
Kirsty Le Doaré, Ruth Bland and Marie-Louise Newell DOI: 10.1542/peds.2012-0405 Pediatrics
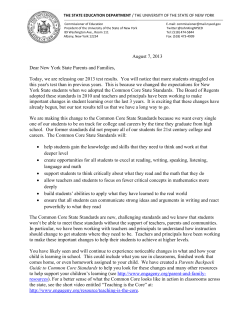
Neurodevelopment in Children Born to HIV-Infected Mothers by Infection and Treatment Status Kirsty Le Doaré, Ruth Bland and Marie-Louise Newell Pediatrics; originally published online October 1, 2012; DOI: 10.1542/peds.2012-0405 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://pediatrics.aappublications.org/content/early/2012/09/26/peds.2012-0405 PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 REVIEW ARTICLE Neurodevelopment in Children Born to HIV-Infected Mothers by Infection and Treatment Status AUTHORS: Kirsty Le Doaré, BA(Hons), MBBS, MRCPCH,a,b Ruth Bland, BSc, MB ChB, DCH, FRPCH, MD,c,d and MarieLouise Newell, MB, MSc, PhDc,e aCentre for International Health and Development, and eMRC Centre of Epidemiology for Child Health, University College London, Institute of Child Health, London, United Kingdom; bCroydon University Hospital, London, United Kingdom; cAfrica Centre for Health and Population Studies, University of KwaZuluNatal, Mtubatuba, South Africa; and dGlasgow University Medical Faculty, Glasgow, United Kingdom KEY WORDS neurodevelopment, HIV, childhood development, antiretroviral therapy, HAART ABBREVIATIONS ARV—antiretroviral drug HAART—highly active antiretroviral therapy Dr Le Doaré prepared and undertook the literature review and was responsible for writing the first draft of this article. Professor Newell and Dr Bland reviewed the data and provided comments during writing, and substantially contributed to, and approved, the final manuscript. www.pediatrics.org/cgi/doi/10.1542/peds.2012-0405 doi:10.1542/peds.2012-0405 Accepted for publication Jun 26, 2012 Address correspondence to: Kirsty Le Doaré, MBBS, MRCPCH, c/o Paediatric Department, Croydon University Hospital, London Road, Croydon CR7 7YE, UK. E-mail: kirstyledoare@gmail.com PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2012 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: The Africa Centre for Health and Population Studies is funded by a core grant from the Wellcome Trust (grant number 082384/Z/07/Z). abstract BACKGROUND: We reviewed the impact of HIV, HIV exposure, and antiretroviral therapy/prophylaxis on neurodevelopmental outcomes of HIV-infected and HIV-exposed-uninfected infants and children. METHODS: A literature search of Medline, Embase, PsychINFO, Web of Science, PubMed, and conference Web sites (1990–March 2011) using the search terms, infant, child, HIV, neurodevelopment, cognition, language, and antiretroviral therapy, identified 31 studies of HIV/ antiretroviral exposure using standardized tools to evaluate infant/ child development as the main outcome. Articles were included if results were reported in children ,16 years of age who were exposed to HIV and antiretrovirals in fetal/early life, and excluded if children did not acquire HIV from their mothers or were not exposed to antiretrovirals in fetal/early life. RESULTS: Infants who acquired HIV during fetal and early life tended to display poorer mean developmental scores than HIV-unexposed children. Mean motor and cognitive scores were consistently 1 to 2 SDs below the population mean. Mean scores improved if the infant received treatment before 12 weeks and/or a more complex antiretroviral regimen. Older HIV-infected children treated with highly active antiretroviral therapy demonstrated near normal global mean neurocognitive scores; subtle differences in language, memory, and behavior remained. HIV-exposed-uninfected children treated with antiretrovirals demonstrated subtle speech and language delay, although not universally. CONCLUSIONS: In comparison with resource-rich settings, HIV-infected and HIV-exposed-uninfected infants/children in resource-poor settings demonstrated greater neurodevelopmental delay compared with HIVunexposed infants. The effects on neurodevelopment in older HIVinfected children commenced on antiretroviral therapy from an early age and HIV-exposed-uninfected children particularly in resource-poor settings remain unclear. Pediatrics 2012;130:1–19 PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 1 Mother-to-child transmission during pregnancy, delivery, or breastfeeding is the dominant mode of acquisition of HIV infection in children.1 Without prophylaxis, ∼15% to 30% of babies born to HIV-infected women will acquire HIV in utero or during delivery and a further 5% to 20% through breastfeeding.2–4 Maternal HIV has been associated with an increased risk of low birth weight (,2500 g)5–7 and small-for-gestationalage infants,6,8,9 both of which are independently associated with an increased risk of mortality and of developmental delay.10–12 HIV-1 is thought to enter the central nervous system days to weeks after primary infection,13–15 causing neuronal damage and cell death.16,17 This infective process manifests in childhood as a progressive encephalopathy, and previously affected 8% to 50% of children diagnosed with HIV infection in the United States and Europe.18–21 Symptoms can vary greatly, with motor manifestations predominating.19,22 Microcephaly can be seen as a result of brain atrophy22,23 and radiologic studies demonstrate periventricular and basal ganglia calcifications and cerebral matter attenuation.24,25 Studies of cerebrospinal fluid from children with progressive encephalopathy found active and persistent brain infection, highlighting the need for antiretroviral drugs (ARVs) that cross the blood-brain barrier. This information has recently been developed into a ranking system to aid clinicians’ ARV prescribing.26 Highly active antiretroviral therapy (HAART), containing ARVs that cross the blood-brain barrier, has been found to reduce the incidence of progressive encephalopathy by 50% compared with non-HAART regimens.27 With the routine use of ARVs in childhood in the United States and Europe, cumulative incidence of progressive encephalopathy in HIVinfected children aged 6 months to 16 2 years has fallen from more than 30% to less than 2%.28–30 Prevention of mother-to-child transmission through maternal ARV prophylaxis and treatment has successfully reduced transmission rates since the 1990s,31,32 and in countries offering a combination of ARV prophylaxis, elective cesarean delivery, and avoidance of breastfeeding, transmission rates of ,2% have been reported.33 HAART has been associated with severe prematurity (twofold increased risk of being born at ,32 weeks’ gestation)34,35 in Europe and the United States. Similar reports from Africa, where most women with HIV infection live, indicated that women on a HAART regimen containing a protease inhibitor were twice as likely to deliver prematurely (before 37 weeks) than those on a regimen not containing a protease inhibitor,36,37 and were 50% more likely to deliver extremely premature infants (before 28 weeks).37 An increased risk has also been reported in regimen containing efavirenz and nevirapine.38,39 Severe prematurity increases the risk of cerebral events, such as hypoxic brain injury and cerebral hemorrhage, which will affect future neurodevelopmental potential.11,12 Interventions to improve development in the first 3 years of life, including nutritional supplementation, developmental stimulation, dedicated health and community-based development centers, have demonstrated sustained improvement in later cognition and schooling in developing countries40,41 but this has not been specifically investigated in children affected by HIV. Assessing neurodevelopmental outcomes is a difficult task owing to potential confounders, such as maternal health, mood, infant-mother bonding and attachment, early years stimulation, maternal substance misuse, poverty, illiteracy, malnutrition, and disease.41 The past 10 years have seen a large investment in prevention of mother-to-child transmission programs and the treatment of HIVinfected children at an earlier disease stage with more aggressive therapy.42 With earlier detection and improved treatment, HIV has become a chronic disease rather than a fatal illness. Therefore, improving the quality of life for infants and children affected by HIV, including interventions to improve neurodevelopmental outcomes and maximize school achievement are vital. This review aims to summarize what has been learned about neurodevelopmental outcomes in HIV-infected and HIV-exposed-uninfected infants and children and discusses the effects of different antiretroviral regimens on neurodevelopmental outcomes. We discuss the implications of these findings to improve the care of children infected and affected by HIV. METHODS We searched the online databases Medline, Embase, PsychINFO, Web of Science, and PubMed for studies published in English between 1990 and March 1, 2011, with the following search terms: “infant,” “child,” “HIV,” “neurodevelopment,” “cognitive impairment,” “motor impairment,” “language impairment,” “antiretroviral therapy.” The search identified 210 studies in Medline; subsequent searches identified additional studies: 16 in Embase, 7 in PsychINFO, and 12 in PubMed. The results of this review have been reported using the checklist described for writing systematic reviews by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).43 The current focus of HIV programs globally is on prevention of mother-tochild transmission and early detection of childhood infection with immediate treatment. Therefore, to determine the effect on neurodevelopment of maternal LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 REVIEW ARTICLE HIV and possible ARV exposure in utero or early life, and of childhood exposure to ARVs, studies were included if they met the following criteria: 1. The study concerned HIV-infected and HIV-exposed-uninfected infants and children ,16 years of age who were exposed to ARVs in fetal and/ or early life 2. The study used a standardized tool to evaluate infant/child development 3. A developmental variable was the main outcome 4. English language articles/abstracts Studies of special groups, such as patients with hemophilia, orphans, or HIV-infected children who had not acquired HIV infection via mother-to-child transmission, were excluded, as these groups would either not have been exposed to HIV/ARVs in utero or have other potential confounders that are known to affect development, independent of child health status.15 In addition, a manual search of the references from selected articles and recent conferences of interest (international AIDS conferences, Conference on Retroviruses and Opportunistic Infections from 2002–2010) was carried out to ensure all relevant articles were identified. This yielded an additional 8 studies that met the inclusion criteria; 31 studies fulfilled the inclusion criteria and were reviewed (Fig 1). CHARACTERISTICS OF STUDIES Three-quarters of the studies reviewed (75%) emanated from the United States or Canada (n = 18)44–61 and Europe (n = 5),62–66 whereas studies from resource-poor settings accounted for 25%: Africa (n = 6),67–72 South/Central America and the Caribbean (n = 1),73 and Asia (n = 1).74 The characteristics of the studies included in this review are outlined in Tables 1, 2, and 3. FIGURE 1 Flowchart of study selection process (based on PRISMA flowchart). The prevalence of infants born before 37 weeks’ gestation ranged from 6% to 29%50,52,55 in HIV-infected children and 2.8% to 17.3% in HIV-exposeduninfected children.48,53,54 The prevalence of low birth weight (,2500 g) among HIV-infected children ranged from 13% to 33%50,55 and 12% to 16% in HIV-exposed-uninfected children.53,54 Only 1 study commented on mean duration of ARVs in pregnancy (17.7 weeks).54 Additional exposure to maternal alcohol and drug abuse, including cocaine, cannabis, and heroine was reported in 31 studies with a prevalence of between 9% and 67%.44,45,48,50–55,57,60–61 All these studies were from the United States or Europe. HIV-INFECTED INFANTS AND CHILDREN EXPOSED TO ARVS IN RESOURCE-RICH SETTINGS HIV-Infected Infants HIV-infected infants examined using the Bayley Scales of Infant Development (I and II, Psychomotor Developmental Index, and Mental Developmental Index, mean score of 100, SD 15)75 displayed mean neurodevelopmental scores more than 1 SD below the population mean. Compared with HIV-exposeduninfected infants, HIV-infected infants PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 3 4 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 1995 1996 1999 1999 Pollack (44) Culnane (48) Raskino (49) 1994 Year Chase (46) Nozyce (45) First Author (Reference No.) US US and France US US US Location Cohort Cohort Cohort Cohort Cohort Study Type 831 332 91 51 274 n All HIV-infected HIV-exposeduninfected HIV-unexposed = 27 HIV-infected = 22 HIV-exposeduninfected = 42 HIV-infected = 24 HIV-exposeduninfected = 27 All HIV-infected Groups Studied Mean age 3.8 y 2 mo–18 y 0–3 y 0-2 y 4–70 mo 3–24 mo Age at Entry TABLE 1 Infants Exposed to HIV/ARVS In Utero and Early Life in Resource-Rich Settings BSID, MSCA, WIT BSID MSCA BSID BSID BSID Development Scale Not stated if antenatally. Infants randomized to receive zidovudine or didanosine monotherapy or combination zidovudine and didanosine therapy Not stated if antenatally. Infants received – zidovudine Not stated if antenatally. 11/18 zidovudine postnatally at mean age of 4.5 mo. Yes, not stated when. ARVS not stated. Not antenatally. On therapy depending on disease stage. ARVs not stated. Exposure to ARVs No SDs in groups for BSID or MSCA. Developmental results improved with combination zidovudine and didanosine. Yes- not stated how many Low birth weight Growth, immunologic parameters, birth weight and gestation Growth failure Mean MDI and PDI predictive of scores comparable neurocognitive at birth but declined scores. versus controls by 12 mo if HIV-infected (83.5 vs 112 vs 116, P = .01). HIV-infected 10.5 times more likely to have mean MDI score .1 SD lower and 4.4 times more likely PDI mean score ,85 (,1 SD) below population mean. Not stated Yes – not stated Not stated Additional Outcome Measures Not stated Early motor delay and mental decline if HIVinfected versus HIVexposed-uninfected. Mean scores decelerate over time. Variable outcomes, even if HIV-infected. Those with worse disease stage at higher risk of lower neurodevelopmental scores than the population mean. Yes – not stated Not stated Developmental Outcomes Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) Smith (50) Chase (47) First Author (Reference No.) 2000 2000 Year TABLE 1 Continued US US Location Cohort Cohort Study Type 114 595 n All HIV-infected HIV-infected = 114 HIV-exposeduninfected = 481 Groups Studied 0–3 y 0–36 mo Age at Entry BSID BSID Development Scale Not stated if antenatally. All infants treated with zidovudine. ARVS not stated. Yes, not stated when. Exposure to ARVs Yes 48% Yes – 38.7% to 55.8% in all mothers Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) Additional Outcome Measures Prematurity, At 4 mo no significant birth weighta difference except in mean scores. Mean score ,1 SD from the population mean by 24 mo for both MDI and PDI, P = .05. Early HIV-1 infection was associated with a decline in estimated mean motor scores of 1 standard score point per mo compared with 0.28 point in the late infected group (P , .02). Estimated mean mental scores of the early-infected group declined 0.72 point/mo, whereas the average decline of the late-infected group was 0.30 point/mo (P , .13). HIV-infected RR of .1 SD Prematurity, maternal education assoc. with below population lower mean mean for neurocognitive neurodevelopment: scores 1.5 CI (1.03–2.18) P = .034; RR .2 SDs below population mean for neurodevelopment: 2.40; 95% CI: 1.27– 4.56; P = .007. RR of PDI .1 SD below population mean: 1.66, CI (1.12-2.45) P = .011; RR .2 SDs below population mean: 3.81; 95% CI: 1.93–7.54; P = .0001. Developmental Outcomes REVIEW ARTICLE PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 5 6 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 2003 2006 Foster (64) UK US Canada Blanchette (51) 2001 Llorente (52) Location Year First Author (Reference No.) TABLE 1 Continued Cohort Cohort Crosssectional Study Type 62 157 50 n HIV-infected All HIV infected HIV-infected = 25 HIV-exposeduninfected = 25 Groups Studied 7–33 mo 0–36 mo 6–37 mo Age at Entry BSID, GMDI BSID BSID Development Scale Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) Not stated if antenatally. Category C disease: all received ARVs; 12/31 mono/dual therapy before HAART, median number of drugs =5 (range 3– 12). Category A/B disease: 23/31 HAART, 9 received mono/dual therapy before HAART. Median number of drugs = 4 (range 2–11). Not stated if antenatally. Either zidovudine monotherapy, dual therapy without protease inhibitor or HAART. Not stated 38% to 63% Not stated when. Yes – 20% in 3 had therapy including HIV-infected mothers a protease inhibitor and reverse transcriptase inhibitors. Others had combination therapy with nucleoside analogs only. Exposure to ARVs Additional Outcome Measures Lower scores if low birth weight or premature and increased risk of mortality Disease stage, Lower verbal scores worse stage = lower than population scores mean. Children with worse disease stage have scores .2 SDs below the population mean, not improved by HAART. Children with worse disease had scores .2 SDs below the population mean. Increased risk of mortality per 10point decrement in initial MDI and PDI scores versus population mean, even after adjusted for treatment. 1.32 (CI 1.07–1.63). Mean MDI lower in HIV- CT abnormalities – scores worse in HIVinfected group (P , infected if also had .001 [71.4 CI 62.4– CT abnormalities. 80.4]) versus 92.3 [CI 84.5–99.9]). Mean PDI lower in HIV-infected group (61.9 [CI 55.3– 68.6] vs 90.9 [CI 80.1– 98.1] P , .001); HIVexposed-uninfected normal scores in all domains. Developmental Outcomes PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 2008 2010 Caplo (63) Williams (53) US Italy US US Location Cohort Crosssectional Cohort Crosssectional Study Type HIV-exposeduninfected = 39 HIV-unexposed = 24 Groups Studied HIV-infected = 15 HIV-exposeduninfected = 14 1840 All HIV-exposeduninfected 29 1211 HIV-infected = 152 HIV-exposeduninfected = 1059 63 n 0–2 y 2 wk–36 mo 0–2 y 18–36 mo Age at Entry BSID DDST BSID BSID Development Scale Excluded Yes -17% Yes – 1694 exposed to any ARVS antenatally. 11% to 25% Prematurity, low birth weight Additional Outcome Measures Not stated MDI 94.8 vs 92.2, PDI 93.9 Infants with low = near normal. birth weight had Improved MDI scores better scores if ARV with increased exposed. duration of maternal therapy (92 for 0 wk versus 95.9 for .26 wk exposure). MDI scores also improved with maternal zidovudine and lamivudine therapy in second and third trimesters. HIV-infected infants 62.5% abnormal scores vs 14% if HIVexposed-uninfected. Treatment before 12 wk of age improved scores versus those treated later. Low birth weight, In pre-protease gestational age inhibitor era, HIVinfected lower MDI and PDI versus HIVexposed-uninfected by 1 y of age and remained lower at age 2 y. Limited improvement in MDI and PDI with addition of PI-based HAART. Percentage MDI scores .1 SD below the population mean 54% vs 25% P = .025; not significant when adjusted for maternal substance misuse. Yes – 51% HIV-exposeduninfected versus 12% HIVunexposed Developmental Outcomes Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) Yes, not stated when. ARVS not stated. 79% antenatally. Infants on HAART 6 protease inhibitor All HAART exposed: at least 3 ARVs for at least 1 wk during pregnancy and zidovudine at delivery and postnatal period (mean 17.7 wk of exposure). Exposure to ARVs BSID, Bayley Scales of Infant Development; CI, confidence interval; MDI, Mental Developmental Index; MSCA, McCarthy Scale of Childhood Abilities; PDI, Psychomotor Developmental Index; PI, protease inhibitor; RR, relative risk; WIT, Wechsler Intelligence Tests. a Children followed until 5 y of age. 2007 2006 Alimenti (54) Lindsey (55) Year First Author (Reference No.) TABLE 1 Continued REVIEW ARTICLE 7 8 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 2000 2000 2001 Fishkin (57) Blanchette (61) 1992 Year Bisiacchi (62) Levenson (56) First Author (Reference No.) Canada US Italy US Location 80 42 49 n Cross- sectional 25 Cross-sectional Cross-sectional Cross-sectional Study Type Groups Studied HIV-infected = 14 HIV-exposeduninfected = 11 HIV-infected = 40 HIV-unexposed = 40 HIV-infected = 29 HIV-exposeduninfected = 13 HIV-infected = 41 HIV-exposeduninfected = 8 TABLE 2 Children Exposed to ARVS in Resource-Rich Settings 5–12 y Mean 9.4 y 3–5 y 6–15 y School-age Age at Entry WIT WIT Own tests MSCA Development Scale Developmental Outcomes Additional Outcome Measures Not stated Not stated Executive function scores lower in HIV-infected than HIV-exposeduninfected; language and memory scores only poorer with worse disease. HIV-exposed scores normal for age. Yes, not stated how All neurocognitive many scores lower in HIV-infected group but not significant, only significant difference executive function: block design 6.08 vs 7.53 P = .002 Not stated Yes, not stated how 44% scored .2 SDs Not stated many below the population mean. Poor verbal and memory scores if HIV-infected and symptomatic. Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) CT changes Not stated when. Yes – 20% in HIVNo differences in 4 children on ARVs + associated with infected mothers cognition. Subtle PI; 8 children visuospatial and fine and gross ARVs without PI; visuomotor motor strength Average no. of difficulties. differences. drugs = 2 (range Significant 0–4) differences in mean scores in HIV-infected with worse disease stage. Not stated when. ARVs not stated Not stated when. ARVs not stated Not stated when. ARVS not stated Exposure to ARVs Smith (60) Jeremy (59) First Author (Reference No.) TABLE 2 Continued 2006 2005 Year US US Location Cohort Cohort Study Type Groups Studied HIV-exposeduninfected = 422 539 HIV-infected = 117 489 All HIV-infected n 3–7 y Mean age 6.8 y 24 mo– 17 y Age at Entry MSCA WIT BSID Development Scale Postnatally owing to infection, not stated if antenatally. Pre-1997: zidovudine/ lamivudine (100), stavudine /ritonavir (97), zidovudine/ lamivudine/ ritonavir (100). Post-1997: stavudine/ nevirapine/ ritonavir (41), stavudine/ lamivudine/ nelfinavir (63), stavudine/ nevirapine/ nelfinavir (44), or the 4-drug (44) Not stated if antenatally. Children treated with: 35% monotherapy, 17% HAART, 10% other multidrug therapy but not HAART. Exposure to ARVs Only children with Lower mean scores associated with the class C viral load, disease primary performed language and poorly. All other maternal scores education. comparable with norms. Yes – 41% Additional Outcome Measures Motor, memory, and Low birth weight, prematurity language scores .1 SD below the population mean at baseline. Small improvement in verbal score only with introduction of PI-based ARVs, no difference between the PIcontaining regimen. Developmental Outcomes Yes, not stated Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) REVIEW ARTICLE PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 9 10 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 Location Study Type 2010 Thomaidis (66) Greece US Cross-sectional Cross-sectional All HIV-infected Groups Studied 60 HIV-infected = 20 HIV-unexposed = 40 HIV-exposeduninfected = 134 325 HIV-infected = 206 22 n 3–18 y Mean age 11.76 y 9–16 y 9.46 y Median 6–17 y Age at Entry WIT GMDI PPVT;WRAT III SON Development Scale All HIV-infected treated with HAART not stated when treatment started. Not stated if antenatal Not stated if antenatal exposure. 84% of youths on ARVS not stated which. 18 postnatally treated with HAART. Not stated antenatally Exposure to ARVs Additional Outcome Measures 33% HIV-infected Youths on ARVS had scored below lower WRAT III 10th centile in scores than those both tests. not taking PPVT:HIV-infected medication mean score 83.9 vs 85.3; HIV-exposeduninfected: mean score 87.5 HIV-infected with CT Prematurity and low birth weight changes had lower mean general, practical and IQ scores P , .001. HIV-infected without CT abnormalities had normal cognitive scores but increased emotional symptoms and hyperactivity P , .05. Not stated Global scores within Higher CD4% at initiation of the average range. therapy and Differences in prolonged executive function therapy noted with mean associated with scores .1 SD better mean below the scores in pattern population mean recognition and in: verbal scores, baseline speed. baseline speed, pattern recognition, shifting set, visuospatial memory all P , .001. Developmental Outcomes Not stated Not stated Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) BSID, Bayley Scales of Infant Development; CI, confidence interval; CT, computed tomography; GMDI, Griffiths Mental Developmental Index; MDI, Mental Developmental Index; MSCA, McCarthy Scale of Childhood Abilities; PI, protease inhibitor; PPVT, Peabody Picture Vocabulary Test; SON, Snijers-Oomen Non-verbal WIT; Wechsler Intelligence Tests; WRAT, Wide-Ranging Ability Test. 2009 2008 Netherlands Cohort Year Brackis-Cott (58) Koekkoek (65) First Author (Reference No.) TABLE 2 Continued 2008 2008 2008 Van Rie (72) Leartvanangkui (74) 1995 Year Smith (71) Gay (73) Author PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 Thailand 2008 2008 Congo South Africa Haiti Location Groups Studied 39 HIV-infected 126 HIV-infected = 28 HIV-exposeduninfected = 98 n Cross304 HIV-infected = 25 sectional HIV-exposeduninfected = 279 HIV-exposeduninfected = 35 HIV-unexposed=90 Cross160 HIV-infected = 35 sectional Cohort Cohort Study Type 0–5 y Mean age 43.7 mo 18–72 mo Mean age 60 mo 0–24 mo Age at Entry TABLE 3 Infants and Children Exposed to HIV/ARVS in Resource-Poor Settings DDST BSID, PPVT, SON GMDI BSID Development Scale Yes, not stated when but part of PMTCT program Yes, not stated when, recruited from HIV treatment and care program so most ,1 mo of HAART at recruitment. Yes – all started HAART at enrollment. Stavudine, lamivudine and ritonavir or efavirenz. Not in utero, 13 infants treated with zidovudine, mean age at initiation 14.6 mo Exposure to ARVs Additional Outcome Measures Gross motor and language delay Stunting and in HIV-infected children, fine wasting motor and language delay in prevalent in the HIV-exposed-uninfected. HIV-infected group Motor and cognitive lower in HIV- Stunting and wasting higher in infected and HIV-exposedthe HIV-infected uninfected children (60% group. cognitive delay in HIV-infected versus 40% in HIV-exposeduninfected; 28.6% motor delay HIV-infected versus 14.3% HIVexposed-uninfected. Delay in language expression 84.6%, comprehension 76.7% P , .01. HIV-infected children aged 18–29 mo performed worse, 91% mental, 82% motor delay, versus 46% and 4% in HIV-infected children aged 30–72 mo. Children presenting before clinically eligible for HAART had better cognitive/ motor scores than those presenting with requirement for HAART. No No Mean cognitive scores were less Weight-for-height than the norm at baseline and at 6 mo despite 6 mo of HAART NB: 86% Xhosa first language (mean scores 67–78 pre-and post-HAART commencement); 33% to 81% subnormal intelligence quotients, 33% abnormal motor function. Mean MDI and PDI scores .1 SD Not stated below the population mean if HIV-infected at 3 mo. Differences between groups increased over time. 33% normal cognitive scores, 50% normal motor scores. Developmental Outcomes No No Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) REVIEW ARTICLE 11 12 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 2011 Zimbabwe 2010 Kandawasvika (68) n HIV-exposeduninfected = 35 HIV-infected = 51 Groups Studied Cohort Cohort 593 HIV-infected = 16 HIV-exposeduninfected = 577 122 All HIV-infected Cross115 HIV-infected = 92 sectional HIV-exposeduninfected = 28 HIV-unexposed = 34 Cross86 sectional Study Type GMDI BSID BINS ,2.5 y, mean age 18.5 mo ,12 mo BSID Development Scale 10–15 mo 1–33 mo Age at Entry Yes- single dose nevirapine in labor, not stated if postnatally. Not stated if antenatally. 18 children receiving HAART Yes, not stated when 66.6% of children on ARVs at recruitment 39.2% antenatally. Exposure to ARVs No No No No Additional In Utero Exposure to Drugs (Cocaine, Heroin, Other) NB: Study in Xhosa through interpreter Not stated Additional Outcome Measures HIV-infected most at risk if discovered HIV-infected before 3 mo of age Children on ARVs had lower developmental scores than the population mean. Head circumference and low birth weight associated with low BINS scores Stunting and wasting common and associated with poorer developmental scores. Motor scores lower in HIVGeneral quotient infected if treatment deferred higher if treated until clinically necessary, with ARVs versus those on treatment from diagnosis. Scores reported as a percentages: 66.6% HIV-infected had motor delay versus 5.7% for controls. Children exposed to ARVs in utero had fewer scores .2 SDs below the population mean than those unexposed to ARVs in utero. Developmental Outcomes BINS, Bayley Infant Developmental Screener; BSID, Bayley Scales of Infant Development; DDST, Denver Developmental Screening Tool; GMDI, Griffiths Mental Developmental Index; MDI, Mental Developmental Index; PDI, Psychomotor Developmental Index; PI, protease inhibitor; PPVT, Peabody Picture Vocabulary Test; SON, Snijers-Oomen Non-verbal. 2009 South Africa 2001 Potterton (70) South Africa 2008 Location 2009 South Africa 2009 2009 Year Laughton (69) Ferguson (67) Author TABLE 3 Continued REVIEW ARTICLE demonstrated a greater proportion of floor scores (scores 3 SD below the population mean or less; ie, scores of ,49). Studies that investigated the effects of other variables known to affect neurodevelopment independent of HIV status reported that prematurity,47,52 low birth weight,52,55 low weight-for-height scores,44 and low maternal education46,51 were all associated with poorer mean neurodevelopmental scores in HIV-infected infants by the age of 12 months compared with the population mean. In general, even when adjusting for these variables, HIV-infected infants demonstrated mean scores .1 SD below the population mean by the age of 12 months. Those infants with worse disease stage and higher viral loads appeared to be at greatest risk of neurodevelopmental delay with mean scores .2 SD from the population mean, indicating moderate to severe neurodevelopmental impairment.45,51,64 The prevalence of HIV-infected infants’ exposure to ARVs in utero ranged from 39.2% to 96.6%.50,55 In HIV-infected and HIV-exposed-uninfected infants exposed to ARVs in utero, mean mental scores ranged from 85 to 96 and mean motor scores from 75.0 to 96.5.50,55 Lindsey et al55 noted that infants born to mothers treated with ARVs in pregnancy had improved motor scores compared with those born to mothers with no ARVs in pregnancy. They also noted that in the pre-protease inhibitor era, mean mental and motor scores in HIV-infected infants ,1 year of age were significantly lower than those among HIVexposed-uninfected infants and remained lower up to 2 years of age and that these mean scores remained significantly lower than those of HIVexposed-uninfected infants even after the introduction of a protease inhibitor. Mean scores declined for both HIVexposed-uninfected infants and HIVinfected infants over time; however, despite this, there was evidence of limited improvement in the HIV-infected infants’ overall mean scores after a protease inhibitor–based treatment had been instigated.55 Despite the widespread use of ARVs in pregnancy, infants with early infection (positive result within 48 hours of life, presumed in utero infection) had lower mean mental and motor scores compared with children diagnosed as infected after 48 hours (presumed peripartum infection),50 and by 24 months, early HIV-infected infants performed significantly less well in both mental and motor mean scores than those infants with later infection.50 There are several limitations to conclusions that can be drawn from this study, namely that it was conducted at a time when maternal HAART in pregnancy was not available and initiation of infants on early treatment was not indicated. Evidence is emerging that infants initiated before the age of 12 weeks have improved locomotor scores compared with those initiated later.62 With the recently changed guidelines recommending early diagnosis and initiation of antiretroviral therapy in infants,42 the impact on the long-term development of these children remains to be documented. LONG-SURVIVING HIV-INFECTED CHILDREN TREATED WITH ARVS IN RESOURCE-RICH SETTINGS Early studies of ARV-naive HIV-infected children .30 months of age at study enrollment demonstrated slower disease progression and better clinical outcomes than infants who seemed to have a more rapidly progressive disease and died early.20,76 These studies did not collect data on maternal ARV treatment in pregnancy and describe characteristics of children who had never been treated with ARVs. In the earliest studies of children aged 3 to 18 years treated with dual therapy, mean global cognitive scores using the Wechsler Intelligence Tests (mean score 100, SD 15)77 and McCarthy Scales of Childhood Abilities (mean 100, SD 15)78 vary from within the normal range57,61,62 to the neurocognitive impairment range (.2 SDs below the population mean).49,56 A proportion of children with severe disease56,57,62 and high viral loads56,61,62 and those who demonstrated changes, such as cerebral atrophy on computed tomography scan,49,61 displayed mean neurocognitive scores ,70, indicating moderate-severe neurocognitive impairment. Differences between scores before and after treatment instigation are reported by Raskino et al,49 who found that the mean score improved by 11 to 13 points after 24 weeks of treatment with combination zidovudine and didanosine therapy but remained in the range of neurocognitive impairment. Most early studies of older children treated with any ARV indicated normal global cognitive scores, although all highlighted subtle significant differences in executive function, memory, and verbal skills. It is important to note that there was a large attrition rate because of disease progression, as most of these studies include children treated at a time when children were commenced on ARVs only in advanced disease, with low numbers of children followed for prolonged periods, making generalizability of the results to today’s situation when ARVs are commenced early in infants and at an earlier stage in children problematic. Recent studies of children treated with a HAART regimen containing a protease inhibitor all indicated normal global cognition mean scores.59,60,65,66 As with earlier studies, subtle significant differences were noted in executive function,59,65 verbal skills,58,59,65 behavior,66 and memory.59,65 This is not universal, however, and a large study by PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 13 Smith et al60 reported no significant differences in cognitive scores between groups unless the child had symptomatic disease. In a small case-control study from the Netherlands (2008), Koekkoek et al65 reported higher, but still below average, global neurocognitive scores among those children with higher CD4 percentage on initiation of HAART and longer duration of HAART compared with children with lower CD4 percentage and shorter duration of treatment. Language skills were the most widely reported deficit in children older than 3 years. Mean scores from 1 to 2 SD below the population mean were reported in overall language ability,56,58 word recognition,58 receptive vocabulary,61 expressive language,58 and verbal fluency.65 Although language skills continued to develop, this appeared to be at a slower rate than in HIV-exposeduninfected children, even taking into account the effect of home circumstances and caregiver arrangements and irrespective of treatment.58 Jeremy et al59 reported no improvement in overall neurocognitive score after commencement with protease inhibitor-based HAART, but noted improvement in verbal scores compared with pretreatment assessment. It is of note that a large proportion of children were tested in a language other than their mother tongue (range 9% to 75%).58,59,65 The effects of being assessed in a second language or via an interpreter on language scores have been reported in only 1 study.60 HIV-EXPOSED-UNINFECTED CHILDREN IN RESOURCE-RICH SETTINGS Few studies have evaluated the effects of perinatal exposure to HIVand ARVs on the neurodevelopment of children who are HIV-exposed-uninfected. Interpretation of these results was difficult because of the heterogeneity of the 14 study populations in terms of sample size (range 44–1694 subjects), sociodemographics, and percentage of maternal substance misuse, together with a lack of clarity surrounding length of maternal antiretroviral therapy in pregnancy. Most studies do not consider results compared with a matched control group, but rather use normative data from the standardization of the neurodevelopmental instrument as a comparison. The scales used are not normed to socioeconomically disadvantaged groups; hence, it is difficult to interpret whether the results reported are a result of social disadvantage, HIV exposure, or ARV exposure. Studies in early infancy and up to the age of 2 years have not demonstrated any global developmental delay in HIVexposed-uninfected children once variables such as maternal substance misuse were allowed for.44,46–48,50,53–55,60,61 However, it appears that subtle deficits in cognition, motor function, expressive and receptive language, and behavior may be present in older children manifesting during the preschool years (ages 3–5 years).58 DEVELOPMENTAL OUTCOMES IN HIV-INFECTED CHILDREN IN RESOURCE-POOR SETTINGS The association between HIV infection and neurodevelopmental impairment in infants and children in resource-poor settings is not well described. In contrast to resource-rich settings, where prevention of mother-to-child- transmission programs are widespread and infants are predominantly formula fed, children in resource-poor settings are, until very recently, less likely to have been exposed to ARVs in utero and early life and are still predominantly breastfed. In ARV-naive children, neurodevelopmental deficits were reported in 6% to 40% of HIV-infected children in resource-poor settings, depending on disease stage.79,80 A direct comparison of studies of children exposed to HIV/ARVs in utero and early life was limited by the use of different methodological designs and the variety of developmental screening and diagnostic tools used: Denver Developmental Scale Test (percentage fail scores)81; Cognitive Adaptive Test, Clinical Linguistics and Auditory Milestones (percentage fail scores)82; Bayley Scales of Infant Development; McCarthy Scales of Childhood Abilities; and Griffiths Mental Development Scale83 (all mean 100 SD 15). In addition, comparisons were hampered by adaptations of these tools, including nonvalidated translation into local language and substitution of items with culturally appropriate alternatives.67,71 As in resource-rich settings, most studies report results compared with normative data from the standardization of the instrument rather than a matched control group. Further, the effect of ARVs on neurodevelopment is only just emerging, and several studies had only abstracts available, meaning an in-depth analysis of factors that may contribute to neurodevelopmental scores could not be fully assessed. In comparison with resource-rich settings, a greater proportion of HIV-infected infants in resource-poor settings had scores ,2 SD below the mean (16% to 85% in Africa),70,72 even when adjusting for birth weight and gestational age.73 Infants demonstrating the most severe neurodevelopmental delay were those diagnosed as HIV-infected before the age of 3 months,68,72 those with the most advanced disease,69,70 those children who were eligible for HAART at the time of presentation,67,69,70 and those children with the lowest weight-for-height scores.70,71 Only one study reported the effect of prevention of mother-to-child transmission programs on neurodevelopmental outcomes. Kandawasvika et al68 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 REVIEW ARTICLE indicated that maternal treatment with single-dose nevirapine in labor did not influence neurodevelopmental outcomes (adjusted odds ration of high risk of neurodevelopmental impairment with single-dose prophylactic nevirapine 0.9; 95% confidence interval 0.99–1.0). The authors report that background risk of neurodevelopmental impairment was 9.4% in both HIV-infected and HIVexposed-uninfected infants, probably owing to survival bias in the HIV-exposeduninfected groups, as the authors speculated that HIV-infected infants with severe disease would not have survived to the 12-month analysis.68 As in resource-rich settings, infants presenting at an earlier disease stage and those commenced on antiretroviral therapy at an earlier age demonstrated some improvement in cognitive and motor developmental scores once commenced on antiretroviral therapy as compared with than those presenting laterand with worse clinical disease at instigation of ARVs.72 There are few studies with long-term follow-up of children born to HIVinfected mothers, and such studies have been hampered by high mortality rates in HIV-infected and HIV-exposeduninfected children.70,72,74 In resourcepoor settings where new HIV treatment guidelines recommending early ARV initiation have not been implemented, older children who survive early childhood would tend to have slowly progressing disease. Young children who developed encephalopathy, and those with more advanced disease generally, would be expected to have a shorter life expectancy.84 This selective attrition was seen in some of the earlier studies in resource-poor settings. So the population samples available may be children who were less at risk for central nervous system effects of HIV disease and therefore function at a higher cognitive level. Additionally, these children would have been diagnosed as HIV-infected at a time when early treatment was not yet available, hindering extrapolation to the current situation with early initiation of antiretroviral therapy and improved survival rates.85 Despite subsequent HAART treatment, high levels of motor delay are noted (66.7% to 85%)67,70 and mean motor scores remained .2 SDs below the population mean. In common with resource-rich settings, language delay was also noted in older HIV-infected children with scores remaining below the mean despite 6 months of antiretroviral therapy.71,74 These studies were limited by their small sample sizes. Few studies in resource-poor settings reportresults forHIV-exposed-uninfected children. Contrary to studies from United States and Europe, these HIV-exposeduninfected children in Africa demonstrated cognitive impairment (40%), motor impairment (14.3%), and language expression delay compared with HIVunexposed infants.72,74 Evidence from Thailand indicated that HIV-exposeduninfected children assessed using the Denver Developmental Screening Test demonstrated language deficits and fine motor problems compared with their HIV-unexposed peers.74 As with studies of older HIV-infected children in this setting, conclusions were difficult owing to the small sample size and cross-sectional nature of the study. CONCLUSIONS All studies identified HIV-infected infants as having worse mean neurodevelopmental scores than the reference population in infancy with mean scores consistently more than 1 SD below the population mean, irrespective of whether they had been exposed to ARVs in utero or not. Infants presenting with HIV infection before the age of 3 months had the lowest scores. Since the advent of prevention of mother-to-child-transmission interventions, studies have indicated variable improvement in mean developmental scores in HIV-infected infants exposed to a protease inhibitor–based HAART regimen in utero. Infants commencing treatment before the age of 12 weeks demonstrated better, but still subnormal, mean locomotor scores, than those with delayed treatment. No studies have yet examined the effect of early antiretroviral therapy on cognitive scores. Older HIV-infected children demonstrated near normal global neurocognitive scores, probably as a result of slower disease progression in this group. However, there is evidence that subtle deficits in higher cognitive functioning (poorer memory, language development) and behavior exist in school-aged children with only limited improvement after initiation of antiretroviral therapy. Evidence suggests that the subtle differences detected in older children in the pre-HAARTera may be improved with more effective HAART and that language skills may be improved with a protease inhibitor–based ARV regimen. The evolution of more effective antiretroviral therapy, from single therapy to HAART, appears to have had a positive impact on mean neurodevelopmental scores in infants and children in the United States and Europe who are HIVinfected and HIV-exposed-uninfected. Lately, results appear to highlight improved outcomes for children treated with ARVs while they are still clinically well. There is also an indication that commencing HAARTat an earlier stage of disease benefits long-surviving children. This highlights the importance of the continuing effort to roll out the World Health Organization recommendations42 in resource-poor settings for early and more effective antiretroviral therapy to all eligible pregnant women and their infants. PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 15 The extent to which HIV-exposeduninfected children are affected by in utero exposure to HIV and ARVs remains unclear. This group has only recently become the focus of attention. Although preliminary studies of neurodevelopment from the United States and Europe are reassuring, these studies have yet to be replicated in Africa, where most these children live. Results of the few small studies from sub-Saharan Africa and Asia indicate that in contrast to normal developmental scores seen in populations from the United States, a larger proportion of HIV-exposed-uninfected infants and children displayed global developmental scores 1 to 2 SDs below the population mean, and children appeared to show deficits in language and behavior by the age of 5 years. There are a number of factors that should be considered when reviewing these results. First, access to ARVs in resource-poor settings in pregnancy has only recently become widespread. Although prevention of mother-to-childtransmission programs began to be established in sub-Saharan Africa from the early 2000s, UNAIDS estimated that only 9% of eligible HIV-infected pregnant women in resource-poor settings received ARVs in pregnancy in 2004, increasing to ∼33% in 2007.86 In addition, in low- and middle-income countries, 47% of eligible adults now have access to ARVs.1 So most children in studies from resource-poor settings included in this review will have been born to mothers who are unwell themselves, with higher viral loads and increased number of associated conditions, such as poor nutrition and concurrent illnesses. This will have had a direct effect on transmission of HIV and ability to care for and stimulate their infants, but also possible longer-term effects including impaired attachment between mother and child, which affects developmental potential, even if the child is HIV-exposed-uninfected. Added factors, such as poverty and early infant malnutrition and growth, also combine to give a more complicated picture of developmental challenges in this environment. tools used, lack of matched control groups, and the need for modification and translation into local languages hinders synthesis and summary of data. Robust studies that use validated neurodevelopmental assessment tools are uncommon, and a large number of studies were excluded from our review because such tools were lacking. What is needed is an internationally validated tool that is easy to adapt culturally and can be administered quickly by laytrained staff in everyday practice to screen and identify developmental delay early. Measures of cognitive, neurologic and behavioral function serve as an indirect means of assessing central nervous system function, along with the more direct measures, such as computed tomography/magnetic resonance imaging. The variety of developmental Interventions to reduce the rate of mother-to-child transmission have been successful in resource-rich settings, and the recent scale up of prevention of mother-to-child transmission programs in resource-poor settings looks set to do the same. Issues remain in unraveling the long-term effect of exposure to HIV and ARVs on HIVexposed-uninfected children and investigating speech, language, and memory deficits in older children who now have earlier access to therapies that cross the blood-brain barrier. Only a concerted, multidisciplinary approach to diagnosing and treating developmental delay, including antiretroviral therapy, physiotherapy, and early psychological/behavioral therapy will enable these children to reach their full potential. 4. Newell ML, Dunn DT, Peckham CS, Semprini AE, Pardi G. Vertical transmission of HIV-1: maternal immune status and obstetric factors. The European Collaborative Study. AIDS. 1996;10(14):1675–1681 5. Brocklehurst P, French R. The association between maternal HIV infection and perinatal outcome: a systematic review of the literature and meta-analysis. Br J Obstet Gynaecol. 1998;105(8):836–848 6. Habib NA, Daltveit AK, Bergsjø P, Shao J, Oneko O, Lie RT. Maternal HIV status and pregnancy outcomes in northeastern Tanzania: a registry-based study. BJOG. 2008;115(5):616–624 7. Rollins NC, Coovadia HM, Bland RM, et al. Pregnancy outcomes in HIV-infected and uninfected women in rural and urban South Africa. J Acquir Immune Defic Syndr. 2007;44(3):321–328 8. Bulterys M, Chao A, Munyemana S, et al. Maternal human immunodeficiency virus 1 infection and intrauterine growth: a prospective cohort study in Butare, Rwanda. Pediatr Infect Dis J. 1994;13(2):94–100 Studies have already indicated the beneficial effects of maternal antiretroviral therapy on child survival87,88 and it is probable that in addition to improving child survival, improving maternal health with HAART would benefit developmental outcomes in HIVexposed-uninfected children. REFERENCES 1. Report G. UNAIDS Report on the Global AIDS Epidemic 2010. WHO Geneva Library Cataloguing-in-Publication Data; 2010 2. De Cock KM, Fowler MG, Mercier E, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA. 2000;283(9):1175–1182 3. Wiktor SZ, Ekpini E, Nduati RW. Prevention of mother-to-child transmission of HIV-1 in Africa. AIDS. 1997;(11 suppl B): S79–87 16 LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 REVIEW ARTICLE 9. Taha TE, Dallabetta GA, Canner JK, et al. The effect of human immunodeficiency virus infection on birthweight, and infant and child mortality in urban Malawi. Int J Epidemiol. 1995;24(5):1022–1029 10. Woythaler MA, McCormick MC, Smith VC. Late preterm infants have worse 24-month neurodevelopmental outcomes than term infants. Pediatrics. 2011;127(3). Available at: www.pediatrics.org/cgi/content/full/127/3/ e622 11. Schendel DE, Stockbauer JW, Hoffman HJ, Herman AA, Berg CJ, Schramm WF. Relation between very low birth weight and developmental delay among preschool children without disabilities. Am J Epidemiol. 1997;146(9):740–749 12. Karimi M, Fallah R, Dehghanpoor A, Mirzaei M. Developmental status of 5-year-old moderate low birth weight children. Brain Dev. 2011;33(8):651–655 13. Sharer LR. Pathology of HIV-1 infection of the central nervous system. A review. J Neuropathol Exp Neurol. 1992;51(1):3–11 14. Persidsky Y, Zheng J, Miller D, Gendelman HE. Mononuclear phagocytes mediate blood-brain barrier compromise and neuronal injury during HIV-1-associated dementia. J Leukoc Biol. 2000;68(3):413– 422 15. Armstrong FD. Neurodevelopment and chronic illness: Mechanisms of disease and treatment. Ment Retard Dev Disabil Res Rev. 2006;12(3):168–173 16. Kaul M, Lipton SA. Signaling pathways to neuronal damage and apoptosis in human immunodeficiency virus type 1-associated dementia: chemokine receptors, excitotoxicity, and beyond. J Neurovirol. 2004;10 (suppl 1):97–101 17. Epstein LG, Gelbard HA. HIV-1-induced neuronal injury in the developing brain. J Leukoc Biol. 1999;65(4):453–457 18. Tardieu M. Update on the neurological consequences of HIV-1 infection (2006) [in French]. Rev Neurol (Paris). 2006;162(1): 19–21 19. Lobato MN, Caldwell MB, Ng P, Oxtoby MJ; Pediatric Spectrum of Disease Clinical Consortium. Encephalopathy in children with perinatally acquired human immunodeficiency virus infection. J Pediatr. 1995; 126(5 pt 1):710–715 20. Englund JA, Baker CJ, Raskino C, et al. Clinical and laboratory characteristics of a large cohort of symptomatic, human immunodeficiency virus-infected infants and children. AIDS Clinical Trials Group Protocol 152 Study Team. Pediatr Infect Dis J. 1996;15(11):1025–1036 21. Neurologic signs in young children with human immunodeficiency virus infection. The European Collaborative Study. Pediatr Infect Dis J. 1990;9(6):402–406 22. Ojukwu IC, Epstein LG. Neurologic manifestations of infection with HIV. Pediatr Infect Dis J. 1998;17(4):343–344 23. Newton HB. Common neurologic complications of HIV-1 infection and AIDS. Am Fam Physician. 1995;51(2):387–398 24. Johann-Liang R, Lin K, Cervia J, Stavola J, Noel G. Neuroimaging findings in children perinatally infected with the human immunodeficiency virus. Pediatr Infect Dis J. 1998;17(8):753–754 25. Lacroix C, Vazeux R, Brousse N, Blanche S, Tardieu M. A neuropathological study of 10 HIV-infected children [in French]. Rev Neurol (Paris). 1993;149(1):37–45 26. Letendre S, Marquie-Beck J, Capparelli E, et al; CHARTER Group. Validation of the CNS Penetration-Effectiveness rank for quantifying antiretroviral penetration into the central nervous system. Arch Neurol. 2008; 65(1):65–70 27. Patel K, Ming X, Williams PL, Robertson KR, Oleske JM, Seage GR III; International Maternal Pediatric Adolescent AIDS Clinical Trials 219/219C Study Team. Impact of HAART and CNS-penetrating antiretroviral regimens on HIV encephalopathy among perinatally infected children and adolescents. AIDS. 2009;23(14):1893–1901 28. Chiriboga CA, Fleishman S, Champion S, Gaye-Robinson L, Abrams EJ. Incidence and prevalence of HIV encephalopathy in children with HIV infection receiving highly active anti-retroviral therapy (HAART). J Pediatr. 2005;146(3):402–407 29. McCoig C, Castrejón MM, Castaño E, et al. Effect of combination antiretroviral therapy on cerebrospinal fluid HIV RNA, HIV resistance, and clinical manifestations of encephalopathy. J Pediatr. 2002;141(1):36– 44 30. Nachman SA, Chernoff M, Gona P, et al; PACTG 219C Team. Incidence of noninfectious conditions in perinatally HIVinfected children and adolescents in the HAART era. Arch Pediatr Adolesc Med. 2009; 163(2):164–171 31. Connor EM, Sperling RS, Gelber R, et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. N Engl J Med. 1994;331(18):1173– 1180 32. Mayaux MJ, Teglas JP, Mandelbrot L, et al. Acceptability and impact of zidovudine for prevention of mother-to-child human im- 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. munodeficiency virus-1 transmission in France. J Pediatr. 1997;131(6):857–862 European Collaborative Study. Mother-tochild transmission of HIV infection in the era of highly active antiretroviral therapy. Clin Infect Dis. 2005;40(3):458–465 Townsend C, Schulte J, Thorne C, et al; Pediatric Spectrum of HIV Disease Consortium, the European Collaborative Study and the National Study of HIV in Pregnancy and Childhood. Antiretroviral therapy and preterm delivery-a pooled analysis of data from the United States and Europe. BJOG. 2010;117(11):1399–1410 Townsend CL, Tookey PA, Newell ML, Cortina-Borja M. Antiretroviral therapy in pregnancy: balancing the risk of preterm delivery with prevention of mother-to-child HIV transmission. Antivir Ther. 2010;15(5): 775–783 Shapiro RL, Hughes MD, Ogwu A, et al. Antiretroviral regimens in pregnancy and breast-feeding in Botswana. N Engl J Med. 2010;362(24):2282–2294 Powis KM, Kitch D, Ogwu A, et al. Increased risk of preterm delivery among HIV-infected women randomized to protease versus nucleoside reverse transcriptase inhibitorbased HAART during pregnancy. J Infect Dis. 2011;204(4):506–514 van der Merwe K, Hoffman R, Black V, Chersich M, Coovadia A, Rees H. Birth outcomes in South African women receiving highly active antiretroviral therapy: a retrospective observational study. J Int AIDS Soc. 2011;14:42 Olagbuji BN, Ezeanochie MC, Ande AB, Oboro VO. Obstetric and perinatal outcome in HIV positive women receiving HAART in urban Nigeria. Arch Gynecol Obstet. 2010;281(6): 991–994 Engle PL, Black MM, Behrman JR, et al; International Child Development Steering Group. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet. 2007;369(9557):229–242 Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007;369(9555):60–70 World Health Organization. WHO Recommendations on the Diagnosis of HIV Infection in Infants and Children. WHO Library Cataloguing-in-Publication Data; Geneva, Switzerland; 2010 Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 17 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 18 the PRISMA statement. Int J Surg. 2010;8(5): 336–341 Pollack H, Kuchuk A, Cowan L, et al. Neurodevelopment, growth, and viral load in HIV-infected infants. Brain Behav Immun. 1996;10(3):298–312 Nozyce M, Hittelman J, Muenz L, Durako SJ, Fischer ML, Willoughby A. Effect of perinatally acquired human immunodeficiency virus infection on neurodevelopment in children during the first two years of life. Pediatrics. 1994;94(6 pt 1):883–891 Chase C, Vibbert M, Pelton SI, Coulter DL, Cabral H. Early neurodevelopmental growth in children with vertically transmitted human immunodeficiency virus infection. Arch Pediatr Adolesc Med. 1995;149(8):850– 855 Chase C, Ware J, Hittelman J, et al; Women and Infants Transmission Study Group. Early cognitive and motor development among infants born to women infected with human immunodeficiency virus. Pediatrics. 2000;106(2). Available at: www.pediatrics.org/cgi/content/full/ 106/2/E25 Culnane M, Fowler MG, Lee SS, et al. Lack of long-term effects of in utero exposure to zidovudine among uninfected children born to HIV-infected women. Pediatric AIDS Clinical Trials Group Protocol 219/076 Teams. JAMA. 1999;281(2):151–157 Raskino C, Pearson DA, Baker CJ, et al. Neurologic, neurocognitive, and brain growth outcomes in human immunodeficiency virus-infected children receiving different nucleoside antiretroviral regimens. Pediatric AIDS Clinical Trials Group 152 Study Team. Pediatrics. 1999;104(3). Available at: www.pediatrics.org/cgi/content/full/104/3/e32 Smith R, Malee K, Charurat M, et al; The Women and Infant Transmission Study Group. Timing of perinatal human immunodeficiency virus type 1 infection and rate of neurodevelopment. Pediatr Infect Dis J. 2000;19(9):862–871 Blanchette N, Smith ML, King S, FernandesPenney A, Read S. Cognitive development in school-age children with vertically transmitted HIV infection. Dev Neuropsychol. 2002;21(3):223–241 Llorente A, Brouwers P, Charurat M, et al; Women and Infant Transmission Study Group. Early neurodevelopmental markers predictive of mortality in infants infected with HIV-1. Dev Med Child Neurol. 2003;45 (2):76–84 Williams PL, Marino M, Malee K, Brogly S, Hughes MD, Mofenson LM; PACTG 219C Team. Neurodevelopment and in utero 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. antiretroviral exposure of HIV-exposed uninfected infants. Pediatrics. 2010;125(2). Available at: www.pediatrics.org/cgi/content/full/125/2/e250 doi:10.1542/peds.20091112 Alimenti A, Forbes JC, Oberlander TF, et al. A prospective controlled study of neurodevelopment in HIV-uninfected children exposed to combination antiretroviral drugs in pregnancy. Pediatrics. 2006;118(4). Available at: www.pediatrics.org/cgi/content/full/118/4/e1139 Lindsey JC, Malee KM, Brouwers P, Hughes MD; PACTG 219C Study Team. Neurodevelopmental functioning in HIV-infected infants and young children before and after the introduction of protease inhibitor-based highly active antiretroviral therapy. Pediatrics. 2007;119(3). Available at: www.pediatrics.org/cgi/content/full/ 119/3/e681 Levenson RL Jr, Mellins CA, Zawadzki R, Kairam R, Stein Z. Cognitive assessment of human immunodeficiency virus-exposed children. Am J Dis Child. 1992;146(12): 1479–1483 Fishkin PE, Armstrong FD, Routh DK, et al. Brief report: relationship between HIV infection and WPPSI-R performance in preschool-age children. J Pediatr Psychol. 2000;25(5):347–351 Brackis-Cott E, Kang E, Dolezal C, Abrams EJ, Mellins CA. The impact of perinatal HIV infection on older school-aged children’s and adolescents’ receptive language and word recognition skills. AIDS Patient Care STDS. 2009;23(6):415–421 Jeremy RJ, Kim S, Nozyce M, et al; Pediatric AIDS Clinical Trials Group (PACTG) 338 & 377 Study Teams. Neuropsychological functioning and viral load in stable antiretroviral therapy-experienced HIV-infected children. Pediatrics. 2005;115(2):380–387 Smith R, Malee K, Leighty R, et al; Women and Infants Transmission Study Group. Effects of perinatal HIV infection and associated risk factors on cognitive development among young children. Pediatrics. 2006;117(3):851–862 Blanchette N, Smith ML, Fernandes-Penney A, King S, Read S. Cognitive and motor development in children with vertically transmitted HIV infection. Brain Cogn. 2001; 46(1-2):50–53 Bisiacchi PS, Suppiej A, Laverda A. Neuropsychological evaluation of neurologically asymptomatic HIV-infected children. Brain Cogn. 2000;43(1-3):49–52 Caplo A, Sa CA, Rubini N, Silva E, Azevedo M, Kalil R. The importance of early neurological delay detection of vertically HIV- 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. infected children. In: AIDS 2008 - XVII International AIDS conference; August 3–8, 2008; Mexico City, Mexico. Abstract Number WEPE0227 Foster CJ, Biggs RL, Melvin D, Walters MD, Tudor-Williams G, Lyall EG. Neurodevelopmental outcomes in children with HIV infection under 3 years of age. Dev Med Child Neurol. 2006;48(8):677–682 Koekkoek S, de Sonneville LM, Wolfs TF, Licht R, Geelen SP. Neurocognitive function profile in HIV-infected school-age children. Eur J Paediatr Neurol. 2008;12(4):290–297 Thomaidis L, Bertou G, Critselis E, Spoulou V, Kafetzis DA, Theodoridou M. Cognitive and psychosocial development of HIV pediatric patients receiving highly active antiretroviral therapy: a case-control study. BMC Pediatr. 2010;10:99 Ferguson G, Jelsma J. The prevalence of motor delay among HIV infected children living in Cape Town, South Africa. Int J Rehabil Res. 2009;32(2):108–114 Kandawasvika G, Gumbo F, Kurewa E, Mapingure P. Risk factors for neurodevelopment impairment among infants born to HIV infected mothers in Harare, Zimbabwe. IAS 2011; July 17–20, 2011; Rome, Italy. Abstract No. WEPE0068 Laughton B, Grove D, Kidd M, et al. Early antiretroviral therapy is associated with improved neurodevelopmental outcome in HIV infected infants: Evidence from the CHER (Children with HIV Early Antiretroviral therapy) trial. Vancouver, Canada: IAS; 2009 Potterton J, Stewart A, Cooper P, Goldberg L, Gajdosik C, Baillieu N. Neurodevelopmental delay in children infected with HIV in Soweto, South Africa. Vulnerable Child Youth Stud. 2009;4(1):48–57 Smith L, Adams C, Eley B. Neurological and neurocognitive function of HIV-infected children commenced on antiretroviral therapy. South African Journal of Child Health. 2008;2(3):108–113 Van Rie A, Mupuala A, Dow A. Impact of the HIV/AIDS epidemic on the neurodevelopment of preschool-aged children in Kinshasa, Democratic Republic of the Congo. Pediatrics. 2008;122(1). Available at: www.pediatrics.org/cgi/content/full/122/1/ e123 Gay CL, Armstrong FD, Cohen D, et al. The effects of HIV on cognitive and motor development in children born to HIVseropositive women with no reported drug use: birth to 24 months. Pediatrics. 1995;96(6):1078–1082 Leartvanangkui C, Voramongkoi N, Jungpanich P, Chunhakuntarose P, Pattarakulvanich S. Growth and development of LE DOARÉ et al Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 REVIEW ARTICLE 75. 76. 77. 78. 79. children born to HIV-positive pregnant women in 4 provinces in Thailand, 2072008. In: 5th IAS Conference on HIV Pathogenesis and Treatment; July 2009; Vancouver, Canada. Abstract number CDC025 Bayley N. Bayley Scales of Infant Development. San Antonio, TX: Psychological Corporation; 1993 Blanche S, Tardieu M, Duliege A, et al. Longitudinal study of 94 symptomatic infants with perinatally acquired human immunodeficiency virus infection. Evidence for a bimodal expression of clinical and biological symptoms. Am J Dis Child. 1990; 144(11):1210–1215 Wechsler D. Wechsler Intelligence Scale for Children-Revised. New York, NY: Psychological Corporation; 1974 McCarthy D. McCarthy Scales of Children’s Abilities. San Antonio, TX: Psychological Corporation; 1972 Boivin MJ, Green SD, Davies AG, Giordani B, Mokili JK, Cutting WA. A preliminary evaluation of the cognitive and motor effects of 80. 81. 82. 83. 84. pediatric HIV infection in Zairian children. Health Psychol. 1995;14(1):13–21 Msellati P, Lepage P, Hitimana DG, Van Goethem C, Van de Perre P, Dabis F. Neurodevelopmental testing of children born to human immunodeficiency virus type 1 seropositive and seronegative mothers: a prospective cohort study in Kigali, Rwanda. Pediatrics. 1993;92(6):843–848 Frankenburg WK, Dodds JB. The Denver Developmental Screening Test. Denver, CO: LADOCA; 1969 Kube DA, Wilson WM, Petersen MC, Palmer FB. CAT/CLAMS: its use in detecting early childhood cognitive impairment. Pediatr Neurol. 2000;23(3):208–215 Griffiths R. The Abilities of Babies: A Study in Mental Measurement. New York, NY: McGraw-Hill; 1954:229 HIV Paediatric Prognostic Markers Collaborative Study. Predictive value of absolute CD4 cell count for disease progression in untreated HIV-1-infected children. AIDS. 2006;20(9):1289–1294 85. Janssen N, Ndirangu J, Newell ML, Bland RM. Successful paediatric HIV treatment in rural primary care in Africa. Arch Dis Child. 2010;95(6):414–421 86. UNAIDS. 2008 report on the global AIDS epidemic. Updated 2008. Available at: http://www.unaids.org/en/dataanalysis/ knowyourepidemic/epidemiologypublications/ 2008reportontheglobalaidsepidemic/. Accessed March 17, 2011 87. Ndirangu J, Newell ML, Tanser F, Herbst AJ, Bland R. Decline in early life mortality in a high HIV prevalence rural area of South Africa: evidence of HIV prevention or treatment impact? AIDS. 2010;24(4):593– 602 88. Patel K, Hernán MA, Williams PL, et al; Pediatric AIDS Clinical Trials Group 219/219C Study Team. Long-term effectiveness of highly active antiretroviral therapy on the survival of children and adolescents with HIV infection: a 10-year follow-up study. Clin Infect Dis. 2008;46(4):507–515 PEDIATRICS Volume 130, Number 5, November 2012 Downloaded from pediatrics.aappublications.org by guest on August 22, 2014 19 Neurodevelopment in Children Born to HIV-Infected Mothers by Infection and Treatment Status Kirsty Le Doaré, Ruth Bland and Marie-Louise Newell Pediatrics; originally published online October 1, 2012; DOI: 10.1542/peds.2012-0405 Updated Information & Services including high resolution figures, can be found at: http://pediatrics.aappublications.org/content/early/2012/09/26 /peds.2012-0405 Citations This article has been cited by 1 HighWire-hosted articles: http://pediatrics.aappublications.org/content/early/2012/09/26 /peds.2012-0405#related-urls Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its entirety can be found online at: http://pediatrics.aappublications.org/site/misc/Permissions.xh tml Reprints Information about ordering reprints can be found online: http://pediatrics.aappublications.org/site/misc/reprints.xhtml PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Downloaded from pediatrics.aappublications.org by guest on August 22, 2014









© Copyright 2025