
Additive Fabrication Technologies Applied to
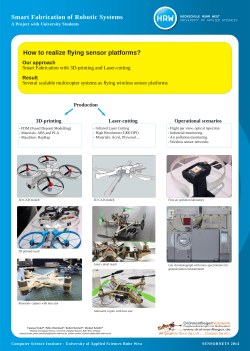
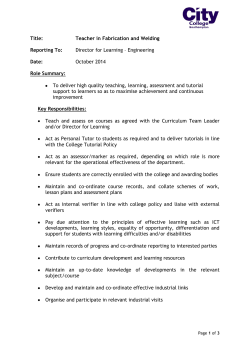
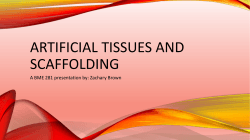
Additive Fabrication Technologies Applied to Medicine and Health Care: A review J. GIANNATSIS AND V. DEDOUSSIS Center for Product Development and Rapid Prototyping University of Piraeus 80 Karaoli & Dimitriou str., 18534 Piraeus, Greece Tel: + 30 210 41.42.320 Fax: + 30 210 41.42.356 e-mail: vdedo@unipi.gr, ggian@unipi.gr ABSTRACT Additive Fabrication (AF) and Rapid Prototyping (RP) technologies are mostly associated with applications in the product development and the design process as well as with small batch manufacturing. Due to their relatively high speed and flexibility, however, they have also been employed in various non-manufacturing applications. A field that attracts increasingly more attention by the scientific community is related to the application of AF technologies in medicine and health-care. The associated research is focused both on the development of specifically modified or new methods and systems based on AF principles, as well as on the applications of existing systems assisting health care services. In this paper representative case studies and research efforts from the field of AF medical applications are presented and discussed in detail. The case studies included cover applications like the fabrication of custom implants and scaffolds for rehabilitation, models for pre-operating surgical planning, anatomical models for the mechanical testing and investigation of human bones or of new medical techniques, drug delivery devices fabrication, as well as the development of new AF techniques specifically designed for medical applications. Keywords: Additive Fabrication; Rapid Prototyping; Rapid Manufacturing; Biomodelling; Scaffold Fabrication; Medical applications 1 INTRODUCTION Additive fabrication (AF) is a relatively new concept that emerged during the last decade in order to describe a set of new or under development manufacturing methods, processes and technologies that function through material addition, in contrast to the established traditional cutting, forming or casting methods. Rapid 1 Prototyping (RP) technologies are the most widely applied and known fabrication methods that are based on additive fabrication principles. Some of the major RP technologies used worldwide are Stereolithography (SL), Selective Laser Sintering (SLS), Fused Deposition Modelling (FDM), 3D printing (3DP), MultiJet Modelling (MJM) and Laminated Object Manufacturing (LOM). Main applications of RP include the fabrication of various kinds of models and prototypes for concept evaluation and presentation as well as functional testing of new products, early in the product development process [1]. The continuous improvement of RP systems accuracy and materials, expand gradually their applications to other areas of the industrial sector like Rapid Manufacturing (RM the actual manufacturing of products in small batches) and Rapid Tooling (RT fabrication of manufacturing tools and moulds). What makes RP particularly appealing for all of the above applications is the fact that compared to alternative manufacturing technologies, like for instance CNC machining, RP systems can fabricate parts of almost any geometrical complexity in relatively lower time and with reduced cost and without significant requirements in technical expertise. This kind of geometric flexibility, which is mostly a consequence of their additive nature, is the main reason that RP technologies are increasingly used or tested in non-industrial applications like medical and architectural modelling [2] or artistic creation [3]. The medical branch in particular has attracted the attention of many researchers and scientists since the first introduction of RP technologies, and has been the topic of various EU research programmes (e.g. Phidias – EC Funded Network Project on Rapid Prototyping in Medicine). What makes RP technologies even more appealing is that they utilize medical imaging data (obtained by techniques like Computed Tomography-CT or Magnetic Resonance Imaging-MRI), almost directly, for the production of customised patient specific parts. The reported medical applications of RP technologies can be classified to the following categories: • Biomodelling, which involves the fabrication of physical models of parts of the human anatomy and biological structures in general, for surgery planning or testing. • Design and fabrication of customised implants for prosthetic operations, rehabilitation and plastic surgery • Fabrication of porous implants (scaffolds) and tissue engineering 2 • Fabrication of specific surgical aids and tools • Drug delivery and micron-scale medical devices Despite of their great flexibility and potential, RP technologies have not yet been widely adopted in the medical and health-care sector. This can be attributed to the high cost and time required for the fabrication of corresponding models which at present can only be justified in relatively complex medical cases [4]. Besides time and cost, there is the issue of accuracy of RP systems, which is not sufficient for some applications due, mainly, to poor or inaccurate medical imaging data, as well as the issue of materials and their properties, i.e. flexibility, strength and biocompatibility [5]. Nevertheless, RP technologies and AF in general have great potential in the area of medical and health-care applications due to their distinct features, and have been therefore the subject of various studies worldwide. The corresponding research covers various areas such as the cost-efficient application of established technologies, the development of new technologies, the virtual modelling/representation of medical data and the development of biocompatible materials. The purpose of the present work is to present and discuss in detail the most representative case studies, covering the main research areas of AF applications in medicine according to the classification given above. 2 FABRICATION OF RP MODELS BASED ON MEDICAL DATA One of the major medical applications of RP is the fabrication of models of parts of human anatomy of a patient based on data obtained through the various well established techniques of CT or MRI [6]. The fabrication process of these physical models, which are nowadays often called biomodels, involves three phases [7]: • The first step is to obtain the data of the patient’s area of interest with the use of the previously mentioned techniques (CT, MRI, etc.), which provide an indirect representation of the patient’s anatomy through a series (stack) of 2D images. • The images are next manipulated employing special software, which facilitate the separation and highlighting of the tissues (soft or hard) 3 that represent the area of the biomodel, and allow the conversion of the 2D image information to a 3D representation. Usually, the standard STL representation is utilized for the latter. • Finally the biomodel is fabricated via an RP system followed by possible (if it is necessary) manual finishing. The accuracy of RP biomodels depends on various factors associated with all phases of the process. Choi et al. [8] analyzed the possible sources of error in SL biomodelling and identified the main sources of error in the second phase, namely, the translation of 2D data to a 3D virtual model. This has led to the development of special software tools like Mimics from Materialise Inc. (www.materialise.com) and Biobuild (www.anatomics.com) that have simplified and enhanced the accuracy of the 2D-3D data transformation process. Regarding the manufacturing accuracy of RP technologies, Santler et al. [9] concluded that it is sufficient for clinical purposes. 3 RP BIOMODELS FOR SURGICAL PLANNING Among the first (and major) applications of AF/RP in medicine and health-care is the production of (physical) biomodels that can be used as an aiding tool for surgical planning and rehearsal [10]. Since every patient is unique, the surgeon must fully understand the anatomy of the patient before operation. Obtaining a full understanding of the patient’s anatomy only by the study of a stack of CT/MRI images in these cases requires great experience from the surgeon, especially in complex surgical operations [11]. In such cases RP biomodels greatly facilitate diagnosis and treatment planning, and decrease the risk of misinterpretation of the medical problem. Having a physical biomodel in hand also facilitates surgery planning and makes possible the rehearsal and simulation of the operation through marking, cutting and reassembling of the biomodel. Furthermore, the pre-surgical study of a biomodel allows not only the detailed evaluation of the operation, without the time pressure present during actual operation, but also possible problem prediction. This way, actual operation time, and consequently operation cost and infection/anaesthesia risk are decreased. Biomodels are also very useful as a communication tool between medical personnel. They are also very useful for the presentation of operation details to 4 people with no medical expertise (e.g. the patient or its relatives), thus increasing consent and trust. In most cases, RP is applied for the fabrication of models of hard tissue parts of the human body, i.e. bones [12]. The most widely reported application of RP biomodelling for surgical planning is in the field of maxillo-craniofacial surgery, which involves the surgical treatment of congenital or acquired deformations (e.g. tumour resections or trauma defections) both for functional and aesthetic purposes [13-19]. The geometry of the skull is quite complex and cannot be easily reproduced in a physical model using cutting manufacturing methods like CNC milling. RP, therefore, presents a reasonable alternative. Among RP technologies, SL is the most commonly used in craniofacial biomodelling. An example of a SL skull model, fabricated at the Center of Product Development and Rapid Prototyping of the University of Piraeus, is presented in Fig.1. This SL model is an accurate replicate of the damaged skull of a young girl, which was injured in a car accident and it has been used for pre-operative planning of the surgery as well as an aid for the design of the prosthetic implant that would restore the anatomy of the damaged area. Figure 1 Muller et al. [19] investigated the usefulness of RP models of the skull in craniofacial and neurosurgical practice. RP biomodels of 52 patients, whose treatment required corrective/reconstructive cranioplasty or involved complex surgical operations, were fabricated. They report that SL models help in better understanding of the anatomy, increase intra-operative accuracy, support accurate fabrication of implants, facilitate pre-surgical simulation and improve education of trainees. Kermer et al. [17] propose in their study an enhancement of the RP biomodelling approach by investigating the possibility of selectively coloured RP biomodels. Their findings indicated that selectively coloured models facilitate the management of ablative surgery and reconstructive procedures as well. The value of SL surgical biomodels has also been shown in the case of reconstructing of complex orbital fractures in a study by Fan et al. [20]. Biomodelling of soft-tissue parts of the human body using RP, are rather rare in practice. This can be mainly attributed to the difficulty of separating the area of interest from the surrounding soft tissues, due to the relatively small differences of greyscale in medical scanned images. D’Urso et al. [21] have 5 studied the possibility of biomodelling of cerebral aneurysms based on data obtained through CT angiography (CTA) and MR angiography (MRA). Their results indicate that the SL models are sufficiently accurate and can be quite useful for surgical planning in complex cases or when the standard imaging is felt to be equivocal. In a similar study Wurm et al. [22] investigated the usefulness of cerebrovascular biomodels for aneurysm surgery with similar results. The feasibility of RP biomodelling for the replication of soft-tissue parts is shown in the study of Binder et al. [23]. They applied SL for the construction of replicates of the mitral valve with good results. Although the results of the previous mentioned studies show the usefulness of biomodels for operation planning and rehearsal, the high fabrication cost and time involved is in most cases a major drawback. In particular, SL and SLS models are very expensive and the associated cost can be justified only in rather complex cases. In order decrease the fabrication cost and time the utilization of 3D-printing is proposed, which is much less expensive and time-consuming [24]. 4 TOOLS FOR INTRA-OPERATION GUIDANCE AND TESTING Of course, biomodels are not used in the pre-surgical phase only. They are also used in actual surgery, during which, biomodels or images obtained by biomodels, can be utilized to guide the operation, assuring the accuracy and the quality of results. D’Urso et al. [25,26] investigated the possibility of using accurate SL biomodels of the patient in planning and rehearsing stereotactic surgery. The method of stereotaxy is a minimally-invasive form of surgical intervention which uses 3D coordinates in order to locate specific targets and perform on them an operation like removal, implantation or injection. The location of the target is based on MRI/CT data and is determined with respect to a reference frame that is attached to the patient’s body. In order to simplify the method and enhance its accuracy, D’Urso et al. [25,26] employed SL biomodels in a neurosurgical operation. They report that biomodel-guided stereotaxy offers significant advantages in terms of speed, simplicity, accuracy, and versatility but with the extra cost and time required for biomodel fabrication. Ngan et al. [27] also proposed the use of RP models, fabricated with SL and 3DP, for preoperative and 6 intraoperative planning of pulmonary atresia surgical treatment. They report that the surgeons found biomodels very useful in visualizing the vascular anatomy, but construction of virtual models was relatively labour intensive and required expert knowledge of the pulmonary vasculature. Another application of SL models is presented by Starly et al. [28], in which the SL model is used as a medium for the transfer of the anticipated skull geometry in a surgical guidance system of over-laying images. In this approach the 3D virtual model of the patient’s skull is constructed first through CT data interpolation. The virtual model is then split in two symmetrical parts, the undamaged half and the defective half that contains the trauma. Next, the defective part is discarded and replaced by the mirror image of the other half and a new virtual model of the skull with the required symmetry is constructed and fabricated with SL. The SL model is then scanned with CT and the obtained stack of images is transferred to the surgery guidance system, thus providing an image reference that accurately guides the surgeon during operation. SL has also been used for the fabrication of surgical guides for the placement of dental implants, a restoration process that requires detailed planning and high accuracy. Sarment et al. [29] investigated the accuracy of dental implant placement with the aid of SL surgical guides, which according to their findings improved the implant placement. In a similar study Di Giacomo et al. [30] came to the same conclusion, but denoted that the technique requires improvement to provide better stability of the guide during the surgery, in cases of unilateral bonesupported and non-tooth-supported guides. SLS and Reverse Engineering (RE) methods have been employed for the construction of protective patient-specific shielding masks that may be used as protective shields during cancer treatment [31,32]. The fabrication procedure proposed by De Beer et al. [31] comprises of three phases: first the face geometry for the mask is captured by 3D photography, subsequently an SLS plastic mask is produced, based on the mask virtual model, and finally a radio protective shell on the mask is applied through spraying of a special metal alloy (see Fig.2). The reported results show that the proposed methodology leads to quicker and more accurately manufactured masks compared to conventional processes, at the expense of higher costs, the latter being mainly associated with the SLS fabrication phase. However, higher accuracy and better fit of masks are expected 7 not only to reduce the trauma experienced by the patient but also to decrease production man-hours consumed, implicitly, therefore, increasing the cost efficiency of the method. The feasibility of the proposed procedure for the production of customer-specific radiation shields is confirmed also in a study by Zemnick et al. [32] who followed a similar process that employs 3D laser scanning and SL. Figure 2 Testing of new treating methods and technologies is another field that RP has been applied successfully. Johnson and Young [33] have investigated the feasibility of using RP biomodels as expendable test parts, in an experimental study of the response of the human head to impact, during a car accident. In a similar manner, SL models of cancellous bones, like those caused by osteoporosis, were fabricated and mechanically tested, in order to investigate the relationship between their geometry and their mechanical strength, implicitly assessing fracture risk [34]. Also, RP models of pelvic bones have been used to prove experimentally the higher efficiency of computer assisted screw insertion procedures over conventional ones in spinal surgery [35]. The study of exposure of the human respiratory system to dangerous or pathogenic aerosols is another area where RP models have been used successfully. Clinkbeard et al. [36] applied SLS for the fabrication of human tracheobronchial airway models and carried out an experimental investigation of the location and the amount of deposition of dangerous aerosols under different conditions. They propose the utilization of such models as the standard for relevant studies. 5 PATIENT-SPECIFIC IMPLANTS Another area that the application of RP systems seems to have great potential is the construction of customized implants for reconstructive and plastic surgery. In this area the connection of medical imaging techniques and RP can lead to significant time savings in operation time and much higher accuracy and quality in surgical operation [37]. He et. al. [38] presented a design method for exact-fit customized implants that employs virtual and RP models of injured or healthy bones in order to reduce the associated time and cost. This methodology is employed in a case study investigated by Truscott et al. [39] that focused on the 8 use of SLS models in the design process of customised titanium elbow implants. According to their findings the complementary use of virtual and physical models greatly improves the accuracy and reduces the cost of the implant design process. Winder et al. [40] present 10 clinical cases, in which the required titanium implants for the reconstruction of skull defects were created using RP models as masters for casting. The geometry of the data was obtained by comparing the defected side of the head to the contralateral, so as to retain symmetry in the final result. Applying a similar method D’Urso et al. [41] used SL models of both the actual defected side and the customized implant (the latter to be used for casting acrylic implants) in cranioplasty operations. They report reduced operating time and excellent results at a ‘reasonable’ cost. SL models have been used for the fabrication of mandible titanium trays, which are implanted in the patient as a replacement of the actual bone that was lost or removed because to a tumour [42]. The implant SL model served as the casting pattern for the construction of a silicon mould and the subsequent casting of an identical wax model, which was finally used as an expendable pattern for the production of the titanium part by investment casting. Singare et al. [42], who carried out this work, report that using CT data and SL provides very accurate implants that have significant functional and aesthetically pleasing results. In a following study Singare et al. [43] employed directly SL Quickcast models as expendable patterns for investment casting of titanium implants. SL models have also been used directly as expendable patterns for casting of a titanium implant for the replacement of a damaged hemi-knee joint [44]. In the same study, SL has also been employed for the fabrication of an expendable mould for a porous bone substitute (see Fig. 3). Both parts were implanted on the patient with good results in terms of functionality and fitting with the surrounding anatomy. Figure 3 Dental applications generally seem rather suitable for RP in view of the complex geometry involved, the low volume and the requirements for customization [45]. According to Chang et al. [46] the integrated use of Abrasive Computer Tomography (ACT), RP and CNC technologies can significantly improve the speed and quality of the orthodontic denture production process. Eggbeer et al. [47] investigated the efficiency of using RP models as expendable casting models in the case of custom made models of removable partial denture 9 (RPD) metal alloy frameworks. These frameworks serve as a medium to retain artificial replacement teeth in the oral cavity. According to their method, RP models of the framework, which are fabricated based on digitally scanned data of an impression of the patient’s mouth, can be used as models for lost-wax casting of the actual framework with great success. Fabrication of titanium replicates of the actual teeth is also reported possible using RP models and vacuum casting for the production of teeth wax models for lost-wax casting [48]. Kruth et al. [49] provide an example of a direct application of RP, particularly SLS, for the fabrication of metal alloy frameworks for dental prosthesis. Selective Laser Melting (SLM) is another AF technology that according to Bibb et al. [50] may be employed successfully for the direct fabrication of chromium-cobalt customized RPD. The feasibility of the SLM produced biocompatible implants was also reported in [51]. Fabrication of Titanium alloy implants with Direct Laser Forming, an AF technology that constructs metal parts with bulk density, have been investigated also in [52]. Direct fabrication of porcelain dental restoration parts is investigated in [53]. The proposed method involves the extrusion of dental powder pastes in a layer-by-layer fashion and the solidification of the extruded powder layer using a laser beam. Using RP models as models for traditional casting methods has been also investigated in cases concerning soft tissue implants like ears [54,55]. In these cases the geometry of the unaffected ear can be mirror-imaged using Reverse Engineering (RE) methods, for example 3D Laser Scanning, and reproduced with an RP method in order to take an accurate symmetrical replicate of the lost ear (see Fig. 4). Direct production of ‘soft’ biocompatible implants employing available RP technologies requires the development of new specialized materials. In order to address this need Bens et al. [56] developed a flexible (meth)acrylatebased resin for SL that could be useful in various bio-medical applications. Figure 4 The versatility of RP methods may enable another route for fabricating metal implants, which is the direct fabrication of a ceramic mould. Curodeau et al. [57] employ this approach to fabricate ceramic shell with 3DP which are used as expendable moulds for casting the desired implant. The production of moulds for implants by RP was also investigated by Hunt et al. [58], who employed SLS for the fabrication of moulds for the production of wax investment casting patterns. 10 According to their findings however, the bone growth in implants fabricated this way is less than in porous implants directly fabricated with SLS. 6 TISSUE AND ORGANISM MANUFACTURING ENGINEERING Due to the additive nature of the processes incorporated in RP technologies, they are also ideal for the fabrication of implants with special geometrical characteristics, like scaffolds for the restoration of tissues [59]. Scaffolds are porous supporting structures that are used as a vessel for the transplantation of tissue cells into the body of the patient [60]. They serve as the platform for the rapid and guided growth of new tissue in damaged or defective bones or even organs of the human body. As in the cases of cranioplasty and dental implants, RP technologies have been used either as a direct method for manufacturing the scaffolds themselves or (indirectly) as a ‘manufacturing tool’ of the moulds required for the casting of scaffolds. Chen et al. [61] present a case where a SL mould of the intended scaffold geometry was used to cast an artificial bone through injection of calcium phosphate cement (CPC), which is a non-toxic soluble material and bone morphogenic protein. Tests performed on animals showed that the artificial bone scaffold accelerated the growth of the actual bone. The same approach has also been used in other studies with similarly successful results in terms of cell growth on the scaffold [62,63]. Scaffold moulds for soft tissue implants have also been fabricated by inkjet printing technology with successful results [64,65]. In this case, the collagen scaffold was cast in the expendable RP mould, which was subsequently removed by ethanol bathing. A possible application of the method is presented by Taylor et al. [66] that investigate aortic valves collagen scaffold construction. Chen et al. [67] employed 3DP in a multi-phase elaborate production process of nano-fibrous scaffolds with controlled architecture in macro-, micro- and nano-scale is presented. In the proposed process 3DP is used for the production of the moulds of PLLA scaffolds that could be used in bone tissue engineering. For direct fabrication of biocompatible scaffolds several RP methods, as well as new AF methods have been investigated. In most cases the methods employed are based on jet printing (3DP, MJM) or liquid deposition techniques (FDM), that seem to be more appropriate for direct scaffold fabrication, due to the 11 ‘flexibility’ in the selection of raw materials. Seitz et al. [68] presented a method of direct 3DP of scaffolds from Hydroxyapatite (HA), a biocompatible implantable ceramic material. The printed ceramic ‘green bodies’ are next cured in a high temperature furnace, so to allow sintering of the powder. In a subsequent study Leukers et al. [69] performed a histological evaluation of 3D printed HA scaffolds, which showed that cells proliferated well into the scaffold, showing the efficiency of this method for scaffold fabrication. HA scaffolds have also been fabricated employing the FDM [70] and Robocasting methods [71]. Chim et al. [70] employed FDM for the construction of scaffolds with poly-e-caprolactone (PCL) and HA-PCL scaffolds in order to study different scaffold architectures and materials. Dellinger et al. [71] used Robocasting, an AF method that consists of the robotic deposition of highly concentrated colloidal suspensions in layers to form the scaffold structure, which is subsequently sintered in high temperature. Miranda et al. [72] also investigated Robocasting for the construction of bioceramic scaffolds for bone tissue engineering. The application of SLS technology for the direct fabrication of biocompatible ceramic scaffolds has been also extensively investigated. Williams et al. [73] assessed the direct fabrication of PCL porous scaffolds. According to their findings the fabricated scaffolds had sufficient mechanical strength and provided a sound platform for the generation of the new bone. PCL sintered scaffolds SLS with a powder blend of polyetheretherketone (PEEK) and hydroxyapatite (HA) has been also tried with promising results [74]. The construction of liver tissues, based on SLS fabricated PCL scaffolds, has been investigated by Huang et al. [75], who suggested that this approach could, in the near future, lead to the development of an implantable liver tissue equivalent for humans. A problem apparent in most studies of RP manufactured scaffolds is the time required for the virtual design and modelling of the scaffolds. 3D scaffold modelling is a trade-off design process (porosity versus structural strength) that requires considerable time and effort employing standard mechanical design software. In order to circumvent this problem Chua et al. [76] suggested utilizing libraries of application-specific polyhedral shapes that are used as constructing elements of the scaffolds. A prototype system that makes use of such primary scaffold elements (see Fig. 5) was proposed by Naing et al. [77]. The system utilizes special algorithms that construct the CAD scaffold model according to 12 user selected scaffold elements and porosity, and based on a surface model that provides the outer geometry of the scaffold. A micro-SL system that could be used for scaffold architecture studies is presented in [78]. According to Lee et al. [78] the redesigned system is capable of fabricating highly accurate 3D polymer structures that could aid the scaffold design process. Figure 5 Due to the materials physical and chemical properties of the models, RP assisted scaffold fabrication has been mainly focused on bone (hard) tissue engineering. For the fabrication of soft tissue scaffolds new techniques, like 3DBioplotting, are under investigation and development [79]. 3D-Bioplotting is a technique that resembles continuous deposition RP technologies like FDM, and allows 3D dispensing of liquids and pastes in liquid media through a pressurecontrolled dispenser. Moroni et al. [80] employed 3D-Bioplotting in the fabrication process of 3D hollow fiber scaffolds from biocompatible polymeric blends. Fiber hollowing is achieved in by selective dissolution of the fiber inner core polymer by extensive immersion of the initial scaffold in solvent. Viscoelastic properties of the obtained scaffolds can be modulated to accomplish mechanical requirements for tailored tissue engineering applications [81]. 3D fiber deposition of metallic scaffolds for orthopaedic applications has also been reported [82]. An emerging concept based on the primary successful research results of AF applications in tissue engineering is the concept of Organism Manufacturing Engineering (OME). OME is defined as the science and technologies that utilize the principles and methods of modern manufacturing science and life science, through controlled direct or indirect 3D assembly of cells, to manufacture live organisms, to substitute or to repair human tissues and organs [83]. According to Xiong et al. [83] main principles of AF could serve as the basis of new OME technologies for direct or indirect controlled cell assembly, and thereby provide a solution to the ever increasing demand for donor organs. Yan et al. [84] proposed a new process for the production of scaffolds for bone tissue engineering. Their method (Low-temperature Deposition Manufacturing – LDM) employs the layer manufacturing principle and an extrusion-type system for the construction of PLLA/TCP composite scaffolds. Compared to established methods like FDM, the LDM process is reported to preserve bio-activities of scaffold materials, because 13 of its non-heating liquefying processing of materials. In a following study [85] LDM was investigated as a production method for implantable bioactive liver substitute with promising results. A similar extrusion-type method is proposed by Vozzi et al. [86] for the fabrication of PLGA (PolyLactic-co-Glycolic Acid) scaffolds with microporosity. In the described method, material is deposited utilizing a pressure micro-syringe and a three-axis system with micro-scale positioning accuracy. In [87] a comparison of four types of nozzle systems, i.e pneumatic microvalve, solenoid microvalve, piezoelectric and precise extrusion deposition (PED) nozzles that deposit sodium alginate and PCL solutions was carried out. The proposed multinozzle manufacturing system can be employed used for the fabrication of bioactive tissue scaffolds, automatic cell loading, and heterogeneous tissue constructs for emerging regenerative medicine. Direct fabrication of 3D neural constructs by jet printing AF has been also investigated [88]. The method proposed by Xu et al. [88] employs conventional inkjet printing technology modified for alternating deposition of neural cell layers and biodegradable fibrin gel layers that form a cohesive 3D neural sheet. Examination of the sheets showed that deposited neurons maintained their basic electrophysiological functions. 7 DRUG DELIVERY AND MICROSCALE DEVICES Another field that RP technologies are expected to prove very useful is the fabrication of customized microsystems and therapeutic devices for controlled highly specific and precise drug delivery. Such devices involve complex micronscale networks of fluidic and electronic components capable of operating in an integrated manner [89]. In their study Razzacki et al. [89] categorized these devices into three major groups: • biocapsules and microparticles for controlled and/or site-specific drug release, • microneedles for transdermal and intravenous delivery and • implantable microsystems. An example of biomedical device that may be used in the area of drug testing and DNA research is reported in [90]. The device presented is a biochemical laboratory in micron scale that may be used for cell-free protein 14 synthesis. This micro-scale laboratory is assembled by biochemical chips fabricated with the method of Hybrid micro-SL, in which the chip functional parts such as one-way valve, ultrafiltration membrane and photo sensor are inserted during the layer construction-solidification process, thus eliminating the subsequent chip assembly phase. A novel layer manufacturing method that could possibly be applied applications in biosensor development, tissue engineering, drug delivery and biomaterials is described by Kızılel et al. [91]. The proposed method permits the construction of the PEG-based hydrogel multilayer structures. Reported advantages are the biocompatibility of materials and the fact that layer formation is achieved in mild photopolymerization conditions using visible instead of ultraviolet light. The fabrication of medical microdevices or microconstructions that are biodegradable and therefore require no special removal operation from the patient’s body is another possibility investigated in conjunction with AF. Methods employed traditionally for micro-scale manufacturing like thin-film deposition, photolithography, etching or methods borrowed from the computer industry, are not suitable for biodegradable polymers [92]. In such applications non-invasive additive fabrication technologies, like micro-SL, may have great potential in both a laboratory and industry scale [92]. Matsuda and Mizutani [93] reported the development of two such photocurable biodegradable liquid copolymers, one hydrophilic and another hydrophobic. Reported results show that the developed copolymers can be easily photocured by UV radiation and are, therefore, suitable for use in micro-SL (see Fig. 6). Itoga et al. [94] presented a novel photolithography device that could be employed preparation of micro-patterned surfaces for biomedical applications, as well as other microfluidic surfaces in a rapid prototyping manner. The device is based on a modified LCD projector and has been tested in the construction of polyacrylamide (PAAm) micro-patterned surfaces. Shape Deposition Manufacturing (SDM) is another RP method that could be potentially employed for micro-scale manufacturing. Cheng and Lin [95] presented such an application of SDM in the fabrication of valve-less micropumps with micro channels. Figure 6 AF may provide alternative ways for the fabrication of drug delivery devices like oral tablets. Rowe et al. [96] presented an application of 3DP 15 technology for the fabrication of oral devices where two different release mechanisms, erosion and diffusion, are mixed in a single device. Other possible applications are tablets with a quick dissolve region that breaks into controlled subunits and pulsatory devices. The SLS process has been also used for the fabrication of porous cylindrical disc matrices that may be used as drug delivery devices by Low et al. [97]. They reported that it is possible to use SLS for producing drug delivery devices that have variable porosity and micro-features. Leong et al. [98] investigated the possibility of building biodegradeable controlled drug delivery devices with SLS. Their experiments with PCL and PLLA as test materials showed that varying porosity discs can be produced by controlled variance of SLS fabrication parameters. 8 DISCUSSION AND CONCLUDING REMARKS In this paper applications of AF/RP technologies in medicine and current research issues in the field of Rapid Medical Prototyping are presented. The review of the international specialized literature showed that custom biomodels fabricated with RP technologies are quite useful for planning and rehearsal of complex surgical operations. According to the results of most studies RP biomodels aid the surgeons in diagnosis, planning, problem prediction and communication, thus reducing operation time infection risk and improving the results of the operation. Among the RP technologies applied to medicine, SL seems to have attracted the attention of most researchers. SL is not only relatively more accurate but also the number of installed SL systems worldwide is very big. Also, SL resins provide the advantage of biomodel clarity and transparency that can be quite useful in surgery rehearsal. However, they are not biocompatible and require special handling; a fact that makes adoption of SL systems in the hospital environment difficult. Both the accuracy and the low surface roughness of SL biomodels makes them ideal as casting patterns for the fabrication of customised metallic or acrylic implants through lost-wax or vacuum casting methods. For the fabrication of biomodels for surgery planning and evaluation purposes, less ‘expensive’ or time-consuming RP technologies, like multicolour 3DP and FDM seem to be the most suitable choice. Another advantage of these two technologies is that they are office friendly and can process biocompatible materials with some minor modifications. Further reduction in the fabrication time 16 involved, can be achieved through higher automation of the medical imaging data manipulation process that is required for the construction of the virtual model. The virtual model construction phase is reported as the main source of observed inaccuracies, mainly due to the low level of detail and information that can be obtained through conventional medical imaging (diagnostic) systems. SLS technology has the greatest potential among commercial RP technologies or direct fabrication of implants. This is mainly due to the fact that SLS can fabricate implants from a variety of materials including metals, ceramics and thermoplastics with sufficient accuracy. In this context the main research issue is to develop and test materials that are biocompatible so that can be used safely for direct fabrication of implants. Fabrication of custom-made scaffolds is another application in which RP can be quite useful. Two approaches have been identified: • Direct Methods - they employ a commercial RP system or a new AF method for the fabrication of the actual scaffold itself (e.g. SLS of biocompatible ceramics) and • Indirect Methods - they employ RP for the fabrication of the tool (pattern or mould) that will be used for the production of the actual scaffold. Due to adverse materials properties direct additive scaffold fabrication is mostly directed to hard-tissue scaffolds (bone tissue engineering). As far as the fabrication of soft-tissue scaffolds new manufacturing methods that apply the principles of AF are currently under development. These new methods employ mostly the jet-printing or deposition operational principles for the construction of layers from biocompatible or biodegradable materials. An aspect that should be considered in scaffold fabrication with powder based RP technologies is the removal of trapped material within the scaffold (trapped volume problem). Also, the minimum grain size sets a limit in the porosity obtainable with these methods. However, the development of finer grain powder materials could greatly alleviate these drawbacks. Obviously, full exploitation of the advantages of AF technologies is directly related to the availability of special design software systems (Bio-CAD) that enable design and manipulation of the relatively complex geometries of scaffolds. Scaffolds also present a challenge in terms of virtual representation that cannot be easily manipulated by currently available industrial CAD systems. 17 Micro- and nano-fabrication variants of AF technologies are expected to make possible the fabrication of controllable drug delivery units or implants in the micron or the submicron level. For custom implants of such fine scale require further improvement of associated technologies such as micro-CT. Fabrication of artificial organ substitutes is a very interesting area of research, where initial results show that extrude-type AF may be employed successfully. Relevant technologies under development mostly focus on deposition techniques that enable controlled ‘assembly’ of living cells and supporting material in order to construct the organ substitute. In conclusion, the literature review carried out in this work showed that although RP technologies exhibit a great potential in the field of medical applications, they have not been widely adopted yet in standard medical practice, because of the high cost and fabrication time involved. RP although faster and more flexible than other manufacturing methods (e.g. CNC machining) is neither fast enough nor cost effective to cater for emergency cases. Depending on the size and complexity of the biomodel, RP fabrication times vary between a few hours to two days, which maybe unacceptably long for emergency cases (depending, of course, on the particular case). Time and cost requirements, therefore, restrict the utilization of RP to rather complex cases where considerable cost savings and quality benefits are expected. Indeed, this is the case with surgical planning biomodels. Also, RP cost and time ‘expenses’ seem to be justifiable for custom implant fabrication applications, e.g. for orthopaedic surgery, simply because in such cases the utilization of conventional manufacturing methods, implies significantly higher fabrication time and cost. Furthermore, the customization of the implant assures accurate fitting, reduces operating time and enhances quality. Ill fitted implants cause discomfort and should be replaced quite frequently, which means that the cost of rectifying or compensating the effects of an ineffective surgery can be far higher than the cost of the actual surgery operation itself [24]. Considering, therefore, these compensating costs the initial investment cost in RP may be well justified. Regarding the tissue engineering, artificial organ manufacturing and drug delivery device fields, initial experimental results show that there is a great potential. However, a lot of research effort is still required for the development of reliable manufacturing systems and materials, which could be employed for the mass production of scaffolds or even organ substitutes. 18 References 1. Wohlers T. (2004) Wohlers Report 2004: Rapid Prototyping, Tooling and Manufacturing State of the Industry Report. Wohlers Ass., Oak Ridge-Colorado, USA. 2. Giannatsis J., Dedoussis V., D. Karalekas (2002) Architectural Scale modeling using Stereolithography. Rap Proto J, 8(3):200-207. 3. H. W. Wai (2001) RP in art and conceptual design. Rap Proto J, 7(4):217-219. 4. Winder J., Bibb R. (2005) Medical Rapid Prototyping Technologies: State of the Art and Current Limitations for Application in Oral and Maxillofacial Surgery. J Oral Maxillofac Surg, 63(7):1006-1015. 5. Gibson I. (2005) Rapid prototyping: from product development to medicine and beyond, Virt Phys Proto, 1(1):31-42. 6. Galantucci L.M., Percoco G., Angelelli G., Lopez C., Introna F., Liuzzi C., De Donno A. (2006) Reverse engineering techniques applied to a human skull, for CAD 3D reconstruction and physical replication by rapid prototyping. J Med Eng Technol, 30(2):102-11. 7. Petzold R., Zeilhofer H.-F., Kalender, W.A. (1999) Rapid prototyping technology in medicine - basics and applications. Comp Med Imag Graph, 23:277-284. 8. Choi J.-Y., Choi J.-H., Kim N.-K., Kim Y., Lee J.-K., Kim M.-K., Lee J.-H., Kim M.-J. (2002), Analysis of errors in medical rapid prototyping models. Int J Oral Maxillofac Surg, 31:23–32. 9. Santler G., Karcher H., Gaggl A. and Kern R. (1998) Stereolithography versus milled three-dimensional models: comparison of production method, indication, and accuracy. Comp Aid Surg, 3:248-256. 10. Webb P.A. (2000) A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Engin Technol, 24(4):149-153. 11. Sanghera B., Naique S., Papaharilaou Y., Amis A. (2001) Preliminary study of rapid prototype medical models. Rap Proto J, 7(5):275-284. 12. Lohfeld S., Barron V., McHugh P.E. (2005) Biomodels of Bone: A Review. Ann Biomed Engin, 33(10):1295–1311. 13. Bill J.S., Reuther J.F., Dittmann W., Kubler N., Meier J.L., Pistner H., Wittenberg G. (1995) Stereolithography in oral and maxillofacial operation planning. Int J Oral Maxillofac Surg, 24:98-103. 14. D’Urso P.S., Atkinson R.L., Lanigan M.W., Earwaker W.J., Bruce I.J., Holmes A., Banker T.M., Effeney D.J., Thompson, R.G. (1998) Stereolithographic (SL) biomodelling in craniofacial surgery. Br J Plas Surg, 51:522-530. 15. Sailer H.F., Haers P.E., Zollikofer C.P., Warnke T., Carls F.R., Stucki P. (1998) The value of stereolithographic models for preoperative diagnosis of craniofacial deformities and planning of surgical corrections. Int J Oral Maxillofac Surg, 27(5):327-333. 16. Kermer, C., Lindner, A., Friede, I., Wagner A., Millesi, W. (1998) Preoperative stereolithographic model planning for primary reconstruction in craniomaxillofacial trauma surgery. J Craniomaxill Surg, 26:136-139. 17. Kermer C., Rasse M., Lagogiannis G., Undt G., Wagner A., Millesi, W. (1998) Colour Stereolithography for planning complex maxillofacial tumor surgery. J Craniomaxill Surg, 26:360-362. 18. D'Urso P.S., Anderson R.L., Weidmann M.J., Redmond M.J., Hall B.I., Earwaker W.J., Thompson R.G., Effeney D.J. (1999) Biomodelling of skull base tumours. J Clin Neurosci, 6(1):31-35. 19. Muller A., Krishnan K.G., Uhl E., Mast G. (2003) The application of rapid prototyping techniques in cranial reconstruction and preoperative planning in neurosurgery J Craniofac Surg, 14(6):899-914. 20. Fan X., Zhou H., Lin M., Fu Y., Li J. (2007) Late Reconstruction of the Complex Orbital Fractures With Computer-Aided Design and Computer-Aided Manufacturing Technique. J Craniofac Surg, 18(3):665673. 19 21. D'Urso P.S., Thompson R.G., Atkinson R.L., Weidmann M.J., Redmond M.J., Hall B.I., Jeavons S.J., Benson M.D., Earwaker W.J. (1999) Cerebrovascular biomodelling: a technical note. Surg Neurol, 52(5):490-500. 22. Wurm G., Tomancok B., Pogady P., Holl K., Trenkler J. (2004) Cerebrovascular stereolithographic biomodeling for aneurysm surgery. Technical note, J Neurosurg., 100(1):139-145. 23. Binder T.M., Moertl D., Mundigler G., Rehak G., Franke M., Delle-Karth G., Mohl W., Baumgartner H. and G. Maurer (2000) Stereolithographic biomodeling to create tangible hard copies of cardiac structures from echocardiographic data In vitro and in vivo validation. J Amer Col Cardiol, 35(1):230-237. 24. Wagner J.D., Baack B., Brown G.A., Kelly J. (2004) Rapid 3-dimensional prototyping for surgical repair of maxillofacial fractures: a technical note. J Oral Maxillofac Surg, 62(7):898-901. 25. D'Urso P.S., Hall B.I., Atkinson R.L., Weidmann M.J., Redmond M.J. (1999) Biomodel-guided stereotaxy. Neurosurg, 44(5):1084-1093. 26. D'Urso P.S., Williamson O.D., Thompson R.G. (2005) Biomodeling as an aid to spinal instrumentation. Spine, 30(24):2841-2845. 27. Ngan E.M., Rebeyka I.M., Ross D.B., Hirji M., Wolfaardt J.F., Seelaus R., Grosvenor A., Noga M.L. (2006) The rapid prototyping of anatomic models in pulmonary atresia. J Thorac Cardiovasc Surg, 132(2):264-269. 28. Starly B., Piatt J.H., Sun W., Faerber E. (2005) Virtual and medical prototype assisted craniofacial reconstructive surgery. In Virtual Prototyping and Rapid Manufacturing - Advanced research in virtual and Rapid Prototyping, Taylor & Francis, London, pp 103-107. 29. Sarment D.P., Sukovic P., Clinthorne N. (2003) Accuracy of implant placement with a stereolithographic surgical guide. Int J Oral Maxillofac Impl, 18(4):571-577. 30. Di Giacomo G.A., Cury P.R., de Araujo N.S., Sendyk W.R., Sendyk C.L. (2005) Clinical application of stereolithographic surgical guides for implant placement: preliminary results. J Periodontol, 76(4):503507. 31. De Beer D., Truscott M., Booysen G. Barnard L., van der Walt J. (2005) Rapid manufacturing of patient-specific shielding masks using RP in parallel with metal spraying. Rap Proto J, 11(5):298-303. 32. Zemnick C., Woodhouse S.A., Gewanter R.M., Raphael M., Piro J.D. (2007) Rapid prototyping technique for creating a radiation shield. J Prosth Dent, 97(4):236-241 33. Johnson E.A.C., Young P.G. (2005) On the use of a patient-specific rapid-prototyped model to simulate the response of the human head to impact and comparison with analytical and finite element models. J Biomech, 38(1):39-45. 34. Bibb R., Sisias G. (2002) Bone structure models using stereolithography: a technical note. Rap Proto J, 8(1):25–29. 35. Peters P., Langlotz F., Nolte L.-P. (2002) Computer assisted screw insertion into real 3D rapid prototyping pelvis models. Clin Biomech, 17(5):376–382. 36. Clinkenbeard R.E., Johnson D.L., Parthasarathy R., Altan M.C., Tan K.H., Park S.M., Crawford R.H. (2002) Replication of human tracheobronchial hollow airway models using a selective laser sintering rapid prototyping technique. AIHA J, 63(2):141-50. 37. Zhang W., Zhang S., Huang X., Wang, C. (2005) 3D treatment planning and simulating for craniofacial skeleton. Int J Adv Manuf Technol, 26: 1043–1047. 38. He Y., Ye M., Wang C. (2006) A method in the design and fabrication of exact-fit customized implant based on sectional medical images and rapid prototyping technology. Int J Adv Manuf Technol , 28: 504–508. 39. Truscott M. , De Beer D., Vicatos G., Hosking K., Barnard L., Booysen G., Campbell I.R. (2007) Using RP to promote collaborative design of customised medical implants. Rap Proto J, 13(2):107-114. 20 40. Winder J., Cooke R.S., Gray J., Fannin, T. and T. Fegan, (1999) Medical rapid prototyping and 3D CT in the manufacture of custom made cranial titanium plates. J Med Engin Technol, 23(1):26-28. 41. D'Urso P.S., Earwaker W.J., Barker T.M., Redmond M.J., Thompson R.G., Effeney D.J., Tomlinson F.H. (2000) Custom cranioplasty using stereolithography and acrylic. Br J Plast Surg, 53(3):200-204. 42. Singare S., Dichen L., Bingheng L., Yanpu L., Zhenyu G., Yaxiong L. (2004) Design and fabrication of custom mandible titanium tray based on rapid prototyping. Med Engin Phys, 26(8):671-676. 43. Singare S. , Yaxiong L. , Dichen L., Bingheng L., Sanhu H., Gang L. (2006) Fabrication of customised maxillo-facial prosthesis using computer-aided design and rapid prototyping techniques. Rap Proto J 12(4):206 – 213. 44. He J., Li D., Lu B. (2006) Custom fabrication of a composite hemi-knee joint based on rapid prototyping. Rap Proto J, 12(4):198–205. 45. Liu Q., Leu M.C., Schmitt S.M. (2006) Rapid prototyping in dentistry: technology and application. Int J Adv Manuf Technol, 29: 317–335. 46. Chang C. C., Lee M. Y., Wang S. H. (2006) Digital denture manufacturing-An integrated technologies of abrasive computer tomography, CNC machining and rapid prototyping. Int J Adv Manuf Technol, 31: 41–49. 47. Eggbeer D., Bibb R., Williams R. (2005) The computer-aided design and rapid prototyping fabrication of removable partial denture frameworks. Proc Inst Mech Eng, 219(3):195-202. 48. Wu M., Tinschert J., Augthun M., Wagner I., Schadlich-Stubenrauch J., Sahm P.R., Spiekermann H. (2001) Application of laser measuring, numerical simulation and rapid prototyping to titanium dental castings. Dent Mater, 17(2):102-108. 49. Kruth J.-P., Vandenbroucke B., Van Vaerenbergh J., Naert I. (2005) Digital manufacturing of biocompatible metal frameworks for complex dental prostheses by means of SLS/SLM. In Virtual Prototyping and Rapid Manufacturing - Advanced research in virtual and Rapid Prototyping, Taylor & Francis, London, pp 139-146. 50. Bibb R., Eggbeer D., Williams R. (2006) Rapid manufacture of removable partial denture frameworks. Rap Proto J, 12(2): 95-99. 51. Vandenbroucke B., Kruth J.-P. (2007) Selective laser melting of biocompatible metals for rapid manufacturing of medical parts. Rap Proto J, 13(4):196-203. 52. Hollander D.A., Von Walter M., Wirtz T., Sellei R., Schmidt-Rohlfing B., Paar O., Erli H.-J. (2006) Structural, mechanical and in vitro characterization of individually structured Ti–6Al–4V produced by direct laser forming. Biomater, 27(7):955-963. 53. Li X., Wang J., Shaw L.L. (2005) Laser densification of extruded dental porcelain bodies in multimaterial laser densification process. Rap Proto J, 11(1):52–58. 54. Ciocca L., Scotti R. (2004) CAD-CAM generated ear cast by means of a laser scanner and rapid prototyping machine. J Prosthet Dent, 92(6):591-595. 55. Al Mardini M., Ercoli C., Graser G.N. (2005) A technique to produce a mirror-image wax pattern of an ear using rapid prototyping technology. J Prosthet Dent, 94(2):195-198. 56. Bens A., Seitz H., Bermes G., Emons M., Pansky A., Roitzheim B., Tobiasch E., Tille C. (2007) Nontoxic flexible photopolymers for medical stereolithography technology. Rap Proto J, 13(1):38-47. 57. Curodeau A., Sachs E., Caldarise S. (2000) Design and fabrication of cast orthopedic implants with freeform surface textures from 3-D printed ceramic shell. J Biomed Mater Res, 53:525–535. 58. Hunt J.A., Callaghan J.T., Sutcliffe C.J., Morgan R.H., Halford B., Black R.A. (2005) The design and production of Co–Cr alloy implants with controlled surface topography by CAD–CAM method and their effects on osseointegration. Biomater, 26(29):5890-5897. 59. Hutmacher D.W., Sittinger M., Risbud M.V. (2004) Scaffold-based tissue engineering: rationale for 21 computer-aided design and solid free-form fabrication systems. Trends Biotech, 22(7):354-362. 60. Kim B.S., Mooney D.J. (1998) Development of biocompatible synthetic extracellular matrices for tissue engineering. Tren Biotech, 16(5):224-230. 61. Chen Z., Li D., Lu B., Tang Y., Sun M., Wang Z. (2004) Fabrication of artificial bioactive bone using rapid prototyping. Rap Proto J, 10(5):327–333. 62. Woesz A., Rumpler M., Stampfl J., Varga F., Fratzl-Zelman N., Roschger P., Klaushofer K., Fratzl P. (2005) Towards bone replacement materials from calcium phosphates via rapid prototyping and ceramic gelcasting. Mat Sci Engin:C, 25(2):181-186. 63. Xu S., Li D., Lu B., Tang Y., Wang C., Wang Z. (2007) Fabrication of a calcium phosphate scaffold with a three dimensional channel network and its application to perfusion culture of stem cells. Rap Proto J, 13(2):99-106. 64. Sachlos E., Reis N., Ainsley C., Derby B., Czernuszka J.T. (2003) Novel collagen scaffolds with predefined internal morphology made by solid freeform fabrication. Biomater, 24(8):1487–97. 65. Yeong W.-Y., Chua C.-K., Leong K.-F. (2006) Indirect fabrication of collagen scaffold based on inkjet printing technique. Rap Proto J, 12(4):229–237. 66. Taylor P.M., Sachlos E., Dreger S.A., Chester A.H., Czernuszka J.T., Yacoub M.H. (2006) Interaction of human valve interstitial cells with collagen matrices manufactured using rapid prototyping. Biomater, 27:2733–2737. 67. Chen V.J., Smith L.A., Ma P.X. (2006) Bone regeneration on computer-designed nano-fibrous scaffolds. Biomaterials, 27:3973–3979. 68. Seitz H., Rieder W., Irsen S., Leukers B., Tille C. (2005) Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J Biomed Mater Res B Appl Biomater, 74(2):782-788. 69. Leukers B., Gulkan H., Irsen S.H., Milz S., Tille C., Schieker M., Seitz H. (2005) Hydroxyapatite scaffolds for bone tissue engineering made by 3D printing. J Mater Sci Mater Med, 16(12):1121-1124. 70. Chim H., Hutmacher D.W., Chou A.M., Oliveira A.L., Reis R.L., Lim T.C., Schantz J.-T. (2006) A comparative analysis of scaffold material modifications for load-bearing applications in bone tissue engineering. Int J Oral Maxillofac Surg, 35:928-934. 71. Dellinger J.G., Eurell J.A.C., Jamison R.D (2006) Bone response to 3D periodic hydroxyapatite scaffolds with and without tailored microporosity to deliver bone morphogenetic protein. J Biomed Mater Res, 76A: 366–376. 72. Miranda P., Saiz E., Gryn K., Tomsia A.P. (2006) Sintering and robocasting of β-tricalcium phosphate scaffolds for orthopaedic applications. Acta Biomat, 2:457–466. 73. Williams J.M., Adewunmi A., Schek R.M., Flanagan C.L., Krebsbach P.H., Feinberg S.E., Hollister S.J. Das S. (2005) Bone tissue engineering using polycaprolactone scaffolds fabricated via selective laser sintering. Biomater, 26(23):4817-4827. 74. Tan K.H., Chua C.K., Leong K.F., Cheah C.M., Cheang P., Abu Bakar M.S., Chua S.W. (2003) Scaffold development using selective laser sintering of polyetheretherketone–hydroxyapatite biocomposite blends. Biomater, 24(18):3115-3123. 75. Huang H., Oizumi S., Kojima N., Niino T., Sakai Y. (2007) Avidin–biotin binding-based cell seeding and perfusion culture of liver-derived cells in a porous scaffold with a three-dimensional interconnected flow-channel network. Biomater, 28:3815–3823. 76. Chua C.K., Leong K.F., Cheah C.M., Chua S.W. (2003) Development of a Tissue Engineering Scaffold Structure Library for Rapid Prototyping. Part 1: Investigation and Classification. Int J Adv Manuf Technol, 21:291–301 77. Naing M.W., Chua C.K., Leong K.F., Wang Y. (2005) Fabrication of customised scaffolds using computer-aided design and rapid prototyping techniques. Rap Proto J, 11(4):249–259. 22 78. Lee S.-J., Kang H.-W., Kang T.-Y., Kim B., Lim G., Rhie J.-W., Cho D.-W. (2007) Development of a scaffold fabrication system using an axiomatic approach. J Micromech Microeng, 17:147–153. 79. Landers R., Pfister A., Hubner U., John H., Schmelzeisen R., Mulhaupt R. (2002), Fabrication of soft tissue engineering scaffolds by means of rapid prototyping techniques. J Mater Sci, 37(15):3107-3116. 80. Moroni L., Schotel R., Sohier J., De Wijn J.R., Van Blitterswijk C.A. (2006) Polymer hollow fiber threedimensional matrices with controllable cavity and shell thickness. Biomater, 27(35):5918-5926. 81. Moroni L., De Wijn J.R., Van Blitterswijk C.A. (2006) 3D fiber-deposited scaffolds for tissue engineering: Influence of pores geometry and architecture on dynamic mechanical properties. Biomater, 27(7):974-985. 82. Li J.P., De Wijn J.R., Van Blitterswijk C.A., De Groot K. (2006) Porous Ti6Al4V scaffold directly fabricating by rapid prototyping: Preparation and in vitro experiment. Biomater, 27(8):1223-1235. 83. Xiong Z., Yan Y., Zhang R., Wang X. (2005) Organism manufacturing engineering based on rapid prototyping principles. Rap Proto J, 11(3):160–166. 84. Yan Y., Wu R., Zhang R., Xiong Z., Lin F. (2003) Biomaterial forming research using RP technology. Rap Proto J, 9(3):142–149. 85. Yan Y., Wang X., Pan Y., Liu H., Cheng J., Xiong Z., Lin F., Wu R., Zhang R., Lu Q. (2005) Fabrication of viable tissue-engineered constructs with 3D cell-assembly technique. Biomater, 26:5864– 5871. 86. Vozzi G., Flaim C., Ahluwalia A., Bhatia S. (2003) Fabrication of PLGA scaffolds using soft lithography and microsyringe deposition. Biomater, 24:2533–2540. 87. Khalil S., Nam J., Sun W. (2005) Multi-nozzle deposition for construction of 3D biopolymer tissue scaffolds. Rap Proto J, 11(1):9–17. 88. Xu T., Gregory C.A., Molnar P., Cui X., Jalota S., Bhaduri S.B., Boland T. (2006) Viability and electrophysiology of neural cell structures generated by the inkjet printing method. Biomater, 27:3580– 3588. 89. Razzacki S.Z., Thwar P.K., Yanga M., Ugaz V.M., Burns M.A. (2004) Integrated microsystems for controlled drug delivery. Adv Drug Del Rev, 56:185– 198. 90. Ikuta K., Takahashi A., Maruo S. (2001) In-chip cell-free protein synthesis from DNA by using biochemical IC chips. Proc 14th IEEE Int Conf MEMS 2001, pp 455-458. 91. Kızılel S., Sawardecker E., Teymour F., Pérez-Luna V.H. (2006) Sequential formation of covalently bonded hydrogel multilayers through surface initiated photopolymerization. Biomater, 27(8):1209-1215. 92. Lu Y., Chen S.C. (2004) Micro and nano-fabrication of biodegradable polymers for drug delivery. Adv Drug Del Rev, 56(11):1621-1633. 93. Matsuda T., Mizutani M. (2002) Liquid acrylate-endcapped biodegradable poly(ε-caprolactone-cotrimethylene carbonate) II. Computer-aided stereolithographic microarchitectural surface photoconstructs. J Biomed Mat Res, 62(3):395-403. 94. Itoga K., Kobayashi J., Yamato M., Kikuchi A., Okano T. (2006) Maskless liquid-crystal-display projection photolithography for improved design flexibility of cellular micropatterns Biomater, 27(15):3005-3009. 95. Cheng Y.-L. and Lin J.-H. (2007) Manufacture of three-dimensional valveless micropump. J Mater Proc Tech, 192-193:229-236. 96. Rowe C.W., Katstra W.E., Palazzolo R.D., Giritlioglu B., Teung P., Cima M.J. (2000), Multimechanism oral dosage forms fabricated by three dimensional printing. J Contr Rel, 66:11–17. 97. Low K.H., Leong K.F., Chua C.K., Du Z.H., Cheah C.M. (2001) Characterization of SLS parts for drug delivery devices. Rap Proto J, 7(5):262-268. 98. Leong K.F., Chua C.K., Gui W.S., Verani (2006) Building Porous Biopolymeric Microstructures for 23 Controlled Drug Delivery Devices Using Selective Laser Sintering. Int J Adv Manuf Tech, 31: 483–489. List of Figures Fig. 1. Skull biomodel of an injured girl for surgical planning fabricated with SL. Fig. 2. SLS lastic and metal sprayed shielding masks [31]. Fig. 3. The SL pattern (a) for the casting of the titanium joint (b) and the negative pattern (c) for the corresponding porous bone (d) [44]. Fig. 4. Ear model manufactured with 3D printing to serve as vacuum casting pattern for the fabrication of an ear substitute [54]. Fig. 5. 3D models of possible scaffold structures for CAD scaffold modeling [77]. Fig. 6. Microneedle array fabricated with micro-stereolithography [93]. 24 Figure 1 25 Figure 2 26 (a) (b) (c) (d) Figure 3 27 Figure 4 28 Figure 5 29 Figure 6 30






© Copyright 2025