
Tuesday - American Association for Thoracic Surgery
TH 95 AATS DAI LY NEW S 2015 A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA TUESDAY EDITION TUESDAY 7:00 a.m. – 8:40 a.m. Cardiac Surgery Forum 7:00 a.m. – 8:40 a.m. General Thoracic Surgery Forum 7:00 a.m. – 8:40 a.m. Adult Cardiac Emerging Technology and Techniques Forum NEW! 7:00 a.m. – 8:40 a.m. General Thoracic Emerging Technology and Techniques Forum NEW! 7:00 a.m. – 8:40 a.m. Video Session 7:00 a.m. – 8:40 a.m. VAD/ECMO Session NEW! 8:45 a.m. – 12:30 p.m. Plenary Scientific Session 11:40 p.m. – 12:30 p.m. HONORED GUEST LECTURE Three Ideas About Changing Things Col. Casey Haskins 12:30 p.m. – 2:00 p.m. President del Nido Counsels Pragmatist Approach W hile applauding the progress in technology and innovation that the cardiothoracic surgery community has made until now, Pedro J. del Nido, MD, used his presidential address “Technological Innovation in Cardiothoracic Surgery: A Pragmatist’s Approach” to ask the question: How can we do better? Certainly, the AATS has made excellent strides so far, he said, pointing out how, through the work of the Scientific Affairs and Government Relations Committee (SAGR), “CT surgery has achieved one of the highest levels of representation within the Study Sections of NIH in the Committee’s history, including CT surgical representation both at the Center for Scientific Review, and now finally within the review panels of the National Cancer Institute.” “We can take great pride in these accomplishments, along with the successes of the Cardiac Surgery Clinical Trials Network and Pediatric Heart Network,” he added. Of particular import toward the development of new research and innovation opportunities has also been the work of David Sugarbaker, MD, and the AATS Graham Foundation, which has been able to provide educational and research opportunities to residents, fellows and young faculty members, providing alternative funding opportunities for young investigators through seed and early career grants. Continued on page 3 Pedro J. del Nido, MD, gave his presidential address stressing the need for innovation. Lunch in the Exhibit Hall 12:45 p.m. – 2:00 p.m. Moderated Poster Competition Continued on page 4 Honored Guest Lecturer: Col. Casey Haskins Tuesday, 11:40 Colonel Casey Haskins will bring his expertise on helping leaders build innovative, creative environments and attitudes. In his army career, he has commanded at every level from platoon through brigade and has served in staff positions from battalion COL. HASKINS through theater army. An accomplished military officer, faculty member at West Point Academy and founder of the consulting firm, BLK SHP INNOVATIONS, Col. Haskins will speak about strategies that facilitate the discovery and reinvention of solutions to challenging problems. M Monday’s Plenary: Improving Outcomes onday’s Plenary Session featured presentations on assessing and improving outcomes in some of the most complex cardiothoracic surgery procedures. Topics ranged from dealing with open thoracoabdominal aneurysm repairs to using concomitant tricuspid annuloplasty during mitral valve repair. The session was moderated by AATS President Pedro J. del Nido, MD, of Boston Children’s Hospital, and Marc R. Moon, MD, of Washington University School of Medicine. Outcomes of Thoracoabdominal Aortic Aneurysm Repair Joseph S. Coselli, MD, presented the results of the study he and his colleagues at Baylor College of Medicine in Houston conducted, analyzing data from 3309 open TAAA repairs performed between October 1986 and December 2014. Their series showed that open TAAA repair produced respectable early outcomes, although preoperative and intraoperative factors were found to influence risk. Joseph S. Coselli, MD, presented data from the largest ever TAAA series. The results showed an operative mortality rate of 7.5% and a 30-day death rate of 4.8, with the adverse event outcome occurring among around 14% of repairs. The statistically significant predictors of operative death were rupture, renal insufficiency, symptoms, procedures targeting visceral vessels, increasing age, and increasing clamp time, while extent IV repair (the least extensive form of TAAA repair) was inversely associated with death. Their analysis showed that the significant predictors of adverse event were use of HCA, renal insufficiency, rupture, extent II repair, visceral vessel procedures, urgent or emergent repair, increasing age, and increasing clamp time. Outcomes differed by extent of repair, with the risk being greatest in extent II repair. Actuarial survival was 63.6% at 5 years, 36.8% at 10 years and 18.3% at 15 years. Freedom from repair failure was nearly 98% at 5 years, around 95% at 10 years and 94% at 15 years. “Along with respectable early outcomes, after repair, patients have acceptable long-term survival, and late repair failure was uncommon. Notably, there are several subgroups of patients that do exceedingly well. Paraplegia in young patients with connective tissue Continued on page 4 DELIVERING MORE INNOVATION CoreValve® TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) PLATFORM Driving the future of TAVR. The CoreValve Platform is now indicated for patients with a failed bioprosthetic aortic valve. Stop by Medtronic booth 537 to learn more about the CoreValve Platform. Innovating for life. CAUTION: Federal law (USA) restricts these devices to sale by or on the order of a physician. For a listing of indications, contraindications, warnings, precautions and adverse events, please review the Brief Statement Documents available at the Medtronic booth. 201506322EN.indd 1 CoreValve is a registered trademark of Medtronic CV Luxembourg S.a.r.l. ©2015 Medtronic. All rights reserved. UC201506322 EN 03/2015 4/2/15 9:04 AM A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER Continued from page 1 He was pleased to note that “In the past year, in partnership with leaders in industry, the Graham Foundation has begun to offer specialized fellowships in fields such as esophageal, arrhythmia and robotic surgery, and plans for several other similar opportunities for our Fellows and young faculty.” “But AATS has not achieved the high status that it enjoys today by resting on its laurels or by focusing on its past achievements,” said Dr. del Nido. The remainder of his presentation outlined his vision of how the Association should proceed. From a review of the history of the field, Dr. del Nido revealed a definitive conclusion: “I contend that the relentless advance of technology and new concepts in our specialty over the last 50 to 70 years is largely a result of our approach to innovation, which exemplifies the pragmatist philosophy.” He cited the Pragmatist School and its leading thinker, William James, who said “Theories thus become instruments, not answers to enigmas in which we can rest.” This translates, according to Dr. del Nido, to the position that “the meaning of an idea can be found in its practical consequences.” This has obvious implications for the development of new knowledge, including in the field of cardiothoracic surgery. “The importance of this philosophical approach to the advancement of our specialty and the advancement of medicine in general cannot be overestimated,” he said. “The pragmatist approach leaves us ‘I contend that the relentless advance of technology and new concepts in our specialty over the last 50 to 70 years is largely a result of our approach to innovation, which exemplifies the pragmatist philosophy.’ open to new ideas and new solutions to problems that may be better than old solutions. This is the mindset at the core of innovation. It drives the innovator’s desire for generating better solutions and the willingness to try something new, not for the sake of novelty, but for a better result.” Cardiothoracic surgery progressed from the 1930s to the 1970s through a period of rapidly changing and exciting times, developing new technologies at an unprecedented pace. But in 1976, Congress passed the Medical Device Amendment to the • S EATTLE , WA AATS 95TH ANNUAL MEETING federal Food, Drug, and Cosmetic Act, expanding the role of the Food and Drug Administration, and thereafter medical devices required review and approval prior to marketing. This had a major impact on industry. Ultimately, the process of bringing technological advances to patients became more structured and along with regulatory and financial pressures on the health care environment, the process of developing a novel therapy became much more complex, often requiring resources that are not readily available to the practicing surgeon. “However, this does not mean we should wait for new technology or therapies to reach us,” counseled Dr. del Nido. “History has shown us that a passive approach will virtually guarantee our obsolescence.” To prevent this requires forging partnerships with others outside the field, whether they are engineers, basic scientists, or even experts in the areas of public policy, regulatory matters, and commercialization. This very often means interactions with industry. “The major benefits of these partnerships include a greater focus on practical application of the discovery and access to the technology, regulatory, and commercial resources of industry, which are often not available in an academic laboratory,” Dr. del Nido said. But he also pointed out that it is not just on the individual level that innovation must be pursued. “Our professional societies can also participate in this process. Indeed they must,” he stated. The AATS plays a critical role in supporting young investigators with grants or special fellowships and advocating for surgical scientists with the National Institutes of Health and other government entities. And an especially important role for AATS is the dissemination of new technology through educational programs such as the Mitral Conclave and the Aortic Symposium. These are all significant activities that it is important for the AATS to continue and expand “to support our specialty in its pursuit of the innovation imperative,” said Dr. del Nido. “And, if you have any doubts as to whether the spirit and pragmatist philosophy is still part of our specialty, I simply ask you to look around and take in what is being presented at this meeting. “If you do, you will find a wealth of new ideas, jam-packed with novel concepts and exciting new technologies. What we need now is for all of us to join forces, reach outside the boundaries of our profession, with a common goal to improve the lives of our patients,” Dr. del Nido concluded. CoreValve® Transcatheter Aortic Valve Replacement (TAVR) Platform INDICATIONS The Medtronic CoreValve system is indicated for use in patients with symptomatic heart disease due to severe native calcific aortic stenosis or failure (stenosed, insufficient, or combined) of a surgical bioprosthetic aortic valve who are judged by a heart team, including a cardiac surgeon, to be at high or greater risk for open surgical therapy (i.e., Society of Thoracic Surgeons operative risk score ≥8% or at a ≥15% risk of mortality at 30 days). CONTRAINDICATIONS The CoreValve system is contraindicated for patients presenting with any of the following conditions: • known hypersensitivity or contraindication to aspirin, heparin (HIT/HITTS) and bivalirudin, ticlopidine, clopidogrel, Nitinol (Titanium or Nickel), or sensitivity to contrast media, which cannot be adequately premedicated • ongoing sepsis, including active endocarditis • preexisting mechanical heart valve in aortic position. WARNINGS General Implantation of the Medtronic CoreValve system should be performed only by physicians who have received Medtronic CoreValve training. This procedure should only be performed where emergency aortic valve surgery can be performed promptly. Mechanical failure of the delivery catheter system and/or accessories may result in patient complications. Transcatheter Aortic Valve (Bioprosthesis) Accelerated deterioration of the bioprosthesis may occur in patients presenting with an altered calcium metabolism. PRECAUTIONS General The safety and effectiveness of the Medtronic CoreValve system have not been evaluated in the pediatric population. The safety and effectiveness of the bioprosthesis for aortic valve replacement have not been evaluated in the following patient populations: • with a native valve lesion which does not meet the criteria for severe aortic stenosis (Aortic valve area ≤1.0 cm2 or aortic valve area index ≤0.6 cm2/m2, a mean aortic valve gradient of ≥40 mm Hg, or a peak aortic-jet velocity ≥4.0 m/s) • who are at moderate or low surgical risk (predicted perioperative mortality risk of <15%) • with untreated, clinically significant coronary artery disease requiring revascularization • with a preexisting prosthetic heart valve with a rigid support structure in either the mitral or pulmonic position if either the preexisting prosthetic heart valve could affect the implantation or function of the bioprosthesis or the implantation of the bioprosthesis could affect the function of the preexisting prosthetic heart valve • with cardiogenic shock manifested by low cardiac output, vasopressor dependence, or mechanical hemodynamic support • The safety and effectiveness of a CoreValve bioprosthesis implanted within a failed preexisting transcatheter or surgical bioprosthesis have not been demonstrated. • Implanting a CoreValve bioprosthesis in a degenerated surgical bioprosthesis (transcatheter aortic valve in surgical aortic valve [TAV in SAV]) should be avoided in the following conditions. The degenerated surgical bioprosthesis presents with a: • Significant concomitant perivalvular leak (between the prosthesis and the native annulus), is not securely fixed in the native annulus, or is not structurally intact (eg, wireform frame fracture) • Partially detached leaflet that in the aortic position may obstruct a coronary ostium • Stent frame with a manufacturer’s labeled inner diameter <17 mm • The safety and effectiveness of the bioprosthesis for aortic valve replacement have not been evaluated in patient populations presenting with the following: • blood dyscrasias as defined: leukopenia (WBC <1000 cells/mm3), thrombocytopenia (platelet count <50,000 cells/ mm3), history of bleeding diathesis or coagulopathy, or hypercoagulable states • congenital bicuspid or unicuspid valve verified by echocardiography • mixed aortic valve disease (aortic stenosis and aortic regurgitation with predominant aortic regurgitation [3-4+]) • moderate to severe (3-4+) or severe (4+) mitral or severe (4+) tricuspid regurgitation • hypertrophic obstructive cardiomyopathy • new or untreated echocardiographic evidence of intracardiac mass, thrombus, or vegetation • native aortic annulus size <18 mm or >29 mm per the baseline diagnostic imaging or surgical bioprosthetic aortic annulus size <17 mm or >29 mm • transarterial access not able to accommodate an 18-Fr sheath • sinus of valsalva anatomy that would prevent adequate coronary perfusion • moderate to severe mitral stenosis • severe ventricular dysfunction with left ventricular ejection fraction (LVEF) <20% as measured by resting echocardiogram • end-stage renal disease requiring chronic dialysis or creatinine clearance <20 cc/min • symptomatic carotid or vertebral artery disease • severe basal septal hypertrophy with an outflow gradient Prior to Use Exposure to glutaraldehyde may cause irritation of the skin, eyes, nose, and throat. Avoid prolonged or repeated exposure to the vapors. Damage may result from forceful handling of the catheter. Prevent kinking of the catheter when removing it from the packaging. This device was designed for single patient use only. Do not reuse, reprocess, or resterilize this product. Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and/or create a risk of contamination of the device, which could result in patient injury, illness, or death. The bioprosthesis size must be appropriate to fit the patient’s anatomy. Proper sizing of the device is the responsibility of the physician. Refer to Instructions for Use for available sizes. Failure to implant a device within the sizing matrix could lead to adverse effects such as those listed in below. Patients must present with access vessel diameters of ≥6 mm or an ascending aortic (direct aortic) access site ≥60 mm from the basal plane. Implantation of the bioprosthesis should be avoided in patients with aortic root angulation (angle between plane of aortic valve annulus and horizontal plane/vertebrae) of >30° for right subclavian/axillary access or >70° for femoral and left subclavian/axillary access. Use caution when using the subclavian/axillary approach in patients with a patent LIMA graft or patent RIMA graft. During Use Adequate rinsing of the bioprosthesis with sterile saline, as described in the Instructions for Use, is mandatory before implantation. During rinsing, do not touch the leaflets or squeeze the bioprosthesis. If a capsule becomes damaged during loading or the capsule fails to close, replace the entire system (bioprosthesis, catheter, and CLS). Do not use a catheter with a damaged capsule. After a bioprosthesis has been inserted into a patient, do not attempt to reload that bioprosthesis on the same or any other catheter. During implantation, if resistance to deployment is encountered (e.g., the micro knob starts clicking or is tight or stuck), apply upward pressure to the macro slider while turning the micro knob. If the bioprosthesis still does not deploy, remove it from the patient and use another system. While the catheter is in the patient, ensure the guidewire is extending from the tip. Do not remove the guidewire from the catheter while the catheter is inserted in the patient. Once deployment is initiated, retrieval of 201506322EN.indd 2 3 the bioprosthesis from the patient (e.g., use of the catheter) is not recommended. Retrieval of a partially deployed valve using the catheter may cause mechanical failure of the delivery catheter system, aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. During deployment, the bioprosthesis can be advanced or withdrawn as long as annular contact has not been made. Once annular contact is made, the bioprosthesis cannot be advanced in the retrograde direction; if necessary, and the frame has only been deployed ≤2/3 of its length, the bioprosthesis can be withdrawn (repositioned) in the antegrade direction. However, use caution when moving the bioprosthesis in the antegrade direction. Use the handle of the delivery system to reposition the bioprosthesis. Do not use the outer catheter sheath. Once deployment is complete, repositioning of the bioprosthesis (e.g., use of a snare and/or forceps) is not recommended. Repositioning of a deployed valve may cause aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. Do not attempt to retrieve a bioprosthesis if any one of the outflow struts is protruding from the capsule. If any one of the outflow struts has deployed from the capsule, the bioprosthesis must be released from the catheter before the catheter can be withdrawn. Ensure the capsule is closed before catheter removal. If increased resistance is encountered when removing the catheter through the introducer sheath, do not force passage. Increased resistance may indicate a problem and forced passage may result in damage to the device and/or harm to the patient. If the cause of resistance cannot be determined or corrected, remove the catheter and introducer sheath as a single unit over the guidewire, and inspect the catheter and confirm that it is complete. Clinical long-term durability has not been established for the bioprosthesis. Evaluate bioprosthesis performance as needed during patient follow-up. Postprocedure, administer appropriate antibiotic prophylaxis as needed for patients at risk for prosthetic valve infection and endocarditis. Postprocedure, administer anticoagulation and/or antiplatelet therapy per hospital protocol. Excessive contrast media may cause renal failure. Preprocedure, measure the patient’s creatinine level. During the procedure, monitor contrast media usage. Conduct the procedure under fluoroscopy. The safety and efficacy of implanting a second CoreValve bioprosthesis within the initial CoreValve bioprosthesis have not been demonstrated. However, in the event that a second CoreValve bioprosthesis must be implanted within the initial CoreValve bioprosthesis to improve valve function, valve size and patient anatomy must be considered before implantation of the second CoreValve bioprosthesis to ensure patient safety (e.g., to avoid coronary obstruction). In the event that valve function or sealing is impaired due to excessive calcification or incomplete expansion, a postimplant balloon dilatation of the bioprosthesis may improve valve function and sealing. To ensure patient safety, valve size and patient anatomy must be considered when selecting the size of the balloon used for dilatation. The balloon size chosen for dilatation should not exceed the diameter of the native aortic annulus or, for surgical bioprosthetic valves, the manufacturer’s labeled inner diameter. Refer to the specific balloon catheter manufacture’s labeling for proper instruction on the use of balloon catheter devices. Note: Bench testing has only been conducted to confirm compatibility with NuMED Z-MED IITM Balloon Aortic Valvuloplasty catheters where CoreValveTM bioprosthesis device performance was maintained after dilation. Data on File. POTENTIAL ADVERSE EVENTS Potential risks associated with the implantation of the Medtronic CoreValve transcatheter aortic valve may include, but are not limited to, the following: • death • cardiac arrest • coronary occlusion, obstruction, or vessel spasm (including acute coronary closure) • emergent surgery (e.g., coronary artery bypass, heart valve replacement, valve explant) • multi-organ failure • heart failure • myocardial infarction • cardiogenic shock • respiratory insufficiency or respiratory failure • cardiovascular injury (including rupture, perforation, or dissection of vessels, ventricle, myocardium, or valvular structures that may require intervention) • ascending aorta trauma • cardiac tamponade • cardiac failure or low cardiac output • prosthetic valve dysfunction including, but not limited to, fracture; bending (out-of-round configuration) of the valve frame; under-expansion of the valve frame; calcification; pannus; leaflet wear, tear, prolapse, or retraction; poor valve coaptation; suture breaks or disruption; leaks; mal-sizing (prosthesis-patient mismatch); malposition (either too high or too low)/malplacement; regurgitation; stenosis • thrombosis/embolus (including valve thrombosis) • valve migration/valve embolization • ancillary device embolization • emergent percutaneous coronary intervention (PCI) • emergent balloon valvuloplasty • major or minor bleeding that may or may not require transfusion or intervention (including life-threatening or disabling bleeding) • allergic reaction to antiplatelet agents, contrast medium, or anesthesia • infection (including septicemia and endocarditis) • stroke, TIA, or other neurological deficits • permanent disability • renal insufficiency or renal failure (including acute kidney injury) • mitral valve regurgitation or injury • tissue erosion • vascular access related complications (e.g., dissection, perforation, pain, bleeding, hematoma, pseudoaneurysm, irreversible nerve injury, compartment syndrome, arteriovenous fistula, stenosis) • conduction system disturbances (e.g., atrioventricular node block, left-bundle branch block, asystole), which may require a permanent pacemaker Please reference the CoreValve Instructions for Use for more information regarding indications, warnings, precautions and potential adverse events. CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician. CoreValve is a registered trademark of Medtronic CV Luxembourg S.a.r.l. © 2015 Medtronic, Inc. All rights reserved. UC201506322 EN 4/2/15 9:04 AM 4 AATS 95TH ANNUAL MEETING Continued from page 1 disorders, even in the most extensive repair (extent II), is remarkably rare – these patients do extremely well across the board,” Dr. Coselli concluded. Comparing Norwoods: SANO vs. BT Early survival advantages of using the Norwood procedure with the Sano shunt (SANO) over the standard Norwood-BT shunt (BT) are confounded by concerns surrounding delayed right ventricular dysfunction Travis J. Wilder, MD, presented data showing SANO bested the BT shunt. Continued from page 1 2:00 p.m. – 5:35 p.m. Adult Cardiac Surgery Simultaneous Scientific Session 2:00 p.m. – 5:35 p.m. Congenital Heart Disease Surgery Simultaneous Scientific Session 2:00 p.m. – 5:35 p.m. General Thoracic Surgery Simultaneous Scientific Session 2:00 p.m. – 5:35 p.m. Aortic/Endovascular Surgery Simultaneous Scientific Session 5:35 p.m. – 6:15 p.m Executive Session (AATS Members only) 7:00 p.m. – 10:00 p.m. AATS Attendee Reception at The Museum of Flight WEDNESDAY 7:00 a.m. – 9:35 a.m. Adult Cardiac Surgery Simultaneous Scientific Session 7:00 a.m. – 9:35 a.m. Congenital Heart Disease Simultaneous Scientific Session 7:00 a.m. – 9:35 p.m. General Thoracic Surgery Simultaneous Scientific Session 9:45 a.m. – 11:15 a.m. Adult Cardiac Masters of Surgery Video Session 9:45 a.m. – 11:15 a.m. Congenital Heart Disease Masters of Surgery Video Session 9:45 a.m. – 11:15 a.m. General Thoracic Masters of Surgery Video Session A PRIL 25-29, 2015 seen after SANO. “In children with hypoplastic left heart syndrome (HLHS), we compared trends in long-term RV dysfunction and tricuspid regurgitation (TR) between these strategies and incorporated survival differences. Our registry results were favorable for SANO over BT across several parameters, a difference from what has been seen in clinical trials,” according to Travis J. Wilder, MD, of the Congenital Heart Surgeons’ Society Data Center in Toronto. Dr. Wilder presented the results that he and his colleagues obtained from an inception cohort of neonates with HLHS who were managed by Norwood palliation, using propensity matching to pair SANO with BT patients. Propensity-adjusted survival was significantly worse with BT and this remained throughout follow-up with no evidence of convergence as late as 5 years, according to Dr. Wilder. “In our analysis, for comparable neonates with HLHS undergoing Norwood operation, SANO offers better late (greater than 3-year) survival, less late TR and possibly less late RV dysfunction than BT. The results from a research registry differ from randomized comparisons between the two strategies,” concluded Dr. Wilder. • W ASHINGTON S TATE C ONVENTION C ENTER Sebastien Gilbert, MD, compared analog and digital pleural monitoring. Digital vs. Analog Pleural Drainage Digital pleural drainage devices are a new and promising tool for optimizing chest tube management after lung resection presumably because of their ability to continuously monitor and record parenchymal air leak flow, and regulate intra-pleural pressure. However, it remains unknown whether or not this technology can benefit all patients or mainly those who have a postoperative air leak, according to Sebastien Gilbert, MD, University of Ottawa, and his colleagues. Dr. Gilbert reported on their study • S EATTLE , WA to examine the impact of using a digital pleural drainage device on time to chest tube removal and on length of stay, stratified according to the presence or absence of an air leak after lung resection. Although they found no significant improvement in these outcomes, they did find a significant decrease in chest tube clamping trials, with use of the digital device. After stratification according air leak status on the first postoperative day, randomization to the new pleural drainage technology did not significantly reduce the duration of chest tube drainage or hospital stay, according to Dr. Gilbert. However, chest tube clamping trials were significantly reduced in digital device patients with an air leak (23% vs. 50%) and in those without an air leak (0% vs. 16%). “Based on the results, we cannot recommend the use of digital devices as an intervention to reduce length of hospital stay after lung resection. Despite the absence of a clear-cut benefit in our study, we still think that the technology presents opportunities to improve efficiency, refine evidence-based practice in chest tube management, and gain a more fundamental understanding of pleural space mechanics after pulmonary resection,” Dr. Gilbert concluded. Biological Engineering–Basic Science Lecture 0 ffering a “glimpse of things to come,” Donald Ingber, MD, PhD, of the Wyss Institute for Biologically Inspired Engineering, outlined an exciting new world on the edge of science fiction – human organs on a chip, robotic insects that can fly, and a miniature human body made of chips. These are not just interesting curiosities, but in fact are proving to be powerful study tools, with not only the potential to replace animal testing of new human drugs, but providing the ability to mimic human physiology and genetics to the point of identifying new drug and therapeutic targets and the very people who are most likely to benefit from them. Part of the goal of the Wyss Institute is to foster the fusion of biology and engineering, of life and non-life, to create new forms of research tools and instrumentation straddling the boundaries of both. The Institute has been so successful that since its inception, it has been producing an article a month in either Science or Nature and has around 1000 patents already. The current drug development model is essentially failing, according to Dr. Ingber. Its costs are skyrocketing, with a price tag of over $2 million to test a Donald Ingber, MD, spoke of the new interface between life and non-life. single candidate in animals. The use of organs on a chip has the potential to replace this with far more relevance, since these have the opportunity to mimic the authentic metabolic and physiological behavior of human organs, something that animal models often fail to do. A good example of this breakthrough technology is the human breathing lung on a chip. This consists of 3 channels – an air channel above, a layer of human lung cells and a circulating blood channel. The cells are made to “breathe” by side chambers that expand and contract to change their configuration. So successful is this model that they have found it capable of imitating the behavior of smog air pollutants as they naturally affect real human lungs, and also capable of mimicking pulmonary edema when appropriately triggered, said Dr. Ingber. Similarly, researchers at the Institute have developed a human gut on a chip which with proper stimulation actually forms human villi-like structures capable of mimicking the behavior of disease and probiotic bacteria. There is also a beating heart on a chip, a human kidney chip that “pees” and even a spleen capable of clearing toxins from human blood. Remarkably all of these new chips can be linked to create an integrated human in a ‘body’ that is capable of passing materials (including drugs) from organ chip to organ chip in a manner that simulates authentic physiological pathways. Ultimately, there is even the opportunity to personalize these chips using individualized patient cells to get unique genomic behaviors, Dr. Ingber concluded. 6 AATS 95TH ANNUAL MEETING T A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA Evaluating Techniques in Congenital Heart Surgery he Ross operation has acceptable outcomes in selected pediatric patients with biventricular circulation. However, there are little data concerning outcomes in patients with univentricular circulation undergoing biventricular conversion, according to Alejandra Bueno, MD, of Boston Children’s Hospital and her colleagues. In Monday’s Congenital Heart Surgery Symposium, Dr. Bueno reported on their study that reviewed the outcomes before and after Ross operations, including patients undergoing AATS Council biventricular conversion with the Damus-Kaye-Stansel (DKS) takedown. They performed a retrospective review on 62 consecutive patients who underwent simple and complex Ross operations at a single institution from March 2000 to October 2014, including eight patients who underwent biventricular conversion with Ross operation and DKS takedown with or without reversal of the cavopulmonary connection (defined as complex). The Ross procedure has good similar short-term results in simple and complex patients and should be considered for use in those undergoing biventricular conversion and DKS takedown. Moreover, the study shows that native PV size should not be a contraindication for the Ross Left to right sitting: Secretary: Marc R. Moon, Washington University; President-Elect: Joseph S. Coselli, Baylor College of Medicine; President: Pedro J. del Nido, Boston Children’s Hospital; Vice President: Thoralf M. Sundt, III, Massachusetts General Hospital; Treasurer: Duke E. Cameron, Johns Hopkins Hospital Standing Councilors: David J. Sugarbaker, Baylor College of Medicine; David R. Jones, Memorial Sloan Kettering Cancer Center; David H. Adams, Mount Sinai Medical Center; J. William Gaynor, Children’s Hospital of Philadelphia; José Pomar, Hospital Clinico de Barcelona; Lars G. Svensson, Cleveland Clinic Alejandra Bueno, MD, presented a study of the Ross procedure. Richard Dobson, MD, reported on adult survivors of tetralogy of Fallot repair. procedure,” Dr. Bueno concluded. Richard Dobson, MD, of the Scottish Adult Congenital Cardiac Service, discussed a study that he and his colleagues performed to examine the long-term outcomes of adult survivors of surgical repair of tetralogy of Fallot with respect to survival, functional capacity, and adverse events, as well as the effect of pulmonary valve replacement (PVR). They found that these patients had excellent long-term survival; although PVR did not convey a survival benefit, despite improvements in functional outcomes. Dr. Dobson reported on a retrospective cohort analysis of 376 adult survivors of repaired tetralogy of Fallot enrolled through a national adult congenital cardiac database. They found that at 40-year follow-up from the date of repair that freedom from death was 83%, from atrial arrhythmia was 60%, from ventricular arrhythmia was 73%, from pacemaker/ ICD insertion was 70%, and from surgical/percutaneous reintervention was 27%. In a multivariate model, the risk of death was significantly increased by older age at repair, atrial arrhythmia by older age at repair, device insertion by the presence of a genetic syndrome, and reintervention by any non-classical form of tetralogy of Fallot and the use of a transannular patch repair. At follow-up, the vast majority of patients were NYHA class 1.The mean QRS duration was 147 milliseconds (ms). Each ms increase raised the risk of all-cause mortality in a univariate model. There were nearly 35% of patients with moderate or greater pulmonary regurgitation (PR) at latest follow-up, with mean PR fraction 25%. “In adult patients with repaired tetralogy of Fallot, long-term survival remains excellent. However morbidity, arrhythmias and repeat intervention are frequent,” Dr. Dobson concluded. A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER Top Gun Contest During the Welcome Reception on Sunday, the top five resident finalists showcased their technical skills as they competed for the designation of the 2015 Resident Top Gun in the Cardiothoracic Surgery Resident “Top Gun” Competition. The winner will be announced on Tuesday morning. AATS Resident Poster Competition The AATS Cardiothoracic Resident Poster Competition provides an opportunity for senior cardiothoracic surgery residents and/or congenital heart surgery fellows to represent their institution in a competition against one another by presenting a scientific poster of their clinical/investigative research. The winners will be announced on Tuesday. • S EATTLE , WA AATS 95TH ANNUAL MEETING 7 8 AATS 95TH ANNUAL MEETING H • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA Monday’s Adult Cardiac Surgery Simultaneous Session ow well do benchmarks and selection criteria predict outcomes for surgical aortic valve replacement (AVR) surgery in elderly, high-risk patients? Results from the arm of the PARTNER-I trial of transcatheter AVR (TAVR) for severe aortic stenosis suggest that benchmarks may do poorly in discriminating across high-risk populations. In fact, despite surgical AVR being performed in institutions whose results generally outperform national bench- Wilson Szeto, MD, spoke on selection criteria for TAVR outcomes. marks, high-risk, operable (PARTNER-IA) patients experienced only average early results and prolonged hospitalization, according to Wilson Szeto, MD, who presented an analysis of the PARTNER patient selection criteria and outcomes at Sunday’s Adult Cardiac Surgery Symposium. Dr. Szeto of the University of Pennsylvania Medical Center, discussed how the PARTNER-1 trial provided the unique opportunity to ask some crucial questions: First, whether outcomes after surgical AVR in an elderly, high-surgical-risk population are accurately predicted by contemporary Society of Thoracic Surgeons (STS) benchmarks; and second, whether their intermediate-term survival was commensurate with that of the gen- Bring the AATS Annual Meeting Home M A PRIL 25-29, 2015 ost presentations from the 2015 AATS Annual Meeting will be available on the AATS website, www.aats.org, immediately following the meeting. Re-visit a session, share with your colleagues, or view a presentation you may have missed. eral population. Dr. Szeto and his colleagues also examined the data to determine whether there was an identifiable subset of these patients whose observed risk after surgical AVR was higher than those patients deemed inoperable in the trial (PARTNER-IB), which would indicate a less-than-optimal selection criteria. Observed operative mortality was not significantly different from the expected. Nor was there a significant difference in the rate of observed stroke or sternal wound infection as compared with expected. However, the observed renal failure (lower than expected) and the observed prolonged length of stay (higher than expected) were both significantly different. Dr. Szeto did note a caveat, that the calibration of observed events across the spectrum of expected risk was poor. In terms of survival, the 1-, 2-, 3-, and 4-year rates were substantially lower than those seen in the matched U.S. population, but higher than those seen in the PARTNER-IB cohort. Risk factors for death included smaller body mass index, lower albumin, history of cancer, longer aortic clamp time, and severe prosthesis-patient mismatch. Only the 10% of patients with a poor risk profile based on preoperative comorbidity had an estimat- George L. Zorn, III, MD, spoke on PPM in SAVR and TAVR. ed 1-year survival less than that of the standard therapy patients. Unlike past surgical series, in which survival of elderly patients was commensurate with a matched U.S. population, PARTNER-IA patients had worse survival, suggesting that they were a less highly selected population. However, after a period of higher early mortality, most PARTNER-IA patients experienced better mid-term survival than inoperable PARTNER-IB patients, suggesting that PARTNER selection criteria for surgical AVR, with a few caveats, may be more appropriate for improving survival than previous practice, according to Dr. Sveto. Prosthesis-patient mismatch may be a factor with implications for left Anelechi Anyanwu, MD, reported on stratifying valve repairs. ventricular mass regression in patients undergoing either surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR). In patients at increased surgical risk and with severe aortic stenosis, prosthesis-patient mismatch (PPM) is more common and more severe in those treated with SAVR than in those treated with TAVR, according to George L. Zorn, III, MD, of the University of Kansas Hospital. Dr. Zorn reported that despite this difference, left ventricular mass regression was observed in both TAVR and SAVR treatment groups. Dr. Zorn and his colleagues compared the incidence of PPM between TAVR using a self-expanding prosthesis and SAVR in the high-risk arm of the CoreValve US Pivotal Trial. They also evaluated the impact of mismatch on left ventricular mass (LVM) regression. “Although LVMI regression was observed in both TAVR and SAVR treatment groups, there was a greater magnitude of regression in the SAVR treatment arm,” Dr. Zorn concluded. Although degenerative valve repairs vary in complexity, depending on lesions encountered, guidelines and publications on process and outcomes of valve repair for degenerative disease generally group patients as a single cohort. Anelechi Anyanwu, MD, and his colleagues at Mount Sinai Medical Center attempted to deal with this disparity by developing a complexity score to allow stratification of valve repairs, and to evaluate the impact of complexity on operative process and outcomes. Dr. Anyanwu reported on their study, which retrospectively analyzed data on 668 consecutive mitral valve operations for degenerative disease. “We developed a lesion score and graded valves based on intraoperative valve analysis and categorized valves into three complexity groups based on the total complexity score,” he said, describing lesion scores of 1: simple (244 patients); 2-4: intermediate (260 patients); 5 or more: complex (164 patients). The researchers compared the results from these three groups. “Despite longer and more technically involved repairs, we observed extremely high repair rates and excellent results in patients with complex lesions,” said Dr. Anyanwu. “Our study shows that lesion scoring can facilitate preoperative planning if applied echocardiographically. A surgeon should be able to predict reparability of a particular valve in their practice. Particularly for asymptomatic patients, surgeons should consider other options if they are not likely to predictably repair the valve based on its complexity. Where the complexity score is high, the surgeon should be facile with a blend of repair techniques and be prepared to commit to a longer operative time and to use multiple techniques to effect a durable repair. A surgeon taking on Complex Valves should be well versed in advanced surgical tech- Daniel Enter, MD, discussed risk factors in mitral valve patients. niques as these were required in half of our complex cases,” Dr. Anyanwu concluded. Daniel Enter, MD, of Northwestern University, spoke on pulmonary hypertension in patients having mitral valve surgery. He explored the question of hypertension as a 30-day risk factor in these patients. 10 AATS 95TH ANNUAL MEETING A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA 2015 AATS Annual Meeting Exhibitors L L L E XIT AATS Exhibit Hall Hours SCIENTIFIC SESSIONS N9 N10 WELCOME CENTER L TO FIRE E XITS Tuesday April 28 9:00 a.m. – 4:30 p.m. N13 C YBER C AF E N12 L NO BOO THS THIS AR EA E XIT E XIT E XIT G AT E 5 G AT E 7 L E XIT G AT E 4 L F&B 140 138 136 134 132 FUTURE MEETINGS 343 Edwards Lifesciences Medtronic MAQUET Medical 337 Systems TOP G UN 9' POSTERS 537 737 531 431 Medtronic Customer Experience Center On-X Life Technologies 333 331 F& B S TAGE SYMPOSIA WALL FHC FE F THE ATER # 1 142 LEARNING CENTER ENTRANCE 144 Association Booths LE TO SOUTH LOB B Y CHARGING STATION 730 831 Medtronic Customer Experience Center 931 48 POSTER BOARDS 128 C WF P UB LIC P HO NE S RO O M 401 2016 BOOTH S ELEC TION 723 520 1023 1123 WO MEN 1017 1116 1117 1011 1110 1111 919 516 Companies highlighted in orange are advertisers of the AATS Daily News C WF WO MEN 917 MEN P UB LIC P HO NE S ME N 617 517 Kapp Surgical 512 512Instrument 817 717 1016 COFFEE 813 511 611 711 709 508 810 808 811 809 910 909 1008 907 1006 908 Admedus DO WN UP 706 505 E XIT 604 605 704 705 804 805 904 COFFEE 501 600 601 603 700 ENTRANCE P UB LIC P HO NE S 504 2310 S Miami Blvd., Suite 240, Durham, NC 27703 www.aemedical.com Abbott Vascular Acelity (KCI) 1325 12930 IH 10 W., San Antonio, TX 78249 www.acelity.com A&E Medical products include MYO/ Wire® temporary pacing wires, MYO/Wire II sternum wires, MYO/Punch rotating surgical punch, MYO/Lead disposable patient cable and DoubleWire high strength sternal closure system. 511 3200 Lakeside Drive, Santa Clara, CA 95054 www.abbottvascular.com MitraClip is the world’s first transcatheter mitral valve repair therapy available, providing an option for select patients with degenerative mitral regurgitation. 1105 1005 1104 1213 1312 1313 1211 1310 1311 1209 1308 1309 1207 1306 1307 1205 1304 1305 504 C OATS A & E Medical Corporation 1325 THE ATER # 2 G AT E 9 E XIT 1225 1324 S TAGE 523 1327 C OFFEE S HOW MAN AG EMENT O FF IC E 1227 1326 Acelity provides a trusted and complementary portfolio of advanced wound therapeutics and regenerative medicine from KCI, LifeCell and Systagenix. Acute Innovations 21421 NW Jacobson Road, Suite 700, Hillsboro, OR 97124 www.acuteinnovations.com 1017 Furthering their reputation as a leader in the thoracic industry, ACUTE Innovations® continues to make advancements in chest-wall stabilization technology. Stop by our training booth #1017 to learn about ACUTE’s NEW and exciting cutting-edge products: the RibLoc® U Plus Chest Wall ENTRANCE P UB LIC P HO NE S F Plating System and the AcuTie® II Sternum Closure System. Admedus 1105 8400 Normandale Lake Blvd, Suite 920, Minneapolis, MN, 55437 www.admedus.com Admedus, a global healthcare group, is working with renowned medical leaders to bring new medical technologies to market. CardioCel®, a cardiovascular scaffold, is the first of our ADAPT® tissue engineered bio-implants and is being used by surgeons to repair simple and complex cardiac defects. Advanced Cardiothoracic Consultants, LLC 1310 12155 Golden Bluff Court, Indianapolis, IN 46236 www.actc4solutions.com 1200 1201 1300 1301 1400 1303 F U P TO 5 Utilizing over 40 years of clinical expertise in cardiothoracic, thoracic transplant/ organ replacement, and advanced heart failure ACTC can evaluate financial and clinical aspects for programs to increase efficiencies. Whether a new or well established program, hospital, or insurer let ACTC assist you in maintaining financial viability and sustaining growth in today’s challenging healthcare market. AtriCure, Inc. 817 6217 Central Park Drive, West Chester, OH 45069 www.atricure.com AtriCure is intent on reducing the global Afib epidemic and healing the lives of those affected through clinical science, education and innovation. We are a leading Afib solu- A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER tions partner with the only FDA-approved surgical treatment for Afib and most widely implanted occlusion device for left atrial appendage management. Bard Davol 617 100 Crossings Boulevard, Warwick, RI 02886 www.davol.com BARD is the market leader in comprehensive soft tissue reconstruction. In addition to this extensive suite of products, or BioSurgery franchise is delivering a growing line of sealants and hemostatic products to complement surgical techniques across thoracic, cardiovascular, and other surgical specialties. BFW, Inc. 917 2307 River Road, #103, Louisville, KY 40206 www.bfwinc.com Surgical headlight innovation is BFW. From its new Ambrose™ and Montauk™ portable LED systems, to introducing solid-state plasma fiber-optic illumination, to pioneering coaxial High-Definition headlight video imaging, BFW’s universal reputation for quality, personalized service and hi-tech leadership is second to none. Biomet Microfixation 804 1520 Tradeport Drive, Jacksonville, FL 32218 www.biomet.com/microfixation Biomet Microfixation is a leading global healthcare provider of orthopedic products. Our thoracic portfolio includes the Pectus Bar for repair of Pectus Excavatum and the SternaLock Blu Primary Closure System for sternal closure. The Blu System aligns and stabilizes the sternum after sternotomy and enables easier closure after minimally invasive access. Bolton Medical Inc. 1213 799 International Pkwy, Sunrise, FL 33325 www.boltonmedical.com Bolton Medical is a subsidiary of the WerfenLife Company. WerfenLife is an international company that manufactures and distributes medical diagnostic solutions and medical devices worldwide. Bolton Medical sells endovascular therapies for thoracic repair, such as Relay Thoracic Stent-Graft in both U.S. and International markets and Relay NBS (non-bare stent) in International markets. CardiacAssist, Inc. 1207 240 Alpha Drive, Pittsburgh, PA 15238 www.cardiacassist.com CardiacAssist, inventor of the TandemHeart® Extracorporeal Circulatory Support System, offers versatile MCS treatment options. While we’re best known for our Left Ventricular Support platform, we recently launched a line of Arterial Cannulae, and the PROTEK Duo™ Veno-Venous dual lumen cannula. Stop by our booth to learn more. Cardiovascular Research Foundation 111 East 59th Street, 11th floor New York, NY 10022-1202 www.crf.org 142 CRF is a global leader at the forefront of today’s treatments and technologies in the fight against heart disease. Since its inception in 1991, CRF has played a pivotal role in advancing the understanding and treatment of cardiovascular disease, realizing dramatic improvements by establishing the safe use of new technologies, drugs, and therapies in the field of interventional cardiovascular procedures. ClearFlow, Inc. 809 1630 S. Sunkist St., Suite E, Anaheim, CA 92806 www.clearflow.com The PleuraFlow® Active Clearance Technology™ System from ClearFlow, Inc. offers a safe way to proactively prevent clot from accumulating in a completely sterile system, thus minimizing Retained Blood Syndrome (RBS) complications that can result from ineffective evacuation of blood after surgery. New! Distributed in the US by Maquet Medical Systems. Cormatrix Cardiovascular, Inc. 1327 1100 Old Ellis Road, Roswell, GA 30076 www.cormatrix.com CorMatrix® Cardiovascular markets its ECM® Bioscaffold devices for vascular repair, pericardial repair and reconstruction, cardiac tissue repair, and CanGaroo ECM Envelope and is currently conducting preclinical studies to evaluate future applications in other cardio and vascular applications. Covidien 1123 555 Long Wharf Drive, New Haven, CT 06511 Covidien is a leading global healthcare products company that creates innovative medical solutions for better patient outcomes and delivers value through clinical leadership and excellence. Please visit www. covidien.com/surgical to learn more. CRC Press - Taylor & Francis Group LLC 1106 6000 Broken Sound Parkway NW., Suite 300, Boca Raton, FL 33487 www.crcpress.com CRC Press – Taylor & Francis Group is a global publisher of print and electronic books for medical, scientific and technical communities. Visit our booth to browse our new and bestselling publications in cardiothoracic surgery and take advantage of convention discounts. Register for email alerts at www.crcpress.com. CryoLife, Inc. 523 1655 Roberts Blvd NW., Kennesaw, GA 30144 www.cryolife.com CryoLife® is one of the world’s leading contemporary medical device companies providing preserved human cardiac and vascular tissues, surgical adhesives and sealants, and cardiac lasers for treatment of refractory angina. CryoLife® is committed to partnering with academic training programs and cardiac surgical societies and associations through their new Thoracic Surgery Education Reform Initiative. • AATS 95TH ANNUAL MEETING 11 S EATTLE , WA CTSNet 140 633 N. St Clair, Chicago, IL www.ctsnet.org CTSNet (www.ctsnet.org), headquartered in Chicago, Illinois, USA, is the leading international source of online resources related to cardiothoracic surgery, as well as the major hub of the international online community of cardiothoracic surgeons and allied health care professionals. CureVentions 1312 595 N. Dobson Rd Suite B-32 Chandler, AZ 85224 www.cureventions.com. Cure Ventions’ Sternal Vest is the only compression vest designed specifically to meet the needs of the cardiothoracic heart patient. For more than a decade, we have consistently delivered a superior quality product with unsurpassed results--maintaining incision stability, reducing pain, improving respiration, and quicker mobilization. With improved patient comfort, prescribed therapies are more likely to be followed. Nurses and surgeons attest to the significant improvement Cure Ventions’ Sternal Vest makes in patients recovery. De Soutter Medical USA 1324 224 Rolling Hill Road, Suite 12A, Mooresville, NC 28117 www.de-soutter.com DeSoutter Medical is a world leader in orthopedic power tools. The Sternudrive Cardiothoracic saw has a unique active damping system that reduces vibration by 30%. Lithium Ion sterile battery technology assures a class leading power to weight ratio and a wrench less micro adjustable blade guard provides optimum control. Designs For Vision, Inc. 431 760 Koehler Avenue, Ronkonkoma, NY, 11779 www.designsforvision.com Just Se It™ with Designs for Vision’s lightweight custom-made surgical Telescopes - See It Even Better™ with the L.E.D. Daylite® or Twin Beam®, L.E.D. Daylite® providing the brightest and safest un-tethered illumination. Introducing the L.E.D. Daylite® Nano Cam HD video from your prospective. EACTS 128 EACTS House, Madeira Walk Windsor, SL4 1EU, United Kingdom www.eacts.org EACTS is the largest European Association devoted to the practice of Cardio-thoracic surgery. The main objective of the Association is to advance education in the field of cardio-thoracic surgery and to promote, for the public benefit, research into cardiovascular and thoracic physiology and therapy and to correlate and disseminate the useful results thereof. Visit booth 124 for information on: membership, future meetings and all activities of EACTS. Journals: EJCTS (European Journal of Cardio-Thoracic Surgery) ICVTS (Interactive Cardiovascular and Thoracic Surgery) and MMCTS (Multimedia Manual of Cardiothoracic Surgery). Edwards Lifesciences 737 One Edwards Way, Irvine, CA 92614 www.edwards.com Edwards Lifesciences is the global leader in the science of heart valves and hemodynamic monitoring. Driven by a passion to help patients, the company partners with clinicians to develop innovative technologies in the areas of structural heart disease and critical care monitoring, enabling them to save and enhance lives. Additional company information can be found at www. edwards.com. Elsevier Inc. 508 1600 JFK Blvd., Ste 1800, Philadelphia, PA 19103 www.elsevierclinicalsolutions.com ELSEVIER is a leading publisher of health science publications, advancing medicine by delivering superior reference information and decision support tools to doctors, nurses, health practitioners and students. With an extensive media spectrum — print, online and handheld, we are able to supply the information you need in the most convenient format. Enova Illumination 1326 1839 Buerkle Road, St. Paul, MN 55110 http://www.enovaillumination.com Introducing Enova’s newest and brightest LED surgical headlight, model XLT-225. It is designed for deep cavity surgery and is the brightest LED surgical headlight in the world!5 year warranty on LED. Made in USA since 2005. ESTS 144 1 The Quadrant, Exeter, Devon, ex2 4le, United Kingdom www.ests.org ESTS is the largest international general thoracic surgery organization with over 1350 members from all Continents. Our mission is to improve quality in our specialty: from clinical and surgical management of patients to education, training and credentialing of thoracic surgeons worldwide. ETHICON 904 190 Lexington Road, Glastonbury, CT 06033 www.ethicon.com Ethicon US LLC , a Johnson & Johnson company, commercializes a broad range of innovative surgical products, solutions and technologies used to treat some of today’s most prevalent medical issues, such as: colorectal and thoracic conditions, women’s health conditions, hernias, cancer and obesity. Learn more at www.ethicon.com, or follow us on Twitter @Ethicon. Fehling Instruments GmbH & Co. KG Hanauer Landstr. 7A, 63791, Karlstein, Germany www.fehlingsurgical.com 331 FEHLING SURGICAL INSTRUMENTS features Minimally Invasive Valve Sets including NEW Retractor designs for unmatched Atrial Exposure. Stop by and take our new MICS Simultator for a spin Continued on page 12 12 AATS 95TH ANNUAL MEETING Continued from page 11 to refine your manual/tactile skills on a “Dummy”! CERAMO® surface means high efficiency through enhanced performace, increased endurance and minimal maintenance. G & N Medical 1308 Maydwell Ave, Off Stane St., Horsham, United Kingdom www.gandn.com G+N Medical is a British medical device company which was established in 1974 originally selling laboratory consumables. Today they are the UK market leaders in DVT prevention and have a range of specialist cardiothoracic products. G+N is an independent company which is proud to supply the highest quality, best value products to customers around the world. Genesee BioMedical, Inc. 711 700 West Mississippi Avenue, Denver, CO 80223-3408 www.geneseebiomedical.com Design Beyond Standard. Genesee BioMedical, Inc. provides unique devices for cardiothoracic surgery including sternal/ thoracic valve retractors for adult, adult congenital and pediatric cardiac surgery, instruments for MICS, coronary graft markers, suture guards, retraction clips and aortic valve repair. Now available “PHOTOFIX” Bovine Pericardial Patch. Denver, CO USA www.geneseebiomedical.com. Gore & Associates, Inc. 1008 1505 N. Fourth Street, Flagstaff, AZ 86004 www.goremedical.com At Gore, we have provided creative therapeutic solutions to complex medical problems for more than 35 years. During that time, more than 35 million innovative Gore Medical Devices have been implanted, saving and improving the quality of lives worldwide. Our extensive family of products includes vascular grafts, endovascular and interventional devices, surgical meshes for hernia and soft tissue reconstruction, staple line reinforcement materials, and sutures for use in vascular, cardiac, and general surgery. We are one of a select few companies to appear on all of the US “100 Best Companies to Work For” lists since the rankings debuted in 1984. For more information, visit www.goremedical.com. Hawaiian Moon 1313 321 S. Missouri Ave., Clearwater, FL 33756 Heart Hugger/Gen’l Cardiac Technology 704 6489 Comden Ave. #106, San Jose, CA 95120 www.hearthugger.com Heart Valve Society 132 500 Cummings Center, Suite 4550, Beverly, MA 01915 www.HeartValveSociety.org An International Heart Team. Leaders in Evaluation, Management and Research. HeartWare, Inc 910 500 Old Connecticut Path, Framingham, MA 01701 www.heartware.com A PRIL 25-29, 2015 HeartWare is dedicated to delivering safe, high-performing and transformative therapies that enable patients with heart failure to get back to life. The company’s breakthrough innovations begin with the HVAD® Pump, designed to be implanted in the pericardial space avoiding the more invasive surgical procedures required with older LVAD technologies. The HVAD Pump is commercially available around the world. Integrated Sensing Systems 1205 391 Airport Industrail Dr., Ypsilanti, MI 48198 www.mems-issys.com Integrated Sensing Systems, Inc. (ISS) is a technology company that has built and maintained a state of the art manufacturing facility that supplies innovative MEMS based solutions to each of its independent business units to empower the business units to deliver breakthrough products that are focused on both large and emerging markets. International BioPhysics Corporation 1110 2101 E. Elmo St. Suite 275, Austin, TX 78744 www.biophysicscorp.com SternaSafe is an active adjustable stability sternum support brace (patents pending) which give patients hand-free mobility. The SternaSafe is made from comfortable, soft, breathing materials developed for sternotomy patients. The brace is worn by the patient after their sternotomy operation. The SternaSafe can be worn during their hospital stay and subsequently at home. The average use time at home is 21 days. International Society of Minimally Invasive Cardiac Surgery 1311 500 Cummings Center, Suite 4550, Beverly, MA 01915 www.ismics.org ISMICS: Innovation, Technologies, and Techniques in Cardiothoracic and Cardiovascular/Vascular Surgery. 2015 ISMICS Annual Scientific Meeting, 3-6 June 2015, InterContinental Hotel, Berlin, Germany www.ismics.org. Intuitive Surgical, Inc. 723 • W ASHINGTON S TATE C ONVENTION C ENTER Kapp Surgical Instrument Inc. 512 4919 Warrensville Center Road, Cleveland, Ohio 44128 www.kappsurgical.com Kapp Surgical is a custom design shop which designs surgical instruments and implants, manufactures them, and sells as well as distributes domestically and internationally. Kapp’s exclusive products are: The Cosgrove Heart Retractor, Strip T’s surgical organizer, and countless surgical devices all FDA approved with several pending approvals. Karl Storz EndoscopyAmerica, Inc. 604 2151 E. Grand Ave., Suite 100, El Segundo, CA 90245 www.karlstorz.com KARL STORZ, a leader in endoscopic technologies for over 70 years, offers solutions for video-assisted thoracic surgery. Among our mediastinoscopy products is the SLIM Distending Mediastinoscope, an ideal solution for advanced procedures at the mediastinum. Our EndoCAMeleon® Laparoscope enables surgeons to adjust the scope’s viewing direction from 0° to 120°. KLS Martin, LP 705 PO Box 16369, Jacksonville, FL 32245 www.klsmartinnorthamerica.com KLS-Martin, a responsive company, is focused on the development of innovative products for oral, plastic and craniomaxillofacial surgery. New product developments in our titanium osteosynthesis plating systems allow these products to be used for rapid sternal fixation and reconstruction. Lara Tape Labs, LLC 1211 8777 N. Gainey Center Drive, Suite 136, Scottsdale, AZ 85258 www.laratapelabs.com Lara Tape Labs is a designer and manufacturer of high performance expanded PTFE films and membranes designed to solve medical applications. LifeNet Health 810 1864 Concert Dr. Virginia Beach, VA 23453 www.lifenethealth.org Intuitive Surgical is the global leader in minimally invasive, robotic-assisted surgery. Its da Vinci® Surgical System – with a 3D-HD vision system and EndoWrist® instrumentation – enables surgeons to offer a minimally invasive approach for a range of complex procedures. da Vinci is used in more than 2,500 hospitals around the world. LifeNet Health helps save lives, restore health, and give hope to thousands of patients each year. We are the world’s most trusted provider of transplant solutions, from organ procurement to new innovations in bio-implant technologies and cellular therapies—a leader in the field of regenerative medicine, while always honoring the donors and healthcare professionals that allow the healing process. JACE Medical LoupeCam by VizVOCUS inc. 1020 Kifer Road Sunnyvale, CA 94086 www.intuitivesurgical.com 1104 17020 Duck Lane, Haymarket, VA 20169 www.jacemed.com JACE is a medical device development company pioneering a fully integrated, re-sequencing technology + application for sternal resection and closure. We innovate with an eye toward providing definitive benefits across the entire five-sided healthcare spectrum of Patient, Physician, Provider, Payer and Regulator. 1225 10245 E. Via Linda Blvd, Suite 210, Scottsdale, AZ 85258 www.loupecam.com The ProHD LoupeCam® takes visualization and HD video recording to a complete different level. This nickel-size camera, with only 0.4 oz, offers a 3.0 MP sensor, a builtin microphone and HD video recording 1280x720p directly to your laptop with full Mac or Windows options. Mounting adapters available for all loupes models. • S EATTLE , WA The Bluetooth Footpedals ensure a complete hands-free experience. www.LoupeCam.com LSI Solutions 1111 7796 Victor-Mendon Rd., Victor NY 14564 www.lsisolutions.com COR-KNOT® delivers instant security with automated knot placement and integrated suture trimming in one easy step. COR-KNOT® may reduce cardiopulmonary bypass and cross-clamp time in your OR. Visit LSI SOLUTIONS® at booth 1111 to learn more. Magic Masseuse 1304 8056 17th Ave NE, Seattle, WA 98115 www.magicmasseuse.com You have to try it, to believe it. Aching back, neck pain, sore hips, knee or ankle pain, sciatica, headaches, fibromyalgia, blood circulation, plantar fascitis, arthritis, tennis elbow. Instant pain relief. Same professional treatment you would get at the doctor or chiropractor office. Easy to use, safe and effective. Mallinckrodt Pharmaceuticals 601 12481 High Bluff Drive #200, San Diego, CA 92130 www.mallinckrodt.com Mallinckrodt is a global specialty biopharmaceutical and medical imaging business that develops, manufactures, markets and distributes specialty pharmaceutical products and medical imaging agents. Mallinckrodt is an industry leader in intravenous analgesia for acute pain management. Visit www.mallinckrodt.com to learn more. MAQUET Medical Systems, USA 337 45 Barbour Pond Road, Wayne, NJ 7470 www.maquet.com MAQUET Medical Systems is a market leader focused on improving patient care and quality of life. We offer a comprehensive portfolio of innovative products designed to meet the needs of clinical professionals in the areas of: advanced hemodynamic monitoring, cardiothoracic and vascular surgery, thoracic drainage, cardiac intervention, perfusion, anesthesia and ventilation. MED Alliance Solutions, LLC 717 3825 Commerce Drive, St. Charles, IL 60174 www.medalliancesolutions.com ISO 13485 certified medical device distributor committed to providing high quality specialty devices for cardiothoracic surgery worldwide. Exclusive US distributor of French instruments manufacturer Delacroix-Chevalier and partner of Michigan based Surge Cardiovascular for open heart surgical products. Medela, Inc. 1011 1101 Corporate Drive, McHenry, IL 60050 www.medela.com Medela concentrates on two divisions: “Breastfeeding”, leading in the development and production of breastfeeding products, and “Healthcare”, engineering and manufacturing highly innovative medical vacuum technology solutions. Medela has 18 subsidiaries, distributes its products in over 90 countries, and employs 1,500 staff worldwide. A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER Medistim 517 14000 25th Ave. N. Ste. 108, Plymouth, MN 55447 www.medistim.com Medistim is the standard of care in the operating room. With the unique combination of transit time flow measurement (TTFM) and high frequency ultrasound imaging guidance to help reduce and minimize the risk of negative postoperative outcomes, Medistim’s quality assessment technology offers surgeons quantifiable validation and guidance during cardiovascular, vascular, transplantation and neurosurgery. Medtronic, Inc. 537 710 Medtronic Parkway MS-LS290, Minneapolis, MN 55432 www.medtronic.com 602 PO Box 1378, Bellaire, TX, 77402 www.microsurgeryusa.com 1227 2207-33 Wood Street, Toronto, ON M4Y 2P8, Canada www.mtmedi.com We offer Exceptional Spring Style and Double Action Titanium Scissors, Forceps and Needle Holders with Tungsten Carbide Inserts for Thoracic and Cardan Surgery. We guarantee 20,000 cuts for our Titanium Scissors and 5 years warranty for Titanium Forceps and Titanium Needle Holders with excellent grasping. Free of charge Trial available. Myriad Genetic Laboratories 611 320 Wakara Way, Salt Lake City, UT 84108 www.myriad.com Myriad Genetics is a leading molecular diagnostic company dedicated to making a difference in patients’ lives through the discovery and commercialization of transformative tests to assess a person’s risk of developing disease, guide treatment decisions and assess risk of disease progression and recurrence. Myriad’s portfolio of molecular diagnostic tests are based on an understanding of the role genes play in human disease and were developed with a commitment to improving an individual’s decision making process for monitoring and treating disease. Myriad is focused on 811 7700 Equitable Drive, Suite 206, Eden Prairie, MN 55344, USA www.neochord.com NeoChord, a U.S.A. medical device company, has developed a new minimally invasive technology that enables beating heart, sternal sparing implantation of artificial chord tendinae, for the treatment of degenerative mitral valve regurgitation. CE mark was obtained in December, 2012, and more than 200 patients have been treated to date. 730 1300 E. Anderson Lane, Bldg. B, Austin, TX 78752 www.onxlti.com On-X® Life Technologies, Inc., Product Description On-X® Heart Valves: Patented natural design and On-X® Carbon offer reduced turbulence in a mechanical valve to rival the clinical and hemodynamic performance of bioprostheses. FDA IDE approved PROACT (Prospective Randomized On-X® Anticoagulation Clinical Trial) is in process. Chord-X PTFE suture is available for mitral valve repair. Orascoptic Microsurgery Instruments is one of the leading suppliers of surgical instruments and loupes. Our instruments include: titanium scissors, needle holders, and debakey forceps. Our Super-Cut scissors are the sharpest in the market, and our newly designed surgical loupes offer up to 130mm field of view, and up to 11x magnification. MT Medi Corp. NeoChord, Inc. On-X Life Technologies, Inc. At Medtronic, we’re committed to Innovating for life by pushing the boundaries of medical technology and changing the way the world treats chronic disease. Medtronic’s breadth of solutions in structural heart and aortic disease management includes: tissue, mechanical and transcatheter valves; irrigated RF and cryo surgical ablation devices; aortic stent graft systems; and OPCAB, MICS CABG, cannulae and perfusion products. Microsurgery Instruments, Inc. strategic directives to introduce new products, including companion diagnostics, as well as expanding internationally. 709 3225 Deming Way #190, Middleton, WI 53562 www.orascoptic.com Orascoptic has been designing and manufacturing award-winning loupes, lights and operator chairs for surgeons, dentists and hygienists for more than 30 years. The Orascoptic focus is superior visualization coupled with oprimal clinical ergonomics. We are recognized as the inovators in the market, being the first company to bring you a portable LED light, the first loupe with a built-in cable-less headlight, and the first loupe with adjustable magnification (zoo) power. Otto Trading, Inc. 1209 1921 Carengie Ave Suite C., Santa Ana, CA 92705 Manufacturer and distributor of hand-held portable digital massager, TENS unit Oxford University Press 808 198 Madison Ave., New York, NY 10016 Peters Surgical 831 42, Rue Benoit Frachon, Bobigny cedex, 93000, France • AATS 95TH ANNUAL MEETING 13 S EATTLE , WA Therapy Systems Together we make the difference in minimally invasive treatment to improve patient outcomes and save lives. With our Live Image Guidance and Data Integration Solutions we aim to remove barriers to safer, more effective, and more reproducible treatments, delivering relevant clinical value where it’s needed most - at the point of patient treatment. and stainless steel precision instruments including: VATS/MIS thoracoscopic instruments, Scanlan® SUPER CUT™ Scissors, and Scanlan® LEGACY titanium needle holders and forceps. Single-use products include Aorta/Vein Punches, VASCU-STATT® bulldog clamps and graft markers. Qualiteam s.r.l. 51 Valley Stream Parkway, Malvern, PA 19355 www.healthcare.siemens.com 1016 Casale Nassio Sopra 15A, Chiaverano, TO, 10010, Italy www.qualiteam.com Founded by a nurse Qualiteam focuses 100% on advancing recovery through prevention of complications after surgery (infections, dehiscence, pain, respiratory issues). Our unique wound support products are patented, FDA-cleared and reimbursable. The high performance is clinically proven in even the worst, post-surgery scenarios. Visit our booth for details. Quest Medical Inc. 909 One Allentown Pkwy., Allen, TX 75002 www.questmedical.com Quest Medical, Inc. is a medical device manufacturer and worldwide distributor specializing in protecting the heart during cardiac surgery with the Quest MPS 2® and Microplegia. Quest also offers a unique variety of aortic punches, safety valves, vascular loops, and an anesthesia line designed for optimum cardiovascular surgery. Rose Micro Solutions 1306 4105 Seneca Street, West Seneca, NY 14224 www.rosemicrosolutions.com Rose Micro Solutions sells High Quality Optical Loupes & LED Lights for Less! Our Loupes start @ $279.00. We are a “Family” Business consisting of 4 Brothers. We named the company after our mother “ROSE”. Stop by Booth # 1307 to see for yourself! RTI Surgical Inc. 805 11801 Research Circle, Alachua, FL 32615 www.rtisurgical.com RTI Surgical™ is a leading global surgical implant company providing surgeons with safe biologic, metal and synthetic implants. Committed to delivering a higher standard, RTI’s implants are used in sports medicine, general surgery, spine, orthopedic, trauma and cardiothoracic procedures and are distributed in nearly 50 countries. Rultract/Pemco Inc. 700 5663 Brecksville Road, Cleveland, OH 441311593 Péters Surgical develops, manufactures and distributes high-end medical devices worldwide. Vitalitec, the US subsidiary, will be highlighting the CYGNET® flexible clamp, Enclose II™ anastomosis assist device and our Péters Surgical® CVT sutures. We will also proudly display the Geister® brand instrumentation that we distribute in the US. PemcoMedical LLC is an international distribution company located in Cleveland, Ohio that focuses on the design and manufacturing of precision Cardiovascular surgical instruments. Currently we represent Pemco Inc., the Rultract “Skyhook” and Sontec Instrument Company. Philips Healthcare One Scanlan Plaza, St. Paul, MN 55107 www.scanlaninternational.com 1023 22100 Bothell-Everett Highway, Bothell, WA 98021 www.usa.philips.com/healthcare Philips Healthcare – Image Guided Scanlan International, Inc. 333 Highest quality surgical products designed and manufactured by the Scanlan family since 1921. Over 3000 titanium Siemens Healthcare 1117 Siemens Healthcare helps providers meet clinical, operational and financial challenges. A global leader in medical imaging, laboratory diagnostics and IT, we understand the entire care continuum—from prevention and early detection to diagnosis and treatment. For more: usa.siemens. com/healthcare Sontec Instruments Inc. 505 7248 South Tucson Way, Centennial, CO, 80112 www.sontecinstruments.com Sontec offers a comprehensive selection of exceptional hand held surgical instruments, headlights and loupes available to the discriminating surgeon. There is no substitute for quality, expertise and individualized service. Sontec’s vast array awaits your consideration at our booth. Sorin Group 343 14401 W. 65th Way, Arvada, CO 80004 www.sorin.com Solo Smart Aortic Pericardial Tissue Valve The Solo Smart aortic pericardial tissue valve is 100% pure tissue – free of stents, suture rings and obstructions to blood flow. Solo Smart has no synthetic material and provides native-like performance. Memo 3D ReChord Annuloplasty Ring With dynamic cell structure allowing true physiological 3D motion, Memo 3D ReChord truly reflects the native mitral annulus. The addition of our innovative cordal guide system makes artificial chordae replacement a more standardized procedure. Spiration, Inc. 1005 6675 185th Ave NE, Redmond, WA 98052 www.olympusrespiratory.com The Spiration® Valve System has a humanitarian device approval in the U.S. to control specific post-operative air leaks of the lung and has CE mark approval for the treatment of diseased lung in emphysematous patients and for damaged lung resulting in air leaks by limiting air flow to selected areas. St. Jude Medical, Inc. 931 6300 Bee Caves Rd., Austin, TX 78746 St. Jude Medical is dedicated to transforming the treatment of some of the world’s most expensive epidemic diseases by creating cost-effective medical technologies that save and improve lives of patients around the world. Continued on page 14 14 AATS 95TH ANNUAL MEETING Continued from page 13 Stroke Prevention Systems 1200 27 Hoku Place, Paia, Maui, HI 96779 The Stroke Prevention System (SPS™) is a patented technology based on external carotid compression, creation of a pressure gradient and deflection of cerebral emboli. It is performed on demand when generation of cerebral emboli is anticipated. The SPS™ device has been used successfully in patients undergoing heart surgery. STS 134 633 N. St Clair, Chicago, IL 60611 www.sts.org The Society of Thoracic Surgeons represents more than 6,900 cardiothoracic surgeons, researchers, and allied health care professionals worldwide who are dedicated to ensuring the best surgical care for patients with diseases of the heart, lungs, and other organs in the chest. The Society offers a wide variety of member benefits, including reduced participation fees in the renowned STS National Database, a complimentary subscription to The Annals of Thoracic Surgery, clinical practice guidelines, dynamic educational offerings, online patient information resources, and much more. Stop by booth #134 or visit www.sts.org to learn more. STS Advocacy Center 136 20 F. St. NW, Washington, DC 20001 www.sts.org Stop by STS Advocacy Center booth #136 where you can receive timely information on federal legislative and regulatory initiatives impacting the specialty, obtain tools to engage members of Congress, and become a Key Contact for government affairs issues in your district. STS members can also contribute to STS-PAC and support champions of cardiothoracic surgery in Congress. Surgitel/General Scientific Corp 907 77 Enterprise Drive, Ann Arbor, MI 48103 www.surgitel.com A PRIL 25-29, 2015 loupes and headlights sold around the world from their headquarters in Ann Arbor, Michigan. Holding a variety of patents, SurgiTel is always on the forefront of Vision and Ergonomics. SynCardia Systems, Inc. 605 1992 E Silverlake Drive, Tucson, AZ 85713 www.syncardia.com The SynCardia temporary Total Artificial Heart (TAH-t) is the world’s only FDA, Health Canada and CE approved Total Artificial Heart. It is approved as a bridge to transplant for patients dying from end-stage biventricular failure. Visit our booth for updates on the Freedom® portable driver, 50cc TAH-t, and destination therapy. Terumo Cardiovascular Group 531 6200 Jackson Road, Ann Arbor, MI 48103 www.terumo-cvs.com Vascutek, a Terumo company, will display Gelweave™ gelatin-sealed, woven and branched vascular grafts. The Vascutek CE-marked Thoraflex™ Hybrid device will also be featured (Not cleared for sale in the USA). Terumo will display the VirtuoSaph® Plus Endoscoipc Vessel Harvesting System, Beating Heart and Surgical Stabilization products for cardiothoracic procedures, and Terumo® Perfusion Products. Thompson Surgical Instruments, Inc. 600 10170 East Cherry Bend Road, Traverse City, MI 49684 www.thompsonsurgical.com Thompson Surgical is a leader in exposure and the original manufacturer of the table-mounted Thompson Retractor. In cardiovascular surgery, surgeons will benefit from the Thompson Surgical Bolling Retractor. The Bolling Retractor provides extremely low profile, stable, and Uncompromised Exposure of the heart structures for valve procedures. SurgiTel is the manufacturer of premium • W ASHINGTON S TATE C ONVENTION C ENTER Thoracic Surgery Foundation for Research and Education 1309 633 N. St Clair, Chicago, IL 60611 www.tsfre.org TSFRE was established in 1988 as a 501c(3) not-for-profit charitable organization by the four leading thoracic surgery societies: AATS, STS, STSA, and WTSA. TSFRE’s mission is to foster the development of surgeon scientists in cardiothoracic surgery; increasing knowledge and innovation to benefit patient care. Thoramet Surgical Products Thoratec Corporation 520 6035 Stoneridge Drive, Pleasanton, CA 94588 www.thoratec.com Thoratec is the world leader in mechanical circulatory support with the broadest product portfolio to treat the full range of clinical needs for patients suffering from advanced heart failure. The company’s products include the HeartMate LVAS and Thoratec VAD, with more than 20,000 devices implanted in patients suffering from heart failure. Transonic Systems Inc. 706 34 Dutch Mill Rd., Ithaca, NY 14850 www.transonic.com Transonic’s new ELSA® Extracorporeal Life Assurance Monitor provides novel quantification of recirculation in VV-ECMO, oxygenator blood volume for VA/VV ECMO as well as Transonic’s gold standard flow measurement for CPB. Vitalcor, Inc. 516 100 E. Chestnut Avenue, Westmont, IL 60559 www.vitalcor.com Latex Free Coronary Artery Balloon Cannulae with self-inflating Balloon (3-year shelf life). Reusable Dingo (Bulldog) Clamp. Titanium and stainless steel specialty instruments and retractors. Reusable stabilizer for Beating Heart AATS Annual Meeting Welcome Reception On Sunday evening, the AATS Welcome Reception helped launch the 95th Annual Meeting and provided meeting attendees with the opportunity to greet their colleagues and visit with industry partners in a convivial environment. 1006 301 Route 17 N, Suite 800, Rutherford, NJ 7070 www.thoramet.net • S EATTLE , WA Surgery and Mitral Valve Retractor. Wexler Surgical 919 11333 Chimney Rock Road Suite #110, Houston, TX 77035 www.wexlersurgical.com Wexler Surgical designs and manufactures a variety of titanium and stainless steel specialty surgical instruments and products for Cardiac, Vascular, Thoracic, and Micro Surgery. Come see our VATS/MICS instruments and ask about our Optimus Series. Visit us online at www.wexlersurgical.com for more information about our products and the services. Wolters Kluwer Health 501 2001 Market Street, Philadelphia, PA 19103 www.wolterskluwer.com Wolters Kluwer is a leading publisher of medical, health and science publications. We offer an extensive selection of medical books, journals, and electronic media for doctors, nurses, specialized clinicians and students. Please visit booth 501 to browse our comprehensive product line. WSPCHS 908 2300 Tupper Street Room C8-29, Montreal, QC, H3H 1P3, Canada The mission of the World Society for Pediatric and Congenital Heart Surgery is to promote the highest quality comprehensive cardiac care to all patients with congenital heart disease, from the fetus to the adult, regardless of the patient’s economic means, with an emphasis on excellence in teaching, research and community service. ZipperBelt.com 1305 3419 Westminster #276, Dallas, TX 75205 The zipper belt Brace was developed for patients who are now zipper club members. Transient events such as coughing or sneezing or even pushing up from a chair can be very painful. The zipper belt is a brace that the patient can wear and at a moments notice can get relief from a violent sneeze or cough instead of just squeezing a pillow. Future AATS Annual Meetings AATS 96th Annual Meeting May 14 - 18, 2016 Baltimore Convention Center Baltimore AATS Centennial “Celebrating 100 Years of Modelling Excellence” April 29 – May 3, 2017 Boston Hynes Convention Center Boston AATS 98th Annual Meeting April 28 – May 2, 2018 San Diego Convention Center San Diego A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER Awards: Lifetime and Scientific Timothy J. Gardner, MD received the 2015 AATS Lifetime Achievement Award from G. Alec Patterson, MD, during Monday’s plenary session. Dr. Gardner was honored for his leadership, commitment, and lifelong contributions to the cardiothoracic surgery specialty. James L. Cox, MD received the 2015 AATS Scientific Achievement Award from G. Alexander Patterson during Monday’s plenary session. Dr. Cox was recognized for his scientific contributions to the field of CT surgery, including his pioneering work in atrial fibrillation, his leadership at the World Heart Foundation, and his mentorship in leading numerous trainees to scientific discoveries. AATS ANNUAL MEETING 2016 • S EATTLE , WA AATS 95TH ANNUAL MEETING 15 “Every Heartbeat Matters” David J. Sugarbaker, MD, thanked Edwards Lifesciences for their continued partnership with AATS in the Every Heartbeat Matters initiative. “With the support provided by the Edwards Lifesciences Foundation we were able to add two new programs to the Graham Foundation portfolio as we strive to fulfill our mission of Driving, Leadership, Learning, and Innovation in the pursuit of excellence.” The first new program is the Every Heartbeat Matters Valve Fellowship which aims to enhance the skills of cardiothoracic surgeons so that they can better treat underserved populations at their home institution. To do this, successful applicants will spend up to three months visiting a host institution for advanced valvular heart disease training to acquire skills that can be clinically implemented in their daily practice. The second new program is the 2015 AATS Cardiovascular Valve Symposium which will be taking place November 20-21 in Sao Paulo, Brazil. This meeting was a perfect complement to the Fellowship program as it allows the AATS to visit an area of need and provide educational programming which will reach hundreds of practicing surgeons and ultimately thousands of underserved patients. PRESIDENT & ANNUAL MEETING CHAIR Joseph S. Coselli ANNUAL MEETING CO-CHAIRS Charles D. Fraser David R. Jones May 14 – 18, 2016 Baltimore Convention Center Baltimore, MD, USA www.aats.org 16 AATS 95TH ANNUAL MEETING H A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA Exploring Improvements in Perioperative Care emodialysis patients are at added risk of complications and mortality from cardiac surgery, compared with patients not on dialysis. A modified perioperative management plan can improve early outcomes, compared with standard methods in these patients, according to Hiroyuki Tsukui, MD, and colleagues from the Tokyo Women’s Medical University. At Monday’s Perioperative Care Symposium, Dr. Tsukui presented a study that evaluated one such Hiroyuki Tsukui, MD, reported on a management system for HD patients. modified perioperative management system in hemodialysis (HD) patients undergoing cardiac surgery, which was designed to improve early outcomes, compared with the previous regimen. The researchers found that their new management system improved both early mortality and morbidity, as well as several other measured outcomes. The new management system was as follows: 1) one week before surgery, they discontinued medications for hyperphosphatemia; 2) a low-fiber diet and medications were introduced for defecation; 3) after surgery, alprostadil alfadex (120 mcg/day) was infused continuously to maintain organ perfusion; 4) continuous HD was used routinely for several days from postoperative day 1, and then at regular intermittent HD was introduced. The researchers studied consecutive HD patients undergoing cardiac surgery. They were divided into two groups (Group M: modified management versus Group P: previous management). Most of the patients took 7 to 10 days to reach the target dry weight after surgery, said Dr. Tsukui. There were no significant differences between the two groups in terms of preoperative status or surgical procedures except for operation time. In terms of mortality, there were no hospital deaths in Group M, whereas eight patients (12.3%) died in Group P, which was a significant difference.. In addition, in terms of postoperative complications, the rate of reexploration for bleeding was significantly lower in Group M, compared with Group P, and there was also a significant difference in favor of Group M in the lengths of intubation period and in-hospital stay Although no statistically significant differences were observed in the following other complications examined, a lower rate was found in Group M of superficial wound infection, mediastinitis, pneumonia, sepsis, ileus, pancreatitis, cholecystitis and respiratory failure requiring tracheotomy. “Modified perioperative management improved early mortality and morbidity, and shortened the length of intubation period and hospital stay in HD patients undergoing cardiac surgery,” concluded Dr. Tsukui. The relative impact of preoperative anemia versus packed red blood cell (PRBC) transfusion on outcomes remains poorly understood, according to Damien J. LaPar, MD, University of Virginia, and his colleagues. He reported on their study that investigated the relative association between preoperative hematocrit (Hct) level versus PRBC transfusion on postoperative outcomes after coronary artery bypass grafting (CABG). They evaluated the records of 21,641 patients who had isolated CABG operations from January 2007 Damien J. LaPar, MD, discussed the role of PRBC transfusions in CABG. to June 2014 at 17 cardiac surgery centers. They used multivariate analysis to estimate the relationship between baseline preoperative Hct level as well as PRBC transfusion and the likelihood for postoperative mortality and morbidity, adjusted for baseline patient risk. As expected, a strong association was observed between preoperative Hct and the likelihood for PRBC transfusion. After risk adjustment, PRBC transfusion (not Hct level) demonstrated stronger associations with post- Marc Ruel, MD, addressed the risk factors for reopening for bleeding. operative mortality, renal failure, and stroke, said Dr. LaPar. Decreasing preoperative Hct was significantly associated with an increased probability of mortality and renal failure. Preoperative anemia (compared with an Hct level of 40%) was associated with up to a 66% increase in the probability of PRBC transfusion, 50% increase in renal failure, and a 43% increase in mortality. They found, however, that packed red blood cell transfusion appeared to be more closely associated with risk-adjusted morbidity and mortality than was the preoperative hematocrit level alone, supporting efforts to reduce unnecessary PRBC transfusions. “However, because preoperative anemia does independently increase the risk of postoperative morbidity and mortality, these data suggest that preoperative hematocrit levels should be included in the STS risk calculators. In addition, efforts to optimize preoperative hematocrit should be investigated as a potentially modifiable risk factor,” Dr. LaPar said. “The results of our analyses have significant clinical implications. Our study’s demonstration that there exists a highly significant and strong association between preoperative Hct and the likelihood for PRBC transfusion further emphasizes the critical role of proper preoperative planning and correction of preoperative anemia when possible to avoid the untoward effects of PRBC transfusion following cardiac surgery. These results further corroborate blood conservation efforts and guidelines advanced by the Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists,” Dr. LaPar concluded. Reopening for bleeding is known to be a lethal, morbid and costly complication of cardiac surgery. Marc Ruel, MD, reported in a study that he and his colleagues at the University of Ottawa performed to establish the risk factors and impact of reopening for bleeding (Rf B) in a large, modern cardiac surgical cohort. The baseline, index procedural, reopening, outcome and readmission characteristics of nearly 17,000 consecutive adult cardiac surgical patients were prospectively entered into a dedicated clinical database. Determinants of Rf B, as well as its independent impact on outcomes and readmission, were examined by using multivariable regression models supplemented with bootstrap simulations. The mean age of the patients was nearly 66 years, and 71.4% of the patients were men. Reopening after the index operation occurred in 4.2% of patients with over 90% of these being Rf B. Perioperative mortality was 2.8% in those who did not undergo Rf B and 12.0% in those who had Rf B, which was a significant difference, independent of other mortality risk factors. Hospital length of stay was greatly increased by RfB (median 12 versus 7 days in patients who did not have RfB, a signficant difference). This increased length of stay was greater than for any other predictor including postoperative atrial fibrillation (median increase by 2 days). RfB also was significantly and independently associated with new-onset postoperative atrial fibrillation (36.3% versus 26.0%) in non-RfB patients. Significant risk factors for Rf B were tricuspid valve repair, on-pump versus off-pump CABG, emergency status, cardiopulmonary bypass (CPB) duration, low body surface area, and low CPB hematocrit. Rf B was not predicted by age, creatinine level, or preoperative hematocrit, and Rf B did not increase the incidence of hospital readmission. “Because reopening for bleeding after cardiac surgery is an independent detrimental effect that surpasses any other known potentially modifiable risk factor, as shown in this large cohort, all efforts should be made to minimize the incidence and burden of Rf B, including further research on transfusion management during CPB,” Dr. Ruel concluded. A PRIL 25-29, 2015 T • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA AATS 95TH ANNUAL MEETING 17 General Thoracic Surgery Adapts to Changing Therapeutics he question of how to manage locally advanced thymomas (LATs) is controversial and, so far, no specific oncological strategies have been recommended, according to Giovanni Leuzzi, MD. In order to address this question, Dr. Leuzzi of the Regina Elena National Cancer Institute in Rome and his colleagues performed a retrospective analysis on the use of multimodal therapies for LATs. In Monday’s General Thoracic Surgery Symposium, Dr. Leuzzi presented their results, which were obtained by assessing a database developed and maintained by the European Society of Thoracic Surgeons (ESTS) Thymic Working Group. Clinico-pathological, surgical, and oncological features were reviewed in a cohort of 370 Masaoka-Koga stage III thymoma patients (WHO Classification A to B3) who were treated at 38 institutions from January 1990 to January 2010. In order to identify independent predictors of outcomes, a multivariate Cox proportional hazard model and a propensity score match were performed to identify independent predictors of Overall (OS), Cancer-specific (CSS) and Relapse-free survival (RFS). Induction and adjuvant therapy were administered to 88 and 245 patients, respectively. Overall, 5 and 10-year Giovanni Leuzzi, MD, discussed the management of LATS. Pier Luigi Filosso, MD, spoke on the most effective treatment for LCNEC. OS, CSS and RFS rates were 82.8%, 88.4% and 80.0%, and, 68.9%, 83.3% and 71.5%, respectively. Induction therapy was associated to similar 5-year CSS and RFS compared to primary surgery. At propensity score analysis, adjuvant therapy was confirmed as the strongest predictive factor for OS and CSS. Pathologic T classification (according to IASLC/ITMIG TNM staging proposal) was an independent factor for relapse. When CSS was adjusted for T classification, adjuvant therapy confirmed a significant survival advantage. On the other hand, for thy- momas larger than 5 cm, stratifying for tumor size and adjuvant therapy did not affect 5-year CSS. “The results of our study indicate that induction therapy does not affect survival in LATs. Our results indicate that adjuvant therapy should be administered whenever possible, mainly in those tumors with specific pathological features (pT2/3 or tumor size < 5 cm). These data may be considered for development of future clinical trials on adjuvant therapy,” Dr. Leuzzi concluded. Large cell neuroendocrine carcinomas (LCNEC) of the lung are neo- Graham Awards Thoralf M. Sundt, III, MD, Vice President AATS Graham Foundation; 2015 – 2016 Graham Memorial Traveling Fellow, Yaxing Shen, MD, Fudan University of Shanghi, China; David J. Sugarbaker, MD, President AATS Graham Foundation Thoralf M. Sundt, III, MD, Vice President AATS Graham Foundation; Pablo Sanchez, MD, University of Maryland, 2015 F. Griffith Pearson Fellowship; David J. Sugarbaker, MD, President AATS Graham Foundation. Not pictured: James Lubawski, MD, Central DuPage Hospital, 2015 F. Griffith Pearson Fellowship. Cardiothoracic Surgical Investigators David J. Sugarbaker, MD, President AATS Graham Foundation; Felix Fernandez, MD, Emory University School of Medicine; Danielle Gottlieb, MD, Columbia Presbyterian Hospital; Mark Onaitis, MD, Duke University; Bo Tang, MD University of Michigan; Thoralf M. Sundt, III, MD, Vice President AATS Graham Foundation. Not shown: Brendon Stiles, MD, Weill Cornell Medical College. plasms with very aggressive biological behavior. In part because of their rarity, there has been a lack of controlled clinical trials concerning their most effective treatment. Currently, the usefulness of adjuvant chemotherapy is still debated, since these tumors do not seem completely responsive to chemo/ radiotherapy and tumor recurrences or metastases are very frequent. This is true even in cases of early-stage neoplasms in which postoperative treatment has been administered, according to Pier Luigi Filosso, MD, of the University of Torino. Dr. Filosso reported on a study he and his colleagues undertook to to evaluate the impact of adjuvant chemotherapy in resected LCNECs. They found that there was no significant impact of adjuvant chemotherapy on survival. Their retrospective study examined a cohort of LCNEC patients operated on between 1992 and 2012 at 17 institutions. Overall survival from date of resection was estimated by the Kaplan-Meier method. Patients receiving adjuvant treatment showed slightly worse three-year survival than the rest of the patients, with no evidence of a protective effect. Sensitive analysis performed using multivariable Cox model showed similar results. Age and advanced TNM stages were significant negative predictors. 18 AATS 95TH ANNUAL MEETING A PRIL 25-29, 2015 Thank you, JTCVS Team Editorial Board Awards The Journal of Thoracic and Cardiovascular Surgery would like to congratulate the following members of the Editorial Board. They are the best performers out of a group of very high achievers and we recognize them for their dedication and accomplishment. Education and Training James I. Fann Thoracic Chadrick E. Denlinger Victor A. Ferraris Raja M. Flores Katie S. Nason Thomas Ng W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA Ethicon and AATS Graham Foundation Partnership Reviewer Awards The Journal of Thoracic and Cardiovascular Surgery would like to congratulate the following reviewers for their performance in 2014. They are the best performers out of the over 560 non-board reviewers! Acquired Grayson H. Wheatley III Tirone E. David Davis C. Drinkwater, Jr. Stephen E. Fremes Craig R. Smith Acquired Paul Kurlansky Vinay Badhwar Richard Lee Leonard N. Girardi Congenital Scott M. Bradley William M. DeCampli Joseph A. Dearani • Congenital Tara Karamlou Paul Chai Osman O Al-Radi Thoracic Wael C. Hanna David R. Jones Betty Caroline Tong Perioperative Management Nicholas D Andersen David J. Sugarbaker, MD, AATS Graham Foundation President, meet with representatives from Ethicon China and the Chinese International Medical Foundation who have partnered with the Graham Foundation to establish the Thoracic Surgery Training Fellowship, which will provide an international training and educational experience for young thoracic surgeons from mainland China to spend between one month and one year studying clinical techniques at North American institutions. Thomas A. D’Amico, MD, Duke University Medical Center is the lead surgeon facilitating both the Ethicon China Fellowship and the Ethicon Fellowship for Advanced Thoracic MIS. Dr. D’Amico provided an update on the unique educational experience that the awardees will be offered including operating room access to observe cases in minimally invasive thoracic surgery, conferences focused on a better understanding of the science and practice of minimally invasive thoracic surgery, and access to the faculty to develop lasting working relationships. Edward Zhou, VP of Ethicon Surgical Care was also part of the presentation. AATS AORTIC SYMPOSIUM 2016 COURSE DIRECTORS Joseph S. Coselli Steven L. Lansman May 12 – 13, 2016 Sheraton New York Times Square Hotel New York, NY, USA www.aats.org/aortic A PRIL 25-29, 2015 • W ASHINGTON S TATE C ONVENTION C ENTER • S EATTLE , WA AATS 95TH ANNUAL MEETING 19 The AATs was pleased to welcome the following new members to AATS during the New Members Induction on Monday Prasad S. Adusumilli New York, NY Shanda H. Blackmon Rochester, MN Cem H. Alhan Istanbul, Turkey Joanna Chikwe New York, NY Matthew Bacchetta New York, NY Ufuk Demirkilic Ankara, Turkey Clifford W. Barlow Southampton, UK Jessica S. Donington New York, NY Emre Belli Le Plessis-Robinson, France Alessandro Giamberti San Donato Milanese, Italy Mark F. Berry Durham, NC Peter J. Gruber Salt Lake City, UT Jay K. Bhama Pittsburgh, PA T. Sloane Guy Philadelphia, PA AATS DAILY NEWS The Official Newspaper of the AATS 95th Annual Meeting AATS Staff Executive Director Managing Editor Cindy VerColen Lorraine M. O’Grady Michael E. Halkos Atlanta, GA Andrew J. Lodge Durham, NC Jianxing He Guangzhou, China S. Chris Malaisrie Chicago, IL David P. Jenkins Cambridge, UK Joseph T. McGinn Staten Island, NY Sunjay Kaushal Baltimore, MD Michael E. Mitchell Milwaukee, WI Minoo N. Kavarana Charleston, SC T. Brett Reece Aurora, CO Bob Kiaii Arva, ON, Canada Nabil Rizk New York, NY Anthony W. Kim New Haven, CT Gu Tianxiang Shenyang, China Young T. Kim Seoul, Republic of Korea Alper Toker Istanbul, Turkey Charles T. Klodell Gainesville, FL Ching Tzao Taipei, Taiwan Christoph Knosalla Berlin, Germany Thomas J. Watson Rochester, NY Christopher J. Knott-Craig Memphis, TN Dennis A. Wigle, Rochester, MN John R. Liddicoat Mounds View, MN THE OFFICIAL NEWSPAPER OF THE ® Serving the cardiothoracic community since 2005 with news, features, and expert analysis from the United States and around the world. Read our Print, Interactive app and Digital Edition! FMC SOCIETY PARTNERS PUBLICATION STAFF Vice President/Group Publisher; Director, FMC Society Partners Associate Editor Mark Branca Design Supervisor Advertising Sales Elizabeth Byrne Lobdell Artie Krivopal Photographers Publication Editors Nationwide Photographers Therese Borden, Mark Lesney Production Specialist Gwendolyn B. Hall Maria Aquino Copyright 2015, American Association for Thoracic Surgery, 500 Cummings Center, Suite 4550, Beverly, MA 01915. Produced and distributed for AATS by Frontline Medical Communications. All rights reserved. No part of this publication may be reproduced or transmitted in any form, by any means, without prior written permission of the AATS. The opinions expressed in this publication are those of the presenters and authors, and do not necessarily reflect the views of the Association. Cover photo: Shutterstock.com Follow us on Twitter (@ThoracicTweets) and like us on Facebook. www.thoracicsurgerynews.com


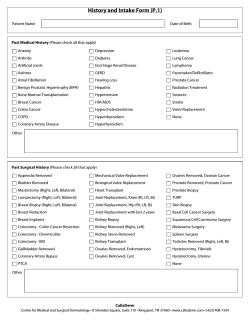







© Copyright 2025