some areas of the United States. Map 4-3 indicates the seroprevalence of antibody to HAV (total anti-HAV) as measured in selected cross-sectional studies among each country’s residents. The seroprevalence of anti-HAV provides an estimate of the endemicity of HAV infections, including asymptomatic infections, within a population (2). Page | 18 MAP 4-03 Prevalence of antibody to hepatitis A virus, by country, 2006. Risk for Travelers Hepatitis A is one of the most common vaccine-preventable infections acquired during travel (3,4). The number of cases associated with travel, as well as the overall incidence, has decreased in recent years, according to notifiable disease data in the United States and Europe (3,5). However, the proportion of overall cases attributed to travel has increased in the United States. Among reported cases in persons younger than 15 years old, 40% were associated with travel (5). The risk for acquiring HAV infection for U.S. residents traveling abroad varies with living conditions, length of stay, and the incidence of HAV infection in the area visited. Travelers to North America (except Mexico), Japan, Australia, New Zealand, and developed countries in Europe are at no greater risk for infection than in the United States. For travelers to other countries, risk for infection increases with duration of travel and is highest for those who live in or visit rural areas, trek in back-country areas, or frequently eat or drink in settings of poor sanitation. Nevertheless, many cases of travel-related hepatitis A occur in travelers to developing countries with â¬Sstandardâ¬ý tourist itineraries, accommodations, and food consumption behaviors (2). Clinical Presentation The incubation period for hepatitis A averages 28 days (range 15-50 days). Hepatitis A typically has an abrupt onset of symptoms that can include fever, malaise, anorexia, nausea, abdominal discomfort, dark urine, and jaundice. The likelihood of having symptoms with HAV infection is related to the infected person’s age. In children younger than 6 years old, most (70%) infections are asymptomatic; if illness does occur, its duration is usually less than 2 months. No chronic or long-term infection is associated with hepatitis A, but 10% of infected persons will have prolonged or relapsing symptoms over a 6- to 9-month Page | 19 period. The overall case-fatality rate among cases reported to CDC is 0.3%; however, the rate is 1.8% among adults older than 50 years of age (1). Prevention Hepatitis A vaccine, immune globulin (IG), or both, are recommended for all susceptible persons traveling to or working in countries with an intermediate or high endemicity of HAV infection. Health-care providers should administer hepatitis A vaccination for persons traveling for any purpose, frequency or duration to countries that have high or intermediate endemicity of HAV infection (1). In addition, health-care providers should be alert to opportunities to provide vaccination for all travelers whose plans might include travel at some time in the future to an area of high or intermediate endemicity, including those whose current medical evaluation is for travel to an area where hepatitis A vaccination is not currently recommended. VACCINE AND IMMUNE GLOBULIN Two monovalent hepatitis A vaccines are currently licensed in the United States for persons at least 12 months of age: HAVRIX, manufactured by GlaxoSmithKline (Table 4-3), and VAQTA (manufactured by Merck & Co., Inc.) (Table 4-4). Both vaccines are made of inactivated hepatitis A virus adsorbed to aluminum hydroxide as an adjuvant. HAVRIX is prepared with 2-phenoxyethanol as a preservative, while VAQTA is formulated without a preservative. All hepatitis A vaccines should be administered intramuscularly in the deltoid muscle (1). TWINRIX, manufactured by GlaxoSmithKline, is a combined hepatitis A and hepatitis B vaccine licensed for persons >18 years of age, containing 720 EL.U. of hepatitis A antigen (50% of the HAVRIX adult dose) and 20 µg of recombinant hepatitis B surface antigen protein (the same as the ENGERIX-B adult dose) (Table 4-5). Primary immunization consists of three doses, given on a 0-, 1-, and 6-month schedule, the same schedule as that commonly used for monovalent hepatitis B vaccine. TWINRIX contains aluminum phosphate and aluminum hydroxide as adjuvants and 2-phenoxyethanol as a preservative. An accelerated schedule of Twinrix (i.e., doses at days 0, 7, and 21) for travelers has been approved by the FDA. A booster dose should be given at 1 year. The first dose of hepatitis A vaccine should be administered as soon as travel to countries with high or intermediate endemicity is considered. One month after receiving the first dose of monovalent hepatitis A vaccine, 94%-100% of adults and children will have protective concentrations of antibody. The final dose in the hepatitis A vaccine series is necessary to promote long-term protection. The immunogenicity of TWINRIX is equivalent to that of the monovalent hepatitis vaccines when tested after completion of the licensed schedule. Many persons will have detectable antibody to hepatitis A virus (anti-HAV) response to the monovalent vaccine by 2 weeks after the first vaccine dose. The proportion of persons who develop a detectable antibody response at 2 weeks may be lower when smaller vaccine dosages are used, such as with the use of TWINRIX. Travelers who receive hepatitis A vaccine less than 2 weeks before traveling to an endemic area and who do not receive immune globulin (either by choice or because of lack of availability) likely will be at lower risk of infection than those who do not receive hepatitis A vaccine or IG. In the case of travel within 4 weeks of vaccine administration, a dose of immune globulin (0.02 mL/kg) may be given alone or in addition to hepatitis A vaccine, at a different site, for optimal protection. In the case of unavailability or refusal of immune globulin, administration of hepatitis A vaccine alone for this group is recommended, but they should be informed that they are not optimally protected from acquiring hepatitis A in the immediate future (i.e., the subsequent 2-4 weeks) (1,2). Page | 20 Although vaccination of an immune traveler is not contraindicated and does not increase the risk of adverse effects, screening for total anti-HAV before travel can be useful in some circumstances to determine susceptibility and eliminate unnecessary vaccination or IG prophylaxis of immune travelers. Such serologic screening for susceptibility might be indicated for adult travelers who are likely to have had prior HAV infection if the cost of screening (laboratory and office visit) is less than the cost of vaccination or IG prophylaxis and if testing will not delay vaccination and interfere with timely receipt of vaccine or IG before travel. Such travelers may include those older than 40 years of age and those born in areas of the world with intermediate or high endemicity. Postvaccination testing for serologic response is not indicated (1). Using the vaccines according to the licensed schedules is preferable. However, an interrupted series does not need to be restarted. Given their similar immunogenicity, a series that has been started with one brand of monovalent vaccine (i.e., HAVRIX or VAQTA) may be completed with the other brand. Hepatitis A vaccine may be administered at the same time as IG or other commonly used vaccines for travelers, at different injection sites (1,2). In adults and children who have completed the vaccine series, anti-HAV has been shown to persist for at least 5-12 years after vaccination. Results of mathematical models indicate that after completion of the vaccination series, anti-HAV will likely persist for 20 years or more. For children and adults who complete the primary series, booster doses of vaccine are not recommended (6). Serologic testing to assess antibody levels after vaccination is not indicated. Travelers who are younger than 12 months of age, are allergic to a vaccine component, or otherwise elect not to receive vaccine should receive a single dose of IG (0.02 mL/kg), which provides effective protection against HAV infection for up to 3 months (Table 4-6). Those who do not receive vaccination and plan to travel for longer than 3 months should receive an IG dose of 0.06 mL/kg, which must be repeated if the duration of travel is longer than 5 months (1,7). Adverse Reactions Among adults, the most frequently reported side effects occurring 3-5 days after a vaccine dose are tenderness or pain at the injection site (53%-56%) or headache (14%-16%). Among children, the most common side effects reported are pain or tenderness at the injection site (15%-19%), feeding problems (8% in one study), or headache (4% in one study). No serious adverse events in children or adults that could be definitively attributed to the vaccine or increases in serious adverse events among vaccinated persons compared with baseline rates have been identified (1). Immune globulin for intramuscular administration prepared in the United States has few side effects (primarily soreness at the injection site) and has never been shown to transmit infectious agents (hepatitis B virus, hepatitis C virus [HCV], or HIV). Since December 1994, all IG products commercially available in the United States have had to undergo a viral inactivation procedure or be negative for HCV RNA before release (1). Precautions and Contraindications These vaccines should not be administered to travelers with a history of hypersensitivity to any vaccine component. HAVRIX or TWINRIX should not be administered to travelers with a history of hypersensitivity reactions to the preservative 2-phenoxyethanol. TWINRIX should not be administered to persons with a history of hypersensitivity to yeast. Because hepatitis A vaccine consists of inactivated virus and hepatitis B vaccine consists of a recombinant protein, no special precautions need to be taken for vaccination of immunocompromised travelers (1). Page | 21 Pregnancy The safety of hepatitis A vaccine for pregnant women has not been determined. However, because hepatitis A vaccine is produced from inactivated HAV, the theoretical risk to either the pregnant woman or the developing fetus is thought to be very low. The risk of vaccination should be weighed against the risk of hepatitis A in women travelers who might be at high risk for exposure to HAV. Pregnancy is not a contraindication to using IG.> OTHER PREVENTION TIPS Boiling or cooking food and beverage items for at least 1 minute to 185°F (85°C) inactivates HAV. Foods and beverages heated to this temperature and for this length of time cannot serve as vehicles for HAV infection unless they become contaminated after heating. Adequate chlorination of water as recommended in the United States will inactivate HAV. Travelers should be advised that, to minimize their risk of hepatitis A and other enteric diseases in developing countries, they should avoid potentially contaminated water or food. Travelers should also be advised to avoid drinking beverages (with or without ice) of unknown purity, eating uncooked shellfish, and eating uncooked fruits or vegetables that are not peeled or prepared by the traveler personally (see Chapter 2) (8). TABLE 4-03. Licensed schedule for HAVRIX1 AGE GROUP DOSE NO. OF SCHEDULE 2 VOLUME (YRS) (EL.U.) DOSES (MONTHS) 1-18 720 0.5 mL 2 0, 6 to 12 ≥19 1,440 1.0 mL 2 0, 6 to 12 1 2 Hepatitis A vaccine, inactivated, GlaxoSmithKline EL.U. = enzyme-linked immunosorbent assay (ELISA) units TABLE 4-04. Licensed schedule for VAQTA1 AGE GROUP DOSE NO. OF SCHEDULE VOLUME (YRS) (EL.U.)2 DOSES (MONTHS) 1-18 25 units 0.5 mL 2 0, 6 to 18 ≥19 50 units 1.0 mL 2 0, 6 to 18 1 Hepatitis A vaccine, inactivated, Merck & Co., Inc. TABLE 4-05. Licensed schedule for TWINRIX1 AGE GROUP DOSE NO. OF SCHEDULE VOLUME 2 (YRS) (EL.U.) DOSES (MONTHS) 2 ≥18 720 EL.U / 20 μg 1.0 mL 3 0, 1, 6 months 0, 7, 21 days ≥18 720 EL.U2 / 20 μg 1.0 mL 4 + 1 year 1 2 Combined hepatitis A and hepatitis B vaccine, GlaxoSmithKline EL.U. = enzyme-linked immunosorbent assay (ELISA) units Page | 22 TABLE 4-06. Recommended doses of immune globulin (IG) for protection against Hepatitis A DURATION OF DOSE (mL/kg)* COVERAGE Short-term (1–2 mos) 0.02 Pre-exposure Long-term (3–5 mos) 0.06† Postexposure --0.02 SETTING *IG should be administered by intramuscular injection into either the deltoid or gluteal muscle. For children aged <12 months, IG can be administered in the anterolateral thigh muscle. †Repeat every 5 months if continued exposure to hepatitis A virus occurs. Treatment No specific treatment is available for persons with hepatitis A. Treatment is supportive. References 1. CDC. Prevention of hepatitis A through active or passive immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morbid Mortal Wkly Rep. 2006; RR 55:1-23. 2. Bell BP, Feinstone SM. Hepatitis A vaccine. In: Plotkin SA, Orenstein WA, editors. Vaccines. 4th edition. Philadelphia: W.B. Saunders, 2004. 3. Mutsch M, Spicher VM, Gut C, Steffen R. Hepatitis A virus infections in travelers, 1988-2004. Clin Infect Dis. 2006;42:490-7. 4. Bacaner N, Stauffer B, Boulware DR, Walker PF, Keystone JS. Travel medicine considerations for North American immigrants visiting friends and relatives. JAMA. 2004;291:2856-64. 5. CDC. Hepatitis Surveillance Report No. 61. 2005. Atlanta: U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. 2006. 6. van Damme P, Banatvala J, Fay O, Iwarson S, McMahon B, Van Herck K, et al. Hepatitis A booster vaccination: is there a need? Lancet. 2003;362:1065–71. 7. Winokur PL, Stapleton JT. Immunoglobulin prophylaxis for hepatitis A. Clin Infect Dis. 1992;14:5806. 8. Fiore AE. Hepatitis A transmitted by food. Clin Infect Dis. 2004;38:705-15. ANTHONY FIORE, BETH BELL Page Located on the Web at http://wwwn.cdc.gov/travel/yellowBookCh4-HepA.aspx Page | 23 Hepatitis, Viral, Type B Description Hepatitis B is caused by the hepatitis B virus (HBV). The clinical manifestations of HBV infection range in severity from no symptoms to fulminant hepatitis. Signs and symptoms of hepatitis B may include fever, malaise, anorexia, nausea, and abdominal discomfort, followed within a few days by jaundice (1). Occurrence HBV is transmitted through activities that involve contact with blood or blood-derived fluids. Such activities can include unprotected sex with an HBV-infected partner; shared needles used for injection of illegal drugs; work in health-care fields (medical, dental, laboratory, or other) that entails direct exposure to human blood; receiving blood transfusions that have not been screened for HBV; or having dental, medical, or cosmetic (e.g., tattooing or body piercing) procedures with needles or other equipment that are contaminated with HBV. In addition, open skin lesions, such as those due to impetigo, scabies, or scratched insect bites, can play a role in HBV transmission if direct exposure to wound exudates from HBV-infected persons occurs (1,2). The prevalence of chronic HBV infection is low (<2%) in the general population in Northern and Western Europe, North America, Australia, New Zealand, Mexico, and Southern South America (Map 4-4). In the United States and many other developed countries, children and adolescents are routinely vaccinated against hepatitis B. The highest incidence of dis-ease is in younger adults, and most HBV infections are acquired through unprotected sex with HBV-infected partners or through shared needles used for injection drug use. The prevalence of chronic HBV infection is intermediate (2%-7%) in South Central and Southwest Asia, Israel, Japan, Eastern and Southern Europe, Russia, most areas surrounding the Ama-zon River basin, Honduras, and Guatemala. The prevalence of chronic HBV infection is high (>8%) in all socioeconomic groups in certain areas: all of Africa; Southeast Asia, including China, Korea, Indonesia, and the Philippines; the Middle East, except Israel; South and Western Pacific islands; the interior Amazon River basin; and certain parts of the Caribbean (Haiti and the Dominican Republic) (1,2). Risk for Travelers The risk of HBV infection for international travelers is generally low, except for certain travelers in countries where the prevalence of chronic HBV infection is high or intermediate. Modes of HBV transmission in areas with high or intermediate prevalence of chronic HBV infection that are important for travelers to consider are contaminated injection and other equipment used for health care-related procedures and blood transfusions from unscreened donors. Unprotected sex and sharing illegal drug injection equipment are also risks for HBV infection in these areas (1,2). Page | 24 Clinical Presentation The incubation period of hepatitis B averages 120 days (range 45-160 days). Constitutional symptoms such as malaise and anorexia may precede jaundice by 1-2 weeks. Clinical symptoms and signs include nausea, vomiting, abdominal pain, and jaundice. Skin rashes, joint pains, and arthritis may occur. The case-fatality rate is approximately 1%. Acute HBV infection causes chronic (long-term) infection in 30%-90% of persons infected as infants or children and in 6%-10% of adolescents and adults. Chronic infection can lead to chronic liver disease, liver scarring (cirrhosis), and liver cancer (1). MAP 4-04 Prevalence of chronic infection with hepatitis B virus, by country, 2006 Prevention VACCINE Hepatitis B vaccination is currently recommended for all U.S. residents who work in health-care fields (medical, dental, laboratory, or other) that involve potential exposure to human blood (3,4). All unvaccinated United States children and adolescents (younger than 19 years old) should receive hepatitis B vaccine (5). In addition, unvaccinated persons who have indications for hepatitis B vaccination independent of travel should be vaccinated, such as men who have sex with men, injection drug users, and heterosexuals who have recently had a sexually transmitted disease or have had more than one partner in the previous 6 months (4,6). Hepatitis B vaccination should be administered to all unvaccinated persons traveling to areas with intermediate to high levels of endemic HBV transmission (i.e., with hepatitis B surface antigen [HBsAg] prevalence >2%). As part of the pre-travel education process, all travelers should be given information about the risks of hepatitis B and other bloodborne pathogens from contaminated medical equipment, injection Page | 25 drug use, or sexual activity, and informed of prevention measures (see below), including hepatitis B vaccination, that can be used to prevent transmission of HBV. Regardless of destination, all persons who might engage in practices that might put them at risk for HBV infection during travel should receive hepatitis B vaccination if previously unvaccinated. It is reasonable for physicians to consider their ability to accurately assess these potential risks when considering if hepatitis B vaccine should be offered. Any adult seeking protection from HBV infection should be vaccinated. Acknowledgment of a specific risk factor is not a requirement for vaccination (4). Two monovalent hepatitis B vaccines are currently licensed in the United States: Recombivax HB, manufactured by Merck and Co., Inc., and Engerix B, manufactured by GlaxoSmithKline. Vaccines available in the United States use recombinant DNA technology to express HBsAg in yeast, which is then purified from the cells by biochemical and bio-physical separation techniques. The usual schedule of primary vaccination consists of three intramuscular doses of vaccine. The recommended dose varies by product and the recipient’s age (Table 4-7). The vaccine is usually administered as a three-dose series on a 0-, 1-, and 6-month schedule. The second dose should be given 1 month after the first dose; the third dose should be given at least 2 months after the second dose and at least 4 months after the first dose. Alternatively, the vaccine produced by GlaxoSmithKline is also approved for administration on a four-dose schedule at 0, 1, 2, and 12 months. There is also a two-dose schedule for a vaccine produced by Merck & Co., Inc., which has been licensed for children and adolescents 11-15 years of age. Using the two-dose schedule, the adult dose of Recombivax-HB is administered, with the second dose given 4-6 months after the first dose. An interrupted hepatitis B vaccine series does not need to be restarted. A three-dose series that has been started with one brand of vaccine may be completed with the other brand (1,5). Twinrix, manufactured by GlaxoSmithKline, is a combined hepatitis A and hepatitis B vaccine licensed for persons 18 years of age or older. Primary immunization consists of three doses, given on a 0-, 1-, and 6-month schedule, the same schedule as that used for single-antigen hepatitis B vaccine (Table 4-5). Twinrix consists of inactivated hepatitis A virus and recombinant HBsAg protein, with aluminum phosphate and aluminum hydroxide as adjuvants and 2-phenoxyethanol as a preservative (1,5). Clinicians may choose to use an accelerated schedule (for either the hepatitis B vaccine or Twinrix) (i.e., doses at days 0, 7, and 21). The FDA has approved the accelerated schedule for Twinrix, but not for the monovalent hepatitis B vaccine. Persons who receive a vaccination on an accelerated schedule should also receive a booster dose at 1 year after the start of the series to promote long-term immunity (7). Ideally, vaccination should begin at least 6 months before travel so the full vaccine series can be completed before departure. Because some protection is provided by one or two doses, the vaccine series should be initiated, if indicated, even if it cannot be completed before departure. Optimal protection, however, is not conferred until after the final vaccine dose. There is no interference between hepatitis B vaccine and other simultaneously administered vaccine(s) or with IG. The optimum site of injection in adults is the deltoid muscle. Long-term studies of healthy adults and children indicate that immunologic memory remains intact for at least 15 years and confers protection against chronic HBV infection, even though hepatitis B surface antibody (anti-HBs) levels can become low or decline below detectable levels. For children and adults whose immune status is normal, booster doses of vaccine are not recommended. Serologic testing to assess antibody levels is not necessary for most vaccinees. (See Chapter 8, for a discussion of the hepatitis B immunization schedule for infants who will be traveling [5,8].) Adverse Reactions Hepatitis B vaccines have been shown to be very safe for persons of all ages. Pain at the injection site (3%29%) and elevated temperature higher than 37.7°C (99.9°F) (1%-6%) are the most frequently reported side effects among vaccine recipients. In placebo-controlled studies, these side effects were reported no more Page | 26 frequently among persons receiving hepatitis B vaccine than among those receiving placebo. Among children receiving both hepatitis B vaccine and diphtheria-tetanus-pertussis (DTP) vaccine, these mild side effects have been observed no more frequently than among children receiving DTP vaccine alone. For hepatitis A vaccine (a component of the combination hepatitis A/hepatitis B vaccine Twinrix), the most frequently reported adverse reactions occurring within 3-5 days were soreness or pain at the injection site and headache. No serious adverse events among children or adults that could be definitively attributed to hepatitis A vaccine or increases in serious adverse events among vaccinated persons compared with baseline rates have been identified (1,5). Precautions and Contraindications These vaccines should not be administered to persons with a history of hypersensitivity to any vaccine component, including yeast. The vaccine contains a recombinant protein (HBsAg) that is noninfectious. Limited data indicate that there is no apparent risk of adverse events to the developing fetus when hepatitis B vaccine is administered to pregnant women. HBV infection affecting a pregnant woman can result in serious disease for the mother and chronic infection for the newborn. Neither pregnancy nor lactation should be considered a contraindication for vaccination (1,5). Behavioral preventive measures are similar to those for HIV infection and AIDS. When seeking medical or dental care, travelers should be advised to be alert to the use of medical, surgical, and dental equipment that has not been adequately sterilized or disinfected, reuse of contaminated equipment, and unsafe injecting practices (e.g., reuse of disposable needles and syringes). HBV and other bloodborne pathogens can be transmitted if tools are not sterile or if the tattoo artist or piercer does not follow other proper infection-control procedures (e.g., washing hands, using latex gloves, and cleaning and disinfecting surfaces and instruments). Travelers should be advised to consider the health risks in deciding to get a tattoo or body piercing in areas where adequate sterilization or disinfection procedures might not be available or practiced (see Chapter 2). Page | 27 TABLE 4-07. Recommended doses of currently licensed formulations of hepatitis B vaccine GROUP SINGLE-ANTIGEN VACCINE COMBINATION VACCINE RECOMBIVAX ENGERIX-B COMVAX1 PEDIARIX2 TWINRIX3 HB DOSE (μg)4 Infants (<1 year) Children (1 - 10 years) Adolescents VOLUME (mL) DOSE (μg)44 VOLUME (mL) DOSE (μg)44 VOLUME (mL) DOSE (μg)44 VOLUME (mL) DOSE (μg)44 VOLUME (mL) 57 5 0.5 0.5 107 10 0.5 0.5 5 5 0.5 0.5 10 10 0.5 0.5 NA5 NA NA NA 106 1.0 NA NA NA NA NA NA NA NA 5 10 0.5 1.0 10 20 0.5 1.0 NA NA NA NA NA NA NA NA 203 20 1.03 1.0 5 0.5 10 0.5 NA NA NA NA NA NA 408 10 409 2.0 NA NA NA NA NA NA 11 - 15 years 11 - 19 years Adults (>20 years) Hemo- dialysis patients and other immuno- compromised persons <20 years7 ≥20 years 1 1Combined hepatitis B-Haemophilus influenzae type b conjugate vaccine. This vaccine cannot be administered before age 6 weeks or after age 71 months. 2 Combined hepatitis B-diphtheria, tetanus, pertussis-inactivated poliovirus vaccine. This vaccine cannot be administered at birth, before age 6 weeks, or after age 7 years. 3 Combined hepatitis A and hepatitis B vaccine. This vaccine is recommended for persons older than 18 years who are at increased risk for both hepatitis A virus and hepatitis B virus infections. 4 Recombinant hepatitis B surface antigen dose. 5 Not applicable. 6 Adult formulation administered on a 2-dose schedule. 7 Higher doses might be more immunogenic, but no specific recommendations have been made. 8 Dialysis formulation administered on a 3-dose schedule at 0, 1, 6 months. 9 Two 1.0-mL doses administered at one site, on a 4-dose schedule at 0, 1, 2, and 6 months. Treatment No specific treatment is available for acute illness caused by hepatitis B. Antiviral drugs are approved for the treatment of chronic hepatitis B (9). References Page | 28 1. Mast E, Mahoney F, Kane M, et al. Hepatitis B vaccine. In: Plotkin SA, Orenstein WA, editors. Vaccines. 4th ed. Philadelphia: W.B. Saunders; 2004. 2. Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe injections in the developing world and transmission of bloodborne pathogens: a review. Bull World Health Organ. 1999;77:789-800. 3. CDC. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV and HIV and recommendations for postexposure prophylaxis. MMWR Morbid Mortal Wkly Rep. 2001;50(RR-11):1-54. 4. CDC. Hepatitis B virus: a comprehensive strategy for eliminating transmission in the United States through universal childhood vaccination. Recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR Morbid Mortal Wkly Rep. 1991;40 (RR-13):1-25. 5. CDC. A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part 1: Immunization of Infants, Children, and Adolescents. MMWR Morbid Mortal Wkly Rep. 2005;54(RR16);1-23 6. CDC. Provisional Recommendations for Hepatitis B Vaccination of Adults—October 2005. Available at: http://www.cdc.gov/nip/recs/provisional_recs/hepB_adult.pdf. Accessed 31 October 2006. 7. Bock HL, Loscher T, Scheiermann N, Baumgarten R, Wiese M, Dutz W, et al. Accelerated schedule for hepatitis B immunization. J Travel Med. 1995;2:213-7. 8. European Consensus Group on Hepatitis B Immunity. Are booster immunisations needed for lifelong hepatitis B immunity? Lancet. 2000;355:561-5. 9. Lok AS, McMahon BJ; Practice Guidelines Committee, American Association for the Study of Liver Diseases (AASLD). Chronic hepatitis B: update of recommendations. Hepatology. 2004:39:857-61. ANTHONY FIORE, BETH BELL Page Located on the Web at http://wwwn.cdc.gov/travel/yellowBookCh4-HepB.aspx Page | 29 Typhoid Fever Description Typhoid fever is an acute, life-threatening febrile illness caused by the bacterium Salmonella enterica serotype Typhi. Occurrence An estimated 22 million cases of typhoid fever and 200,000 related deaths occur worldwide each year (1). Approximately 400 cases of typhoid fever among persons with onset of illness in the United States, most of whom are recent travelers, are reported to CDC each year. Risk for Travelers Risk is greatest for travelers to South Asia and developing countries in Asia, Africa, the Caribbean, and Central and South America. Travelers to South Asia are at highest risk for infections that are nalidixic acidresistant or multidrug-resistant (i.e., resistant to ampicillin, chloramphenicol, and trimethoprimsulfamethoxazole) (2). Travelers who are visiting relatives or friends and who may be less likely to eat only safe foods (cooked and served hot) and beverages (carbonated beverages or those made from water that has been boiled) are at greater risk. Travelers have acquired typhoid fever even during brief visits of less than 1 week to countries where the disease is endemic (3). Clinical Presentation The hallmark of typhoid infection is persistent, high fever as high as 103° to 104° F (39° to 40° C). Other common symptoms and signs include headache, malaise, anorexia, splenomegaly, a rash of flat, rose-colored spots, and relative bradycardia (4). Many mild and atypical infections occur. Prevention Typhoid vaccination is not required for international travel, but CDC recommends it for travelers to areas where there is a recognized risk of exposure to S. Typhi. Vaccination is particularly recommended for those who will be traveling in smaller cities, villages, and rural areas off the usual tourist itineraries, where food and beverage choices may be more limited. While immunization is recommended, travelers should be cautioned that none of the available typhoid vaccines is 100% effective, nor do they provide cross-protection against other common causes of gastrointestinal infections. Typhoid vaccination is not a substitute for careful selection of food and drink (see Chapter 2). VACCINE Page | 30 Two typhoid vaccines are currently available in the United States: an oral live, attenuated vaccine (Vivotif Berna vaccine, manufactured from the Ty21a strain of S. Typhi by the Swiss Serum and Vaccine Institute) and a Vi capsular polysaccharide vaccine (ViCPS) (Typhim Vi, manufactured by sanofi pasteur) for intramuscular use. Both vaccines protect 50%-80% of recipients (5,6). The intramuscular heat-phenolinactivated vaccine (manufactured by Wyeth-Ayerst) was discontinued in 2000. Combined hepatitis A/typhoid fever vaccines are not licensed in the United States, but may be available in other countries (7). Table 4-21 provides information on vaccine dosage, administration, and revaccination. The time required for primary vaccination differs for the two vaccines, as do the lower age limits. Primary vaccination with oral Ty21a vaccine consists of four capsules, one taken every other day. The capsules should be kept refrigerated (not frozen), and all four doses must be taken to achieve maximum efficacy. Each capsule should be taken with cool liquid no warmer than 37° C (98.6° F), approximately 1 hour before a meal. This regimen should be completed 1 week before potential exposure. The vaccine manufacturer recommends that Ty21a not be administered to infants or children younger than 6 years of age. Primary vaccination with ViCPS consists of one 0.5-mL (25-µg) dose administered intramuscularly. One dose of this vac-cine should be given at least 2 weeks before expected exposure. The manufacturer does not recommend the vaccine for infants and children younger than 2 years of age. (See Chapter 8 for a discussion of typhoid immunization for infants who will be traveling.) Adverse Reactions Information on adverse reactions is presented in Table 4-22. Information is not available on the safety of these vaccines in pregnancy; it is prudent on theoretical grounds to avoid vaccinating pregnant women (see Chapter 9). Live, attenuated Ty21a vaccine should not be given to immunocompromised travelers, including those infected with HIV. The intramuscular vaccine presents a theoretically safer alternative for this group. The only contraindication to vaccination with ViCPS vaccine is a history of severe local or systemic reactions after a previous dose. Neither of the available vaccines should be given to persons with an acute febrile illness. Precautions and Contraindications Theoretical concerns have been raised about the immunogenicity of live, attenuated Ty21a vaccine in persons concurrently receiving antibiotics, immune globulin, or viral vaccines (9). The growth of the live Ty21a strain is inhibited in vitro by various antibacterial agents. Vaccination with Ty21a should be delayed for >24 hours after the administration of any antibacterial agent. Available data do not suggest that simultaneous administration of oral polio or yellow fever vaccine decreases the immunogenicity of Ty21a. If typhoid vaccination is warranted, it should not be delayed because of administration of viral vaccines. Simultaneous administration of Ty21a and immune globulin does not appear to pose a problem. OTHER PREVENTION See Risks from food and drink in Chapter 2. Page | 31 TABLE 4-21. Dosage and schedule for typhoid fever vaccination VACCINATION AGE (YRS) DOSE/MODE OF ADMINISTRATION NO. OF DOSES DOSING INTERVAL BOOSTING INTERVAL Oral, live, attenuated Ty21a vaccine ≥6 1 capsule1, oral 4 48 hrs Not applicable Booster ≥6 Vi Capsular polysaccharide vaccine 1 capsule1, oral 4 48 hrs Every 5 yrs Primary series Primary series ≥2 0.50 mL,intramuscular 1 Not applicable Not applicable Booster ≥2 0.50 mL,intramuscular 1 Not applicable Every 2 yrs 1 Administer with cool liquid no warmer than 37°C (98.6°F). TABLE 4-22. Common adverse reactions to typhoid fever vaccines VACCINATION Ty21a* Vi Capsular polysaccharide> AGE (YRS) 0%-5% REACTIONS DOSE/MODE OF ADMINISTRATION 0%-5% 0%-1%/td> 16%-20%/td> NO. OF DOSES Not applicable 7% erythema or induration 1 cm *The side effects of Ty21a are rare and mainly consist of abdominal discomfort, nausea, vomiting, and rash or urticaria. Treatment Specific antimicrobial therapy shortens the clinical course of typhoid fever and reduces the risk of death. Persons who may have been exposed to Salmonella enterica serotype Typhi and who develop symptoms of typhoid fever should seek medical care. Antimicrobial therapy should be guided by data on antimicrobial sensitivity, particularly for travelers to South Asia. Patients should be monitored to ensure that fever wanes within a few days of starting treatment. If fever does not subside, alternative antimicrobial agents or other foci of infection should be considered. References 1. Crump JA, Luby SP, Mintz ED. The global burden of typhoid fever. Bull World Health Organ. 2004;82(5):346-53. 2. Ackers ML, Puhr ND, Tauxe RV, Mintz ED. Laboratory-based surveillance of Salmonella serotype Typhi infections in the United States: antimicrobial resistance on the rise. JAMA. 2000;283(20):266873. Page | 32 3. Steinberg EB, Bishop R, Haber P, Dempsey AF, Hoekstra RM, Nelson JM, et al. Typhoid fever in travelers: who should be targeted for prevention? Clin Infect Dis. 2004;39:186-91. 4. Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid fever. N Engl J Med. 2002;347:1770-82. 5. Klugman KP, Gilbertson IT, Koornhof HJ, Robbins JB, Schneerson R, Schulz D, et al. Protective activity of Vi capsular polysaccharide vaccine against typhoid fever. Lancet. 1987;2:1165-9. 6. Simanjuntak CH, Paleologo FP, Punjabi NH, Darmowigoto R, Soeprawoto, Totosudirjo H, et al. Oral immunisation against typhoid fever in Indonesia with Ty21a vaccine. Lancet. 1991;338:1055-9. 7. Beeching NJ, Clarke PD, Kitchin NR, Pirmohamed J, Veitch K, Weber F. Comparison of two combined vaccines against typhoid fever and hepatitis A in healthy adults. Vaccine. 2004;23:29-35. 8. CDC. Typhoid immunization: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morbid Mortal Wkly Rep. 1994;43(RR-14):1-7. 9. Kollaritsch H, Que JU, Kunz C, Wiedermann G, Herzog C, Cryz SJ Jr. Safety and immunogenicity of live oral cholera and typhoid vaccines administered alone or in combination with antimalarial drugs, oral polio vaccine, or yellow fever vaccine. J Infect Dis. 1997;175:871-5. SHARON GREENE, ERIC MINTZ Page Located on the Web at http://wwwn.cdc.gov/travel/yellowBookCh4-Typhoid.aspx Page | 33 Rabies Description Rabies is an acute, progressive, fatal encephalomyelitis caused by neurotropic viruses in the family Rhabdoviridae, genus Lyssavirus (1,2). The disease is almost always transmitted by an animal bite that inoculates the virus into wounds. Very rarely, rabies has been transmitted by exposures other than bites that introduce the virus into open wounds or mucous membranes (3-5). All mammals are believed to be susceptible, but reservoirs are carnivores and bats. Although dogs are the main reservoir in developing countries, the epidemiology of the disease differs sufficiently from one region or country to another to warrant the medical evaluation of all mammal bites (6-8). Occurrence Rabies is found on all continents except Antarctica. In certain areas of the world, canine rabies remains highly endemic, including (but not limited to) parts of Africa, Asia, and Central and South America (8,9). Table 4-14 lists countries that have reported no cases of rabies during the most recent period for which information is available (formerly referred to as “rabies-free countries”). Additional information can be obtained from the World Health Organization (http://wwwn.cdc.gov/travel/forward.aspx?t=http://www.who.int/rabies/rabnet/en/), the Pan American Health Organization (http://wwwn.cdc.gov/travel/forward.aspx?t=http://www.paho.org/english/ad/dpc/vp/rabia.htm), the Rabies Bulletin-Europe (http://wwwn.cdc.gov/travel/forward.aspx?t=http://www.rbe.fli.bund.de), the World Organization for Animal Health (http://wwwn.cdc.gov/travel/forward.aspx?t=http://www.oie.int/eng/en_index.htm), local health authorities of the country, the embassy, or the local consulate’s office in the United States. Lists are provided only as a guide, because up to date information may not be available, surveillance standards vary, and reporting status can change suddenly as a result of disease re-introduction or emergence (10,11). Page | 34 TABLE 4-14. Countries and political units reporting no indigenous cases of rabies during 20051 REGION COUNTRIES Africa Cape Verde, Libya, Mauritius, Réunion, São Tome and Principe, and Seychelles North: Bermuda, St. Pierre and Miquelon Americas Caribbean: Antigua and Barbuda, Aruba, Bahamas, Barbados, Cayman Islands, Dominica, Guadeloupe, Jamaica, Martinique, Montserrat, Netherlands Antilles, Saint Kitts (Saint Christopher) and Nevis, Saint Lucia, Saint Martin, Saint Vincent and Grenadines, Turks and Caicos, and Virgin Islands (UK and US) South: Uruguay Asia Hong Kong, Japan, Kuwait, Lebanon, Malaysia (Sabah), Qatar, Singapore, United Arab Emirates Austria, Belgium, Cyprus, Czech Republic2, Denmark2, Finland, France2, Gibraltar, Greece, Iceland, Europe Ireland, Isle of Man, Italy, Luxemburg, Netherlands2, Norway, Portugal, Spain2 (except Ceuta/ Melilla), Sweden, Switzerland, and United Kingdom2 Australia2, Northern Mariana Islands, Cook Islands, Fiji, French Polynesia, Guam, Hawaii, Kiribati, Oceania Micronesia, New Caledonia, New Zealand, Palau, Papua New Guinea, Samoa, and Vanuatu 1 Bat rabies may exist in some areas that are reportedly free of rabies in other animals. 2 Bat lyssaviruses are known to exist in these areas that are reportedly free of rabies in other animals. 3 Most of Pacific Oceania is reportedly rabies-free. Risk for Travelers Rabies vaccination is not a requirement for entry into any country. However, travelers to rabies-endemic countries should be warned about the risk of acquiring rabies and educated in animal bite prevention strategies (12-16). Travelers with extensive unprotected outdoor exposure such as might be experienced while bicycling, camping, hiking, or engaging in certain occupational activities, might be at higher risk even if their trip is brief. Also, children are considered at higher risk because of their tendencies to play with animals and to not report bites. Casual exposure to cave air is not a concern, but cavers should be warned not to handle bats (3). Clinical Presentation After infection, the incubation period is highly variable, but lasts approximately 1-3 months. The disease progresses from a nonspecific prodromal phase to paresis or paralysis; spasms of swallowing muscles can be stimulated by the sight, sound, or perception of water (hydrophobia); delirium and convulsions can develop, followed rapidly by coma and death. No treatment is effective after the development of clinical signs, but the extremely rare case of recovery after extensive medical intervention offers hope that future experimental therapeutics may be developed (17-18). Prevention Pre-exposure vaccination with human diploid cell rabies vaccine (HDCV), or purified chick embryo cell (PCEC) vaccine, may be recommended for international travelers based on the local incidence of rabies in Page | 35 the country to be visited, the availability of appropriate antirabies biologicals, and the intended activity and duration of stay of the traveler (19). Different schedules, alternative routes of administration, and other rabies vaccines besides HDCV and PCEC may be found abroad (20,21). Pre-exposure vaccination may be recommended for veterinarians, animal handlers, field biologists, spelunkers, missionaries, and certain laboratory workers. Table 4-15 provides criteria for pre-exposure vaccination. Pre-exposure vaccination does not eliminate the need for additional medical attention after a rabies exposure but simplifies postexposure prophylaxis in populations at risk by eliminating the need for rabies immune globulin (RIG) and by decreasing the number of doses of vaccine required. Pre-exposure vaccination is of particular importance for travelers at risk of exposure to rabies in countries where biologicals are in short supply and locally available rabies vaccines might carry a higher risk of adverse reactions (20). Pre-exposure vaccination may also provide some degree of protection when there is an unapparent or unrecognized exposure to rabies and when postexposure prophylaxis might be delayed. Planning is needed to ensure compliance in completion of the three pre-exposure vaccine doses, prior to commencing travel (22). Travelers should be advised that any animal bite or scratch should receive prompt local treatment by thorough cleansing of the wound with copious amounts of soap and water (and povidone iodine, if available). This local treatment will substantially reduce the risk of rabies. Travelers who might have been exposed to rabies should be advised to always contact local health authorities immediately for advice about postexposure prophylaxis and should also contact their personal physician or state health department as soon as possible thereafter. Equine rabies immune globulin (ERIG), or purified fractions of ERIG, has been used effectively in some developing countries where human rabies immune globulin (RIG) might not be available (20). If necessary, such heterologous products are preferable to no RIG administration in human rabies postexposure prophylaxis. The incidence of adverse reactions after the use of these products has been low (0.8%-6.0%), and most of those reactions were minor. However, such products are neither evaluated by U.S. standards nor regulated by the U.S. Food and Drug Administration, and their use cannot be unequivocally recommended at this time (19). In addition, unpurified antirabies serum of equine origin might still be used in some countries where neither human RIG nor ERIG is available. The use of this antirabies serum is associated with higher rates of serious adverse reactions, including anaphylaxis. Tables 4-16 and 4-17 provide information on pre-exposure and postexposure prophylaxis. Routine serologic testing is not necessary for travelers who receive the recommended pre-exposure or postexposure regimen with HDCV or PCEC vaccines. Exposed travelers previously vaccinated with vaccines other than those produced by cell culture should receive the complete postexposure regimen unless they have developed a laboratory-confirmed virus neutralizing antibody response to the primary vaccination. Serologic testing is still recommended for travelers whose immune response might be diminished by drug therapy or by diseases. Rabies pre-exposure prophylaxis may not be indicated for travelers to the countries in Table 4-14, and postexposure prophylaxis is rarely necessary after exposures to domestic animals in these countries. Practitioners are urged to follow established current guidelines for schedules and doses of vaccine used in rabies prophylaxis (23). ADVERSE REACTIONS Travelers should be advised that they may experience local reactions after vaccination, such as pain, erythema, swelling, or itching at the injection site, or mild systemic reactions, such as headache, nausea, abdominal pain, muscle aches, and dizziness (19,20). Approximately 6% of persons receiving booster vaccinations with HDCV may experience an immune complex-like reaction characterized by urticaria, pruritus, and malaise. Once initiated, rabies postexposure prophylaxis should not be interrupted or discontinued because of local or mild systemic reactions to rabies vaccine. Page | 36 PRECAUTIONS AND CONTRAINDICATIONS Pregnancy Pregnancy is not a contraindication to postexposure prophylaxis (19,20). Age In infants and children, the dose of HDCV or PCEC for pre-exposure or postexposure prophylaxis is the same as that rec-ommended for adults (19,20). The dose of RIG for postexposure prophylaxis is based on body weight (Table 4-17). TABLE 4-15. Criteria for pre-exposure immunization for rabies RISK CATEGORY NATURE OF RISK TYPICAL POPULATIONS PREEXPOSURE REGIMEN Virus present continuously, often in high concentrations Continuous Specific exposures likely to go unrecognized Bite, non-bite, or aerosol exposure Exposure usually episodic with source recognized, but exposure might also be unrecognized Frequent Infrequent (greater than general population) Rare (general population) Bite, nonbite, or aerosol exposure possible Exposure nearly always episodic with source recognized Bite or nonbite exposure Exposure always episodic, with source recognized Rabies research laboratory workers1, rabies biologics production workers Primary course: Serologic testing every 6 months; booster vaccination if antibody titer is below acceptable level2 Rabies diagnostic laboratory workers1, cavers, veterinarians and staff, and animal control and wildlife workers in rabiesepizootic areas Primary course: Serologic testing every 2 years; booster vaccination if antibody titer is below acceptable level2 Veterinarians, animal control and wildlife workers in areas with low rabies rates; veterinary students; and travelers Primary course: No visiting areas where rabies is enzootic serologic testing or booster and immediate access to appropriate vaccination medical care, including biologics, is limited. U.S. population at large, including individuals in rabies-epizootic areas No pre-exposure immunization necessary Page | 37 1 Judgment of relative risk and extra monitoring of vaccination status of laboratory workers is the responsibility of the laboratory supervisor (see U.S. Department of Health and Human Service’s Biosafety in Microbiological and Biomedical Laboratories, 1999). 2 Preexposure booster immunization consists of one dose of human diploid cell [rabies] vaccine (HDCV), or purified chick embryo cell (PCEC) vaccine, 1.0-mL dose, intramuscular (IM) (deltoid area). Minimum acceptable antibody level is complete virus neutralization at a 1:5 serum dilution by the rapid fluorescent focus inhibition test. A booster dose should be administered if titer falls below this level. TABLE 4-16. Pre-exposure immunization for rabies1 VACCINE DOSE (mL) NO. OF DOSES SCHEDULE (DAYS) ROUTE HDCV 1.0 3 0, 7, 21 or 28 Intramuscular PCEC 1.0 3 0, 7, 21 or 28 Intramuscular HDCV, human diploid cell vaccine; PCEC, purified chick embryo cell.1Patients who are immunosuppressed by disease or medications should postpone pre-exposure vaccinations and consider avoiding activities for which rabies pre-exposure prophylaxis is indicated. When this course is not possible, immunosuppressed persons who are at risk for rabies should have their antibody titers checked after vaccination. TABLE 4-17. Postexposure immunization for rabies1 IMMUNIZATION STATUS VACCINE / PRODUCT RIG plus SCHEDULE (DAYS) ROUTE 1 0 Infiltrated at bite site (if possible); remainder intramuscular. HDCV or PCEC 1.0 mL 5 0, 3, 7, 14, 28 Intramuscular HDCV PCEC 2 0, 3 Intramuscular Not previously immunized Previously immunized2, 3 NO. OF DOSES DOSE 20 IU/kg body weight 1.0 mL RIG, rabies immune globulin; HDCV, human diploid cell (rabies) vaccine; PCEC, purified chick embryo cell. 1 All postexposure prophylaxis should begin with immediate, thorough cleansing of all wounds with soap and water. 2 Pre-exposure immunization with HDCV or PCEC; prior postexposure prophylaxis with HDCV or PCEC; or persons previously immunized with any other type of rabies vaccine and a documented history of positive antibody response to the prior vaccination. 3 RIG should not be administered. References 1. Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363:959-69. 2. Nel L. Vaccines for lyssaviruses other than rabies. Expert Rev Vaccines. 2005;4:533-40. 3. Gibbons RV. Cryptogenic rabies, bats, and the question of aerosol transmission. Ann Emerg Med. 2002;39:528-36. 4. Srinivasan A, Burton EC, Kuehnert MJ, Rupprecht C, Sutker WL, Ksiazek TG, et al. Transmission of rabies virus from an organ donor to four transplant recipients. N Engl J Med. 2005;352:1103-11. Page | 38 5. Hellenbrand W, Meyer C, Rasch G, Steffens I, Ammon A. Cases of rabies in Germany following organ transplantation. Euro Surveill. 2005;10:E050224.6. 6. Fooks AR, McElhinney LM, Pounder DJ, Finnegan CJ, Mansfield K, Johnson N, et al. Case report: isolation of a European bat lyssavirus type 2a from a fatal human case of rabies encephalitis. J Med Virol. 2003;71:281-9. 7. Taplitz RA. Managing bite wounds. Currently recommended antibiotics for treatment and prophylaxis. Postgrad Med. 2004;116:49-52, 55-6, 59. 8. Gupta RK. Recent outbreak of rabies infections in Brazil transmitted by vampire bats. Euro Surveill. 2005;10:E051110.3. 9. Knobel DL, Cleaveland S, Coleman PG, Fevre EM, Meltzer MI, Miranda ME et al. Re-evaluating the burden of rabies in Africa and Asia. Bull World Health Organ. 2005;83:360-8. 10. Hore C. Important unusual infections in Australia: a critical care perspective. Crit Care Resusc. 2001;3:262-72.11. 11. Kim CH, Lee CG, Yoon HC, Nam HM, Park CK, Lee JC, et al. Rabies, an emerging disease in Korea. J Vet Med B Infect Dis Vet Public Health. 2006;53:111-5.12. 12. Wilde H, Briggs DJ, Meslin FX, Hemachudha T, Sitprija V. Rabies update for travel medicine advisors. Clin Infect Dis. 2003;37:96-100. 13. Strauss R, Granz A, Wassermann-Neuhold M, Krause R, Bago Z, Revilla-Fernandez S, et al. A human case of travel-related rabies in Austria, September 2004. Euro Surveill. 2005;10:225-6. 14. Smith A, Petrovic M, Solomon T, Fooks A. Death from rabies in a UK traveler returning from India. Euro Surveill. 2005;10:E050728.5. 15. Rendi-Wagner P, Jeschko E, Kollaritsch H, osterreichische Expertengruppe fur Reisemedizin. Travel vaccination recommendations for Central and Eastern European countries based on country-specific risk profiles. Wien Klin Wochenschr. 2005;117 Suppl 4:11-9. 16. Richardson M. The management of animal and human bite wounds. Nurs Times. 2006;102:34-6. 17. Jackson AC, Warrell MJ, Rupprecht CE, Ertl HC, Dietzschold B, O’Reilly M, et al. Management of rabies in humans. Clin Infect Dis. 2003;36:60-3. 18. Willoughby RE Jr, Tieves KS, Hoffman GM, Ghanayem NS, Amlie-Lefond CM, Schwabe MJ, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352:2508-14. 19. CDC. Human rabies prevention — United States, 1999. Recommendations of the Advisory Committee on Immuniza-tion Practices (ACIP). MMWR Morbid Mortal Wkly Rep. 1999;48(RR1):1-21. 20. World Health Organization Expert Consultation on Rabies. World Health Organ Tech Rep Ser. 2005;931:1-88. 21. Khawplod P, Wilde H, Sirikwin S, Benjawongkulchai M, Limusanno S, Jaijaroensab W, Chiraguna N, et al. Revision of the Thai Red Cross intradermal rabies post-exposure regimen by eliminating the 90-day booster injection. Vaccine. 2006;24:3084-6. 22. Heudorf U, Tiarks-Jungk P, Stark S. Travel medicine and vaccination as a task of infection prevention. Gesundheitswesen. 2006;68:316-22. 23. Rupprecht CE, Gibbons RV. Clinical practice. Prophylaxis against rabies. N Engl J Med. 2004;351:2626-35. CHARLES E. RUPPRECHT Page Located on the Web at http://wwwn.cdc.gov/travel/yellowBookCh4-Rabies.aspx Page | 39



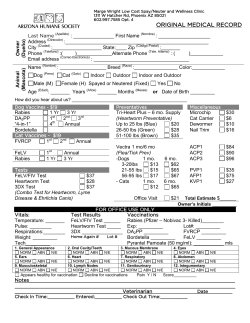







© Copyright 2025