
NEWS OF NEW YORK - Medical Society of the State of New York
Workers’ Comp Survey MEDICAL SOCIETY OF THE STATE OF NEW YORK NEWS OF NEW YORK Volume 71 • Number 2 • www.mssny.org pages 6-8 Providing Information to Assist Physicians in the State of New York Results of MSSNY’s Workers’ Compensation Poll MSSNY conducted a poll of physician members in December about the Workers’ Compensation Program. The purpose was to generate data that was incorporated into testimony delivered by Dr. Robert Goldberg – a member of MSSNY’s Workers’ Comp Committee – to an Assembly committee hearing in December. See page 6 for more poll results and physician comments. High-Volume Hydraulic Fracturing Will Not Move Forward in NY The NYS Department of Health has completed its public health review of high-volume hydraulic fracturing (HVHF) and DOH Commissioner Dr. Howard Zucker recommended that high-volume hydraulic fracturing should not move forward in New York State. DOH’s review can be found at: www.health.ny.gov/press/reports/docs/high_volume_hydraulic_fracturing.pdf “I have considered all of the data and find significant questions and risks to public health which as of yet are unanswered,” said Dr. Zucker. “I think it would be reckless to proceed in New York until more authoritative research is done. I asked myself, ‘would I let my family live in a community with fracking?’ The answer is no. I therefore cannot recommend anyone else’s family to live in such a community either.” DEC will incorporate the findings of the public health review into the Final SGEIS, which will be released with a response to public comments early next year. DOH’s review found significant uncertainties about: the adverse health outcomes that may be associated with HVHF; the likelihood of occurrence of adverse health outcomes; and the adequacy of mitigation measures to protect public health. DOH’s report concludes that it will be years until science and research provide sufficient information to determine the level of risk HVHF poses to public health and whether those risks can be adequately mitigated. Given the red flags raised by current studies, absent conclusive studies that disprove health concerns, the report states the activity should not proceed in New York State. In conducting its public health review, DOH reviewed and evaluated scientific literature, sought input from outside public health experts, engaged in field visits and discussions with health and environmental authorities in nearly all states where HVHF activity is taking place, and communicated with local, state, federal, international, academic, environmental and public health stakeholders. Join the White Coat Armada on March 4 in Albany! Call your County Executive for more information today! February 2015 MSSNY Urges Governor and Legislature to Delay E-Prescribing Requirement; Physician Action Needed MSSNY is urging that New York State delay implementation of the E-prescribing requirement for all substances due to the fact that several EHR systems currently used by physicians and hospitals have not yet been certified by the DEA to enable electronic prescribing of controlled substances. As such, MSSNY has argued that it is unfair to hold physicians responsible for the failure of vendors to meet this deadline. MSSNY leadership and staff have had discussions with the administration and some members of the Legislature to request this delay. MSSNY is urging physicians to assist in this effort by sending a letter calling for delay of the implementation date. Physicians can send a letter to their legislators and Governor Cuomo urging a postponement of this mandate by going here. The E-prescribing requirement goes into effect for non-controlled and controlled substances on March 27, 2015. This requirement was part of the I-STOP law that was approved unanimously by the Legislature. MSSNY has had numerous discussions with state officials and key legislative leaders to make them fully aware of the significant obstacles many physicians of all practice configurations will face in complying with this law, and the potential medication disruptions patients could face as a result. MSSNY, along with various medical specialties, will be sending a letter to Acting Commissioner Howard Zucker, MD, JD also asking for delay. MSSNY has also had extensive discussions with the state to assure that the process for physicians to apply for a waiver of this requirement will not be unduly burdensome. The law provides that physicians may apply for a waiver of this e-prescribing requirement as a result of a) economic hardship b) technological limitations that are not reasonably within the control of the physician, or c) other exceptional circumstance. MSSNY is encouraging that DOH consider including – as an example of an acceptable exigent circumstance which qualifies for a waiver – those instances where the physician prescribes less than 25 prescriptions per year. Send a letter to your legislator and Governor Cuomo urging a postponement of this mandate by clicking on this link http://bit.ly/1CZHBVE. Governor Cuomo Appoints Howard Zucker, MD Commissioner of NYSDOH Governor Cuomo recently appointed Howard Zucker, MD to serve as Commissioner of the State Department of Health. The appointment requires Senate confirmation. Previously, Dr. Zucker served as Acting Commissioner of the Department of Health as well as First Deputy Commissioner. Prior to that, he was a professor of Clinical Anesthesiology at Albert Einstein College of Medicine of Yeshiva University and a pediatric cardiac anesthesiologist at Montefiore Medical Center Howard Zucker, MD in the Bronx. He was also an adjunct professor at Georgetown University Law School, where he taught biosecurity law. His public policy experience began as a White House Fellow under then-Health and Human Services Secretary Tommy Thompson. He then became the Deputy Assistant Secretary of Health where he developed the nation’s Medical Reserve Corps. Dr. Zucker has also served as an Assistant Director-General of the World (Continued on page 2) Commissioner’s Grand Rounds: Ebola Past & Present (l-r): Katherine Hawkins, MD, NYSDOH; Anthony Shih, MD, Executive Vice President, NYAM; Hedva Shamir, MD, NYSDOH; Daniel S. Chertow MD, Department of Critical Care Medicine, National Institutes of Health; Lauren Johnston RN, Senior Vice President/ Chief Nursing Officer, NYCHHC; Charles Gonzalez, MD, NYSDOH; Andrew Kleinman, MD, MSSNY President Inside News E-prescribing: Use MSSNY-approved DrFirst.............page 2 Dr. Kleinman: “You can make a difference”....page 4 New Legislative session: meet your local rep..........page 4 DFS out of network proposal for resolution........page 5 Save the Dates for Legislation Day and AMSSNY Membership Meeting Join us in Albany on March 4th for Legislation Day as we lobby our legislators on behalf of our physician spouses. And mark your calendars for April 30 and May 1, when we’ll hold our 79th Annual AMSSNY Membership Meeting in Saratoga Springs in conjunction with the MSSNY House of Delegates. We ask your involvement in both of these events as a show of support to your physician spouse. We will provide further information in the next issue of News of New York. Over the last few months, Alliance members have been fundraising all across the state for scholarships for students entering health careers and for local community organizations. Some highlights include Richmond County Alliance members, who held a cocktail party December 7. Members and guests also brought unwrapped toys for the Salvation Army to distribute. In Onondaga County, Alliance members made a donation to the Athletic and Education Center on behalf of inner city youth and ARC of Onondaga County, which serves mentally handicapped children. Their holiday luncheon raised over $1500 for scholarships. AMSSNY is proud to support the New York State Physicians Home, an organization that helps physician families in need when a life crisis occurs. Please send contributions to Physicians Home, care of Dr. Joseph B. Cleary, President of the Physicians Home, 445 Park Ave, 9th Floor, NY, NY 10022 to honor a friend or family member or as a memorial to a family member, physician or friend. Our state Alliance contributes a portion of the funds raised at our Fall Leadership Conference and our Spring Annual Membership meeting to this worthy cause. We are grateful to our Kings County Member, Mrs. Betti Jabbour, who has been our liaison to the Physicians Home for the past ten years. Our organized counties in the state still contribute annually to the Physicians Home. Please check out the AMA Alliance online newsletter, The Alliance in Motion and the online resource Physician Family, edited by Donna Rovito with topics relating to physicians and spouses from residency to retirement. Not a member of AMSSNY? Please contact our Executive Director, Kathleen Rohrer at Krohrer@mssny.org or phone 1-800-523-4405 for an application. We welcome all spouses and domestic partners of physicians. See you in Albany and Saratoga Springs! Howard Zucker, MD Named Commissioner of NYSDOH (Continued from page 1) Health Organization and as an Institute of Politics Fellow at Harvard Kennedy School. He is a pediatrician, anesthesiologist, intensive care specialist and pediatric cardiologist trained at Johns Hopkins, University of Pennsylvania and Harvard, respectively, and has held faculty appointments at Yale, Columbia and NIH. Dr. Zucker has a B.S. from McGill University, an M.D. from George Washington University, a J.D. from Fordham University Law School, an LL.M from Columbia Law School and a postgraduate diploma in global health policy from the London School of Hygiene and Tropical Medicine. Comply with the DOH E-prescribing Mandate: Special Discount for MSSNY Members All Physicians Must Prescribe Electronically by March 27, 2015! Be Ready! MSSNY announced a new member benefit that will support you and your practice in complying with the new DOH mandate for e-prescribing. Through a special partnership with DrFirst, the industry leader in e-medication management, MSSNY members can receive a discount on Rcopia® and EPCS GoldSM, which will allow providers to e-prescribe both legend drugs and controlled substances in a single workflow. The software also includes real-time prescription monitoring, instant access to medication histories for patients, patient-specific formulary data, and clinical alerts such as drug-drug and drug-allergy interaction warnings. In addition, DrFirst will guide MSSNY members through the identity proofing and authentication processes that are required by the Drug Enforcement Agency to allow doctors to prescribe controlled substances electronically. For more information, and to receive your special MSSNY member discount, visit www.drfirst.com/MSSNY, or call the special MSSNY E-prescribing Hotline at 866-980-0553. Non-Acute Pain Treatment Guidelines for Workers Compensation Go Into Effect The New York State Workers Compensation Board issued a Bulletin in December (www.wcb.ny.gov/content/main/SubjectNos/sn046_742.jsp) noting that the new Non-Acute Pain Medical Treatment Guidelines, as well as the revisions to the existing Medical Treatment Guidelines, went into effect on December 15, 2014. To view the guidelines, click here: www.wcb.ny.gov/ content/main/hcpp/MedicalTreatmentGuidelines/NonAcutePainMTG2014.pdf. An online program to assist physicians and their staff in learning these new guidelines, which provides CME credit, are available on MSSNY’s website. The pain treatment guidelines were developed by a 13-member committee that included 11 physicians representing various specialties. These physicians included MSSNY Board of Trustees member and Touro College of Osteopathic Medicine Dean Robert Goldberg, MD and former MSSNY Board member and Rochester orthopedic surgeon Ted Tanner, MD as well as WCB medical directors Jamie Szeinuk, MD and Elaine Sobol Berger, MD, JD. To read a full list of the physicians on the committee, click here: www.wcb.ny.gov/content/ main/hcpp/MedicalTreatmentGuidelines/CoverltNonAcutePainMTG.pdf. Are you ready to e-prescribe on March 27, 2015? You will not be able to prescribe for your patients on March 28 if you do not have an electronic prescribing system in place. Page 2 • MSSNY’s News of New York • February 2015 THE POWER OF DIVIDENDS Dividends provide meaningful financial relief to policyholders of mutual insurance companies. We at MLMIC declare them when we can as part of our mission. Since 1975, we have returned in excess of $300 million to our policyholders – an accomplishment unmatched by any of our competitors. Endorsed by MSSNY Learn more at MLMIC.com/dividends or call (888) 996-1183 February 2015 • MSSNY’s News of New York • Page 3 MEDICAL SOCIETY OF THE STATE OF NEW YORK NEWS OF NEW YORK Medical Society of the State of New York Andrew Y. Kleinman, MD President Michael Rosenberg, MD Chairman of the Board Philip A. Schuh, CPA Executive Vice President COMMUNICATIONS AND PUBLICATIONS L. Carlos Zapata, MD, Commissioner News of New York Published by Medical Society of the State of New York Vice President, Communications and Editor Christina Cronin Southard, Editor csouthard@mssny.org News of New York Staff Julie Vecchione DeSimone, Assistant Editor jvecchione@mssny.org Roseann Raia, Communications Coordinator rraia@mssny.org Steven Sachs, Web Administrator ssachs@mssny.org Susan Herbst, Page Designer News of New York Advertising Representatives For general advertising information contact Christina Cronin Southard Phone 516-488-6100 ext 355 csouthard@mssny.org The News of New York is published monthly as the official publication of the Medical Society of the State of New York. Information on the publication is available from the Communications Division, Medical Society of the State of New York, 865 Merrick Avenue, P.O. Box 9007, Westbury, NY 11590. The acceptance of a product, service or company as an advertiser or as a membership benefit of the Medical Society of the State of New York does not imply endorsement and/or approval of this product, service or company by the Medical Society of the State of New York. The Member Benefits Committee urges all our physician members to exercise good judgment when purchasing any product or service. Although MSSNY makes efforts to avoid clerical or printing mistakes, errors may occur. In no event shall any liability of MSSNY for clerical or printing mistakes exceed the charges paid by the advertiser for the advertisement, or for that portion of the advertisement in error if the primary or essential message of the advertisement has not been totally altered or substantially rendered meaningless as a result of the error. Liability of MSSNY to the advertiser for the failure to publish or omission of all or any portion of any advertisement shall in no event exceed the charges paid by the advertiser for the advertisement, or for that portion of the advertisement omitted if the primary or essential message of the advertisement has not been totally altered or substantially rendered meaningless as a result of the omission. MSSNY shall not be liable for any special, indirect or inconsequential damages, including lost profits, whether or not foreseeable, that may occur because of an error in any advertisement, or any omission of a part or the whole of any advertisement. MEDICAL SOCIETY OF THE STATE OF NEW YORK AT YOUR SERVICE MSSNY’S WESTBURY OFFICE Main Phone Number......................................516-488-6100 Toll Free Number...........................................800-523-4405 Main Fax Number..........................................516-488-1267 MSSNY Website......................................... www.mssny.org Extensions for specific services Alliance.. ........................................................................396 Communications............................................................ 351 Computer Information Systems..................................... 361 Member Benefits/Marketing.......................................... 424 Membership Information............................................... 336 Medical, Educational & Scientific Foundation.............. 350 Office of the Executive Vice President.......................... 397 Ombudsman Claims Assistance..................................... 318 Physician Records/Credentials....................................... 367 Socio-Medical Economics............................................. 332 albany office Continuing Medical Education...........518-465-8085 ext.17 Public Health Committees.................518-465-8085 ext. 11 Governmental Affairs.....................................518-465-8085 Fax..................................................................518-465-0976 Other Numbers Committee for Physicians’ Health.................800-338-1833 Dispute Resolution Agency............................516-437-8134 Kern, Augustine, Conroy & Schoppman.......516-294-5432 Page 4 • MSSNY’s News of New York • February 2015 PRESIDENT’S COLUMN You Can Make A Difference Can you really make a difference in the future of medicine? Absolutely. Can taking one day away from your practice to lobby in Albany really have a meaningful impact on the development of policy? You bet it does. I implore you to join the hundreds Andrew Y. of your physician colleagues from Kleinman, MD across the State on Wednesday, March 4 in Albany to advocate on behalf of our patients so they can continue to receive the timely quality care they need and deserve. Contact your county medical society today to make arrangements to attend! With the endless array of issues we face this year, it is more important than ever for physicians to be seen and heard. And with government officials discussing profound changes to how health care is paid, it is essential that physicians have a major part in these discussions rather than only health insurance companies and large institutions. We have a talented and dedicated group of lobbyists fighting on our behalf every day in Albany, but there is nothing that can quite replace the impact of your legislators hearing directly from you on their “home turf,” preferably in your white coat, about the concerns that impact your patients and their constituents. It is so important that the legislators and staff who shape our health care policy see an armada of white coats walking through the Capitol and through the Legislative Office Building so they have an immediate and clear reminder of the impact that their proposed policies will have on the delivery of care to the patients in their districts. This year, we will be returning to the format we used in previous years where hundreds of our physician colleagues, medical students, medical staff, spouses and physician association staff gather in “The Egg” to hear from our top legislative leaders and key committee chairs as to how they plan to address our concerns, and respond to our questions. After this program, you will then have the opportunity to meet with your local legislators, arranged by your county medical society. Our Fight Among the many issues we will be fighting for is fixing narrow physician networks, addressing excessive roadblocks imposed by greedy insurance companies standing in the way of our patients receiving needed care, and assuring our patients can purchase comprehensive out of network coverage. We will be fighting State Budget proposals that would impose heavy-handed regulation of physician owned urgent care centers and office-based surgery sites. We will be fighting to prevent legislation to expand non-physicians’ scope of practice that threaten our patients’ health. We will be fighting to assure fair and flexible implementation of the new e-prescribing mandate that potentially threatens our patients’ ability to receive needed medications. And we will, of course, continue to fight for needed reforms to bring down our exorbitant medical liability costs. I know many of you visit with your local legislators back in their district office, and that is extremely important as well. However, every week in Albany legislators hear from numerous interest groups with legislative agendas that directly conflict with ours and our patients. Insurance companies and business groups argue why there should be (Continued on page 12) mssnypaC Legislative Session Begins Anew: Great Opportunity to Weigh in With New Members While the unfortunate passing of former Governor Mario Cuomo temporarily delayed the official start of the Legislative Session, we’ve now received the Governor’s State of the State Message and proposed budget for 2015-16 and work in Albany has spun up to a fever pitch. There is no shortage of issues that your MSSNY and MSSNYPAC are working on your behalf. We need your continued support and help. In his State of the State, the Governor presented his vision for 2015 entitled the ‘Opportunity Agenda’ designed to restore economic opportunity, create the best education system in the nation, and restore the public’s confidence and trust in our justice system. The Governor’s $142B proposed state budget sought to advance private capital investments to assist in supporting the restructuring of the health care delivery system and to empower the development and reimbursement for integrated care delivery systems such as the DSRIP Performing Provider Systems (PPSs). He also, however, proposed to enable the development of corporately owned care settings such as clinics in retail spaces while also proposing significant new regulation of the care which can be delivered by certain urgent care and office based surgical physician practices. Much attention will now focus on the details of these proposals. MSSNY will deliver its budget testimony to the Joint Hearing of the Assembly Ways & Means and Senate Finance Committee on February 2nd. The testimony will be accessible through the MSSNY website. We are also faced with the implementation of the e-prescribing mandate enacted into law without one negative vote two years ago. MSSNY has joined with 17 other prescriber and long term care organizations to request a delay in the implementation of this law. Moreover, MSSNY has invited its physicians and their patients to weigh in with the legislature on this request. Patients need to know what will happen in the event that their pharmacy does not have on hand the specific controlled substance prescribed to them because once the e-script is received by a pharmacy, the pharmacist may not send it on to another pharmacy. In addition, patients like to shop around for the lowest cost drugs, particularly when medication is in short supply. The e-prescribing law will now prevent them from doing so. In total, 27 new state lawmakers were elected in the November elections. There are 10 new state senators, among them seven Republicans who helped the party seize outright control in the upper house. In the Assembly there are 17 new members, including a number of Democratic pickups expanding the Democratic super majority to 106. It is important for organized medicine to get to know these new members and to inform them of our concerns regarding the important issues we confront. Please take time to reach out to your elected officials. It is also more important than ever before for physicians to join MSSNYPAC. If you are a member of MSSNYPAC, thank you! You have shown true dedication to your profession and patients. But we need so many more to also contribute. If you haven’t yet joined, please do so immediately by going to MSSNYPAC under the Governmental Affairs Tab on MSSNY’s new website. Together all of medicine can achieve tangible objectives which protect physician practices and the patient’s they serve. Please contribute now. Unless we play our fair part in political action, we risk losing further ground to those who seek to take away our ability to control the care we provide to our patients. Join MSSNYPAC today at www.mssny.org Regulations to Implement Independent Dispute Resolution for ER and “Surprise” Out-Of-Network Bills Proposed By DFS The New York State Department of Financial Services has formally proposed regulations to implement the Independent Resolution Dispute (IDR) component of the comprehensive out-of-network reform legislation enacted last year. To read a summary of the regulations, click here: http://dfs.ny.gov/ insurance/r_prop/rp200u.pdf. MSSNY has been engaged in substantial discussions on this proposed regulation with top DFS staff throughout the fall. If you have any comments on these proposed regulations, please contact ldears@mssny.org or mauster@mssny.org. As a reminder, the new law provides that, as of April 1, 2015, all bills for emergency care and other “surprise bills” for care by out-of-network physicians can be brought for resolution to an IDR entity after an insurer makes an initial “reasonable payment” for such care, and efforts to informally settle the payment dispute have been unsuccessful. Either the physician or insurer can apply for resolution by the IDR entity. The statute requires the IDR entity to choose between the plan’s payment or the out-of-network physician’s fee (“baseball arbitration”). Only in the rare instances where the reviewer believed that a settlement is reasonably likely or both the physician fee and insurer payment represent unreasonable extremes, the reviewer can give the parties 10 business days to negotiate a compromise. Claims for certain CPT codes under $600 are exempted from the IDR altogether. A physician of the same or similar specialty as the physician providing treatment is required to be involved in the review of the fee (the physician shall be licensed to practice in this state, to the extent practicable). The IDR entity is required to consider: • Whether there is a “gross disparity” between the fee charged by the out-of-network physician as compared to what they usually charge in other non-par situations Regressive Liability Bills Re-Introduced Among the first batch of bills re-introduced in the 2015 legislative session are a group of bills that MSSNY has strenuously opposed in previous legislative sessions that would impose huge new liability costs on physicians at a time when, as a result of significant Medicare, Medicaid, and commercial insurance company payment cuts, no increases in liability costs can be tolerated. These bills include: • A.164 (Weinstein)/S.336 (DeFrancisco) – would expand the nature of damages in wrongful death actions to include “pain and suffering” – estimated to increase premiums by 53%; • A.242 (Weinstein)/S.287 (DeFrancisco) – would prohibit “ex parte” interviews by defense counsel of plaintiff’s treating physicians in medical liability actions – estimated to increase premiums by 5%; • A.244 (Weinstein) – changes loss share rules regarding non-settling defendants – estimated to increase premiums by 5%; and • A.285 (Weinstein) – changes the existing 2.5-year statute of limitations for medical liability actions to a “date of discovery” rule – estimated to increase premiums by 15%. • Whether there is a “gross disparity” between the fee charged by the out-of-network physician as compared to other fees paid to similarly qualified non‐par physicians in the same region • The non-par physician’s usual charge for comparable services • Individual patient characteristics • The level of training, education and experience of the physician • The circumstances and complexity of the case, including the time and place of the services; and • The usual and customary cost of the service All decisions by the IDR entity, including those involving claims which the reviewer requests the parties to renegotiate, are required within 30 days of the application for decision by the IDR entity. Numerous Insurance Reform Bills Re-Introduced Including Top-Priority Collective-Negotiation Legislation Numerous pieces of legislation strongly supported by MSSNY in previous legislative sessions to address a wide variety of health insurer abuses have been re-introduced. These bills include: • A.355 (Gottfried)/S.1157 (Hannon) - enables independently practicing physicians to jointly negotiate patient care terms with health insurance companies under close supervision by the state; • A.368 (Pretlow) - requires health insurers to issue joint checks for payment to an insured and their treating physician for payments for out-of-network care; • A.443 (Gottfried) – requires health insurers to use uniform credentialing and re-credentialing forms; • A.445 (Gottfried) – requires health insurers to use physicians of a same or similar specialty as the treating physician before denying coverage for such care; • S.695 (Avella) - requires health insurers to assure continuity of coverage of necessary for prescription drugs for patients when formularies/tier status changes. Proposed Regulations on Marijuana Use for Treatment of Certain Conditions Governor Andrew Cuomo recently released regulations on the use of marijuana for certain medical conditions. The regulations are now subjected to a 45 day public comment period. A. 6357E/S.7923 was sponsored by Assembly member Richard Gottfried and Senator Diane Savino. Under the bill’s provisions (A.6357E/S.7923), the New York State Department of Health will operate the program and physicians will need to register with DOH to be able to “certify” that the patient meets the criteria for medical use of marijuana. A copy of the regulations is posted here. MSSNY will be submitting comments and MSSNY physicians are encouraged to submit these comments to Pat Clancy, MSSNY’s vice president for Public Health and Education at: pclancy@mssny. org. Comments will be organized into a letter and submitted to the state. February 2015 • MSSNY’s News of New York • Page 5 Results of MSSNY’s Wor (Continued from page 1) Anesthesiologists Money needs to be earned a minimum of 4 times: once to see the patient; another to deal with paperwork/forms/work notes/ disability paperwork; another to bill it; and another to collect it again and again. Then we need time to call patient’s attorneys to get it collected, plus time to review guidelines to determine if testing or procedures can be done. Oops, if we mess up, we may do diagnostic studies on a patient whose insurance requires them to go somewhere else and we will never get paid. Rates are dismally low for anesthesiologists. If I had a choice, I would never treat a WC patient. If cuts go through, I will not be able to maintain office salaries needed to process and care for WC patients. If these changes are made, we will not be able to afford to take care of WC patients and will withdraw from WC. Emergency Physicians In light of more time consumption in administrative process, physician time, etc., deserved compensation to pay for office expenses should be not curtailed. Family Practitioners If payments are decreased, or even stay the same, I will soon stop treating WC patients. The main problem with Workers’ Compensation patients is the tendency of the patient to become manipulative with regard to their return to work status, and employer’s unwillingness to accept work restricted employees. Private insurers deny the claims and give strange and novel reasons. If rates are cut, we will drop our remaining workers comp patients. We already have stopped accepting new Workers’ Comp patients because of the headaches involved. WC should provide in service training for providers with very clear guidelines for treatment of WC patients. (needs clarity and simplicity). I no longer participate in Workers’ Comp. I currently do NOT take new WCB patients because of the low reimbursement and paperwork required. We need an increase, at least to the Medicare rate. Payment is not the issue. Comp fails to provide good care for patients. Patients are very stressed by the delays in approval for testing, therapy and medications. I would appreciate emails from WCB regarding guidelines, statistics, education, etc. General Surgeons This is another insurance company plan to increase their profit bottom line at the expense of physicians. Worker’s Compensation Board should be abolished. Lot of folks (MDs, patients, PTs, OTs, pharmacists, lawyers, etc.) take advantage. Internal Medicine Physicians Before working for a hospital, WC cases represented a significant drain on resources without commensurate compensation. Services were performed as a service to the patient. It was generally looked on as a money-losing situation. I rarely accept WC because of these issues. I hate when I have a WC case – I hate the form – it can turn a simple visit into a long visit just so I can get the form done. I avoid WC patients. Neurologists If cuts of this magnitude are instituted I will be forced to leave practice in NY State and look for employment in another part of the country. Page 6 • MSSNY’s News of New York • February 2015 If there are cuts I will no longer accept WC patients. There should be an increase in the compensation, not a decrease! I have decreased the number of Comp cases that I see due to the fact that I have to literally fight to get paid by insurance companies at NYS comp rates. The work that goes into a Comp claim is far beyond that which any person should have to tolerate. I get upset once the patient gets validity to a comp claim and then goes to an “under the table” type of job. It happens more often than you think. physician who is willing to treat them for fewer reimbursements. Some of these reasons are also the reason why more and more physicians are opting out of Medicare as well. To follow in Medicare’s footsteps will be detrimental to workers and physicians. In this specialty the annual overhead including malpractice is well over $250,000. You would need to treat many, many, many workers to break even and exhausted physicians are not good physicians. If anything, an increase in reimbursements is overdue. Would be a huge burden. Opthalmologists I dropped my WC load to near zero because of the paperwork hassle, the low frequency of payments and the low payments. The fee schedule has not changed in more than 10 years. Very hard system to deal with. Neurosurgeons I am clinical director of a Level 1 trauma center in Buffalo. I always treat Workers’ Compensation patients, and make great efforts. The hospital expects no less. Recently I have declined to accept non-emergency WC cases because of anticipated legal/insurance disputes. If they lower the fees then I will resign from seeing WC patients. It will not be cost effective. WC patients take up a substantial amount of time with accident history, physical exams, administration (forms, authorizations, reports, disability, hearings, medical records, depositions, letters to employers). If the reimbursements were to decrease, the patient (workers) will suffer greatly because providers will no longer want to participate with WC and it would be harder for the patient (worker) to find a board certified The workers comp system is so bad that lots of patients prefer to be treated under their own insurance for an injury sustained at work, rather than WC. Orthopedic Surgeons I spend a considerable amount of time dealing with Workers’ Comp patients. It is fair to say that these patients are the most challenging to deal with because of their work related issues that I need to sort out. They represent a significant increase (at least double) in the amount of time my staff and I deal with them in the office as well as the post clinic administrative expenses they present. Comp injuries need to be treated in a timely matter but it is significantly more cost intensive to the practice. A decrease in payment will definitely force us to stop or limit compensation patients. If WC compensation decreases, we will stop seeing those patients. Patient care is slowed down due to paper- rkers’ Compensation Poll work processes. Authorization processes cause delays. Paperwork delays cause patient care delays. If the proposed reimbursement changes go through, I would be unable to add any new WC patients to my practice. I am looking at unpaid claims for greater than 6 months. This is not sustainable for my practice. This would affect no-fault fees, which have their own problems. I would be inclined to stop taking care of WC patients if the proposed adjustment goes forward. If WC decreases their fee schedule, I will no longer accept WC patients. Too much work and risk for already low compensation. My practice is talking about no longer seeing Workers’ Comp patients. If the fees are reduced to 130% of Medicare then I will no longer treat WC patients. We are eager to drop WC from our practice. Too much of a headache. Changing the fee structure using the Medicare RBRVS will negatively and critically impact the ability for the orthopedic practice to continue to treat Workers’ Compensation patients. If the proposed changes are enacted, I will no longer accept WC patients. We would like to continue to take care of our WC patients, but the administrative burden of treating these patients continues to grow. All we ask for is a fair reimbursement for the significant amount of time and manpower this requires. I would not accept or treat WC patients if they were reimbursed at the Medicare Fee schedule. The combination of the administrative burden, authorization and complex pre-op and post-operative complaints would make it impossible from a time/economic standpoint. As an orthopedic surgical practice, my staff and I tolerate the WC paperwork because payment for surgery cases is higher than commercial. Pick a state that has a WC system that works for patients and doctors and copy that. I will stop seeing WC patients if paid as Medicare. When we call for non-payment of bills, insurance carriers do not return our calls or say they have nothing on file. Very frustrating, If rates are dropped, I, along with my 15 partners, will no longer be able to see WC patients. It would be too taxing on our office staff/bottom line without appropriate reimbursement. If there are significant cuts I just won’t do any Workers’ Compensation. If the fee schedule is inappropriately reduced, we will anticipate cutting back on the number of Workers’ Compensation patients that we see, and may need to discharge patients given the administrative burden that WC patients place on our practice. I have one full time employee and one part-time employee whose only job is just dealing with WC paper work and issues. If WC decreases their fees I will stop seeing these patients and not waste my time. It is much more expensive to provide care for WC patients in terms of money and time. I will not accept WC patients at the Medicare fee schedule. Will VERY strongly consider discontinuing seeing WC patients if reimbursement is decreased. It is simply not cost effective and, quite frankly, not rewarding. The ‘hassle factor’ is barely offset by the present reimbursement rates. Add in the across-the-board poorer outcomes in this population and it is, generally speaking, an undesirable duty to provide care to these patients. Secondary gain is rampant. There will continue to be an exodus of caregivers if reimbursement is decreased and that is a cold, hard fact. It will simply be ‘not worth it’ on many levels. If the rest of my group would allow it, I would refuse to see Workers’ Comp patients because the administrative burdens are enormous. I will no longer see WC patients if fees are reduced as planned. I will probably not take care of Workers’ Compensation patient’s issues if there is a payment reduction. I will not be able to survive in my practice in Workers’ Compensation rates. Reimbursement needs to be increased; otherwise, we will drop it. The changes to the WC program have made it a HUGE administrative burden. Many of my colleagues quit taking WC patients altogether. The reimbursement verses the expense is grossly disproportionate and I too am on the verge of saying NO to NYS WC patients. We will stop seeing any WC patients if this change goes through. The paperwork burden is much too large. If reimbursement decreases, I will definitely see less WC patients, and I may simply give up my WC number. State insurance fund is the worst! If there are any reductions in payments for WC patients, I will no longer be able to provide care for these injured workers. It simply would not be feasible. I will not be able to continue to see WC patients if this change is made. If the present rates for WC are cut to the proposed level, then it will no longer make any sense to employ the extra staff or deal with the administrative burden and inefficient WC system. All that will change will be the reimbursement. I will no longer participate in WC as it will be work that will occur at a loss financially. This will also affect NF rates potentially and that will put further strain on fragile office expense/profitability issues. I am considering non-participation in WC if these changes occur. We plan to strongly consider dropping WC if the proposed new fee schedule is adopted. Orthopedic surgeons treat most workers comp patient. Reducing the reimbursement rate to help primary MDs will not aid W/C patients, as primary MDs will not fill the deficits of lost orthopedic surgeons. Demands on the office are overwhelming with MTGs causing constant time spent complying. loss of income benefits for the patient who has his/her recovery delayed by the system. I have been semi-retired for 2 years, enjoy it and feel I provide a service of non-op ortho, but must fully retire because of increased cost, EMR, CME, document requirements and malpractice. Would not consider treating WC at anywhere near the Medicare fee schedule. WC patients are taxing to myself and my staff and I cannot treat them at a lower fee schedule. Reducing payments to the level of normal insurance reimbursement will make it less likely that I would care for a WC patient. Without the shadow of a doubt I will withdraw from Workers’ Comp if any such fee change occurs. We have one of the worst paying and broken WC systems in the country. We should be using a percentage of Fairhealth, not Medicare. This is outrageous. Medicare is a government run charity. Workers’ Comp should be paid like Illinois or New Jersey. It’s time consuming with the most challenging patients. This is where doctors must unite and we need a fee increase as a percentage of Fairhealth. I know a survey conducted by the NYSOS revealed that over 85 percent of orthos will withdraw from Workers’ Comp. This is truly an all-out assault on our value as physicians in NY state. Will probably not take WC patients if proposed fee schedule is implemented. If the proposed fee schedule is adopted, there will be significant access issues. I have made plans to significantly limit the number of new WC patients I see. Probable reduction of at least 75% of the numbers I see now. Workers’ Comp cases are harder to treat because there are challenges and questions that slow things down every step of the way. We use more phone and staff time on WC than any other carrier. We are asked to justify the work-relatedness (which is understandable) and we are often trapped between the carrier and the patient whom we are trying to help. Orthopedics (my specialty) is especially important in treating WC patients and needs to be able to make decisions. If this goes to Medicare equivalent rates I will no longer participate in Workers’ Compensation. If Worker’s Compensation rates do not increase there will be no treatment of these patients. If cuts are made, I will ration access to comp patients significantly. It is just not worth my time, if I am not adequately reimbursed. Instead of 4-6 new comp patients per day, I envision allowing one appointment per day. They will just have to wait or find someone else. Pain Management Physicians NY State WC expenses are so much higher because the doctor’s decisions for tests and surgery can be challenged. The expense is not only from lawyer and court costs and increased administrative costs for the doctor’s office, but also from the huge increase of costs to the employer for the amount of extra time the patient is out of work and the WC patients require significantly more time, patience and medical care compared to the non-WC patients. WC administrative tasks are very burdensome, time consuming and full of loopholes. Even after completing all the requirements, payments are low and often not made at all. Then there’s the administra- I have stopped taking new WC patients because of all the aggravation there is in trying to treat these patients. Time spent, slow or no pay, hearings and paperwork, etc. Will stop accepting WC patients if this is passed. I have considered not seeing WC patients because of the amount of work needed and the poor reimbursement offered. (Continued on page 8) February 2015 • MSSNY’s News of New York • Page 7 Workers’ Compensation Survey (Continued from page 7) tive burden, time and resources to follow up on all the non-payments and under payments. A small practice cannot sustain itself with a Medicare-based WC fee schedule. Ultimately these WC patients will not have any physicians to see as we will most likely stop participating with WC, which is most likely the outcome WC wants in the end, at the expense and detriment to their own patients. Physical Medicine & Rehabilitation Physicians The paperwork associated with WC is excessive. Carriers use of out of state reviewers who use non-NY guidelines to down code and apply edits, reducing or denying payments. There is no recourse without needing additional manpower and time to appeal the denials. Invariably, the additional overhead cost negates any additional reimbursement that may be received. We end up writing off amounts rather than spending additional time and money trying to fight the carrier. The burden of documentation required for office visits is much more than that required for non WC patients as the narrative requires additional medical/legal documentation to support the multiple issues that need to be addressed in addition to the medical care. Medicare already underpays. But with the additional administrative burden of WC cases, my practice is very likely to stop seeing WC patients if the fee schedule changes for Electro diagnostic testing (my primary focus). Unfortunately, we already have a severe deficit of providers willing to see these patients and the fee schedule change will make it less likely that specialists like me will see them at all. Need payment increases; if it goes down, I will definitely stop taking Workers’ Comp. Plastic Surgeons The costs of practicing medicine have gone up. Rent, utilities, supplies and equipment, employee salaries (other than me) and malpractice until last year. Reducing already low fees makes no economic sense. Ask the legislators to consider how they would cope with a cut in their salaries by the same percentage as they will be cutting our reimbursements. How would they deal with the shortfall in income? How is it fair by any standard? Workers’ Compensation patients are often more complicated than the typical Medicare patient with complex injuries. Also, the expectations of the patients are different and can be more difficult and time consuming to manage. Every intervention requires an exhaustive approval process and my staff spends a significant amount of time with c4 forms, etc. I often need to have extra visits for no other reason than to document degree of disability. As Workers’ Compensation has been developed over the years, the reporting requirements have become more and more onerous. The most burdensome part of the program is the need to use their unique forms for almost all cases. For most of my 40 years in practice, I have written WCB patient reports with all the relevant WCB information in the report, including date of injury, employer, insurance, WCB #, Carrier Case#, etc., and have carefully outlined what we see on exam, hear on history and what we plan to do in response. To have to then repeat this same information repeatedly to justify a medication, to get a test or treatment and then to have to wait for, and often again protest, a response, is absurd. The system has been built to make it easy for the claims examiners, not for the patients and providers. Psychiatrists 1. Fees for psychiatry are totally inadequate. 2. No provisions to have effective punishment or fines for companies who are chronically very late in payment. 3. I have been told that I am the only psychiatrist in the area who still accepts WCB cases. I may change my policy unless the above two elements are remedied. We find these claims so time-consuming we outsource to eliminate the hassle, so it costs us more to see WC patients. Sports Medicine Physicians If the board elects to change reimbursement to a Medicare-like model, I believe this will cause a mass exodus of physicians due to the reality of not being FAIRLY compensated for all the work involved with taking care of each WC patient. Medicare doesn’t require constant requests for treatment, constant denials, and the stress of constant depositions which involve review of records and time taken outside of the practice for excessive paper work. Thoracic Surgeons I will no longer accept Workers’ Comp patients if the proposed changes go into effect. Urgent Care Physicians Workers’ Comp favors the insurance companies and is not fair to the patients or the doctors. We are one of the few practices taking it and are thinking of dropping it...major pain to deal with, no control of paper, fees, etc. I can no longer accept any new WC patients unless they dramatically increase the payments and adhere to the current CPT codes in use by all insurers including Medicare, not the outdated improper one. Vascular Surgeons Radiologists The denial rate for imaging services is close to 50% and it can take close to two years for the cases to be closed out. Cases are denied for no medical reason, but at the discretion of the carrier. Insurmountable paperwork now – everything is in favor of the carriers. LPNs and RNs dictating care along with deviant IME physicians providing opinions without proper exams. Dermatologists WC is a huge burden. If rates are cut, we will no longer agree to provide care to WC patients. Webinar on E-Prescribing Requirements Free To MSSNY Members An archived webinar on “New York State Requirement for E-Prescribing of ALL Substances” is now available free of charge to all MSSNY members. This program has been accredited for 1 AMA PRA Category 1 Credits™ and the educational objectives are to describe the following: • E-prescribing mandate, to whom it applies, when it becomes effective, and how physicians can comply with its requirements • the practitioner electronic prescribing of controlled substances registration process, to whom it pertains, and the information required to be provided by physicians in order to register eRX software with the Bureau of Narcotics Enforcement • exceptions to the e-prescribing mandate and any additional requirements associated with those exceptions • application process and criteria for a waiver from the e-prescribing mandate • rules that pertain to physicians who only prescribe non-controlled substances MSSNY physicians may register and access the archived webinar on the MSSNY website at: www.mssny.org/MSSNY/Public_ Health/Eprescribing.aspx The course is available to non-MSSNY physicians for $125 which can be applied to a MSSNY membership. Medical Society of The State of New York 2015 Albion O. Bernstein, MD Award The Medical Society of the State of New York is accepting nominations for the 2015 Albion O. Bernstein, MD Award. This prestigious award is given to “…the physician, surgeon or scientist who shall have made the most widely beneficial discovery or developed the most useful method in medicine, surgery or in the prevention of disease in the twelve months prior to December 2014.” This $2000 award was endowed by the late Morris J. Bernstein in memory of his son, a physician who died in an accident while answering a hospital call in November 1940. The award will be presented to the recipient during a MSSNY Page 8 • MSSNY’s News of New York • February 2015 Council Meeting. Nominations must be submitted on an official application form and must include the nominator’s narrative description of the significance of the candidate’s achievements as well as the candidate’s curriculum vitae including a list of publications or other contributions. To request an application, please contact: Committee on Education, Joanne Wise, Manager, Continuing Medical Education, Medical Society of the State of New York, 99 Washington Avenue, Suite 408, Albany, NY 12210 Call 518465-8085 or email jwise@mssny.org DEADLINE FOR NOMINATIONS: May 31, 2015. 257,000 Physicians Will Have Payments Cut in 2015 for Not Adopting EHR More than 257,000 U.S. doctors will see their Medicare payments cut by 1% this year because they didn’t meet federal goals for using electronic medical records, said the Centers for Medicare and Medicaid Services. Some 28,000 providers will be docked another 1% of Medicare pay for not prescribing medications electronically. About 200 hospitals were informed in October that they also will lose 1% of their Medicare payments in 2015 for missing a deadline for EMR use. The rules, part of the 2009 stimulus package, were designed to spur the health-care industry’s transition from paper files to electronic record keeping. Initially the law offered lucrative incentive payments if providers could demonstrate “meaningful use” of EMRs. Payment Adjustments Summary Applied to all Medicare reimbursement +As of April 1, 2013. ^Only groups with 100+ eligible professionals in 2015, and >10 in 2016. ~Penalties reported as maximums. Competency-Based Admissions: A New Initiative at the Albert Einstein College of Medicine Siobhan M. Dolan, MD, MPH, Noreen Kerrigan, MPA, and Michael J. Reichgott, MD, PhD, Albert Einstein College of Medicine, Bronx, NY The Association of American Medical Colleges (AAMC) has spearheaded two initiatives over the past 5 years that are having a strong effect on medical school admissions committees. These are holistic review of applicants and competency-based admissions. Together, these initiatives share the overall goal of assuring a diverse student body that will be capable of meeting the nation’s health care needs in the 21st century. These needs have been characterized as: access for all to preventive care; appropriate intervention when disease exists; and removal of disparities based on age, gender, ethnicity, disability, sexual orientation or any other personal characteristic.[1] While admissions standards for medical school have not changed over many years, the health care system has certainly changed in recent years to emphasize, “…greater integration across the medical education continuum, highly networked teams in discovery research, and inter-professionalism in clinical care[2].” These changing characteristics of the health-care system impact which candidates might be best suited to a successful career in medicine. Medical school admissions processes have historically placed greatest emphasis on measures of academic performance such as grades and standardized test scores. Now AAMC leaders are suggesting that fundamental change is needed in order to, “… select physicians with both the academic and interpersonal and intrapersonal competencies necessary to operate in the health care system of the future [3].” One means of achieving this is through holistic review of applicants, defined as a “flexible, highly individualized process by which balanced consideration is given to the multiple ways in which applicants may prepare for and succeed as medical students and doctors[4].” This holistic approach requires consideration of the many personal characteristics and abilities in addition to academics that best define a physician. Competency-Based Admissions In order to prepare applicants for a review that will evaluate, equally, their personal characteristics as well as their academic readiness for medical school, the Albert Einstein College of Medicine has developed a Competency-Based Admissions (CBA) process. This approach identifies for candidates the full set of skills and abilities they must have achieved at an acceptable, entry level, rather than just a checklist of courses that must have been completed. CBA provides applicants with greater flexibility, for example, by allowing scientific experience gained while employed, to be substituted for laboratory and/or course requirements taken in school. It also allows students the option of meeting academic expectations through appropriate work experiences, or by taking online courses, thereby freeing up time to pursue activities and interests that enhance an applicant’s level of maturity, cultural awareness, ability to work in team settings and other elements of readiness for medical practice in the 21st century. CBA supports Einstein’s explicit mission to identify matriculants who will undertake state-of-the art scientific inquiry while serving the need of the Bronx community by providing the highest quality clinical care. CBA promises to minimize obstacles to admission and supports the goal of educating physicians that are representative of and who will ultimately work in our Bronx community of over 1.4 million residents, 43.3% of whom identify as Black or African American and 54.6% who report some Hispanic or Latino ancestry[5]. (Continued on page 12) Suffolk County Announces Partnership with Adelphi University for MBA Program The Suffolk County Medical Society has announced a partnership with Adelphi University to offer its members an accelerated MBA program. The MBA program is designed to provide physicians with the tools necessary to run a more cost-effective practice, as well as become proficient in business strategies and acquire the skills necessary to become effective leaders in the rapidly-changing business of health care delivery. The program offered is 42 credits (14 threecredit courses), and will be taught by Adelphi University’s Robert B. Willumstad School of Business faculty. In addition, guest speakers will be invited to lecture which will bring added value to the program on updated busi- ness principles and how they affect healthcare. The program will be held in Islandia in the Suffolk County Medical Society Board Room one night a week. The projected start date of the program is February 2015. Maria A. Basile, MD, SCMS President and recent MBA graduate stated: “All around me I see strong physician leaders, members of our Medical Society and ‘The House of Medicine.’ You are a leader, just as I am, because of the trusted role we all play every day in people’s lives – trust, compassion, stability and hope are qualities people seek from their leaders. Aren’t these also traits that define ‘A True Physician’?” Special Discount for MSSNY Members: Comply with New York’s E-prescribing Mandate: Get Started with eRx Today NY Law: All Physicians Must Prescribe Electronically by March 27, 2015! Buy E-prescribing at a Reduced Rate The Internet System for Tracking OverPrescribing Act (I-STOP) was passed by the New York State legislature to help combat the rising rates of prescription drug abuse. On March 27th, all New York providers will need to electronically prescribe all legend drugs and controlled substance prescriptions. Complying with New York’s e-prescribing mandate is easy, and as a special member benefit, you will receive a reduced rate on DrFirst’s industry leading Rcopia® with EPCS GoldSM, which allow providers to e-prescribe both legend drugs and controlled substances in a single workflow. In addition, DrFirst will guide MSSNY members through the identity proofing and authentication processes that are required by the Drug Enforcement Agency to allow doctors to prescribe controlled substances electronically. DrFirst and MSSNY are hosting e-prescribing webinars to help you learn more about I-STOP and how you can become compliant by March 27th. Sign-up today using the registration links below: 1/27 @ 10:30am ET - http://bit.ly/1JtZX3s 2/4 @ 2pm ET - http://bit.ly/1JtZfDl 2/12 @ 4:30pm ET - http://bit.ly/188CUzF For more information, and to receive your special MSSNY member discount, visit www.drfirst.com/MSSNY, or call the special MSSNY E-prescribing Hotline at 866-980-0553. February 2015 • MSSNY’s News of New York • Page 9 MSSNY’s Socio-Med Division Helped Members to Recover over $168K MSSNY’s Division of Socio-Medical Economics was successful in helping MSSNY member physicians recover over $168K from various health plans during 2014. This activity was done for MSSNY members who availed themselves of the services of the Ombudsman Program. The Socio-Medical Economics Division is, for the most part, able to reach appropriate health plan staff to have claims paid, appealed and/or re-evaluated for proper reimbursement for services rendered to patients. If you have a claim problem, please call 516-488-6100 ext. 334. Resident/Fellow/Student Poster Symposium Abstract Submissions Now Open OBITUARIES MSSNY announces its next Resident/Fellow/Medical Student Poster Symposium, to be held Friday, May 1, 2015 at the Saratoga Hilton in Saratoga Springs, New York, from 2-4:30 pm. The deadline for abstract submission is 4 pm, February 15, 2015. Up to 70 abstracts will be chosen for poster presentation. Participants must either be a medical student or active in a residency/fellowship training program and they must be able to attend the meeting to present and discuss their entry. Additionally, they must hold current MSSNY membership. Membership is free for first-time resident/fellow members. Nonmember students and resident/fellows may join online at www.mssny. org. Detailed guidelines are available at http://tinyurl.com/q6gnknk or by contacting sbennett@mssny.org,516-488-6100 x 383. We are also seeking abstract scorers. If you are interested, please contact sbennett@mssny.org or call 516-488-6100 x 383. ANLLO, Victorino; North Tonawanda NY. Died December 02, 2014, age 91. Erie County Medical Society BRICKNER, Merol Ernest; Gloversville NY. Died December 09, 2014, age 102. Medical Society County of Fulton CHRISTIE, Joan Ann; Gloversville NY. Died December 09, 2014, age 82. Medical Society County of Fulton ELLISON, John Bingham; Middletown NY. Died March 22, 2014, age 86. Medical Society County of Orange FUCHS, Magdalena; New York NY. Died July 06, 2014, age 91. New York County Medical Society GLENN, Morton Bernard; West Palm Beach FL. Died March 01, 2014, age 91. New York County Medical Society KAPLAN, Norman Lionel; New York NY. Died November 14, 2014, age 81. New York County Medical Society LEPKO, Ervin Eugen; Englewood Cliffs NJ. Died May 03, 2014, age 86. New York County Medical Society MATTIMORE, Joseph M.; Hamburg NY. Died November 27, 2014, age 86. Erie County Medical Society MELAMED, Myron R.; Valhalla NY. Died December 15, 2014, age 87. New York County Medical Society POINTON, David Samuel; Johnstown NY. Died December 09, 2014, age 84. Medical Society County of Fulton RANDALL, Frederick R.; New York NY. Died March 29, 2014, age 91. New York County Medical Society SAMUELLY, Israel; Brooklyn NY. Died December 11, 2014, age 87. Medical Society County of Kings SAXE, David H.; Centereach NY. Died December 13, 2014, age 101. New York County Medical Society SAYOC, Oscar Z.; Orchard Park NY. Died December 13, 2014, age 77. Erie County Medical Society SHANBHAG, Madhukar A.; East Amherst NY. Died December 06, 2014, age 79. Erie County Medical Society SLOAN, Don; New York NY. Died December 16, 2014, age 85. New York County Medical Society WALKER, Leslie Allan; Fredericksburg VA. Died November 01, 2014, age 90. Monroe County Medical Society WHELAN, Joseph R.; Great Neck NY. Died December 22, 2014, age 89. Nassau County Medical Society Save the Date: MSSNY STATE LOBBY Day is March 4, 2015 Not a MSSNY Member? Join Now: 516-488-6100 Page 10 • MSSNY’s News of New York • February 2014 Members in the News Dr. William Spencer Named Long Islander News’ 2014 Person of the Year Long Islander News recently named Suffolk County Legislator William R. Spencer, MD, its 2014 Person of the Year for his “significant contributions to the Town of Huntington.” Each year, the newspaper honors William R. Spencer, MD “a dynamic force who has made history, gone above and beyond a call of duty and made Huntington a better place.” Now in his third year as a Suffolk County Legislator, Spencer has waged major battles to pass legislation—including a firstin-the-nation law that banned the marketing of energy drinks to minors; barring dangerous fracking byproducts from being used in the county; and raising the tobacco-buying age in Suffolk from 19 to 21. He serves as Chair of the Health Committee for the Suffolk County Health Department. A member of MSSNY since 2010, Dr. Spencer currently serves as the Presidentelect of the Suffolk County Medical Society and President of the Suffolk Academy of Medicine. He received his undergraduate degree from Wesleyan University and his medical degree from the University Of Connecticut School of Medicine. After completing his internship and residency in surgery at St. Vincent’s Hospital, Dr. Spencer completed a residency in otolaryngology at New York Eye and Ear Infirmary and a fellowship in pediatric otolaryngology at the University of Miami. In 2000, he opened his private practice, Long Island Otolaryngology and Pediatric Airway in Huntington. He currently serves as the Chief of Otolaryngology at Huntington Hospital. Dr. Victor Filadora Named Chief of Clinical Services at Roswell Park Cancer Institute Roswell Park Cancer Institute (RPCI) has named MSSNY member Victor Filadora, MD, as Chief of Clinical Services. In this new role, Dr. Filadora, an anesthesiVictor ologist first appointed Filadora, MD to the Institute’s medical staff in 2003, is responsible for managing the com- prehensive cancer center’s Ambulatory Services, Perioperative Services, Sterile Processing, Pharmacy, Patient and Family Experience, Endoscopy Services and Therapeutic Services programs, and will also provide leadership and guidance to clinical department administrators throughout the Institute. Dr. Filadora joined RPCI in 2003 from Brigham and Women’s Hospital in Boston, an affiliate of Harvard Medical School, where he served as Chief Resident for the Department of Anesthesiology. He served on the staff of Newton-Wellesley Hospital and the Tufts University School of Medicine The Health Care Law Experts Representing Medical Professionals for More than 25 Years JEROME I. SAGER Attorney At Law Former Assistant District Attorney CLASSIFIED ADVERTISING See us for: Classified ads can be accessed on MSSNY’s website at www.mssny.org. Click classifieds. • Professional Medical Conduct Defense MARCH 2015 ISSUE CLOSES FEBRuary XX $150 per ad; $200 with Photo • Medicaid and Medicare Fraud Cases PHYSICIANS’ SEARCH SERVICES • ALLIED MEDICAL PLACEMENTS • LOCUM TENENS practice valuation • practice brokerage • practice consulting • Real estate • DEA and Controlled Substance Issues for help, information or to place your ad, call 516-488-6100 x355 • Fax 516-488-2188 Physician opportunities • Third party insurance issues Seeking BE/BC OBGYN Midtown NYC female group seeks full time BE/BC OBGYN to join our growing practice. Immediate hire is available. Flexible office hours (no weekend office hours) with rotating call schedule. Excellent salary with productivity bonus with future partnership discussions available, written contract, benefits and retirement offering. Email CV to mmessite@aol.com. Practice for sale My firm can handle most legal matters. Call us for a free consultation. Internal Medicine Practice For Sale: • N/E Bronx (Near Parkchester) • Doctors office for 60 years • Current MD relocating • Turn Key Operation • EMR • Great Opportunity • Long Lease Call Dr. S. for further inquiries (917) 834-7183 212-685-2333 • 917-312-6631 jeromesager@cs.com Place Your Classified Ad In News Of New York! Leasing or Selling Space? Selling your practice or equipment? All Ads $150; $200 with Photo • Call 516-488-6100, ext 355 CDC’s Ten Most Challenging Public Health Threats of 2014 faculty from 2004-05, at which point he returned to RPCI as Chief of Perioperative Medicine and Director of the Center for Preoperative Evaluation After earning his undergraduate degree in psychobiology from the State University of New York at Binghamton, Dr. Filadora went on to earn his medical degree, a master’s degree in natural science/biochemistry and an MBA from University of Buffalo. In addition to MSSNY, he is a member of the American Medical Association, American Society of Anesthesiologists, Massachusetts Medical Society and New York State Society of Anesthesiologists. Untitled-1 1 business showcase 11/13/14 3:59 PM The CDC has released its list of the 10 most challenging public health threats of 2014: 1. Ebola 2. Antibiotic resistance 3. Enterovirus D-68 4. Middle Eastern Respiratory Syndrome coronavirus (MERS-CoV) 5. HIV/AIDS 6. Polio (with this caveat: “The world is on the brink of eradicating polio, but we risk losing valuable ground.”) 7. Laboratory safety 8. Cardiovascular disease 9. Cigarette smoking 10. Prescription drug overdose February 2014 • MSSNY’s News of New York • Page 11 PRESIDENT’S COLUMN (Continued from page 4) even narrower networks and even greater limitations on the care that physicians can provide to their patients. Non-physician groups like dentists, nurse anesthetists, optomoetrists, podiatrists and psychologists argue that their training enables them to provide patient services currently only provided by physicians. And health insurers and large health systems want to profoundly change how payments for care will be made without your input. Doctors Need to Be Seen and Heard That’s why they need to see you, in your white coat, on their “home turf.” I know many physicians wish this was not the case, but the delivery of care is inexorably linked to public policy. So we have an obligation – to ourselves, to our colleagues, and to our patients – to make sure that these policies further enable our patients’ ability to receive quality care from appropriately trained physicians, instead of hindering our patients’ ability to receive this care. I look forward to seeing you all in Albany on March 4. And make sure you urge your colleagues to come to Albany as well. Our future depends on it. Competency-Based Admissions (Continued from page 9) In order to transition CBA, the Committee on Admissions in September, 2011 began a four-year process by participating in an AAMC full day Holistic Review in Admissions workshop on site in the Bronx. This workshop identified a need to clarify the Admissions Committee Mission Statement. This was revised to read as follows: “The Albert Einstein College of Medicine strives to matriculate a diverse group of outstanding students whose academic accomplishments, clinical experiences, community service and research indicate that they will become exceptional healers, educators, colleagues, patient advocates, scientists, role models and life-long learners. We are committed to identifying individuals who already have demonstrated the qualities of compassion, empathy, kindness, creativity, professionalism, leadership and maturity. A diverse student body is consistent with the history and mission of Einstein and supports a key educational objective which is to raise the cultural awareness and competence of our graduates.” [6] Four Major Competencies Subsequently, using an iterative process the Committee established four major competencies that applicants must demonstrate in order to be considered for admission. These are: 1. Co-Curricular Activities and Relevant Experiences • Clinical experiences, community service and research 2. Communication Skills • Excellent spoken and written English language skills, ability to connect interpersonally, show empathy and demonstrate cultural competence 3. Personal and Professional Development • Ethical behavior, teamwork, leadership, maturity, ability to handle stress and show resilience 4. Knowledge 1. Chemistry/Biochemistry 2. Biology 3. Physics 4. Mathematics 5. Humanities, Social and Behavioral Sciences A detailed description of these competencies is available on the Einstein website[7]. Beginning with the 2014-2015 applicant class, the Committee on Admissions is using CBA by specifically searching the entire application to ensure that the candidate has demonstrated reasonable accomplishment of all of the identified competencies. We read in detail the AMCAS application, academic record, personal comments, roster of experiences, letters of recommendation, the Einstein secondary application, and written and verbal communication with the Admissions Office. We ask students to tell us how they have achieved the knowledge competencies on our secondary application. Interpersonal interaction and communications skills are evaluated during the interview. Einstein has used this broad review of applicant characteristics for many years, and our graduates historically have met our goals of being both well-trained in medical science and highly effective in clinic practice. Implementation of CBA provides a more explicit and transparent approach to the holistic review process. We will be tracking outcomes over the next several years to assure that our selection process continues to be successful, and to determine whether this approach actually results in the training of a physician workforce best able to serve the nation’s health. REFERENCES [1] Koop, C.E., Health and Health Care for the 21st Century: For All the People. Am. J. Public Health, 2006; 96: 2090-2092 [2] Kirch DG. The Flexnerian Legacy in the 21st Century. Academic Medicine. 2010; 85:190–192. [3] Mahon KE, Henderson MK, Kirch DG. Selecting tomorrow’s physicians: the key to the future health care workforce. Academic Medicine. December 2013. Vol 88(12):1806-11. [4] Addams AN, Bletzinger RB, Sondheimer HM, White SE, Johnson LM. Roadmap to Diversity: Integrating Holistic Review Practices Into Medical School Admission Processes. Washington, DC: Association of American Medical Colleges; 2010. https://members.aamc.org/eweb/upload/ Roadmap%20to%20Diversity%20 Integrating%20Holistic%20Review.pdf. Accessed January 8, 2015. [5] United States Census Bureau. http://quickfacts.census.gov/qfd/states/36/36005. html. Accessed January 8, 2015. [6] Albert Einstein College of Medicine Website. http://www.einstein.yu.edu/education/ md-program/admissions/admissions-mission-statement/. Accessed January 8, 2015. [7] Albert Einstein College of Medicine Website. http://www.einstein.yu.edu/education/ md-program/admissions/applicationprocedure/course-requirements.aspx. Accessed January 8, 2015. Page 12 • MSSNY’s News of New York • February 2014 AMA: Top 10 of What You Need to Know About the 2015 Medicare Fee Schedule Chances are you haven’t been able to read through the nearly 1,200 pages that constitute the 2015 Medicare Physician Fee Schedule final rule released Oct. 31 and published in the Federal Register. Here are the 10 top payment policy changes discussed in this mammoth document that you need to know about: 1. The sustainable growth rate (SGR) formula calls for a 21.2 percent cut to physician payments, effective April 1. While this is a steep reduction, it is a considerable drop from the nearly 30 percent cut projected just a few years ago. The reduction is thanks to nearly flat growth in utilization of physician services over the past several years. The AMA continues to press Congress to repeal the SGR formula to eliminate the perennial payment cut threats and temporary legislative patches. 2. Continuing Medical Education (CME) will not be reported under the Physician Payments Sunshine Act. The Centers for Medicare & Medicaid Services (CMS) proposed including CME activities in reports of physicians’ financial interactions with medical device and drug manufacturers in the new “Open Payments” public database. The AMA led dozens of other medical associations in calling on the agency to eliminate this requirement because it would “chill physician participation in independent [continuing education] programs.” 3. Proposed penalties under the value-based payment modifier (VBM) will be scaled back. CMS intended to increase payment penalties under the modifier from 2 percent to 4 percent, beginning in 2017. The AMA strongly objected to this proposal, noting in a comment letter on the proposed rule that some physicians would be vulnerable to payment cuts totaling more than 11 percent as a result of the VBM and other Medicare reporting programs – a move that could mean some of Medicare’s sickest patients would lose access to their doctors. While the final rule still maintains a potential pay cut of 4 percent for larger medical groups, practices with fewer than 10 physicians will not be subject to more than a 2 percent VBM penalty. 4. The Physician Quality Reporting System (PQRS) becomes a penalty-only program next year. Physicians must successfully report in 2015 to avoid PQRS and VBM penalties in 2017. Among other things, they’ll have to report on at least nine quality measures that cover three “domains.” In addition, the final rule requires physicians to report on at least one of the 18 new “cross-cutting measures.” CMS originally said physicians would be obligated to report on at least two cross-cutting measures but cut that requirement in half after the AMA urged the agency not to create additional mandates that physicians would struggle to meet. The agency also had planned to shorten the period physicians have to review their feedback reports to just 30 days. Following AMA lobbying, CMS decided to leave the review period at 60 days. 5. The Physician Compare website will continue to expand – but not as much as planned. Continued pressure from the AMA has led CMS to commit to better prevention and correction of errors on this website that has been riddled with problems. The agency also will notify physicians when they can preview their reports. While the agency’s plans to post benchmarks to the site have been put aside for now, the website will show physicians’ performance under PQRS, the electronic health record meaningful use program and Medicare Accountable Care Organizations. 6. Chronic care management services will be supported by a monthly payment. Beginning next year, CMS will pay $42.60 per month for these services when CPT code 99490 is reported. This policy change reflects several years of advocacy by the AMA, the CPT Editorial Panel and the AMA/Specialty Society Relative Value Scale Update Committee (RUC). The groups will continue to urge the agency to also adopt higher values and pay for multiple complex chronic care coordination services so that patients have ongoing access to this important care. 7. Four services now are eligible for telehealth payment. These services are Medicare’s annual wellness visit (coded with HCPCS G0438 and G0439), prolonged evaluation and management services (reported with CPT codes 99354 and 99355), family psychotherapy (CPT codes 90846 and 90847) and psychoanalysis (CPT code 90845). 8. Surgical global periods will change from 10-day and 90-day periods to 0-day periods. Despite strong opposition from the AMA and many medical specialty societies, CMS will be transitioning all services with a 10-day global period to a 0-day global period by 2017. All 90-day global periods will be shifted to 0-day global periods by 2018. 9. There are 350 CPT codes identified as new, revised or potentially misvalued—318 of these changes were based on physician input. These changes represent 86 percent of those recommended by the RUC, a group of more than 300 participants that includes physician advisers from every medical specialty and a dozen other health care professionals. The group provides input on values based on their highly technical expertise. 10. The timeline for submitting new codes and revaluations of services will shift. The deadline for receiving all code and value recommendations for the following year’s payment policies will be February to allow more time for public comment. This change will take place for the 2017 Medicare Physician Fee Schedule. CPT and RUC timelines will be modified to accommodate the new process, thereby ensuring physicians continue to have strong input on appropriate values for services. Physicians prefer facts to speculation. These are the facts. • The actions of New York State Government deeply affect the professional practice of every single New York physician and the thousands of patients to whom they provide care. • You can substantially influence whether this effect is positive or negative through engaging in collective political action with your colleagues by joining MSSNYPAC – the physician’s political action committee. Every physician in New York State CAN AND SHOULD JOIN MSSNYPAC. Join online or find out more by visiting www.mssnypac.org.









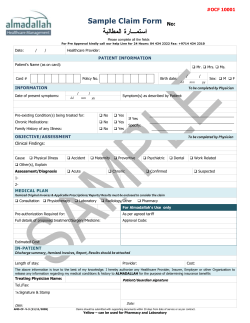
© Copyright 2025