
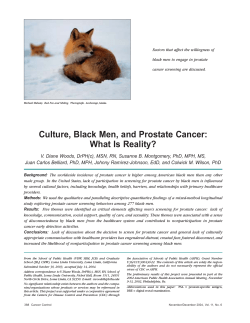
Educating African American Men about the Prostate Cancer
Educating African American Men about the Prostate Cancer Screening Dilemma: A Randomized Intervention Kathryn L. Taylor, Jackson L. Davis III, Ralph O. Turner, et al. Cancer Epidemiol Biomarkers Prev 2006;15:2179-2188. Updated version Access the most recent version of this article at: http://cebp.aacrjournals.org/content/15/11/2179 Cited Articles This article cites by 46 articles, 3 of which you can access for free at: http://cebp.aacrjournals.org/content/15/11/2179.full.html#ref-list-1 Citing articles This article has been cited by 6 HighWire-hosted articles. Access the articles at: http://cebp.aacrjournals.org/content/15/11/2179.full.html#related-urls E-mail alerts Reprints and Subscriptions Permissions Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at pubs@aacr.org. To request permission to re-use all or part of this article, contact the AACR Publications Department at permissions@aacr.org. Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2179 Educating African American Men about the Prostate Cancer Screening Dilemma: A Randomized Intervention Kathryn L. Taylor,1 Jackson L. Davis III,2 Ralph O. Turner,2 Lenora Johnson,3 Marc D. Schwartz,1 Jon F. Kerner,4 and Chikarlo Leak1 1 Cancer Control Program, Lombardi Comprehensive Cancer Center, Georgetown University Medical Center; 2Most Worshipful Prince Hall Grand Lodge of the District of Columbia, Washington, District of Columbia; 3Office of Education and Special Initiatives, The National Cancer Institute, Rockville, Maryland; and 4Division of Cancer Control and Population Sciences, National Cancer Institute, Rockville, Maryland Abstract Background: Until there is a definitive demonstration that early diagnosis and treatment of prostate cancer reduces disease-related mortality, it is imperative to promote informed screening decisions by providing balanced information about the potential benefits and risks of prostate cancer screening. Within a community/academic collaboration, we conducted a randomized trial of a printed booklet and a videotape that were designed for African American (AA) men. The purpose of the trial was to determine the effect of the interventions on knowledge, decisional conflict, satisfaction with the screening decision, and self-reported screening. Methods: Participants were 238 AA men, ages 40 to 70 years, who were members of the Prince Hall Masons in Washington, DC. Men were randomly assigned to the (a) video-based information study arm, (b) print-based information study arm, or (c) wait list control study arm. Intervention materials were mailed to men at home. Assessments were conducted at baseline, 1 month, and 12 months postintervention. Multivariate analyses, including ANCOVA and logistic regression, were used to analyze group differences. Results: The booklet and video resulted in a significant improvement in knowledge and a reduction in decisional conflict about prostate cancer screening, relative to the wait list control. Satisfaction with the screening decision was not affected by the interventions. Self-reported screening rates increased between the baseline and the 1-year assessment, although screening was not differentially associated with either of the interventions. In exploratory analyses, prostatespecific antigen testing at 1 year was more likely among previously screened men and was associated with having low baseline decisional conflict. Conclusions: This study represents one of the first randomized intervention trials specifically designed to address AA men’s informed decision making about prostate cancer screening. We have developed and evaluated culturally sensitive, balanced, and disseminable materials that improved knowledge and reduced decisional conflict about prostate cancer screening among AA men. Due to the high incidence and mortality rates among AA men, there is a need for targeted educational materials, particularly materials that are balanced in terms of the benefits and risks of screening. (Cancer Epidemiol Biomarkers Prev 2006;15(11):2179 – 88) Introduction Prostate cancer is the most commonly diagnosed cancer and the third leading cause of cancer death among men in the United States, with 234,460 expected diagnoses and 27,350 expected deaths this year (1). These statistics have led some organizations to recommend routine prostate cancer screening, particularly for men at high risk for the disease, including African American (AA) men. Compared with white men, AA men have a 60% higher incidence rate and a mortality rate that is more than double that of white men (1). However, the available data on screening outcomes are not yet definitive, leading to inconsistent screening recommendations from different professional organizations. Consequently, men and their health care providers are left to make their own decisions about the utility of screening. The efficacy of screening asymptomatic men is a contentious issue. Although surveillance data indicate that prostate Received 6/6/06; revised 8/15/06; accepted 8/23/06. Grant support: Centers for Disease Control and Prevention grant TS290 and National Cancer Institute grant K07 CA72645-01. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Requests for reprints: Kathryn L. Taylor, Cancer Control Program, Lombardi Comprehensive Cancer Center, Georgetown University Medical Center, 3300 Whitehaven Street, Northwest, Suite 4100, Washington, DC 20007. Phone: 202-687-0649; Fax: 202-687-8444. E-mail: TAYLORKL@georgetown.edu Copyright D 2006 American Association for Cancer Research. doi:10.1158/1055-9965.EPI-05-0417 cancer is being diagnosed at earlier stages and that prostate cancer mortality has decreased since the advent of prostatespecific antigen (PSA) testing (2, 3), there has not yet been a definitive demonstration that early diagnosis and treatment of prostate cancer reduces disease-related mortality. The debate centers around whether PSA testing may result in overdiagnosis, the detection of disease that otherwise would not have caused a clinical problem (4, 5), and whether the stage shift and decreased mortality are indeed due to the increased rates of screening. The National Cancer Institute’s Prostate, Lung, Colorectal, and Ovarian (PLCO) cancer screening trial is addressing these issues, but the results will not be available for several years (6). In addition to the uncertain efficacy, screening also results in a substantial false-positive rate, leading to a biopsy for a sizeable portion of disease-free men. Although the professional community debates the merits of screening (7-12), millions of asymptomatic men in the United States undergo screening each year. However, several studies have reported low knowledge and little awareness of the lack of consensus for the efficacy of screening (13-18). Most men who are screened believe that the medical community unequivocally accepts the benefits of screening. This situation parallels earlier controversies, in which hotly debated cancer screening techniques were in widespread use before the completion of definitive studies, and the tests either did (cervical cancer screening; ref. 19) or did not (lung cancer screening; ref. 20) ultimately prove effective. As the efficacy of prostate cancer screening will not be known for some time, Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2180 African American Men and Prostate Cancer Screening it is imperative to promote informed screening decisions by providing accurate and balanced information about the potential benefits, risks, and limitations of prostate cancer screening. To date, there have been 13 published randomized trials of print, verbal, videotape, and face-to-face patient education trials for prostate cancer screening (18, 21-32). Of the eight trials that have measured knowledge (18, 23-29), all have shown improved knowledge about the advantages and disadvantages of screening. Four trials measured additional psychosocial outcomes and reported that, relative to the control arms, men in the intervention arms reported lower decisional conflict at post-test (22, 24, 25) and a more active role in doctor/patient discussions (22, 29). Of the 10 trials that assessed actual screening behavior (excluding those that only measured intentions), 3 reported reduced screening among participants who received educational interventions (26-28), 4 reported no difference in screening rates (18, 22, 23, 29), and 3 reported increased screening rates in the active intervention condition (30-32). Two of the three trials that reported increased screening rates included interventions that were not informed decision making trials but were designed to increase screening (30, 32), whereas one of the trials was designed to improve informed decision making (31). A further difference is that these three trials were the only trials that have had either an exclusively AA (30, 31) or largely AA sample (32). Although AA men have been well represented in several observational studies (15, 33-38), to date only these three randomized trials have included a significant number of AA men (30-32). The present study represents a community/academic collaboration with the Most Worshipful Prince Hall Grand Lodge of the District of Columbia (Prince Hall Masons), an international, fraternal, AA organization dedicated to community service. We sought to develop and evaluate accessible and easily disseminable health communication methods that were targeted specifically to AA men and that contained balanced information about the benefits and limitations of prostate cancer screening. We selected video and print media because these were the preferred media suggested in our formative research for this project (39). Although all men need information and support in making the screening decision, it is particularly difficult for AA men, given their high-risk status, the prevalence of the disease among friends and family, and the fact that the focus of the media and much of the medical establishment is on increasing screening. As a result of these factors, particularly strongly held beliefs in support of screening may already be in place (39), making it particularly challenging to communicate the existence of a controversy. A final reason for developing and evaluating materials for AA men is that much of what is known about men’s understanding of the controversy and effective methods to communicate that controversy has been conducted in studies that primarily consisted of samples of Caucasian men. Our goal was to develop balanced materials that were specifically designed for AA men and that did not provide a recommendation for or against screening but encouraged men to reach their own decision in collaboration with their doctor and family members. We conducted a randomized clinical trial to evaluate the effect of a printed booklet and a videotape intervention and hypothesized that both interventions would result in increased knowledge, decreased decisional conflict, and increased decisional satisfaction at the 1-month assessment, relative to a wait list control group. We also evaluated the effect of the materials on self-reported screening behavior assessed 1 year following the intervention and conducted exploratory analyses of predictors of screening behavior. Materials and Methods Participants. Participants were members of the Most Worshipful Prince Hall Grand Lodge of the District of Columbia (Washington, DC). Inclusion criteria were the following: 40 to 70 years of age, no history of prostate cancer, and not having been a participant in the focus groups conducted for the formative research. Prior screening was not an exclusion criterion. Participants were accrued between January 2001 and August 2002 and follow-up interviews were completed by July 2003. The Georgetown University Institutional Review Board approved this study and informed consent was obtained from each subject. Figure 1 presents the study procedures, baseline accrual rate, retention rates at each stage of the study, and reasons for subject attrition. Loss to follow-up between baseline and the 1-month interviews was equally distributed across the three arms [X 2 (277) = 0.56; P > 0.20]. The reasons for loss to followup at the 1-month assessment are presented in Fig. 1. Compared with the 238 participants who completed the 1-month assessment (n = 119 in the print arm and n = 119 in the video arm), the 39 noncompleters were more likely to be as follows: younger (P < 0.01), unmarried (P < 0.01), and working (P < 0.05). For the 1-year assessment, 193 completed the mailed questionnaire, an 81% (193 of 238) retention rate since the 1-month assessment, a 65.6% (193 of 294) overall retention rate, and 62.9% (185 of 294) completed all three assessments. Due to incomplete data (see Fig. 1), 164 subjects were available for analysis at 1 year. We assessed whether the 74 noncompleters of the 12-month interview differed from the 164 completers. Completers were more likely to have been screened in the past year than the noncompleters: PSA [X 2 (237) = 6.6; P = 0.01] and digital rectal examination [DRE; X 2 (237) = 3.2; P = 0.07]. There were no other demographic or screening differences between completers and noncompleters, including age, education, marital status, employment status, family history of prostate cancer, or intention to be screened in the future. Procedure. The Most Worshipful Prince Hall Grand Lodge of the District of Columbia consists of 27 groups (lodges), each containing 100 or more members. Within each lodge, a lodge coordinator was designated to identify interested men. The lodge coordinators discussed the project at lodge meetings, distributed project brochures, identified interested men, and were paid $50 for their assistance in accruing participants. The Lombardi Comprehensive Cancer Center research assistant called the interested men to describe the study further, obtain verbal consent, enroll eligible men, and conduct the baseline interview. Following completion of the baseline interview, participants were randomly assigned to one of three arms: (a) video-based information, (b) print-based information, or (c) wait list control (see Fig. 1). Participants in the print and videotape arms were mailed a cover letter, the intervention materials, and the written consent form. The cover letter included a statement about the rationale for the study, length of time needed to watch the video/read the booklet, instructions about return of the consent form, a reminder about the upcoming 1-month follow-up interview, a request to not share the intervention materials with other Masons (to prevent contamination between groups), and phone numbers to call for more information. We did not provide information about local prostate cancer screening locations, as the goal of the study was not to provide men with a particular screening opportunity but to provide an educational intervention and then to measure whether men sought screening (as well as measurement of the three other outcome variables). Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention 2181 Figure 1. Study procedures. After 1 month, video and print arm participants completed the first follow-up telephone assessment. Men who reported that they had not yet had a chance to read/watch the materials were given an additional week to do so and called again to complete the follow-up assessment. Men in the wait list arm were called 1 month following study enrollment to complete their baseline interview (see Fig. 1). Following their baseline interview, wait list participants were randomly assigned to either the print or videotape arm. After 1 month, wait list participants were called for their first follow-up interview. All participants were mailed $25 for their participation following completion of the 1-month interview. At 1-year postintervention, all participants completed a brief mailed questionnaire to assess whether men had been screened postintervention. We used a wait list control group due to community collaborators’ concerns that a ‘no treatment’ control would adversely affect participation and retention rates and add to participant burden. As a result of these concerns, we did not use a traditional wait list control, in which participants complete two interviews before the intervention. Rather, wait list participants completed a single preintervention interview that occurred 1 month following randomization but before their receipt of the intervention (Fig. 1). The timing of the baseline assessment for the wait list group coincided with the 1-month assessments of the print and videotape arms, providing a randomized comparison group who had not yet been exposed to an intervention. After completing their delayed baseline assessment, wait list participants were randomized to one of the two active intervention arms. Development of the Intervention Materials. The development of the videotape and booklet are described in detail elsewhere (39, 40). Briefly, to determine the educational needs of AA men between 40 to 70 years of age, we conducted a series of eight focus groups with members of the Prince Hall Mason as well as two focus groups with urologists and internists. The print and video materials were designed to be identical in content and to provide a balanced presentation of the benefits and the limitations of prostate cancer screening. Our research team consisted of five AA health professionals (two urologists, a registered nurse, and two Master of Public Health-level health educators), two AA men who were members of the Masons, the Centers for Disease Control and Prevention behavioral science staff (as this was funded by a cooperative agreement from the Centers for Disease Control and Prevention), and the Georgetown University behavioral science staff. Each of these groups was closely involved in the writing and production of the intervention materials and reviewed them at each step during their development. Further, as some team members were in support of screening for AA men and others were more conservative in their view of screening, all members of the team had a vested interest in insuring that the message was balanced and was not slanted toward one decision or the other. Although we did not test whether the materials were balanced according to a lay group of AA men, they were considered balanced by a group of community members and a group of experts. Printed Guide. The 16-page, three-color, printed guide includes prostate cancer symptoms, anatomy and function, prostate cancer risk factors, the benefits and limitations of screening, sample questions for men to ask their doctors, and a glossary of terms (40). Frank Robinson, the Hall of Fame baseball player and the first AA manager of a major league Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2182 African American Men and Prostate Cancer Screening baseball team, as well as a prostate cancer survivor, was highlighted as the celebrity spokesperson. Although Frank Robinson is a prostate cancer survivor, this was not a widely known fact at the time that this study was completed. Most importantly, in the intervention materials, Mr. Robinson did not refer to himself as a survivor and his message was completely neutral (i.e., along with the advice of professionals and your family, the choice is yours about whether you are tested for prostate cancer). There was no mention of Mr. Robinson’s own screening practices or of his treatment choices for prostate cancer. Videotape. The 25-minute videotape focuses on a middleaged AA man as he discusses prostate cancer screening with his friends, family, and doctor. The videotape shows his attempts to understand the screening dilemma, including his fears, doubts, and questions about prostate cancer. In the doctor’s office, he is shown with diagrams of the prostate and the rationale for and against screening. The videotape also included Frank Robinson as the celebrity spokesperson. Measures Demographic and Medical Information. We assessed age, education, marital status, employment status, access to and utilization of medical care, availability of health insurance, personal history of cancer, and family history of prostate cancer. Prostate Cancer Screening History, Intentions, and Behavior. We assessed participants’ self-reported prostate cancer screening history, prior abnormal findings, and the results of subsequent work-ups. Subjects’ intent to undergo screening was assessed at baseline and 1 month using the following question: Do you plan to undergo prostate cancer screening within the next year (rated on a five-point scale from ‘definitely’ to ‘definitely not’). At the 1-year assessment, subjects’ self-reported screening behavior in the past year was assessed: When were you last tested for prostate cancer (month/date for PSA and for DRE or never). Although there are limitations of self-reported prostate cancer screening (41, 42), verification of screening in this community-based study was not feasible given the number of possible places where screening may occur. Process Variables. At the 1-month assessment, we assessed men’s use and perception of the intervention materials (see Table 2 for the list of items assessed). Prostate Cancer Knowledge. Based on our prior research (17), we developed an 11-item knowledge scale. Items were drawn from (a) the National Cancer Institute Cancer Facts sheet on prostate cancer, (b) a qualitative study of patients’ and experts’ opinions of what men should be told about prostate cancer screening (43), and (c) a study of prostate screening by Volk et al. (44). The measure assessed symptoms of prostate cancer, the controversy surrounding screening, risk factors for prostate cancer, false-positive and false-negative results, and the natural history of the disease. The response format was true/ false/don’t know. ‘Don’t know’ was coded as an incorrect response. Correct items were summed to form a total score. Decisional Conflict Scale. We used the 10-item version of the decisional conflict scale (DCS) (45). The 10-item version has a three-level response format (yes, no, and unsure) and the items were worded in the form of a question. A higher score indicates greater decisional conflict. Two items were excluded as they were confusing to pilot subjects (‘Are you choosing without pressure from others’ and ‘Do you know which options are available to you’). The a reliability of the eight-item total score was 0.76. Due to the skewed responses (the majority of subjects had low decisional conflict), we dichotomized the total score for use in the analyses. Satisfaction with the Screening Decision. We assessed satisfaction with a single item, ‘Are you satisfied with your decision about prostate cancer testing.’ Participants responded on a four-point scale, from ‘very satisfied’ to ‘not at all satisfied.’ As the majority reported that they were ‘very satisfied,’ we used a dichotomized score in the analyses. Data analytic Strategy and Power Calculation. We conducted the data analyses in several steps. We evaluated baseline group differences on the demographic, medical, and process variables (Tables 1 and 2). We have presented the following analyses for each outcome variable. First, for each outcome variable, we evaluated baseline group differences and whether there were within group changes from baseline to 1 month Table 1. Baseline demographic and medical characteristics Age (mean, SD), y Education <High school degree Some college >College degree Married Employment status Working (full time/part time) Retired VCR at home Regular doctor Have insurance Family history of prostate cancer Personal cancer history Ever had a DRE DRE within past year* Plan to have DRE within next year Ever had a PSA PSA within past year*,c b Plan to have PSA within next year DRE and PSA within past year Print (n = 84), % Video (n = 80), % Wait list* (n = 74), % Entire sample (N = 238), % 56.6 (7.8) 56.3 (7.8) 55.1 (8.6) 56.0 (8.0) 28.6 46.4 25.0 77.4 29.1 32.9 38.0 70.0 29.7 45.9 24.3 79.7 29.1 41.8 29.1 75.6 67.9 31.0 98.8 95.2 98.8 20.2 1.2 86.9 53.6 81.0 61.9 41.7 81.0 35.7 63.8 36.3 98.8 92.5 98.8 20.0 1.3 92.5 50.6 78.8 65.8 49.4 90.0 37.5 77.0 18.9 98.6 94.6 98.6 16.4 2.7 87.8 44.6 77.0 63.5 40.5 94.6 27.0 69.3 29.0 98.7 94.1 98.7 19.0 1.4 89.1 49.6 79.0 63.4 43.7 88.2 33.6 *Percentages for DRE and PSA in past year is the percentage of the entire samples not just those who have ever been screened. This makes these percentages comparable with screening in past year at the 1-year assessment. cWhen the wait list participants are collapsed into their respective print or video arms, there is a single group difference on ‘PSA within the past year,’ which is greater among video arm Ss (P < 0.05). This variable is controlled in multivariate analyses, in which the wait list arm is combined with the print and video arms and in the analyses predicting PSA completion at the 1-year assessment. bP < 0.05. Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention 2183 Table 2. Participants’ evaluation of the print and video interventions at the 1-month assessment Watched/read the materials Once Two or more times Discussed prostate screening with others (yes) Learned new information (yes)* c Helpful in decision (very helpful) Think of questions for doctor (yes) Length about right (‘about right’) b Amount of information (‘about right’) Held your attention (yes) Made you nervous (no) Used other informational sources (yes)*,x Reading pamphlets/booklets* b Talking with friends or family Talking with your doctor* Using the internet Recalled celebrity (correct) b Recalled final information in materials (correct) Contamination between trial arms Saw material from other arm Showed intervention material to other Masons The intervention materials suggest You should be screened You should not be screened Did not suggest one decision over another Print (n = 119), % Video (n = 119), % 53.5 46.5 46.2 75.6 90.6 59.7 94.1 94.1 94.9 88.2 17.6 5.9 9.2 5.0 5.9 54.6 49.6 45.9 54.1 53.8 58.0 81.3 54.6 91.6 84.0 93.3 89.1 35.3 16.8 18.5 16.8 7.6 46.2 62.2 2.5 6.0 1.7 3.4 79.0 0 21.0 75.6 0 24.4 *P < 0.01. cP < 0.10. bP < 0.05. xLess than 3% of the sample reported using books, radio, other videos, newspaper, or TV. (Table 3). Second, to evaluate the effect of the two active interventions relative to the wait list arm, we compared the outcomes at 1 month using one-way ANCOVA, adjusting for the relevant covariates. Third, we conducted bivariate analyses between potential covariates (baseline demographic and medical variables) and the 1-month and 1-year outcome variables (Table 4). Fourth, we collapsed wait list participants into their subsequent group assignment and evaluated the effect of print versus video on each outcome variable, adjusting for the respective baseline score and covariates. A repeated measure ANCOVA was used for the continuous measure of knowledge and logistic regression was used for the dichotomized outcomes of decisional conflict and satisfaction. Finally, to test for group differences (print versus video) on the self-reported screening outcome at 1 year, we used logistic regression followed by an exploratory logistic regression analysis to identify predictors of the screening outcome. In terms of power, this study had an adequate sample size to detect our predicted effects. For example, for analyses comparing the print to video interventions after collapsing the wait list control condition, our sample size (N = 238) provided 80% power to detect differences as small as 0.36 SDs at follow-up. This minimum detectable effect size falls about midway between a small (0.20 SDs) and medium (0.50 SDs) effect (46). For analyses involving comparisons with the wait list control condition, we hypothesized a somewhat larger effect—because we were comparing active interventions to an inactive control. Thus, we powered the study to be able to detect medium effect sizes of 0.5 SDs. For continuous outcomes, we had power of 87% to detect the difference between the video and control arms and power of 88% to detect the predicted difference between the print and control arms. Results Descriptive Information. Table 1 presents demographic and medical information, stratified by group membership. There was only one significant group difference: fewer men in the print arm intended to have a PSA test within the next year (this variable was included as a covariate in subsequent analyses). The sample was well educated, (29% had a college degree) and almost all participants reported having a regular doctor and insurance. In the past year, approximately one half had received a DRE and/or a PSA test. Table 3. Descriptive information for outcome variables at baseline and 1 month Knowledge (mean, SD) Baseline 1 Month Decisional conflict (% high) Baseline 1 Month Decisional satisfaction (% high) Baseline 1 Month Print (n = 84) Video (n = 80) Wait list (n = 74) Entire sample (N = 238) 7.2 (1.5)* c 9.2 (1.4) 7.2 (1.6)* c 8.5 (1.7) 6.9 (1.3)* N/A 7.1 (1.5) 8.9 (1.5) 33.3* c 8.3 31.3* 24.1* 41.9* N/A 35.3 15.2 76.1* 84.5* 78.1* 79.7* 75.7* N/A 76.6 83.5 NOTE: The analyses to assess for baseline group differences are adjusted for the variable ‘Plan to have a PSA in the next year’ due to the baseline group difference on this variable. *There were no between group differences at baseline on any of the measures, as indicated by the like superscripts. cThere were three significant within group changes from baseline to 1 month, as indicated by the differing superscripts (* versus c). Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2184 African American Men and Prostate Cancer Screening Table 4. Bivariate analyses for 1-month and 1-year outcomes Baseline categorical predictors Levels 1-Month assessment Knowledge (N = 238) DCS (% high; N = 238) 1-Year assessment Decisional satisfaction (% high; n = 237) Screening in past year (% yes) PSA and DRE (n = 148) Age Education Marital status Employment status Regular doctor Family history of prostate cancer DRE past year PSA past year Plan to have DRE in next year Plan to have PSA in next year V55 >56 VHigh school degree Some college zCollege degree Not married Married Employed Retired No Yes No Yes No Yes No Yes No Yes No Yes 8.9 8.8 8.8 9.1 8.7 8.7 8.9 8.8 9.1 8.8 8.9 8.9 8.9 8.9 8.9 8.9 8.8 8.8 8.9 8.9 9.0 (1.5) (1.6) (1.7) (1.5) (1.4) (1.5) (1.5) (1.5)* (1.6) (1.4) (1.5) (1.6) (1.4) (1.4) (1.6) (1.4) (1.8) (1.6) (1.4) (1.5) (1.7) 10.9* 19.5 c 25.0 11.1 11.6 c 24.1 12.3 20.8 12.7 c 35.7 13.9 16.8 8.9 16.8 13.7 c 19.7 9.6 13.4 22.0 15.3 14.3 87.4 79.5 79.7 84.5 85.5 79.3 84.8 84.5 83.0 92.9 82.9 83.7 82.2 83.2 83.6 84.8 81.6 c 71.4 86.6 77.8 84.2 c 54.1 70.3 61.7 63.8 59.5 71.4 59.3 58.9 67.9 66.7 62.0 63.6 56.7 c 50.8 71.1 c 53.8 72.1 c 42.9 66.7 53.3 63.2 PSA (n = 164) DRE (n = 159) c 66.7 83.1 70.0 75.0 80.0 82.1 72.8 78.2 73.4 85.7 74.5 76.2 70.6 c 67.1 81.8 63.9x 86.4 67.6 76.9 64.7 76.2 c 63.8 78.5 68.1 72.7 71.1 81.6 67.8 78.2 67.3 71.4 71.1 72.4 64.5 b 58.8 80.2 65.9 77.5 60.7 73.3 77.8 70.2 * P < 0.10. cP < 0.05. bP < 0.01. x P < 0.001. 1-Month Outcomes Process Variables. Table 2 presents participants’ responses to the educational materials, stratified by intervention arm (wait list participants were combined into their respective intervention arms for these analyses). All participants reported reviewing the materials at least once, and the majority reported that the materials were helpful in making a screening decision, that the length and amount of information provided was about right, that the materials held their attention, and that the information did not make them nervous. Print arm participants were more likely to report that they learned new information, whereas video arm participants were significantly more likely to have used other information sources, particularly other pamphlets or booklets, talking with friends or family, or talking with their doctor. About our assessment of whether participants watched/read the materials in their entirety, only about one half correctly recalled the celebrity spokesperson, and the correct recall of the final piece of information presented was significantly better in the video arm. There was a minimal contamination between the arms. Finally, although our goal was to present a balanced picture of the pros and cons of screening, approximately three quarters of men thought that the materials suggested they should be screened, whereas one quarter thought that the materials were neutral, and no one reported that the materials discouraged screening. Knowledge. Table 3 presents descriptive information for knowledge (and the other outcome variables) at the baseline and 1-month assessments. There were no baseline group differences for knowledge. Knowledge improved significantly from baseline to the 1-month assessment within both the print [t (83) = 10.3; P < 0.0001] and video [t (79) = 5.9; P < 0.0001] arms (Table 3). Next, to determine whether the two active intervention arms improved knowledge relative to the wait list control, we conducted a one-way ANCOVA (adjusting for employment status; see Table 4). We compared the baseline assessment of the wait list group with the 1-month assessments of the print and video groups (see study design in Fig. 1). There was a significant main effect for group [F (2, 234) = 49.1; P < 0.0001]. Mean comparisons indicated that, relative to the wait list arm, knowledge was higher in the print [F (1, 155) = 112.9; P < 0.0001] and video arms [F (1, 151) = 43.2; P < 0.0001; see Fig. 2]. These analyses provide evidence that the interventions were having the expected effect on knowledge. Further, the results remained significant when the sample was limited to those who correctly recalled the celebrity spokesperson [F (2, 116) = 34.2; P < 0.0001], indicating that differential exposure to the two interventions did not explain the group differences. Next, we collapsed the wait list participants into their respective active intervention arms (print or video) and conducted a repeated measure ANCOVA adjusting for the significant covariate, employment status (see Table 4). This Figure 2. Effect of the interventions on knowledge of prostate cancer screening at the 1-month assessment. The wait list arm was assessed once before the intervention. Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention 2185 analysis revealed a significant group time interaction [F (1, 235) = 3.9; P < 0.05], indicating that the print arm resulted in improved knowledge relative to the video arm at the 1-month assessment. Neither age nor education moderated the group time interaction (Ps > 0.20). Again, when the sample was limited to those who correctly recalled the celebrity, the analysis remained significant [F (1, 117) = 5.4; P < 0.05]. Decisional Conflict. There were no baseline group differences on the DCS (Table 3). The percentage of participants reporting high decisional conflict decreased significantly from baseline to the 1-month assessment only in the print arm [X 2 (1, n = 84) = 14.8; P < 0.0001]. After adjusting for the relevant covariates (Table 4), logistic regression revealed that relative to the wait list arm, the print [odds ratio (OR), 0.098; 95% confidence interval (95% CI), 0.04-0.26] and video arms (OR, 0.46; 95% CI, 0.21-0.99) both resulted in significantly reduced decisional conflict (see Fig. 3 and Table 3). Limiting the sample to those who correctly recalled the celebrity revealed that, relative to the waitlist arm, the print (OR, 0.089; 95% CI, 0.02-0.36) resulted in significantly reduced decisional conflict, and the video arm (OR, 0.34; 95% CI, 0.10-1.07) approached a significant reduction (P = 0.065). We conducted a logistic regression, collapsing the wait list participants into their respective active intervention arms (print or video) and adjusted for baseline DCS and the significant covariates (Table 4). The print intervention resulted in significantly reduced decisional conflict, relative to the video arm (OR, 0.21; 95% CI, 0.09-0.52). Limiting the sample to those who correctly recalled the celebrity spokesperson (n = 118) resulted in similar results (OR, 0.30; 95% CI, 0.08-1.1) although attenuated due the reduced sample size. Satisfaction with the Screening Decision. There were no baseline group differences on satisfaction. Participants were highly satisfied with their screening decision at baseline and there were no within group changes in satisfaction for either the print or video arms (Table 3). In addition, the wait list arm at baseline was not significantly different from the two intervention arms at the 1-month assessment. We conducted a logistic regression, collapsing the wait list participants into their respective active intervention arms (print or video) and adjusted for the significant covariate (Table 4). Satisfaction with the screening decision was not related to intervention arm (OR, 0.64; 95% CI, 0.28-1.4). 1-Year Screening Outcomes There was an overall increase in the self-reported rate of DRE and PSA screening between the baseline and 1-year assessments. Among the men who completed the 1-year assessment, 57.2% reported having received a DRE within the past year at baseline compared with 71.1% who had received a DRE within the past year at the 1-year assessment [X 2 (1, 159) = 8.7; P < 0.01]. Similarly, 49.4% reported having had a PSA test within the past year at baseline compared with 75.0% at the 1-year assessment [X 2 (1, 164) = 11.1; P = 0.001]. For PSA and DRE combined, 38.5% reported having received both tests within the past year at baseline compared with 62.2% at the 1-year assessment [X 2 (1, 148) = 11.1; P = 0.001]. As the wait list participants were provided with the intervention before the 1-year assessment, we were not able to determine the effect of interventions on screening relative to no intervention. We assessed whether the interventions were differentially associated with self-reported completion of either of the screening tests at the 1-year assessment. In a logistic regression predicting whether men had had a DRE within the year following the intervention, we controlled for DRE in the year before baseline (OR, 2.7; 95% CI, 1.3-5.6) and age (OR, 1.6; 95% CI, 0.75-3.3) on step 1 followed by intervention arm (OR, 1.8; 95% CI, 0.87-3.8) on step 2. These results suggest that the print (77.0%) and video (65.9%) arms were not significantly associated with having had a DRE in the past 12 months. None of the baseline values of the knowledge or decisional variables interacted with intervention group to predict the DRE outcome. In the logistic regression predicting whether men reported having had a PSA during the year following the intervention, we controlled for PSA (OR, 2.9; 95% CI, 1.2-7.2) and DRE in the year before baseline (OR, 1.2; 95% CI, 0.52-2.9) and age (OR, 1.7; 95% CI, 0.76-3.7) on step 1 followed by intervention arm (OR, 1.5; 95% CI, 0.69-3.1) on step 2. These results also indicated that intervention arm was not related to having had a PSA in the 12 months following the intervention (77.9% in the print arm versus 72.4% in the video arm). Similarly, intervention arm was not related to having both a PSA and a DRE (OR, 1.6; 95% CI, 0.79-3.3). As reported above for the DRE analyses, the baseline values of the knowledge and decisional variables did not interact with intervention group to predict PSA screening (or the PSA/DRE combined) at 1 year. Exploratory Analyses of 1-year Screening Rates. Given that the interventions were not differentially related to either of the screening outcomes at 1 year, we conducted exploratory analyses to determine whether any of the baseline knowledge or decisional variables were predictive of the increase in screening. We collapsed the print and video arms into one group and controlled for intervention arm in the multivariate analyses. There was only one significant bivariate association with self-reported screening rates at 1 year: high baseline decisional conflict was significantly associated with a lower rate of PSA screening at 1-year [X 2 (164) = 4.5; P < 0.05; Table 5]. We conducted a hierarchical logistic regression analysis to determine whether decisional conflict would remain in the model predicting PSA screening after adjusting for the relevant covariates (Table 4). For the final model predicting PSA screening, prior DRE screening (OR, 1.1; 95% CI, 0.48-2.7), older age (OR, 1.9; 95% CI, 0.83-4.2), and the intervention arm (OR, 1.5; 95% CI, 0.70-3.3) were not significantly associated with the outcome. Prior PSA screening (OR, 2.7; 95% CI, 1.16.8) was significantly associated with PSA screening at 1 year. There was a marginally significant association between lower decisional conflict at baseline and having undergone screening at 1 year (OR, 2.1; 95% CI, 0.98-4.7; P = 0.056). Discussion Figure 3. Effect of the interventions on decisional conflict at the 1-month assesment. This study represents one of the first randomized interventions designed to address informed decision making about prostate cancer screening among AA men. As hypothesized, the interventions resulted in improved prostate cancer knowledge and reduced decisional conflict about screening, relative to the wait list control. Satisfaction with the screening decision was not affected by the interventions, largely due to very high baseline satisfaction. Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2186 African American Men and Prostate Cancer Screening Table 5. Evaluation of baseline knowledge and decisional predictors of screening at 1 year PSA (n = 164), % Screened Knowledge Low 56.9 High 43.1 Decisional conflict Low 71.5 High 28.5 Decisional satisfaction Low 21.1 High 78.9 DRE (n = 159), % Not screened PSA and DRE (n = 148), % Screened Not Screened Screened with both Screened with none or 1 51.2 48.8 63.7 36.3 47.8 52.2* 58.7 41.3 53.6 46.4 53.7 c 46.3 72.6 27.4 63.0 37.0 73.9 26.1 58.9 41.1* 33.3 66.7 21.4 78.6 27.5 72.5 20.0 80.0 30.0 70.0 *P < 0.10. cP < 0.05. Our findings replicate prior prostate cancer informed decision making trials, as each of the eight trials that measured knowledge also reported a significant improvement in knowledge in the intervention arm, relative to the control arm (18, 23-29). Compared with other trials, our sample began with a much higher level of knowledge, as on average, 65% of items were answered correctly at baseline, compared with other samples, in which f30% of items were answered correctly at baseline (e.g., refs. 25, 44). In these prior studies, the percentage of correct knowledge items improved by 20% to 25% in the intervention conditions, whereas, in our study, they improved slightly less, presumably due to the high baseline scores: 14% (video) to 18% (print arm) improvement in the percentage answered correctly. About decisional conflict, the three prostate screening informed decision making trials that have measured it also reported lower decisional conflict in the intervention arm, relative to the control arm (22, 24, 25). These studies used a summed measure of the 16-item DCS; thus, we were unable to compare our sample to previous samples on this measure. To date, there are no published studies on any topic that have used the short-form of the DCS, although there are several under way. In the current study, the print intervention had a greater effect on knowledge and decisional conflict outcomes compared with the video intervention. There have been two prior randomized trials in prostate cancer screening that have compared video and print interventions (25, 29). Gattellari and Ward (25) showed that written materials had a greater effect on knowledge and decisional conflict when compared with the video, whereas Partin et al. (29) found that the video condition resulted in greater knowledge than the print condition (decisional conflict was not measured). As different intervention materials were used in each of these three studies, it is difficult to determine whether group differences were due to the quality of the actual materials or to the medium, in which they were delivered. However, we speculate that in our study, these differences may have been due to the relative ease of rereading sections of the booklet and perhaps due to this age cohort’s greater familiarity with using print materials for obtaining health information compared with using a videotape. About screening behavior, our results were contrary to several randomized trials in informed decision making in prostate cancer screening, which have reported that screening rates decreased following the intervention (18, 22, 23, 26-29). However, our results corroborated two other studies that have found a significant increase in screening following exposure to a decision tool, one with AA men (31), and another that found this result among a subsample of AA men (27). Whether these findings may be due to racial or cultural differences and/or to being at high risk for prostate cancer (31) is unclear at present. Our findings suggest that among men who have a considerable screening history and a favorable view of screening, balanced educational materials may serve to reduce any uncertainties that may have existed before the intervention and, in fact, strengthen previously held beliefs. This finding is somewhat counterintuitive, as it would seem that potential disadvantages would be most salient to men who are ‘pro screening.’ However, one post-hoc interpretation is that men were drawn to the information that confirmed their preexisting positive beliefs about screening, which led to the increased rates of self-reported screening. To address this possibility, we are in the development phase of a web-based decision tool designed to insure that men are exposed to the viewpoint that differs from their own. For example, men who report that they favor screening at baseline will be systematically exposed to the potential limitations of screening, and men who do not favor screening will be exposed to the potential benefits of screening. This method may help to better educate men who are highly committed to their beliefs either for or against screening. Similarly, the fact that 75% to 80% of our sample reported that the intervention suggested that men should be screened indicates that men may have selectively focused on the positive aspects of screening that were contained in the materials. Alternatively, this finding could suggest that the interventions subtly promoted screening. However, our community and expert reviewers did not find evidence for this, and as noted earlier, the bias against prostate cancer screening among several members of the team makes it unlikely that the materials favored screening. As the men who volunteered for this study had a strong screening history and clear intentions to continue screening, their interpretation that the materials favored screening (as well as their increased screening rates) may suggest that men were simply making a decision consonant with their own pre-existing values and/or that exposure to balanced materials served to deepen their existing beliefs. It will require further research to determine the extent to which these findings are related to this sample’s strong preexisting beliefs about screening, to their high-risk status, racial or cultural differences, or some combination of these factors. Participation in a prostate cancer educational study may be associated with a willingness to be screened. In a quasiexperimental study of balanced prostate cancer screening education, there was a significant increase in screening regardless of intervention arm, and previous screening was positively associated with screening postintervention (47). In exploratory analyses, we found that previously screened men and men with low baseline decisional conflict were more likely to have undergone PSA testing by the 1-year assessment. These findings corroborate the role that past screening (47) and a positive attitude toward screening (20) have in subsequent screening and lend support for the conclusions of several recent reviews of patient decision aids, which suggested that decisional factors play a role in understanding screening behavior (48-50). Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention 2187 There are multiple challenges inherent in educating patients about controversial medical procedures, such as prostate cancer screening. For numerous reasons, the public’s ability to consider the full spectrum of facts about screening effectiveness is becoming more and more limited (51). For example, due to the rapidity with which new technologies are accepted into clinical use by both physicians and patients, educational efforts have the difficult task of asking people to reconsider a decision they have already made. Further, the detrimental effect that the media has on people’s understanding of controversial public health issues has been highlighted (52) as well as the implications of the widespread enthusiasm for cancer screening (53). Therefore, innovative methods to help the public contend with increasingly complex health-related decisions are essential. For AA men, the increased prostate cancer incidence and mortality rates serve to only further complicate these already difficult issues, as there is a drive to address these disparities, and screening is the only tool available at present. Thus, until the PLCO results are released, improved methods are needed to assist men in understanding these complex issues. If the PLCO results do not provide a definitive recommendation for or against screening, then these issues will need to be addressed going forward. Thus, it is critical that we develop improved methods for fostering informed decisions for controversial medical tests and procedures. Several study limitations should be considered in the interpretation of the results. First, due to concerns about the potential for participant drop out, the wait list arm was not followed for the entire year, which meant that we did not have the ‘no treatment control’ group needed to fully understand the rate of screening at 1 year. Further, the wait list group was not measured on two consecutive occasions before the intervention. However, the strength of this design was that the delayed baseline assessment of the wait list arm coincided in time with the 1-month follow-up assessment of the two active intervention arms, providing a randomized comparison group who had not been exposed to an intervention. Second, this sample was a relatively homogenous group of AA men, in terms of education level and screening history. Thus, these results may not apply to lower SES men or an unscreened sample of AA men. However, for this initial intervention conducted with these newly developed educational materials, we believed it was preferable to obtain a more representative sample of a homogeneous group than to risk having a very low response rate in a populationbased study. Third, retention at 1 year was higher among those who had been screened previously, so the rates of self-reported screening after 1 year may have been unusually high. A fourth limitation was that we were unable to verify screening behavior by medical record review due to the fact that this was a community-based study without a specified screening location. Previous randomized trials of prostate screening decision tools, with one exception (27), have used a medical record review to assess screening outcomes. However, there are limitations of a medical record review as an assessment of screening outcomes, as men may be screened in settings other than the observed clinics; therefore, it may present an underestimate of the percentage of men who are screened (29, 31, 42). This suggests that the screening rates in the current study may be higher than in previous studies due to this measurement difference. On the other hand, self-reports of PSA testing also need to be interpreted with caution, as Chan et al. (41) has reported in an observational study that PSA screening was underreported due to men’s lack of awareness that they had been tested. Finally, it is possible that socially desirable responding may have resulted in the fact that all men reported using the materials and in the highly prevalent belief that the materials were proscreening. However, there are several other potential explanations for the report that 100% of the sample reviewed the materials. (a) When men were called for their 1-month follow-up assessment, those men who had not yet viewed the materials were called again in 1 week’s time to provide men with an additional opportunity to review the materials before completing the assessment. (b) As the proscreening response is consistent with subjects’ significant screening history, it is arguable that this was not socially desirable responding but simply a reflection of their beliefs. (c) As the materials were designed to provide a balanced picture of screening by presenting an equal number of ‘pro’ and ‘con’ viewpoints, we believe that men may have focused on the message that matched their preexisting beliefs, suggesting that the positive responses were not necessarily socially desirable but, again, just a reflection of the belief that men should be screened. Thus, although socially desirable responding may have played a role in men’s report of their use and perception of the materials, there are several equally plausible alternative explanations to these findings. Most importantly, when considering the screening outcomes of the randomized trial, socially desirable responding was equally likely to occur in the print and video arms, as both are active interventions. Therefore, socially desirable responding is unlikely to have had an effect on the conclusions made about comparisons of the print and video arms. The strength of this research began with the unique opportunity for conducting collaborative research within this community/academic partnership. The involvement of the Masonic leadership was central to overcoming many of the barriers that are typically encountered in community-based research with minority populations. We have developed and evaluated culturally sensitive, inexpensive, balanced, and disseminable materials that were successful in improving knowledge and reducing decisional conflict among AA men. Due to the high incidence and mortality rates among AA men, there is a need for targeted educational materials, particularly materials that are balanced in terms of the benefits and limitations of screening. However, it is increasingly difficult to fully educate the public about a behavior that is widely practiced and that is promulgated as a certainty by the media, suggesting that educational materials that are accessible to large groups of men will be necessary to ensure informed decision making on this topic. Finally, decision tools to help men evaluate the usefulness of screening tests must be a central aspect of educational campaigns of this kind. Providing screening to men without giving them every opportunity to understand the current state of the science is unethical. Until the results of the PLCO trial are available, the task at hand is to help men make the best decision for themselves, based on a clear understanding of the available data. References 1. 2. 3. 4. 5. 6. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin 2006;56:106 – 30. Surveillance, Epidemiology, and End Results (SEER) Program (http:// www.seer.cancer.gov) SEER*Stat Database: Mortality—All COD, Public-Use with State, Total U.S. (1969-2002), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2005. Underlying mortality data provided by NCHS (http:// www.cdc.gov/nchs). Surveillance, Epidemiology, and End Results (SEER) Program (www.seer. cancer.gov) SEER*Stat Database: Incidence-SEER 9 Registries Public-Use, Nov 2004 Submission (1973-2002), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2005, based on the November 2004 submission. Etzioni R, Berry KM, Legler JM, Shaw P. Prostate-specific antigen testing in black and white men: an analysis of medicare claims from 1991-1998. Urology 2002;59:251 – 5. Yao SL, Lu-Yao G. Understanding and appreciating overdiagnosis in the PSA era. J Natl Cancer Inst 2002;94:958 – 60. Prorok PC, Andriole GL, Bresalier RS, et al. Design of the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. Control Clin Trials 2000;21:273 – 309S. Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research. 2188 African American Men and Prostate Cancer Screening 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. Woolf SH, Rothemich SF. Screening for prostate cancer: the roles of science, policy, and opinion in determining what is best for patients. Annu Rev Med 1999;50:207 – 21. Brawley OW. Prostate cancer screening: clinical applications and challenges. Urol Oncol 2004;22:353 – 7. Partin MR, Wilt TJ. Informing patients about prostate cancer screening: identifying and meeting the challenges while the evidence remains uncertain. Am J Med 2002;113:691 – 3. Murphy AM, McKiernan JM, Olsson CA. Controversies in prostate cancer screening. J Urol 2004;172:1822 – 4. Pauker SG, Kassirer JP. Contentious screening decisions: does the choice matter? N Engl J Med 1997;336:1243 – 4. Mitka M. Is PSA testing still useful? JAMA 2004;292:2326 – 7. Diefenbach PN, Ganz PA, Pawlow AJ, Guthrie D. Screening by the prostate-specific antigen test: what do the patients know? J Cancer Educ 1996;11:39 – 44. Mercer SL, Goel V, Levy IG, Ashbury FD, Iverson DC, Iscoe NA. Prostate cancer screening in the midst of controversy: Canadian men’s knowledge, beliefs, utilization, and future intentions. Can J Public Health 1997;88: 327 – 32. Myers RE, Wolf TA, McKee L, et al. Factors associated with intention to undergo annual prostate cancer screening among African American men in Philadelphia. Cancer 1996;78:471 – 9. O’Dell KJ, Volk RJ, Cass AR, Spann SJ. Screening for prostate cancer with the prostate-specific antigen test: are patients making informed decisions? J Fam Pract 1999;48:682 – 8. Taylor KL, Shelby R, Kerner J, Redd W, Lynch J. Impact of undergoing prostate carcinoma screening on prostate carcinoma-related knowledge and distress. Cancer 2002;95:1037 – 44. Wilt TJ, Paul J, Murdoch M, Nelson D, Nugent S, Rubins HB. Educating men about prostate cancer screening. A randomized trial of a mailed pamphlet. Eff Clin Pract 2001;4:112 – 20. Laara E, Day NE, Hakama M. Trends in mortality from cervical cancer in the Nordic countries: association with organised screening programmes. Lancet 1987;1:1247 – 9. Collins MM, Barry MJ. Controversies in prostate cancer screening. Analogies to the early lung cancer screening debate. JAMA 1996;276:1976 – 9. Wolf AM, Nasser JF, Wolf AM, Schorling JB. The impact of informed consent on patient interest in prostate-specific antigen screening. Arch Intern Med 1996;156:1333 – 6. Davison BJ, Kirk P, Degner LF, Hassard TH. Information and patient participation in screening for prostate cancer. Patient Educ Couns 1999;37: 255 – 63. Schapira MM, VanRuiswyk J. The effect of an illustrated pamphlet decision-aid on the use of prostate cancer screening tests. J Fam Pract 2000;49:418 – 24. Gattellari M, Ward JE. Does evidence-based information about screening for prostate cancer enhance consumer decision-making? A randomised controlled trial. J Med Screen 2003;10:27 – 39. Gattellari M, Ward JE. A community-based randomised controlled trial of three different educational resources for men about prostate cancer screening. Patient Educ Couns 2005;57:168 – 82. Flood AB, Wennberg JE, Nease RF, Jr., Fowler FJ, Jr., Ding J, Hynes LM; Prostate Patient Outcomes Research Team. The importance of patient preference in the decision to screen for prostate cancer. J Gen Intern Med 1996;11:342 – 9. Volk RJ, Spann SJ, Cass AR, Hawley ST. Patient education for informed decision making about prostate cancer screening: a randomized controlled trial with 1-year follow-up. Ann Fam Med 2003;1:22 – 8. Frosch DL, Kaplan RM, Felitti VJ. A randomized controlled trial comparing internet and video to facilitate patient education for men considering the prostate specific antigen test. J Gen Intern Med 2003;18:781 – 7. Partin MR, Nelson D, Radosevich D, et al. Randomized trial examining the effect of two prostate cancer screening educational interventions on patient knowledge, preferences, and behaviors. J Gen Intern Med 2004;19:835 – 42. Myers RE, Chodak GW, Wolf TA, et al. Adherence by African American men to prostate cancer education and early detection. Cancer 1999;86: 88 – 104. Myers RE, Daskalakis C, Cocroft J, et al. Preparing African-American men in 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. community primary care practices to decide whether or not to have prostate cancer screening. J Natl Med Assoc 2005;97:1143 – 54. Weinrich SP, Boyd MD, Weinrich M, Greene F, Reynolds WA, Jr., Metlin C. Increasing prostate cancer screening in African American men with peereducator and client-navigator interventions. J Cancer Educ 1998;13:213 – 9. Ashford AR, Albert SM, Hoke G, Cushman LF, Miller DS, Bassett M. Prostate carcinoma knowledge, attitudes, and screening behavior among African-American men in Central Harlem, New York City. Cancer 2001;91: 164 – 72. Steele CB, Miller DS, Maylahn C, Uhler RJ, Baker CT. Knowledge, attitudes, and screening practices among older men regarding prostate cancer. Am J Public Health 2000;90:1595 – 600. Weinrich SP, Weinrich MC, Priest J, Fodi C. Self-reported reasons men decide not to participate in free prostate cancer screening. Oncol Nurs Forum 2003;30:E12 – 6. Myers RE, Wolf TA, Balshem AM, Ross EA, Chodak GW. Receptivity of African-American men to prostate cancer screening. Urology 1994;43:480 – 7. Myers RE, Hyslop T, Wolf TA, et al. African-American men and intention to adhere to recommended follow-up for an abnormal prostate cancer early detection examination result. Urology 2000;55:716 – 20. Weinrich SP, Weinrich MC, Boyd MD, Atkinson C. The impact of prostate cancer knowledge on cancer screening. Oncol Nurs Forum 1998;25:527 – 34. Taylor KL, Turner RO, Davis JL III, et al. Improving knowledge of the prostate cancer screening dilemma among African American men: an academic-community partnership in Washington, DC. Public Health Rep 2001;116:590 – 8. Georgetown University Medical Center and The Most Worshipful Prince Hall Grand Lodge of the District of Columbia. The right decision is yours. A guide to prostate cancer. Available from: http://lombardi.georgetown.edu/ research/areas/cancercontrol/prostate.htm. Funded by the U.S. Centers for Disease Control and Prevention, Cooperative Agreement #TS-290 and the National Cancer Institute, # K07 CA72645. May 2000. Chan EC, Vernon SW, Ahn C, Greisinger A. Do men know that they have had a prostate-specific antigen test? Accuracy of self-reports of testing at 2 sites. Am J Public Health 2004;94:1336 – 8. Volk RJ, Cass AR. The accuracy of primary care patients’ self-reports of prostate-specific antigen testing. Am J Prev Med 2002;22:56 – 8. Chan EC, Sulmasy DP. What should men know about prostate-specific antigen screening before giving informed consent? Am J Med 1998;105: 266 – 74. Volk RJ, Cass AR, Spann SJ. A randomized controlled trial of shared decision making for prostate cancer screening. Arch Fam Med 1999;8: 333 – 40. O’Connor AM. Decisional conflict scale. 4th ed. 1999. p. 1 – 33. Available from: http://decisionaid.ohri.ca/docs/Eval_Meas/User_Manuals/UM_DCS. pdf. Ottawa Health Research Institute, Ottawa, Canada. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988. Frosch DL, Kaplan RM, Felitti V. The evaluation of two methods to facilitate shared decision making for men considering the prostate-specific antigen test. J Gen Intern Med 2001;16:391 – 8. Agency for Healthcare Research and Quality. Impact of cancer-related decision aids. Summary, Evidence Report/Technology Assessment: Number 46 (AHRQ Publication No. 02-E004). July 2002. Rockville, MD. Available from: http://www.ahrq.gov/clinic/epcsums/caaidsum.htm. O’Connor AM, Fiset V, DeGrasse C, et al. Decision aids for patients considering options affecting cancer outcomes: evidence of efficacy and policy implications. J Natl Cancer Inst Monogr 1999;25:67 – 80. O’Connor AM, Stacey D, Entwistle V, et al. Decision aids for people facing health treatment or screening decisions (Cochrance review). Cochrane Database Syst Rev 2003;2:CD001431. Taylor KL, Africano NL, Cullen J, Lamond TW, Williams RM, Davis KM. Screening for chronic disease: the prostate cancer dilemma. In: Trafton JA, Gordon WP, editors. Best practices in the behavioral management of chronic disease. Los Altos (CA): Institute for Brain Potential; 2006. Schwartz LM, Woloshin S. The media matter: a call for straightforward medical reporting. Ann Intern Med 2004;140:226 – 8. Schwartz LM, Woloshin S, Fowler FJ, Jr., Welch HG. Enthusiasm for cancer screening in the United States. JAMA 2004;291:71 – 8. Cancer Epidemiol Biomarkers Prev 2006;15(11). November 2006 Downloaded from cebp.aacrjournals.org on June 9, 2014. © 2006 American Association for Cancer Research.


















© Copyright 2025