
23 Internistendagen Abstractboek 13-15 april 2011
Inhoud 23e Internistendagen Abstractboek 13-15 april 2011 MECC, MAASTRICHT Voorwoord/Introduction 3 I Oral Presentations Research 4 II Oral Presentations Case reports 24 III Endocrinology Research 48 IV Endocrinology Case reports 50 V Diabetes Mellitus Research 58 VI Diabetes Mellitus Case reports 61 VII Haematology Research 62 VIII Haematology Case reports 63 IX Oncology Research 71 X Oncology Case reports 72 XI Vascular Medicine Research 80 XII Vascular Medicine Case reports 83 XIII Gastro-Enterology Research 86 XIV Gastro-Enterology Case reports 88 XV Infectious Diseases Research 92 XVI Infectious Diseases Case reports 93 XVII Nephrology Research XVIII Nephrology Case reports 111 XIX Intensive Care Research 113 XX Intensive Care Case reports 115 XXI Rheumatology Research 117 XXII Rheumatology Case reports 118 XXIII General Internal Medicine Research 120 XXIV General Internal Medicine Case reports 124 XXV Immunology/Allergology Research 136 XXVI Immunology/Allergology Case report 136 109 XXVII Other Research 137 XXVIII Other Case reports 138 Index 139 1 V OO R W OO R D / I N T R ODU C T I ON Voorbereidingscommissie Mw. Dr. H.A.H. Kaasjager Dr. M.A. van Agtmael Prof.drs. J.F.W.M. Bartelsman Prof.dr. J.W. Cohen Tervaert Dr. P.W. Kamphuisen Dr. E.J.P. de Koning Mw. Dr. A. Reyners Mw. Dr. A.W. Rijneveld Mw. Dr. F. Waanders (JNIV) Met genoegen presenteer ik u het abstractboek van de 23e Internistendagen, die worden gehouden van 13 tot 15 april 2011 in het MECC te Maastricht. De abstracts betreffen zowel wetenschappelijk onderzoek als casereports. Uit alle windrichtingen zijn de abstracts in grote getale ingestuurd. Er zijn 259 abstracts ingediend, die zijn opgenomen in dit abstractboek. Uit deze abstracts werden 84 abstracts geselecteerd voor orale presentatie. Deze worden eerst vermeld, gevolgd door de overige abstracts, geclassificeerd per vakgebied. De selectie is gebaseerd op wetenschappelijke inhoud, originaliteit en presentatie. De selectie gebeurt anoniem (auteurs en instituut worden geblindeerd) door drie leden van de commissie. De abstracts met de hoogste scores zijn geselecteerd voor orale presentatie. Ook dit jaar is er voor gekozen de abstracts zoveel mogelijk per onderwerp te bundelen in de verschillende sessies. Deelnemende verenigingen Nederlandse Internisten Vereniging (NIV) Internistisch Vasculair Genootschap Juniorafdeling Nederlandse Internisten Vereniging Nederlandse Federatie voor Nefrologie Nederlandse Vereniging voor Allergologie Nederlandse Vereniging voor Diabetes Onderzoek Nederlandse Vereniging voor Endocrinologie Nederlandse Vereniging voor Gastro-Enterologie Nederlandse Vereniging voor Haematologie Nederlandse Vereniging voor Immunologie Nederlandse Vereniging voor Intensive Care Nederlandse Vereniging voor Klinische Farmacologie Nederlandse Vereniging voor Medische Oncologie Nederlandse Vereniging voor Medisch Onderwijs Nederlandse Vereniging voor Oncologie Nederlandse Vereniging voor Vasculaire Geneeskunde NIV Sectie Acute Interne Geneeskunde NIV Sectie Ouderengeneeskunde Vereniging voor Infectieziekten Het grote aantal ingezonden abstracts onderschrijft dat dit een belangrijk onderdeel is van de Internistendagen. In de eerste plaats voor de arts-assistenten omdat de Internistendagen een uniek podium zijn om resultaten van onderzoek of bijzondere observaties te presenteren aan een enthousiast publiek. In de tweede plaats voor de toehoorders, die kunnen vernemen wat er gebeurt aan het front van de Interne Geneeskunde in Nederland en in de derde plaats om de diverse onderzoeksgebieden binnen de Interne Geneeskunde met elkaar in contact te brengen. Ook dit jaar zal per sessie een winnaar worden aangewezen die een prijs van 500 euro overhandigd zal krijgen! Namens de hele Commissie Internistendagen wens ik u veel plezier toe met het lezen maar vooral aanhoren van de vaak gloednieuwe onderzoeksresultaten en het oplossen van de leerzame puzzels in de casereports uit alle klinieken van Nederland! Organiserende vereniging Dr. H.A.H. Kaasjager Voorzitter Commissie Internistendagen Nederlandse Internisten Vereniging (Medicinae Internae B.V.) Postbus 20066 3502 LB Utrecht Tel.: 030-282 32 29 Fax: 030-282 32 25 www.internistendagen.nl/www.internisten.nl This abstract book contains all abstracts that have been submitted to the Annual Meeting of the Netherlands Association of Internal Medicine, 13-15 april 2011 in Maastricht, the Netherlands. Both research abstracts and case reports are included, representing all disciplines of Internal Medicine, 84 abstracts have been selected for oral presentation. These abstracts are printed first, in the order of presentation. The remainder of abstracts is categorized according to discipline. Congressecretariaat Congress & Meeting Services Holland Postbus 18 5298 ZG LIEMPDE Tel. 0411-633476 Fax 0411-633805 E-mail: internistendagen@congresservice.nl Dr. H.A.H Kaasjager Chairman Organizing Committee Uitgever Van Zuiden Communications B.V. Postbus 2122 2400 CC Alphen aan den Rijn Tel.: 0172-47 61 91 Fax: 0172-47 18 82 E-mail: zuiden@zuidencom.nl Internet: www.vanzuidencommunications.nl © 2011 Overname van delen uit dit abstractboek kan alleen plaatsvinden na schriftelijke toestemming van de uitgever. ISBN: 978-90-8523-153-0 2 3 I. ORAL PRESENTATIONS RESEARCH 1. 2. CD20 directs cell positioning in secondary lymphoid organs T. van Meerten1 , R.S. van Rijn 2 , A. Hagenbeek 3 , A.C.M. Martens3, T. Mutis3 1 Gelderse Vallei Hospital, Department of Internal Medicine, Willy Brandtlaan 10, 6716 RP EDE, the Netherlands, e-mail: tvanmeerten@gmail.com, 2Erasmus Medical Centre, ROTTERDAM, the Netherlands, 3University Medical Centre Utrecht, UTRECHT, the Netherlands Tipping the Noxa/Mcl-1 balance to overcome ABT-737 resistance in chronic lymphocytic leukemia M. Tromp, C.R Geest, T. Beaumont, A.P. Kater, M.H.J. van Oers, E. Eldering Academic Medical Centre, Department of Hematology, Meibergdreef 9, 1105 AZ AMSTERDAM, the Netherlands, e-mail: j.m.tromp@amc.uva.nl Human CD20 is a B-cell restricted transmembrane molecule and the most successful monoclonal antibody targeted antigen, used worldwide to treat patients with B-cell non-Hodgkin’s Lymphoma (B-NHL). Unfortunately, the majority of B-NHL patients develops resistance to anti-CD20 therapy, resulting in relapse of the disease. Anti-CD20 antibody resistance is poorly understood and a current focus of investigation. Antibody resistance may be related to the interaction of tumor cells via CD20 with the microenvironment. However, although the CD20 molecule was discovered 30 years ago, its exact function is still unknown. To explore the function of CD20, we used a system that isolates human CD20 from other B-cell surface molecules by retrovirally transferring the human CD20 gene into normal human T-cells. Initial in vitro assays comparing peptide-specific CD20-positive T-cell clones with nontransduced parental clones demonstrated no altered proliferative activity or cytokine production associated with CD20 transduction. We then injected a T-cell population containing 20% CD20-positive T-cells into immune deficient RAG2-/-yc/-mice (n=10) to compare the distribution of the cells into the organs with the distribution of normal human T-cells (control mice n=10) and human B-cells (control mice n=5). Immunohistochemical staining of the organs revealed a remarkable phenomenon in all 10 spleens of the mice that received the transduced T-cells: while normal T-cells were scattered throughout the spleen, the CD20-positive T-cells had positioned themselves periarteriolar in the same way as the human B-cells do. In the other organs, like the gut, liver and lungs, in contrast, the distribution of the CD20-positive T cells did not differ from the normal T-cells. To confirm the hypothesis that the migration capacity of T cells is altered following expression of the CD20 molecule, we studied the influence of CD20 expression on T-cells in in vitro transwell migration assays. In these assays CD20-positive T-cells exhibited a 50% decreased migration capacity towards stroma cells compared to the normal T-cells (p=0.0075). In summary, these data show that the CD20 molecule directs the positioning of cells in secondary lymphoid Introduction: Chronic Lymphocytic Leukemia (CLL) is the most common leukemia in the Western world. CLL is still an incurable disease despite new treatment strategies developed in the last decade. Current treatment of CLL is hampered by relapses, putatively originating from lymph nodes (LNs) and novel therapeutic strategies are warranted. In vitro CD40-stimulation of CLL cells partially mimics the LN microenvironment by altering levels of apoptosis-regulating Bcl-2 family members, resulting in resistance to both known cytotoxic drugs as well as novel drugs, such as the BH3 mimetic ABT-737, that antagonizes the anti-apoptotic proteins Bcl-XL and Bcl-2, but not Mcl-1 or Bfl-1. Currently, it is unclear which anti-apoptotic proteins contribute to resistance towards ABT-737 in CLL. Aim: We used the CD40 in vitro system to investigate the anti-apoptotic proteins associated with resistance to ABT-737 and to determine whether combination of known anti-leukemia drugs and ABT-737 resulted in apoptosis of CLL cells. Methods and results: To mimic the lymph node microenvironment, peripheral blood lymphocytes of CLL patients were cultured in vitro on feeder cells expressing human CD40L. We demonstrate that upon CD40-stimulation, patient-specific variations towards resistance to ABT-737 developed, that correlated with differences in the relative expression levels of Mcl-1 versus its antagonist Noxa (a pro-apoptotic protein). Furthermore, Noxa knockdown, as well as Mcl-1 overexpression, in human B cells by retroviral transduction resulted in resistance to ABT-737, corroborating the importance of the Noxa/Mcl-1 ratio in the development of resistance to ABT-737. Promisingly, increasing the Noxa/Mcl-1 balance, by lowering Mcl-1 with the tyrosine kinase inhibitor dasatinib or increasing Noxa levels with the purine analogue fludarabine, resulted in clear synergistic effects at low doses of ABT-737. Conclusions: Our in vitro data provide a rationale to investigate the combination of fludarabine or dasatinib with ABT-737 in a clinical setting as a novel treatment modality for refractory CLL. 4 organs. Our findings indicate that CD20 holds back further migration of the cells in order to take a periarteriolar position, which may be the optimal site for the physiological (T-cell independent) B-cell antigen recognition. In addition, these data help to understand the role of CD20-positive cells in their micro-environment, which opens up new ways to conquer anti-CD20 antibody resistance in the treatment of B-NHL. of the AIx variation during tilting could be explained by MAP and TR and 76% of the cfPWV variation by MAP and by gender. Conclusion: Instantaneous BP is a determinant of AIx and cfPWV in AF patients. Moreover, changes in AIx are unrelated to changes in cfPWV, indicating that these measures of vascular stiffness provide different information. 3. 4. Instantaneous blood pressure is a determinant of aortic augmentation index and pulse wave velocity: observations in patients with autonomic failure Near-peer teaching during the clerkship internal medicine: a randomized cross-over trial N. Wlazlo1 , B. Winkens2, C.P.M. van der Vleuten 2, W.G. Peters1 1 Catharina Hospital, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: nick.wlazlo@cze.nl, 2 Maastricht University, MAASTRICHT, the Netherlands A.M.T. Huijben1 , F.U.S. Mattace-Raso2, J. Deinum3, J. Lenders3, A.H. van de Meiracker2 1 St. Elisabeth Hospital, Department of Internal Medicine, Tilburg, the Netherlands, e-mail: aukehuijben@hotmail.com, 2 Erasmus Medical Centre, ROTTERDAM, the Netherlands, 3 Radboud University Medical Centre, NIJMEGEN, the Netherlands Introduction and aim: The use of near-peer teaching in procedural skills training and in PBL tutorial skills has been proven equal to training by faculty or staff members. However, it is unclear if senior students are also able to teach theoretical matters in a clinical clerkship setting. Therefore we compared the quality and desirability of teacher-led versus student-led education in a randomized, cross-over study. Methods: Twenty-six fourth year medical students doing an internship in internal medicine were given one hour of theoretical education in general internal medicine once a week. This training was alternatively provided by a final year undergraduate medical student (senior student) and a staff member (internist-haematologist). Students were randomized into a group that started with the senior student and a group that started with the internist. Topics discussed were (differential) diagnosis and treatment of common disorders in internal medicine, like anaemia, jaundice, liver failure, fluid and electrolytes, thyroid disorders, renal failure and haematological malignancies. Each student evaluated 4 teaching sessions on a 16 item questionnaire, and rated the session and the teacher. Both grades and the mean score of the 16 items (overall assessment) were compared using linear mixed models. Results: Altogether, 92 questionnaires were obtained. The grade for the senior student as tutor (8.38) was significantly higher than for the internist (7.94; p=0.010). Moreover, education sessions with the senior student received higher grades than with the internist (8.28 vs. 7.80; p<0.001). The overall assessment of the training (mean of 16 items) was significantly higher for the senior student (8.31) than for the internist (8.00; p=0.004). Scores at the item level showed that this was due to more interactivity and stimulation in a comfortable learning environment, as well Introduction: Acute lowering of blood pressure (BP) with vasodilating agents is associated with a reduction in aortic augmentation index (AIx), whereas carotid-femoral pulse-wave velocity (cfPWV) is largely unaffected. Aim: We explored the effect of acute BP lowering on these two indices of vascular aging, AIx and cfPWV, in patients with autonomic failure (AF). Materials and methods: In 10 AF patients (age 61±15 years, 4 males) and 14 age- and sex-matched controls finger blood pressure was measured with the finometer device (TNO-TPD Biomedical Instrumentation, Amsterdam) and cfPWV, AIx, normalized for heart rate, and time to aortic wave reflection (TR) with the SphygmoCor device (AtCor Medical, Sydney). Measurements were performed after subject had rested for 20 minutes in supine position and during 300 and 600 passive head-up tilting by means of motor-driven tilt table. Left ventricular ejection time (LEVT) were derived from the finger blood pressure signal using the BeatScope program (TNO-TPD Biomedical Instrumentation, Amsterdam). Results: At baseline mean BP (127.6±21.5 and 98.2±8.3 mmHg), AIx (32.4±13 and 20.4±12.2%) and cfPWV (12.1±3.6 and 8.7±1.6 m.s-1) were higher in patients than in controls. In patients, in response tot 30° en 60° MAP decreased by 18.7±9.8 and 39.6±11.6%, LEVT by 11.5±3.2 and 20.4±5.5%, AIx by 39.2±27.5 and 100.9±78.1%, cfPWV by 12.0±10.5 and 27.5±13.5% and HR increased by 5.2±7.7 and13.9±17.6% (all p<0.05), whereas TR did not change. In patients the fall in BP and decreases in AIx and cfPWV closely correlated (r=0.64, p=0.003 and r=0.74, p=<0.001). Postural decreases in AIx were not related to changes in cfPWV. In adjusted analysis, 68% 5 as more overview and physiology in the senior student’s training. Conclusion: Teaching of theoretical matters by a senior student received significantly higher assessments compared with teaching by a staff member. However, it is better to conclude that near-peer teaching produces similar results, given the small differences in grades. These results might be explained by cognitive and social congruence, or teaching skills being more important than content expertise. Near-peer teaching could therefore be implicated in clinical internships, and might attenuate the work load of specialists. 5. related to the determination of ferritin (p<0.05). In total 75 (5.6%) patients were diagnosed with IDA and 181 (13,4%) with ACD according to the DGPG. In only 1 patient with ferritin levels between 15 and 100 mg/l an elevated serum transferrin was established. Conclusion: Anemia analysis according to Dutch General Practitioners’ guidelines is followed only in the minority of patients, possible leading to an underdiagnosis of for instance IDA. 6. Adherence to the protocollar approach in diagnosing anemia in general practice; a retrospective cohort study Performance of four clinical decision rules in the diagnostic management of acute pulmonary embolism – the Prometheus diagnostic accuracy study R.A. Douma1, I.C.M. Mos2, P.M.G. Erkens3, T.A.C. Nizet 4, M.F. Durian5 , M.M. Hovens4 , A.A. van Houten6, H.M.A. Hofstee7, F.A. Klok2, H. ten Cate3, E.F. Ullmann 4, H.R. Büller1, P.W. Kamphuisen1, M.V. Huisman2 1 Academic Medical Centre, Department of Vascular Medicine, Meibergdreef 9, 1105 AZ AMSTERDAM, the Netherlands, e-mail: r.a.douma@amc.uva.nl, 2Leiden University Medical Centre, LEIDEN, the Netherlands, 3Maastricht University Medical Centre, MAASTRICHT, the Netherlands, 4Rijnstate Hospital, ARNHEM, the Netherlands, 5Erasmus Medical Centre, ROTTERDAM, the Netherlands, 6Maasstad Hospital, ROTTERDAM, the Netherlands, 7VU University Medical Centre, AMSTERDAM, the Netherlands J. Droogendijk1, P.B. Berendes2, R. Beukers2, P. Sonneveld1, M-D. Levin2 1 Erasmus Medical Centre, Department of Haematology, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: j.droogendijk@erasmusmc.nl, 2 Albert Schweitzer Hospital, DORDRECHT, the Netherlands Background: Iron deficiency anemia (IDA) is often encountered by general practitioners and other clinicians. Although IDA is a clinically relevant diagnosis, it often is difficult to recognize and distinguish from other causes of anemia such as anemia of chronic disease (ACD). For this reason guidelines are developed such as the Dutch General Practitioners’ guideline (DGPG). Aim: To retrospectively study the adherence of general practitioners to the DGPG in case of patients with newly discovered anemia. Materials and methods: We retrospectively evaluated all laboratory tests of patients with a new anemia diagnosed by general practitioners in the region of the Albert Schweitzer hospital from January 1st 2004 until 31 December 2005. We included women older than 50, in order to exclude a predominance of iron deficiency due to menstrual blood loss, and men 18 years and older with no diagnosis of anemia in the previous two years. Results: In two years time 1342 men and postmenopausal women were diagnosed with a newly discovered anemia by 63 participating general practitioners. 1103 patients (82%) displayed a normocytic anemia (mean corpuscular volume between 80 and 100), 131 (10%) microcytic (MCV below 80) and 65 (5%) macrocytic (MCV higher than 100). Ferritin, soluble iron, transferrin and total iron binding capacity were determined in 396 (32%), 367 (30%), 344 (28%) and 338 (27%) of patients with normocytic and microcytic anemia, respectively. Lower haemoglobin, lower MCV, male gender and higher creatinin were significantly Introduction: Pulmonary embolism (PE) is a frequently occurring and potentially fatal condition. Correct exclusion of the diagnosis demands a simple yet accurate diagnostic strategy. Several clinical decision rules (CDRs) are available for the exclusion of acute PE, including recently introduced simplified scores. However, these scores have not been directly compared. Aim: To directly compare the performance of four CDRs (Wells rule, revised Geneva score, simplified Wells rule and simplified revised Geneva score) in excluding PE in combination with D-dimer testing. Materials and method: Design: A prospective cohort study was performed including consecutive patients with suspected acute PE from seven academic and non-academic Dutch hospitals. The clinical probability of PE was assessed using a computer program, which calculated all CDRs and indicated the next diagnostic step. Clinical care was guided by the results of the CDRs and D-dimer results. A ‘PE unlikely’ result according to all CDRs in combination with a normal D-dimer result excluded PE, while patients with ‘PE likely’ according to at least one of the CDRs or an abnormal D-dimer result underwent CT-scanning. CDR results were compared with PE prevalence indentified by CT-scanning or venous thromboembolism during 3-month follow-up. 6 Results: 807 consecutive patients were included; PE prevalence was 23%. The number of patients categorized as ‘PE unlikely’ ranged from 62% (simplified Wells rule) to 72% (Wells rule); PE prevalence was comparable (13-16%). Combined with a normal D-dimer level, the CDRs excluded PE in 22-24% of patients. The total failure rates of the CDR-D-dimer combinations were similar (1 failure, 0.5- 0.6%, upper 95% CI 2.9- 3.1%). Despite 30% of the patients had discordant CDR outcomes, PE was missed in none of the patients with discordant CDRs and a normal D-dimer result. Conclusions: All four CDRs show similar performance for exclusion of acute PE in combination with a normal D-dimer level. This prospective validation indicates that the simplified scores may be used in clinical practice. 7. Materials and methods: Open-label, single-arm, multiCentre clinical trial of patients with objectively proven acute pulmonary embolism, conducted in twelve hospitals in the Netherlands from 2008 to 2010. Patients with acute PE were triaged with eleven predefined Hestia criteria for eligibility for outpatient treatment starting with therapeutic weight adjusted doses of LMWH (Nadroparin), followed by vitamin K antagonists. All patients eligible for outpatient treatment according to the Hestia criteria, were sent home either immediately or within 24 hours after PE was objectively diagnosed. Outpatient treatment was evaluated with respect to recurrent venous thromboembolism (VTE), including PE or deep venous thrombosis (DVT), major haemorrhage and total mortality during initial LMWH treatment and three months follow up. We considered outpatient treatment to be effective if the upper limit of the 95% confidence interval of the incidence of recurrent VTE would not exceed 7%. Results: Of 297 included patients, who all completed follow-up, 6 patients (2.0%; 95% confidence interval [CI], 0.8-4.3) had recurrent VTE (5 PE (1.7%), 1 DVT (0.3%)). Three patients (1.0%, 95% CI 0.2-2.9) died during three months follow-up, but none as a result of fatal PE. One patient died of fatal intracerebral haemorrhage, the other two patients died of progressive malignancy. In addition to the patient with intracranial bleeding, one other patient had a major bleeding event (0.7%, 95% CI 0.08%-2.4%). Conclusion: Outpatient anticoagulant treatment is potentially effective and safe for patients with pulmonary embolism who have been selected with the Hestia criteria. These data have to be confirmed by a randomized controlled trial. (Dutch Trial Register NTR1319) Outpatient treatment in patients with acute pulmonary embolism: the Hestia study W. Zondag 1 , I.C.M. Mos 1 , D. Creemers 2 , A.D.M. Hoogerbrugge3, O.M. Dekkers1, J. Dolsma 4, M. Eijsvogel5, L.M. Faber6, H.M.A. Hofstee 7, M.M.C. Hovens8, G.J.P.M. Jonkers9, K.W. van Kralingen1, M.J.H.A. Kruip10, T. Vlasveld11, M.J.M. de Vreede12, M.V. Huisman1 1 Leiden University Medical Centre, Department of Vascular Medicine, Albinusdreef 2, 2333 ZA LEIDEN, the Netherlands, e-mail: w.zondag@lumc.nl, 2Haga Hospital, THE HAGUE, the Netherlands, 3Spaarne Hospital, HOOFDDORP, the Netherlands, 4Diaconessenhuis, LEIDEN, the Netherlands, 5 Medical Spectrum Twente, ENSCHEDE, the Netherlands, 6 Rode Kruis Hospital, BEVERWIJK, the Netherlands, 7VU University Medical Centre, AMSTERDAM, the Netherlands, 8 Rijnstate Hospital, ARNHEM, the Netherlands, 9Rijnland Hospital, LEIDERDORP, the Netherlands, 10Erasmus Medical Centre, ROTTERDAM, the Netherlands, 11Bronovo Hospital, THE HAGUE, The Netherland, 12Haaglanden Medical Centre, THE HAGUE, the Netherlands 8. Somatostatin receptor scintigraphy in sarcoidosis P.M. van Hagen1, L.S.J. Kamphuis1, J.A.M. van Laar1, P.L.A. van Daele1, G.S. Baarsma2, D.J. Kwekkeboom1 1 Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: p.m.vanhagen@erasmusmc.nl, 2Het OogHospital, ROTTERDAM, the Netherlands Introduction: Patients with pulmonary embolism (PE) are initially treated in the hospital with low molecular weight heparin (LMWH). The most recent guideline of the American College of Chest Physicians on Antithrombotic therapy 2008 reports some small studies on outpatient treatment in patients with pulmonary embolism, which suggest outpatient treatment in selected patients with PE is potentially effective and safe but firm recommendations for clinical practice are lacking. Clinicians urgently need reliable, easy-to-use selection criteria for selection of patients with pulmonary embolism eligible for outpatient treatment. Aim: To evaluate the efficacy and safety of outpatient treatment according to predefined criteria (Hestia criteria) in patients with acute PE. Objectives: Somatostatin receptor scintigraphy (SRS) localizes granulomas by binding to somatostatin receptors that are expressed in sarcoidosis, a granulomatous disease frequently involving lungs, skin or eyes. We correlated uptake patterns on SRS and to disease parameters. Materials and methods: The degree of intensity (DoI) of uptake and localization of sarcoidosis associated lesion (SAL) in 218 patients were determined. DoI was compared with serum angiotensin converting enzyme (ACE) and serum soluble interleukin-2 receptor (sIL-2R). Typical patterns on SRS were compared to conventional chest CT and -x-ray. 7 Results: Therapeutic and symptomatic response was seen in four out of five (80%) patients in the observational period of 12 weeks. This was accompanied by decreased uptake on SRS and more than 15% reduction of pathological lymph node volumes on the CT-scan. Clinical symptoms improved followed by a fall of the inflammatory cytokines interferon-? (IFN-?) and interleukin-8 (IL-8). Conclusion: Four out of five patients (80%) patients were considered to benefit from the adalimumab treatment within 12 weeks. The clinical improvement was accompanied by more than 18% decrease of initially elevated serum IFN-? en IL-8 levels. This is the first study demonstrating both a trend in clinical and biochemical improvement after adalimumab treatment in chronic sarcoidosis. Results: SRS was negative in 28 patients, 10 patients had one -and 180 patients had more SAL. The DoI correlated significantly with ACE (p<0.001) sIL-2R levels (p<0.01). Mediastinal lesions together with either eye, salivary glands, clavicular or hilar localizations on SRS demonstrated a significant characteristic pattern. All patients with abnormal conventional tests had SRS uptake. Moreover, of 94 patients with normal radiological findings 49 expressed pathological SRS uptake. In 36 of these 49 patients a lung biopsy was taken, which revealed sarcoidosis in 31. Conclusion: The DoI in SRS correlates with sarcoidosis activity. SRS is more sensitive in diagnosing sarcoidosis, even in patients with normal chest radiology. SRS therefore provides a useful and sensitive imaging technique to monitor organ involvement and therapy in patients with sarcoidosis. 10. 9 Efficacy of adalimumab in sarcoidosis J.A.M. van Laar 1 , L.S.J. Kamphuis1, W.K. Lam-Tse2, W.A. Dik1, J. Bastiaans3, P.L.A. van Daele1, P. van Biezen1, D.J. Kwekkeboom, R.W.A.M. Kuijpers1, H. Hooijkaas1, G.S. Baarsma3, P.M. Van Hagen1 1 Erasmus Medical Centre, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: j.vanlaar@erasmusmc.nl, 2Sint Franciscus Gasthuis, ROTTERDAM, the Netherlands, 3Het OogHospital, ROTTERDAM, the Netherlands Steroid use and polymyalgia rheumatica predict redundant temporal artery biopsy in patients with suspected giant cell arteritis A.N. den Brok, I. Thomassen, C.J.A.M. Konings, S.W. Nienhuis, M.C.G. van de Poll Catharina Hospital Eindhoven, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: avalon.d.brok@catharina-Hospital.nl Introduction: Temporal artery biopsy (TAB) is the golden standard for the diagnosis of giant cell arteritis (GCA). This invasive procedure is experienced as unpleasant and upsetting for many patients. The yield of TAB is low (< 35% positive findings reported in the literature). In addition due to the relatively high rate of false negative outcomes, negative histology is sometimes ignored, making the biopsy redundant. Aim: To investigate clinical predictors of negative TAB and to assess clinical factors associated with not attaching clinical implications to a negative TAB. Materials and methods: One-hundred thirty consecutive patients undergoing successful TAB in our hospital were retrospectively analyzed. Univariate analyses (X2-test) and multivariate analyses (logistic regression analysis) were performed to identify associated factors and independent predictors for negative or redundant TAB. Results: Histological examination showed 33 positive and 97 negative TABs. Univariate analyses showed that the proportion of male patients with a negative TAB (48.5%) was significantly higher than the proportion of male patients with a positive TAB (15.2%) (p=0.001). In addition mandibular claudication was present in 8.2% of the patients with negative TAB versus 39.4% in patients with a positive TAB (p<0.001). Also the prevalence of headache was significantly lower in patients with a negative TAB (p=0.016). Interestingly, the prevalence of polymalgia rheumatica was significantly Introduction: Adverse effects and lack of specificity often hamper the use of conventional immunosuppressive drugs in patients with systemic sarcoidosis. Adalimumab, a monoclonal antibody directed against the key cytokine involved in sarcoidosis, tumor necrosis factor (TNF)-a, is used in patients with various immunological disorders. Improved specificity, hence less adverse effects are the major advantages of this new class of drugs leading to an exponentially increasing role in their clinical use. However, few reports involving adalimumab in patients with sarcoidosis have been published so far and are restricted to case reports. Aim: To investigate clinical and biochemical effects of adalimumab therapy in chronically active systemic sarcoidosis patients. Material and methods: Five patients with active, symptomatic and biopsy-proven systemic sarcoidosis received adalimumab with an induction scheme of 160mg at week 0, 80mg at week 2 and 40mg every other week for the observational period of 12 weeks. Therapeutic efficacy was monitored by computered tomography (CT)-scan, somatostatin receptor scintigraphy (SRS), pulmonary function tests, physical examination and various inflammatory parameters. 8 higher in patients with a negative TAB (9.1% vs. 28.9%, p=0.021). Multivariate analysis identified male gender (p=0.003), the absence of mandibular claudication (p=0.010) an erythrocyte sedimentation rate (ESR) < 60 mm (p=0.030) and a diagnosis of polymyalgia rheumatica (PMR) (p=0.023) as significant independent predictors of a negative TAB. In 29 patients using steroids at the time of TAB steroids were continued despite a negative TAB. In 15 cases steroids were started despite a negative TAB. In these patients TAB was considered redundant. Uni- and multivariate analyses identified an ESR < 60 mm (p=0.055), a diagnosis or suspicion of PMR (p<0.001) and the start of steroids before the biopsy (p<0.001) as independent predictors of redundant TAB. Conclusion: Temporal artery biopsy is often performed without attaching clinical consequences and could be refrained from in patients with a high clinical suspicion of giant cell arteritis or polymyalgia rheumatica. Steroid use and polymyalgia rheumatica are independent predictors of such redundant temporal artery biopsy. 11. for both the serum creatinine measurements and the MDRD-eGFRs were calculated. We created crosstabs to evaluate classification of patients when a Jaffe or an enzymatic assay was used to estimate MDRD-eGFR compared to when the ID-MS traceable MDRD was used. Results: Bias depended strongly on the creatinine concentration. Jaffe vs. an enzymatic technique showed a bias of 19% vs. 0% for the reference 52 mmol/l, and 0.8 vs. 2.3% for reference category 262 mmol/l, respectively. Such deviations in creatinine measurements resulted in erroneous CKD-staging. 23.4% vs. 14% of the 40-year-old subjects with a CKD stage of 60-90 ml/min/1.73m2 (when the ID-MS traceable MDRD was used) were classified in CKD stage 45-60 ml/min/1.73m2, when a Jaffe technique respectively an enzymatic technique was used to measure SCr. In the CKD stage 45-60 ml/min/1.73m2 77% compared to 87% of the 60-year-old patients would have been correctly staged when a Jaffe respectively an enzymatic technique was used to estimate GFR. Conclusion: Accurate and precise measurements of creatinine are required for a reliable estimation of GFR. The enzymatic technique to measure serum creatinine results in substantial less variability than the Jaffe technique compared to ID-MS reference values, leading to more reliable estimates of GFR. To allow improvement of reliability of eGFR calculations, the enzymatic technique to measure creatinine is preferable over the Jaffe technique. Effect of analytic variations in serum creatinine on eGFR assessment and chronic kidney disease staging I. Drion1, C. Weykamp2, C. Cobbaert 3, N. Kleefstra1, H.J.G. Bilo1 1 Isala Clinics, Thomas à Kempisstraat, 8021 BB ZWOLLE, the Netherlands, e-mail: i.drion@isala.nl, 2Streek Hospital Koningin Beatrix, WINTERSWIJK, the Netherlands, 3 Amphia Hospital, BREDA, the Netherlands 12. The anti-proteinuric effect of indomethacin is associated with a renoprotective urinary biomarker profile M.H. de Borst1, F.L. Nauta1, L. Vogt 2, R. Gansevoort1, G. Navis1 1 University Medical Centre Groningen, Department of Internal Medicine, PO Box 30.001, 9700 RB GRONINGEN, the Netherlands, e-mail: m.h.de.borst@int.umcg.nl, 2 Academic Medical Centre, AMSTERDAM, the Netherlands Introduction: Measurements of serum creatinine (SCr) are increasingly supplemented with creatinine-based estimations of glomerular filtration rate (eGFR). There are different methods to assess SCr, however. Estimates of GFR might be biased, depending on the technique of SCr measurement used. Aim: To examine the degree of variation and reproducibility of different methods of SCr assessment in Dutch laboratories and its consequences for eGFR and chronic kidney disease (CKD) staging. Materials and methods: Cross-sectional study evaluating SCr data from the external quality assessment program in 2009 from the Dutch external quality assessment organization for laboratories. All 139 participating laboratories measured serum creatinine using a Jaffe method and/or an enzymatic method. Reference values for creatinine (a linearity sequence ranging from 52-262 mmol/l as assessed by ID-MS) were determined by a Joint Committee for Traceability in Laboratory Medicine (JCTLM) accredited laboratory. GFR was estimated using the Modification of Diet in Renal Disease (MDRD) formula in three virtual age categories (40, 60 and 80 years). Bias and precision Background: Under specific conditions, non-steroidal anti-inflammatory drugs (NSAIDs) may be used to lower therapy-resistant proteinuria. Despite their favorable antiproteinuric effect, NSAIDs may also have deleterious renal effects, e.g. decreased GFR. Large-scale randomized trials investigating the long-term renoprotective effects of NSAIDs are lacking. We investigated whether indomethacin reduces urinary biomarkers of glomerular damage and, subsequently, proximal and distal tubular damage. We also investigated whether indomethacin reduces proteinuria-induced tubulo-interstitial inflammation, known to mediate progressive renal damage. Methods: Chronic kidney disease (CKD) patients (n=16) with preserved renal function and stable residual 9 Introduction: Fetal exposure to maternal hypercholesterolemia increases the extent of fatty-streak formation in fetal aortas as well as the rate of progression, and may therefore increase coronary heart disease (CHD) risk later in life. Aim: To determine whether the risk of CHD in untreated individuals with familial hypercholesterolemia (FH) is more extreme when the disease is transmitted maternally. Materials and methods: In a large Dutch pedigree carrying the V408M mutation in the low-density lipoprotein (LDL-) receptor gene, 161 individuals over seven generations were identified for which FH status and parent of origin of FH was known. We calculated standardized mortality ratios (SMR) and compared the consequences of maternal and paternal inheritance of FH by Poisson regression analysis. Results: Maternally inherited FH was associated with significantly higher excess mortality than FH transmitted by fathers (relative risk 2.2; p=0.048): the SMR of maternal inheritance was 2.49 (95% confidence interval (CI) 1.45-3.99; p=0.001), whereas it was not significantly increased in paternally inherited FH (SMR 1.30, 95% CI 0.65-2.32; p=0.234). Conclusions: Mortality rates are more increased when FH is inherited through the mother, supporting the fetal origin of adulthood disease hypothesis with all cause death, the most indisputable outcome measure. Future research should explore safe options for cholesterollowering therapy of pregnant women with FH in order to prevent unfavourable epigenetic consequences in their children. When carefully extrapolating to the general population, this study emphasizes the importance of a healthy lifestyle and low LDL-cholesterol levels during pregnancy. proteinuria of 4.7±4.1 g/d were studied. After a wash-out period of 4 wks without any RAAS blocking agents (CKD baseline), patients received indomethacin 75 mg BID for 4 weeks (CKD+NSAID). Adequate and stable blood pressure control was achieved during wash-out by non-RAAS blocking antihypertensive agents. At the end of the study, the 24h-excretion and plasma levels of total IgG, IgG4, kidney injury molecule-1 (KIM-1), beta-2-microglobulin (B2M), vitamin D binding protein (VDBP), neutrophil gelatinase associated lipocalin (NGAL), N-acetyl-betaglucosaminidase (NAG), heart-fatty acid binding protein (H-FABP) and monocyte chemotactic protein-1 (MCP-1) were determined in duplo using ELISA. Biomarkers were also determined in 24h urine of healthy kidney donors (n=10). Data are presented as mean±SD. Results: At baseline, proteinuria was 3.8±3.1 g/d and reduced to 2.4±3.4 g/d by indomethacin (p<0.001). The glomerular biomarkers total IgG (healthy controls 4±2 mg/d vs.CKD baseline 299.2±361.5, p<0.0001, CKD+NSAID 163.2±247.0, p<0.01) and IgG4 (0.5±1.6 mg/d vs. 58.9±71.8, p<0.0001 vs.17.4±18.8, p<0.001) were strongly increased in CKD patients at baseline compared to healthy controls, and strongly reduced by indomethacin. Some markers of proximal tubular damage (KIM-1 [3.9±4.0 ug/d vs. 9.5±5.5, p<0.01 vs.5.6±4.3, p<0.01], B2M [0.1±0.0 mg/d vs. 1.9±2.3, p<0.05 vs.1.0±2.2, p<0.05], and VDBP [0.1±0.0 mg/d vs. 18.4±43.2, p<0.001 vs.14.3±37.1, p<0.05]) but not all (NGAL, NAG) were reduced by the NSAID. The distal tubular marker H-FABP was not affected by IND (0.3±1.6 ug/d vs. 60.1±62.4, p<0.0001 vs.60.6±107.6). Surprisingly the antiinflammatory drug indomethacin did not reduce urinary excretion of the inflammation markers MCP-1 (1.0±0.9 ug/d vs. 1.9±1.1, p=0.01 vs.1.8±0.8) and NGAL, but did reduce plasma MCP-1 levels (CKD baseline 0.23±0.13 ug/l, CKD+NSAID 0.14±0.14, p=0.001). Conclusion: The anti-proteinuric effect of indomethacin is associated with strongly reduced urinary excretion of biomarkers of glomerular damage. Although indomethacin did not affect markers of tubulo-interstitial inflammation, it did clearly reduce proximal tubular markers, probably as a consequence of the anti-proteinuric effect. 13. 14. Genetic variant of the scavenger receptor BI in humans M. Vergeer1 , S. Korporaal 2, R. Franssen1, I. Meurs2, R. Out 2, G.K. Hovingh1, M. Hoekstra 2, J.A. Sierts1, G.M. Dallinga-Thie1, M.M. Motazacker1, A.G. Holleboom1, Th. van Berkel 2 , J.J.P. Kastelein 1, M. van Eck 2 , J.A. Kuivenhoven1 1 Academic Medical Centre, Department of Vascular Medicine, Meibergdreef 9, 1105 AZ AMSTERDAM, the Netherlands, e-mail: mennovergeer@hotmail.com, 2Gorlaeus Laboratories, LEIDEN, the Netherlands Maternal inheritance of familial hypercholesterolemia increases mortality J. Versmissen 1 , I.P.G. Botden 1, R. Huijgen 2 , D.M. Oosterveer1, J.C. Defesche2, T.C. Heil1, A. Muntz1, J.G. Langendonk 1, A.F.L. Schinkel1, J.J.P. Kastelein 2, E.J.G. Sijbrands21 1 Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: Jorievers@hotmail.com, 2 Academic Medical Centre, AMSTERDAM, the Netherlands Introduction: In mice, the scavenger receptor class B type I (SR-BI) is essential for the delivery of high-density lipoprotein (HDL) cholesterol to the liver and steroidogenic organs. Paradoxically, elevated HDL cholesterol levels are associated with increased atherosclerosis in SR-BIknockout mice. Aim: To elucidate the role of SR-BI in human metabolism. 10 Methods: We sequenced the gene encoding SR-BI in persons with elevated HDL cholesterol levels and identified a family with a new missense mutation (P297S). The functional effects of the P297S mutation on HDL binding, cellular cholesterol uptake and efflux, atherosclerosis, platelet function, and adrenal function were studied. Results: Cholesterol uptake from HDL by primary murine hepatocytes that expressed mutant SR-BI was reduced to half of that of hepatocytes expressing wild-type SR-BI. Carriers of the P297S mutation had increased HDL cholesterol levels (1.8 mmol per liter, vs. 1.4 mmol per liter in noncarriers; p<0.001) and a reduced capacity for efflux of cholesterol from macrophages, but the carotid artery intima-media thickness was similar in carriers and in family noncarriers. Platelets from carriers had increased unesterified cholesterol content and impaired function. In carriers, adrenal steroidogenesis was attenuated, as evidenced by decreased urinary steroid excretion, a decreased response to corticotropin stimulation, and symptoms of diminished adrenal function. Conclusion: We identified a family with a functional mutation in SR-BI. The mutation carriers had increased HDL cholesterol levels and a reduction in cholesterol efflux from macrophages but no significant increase in atherosclerosis. Reduced SR-BI function was associated with altered platelet function and decreased adrenal steroidogenesis. 15. Aim: To investigate whether circulating PCSK9 levels are associated with the FCHL phenotype and – when positive – to determine the strength of its heritability. Secondly, to study the response in PCSK9 levels to treatment with standard lipid lowering therapy. Materials and methods: Plasma PCSK9 levels were measured with a sandwich ELISA (developed by Eli Lilly and company) in FCHL patients (n=45), their normolipidemic relatives (n=139) and spouses (n=72). The heritability estimates for PCSK9, i.e. to what extent the variance in plasma PCSK9 levels can be accounted for by genetic factors, were calculated with SOLAR and FCOR. In addition, PCSK9 levels were determined in eleven FCHL patients before and after treatment with atorvastatin 40mg once daily for eight weeks. Results: Plasma PCSK9 levels (interquartile range) were significantly higher in FCHL patients when compared to normolipidemic relatives and their spouses: 96.1 (37.7132.9) versus 78.7 (60.6-100.3) and 82.0 (65.3-97.9) ng/ml, p=0.004 and p=0.002, respectively. PCSK9 was positively associated with both triglycerides and apolipoprotein B levels (p<0.001). The latter relation was primarily accounted for by LDL-apoliprotein B (r=0.31, p=0.02), but not by VLDL-apolipoprotein B (r=0.09, p=0.49), as demonstrated in a subgroup of subjects (n=59). Heritability calculations for PCSK9 yielded estimates of 67 and 84% (p<0.0001). Finally, circulating PCSK9 increased significantly from 122 to 150 ng/ml in eleven FCHL patients treated with atorvastatin 40mg once daily for 8 weeks (p=0.018). Conclusion: This study demonstrates that plasma PCSK9 is a highly heritable trait that is associated with both FCHL diagnostic hallmarks. These results warrant further studies to unravel the exact role of PCSK9 in the pathogenesis this genetic dyslipidemia. In this respect, the upstream sterol regulatory element binding protein 2 (SREBP2) pathway is of particular interest. Finally, the significant rise in PCSK9 levels after statin treatment suggests that FCHL patients could benefit from PCSK9 antagonizing therapy, which is currently under development. Circulating proprotein convertase subtilisin kexin type 9 is a highly heritable trait of familial combined hyperlipidemia M.C.G.J. Brouwers1, M.M.J. van Greevenbroek1, J.S. Troutt2, Angela Bonner Freeman2, Ake Lu3, N.C. Schaper1, R.J. Konrad2, C.D.A. Stehouwer1 1 Maastricht University Medical Centre, Department of General Internal Medicine and Endocrinology, PO Box 5800, 6202 AZ MAASTRICHT, the Netherlands,email:martijn.brouwers@maastrichtuniversity.nl,, 2 Eli Lilly and Company, INDIANAPOLIS, USA, 3University of California Los Angeles, LOS ANGELES, USA 16. Introduction: Familial combined hyperlipidemia (FCHL) is the most prevalent genetic dyslipidemia in Western Society. Its characteristic dyslipidemia is the consequence of hepatic VLDL-overproduction – at a background of insulin resistance – combined with an impaired clearance of remnants and LDL-particles. Proprotein convertase subtilisin kexin type 9 (PCSK9) is an important, inverse regulator of LDL-particle clearance, since it promotes the degradation of the LDL receptor in hepatocytes. Furthermore, recent studies have suggested that PCSK9 is also involved in VLDL-production. PCSK9 is therefore an intriguing candidate to evaluate its involvement in FCHL. Sensitivity, specificity and reproducibility of the aldosterone-to-renin-ratio as a screening test for primary aldosteronism – results of the dutch Arrat study P.M. Jansen, A.H.J. Danser, A.H. van den Meiracker Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: jansen.pm@gmail.com Background: The aldosterone-to-renin ratio (ARR) is a widely used screening test for primary aldosteronism (PA). A commonly adopted cut-off value according to 11 Objective: To describe the first results of renal sympathetic nerve denervation for treatment of therapy resistant hypertension in Rotterdam, the Netherlands. Design and methods: From September until December 2010 eight patients (mean age 48±8 years, 3 males) with treatment resistant hypertension (defined as a blood pressure above goal despite use of 3 or more antihypertensives) were treated with a new endovascular catheterguided technique, in which the renal nerves are denervated through radiofrequency ablation via the lumen of the renal arteries. Blood pressure and heart rate (mean of 10 automated measurements), estimated glomerular filtration rate (GFR), plasma noradrenalin (as a marker for sympathetic activity) and renin (as a marker for activity of the renin-angiotensin system) were measured before and 1 week and 1 month after the procedure. Results: Baseline blood pressure was 164±17/103±15 mmHg, heart rate 83±24 bpm and GFR 72.9±14.5 ml/min. The average number of antihypertensives was 5.3 (range 4-7). Renal sympathetic nerve denervation was performed uncomplicated in all patients. Four out of 8 patients (baseline blood pressure 162±3/103±12 mmHg) showed a marked decrease in blood pressure (136±16/84±16 mmHg after 1 week and 137±9/85±7 mmHg after 1 month). The other patients did not show any change in blood pressure. Plasma noradrenalin concentration decreased from 402±97 to 308±103 pg/ml (p=NS) after 1 week and to 350±137 pg/ ml (p=NS) after 1 month. Plasma renin concentration at baseline (median 13 uU/ml) did not change significantly (16 uU/ml after 1 week and 18 uU/ml after 1 month). For all 8 patients changes in SBP were not related to baseline blood pressure or changes in plasma noradrenalin or plasma renin concentration. Heart rate, GFR and number of antihypertensives after 1 week and 1 month did not change. Conclusion: In patients with therapy resistant hypertension renal sympathetic nerve denervation was associated with a response rate of 50%. The response was unrelated to changes in plasma noradrenalin or plasma renin concentration. the Endocrine Society guidelines is 91 pmol/l per mU/l. However, its sensitivity, specificity, and reproducibility have not been studied extensively. Objective: To characterize the main test characteristics of the ARR. Design and methods: In 99 patients with uncontrolled hypertension (despite the use of at least 2 antihypertensive drugs) plasma renin and aldosterone levels were assessed twice with an interval of 2 to 4 weeks. Betablockers and/ or potassium sparing diuretics were discontinued at least 4 weeks before the first measurement. In all patients an intravenous salt loading test (SLT) was performed. Patients with a post-test plasma aldosterone concentration exceeding 235 pmol/l were considered to have PA. Subsequently, aldosterone and renin measurements were repeated in a subset of 64 patients after at least 4 weeks on standardized treatment consisting of a calcium-channel blocker and/or alphablocker. In the other 35 patients it was not possible to change the antihypertensive regimen due to very high blood pressure levels or side effects of standardized treatment. Sensitivity and specificity were calculated under random and standardized medication. Reproducibility was evaluated by Bland-Altman analysis of log-transformed ARR levels at the first (ARR1) and second (ARR2) measurement. The 95% limits of agreement were expressed as ARR1/ARR2 ratios. Results: Fifteen patients had PA based on a positive SLT. The other 84 patients were considered essential hypertensives (EH). The median ARR was 36.5 (range 6.2-295.5) in PA patients versus 6.7 (0.2-65.7) in EH (p<0.001). Under random medication the ARR had 33% sensitivity and 100% specificity when a cut-off value of 91 was used. In the subgroup receiving standardized treatment the ARR rose from 10.3 (range 0.2-295.5) to 17.2 (0.9-438.6) (p<0.001). However, sensitivity remained low at a level of 37.5% with a specificity of 98.2%. Ninety-five percent of ARR1/ARR2 ratios were between 0.2 and 2.6 for PA patients, and between 0.3 and 4.0 for EH patients. Conclusion: When applying the commonly adopted ARR cut-off value of 91, sensitivity for PA is low,even under ARR-neutral medication,. Reproducibility is poor, stressing the need for repeated measurement of the ARR. On behalf of the Dutch ARRAT Investigators. 17. 18. Renal sympathetic nerve denervation for the treatment of resistant hypertension: first results in Rotterdam, the Netherlands The value of the mortality in emergency department sepsis (MEDS) score, CRP, and lactate in predicting 28-day mortality of sepsis in a dutch emergency department M.A.W. Hermans, P. Leffers, L.M. Jansen, Y.C.A. Keulemans, P.M. Stassen Academic Hospital Maastricht, Department of Internal Medicine, PO Box 5800, 6202 AZ MAASTRICHT, the Netherlands, e-mail: p.stassen@mumc.nl N.A.J. van der Linde, A.H. van den Meiracker Erasmus Medical Centre, Department of Vascular Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: n.vanderlinde@erasmusmc.nl Introduction: The tendency of sepsis to progress rapidly and the benefit of early start of therapy emphasize the 12 importance of fast and adequate risk stratification in the Emergency Department (ED). The Mortality in Emergency Department Sepsis (MEDS) score was developed in the U.S.A. to distinguish high- from low-risk patients that present to the ED with sepsis. Aim: This study aimed to (1) validate the MEDS score as a predictor of 28-day mortality in ED sepsis patients in the Netherlands, (2) investigate the value of C-reactive protein (CRP) and lactate in predicting 28-day mortality and compare these to the MEDS score. Materials and methods: Cohort study in a Dutch secondary and tertiary care university hospital. Patients were included if they were seen by an internist in the ED, fulfilled the criteria for (suspected) sepsis, and were admitted to the hospital. Primary outcome was all-cause, in-hospital mortality within 28 days of presentation. Results: In our six-month study period, 331 patients were included, of whom 38 (11.5%) died. Mortality varied significantly per MEDS category: < 4 points (very low risk: 3.1%), 5-7 points (low risk: 5.3%), 8-12 points (moderate risk 17.3%), 13-15 points (high risk: 40.0%), > 15 points (very high risk: 77.8%). These mortality rates were higher than those of the original validation study. The mortality rate for CRP levels < 100 mg/ml was 7.6% (SD 2.2) vs. 14.9% for CRP levels > 100 mg/ml (p 0.039). For lactate levels < 4, and > 4 mmol/l, mortality rates were 24.2% (SD 7.5) and 74.3 (SD 12.8), respectively. In ROC-analysis, the MEDS score was better in predicting 28-day mortality than CRP (AUCs 0.81 and 0.68, respectively). Lactate was not measured in enough patients (47) for a valid evaluation, but it seemed to predict mortality fairly (AUC 0.75). Conclusion: The MEDS score is an adequate tool for predicting mortality in patients with sepsis in a Dutch ED population. CRP is less useful in this context. Lactate appears to be a fair predictor of mortality, but needs to be investigated more systematically in a larger population. 19. of which endocarditis is the most common manifestation. Q fever endocarditis requires long-term antibiotic treatment and has poor prognosis if left untreated. The estimated risk of developing Q fever endocarditis after primary infection for patients with pre-existent valvulopathy was 39% in a retrospective study, with the highest risk for patients with prosthetic valves. In the Netherlands, there has been a large outbreak of acute Q fever with over 4000 notified cases since 2007, which allows a more precise estimation of the risk for chronic Q fever in high-risk groups. Aim: We studied the prevalence of chronic Q fever in an endemic area in patients with a history of cardiac valve surgery, including valve prosthesis. Materials and methods: We identified patients with a history of cardiac valve surgery from our cardiology outpatient clinic and invited them by letter for microbiological screening. IgG antibodies to phase I and II antigens of C. burnetii were tested by immunofluorescence assay. If phase I IgG antibodies were present, polymerase chain reaction (PCR) on blood for C. burnetii DNA was also performed. Chronic Q fever was considered probable if phase I IgG antibody titre was =1024 and proven in case of positive C. burnetii PCR in blood. Results: A total of 663 patients was identified with a history of valve surgery and unknown C. burnetii serostatus. As of January 2011, 200 patients had been invited for screening. In total, 175 patients (87.5%) responded and were available for serological screening. Of these, 31/175 patients (17.7%) had phase I and/or phase II IgG antibodies against C. burnetii, indicating a previous C. burnetii infection. In this group, 2/31 patients (6.5%) had phase I antibodies titres =1024, indicating probable chronic Q fever endocarditis. C. burnetii PCR was negative for both patients. Conclusion: Despite a seroprevalence of IgG antibodies against C. burnetii of 17.7% in patients with a high risk of developing chronic Q fever, only 6.5% of these patients had probable chronic Q fever endocarditis. Compared to the previously reported risk of 39% in case of valvulopathy, we found a considerable lower percentage of patients who progressed to chronic Q fever after C. burnetii infection. However, as chronic Q fever can develop years after primary infection, further follow-up of seropositive patients is warranted. Low prevalence of Coxiella burnetii endocarditis in patients with a history of cardiac valve surgery or cardiac valve prosthesis in a Q fever endemic area L.M. Kampschreur1 , J.J. Oosterheert 2, P.J. Lestrade3, I.M. Hoepelman2, N.H.M. Nicole3, P. Elsman3, P.W. Wever3 1 University Medical Centre Utrecht/Jeroen Bosch Hospital, Department of Internal Medicine and Infectious Diseases, PO Box 85500, 3508 GA UTRECHT, the Netherlands, e-mail: l.m.kampschreur@umcutrecht.nl, 2University Medical Centre Utrecht, UTRECHT, the Netherlands 3Jeroen Bosch Hospital, ’s-HERTOGENBOSCH, the Netherlands 20. A randomized study comparing no treatment with 24 or 60 weeks of antiretroviral treatment during primary HIV infection M.L. Grijsen1 , R. Steingrover2 , F.W.N.M. Wit 2 , S. Jurriaans1, A. Verbon3, K. Brinkman4, M.E. van der Ende5, R. Soetekouw6, F. de Wolf7, J.M.A. Lange2, H. Schuitemaker1, J.M. Prins1 1 Academic Medical Centre, Department of Internal Medicine, Division of Infectious Diseases, Tropical Medicine and AIDS, Introduction: Q fever is a zoonosis caused by Coxiella burnetii. Following primary infection, which is often asymptomatic, 1-5% of patients develop chronic Q fever, 13 Conclusions: Temporary cART during PHI lowers the viral setpoint and defers the start of cART during chronic HIV infection. Meibergdreef 91, 1105 AZ AMSTERDAM, the Netherlands, e-mail: m.l.grijsen@amc.nl, 2 Academic Medical Centre, Amsterdam Institute for Global Health and Development, AMSTERDAM, the Netherlands, 3Maastricht University Medical Centre, MAASTRICHT, the Netherlands, 4Onze Lieve Vrouwe Gasthuis, AMSTERDAM, the Netherlands, 5 Erasmus Medical Centre, ROTTERDAM, the Netherlands, 6 Kennemer Gasthuis, HAARLEM, the Netherlands, 7Stichting HIV Monitoring, AMSTERDAM, the Netherlands 21. Evaluation of a novel leptospirosis test in a Dutch population A.M. Zonneveld1, W.E. Fiets1, M.L. Hijmering2, J. Weel3 1 Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: a.m.zonneveld@mdl.umcg.nl, 2Isala Clinics, ZWOLLE, the Netherlands, 3Izore, LEEUWARDEN, the Netherlands Background: Management of primary HIV infection (PHI) remains controversial. We assessed the clinical benefit of temporary combination antiretroviral therapy (cART) during PHI. Methods: Patients with laboratory evidence of PHI were randomly assigned to receive no treatment, 24 or 60 weeks of cART (3-way randomization). If therapy was clinically indicated, subjects were randomized over the 2 treatment arms. Primary endpoints were the viral setpoint, defined as the plasma viral load (pVL) 36 weeks after randomization in the no treatment arm and 36 weeks after treatment interruption in the treatment arms, and the total time that patients were off therapy, defined as the time between randomization and start of cART in the no treatment arm, and the time between treatment interruption and restart of cART in the treatment arms. cART was (re)started in case of confirmed CD4 count <350 cells/mm3 or symptomatic HIV disease. Time off therapy was compared across study arms using KM plots and multivariate Cox survival analyses adjusted for confounding factors. Results: 173 patients were randomized. The modified ITT-analysis comprised 168 patients: 115 were 3-way randomized and 53 2-way randomized. In the 3-way randomized patients, mean age was 40 (SD 10) years, 96% were men, 84% were MSM, 73% had a negative or indeterminate Western blot and 83% were symptomatic during PHI. Mean viral setpoint was 4.8 (SD 0.6) log10 c/ml in the no treatment arm, and 3.9 (1.1) and 4.2 (1.0) log10 c/ml in the 24-and 60-week treatment arms (p<0.001). The mean CD4 count at viral setpoint in the no treatment arm was 381 (SD 167) cells/mm3, and 571 (195) and 528 (263) cells/ mm3 in the 24- and 60-week treatment arms (p<0.001). The median total time off therapy in the no treatment arm was 0.7 (95% CI, 0.2-1.2) years compared to 3.1 (2.3-3.8) and 2.1 (0.4-3.8) years in the 24- and 60-week treatment arms (Log-rank, p<0.001). Combining all treated patients, the median total time off therapy was not different between the 24- and 60-week treated patients (p=0.14). In the adjusted Cox analysis, independent predictors of time to (re)start of cART were pVL at setpoint (HR for each 1 log10 c/ml increase: 1.69 [95% CI 1.08-2.65], p=0.02), CD4 count at viral setpoint (HR for 1 log10 cells/mm3 increase: 0.002 [0.0-0.03], p<0.001) and temporary cART during PHI (HR 0.36 [0.19-0.7], p=0.003). Introduction: Leptospirosis is a bacterial infection which is uncommon in the developed world. Most cases are mild but some patients develop a severe infection with sepsis and shock. The Microscopic Agglutination Test (MAT) is the gold standard, however it is based upon serconversion, which takes several weeks. The Leptocheck (Zephyr) is a simple rapid serological test for leptospirosis, based upon anti-IgM and can therefore be used in early disease. Sensitivity and specificity have not been evaluated in a non-endemic environment. Aim: Evaluation of the sensitivity and specificity of the Leptocheck and description of clinical features, treatment and outcome leptospirosis in a Dutch cohort. Materials and methods: Between January 2004 and November 2008 we collected data for all patients with a leptospirosis infection who were admitted to one of the participating Centres. Data including clinical features, treatment and outcome were collected from the original medical records. The MAT was performed by the laboratory of Tropical Diseases (KIT) in Amsterdam. The Leptocheck was performed by experienced staff at the Laboratory of Infectious Diseases in Leeuwarden (Izore) and they were blinded for all previous test results. We added 50 sera of patients with Borrelia (n=15), Treponema (n=10), acute EBV (n=15) and acute CMV (n=10) to evaluate the specificity. Statistical significance was calculated with the McNemar test. Results: 28 Patients with leptospirosis were included. Eight patients were admitted to the ICU, three of them died. Mortality in this cohort was 15% and we found permanent impaired renal function in 10% of patients. The first MAT was positive in 10 of 28 patients, resulting in a sensitivity of 36%. The Leptocheck in the same sera was definite positive in 20/28 patients at admission resulting in a sensitivity of 71%. In 3/28 patients the test was weakly positive. Overall we found a sensitivity of 81% a specificity of 95% for the Leptocheck (p-value 0,0098). Conclusion: Establishing the diagnosis leptospirosis is mainly based upon medical history, clinical signs and 14 symptoms. Early and aggressive treatment should be started immediately. The Leptocheck is an excellent and statistical significant better test for leptospirosis with a higher sensititvity and specificity than the gold standard: the MAT. Hopefully better and faster diagnostics will improve outcome in leptospirosis, which is still unacceptably high. 22. higher than those reported in the original studies, using the MEDS and CURB-65. Feasibility-analysis showed missing laboratory items were the main reason why scoring systems could not be calculated completely. The MEDS, REMS and RAPS were most feasible since they could be calculated completely in more than 99%. Conclusion: In this study, the MEDS score predicted mortality in patients with sepsis visiting the ED best, although other scoring systems predicted mortality also fairly well. The MEDS, RAPS and REMS turned out to be most feasible. Overall, the MEDS score was the most adequate tool for predicting 28-day mortality in septic patients at the ED. Validity and feasibility of risk stratification scoring systems to predict 28-day mortality of septic patients in a Dutch emergency department P.M. Stassen1, J.M. Hilderink1, P. Leffers2, A.W. Hermans1, C. Keulemans1 1 Academic Hospital Maastricht, Department of Internal Medicine, MAASTRICHT, the Netherlands, e-mail: pstassen@home.nl, 2Department of Epidemiology, Maastricht University, MAASTRICHT, the Netherlands 23. Genito-urinary tuberculosis: easy to diagnose? M. Janssen1, C. Richter1, K. Hendricksen1, P.C. Weijerman1, J.W.R. Meijer1, C. Erkens2, R.C.G. Bruijnen1 1 Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: m3janssen@alysis.nl, 2KNCV Tuberculosis Foundation, THE HAGUE, the Netherlands Sepsis is a clinical syndrome which tends to progress rapidly to severe sepsis or septic shock and leads to high mortality rates. Early therapy has proven to decrease mortality; therefore a reliable risk stratification tool that quickly quantifies a patient’s risk of bad outcome would be helpful. Objectives: We selected six scoring systems. Our objectives were a) to investigate which scoring system predicts 28-day mortality best in septic patients in an emergency department (ED); b) to identify which scoring system is the most feasible score for the ED setting. Methods: This historical cohort study was performed in our secondary and tertiary university hospital. Patients were included when they visited the ED between August 2009 and August 2010, were seen by an internist in the ED, fulfilled the clinical criteria for sepsis, and were admitted to the hospital. The six scoring systems MEDS, CURB-65, SOFA, APACHE II, RAPS and REMS were assessed from patient charts and hospital databases. Primary outcome was all cause in-hospital mortality within 28 days. The discriminating ability of the scoring systems expressed as the area under the receiver operating characteristics (ROC) curve. Our observed mortality rates were compared with mortality reported in the original studies to assess the external validation. We assessed the feasibility of every scoring system by calculating the number of patients in which the score could be filled out completely in the ED. Results: A total of 664 patients were included, of whom 83 (12.5%) died within 28 days. The median age was 64 years. ROC-analysis showed that the MEDS score predicted mortality significant better than the RAPS and REMS score (p<0.005) and had the highest area under the curve (AUC =0.82, CI 0.77-0.87), although the other scoring systems were also fair predictors. Our mortality rates were Introduction: Genito-urinary tuberculosis (GUTB) is rarely seen. In the Netherlands about 25 cases every year have been detected over the last 10 years. Data of the national tuberculosis register indicate that the diagnosis is often made with a long doctor’s delay. Moreover, the diagnosis can easily be missed if it is not considered by the clinician and urine is not sent for specific TB examinations. The consequences of (especially late detected) GUTB can be severe like renal failure or infertility. In our hospital we diagnosed five patients in the last four years with GUTB. In a coproduction with urologists, a pathologist, a senior TB consultant at KNCV Tuberculosis Foundation and a radiologist we described these cases and hoped to provide some clues for physicians to diagnose GUTB. Cases: Two patients presented with a painless swelling of one of their testicles, after orchiectomy the pathology results showed a granulomatous inflammation. One of the patients had been treated for pulmonary tuberculosis (TB) about 30 years ago. Another patient presented with a, accidentally found, sterile leukocyturia. Urine was sent for TB examination and was positive. Retrospectively he had a renal calcification for about six years. A fourth patient, a woman, had symptoms of abdominal discomfort, urine incontinence and bladder retention. The fifth patient presented with a rectovesical fistula which needed operation. He developed disseminated TB shortly after the operation. This patient turned out to be HIV-positive. Background: As the cases describe, GUTB can present on different ways. Most patients complain of local symptoms like hematuria, abdominal pain and incontinence. About 15 23% has symptoms like fever and general discomfort. In the patients’ history a previous pulmonary TBC or originally being form a TBC endemic country can lead to the suspicion of GUTB. Radiographic clues are renal calcification or signs of (old) pulmonary TB. When granulomatous inflammation is found by pathological examination, tuberculosis should be considered as a possible diagnosis. When UGTB is suspected morning urine should be collected for three mornings in a row and be examined for Ziehl Neelsen, TB-cultures and PCR for tuberculosis. Once the diagnosis is established, therapy with tuberculostatics (rifampicin, isoniazide pyrazinamide and ethambutol) should be started. In general treatment of GUTB in the Netherlands is successful. Conclusion: GUTB is rarely seen, but can have severe consequences. It’s important to establish the diagnosis in an early stage and start with tuberculostatics. 24. pathways. MBL binding to its ligand was dose dependently prevented by recombinant rP8, however MASP-2 activity was unaffected. In addition, rP8 reduced complementmediated killing of B. burgdorferi s.l. by inhibiting formation of C5b-9 membrane attack complexes in vitro. Other complement effector functions, such as migration of human neutrophils towards Borrelia-induced inflammation and phagocytosis of B. burgdorferi s.l. by human neutrophils, were also inhibited by rP8. Importantly, in vivo experiments, in which mice were intradermally inoculated with Borrelia in the presence or absence of rP8, showed that rP8 inhibited inflammation and influx of leukocytes 18 hours after inoculation and we observed higher Borrelia numbers in murine skin 2 weeks post infection in mice inoculated with Borrelia in the presence of rP8. Conclusions: We here demonstrate, for the first time, that the MBL complement pathway is crucially important in the clearance of B. burgdorferi s.l. and that the novel tick salivary protein P8 facilitates survival of Borrelia by specifically inhibiting the MBL complement pathway. Currently, by RNAi in ticks and passive immunization studies in mice, we are determining the role of P8 in tick feeding and also Borrelia transmission, potentially identifying P8 as a candidate for an anti-tick vaccine to prevent Lyme borreliosis. A novel tick MBL complement pathway inhibitor facilitates survival of the causative agent of Lyme borreliosis T.J. Schuijt1 , J. Coumou 1, S. Narasimhan 2, J. Dai 2, T. van der Poll1, E. Fikrig2, J.W.R. Hovius1 1 Academic Medical Centre, Department of Internal Medicine, AMSTERDAM, the Netherlands, e-mail: j.w.hovius@amc.uva.nl, 2Yale University, School of Medicine, NEW HAVEN, CONNECTICUT, USA 25. Introduction: Lyme borreliosis – caused by Borrelia burgdorferi sensu lato and transmitted through Ixodes ticks – is the most prevalent arthropod-borne disease in the Western world. The estimated yearly incidence is approximately 133/100.000 inhabitants in the Netherlands. Upon entry of the spirochete into the host skin it is subjected to the host immune system. The complement cascade is a fundamental part of the mammalian innate immune response against both ectoparasites, e.g. Ixodes ticks, as well as the microbes they transmit, including the causative agent of Lyme borreliosis. Both ticks and Borrelia spirochetes are known to employ several strategies to circumvent activation of the complement system. Recently, using yeast display technology, we have identified multiple novel tick salivary proteins. One of these proteins, designated P8, was found to have anti-complement activity. Methods and results: In the current study, we demonstrate that p8 is expressed early during tick feeding and is upregulated in the presence of B. burgdorferi. Using standardized complement activity assays, we show that Drosophila-expressed recombinant P8 (rP8) specifically inhibited the human Mannose-binding lectin (MBL) complement pathway, but not the classical and alternative The lectin-like domain of thrombomodulin impairs host defense in murine pneumococcal pneumonia M. Schouten1, J. de Boer2, C. van ’t Veer2, J.J.T.H. Roelofs2, J.J.C.M. Meijers2, M. Levi2, T. van der Poll2 1 St Lucas Andreas Hospital, Department of Internal Medicine, AMSTERDAM, the Netherlands, e-mail: m.schouten@amc.uva.nl, 2 Academic Medical Centre, AMSTERDAM, the Netherlands Introduction: Thrombomodulin (TM) is an endothelial cell glycoprotein that, via distant structural domains, interacts with multiple ligands, thereby modulating coagulation, fibrinolysis, complement activation and inflammation. Recently, the lectin-like domain (LeD) of TM has been shown to interfere with monocyte and neutrophil adhesion, with complement activation and to block the activity of the pro-inflammatory cytokine HMGB1; factors which play an important role in bacterial infection. To date, the role of TMLeD in severe infection, like pneumonia and sepsis, is unknown. Worldwide, pneumococcal pneumonia is a frequent cause of sepsis and mortality. We here determined the role of TMLeD in our well established model of murine pneumococcal pneumonia. Aim: To determine the role of TMLeD in murine pneumococcal pneumonia. 16 Materials and methods: Ten weeks old wild-type (WT) and TMLeD KO mice were infected intranasally with viable <i>S. pneumoniae</i>. Animals were either observed in a survival study or sacrificed at 6, 24 or 48 hours after induction of pneumonia. Bacterial loads were determined in lung, blood, spleen and liver homogenates. Lung pathology was assessed. Pulmonary influx of neutrophils was determined by Ly-6G staining and measurement of levels of myeloperioxidase (MPO). Cytokine and chemokine levels were measured in lung homogenates and plasma. Activation of coagulation was determined by measurement of lung thrombin-antithrombin complexes (TATc). Results: TMLeD KO mice had a markedly better survival in pneumococcal pneumonia as compared to WT mice. Moreover, at 48 hours after induction of pneumonia, TMLeD KO had lower bacterial loads in blood and liver. At this time point, TMLeD KO mice showed less lung inflammation as evidenced by lower lung histopathology scores, less pulmonary neutrophil influx, MPO and chemokine levels. Moreover, at 24 and 48 hours plasma cytokine levels were lower in TMLed KO mice than in WT mice. In addition, at 48 hours after infection, lung TATc levels were lower in TMLeD KO mice than in WT mice. Conclusion: In pneumococcal pneumonia, TMLeD plays a detrimental role by hampering antibacterial defense at later time points, which results in higher bacterial loads, more pulmonary inflammation and activition of coagulation, more systemic inflammation and a higher mortality. Whether this can be attributed to a direct role of TMLeD in bacterial killing or to a role of TMLeD in modulating the inflammatory response in a negative way, needs to be addressed. 26. Introduction: Venous thrombosis has frequently been reported in patients with Cushing’s syndrome (CS). Aim: To evaluate the incidence of venous thromboembolism (VTE) in patients with CS prior to treatment onset and after surgery, in a multicentre cohort study Materials and methods: Medical records of all patients with endogenous CS of benign origin were reviewed among all university medical centres in the Netherlands. All objectively confirmed VTE’s during three years prior to, and three years after treatment onset, within the study period of January 1st, 1990 to June 6th, 2010, were documented. Patients surgically treated for non-functioning pituitary adenoma served as a control group for the incidence of post-operative VTE in adrenocorticotropic hormone (ACTH)-dependent CS. Incidences of VTE were expressed as incidence rates. Results: A total of 473 patients with CS (mean age 42 years, 363 women) were included (360 with ACTH-dependent CS). The total number of person years was 2526. Thirty-seven patients experienced a VTE during the study period, resulting in an incidence rate of 14.6 (95% confidence interval [CI] 10.3-20.1) per 1000 personyears. The incidence rate for first-ever VTE prior to treatment was 12.9 (95% 7.5-12.6) per 1000 person-years (17 events). The risk of post-operative VTE, defined as the incidence rate in three months after surgery, was 0% for ACTH-independent and 3.4 (95% CI 2.0-5.9%) for ACTH- dependent CS (12 events in 350 patients); most events occurred between 1 week and 2 month after surgery. Compared to the control group, the incidence rate ratio was 4.6 (95% CI 1.4-15.1%) for post-operative VTE in patients undergoing transsphenoidal surgery for ACTH-dependent CS. Conclusion: Patients with Cushing’s syndrome are at high risk of venous thromboembolism, especially during active disease and after surgery. General guidelines on the choice, intensity and duration of thromboprophylaxis are urgently needed. Incidence of venous thromboembolism in patients with Cushing’s syndrome: a multicentre cohort study D.J.F. Stuijver1, B. van Zaane1, J. Debeij2, S.C. Cannegieter2, R.A. Feelders3 , W. de Herder 3 , A.R. Hermus 4 , M.A. Wagenmakers4, G. van den Berg5, M.N. Kerstens5, E. Fliers6, P.M.J. Zelissen7, N. Schaper 7, M.L. Drent8, O.M. Dekkers2, V.E.A. Gerdes1, A.M. Pereira2 1 Academic Medical Centre/Slotervaarthospital Amsterdam, Department of Vascular/Internal Medicin,AMSTERDAM, the Netherlands, e-mail: d.j.stuijver@amc.uva.nl, 2Leiden University Medical Centre, LEIDEN, the Netherlands, 3 Erasmus Medical Centre, ROTTERDAM, the Netherlands, 4 Radboud University Medical Centre, NIJMEGEN, the Netherlands, 5University Medical Centre Groningen, GRONINGEN, the Netherlands, 6Academic Medical Centre, AMSTERDAM, the Netherlands, 7University Medical Centre Utrecht, UTRECHT, the Netherlands, 8VU University Medical Centre, AMSTERDAM, the Netherlands 27. The clinical effects of GLP-1 analogues added to insulin treated type 2 diabetes K. Hoogenberg Martini Hospital Groningen, Department of Internal Medicine, PO Box 30033, 9700 RM GRONINGEN, the Netherlands, e-mail: k.hoogenberg@mzh.nl Introduction: Type 2 diabetes mellitus (T2DM) is often complicated by obesity and insulin resistance. These are difficult to treat as lifestyle changes are tough and as blood glucose (BG) lowering is often accompanied by weight gain. GLP-1 analogues are a new pharmacologic modality registered for T2DM patient on oral antidiabetics (OAD) 17 Introduction: Results from our randomized controlled trial (RCT) showed that with continuous intraperitoneal (IP) insulin infusion with an implantable pump it is possible to achieve better glycemic control and quality of life (QoL) compared to subcutaneous insulin administration in patients with type 1 diabetes (T1DM) after 6 months of therapy. Aim: The aim of this analysis was to investigate patients therapy choice, QoL and glycemic control 30 months after the end of the trial. Materials and methods: The 23 patients that ended the RCT in 2007/2008 all continued to use the IP pump. Last known HbA1c values were collected in the 1st quarter of 2010. Status regarding therapy mode were extracted from hospital records. A questionnaire regarding QoL (SF-36, WHO-5), treatment satisfaction (DTSQ) and other parameters was sent to patients in the 2nd quarter of 2010. Paired t-tests were used to compare HbA1c at the end of the IP study phase with mean HbA1c at follow up. Results: In March 2010, 22 (12 female, 10 male) patients were still treated with IP insulin, 1 patient (female) was back on subcutaneous insulin due to neuropathic pains, which the patient blamed the IP pump for. Mean (SD) age at follow up was 46.6 (12.0) years; mean (SD) diabetes duration at the start of the study was 22.6 (10.6) years; mean HbA1c 8.6 (1.1)%; HbA1c > 7.5% in 20 subjects; hypoglycemic events =5/week in 14 subjects. HbA1c was collected at 2.3 (0.6) years (mean (SD)) after the end of the study. Mean (SD) HbA1c was 7.7 (1.1)%. Compared to the baseline HbA1c value, this is a significant reduction of 0.83% (CI; -1.3, -0.4). Compared to the end of the IP phase of the trial, the results are comparable (0.2% (CI; -0.3, 0.7). Regarding QoL, compared to baseline, at follow up scores on the SF-subscales ‘social functioning’, ‘vitality’, ‘bodily pain’, ‘general health‘ were significantly higher. Compared to the end of the IP trial, scores are at the same level at follow up. Conclusion: Our analysis shows that with IP therapy it is possible not only to improve glycemic control in the short term, but to achieve sustained improvement in glycemic control in patients with T1DM who were insufficiently controlled previously despite intensified subcutaneous insulin regimens. IP insulin therapy also continues to improves quality of life parameters and has a high patient satisfaction, with a low drop out rate (1 out of 23 of patients). that decrease HbA1c and body weight. These benefits may also account for T2DM on insulin. Limited experience in these patient show a variable weight loss and conflicting HbA1c effects. Aim: To investigate the effects of GLP-1 on HbA1c, insulin needs, body weight and costs of BG lowering medication in T2DM patients on insulin therapy. Materials and methods: GLP-1 was given to overweight (BMI > 35 kg/m2), insulin treated T2DM patients according to a prespecified protocol. Patients that started GLP-1 with OAD served as a comparison. HbA1c, body weight, daily insulin, OAD, and side-effects were recorded. Costs of BG therapy were calculated. Analysis of the outcome parameters was done at the time intervals of 0 to 3, 3 to 6, 6 to 9, 9 to 12 and 12 to 18 months. Results: A total of 157 patients (122 on insulin, 35 on OAD) started GLP-1 treatment. 142 continued GLP-1 therapy and 15 stopped.due to side-effects or lack of effects. 120 patients were analysed at 3 months follow-up, 81 at 6 months,57 at 9 months, 36 at 12 months and 9 at =18 months. At baseline, body weight was 118± 1,8 kg (mean±SE), BMI was 39,9± 0,5 kg/m2, HbA1c was 8,1± 0,1% and daily insulin was 123± 8 U. Body weight decreased linearly: -4,8±0,4 kg at 3 months, -6,4± 0,6 kg at 6 months, -6.4± 0,7 kg at 9 months, 7.3± 1,0 kg at 12 months and 6± 1,9 kg at =18 months, p<0.001 for all. HbA1c improved with -0,6± 0,09% at 3 months (p<0.001) and did not decline further. Overall insulin doses dropped with 33±16 U/day. Costs were approximately reduced by v 20,– so that overall extra costs of GLP-1 therapy were v 60,– per month. 38% Patients reported nausea and/or vomiting and 8% had other adverse events whereas 54% patients had no adverse events. Conclusion: GLP-1 analogues added to insulin in T2DM decreases body weight in a linear fashion, improves HbA1c values and is associated with significant decrease in insulin need leading to a modest decrease in the costs of these medication. 28. Sustained improvement of glycemic control and quality of life with continuous intraperitoneal insulin infusion in type 1 diabetes after 2.5 years of follow-up S.J.J. Logtenberg 1 , N. Kleefstra 2 , S.T. Houweling 3 , K.H. Groenier4, H.J.G. Bilo2 1 Isala Clinics, Department of Internal Medicine, PO Box, 8000 GK Zwolle, the Netherlands, e-mail: s.j.j.logtenberg@isala.nl, 2Diabetes Centre, Isala Clinics, ZWOLLE, the Netherlands, 3Langerhans Medical Research Group, ZWOLLE, the Netherlands, 4General Practice, University Medical Centre Groningen, GRONINGEN, the Netherlands 29. Risk of cancer in patients on insulin glargine in comparison to those on human insulin: results from a large population-based follow-up study R. Ruiter 1 , E. Visser 1, M.P.P. van Herk Sukel 2 , J.W.W. Coebergh1, H.R. Haak3, P.H. Geelhoed-Duivestijn 4, S.M.J.M. Straus5, R.M.C. Herings2, B.H.Ch. Stricker1 18 1 30. Erasmus Medical Centre, Department of Epidemiology, PO Box 2040, 3000 CA ROTTERDAM, the Netherlands, e-mail: r.ruiter@erasmusmc.nl, 2PHARMO Institute for Drug Outcomes Research, UTRECHT, the Netherlands, 3Máxima Medical Centre, EINDHOVEN, the Netherlands, 4Medical Centre Haaglanden, THE HAGUE, the Netherlands, 5College ter Beoordeling van Geneesmiddelen, THE HAGUE, the Netherlands Sustained cardiac remodeling after a short-term very low calorie diet in type 2 diabetes mellitus J.T. Jonker, M. Snel, S. Hammer, I.M. Jazet, R.W. van der Meer, H. Pijl, A.E. Meinders, A. de Roos, H.J. Lamb, J.A. Romijn, J.W.A. Smit Leiden University Medical Centre, Department of Endocrinology, Albinusdreef 2, 2333 ZA LEIDEN, the Netherlands, e-mail: j.t.jonker@lumc.nl Introduction: Several publications suggest an association between certain types of insulin and cancer but with conflicting results. However, whether use of different types of insulin may be a cause of cancer is an issue of ongoing debate. Aim: To analyze the hypothesis that the use of insulin glargine is associated with an increased risk of cancer in comparison to the use of human insulin. Methods: Data for this study were obtained from the PHARMO Record Linking System which includes drug dispensing records from community pharmacies linked on a patient level to hospital discharge records of approximately 2.5 million individuals in the Netherlands. Only incident users of insulin with prior use of oral glucose lowering drugs (OGLD) were included. The association between use of insulin glargine and cancer in comparison to use of human insulin was analyzed using Cox proportional hazard models with cumulative duration of drug use as a time-varying determinant. A fixed cohort analysis as well as an as treated analysis were performed. The first hospital admission with a primary diagnosis of cancer was considered as main outcome; specified cancers were analyzed as secondary outcome. Results were adjusted or stratified for age, sex, number of other unique drugs used in the year prior start of insulin, number of hospitalizations in the year prior to start of insulin, calendar time, the number of days of oral glucose lowering drug use in the year prior to start of insulin and use as of 1998, the average dosage per insulin category over the previously dispensed prescriptions, baseline dosage of first prescription of insulin and type of OGLD use prior to start of insulin. Results: 19,337 incident insulin users were enrolled, of whom 878 developed cancer. Use of insulin glargine was associated with a lower risk of malignancies in general in comparison to users with a similar length of use of human insulin (HR 0.73, 95% CI: 0.69-0.77); in contrast, an increased risk was found for breast cancer (HR 1.39, 95% CI 1.08-1.79). Conclusion: Users of insulin glargine had a lower risk of cancer in general than those on human insulin. The association might be a consequence of residual confounding or competing risk. However, like a previous study, we demonstrated an increased risk of the use of insulin glargine on the risk of breast cancer. Background: A very low calorie diet (VLCD) in patients with type 2 diabetes mellitus (T2DM) results in cardiac remodeling and improved diastolic function. It is unknown how long these effects sustain after reintroduction of a regular diet. Objective: To assess the long-term effects of initial weight loss by a VLCD on cardiac dimensions and function in T2DM patients. Materials and methods: Fourteen patients with insulindependent T2DM (mean±SEM: age 53±2 years; body mass index (BMI) 35±1 kg/m2) were treated by a VLCD (450 kcal/ day) during 16 weeks. Cardiac function was measured by magnetic resonance imaging before and after the 16-week VLCD and again after 14 months of follow-up on a regular diet. Results: BMI decreased from 35±1 kg/m2 to 28±1 kg/m2 after the VLCD and increased again to 32±1 kg/m2 at 18 months (both p<0.05 vs. baseline). Left ventricular (LV) end-diastolic volume index increased after the 16-week VLCD (80±3 to 89±4 ml/m2, p<0.05) and remained increased after 14 months of follow-up (90±3 ml/m2; p<0.05 vs. baseline) at comparable filling pressures. The improvement in LV diastolic function after the 16-week VLCD, was sustained after 14 months of follow-up (early (E)/atrial (A) diastolic filling phase ratio: 0.96±0.07 (baseline); 1.12±0.06 (after VLCD); 1.06±0.07 (18 months, p<0.05 vs. baseline)). Conclusion: Weight reduction by a 16-week VLCD in T2DM patients results in sustained cardiac remodeling and improved diastolic function after 14 months of follow-up, despite weight regain on a regular diet. 31. Familial longevity is marked by enhanced insulin sensitivity C.A. Wijsman, M.P. Rozing, T.C.M. Streef land, S. Le Cessie, S.P. Mooijaart, P.E. Slagboom, R.G.J. Westendorp, H. Pijl, D. van Heemst Leiden University Medical Centre, Department of Ouderengeneeskunde, PO Box 9600, 2300 RC LEIDEN, the Netherlands, e-mail: c.a.wijsman@lumc.nl Introduction: The mechanisms involved in human longevity are largely unknown. In the Leiden Longevity Study, we recruited long-lived siblings (aged 90 years or 19 older) and their offspring (mean age 60 years) to study familial determinants of longevity. These offspring show a 30% lower mortality rate compared to the general population. Their partners, whith whom they share their environment, do not have this mortality benefit, implying that the offspring have a familial predisposition for longevity. Previously we showed that the offspring had better glucose tolerance compared to their partners as controls. Aim: To compare insulin action between offspring from long-lived nonagenarian siblings and controls. Methods: We performed a two step hyperinsulinemiceuglycemic clamp in a subgroup of the Leiden Longevity Study comprising 24 subjects of which 12 offspring and 12 controls. Results: Offspring and controls were similar with regard to sex distribution, age and body composition. During the clamp study, a higher glucose infusion rate was required to maintain euglycemia during 40 mU/m2/min insulin infusion in offspring compared to controls (p=0.036), reflecting higher whole body insulin sensitivity. After adjustment for sex, age and fat mass, the insulin-mediated glucose disposal rate was higher in offspring than controls (42.5±2.7 vs. 33.2±2.7 mmol/kg * min, mean±SE, p=0.025). The insulin-mediated suppression of endogenous glucose production and lipolysis did not differ between groups (all p>0.05). Furthermore, the glucose disposal rate was positively and significantly correlated with the mean age of death of the parents in both the whole group (p=0.007) and the group of controls only (p=0.022). Conclusion: Offspring from long-lived siblings are marked by enhanced insulin sensitivity, suggesting a relation between familial longevity and insulin action. Future research will focus on identifying the underlying biomolecular mechanisms involved, with the aim to promote health in old age. 32. to the intensive care unit (ICU) have hypomagnesemia. For the emergency department (ED) setting, no information on this subject exists. Aim: This study aimed to (1) assess the number of serum magnesium determinations in the ED, (2) investigate the indication for determination of magnesium status, (3) determine the clinical implications of hypomagnesemia in the ED. Materials and methods: During a 3 month period (June until September 2010), we evaluated the charts of patients who visited the internist in the ED and in whom serum magnesium level was determined. From these charts, we retrieved why the magnesium level was determined, symptoms of hypomagnesemia, probable causes (medication, underlying disease) and other electrolyte imbalances, in-hospital mortality, cardiac dysrhythmias and treatment. Results: During 3 months, 1286 patients visited the ED. In 28 patients (2.2%), serum magnesium level was determined. In 27 patients admitted to the ICU/medium care unit (MCU), magnesium level was determined in 2 patients (7.4%) (later in 3 additional patients). Main reasons for determining magnesium level were chemotherapy (28.6%), gastro-intestinal loss (25%) and hypocalcemia (10.7%). In 10 patients (8 female, 2 male), magnesium was below 0.7 mmol/l, while in 2 of these, serum magnesium was below 0.5 mmol/l. Three patients (30%) had symptoms related to hypomagnesemia. No differences in mortality, ICU/MCU admission or admission duration were observed in those with a normal or low magnesium level. The probable causes of hypomagnesemia were gastro-intestinal loss (30%), renal loss due to cisplatin use (20%) and 2 (20%) used protonpump inhibitors. Less common causes were malnutrition and malabsorption due to pancreatic insufficiency. Magnesium suppletion was adequate in 4 patients (40%). Conclusion: Determination of serum magnesium levels is thought to be important in critically ill patients, but is determined in only a minority of internistic patients (2.2%) visiting the ED. Gastro-intestinal loss and medication (cisplatin, protonpump inhibitor) were at least in part responsible for low magnesium status in the majority of cases. Last, hypomagnesemia remained untreated in 60% of the patients. Determination and clinical implications of serum magnesium in the emergency department (ED) P.M. Stassen, Y.H.A.M. Kusters, M.J. Noeverman Academic Hospital Maastricht, Department of Internal Medicine, Karposthegge 19, 6225 KJ MAASTRICHT, the Netherlands, e-mail: pstassen@home.nl Introduction: Magnesium is a critical cofactor in ATP-powered reactions; therefore hypomagnesemia can have dramatic effects on metabolism. It also acts as a calcium channel antagonist, thereby affecting any activity driven by intracellular calcium concentration fluxes. Hypomagnesemia is described to be one of the most common electrolyte deficiencies. Approximately 10 to 20% of hospitalized patients and 50 to 60% of patients admitted 33. Cardiovascular drugs and sex differences in adverse drug reactions causing hospital admissions E.M. Rodenburg, B.H.Ch. Stricker, L.E. Visser Erasmus Medical Centre, Department of Epidemiology, PO Box 2040, 3000 CA ROTTERDAM, the Netherlands, e-mail: e.rodenburg@erasmusmc.nl 20 Background: Cardiovascular disease in women is often undervalued and drug effects of cardiovascular drugs differ between the sexes because of pharmacokinetic and pharmacodynamic differences. Adverse drug reactions (ADRs) within these drug classes may have serious consequences, leading to hospital admission. Aim: To study differences between men and women in hospital admissions for adverse drug reactions due to cardiovascular drugs. Methods: We conducted a nationwide study of all hospital admissions between 2000 and 2005 with data from the Dutch National Medical Register. Relative risks were calculated of hospital admissions due to the different cardiovascular drug groups for women compared to men. Risks were adjusted for the total number of hospital admissions, age and total number of prescriptions. Results: In total, 14,207 of the hospital admissions (34% of all ADR related admissions) were attributed to cardiovascular drugs (7,690 in women (54%; 95% CI 53%, 55%)). ‘Anticoagulants and salicylates‘ (n=8988), ‘high and low ceiling diuretics‘ (n=2242) and ‘cardiotonic glycosides’ (n=932) were responsible for the majority of the ADR-related hospital admissions. The most pronounced sex-differences were seen within low ceiling diuretics (RR 3.44; 95% CI 2.66, 4.43), cardiotonic glycosides (RR 1.92; 95% CI 1.66, 2.21), high ceiling diuretics (RR 1.73; 95% CI 1.57, 1.91) and coronary vasodilators (RR 0.66; 95% CI 0.56, 0.78). Conclusion: Clear sex differences exist in ADRs requiring hospital admission for different cardiovascular drug groups. Sex differences should be taken into account in the prescription and evaluation of drugs. 34. childhood cancer survivors described small populations, included one type of cancer or had a short follow-up time. Aim: This study assessed long-term effects on reproductive endocrine status in adult male five-year survivors of childhood cancer, evaluated treatment-related risk factors for the occurrence of disturbances in reproductive endocrinology and assessed the association between the FSH level and the later need for assisted reproductive techniques. Methods: The study cohort included adult male five-year survivors of childhood cancer treated in the Emma Children’s Hospital/Academic Medical Centre between 1966 and 2003. Survivors who had reached the age of at least 18 years on January 1st 2008 were eligible for this study. Data concerning patient and treatment characteristics, endocrine status (FSH, LH and testosterone levels), fertility and pregnancy outcome were collected. Multivariate regression analyses were performed to evaluate treatment-related risk factors for disturbances in reproductive endocrinology. The diagnostic and predictive values of elevated FSH levels and later need for assisted reproductive techniques were evaluated. Results: Data on reproductive endocrine status were available for 488 survivors (86.4%) of the 565 male survivors who visited the outpatient clinic for the first time after their 18th birthday. The median follow-up time until first visit to the outpatient clinic was 15 years (range: 5.0-39.0 years). The prevalence rates of elevated FSH levels and decreased testosterone levels were 33% and 12%, respectively. Use of procarbazine, cyclophosphamide, vinca-alkaloids, other alkylating agents, pelvic/abdominal irradiation, total body irradiation (TBI) and surgery of the testicular region were identified as treatment-related risk factors for elevated FSH levels, and TBI was the only risk factor for a decreased testosterone level. During the follow-up period, 73 men reported 120 conceptions, which resulted in 103 live births. All men whose partners conceived by assisted reproductive techniques (n=13) had elevated FSH levels (sensitivity: 100%; 95% CI: 71%-100%) and all male survivors with a normal FSH level did not need assisted reproductive techniques (negative predictive value: 100%; 95% CI: 89%-100%). Conclusion: One third of adult male survivors of childhood cancer has elevated FSH levels. FSH is a sensitive marker for the need of assisted reproductive techniques in male childhood cancer survivors. Reproductive status in adult male long-term survivors of childhood cancer J.J.M. Claessens1 , K. Tromp1,2 , S.L. Knijnenburg 2,3 , H.J.H. van der Pal2,3, F.E. van Leeuwen 4, H.N. Caron2, C.C.M. Beerendonk1, L.C.M. Kremer5 1 Radboud University Medical Centre Nijmegen, Department of Obstetrics and Gynaecology, PO Box 9101, 6500 HB NIJMEGEN, the Netherlands, e-mail: j.claessens@obgyn.umcn.nl, 2Emma Children’s Hospital/ Academic Medical Centre, Amsterdam, the Netherlands, 3 Academic Medical Centre, AMSTERDAM, the Netherlands, 4 the Netherlands Cancer Institute, AMSTERDAM, the Netherlands Introduction: Between the 1960s and 1990s, five-year survival for childhood cancer increased from 23% to 70% due to advances in treatment. Unfortunately, iatrogenic reproductive failure and endocrine disturbances are frequently encountered late effects which have major impact on quality of life. Previous studies on late effects in 35. Patient selection for oncology phase i trials – a multiinstitutional study of prognostic factors M.H.G. Langenberg1, D. Olmos2, R. A’Hern3, S. Marsoni 4, J. Tabernero5, C. Gomez-Roca6, J. Verweij7, P. Schoffski8, J. Ern Ang3, N. Penel9, J.H.M. Schellens10, L. Gianni11, 21 A.T. Brunneto2, J. Evans12, R. Wilson13, C. Sessa14 , R. Plummer 14 , R. Morales5, J.C. Soria6, S.B. Kaye2, M. Lolkema15 1 University Medical Centre Utrecht, Department of Medical Oncology, Heidelberglaan 100, 3584 AX UTRECHT, the Netherlands, e-mail: m.langenberg@umcutrecht.nl, 2The Royal Marshden NHS Foundation Trust, SUTTON, United Kingdom, 3The Institute of Cancer Research, SUTTON, United Kingdom, 4Southern Europe New Drug Organization Foundation, MILAN, Italy, 5Vall d’Hebron University Hospital, BARCELONA, Spain, 6Institut Gustav Roussy, VILLEJUIF, France, 7Erasmus Medical Centre, ROTTERDAM, the Netherlands, 8University Hospital Gasthuisberg, LEUVEN, Belgium , 9 Centre Oscar Lambret, LILLE, France, 10the Netherlands Cancer Institute, AMSTERDAM, the Netherlands, 11Fondazione IRCCS Instituto Nazionale dei Tumoni, MILAN, Italy, 12 The Beatson West of Scotland Cancer Centre, GLASGOW, United Kingdom, 13Centre for Cancer Research & Cell Biology, QUEEN’S UNIVERSITY BELFAST, United Kingdom, 14Instituto Oncologico della Svizzera Italiana, BELLINZONA, Switzerland, 15University Medical Centre Utrecht, UTRECHT, the Netherlands number of metastatic sites, clinical tumour growth rate, lymphocytes and WBC. Prognostic models for 90-day mortality derived from these factors achieved specificities > 85% and sensitivities of ~50%. These overall were not superior to a previously published RMH score. Conclusions: Patient selection using scores comprising 3 to 7 prognostic factors will reduce 90-day mortality in Phase I trials by half. However, their adoption should be balanced against a reduction in recruitment to Phase I studies by 20%. These data show that we can modestly improve the risk/benefit ratio for participants in early clinical trials. A further major improvement in patient selection will be derived by the application of predictive molecular biomarkers which reflect tumour and host biology. BMI was not associated with OS in 730 patients who participated in the CAIRO2 study, although a trend was observed (median OS 16.6, 17.8, 21.0, and 21.4 months for BMI categories I, II, III and IV, respectively; p=0.8068). Conclusions: These results show that BMI is an independent prognostic factor for survival in patients receiving chemotherapy, but not in patients receiving chemotherapy and targeted therapy. The possible decreased efficacy of bevacizumab in obese patients may explain this discrepant result. The role of BMI in patients receiving targeted therapy should be further tested 36. J. Hofland1, R.A. Feelders1, R. van der Wal1, M.N. Kerstens2, H.R. Haak3, W.W. de Herder1, F.H. de Jong1 1 Erasmus Medical Centre, Department of Internal Medicine, Dr. Molenwaterplein 50-60, 3015 GE ROTTERDAM, the Netherlands, e-mail: j.hofland@erasmusmc.nl, 2University Medical Centre Groningen, GRONINGEN, the Netherlands, 3 Máxima Medical Centre, EINDHOVEN, the Netherlands Influence of body mass index on outcome in advanced colorectal cancer patients receiving chemotherapy with or without targeted therapy L.H.J. Simkens1, M. Koopman2, L. Mol3, G.J. Veldhuis4, D. ten Bokkel Huinink5, E.W. Muller6, V.A. Derleyn7, S. Teerenstra1, C.J.A. Punt1 1 Radboud University Medical Centre Nijmegen, Department of Medical Oncology, PO Box 9101, 5600 HB NIJMEGEN, the Netherlands, e-mail: l.simkens@onco.umcn.nl, 2University Medical Centre Utrecht, UTRECHT, the Netherlands, 3 Comprehensive Cancer Centre East (IKO), NIJMEGEN, the Netherlands, 4 Antonius Hospital, SNEEK, the Netherlands, 5 Diakonessenhuis, UTRECHT, the Netherlands, 6Slingeland Hospital, DOETINCHEM, the Netherlands, 7Elkerliek Hospital, HELMOND, the Netherlands Introduction: The selection of appropriate cancer patients for early clinical trials represents a challenge due to the difficult underlying risk/benefit assessments. The main ethical challenge for these studies is that therapeutic utility is not a conventional primary endpoint of these dose and toxicity-finding studies while potential patients are vulnerable due to the presence of advanced, progressive malignant disease coupled to the lack of standard treatment options. Many reported studies have attempted to address these issues but are severely limited due to small patient numbers and larger inter-practice heterogeneity. Aim: This study aims to define prognostic factors to guide risk/benefit assessments using a large patients database from multiple Phase I units. Methods: Data were collected from 2182 eligible patients treated in Phase I trials between 2005 and 2007 in 14 different institutions. We derived and validated independent prognostic factors for 90-day mortality. Results: The 90-day mortality was 16.5% with a drugrelated death rate of 0.4%. Trial discontinuation within 3 weeks occurred in 14% of patients, due to disease progression in the majority. Overall objective radiologic response rate was 9.82%, disease stabilization rate at 3 and 6 months were 26.05% and 10.1%, respectively. The proportion of patients who had progressive disease at first imaging evaluation was 49.53%. The median PFS was 10.9 weeks (95% CI: 10.2-11.5). We derived and validated eight different prognostic variables for 90-day mortality: performance status, albumin, lactate dehydrogenase, alkaline phosphatase, Introduction: Obesity is associated with an increased risk of development and recurrence of colorectal cancer. However, the role of obesity in advanced colorectal cancer (ACC) patients is unknown. We investigated the effect of body mass index (BMI) on overall survival (OS) in ACC patients receiving systemic treatment in two large phase III studies (CAIRO and CAIRO2, Dutch Colorectal Cancer Group). Patients and methods: Treatment data were obtained and analyzed from 796 ACC patients who were treated with chemotherapy in the CAIRO study, and in 730 ACC patients who were treated with chemotherapy plus targeted therapy in the CAIRO2 study. Baseline height and weight were used to assign patients to one of the following BMI categories: I (< 18.5 kg/m2), II (18.5-24.9 kg/m2), III (25.0-29.9 kg/m2) and IV (= 30.0 kg/m2). Results: In 796 patients of the CAIRO study a high BMI was associated with better median OS (8.0, 14.9, 18.4, and 19.5 months for BMI categories I, II, III, and IV, respectively; p=0.001), and was an independent prognostic factor for OS in a multivariate analysis. 22 37. Conclusion: Inhibin pro-aC is produced by the adrenal gland and its serum levels may serve as a tumor marker for adrenocortical carcinomas. 38. Surgery in adrenocortical carcinoma; importance of national cooperation and centralized surgery I.G.C. Hermsen1 , T.M.A. Kerkhofs2, G. den Butter2, J. Kievit3, C. Eijck 4, E. Nieveen van Dijkum5, H.R. Haak2 1 Máxima Medical Centre Eindhoven/Veldoven, Department of Internal Medicine, De run 4600, 5504 DB VELDHOVEN, the Netherlands, e-mail: i.hermsen@mmc.nl, 2Máxima Medical Centre, EINDHOVEN/VELDHOVEN, the Netherlands, 3 Leiden University Medical Centre, LEIDEN, the Netherlands, 4 Erasmus Medical Centre, ROTTERDAM, the Netherlands, 5 Academic Medical Centre, AMSTERDAM, the Netherlands Serum inhibin pro-alphaC is a tumor marker for adrenocortical carcinomas Introduction: The low incidence rate of adrenocortical carcinoma requires a multidisciplinary approach in which specialised surgery has an essential role as complete resection of the primary tumour is the only chance of cure. In order to improve patient care, insight into surgical results within the ACC population is essential. In 2007, a Dutch Adrenal Network Registry has been created encompassing care and outcome of patients treated for ACC in the Netherlands since 1965. Using this database a study was performed with the following objectives: (1) to gain insight into surgical performance in the Netherlands, (2) to compare surgical data with international literature. Patients and methods: The data of 175 patients treated from 1965 until January 2008, were studied. The following data were collected; age, gender, functionality of the tumour, stage at diagnosis (ENS@T staging), surgical procedure, completeness of surgery, disease recurrence, adjuvant mitotane therapy, recurrence free survival and overall survival. Results: 149 patients were operated. Patients with complete resection had significantly longer survival than patients with incomplete resection (p=0.01). Patients operated in a Dutch Adrenal Network centre had significantly longer survival in both univariate (p=0.01) and multivariate analysis (p=0.01). Significant longer survival was observed in operated stage IV patients compared to non-operated patients (p=0.00). Conclusion: Our data confirm the relevance of national cooperation and centralized surgery in ACC. In selected patients with stage 4 disease surgery can be beneficial in extending survival. On the basis of the retrospective analysis surgery in the Netherlands will and can be improved. Introduction: The increased detection rate of adrenal incidentalomas and the lack of diagnostic accuracy of currently available tests for differentiation between benign and malignant adrenocortical disease emphasize the need for novel tumor markers for adrenocortical carcinoma (ACC). Aim: Since the inhibin a-subunit is expressed within the adrenal cortex and inhibins can serve as ovarian tumor markers, the role of serum inhibin pro-aC as tumor marker for ACC was studied. Materials and methods: In vivo regulation of adrenal pro-aC secretion was investigated by adrenocortical function tests. Serum inhibin pro-aC levels were measured in controls (n=181) and patients with adrenocortical hyperplasia (n=45), adenoma (ADA, n=32), ACC (n=32) or non-cortical tumors (n=12). Steroid hormone, adrenocorticotrophin (ACTH) and inhibin A and B levels were also estimated in subsets of patients. In ten ACC patients samples were collected before and after treatment. Results: Serum inhibin pro-aC levels increased after stimulation with ACTH (p=0.043). ACC patients had higher serum inhibin pro-aC levels than controls (p<0.0001) and patients with adrenocortical hyperplasia, ADA or other adrenal tumors (p=0.0003). Inhibin pro-aC measurement in ACC patients had a sensitivity of 59% and specificity of 84% for differentiation from ADA patients. ROC analysis displayed areas under the curve of 0.87 for ACC versus controls and 0.81 for ACC versus ADA (both p<0.0001). Surgery or mitotane therapy was followed by a decrease of inhibin pro-aC levels in all ACC patients tested (p=0.0065). 23 39. Sunitinib-induced hypothyroidism is associated with induction of deiodinase type 3 activity and capillary regression well as a decreased vessel-to-follicle ratio in 5 high power fields compared to controls (0.31±0.02 vs. 0.96±0.10; p<0.0001). Conclusion: Sunitinib induces thyroid dysfunction in both patients and rats which is due to the combination of thyroid capillary regression and alterations in T4/T3 metabolism. M.H.W. Kappers1, J.H.M. van Esch1, F.M.M. Smedts2, R.R. de Krijger1, K. Eechoute1, R.H.J. Mathijssen1, S. Sleijfer1, F. Leijten1, A.H.J. Danser1, A.H. van den Meiracker1 1 Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: m.h.w.kappers@erasmusmc.nl, 2Reinier de Graaf Gasthuis, DELFT, the Netherlands Introduction: Blocking vascular endothelial growth factor (VEGF)-mediated signaling by the VEGF receptor tyrosine kinase inhibitor sunitinib is an established treatment for various types of cancer, but is associated with thyroid dysfunction. Aim: To obtain more insight into the mechanisms causing thyroid dysfunction. Materials and methods: The effects of sunitinib on thyroid function and thyroid hormone metabolism were studied in patients with metastatic renal cell carcinoma or gastrointestinal stromal tumors participating in a retro- (n=108) or prospective (n=15) study. In addition, in Wistar Kyoto rats the effects of sunitinib administration (n=9) for 8 days and sunitinib withdrawal (n=7) for 11days on thyroid function, hepatic type 1 (D1) and type 3 (D3) deiodinase, urinary thyroid hormone excretion, and thyroid histology were assessed and compared to control rats (n=6). Results: Retrospective analysis in patients demonstrated that 42% of the 83 evaluable patients developed elevated TSH levels (TSH > 5.0 mU/l), which in 14% of patients was preceded by TSH suppression, occurring equally in men and women. In 20% of patients with elevated TSH levels, TSH rose above 10 mU/l. Prospective analysis in 15 patients showed an increase in TSH levels from 1.12±0.26 to 4.27±1.23 mU/l already after 10 weeks of treatment, accompanied by a decrease in T3/rT3-ratio, indicating enhanced thyroid hormone metabolism. Anti-thyroid peroxidase antibodies did not change during treatment with sunitinib. In rats on sunitinib, hepatic D3 activity was increased (0.22±0.01 fmol/min/mg vs. 0.14±0.02 fmol/ min/mg) and D1 activity was decreased (12.6±1.2 pmol/ min/ml vs. 20.6±0.9 pmol/min/ml; p<0.05), accompanied by decreased serum T4 (43.9±1.8 nmol/l vs. 61.3±3.7 nmol/l; p<0.05) and T3 levels (0.74±0.05 nmol/l vs. 0.94±0.05 nmol/l; p<0.05) compared to control rats. Changes in both deiodinase activities were reversible after treatment discontinuation, but thyroid hormone levels did not normalize. Urinary excretion of T3 and T4 was very low at baseline and did not change during sunitinib administration. Histological examination of haematoxilin-eosinstained thyroid sections showed a decrease in total vessel number in rats on sunitinib (36±3 vs. 71±8; p<0.0001) as II. ORAL PRESENTATIONS CASE REPORTS 40. A rare cause of febris eci: intravascular large cell lymphoma J.L. Witmer, W.M. Smit, G.J. Kootstra, Chr.H.H. ten Napel, J. van Baarlen Medical Spectrum Twente, Department of Internal Medicine, Ariensplein 1, 7500 KA ENSCHEDE, the Netherlands, e-mail: jorindewitmer@hotmail.com Case: A 83-year-old female with a history of hypertension, hysterectomy and subclinical hypothyroidism was admitted to the hospital because of fever and malaise. No abnormalities were found on physical examination. Laboratory testing showed a normocytic anemia, erythrocyte sedimation rate of 59 mm/h, mild hyponatremia (132 mmol/l), and LDH 645 U/l (n <450). Chest-X-ray, ultrasound of liver and spleen, and CT-scan of thorax and abdomen revealed no abnormalities and no explanation for the fever. Cultures of feces, sputum and blood were all negative. A bone marrow biopsy showed no abnormalities; the mycobacterial culture was negative. Additional laboratory test revealed panhypopituitarism without involvement of the pituitary-adrenal axis (TSH 0.73 mU/l, FT4 6.5 pmol/l, T3 < 0.62 nmol/l, IGF-1 32 mg/l, ACTH 3.6 pmol/l, cortisol 0.5 mmol/l, prolactine 0.57 U/l, LH < 1.0 U/l, FSH 8.2 U/l, oestradiol 140 pmol/l, urine cortisol 560 nmol/24h). An MRI of the brain showed a considerably large pituitary gland (9 mm) compatible with an adenoma probably ACTH-producing. A few weeks later the patient was admitted again because of persisting fever, headache and hypotension. The anemia was progressive (4.8 mmol/l), trombocytes were 108 x 10?/l, and LDH 1442 U/l, suggesting (micro-angiopathic) intravascular hemolysis. During fluid challenge, she developed right-sided heart failure and acute renal failure, although an ultrasound of the heart showed a normal left ventricular function and only a slightly elevated serum NTproBNP. The situation deteriorated quickly and she died. Autopsy revealed a intravascular large B-cell-lymphoma in the small en larger vessels of the lungs and pituitary gland. Localization in the lung-vessels caused hypoxemia and 24 Initially, a cathastrophic antiphospholipid syndrome was suspected, but could not be confirmed (LAC test, B2GP1 antibody test and ACA were all negative). Additional diagnostic and laboratory investigations for (un)common coagulation disorders like vasculitis, cardiac embolus, factor V Leiden, prothrombin G20210A or JAK2 V617F gene mutation and paroxysmal nocturnal hemoglobinuria (PNH) showed no abnormalities. Because we could not identify a disorder associated with arterial thrombosis, we hypothesize that desmopressin in an oral dose of at least 0.2mg must have been the cause of this dramatic vascular complication (the exact dose she took was unclear and unfortunately a desmopressin level could not be measured). Indeed, factor VIII activity, vWF activity ristocetin cofactor and vWF antigen were strikingly elevated (268%, 590%, 740% respectively). We believe this could be a desmopressin effect, although we realize that major ischaemia may have contributed to this remarkable elevation. Thrombotic events (cerebrovascular accidents and acute coronary syndromes) associated with the use of desmopressin are rare and have only been described after intravenous administration. Our patient used oral desmopressin. Conclusion: To the best of our knowledge this is the first report suggesting a relationship between oral desmopressin use and life-threatening abdominal arterial thrombosis. probably leukostasis a, resulting in an elevated pressure in pulmonary vessels which cardial ischemia and secondary heart failure. There was only a minimal presence of the lymphoma in the bone marrow. Discussion: Intravascular large B-cell lymphoma (ILCL) is a rare subtype of large cell lymphoma with an unknown incidence. Patients present with a variety of symptoms caused by occlusion of small vessels. The majority of patients have B-symptoms and any organ can be involved. The clinical presentation seems to be dependent of the country of origin. Conclusion: We present a patient with fever (of unknown origin),heart failure and pituitary gland insufficiency caused by infiltration of small and larger vessel by an intravascular large B-cell lymphoma. 41. An unusual case of abdominal arterial thrombosis in a young woman using desmopressin E.J.M. Schrijver, W. Deenik, H. Chon, N.Koedam., A. Spoelstra-de Man Tergooi Hospitals Hilversum, Department of Intensive Care, Michelangelostraat 7-2, 1077 BN AMSTERDAM, the Netherlands, e-mail: ejm.schrijver@gmail.com Introduction: Desmopressin, a synthetic vasopressinanalogon, is prescribed for the treatment of nocturnal enuresis. It stimulates the release of factor VIII and promotes the release of Von Willebrand factor (vWF), also making it an effective drug for coagulation disorders. Case: A 27-year-old woman presented at the emergency room with a 7-week history of abdominal pain and diarrhoea. Her medical history included borderline personality disorder with multiple hospital admissions. Because of nocturnal enuresis, she used desmopressin 0.2 mg once daily since three months in combination with aripiprazole, citalopram, alprazolam and topiramate. On physical examination her vital signs were normal. Abdominal examination revealed normal bowel sounds with diffuse abdominal pain without muscular defense. Rectal examination was normal. Her laboratory results showed: sodium 132 mmol/l, potassium 3.3 mmol/l, C-reactive protein 180 mg/l, leukocytes 23.7 x 109 IU/l (10% band-forms), lactate 4.8 mmol/l and creatinine 47 umol/l. An abdominal CT scan was not conclusive. An exploratory laparotomy revealed small bowel ischaemia due to occlusion of the celiac trunk and superior mesenteric artery. A thrombectomy of these arteries was performed. The majority of the small bowel was resected, leaving a residual small intestinal length of less than 100cm. An aortahepatic bypass was made because remarkably, thrombosis of the celiac trunk recurred during the procedure, suggestive of a coagulation disorder. 42. Thrombotic microangiopathy in new-onset systemic lupus erythematosus Y. Sandberg, M.F. Durian, S.P. Berger, E. Hoorn Erasmus Medical Centre Rotterdam, Department of Internal Medicine, S’-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: y.sandberg@erasmusmc.nl Case: A 25-year-old Cambodian woman was admitted to a general hospital because she had been feeling unwell for two weeks and had a subfebrile temperature (38.0 °C). Her previous medical history included tuberculosis in 1999 with vertrebral involvement leading to partial paraplegia. Furthermore, a presumptive diagnosis of rheumatoid arthritis (RA) was made based on an arthritis of her hands and positive anti-cyclic citrullinated antibodies. She was being treated with methotrexate (25 mg/week) and folic acid. On admission, she was given antibiotics because of suspected pneumonia. Pancytopenia was also noted, which was ascribed to the use of methotrexate. Three days later, however, she developed a sudden and transient loss of vision and seizures, after which she was transferred to the intensive care unit. There, hemolysis with schistocytes and renal insufficiency were noted, raising the 25 possibility of thrombotic thrombocytopenic purpura (TTP). Her blood pressure was variable, but reached a maximum of 160/110 mmHg. Although a normal ADAMTS13 activity (58%) was detected, plasmapheresis and prednisone were started. She was transferred to our university hospital for further analysis and treatment. After four days of plasmapheresis, an ADAMTS13 activity of 91% was found and plasmapheresis was discontinued and analysis for other causes was started. No known association between methotrexate and TTP was found and plasma levels of methotrexate were undetectable. Other causes were also excluded, including human immunodeficiency and parvo B19 viruses, pregnancy, and the antiphospholipid syndrome. Ultimately, a diagnosis of systemic lupus erythematosus (SLE) could be established based on the previously observed arthritis, pancytopenia, positive antinuclear antibodies (1:2560 dilution, normal < 1:80), anti double-stranded DNA antibodies (215 IU/ml, normal < 10 IU/ml), and diffuse glomerulonephritis with global involvement (class IV-G SLE nephritis). Treatment with prednisone, mycophenolate mofetil and angiotensin converting enzyme inhibitors led to complete remission. Conclusions: New-onset SLE can be complicated by thrombotic microangiopathy with normal ADAMTS13 activity. Possible explanations include a hypertensive crisis and TTP. These were difficult to differentiate in this particular case, because SLE nephritis was accompanied by hypertension. It is important to recognize that TTP in SLE is divided into two separate entities based on normal and low ADAMTS13 activity. Only the latter category requires plasmapheresis. Although incompletely understood, TTP in SLE with normal ADAMTS13 activity carries a worse overall prognosis. The second teaching point is that anti-cyclic citrullinated antibodies can be positive in SLE and therefore SLE should always be excluded prior to diagnosing RA. 43. He used salmeterol/fluticasone and mometasone furoate for a mild COPD. Perindopril, metoprolol, spironolactone and acenocoumarol were recently prescribed by the cardiologist. Physical examination showed a blood pressure of 90/60 mmHg and peripheral oedema. Initial aberrant laboratory tests were haemoglobin 7.7 mmol/l, erythrocyte sedimentation rate 63 mm/h, C-reactive protein 34 mg/l and a total protein of 85 g/l (without M-protein). Cardiomyopathy, polyneuropathy and eosinophilia each have a large differential diagnosis. After a thorough work up it was concluded that the underlying disorder was a primary hypereosinophilia. Therefore the differential diagnosis was narrowed to chronic eosinophilic leukaemia (CEL), CEL unclassified, T-cell mediated hypereosinophilic syndrome (HES) and HES. Because testing for the FIP1-like-1-platelet-derived growth factor receptor-fusion protein (FIP1L1-PDGFRalpha) was negative, CEL was excluded. Bone marrow examination showed 30% eosinophils; no blasts, mast cells, fibrosis or cytogenetical abnormalities were found. There was a normal T-cell subset at immunophenotyping. Molecular cytogenetical studies were negative for JAK2, BCR-ABL and KIT D816V mutations. A skin-fascia-muscle biopsy showed eosinophilic fasciitis and eosinophilic myositis. With those results a systemic mastcytosis, CEL unclassified and T-cell associated HES were excluded and the diagnosis HES was made. Our patient fulfilled the WHO criteria for idiopathic HES; an eosinophil count > 1.5 x 109/l for more than six months, exclusion of reactive eosinophilia as well as eosinophilia associated with neoplasias, and evidence of tissue damage as result of hypereosinophilia. Although our patient was FIP1L1-PDGFRalpha negative, treatment with imatinib 100 mg per day was started. After 10 weeks of therapy he experienced a better condition, less neuropathy and a weight gain of 4 kg. His white blood cell count normalized and the eosinophils dropped to < 2 x 109/l. Discussion: There are some more case reports of patients with FIP1L1-PDGFRalpha negative HES responsive to imatinib, indicating that an as yet unidentified target of imatinib is responsible for HES in these cases. A patient with cardiomyopathy, polyneuropathy and an eosinophilia: a diagnostic challenge C. Bethlehem, P. Joosten Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: carina.bethlehem@znb.nl 44. Ungoing HIV replication in cerebrospinal fluid under longterm ritonavir/lopinavir monotherapy M. Bierhoff1, C.A.B. Boucher2, J. Kuster1, R.W. ten Kate1 Kennemer Gasthuis, Department of Internal Medicine, Boerhaavelaan 22, 2035 RC HAARLEM, the Netherlands, e-mail: m.bierhoff@kg.nl, 2Erasmus Medical Centre, ROTTERDAM, the Netherlands Case: A 56-year-old male patient with a recently diagnosed cardiomyopathy and sensorimotor axonal polyneuropathy was seen because of an eosinophilia (4.8-8.8 x 109/l), existing for more than one year. During the past three months he was complaining about dyspnoea d’effort, deafness in his feet and progressive weight loss. There were no signs of fever, cough, muscle pains, pruritus or diarrhoea. Our patient did not smoke or use much alcohol. 1 Case: A 57- year HIV infected man was started on highly active antiretroviral therapy (HAART) in 1999 at CD4 26 count of 620 x 106/ml and HIV-1 viral load of 114 copies/ ml on a regimen of lamivudine/zidovudine 150/300 mg twice daily and nevirapine 200 mg twice daily. Due to side effects of different regimens available at that time he was ultimately successfully treated from 2001 with mono therapy at first nelfinavir and subsequently ritonavir/ lopinavir (r/lPV) 50/200 twice daily 2. At that point his HIV-1 viral load in serum was almost always beneath 400 copies/ml. This regimen was kept unchanged until he presented in 2010 with dysarthria, dysfagia, dyskinesia and tremor. A cerebral MRI showed changes in white matter. A lumbar puncture was performed. Cerebrospinal fluid (CSF) was negative for cytomegalovirus, Epstein-Barr virus, herpes simplex virus, JC virus, varicella zoster virus, enterovirus. HIV-1 viral load was 4500 copies/ml in CSF with serum viral load of 400 copies/ml and a CD4 count of 930 x 106/ml. LPV level in CSF 6 hours after intake was 0.07 mg/l and serum level 11.0 mg/l in plasma. This is a normal plasma/CSF ratio. His regimen was switched to etravirine 400mg twice daily and lamivudine/zidovudine 150/300mg twice daily and after two months the HIV-1 RNA viral load was again undetectable in both serum as well as in CSF but the patient remained clinically unchanged. Conclusion: Despite a longstanding suppression of viral replication in plasma we found substantial viral replication in the CSF possibly responsible for the symptoms and signs in our patient. Our observation support the suggestion from recent literature that with mono therapy with ritonavir/lopinavir is not 45. Biopsies revealed chronic inflammation with granuloma formation, suggestive for early Crohn’s disease (CD). After exclusion of (latent) TBC infection using an IGRA-test and X-thorax, a ‘top-down’ regimen was started consisting of prednisone, azathioprine and remicade. However, complaints remained and fever developed. A CT-scan showed infiltration surrounding the coecum and terminal ileum without abscess. The patient underwent an extensive ileocecal resection. During surgery, multiple lesions on the peritoneum and small intestine were found. Cultures of resection material were positive for M. tuberculosis. A Mantoux test was strongly positive. After initiation of appropriate treatment, the patient recovered. Case 2: A 75-year-old Italian man was admitted for general malaise, chest pain and confusion. Physical examination was normal. Laboratory revealed slightly elevated CRP, blood cultures were negative. CT angiography showed a thoracic aortic aneurysm of 7.2 cm and multiple perilymphatic pulmonary nodules. Sarcoidosis and tuberculosis were considered. Bronchoalveolar lavage (BAL) and surgery were postponed due to the aneurysm and the patient’s poor condition, respectively. The patient had a BCG scar, an IGRA test was negative. A liver biopsy showed granulomatous inflammation with a negative ZN stain. Treatment for sarcoidosis was started with prednisone. Within days he developed high spiking fever. Clinical diagnosis of miliary TB was made, later confirmed by positive ZN staining, BAL (PCR) and blood cultures. Appropriate treatment was started, but unfortunately the patient died after a couple months. Discussion: Here we describe two cases in which a false negative IGRA test had dramatic consequences for the patients involved. IGRA tests have high specificity. However, sensitivity for detecting (latent) infection is variable and dependent on time since infection. Conclusion: A negative IGRA test does not rule out TBC and combined IGRA/Mantoux testing should be considered in case of doubt. Severe consequences of a missed diagnosis of TBC infection due to a false negative Interferon Gamma Release Assay M. Kramer, A. Tan, G. den Hartog, E.H. Gisolf, C. Richter Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: m3kramer@alysis.nl 46. Introduction: Interferon Gamma (IFNy) Release Assays (IGRA’s) for the detection of (latent) TBC infection are based on host IFNy production following recognition of M. tuberculosis antigens and display superior specificity compared to the Mantoux test. Sensitivity of the test, however, is variable. Here, we describe 2 cases in which a false-negative IGRA has led to a delayed onset of adequate treatment with fatal outcome in one of the patients. Case 1: A 42-year-old Dutch female presented with a painful swelling in the lower right abdomen. Laboratory analysis showed normal infection parameters and ultrasound imaging was normal. Colonoscopy showed a significant stenosis with ulceration in the ascending colon. Put on the wrong track by Staphylococcus aureus I.M.E. Wentholt, W.E.M. Schouten, P.H.J. Frissen Onze Lieve Vrouwe Gasthuis, Department of Infectious Diseases, Oosterpark 9, 1091 AC AMSTERDAM, the Netherlands, e-mail: i.m.wentholt@amc.uva.nl Introduction and anamnesis: A 44-yr old Somalian man visited the Surgical outpatient clinic with a posttraumatic haematoma in his right lower abdomen. Considered an infected haematoma, the surgeon performed incision and drainage of the mass, which appeared to be an impressive subcutaneous abscess. Culture of the wound demonstrated Staphylococcus aureus and coagulase-negative 27 Staphylococcus species, for which he received flucloxacillin. Wound recovery was protracted for months. Therefore, the infectiologist was consulted. In addition, the patient reported 6 kg weight loss, night sweats and two painful masses on the right side of his back. Physical examination: A cachectic man with normal vital parameters. Body temperature 37.2 °C, a granulating wound (5 x 2 cm) at the right lower abdomen, two painful masses (diameter 3 and 5 cm, respectively) on the right part of his back and one (diameter 2 cm) in the right inguinal area. No neurological abnormalities. Laboratory findings: ESR 51 mm/h, Hb 7,5 mmol/l, leucocytes 7,9 giga/l, CRP 124 mg/l Microbiology: Smear of the abdominal wound and abscess at the back demonstrated acid-fast bacilli in the Auraminerhodamine stain. PCR assay detected a weak signal of Mycobacterium tuberculosis (TB) DNA. TB was isolated from liquid culture. HIV serology was negative. Imaging: Chest-X-ray: no abnormalities. MRI: spondylitis of L1 with partial destruction.and abscesses in musculus psoas and behind the musculus erector spinae on the right side, with intraspinal and epidural expansion at the level of the conus, with compression. Course and conclusion: Patient had TB spondylitis with impressive soft tissue infection, stretching out over a 40 cm long abscess leading to a cutaneous fistula. The abscesses were drained and tuberculostatic quadruple therapy was initiated. Apparently, the surgeon had been put on the wrong track by (1) the isolated Staphylococcus aureus, which was erroneously assumed to be the causative pathogen and (2) the absence of fever and acute illness, which is typical for a “cold” TB abscess. The patient’s ethnical origin should have raised strong suspicion for TB and specific cultures should have been ordered. Even though he recovered well, the patient had been at risk of neurological function loss. In conclusion, whenever a high risk patient presents with a persisting open wound, the diagnosis of TB with formation of a cutaneous fistula should be considered. 47. symptom onset. She did not meet with the nation-wide vaccination criteria, but decided herself to take the vaccination proposed by her company. Physical examination showed a somnolent patient with meningeal signs and left sided hemiparesis. Laboratory tests revealed leukocytes 19.4 x 109/l and CRP 100 mg/l. Cerebral-CT-scan showed bilataral tempero-parietal edema. Analysis of cerebrospinal fluid (CSF) revealed a leukocytosis and high protein- and glucose levels. As the diagnosis meningoencephalitis was assumed, penicillin, ceftriaxone, acyclovir and dexamethasone was started. Cultures of cerebrospinal fluid, viral and mycobacterial PCR-tests were negative. After several days her clinical condition dramatically deteriorated, leading to coma and respiratory insufficiency. She was intubated and artificially ventilated in the ICU. MRI showed extensive cerebral and brainstem white matter lesions. By rising intracranial pressure, a decompressive hemicraniectomy was performed, leaving a permanent opening in the skull. Because of symptoms and MRI, acute disseminated encephalomyelitis (ADEM) was suspected. She was referred to an academic hospital where brainbiopsy confirmed the diagnosis. She was treated with high dose steroids, immunglobulins and plasma-exchange. Unfortunately, her clinical condition deteriorated, leading to irreversible coma and severe epileptic activity. ADEM, also known as post-infectious encephalomyelitis, typically follows a (minor) infection or vaccination with a latency period of 2-30 days. It is an immune-mediated inflammatory demyelinating disorder with an acute onset of focal neurological signs and encephalopathy. MRI is essential for the diagnosis, showing diffuse or multifocal lesions throughout the white matter on T2- and FLAIRweighted sequences. Viral infections like measles, rubella, influenza, Epstein-Barr, HIV, herpes, CMV and West Nile virus have been described as causative agent. Also infections with streptococcus, mycoplasma, chlamydia, rickettsia, leptospira and mycobacteria may induce ADEM. Post-vaccination ADEM has been described after several, especially primary, vaccinations for rabies, diphtheriatetanus-polio, smallpox, measles, mumps, rubella, Japanese B-encephalitis, pertussis, influenza and hepatitis B. There is no proven standard treatment for ADEM; present therapy focuses on immunesuppression and immunomodulation. Although the prognosis of ADEM is generally favorable, fulminant untreatable cerebral edema occurs occasionally. Predictors of poor outcome are older age, female gender, high CSF protein level, spinal cord involvement and poor response to corticosteroids. This dramatic case of fulminant ADEM after H1N1-vaccination illustrates the fact that the potential benefit and adverse events of every medical treatment have to be weighed carefully! A breath-taking complication of H1N1-vaccination: ADEM L.M.H. van de Winkel, J. Buijs, T. Schreuder Atrium Medical Centre, Department of Internal Medicine, PO Box 4446, 6401 CX HEERLEN, the Netherlands, e-mail: l.vandewinkel@alumni.maastrichtuniversity.nl A 27-year-old woman presented at the emergency room with fever, tachycardia and unconsciousness for several minutes. Her medical history was unremarkable. She recieved the influenza-H1N1-vaccine one week prior to 28 48. Fishing for parasites 49. A.M. Vondeling, J.W. Dorigo-Zetsma, S. Lobatto Tergooi Hospitals, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: arielvondeling@gmail.com An unusual case of intermittend fever: chronical meningococcemia G.L. van Sluis1 , E.L.E de Bruijne1, L. Spanjaard 2 , B. Diederen3, E. Kerver1 1 Rode Kruis Hospital, Department of Internal Medicine, Vondellaan 13, 1942 LE BEVERWIJK, the Netherlands, e-mail: geertevansluis@gmail.com, 2Netherlands Reference Laboratory of Bacterial Meningitis, AMSTERDAM, the Netherlands, 3 Regional Laboratoy of Public Health, HAARLEM, the Netherlands A 35-year-old female presented with complaints of fever and malaise. She had no medical history. There were no respiratory or urinary tract symptoms. She had recently visited Northern Italy, but not the tropics. Her father had similar complaints. On physical examination the patient was afebrile and no abnormalities were detected. Laboratory results showed mildly elevated liver enzymes, CRPl 39 mg/l and leukocyte count 11.2 x 109/l, 30 percent eosinophils. Chest X-ray and abdominal ultrasound showed no liver abscess or other abnormalities. Because of the eosinophilia parasitological examination of the stool was performed. On microscopy one liverfluke egg was detected. PCR on the stools confirmed an Opistorchis felineus infection. World wide the number of human infections with Opisthorchis felineus has been estimated to be 1.2 million, most in south-east Asia. Infection in Western Europe is extremely rare. The parasite lives in the biliary duct of mammals where it reproduces. The eggs are excreted with the faeces. Water snails eat these eggs and and are passed on to freshwater fish such as the tench (member of the carp family). By eating raw fish mammals can be infected. The incubation period is 2-4 weeks. Acute symptoms are abdominal pain, fever and malaise. Chronic complications include liver abscess and biliary duct carcinoma. The diagnosis is made by microscopic detection of eggs in the faeces. It is impossible to differentiate microscopically between species of liver flukes, hence specific PCR testing is needed. The diagnosis can be confirmed by a positive antibody test. Our patient had eaten raw fish in a restaurant in Italy, carpaccio of tench. After returning from holidays, she was seen in a hospital 1500 km from where she was infected. Local physicians contacted us about the diagnosis because we were the first to diagnose opisthorchiasis.. Of the 52 people who had dinner in the restaurant concerned, 45 presented with symptoms to the local hospital. Eight of them were admitted. One patient developed a liver abscess. All patients were treated with praziquantel 75 mg/kg/dd. Our patient made a full recovery. To our knowledge she is the first with opisthorchiasis in the Netherlands. Only a small number of outbreaks has been reported to date. Doctors, patients and caterers should be aware that changing eating habits, e.g. consumption of raw fish in Europe, can lead to an increase of parasitic infections. A 19-year-old woman presented with intermittent fever up to 39 °C and chills every 3 days and little red/blue spots on her body. She also complained of joint pain, a sore throat, headache and a neck stiffness. Her medical history was uneventful. She used oral contraception as medication. She was vaccinated according to the State Vaccination Programme and had not visited foreign countries recently. On physical examination we saw a hemodynamically stable, moderately ill-looking young woman with a temperature of 39 °C. Purple skin lesions were observed on the extremities and torso varying from several millimetres to one centimetre, some with petechiae as well. Searches for a focus of infection were unrevealing, and no signs of meningeal irritation were found. Laboratory investigation revealed a leukocytosis of 23 x 109/l with 21 x 109/l neutrophils and an elevated C-reactive protein of 86 mg/l. IgA was found repetitively low (< 0.4 g/l). Serological screening assays for vasculitis were all negative. A skin biopsy showed a leukocytoclastic vasculitis and the gram stain showed no bacteria. In the absence of persistent complaints and acute illness she was admitted for observation and no antibiotics were administered. The initial working diagnosis was a post-infectious syndrome. After discharge she visited the emergency department several times with the same complaints and observations. Repetitive blood cultures drawn during these visits grew Neisseria meningitidis serogroup C. She was treated with benzylpenicillin 12 million IU/24 hours intravenously for 14 days and her housemates were treated with rifampicin 600mg two times a day during two days. Her recovery was without remaining complaints. In conclusion we saw a young woman with a chronic meningococcemia due to group C N.meningitidis despite vaccination. Probably due to IgA deficiency she had an increased susceptibility to infection. Further investigation into underlying immune deficiency is underway. In the 8 years of vaccination with the menC vaccine in the Netherlands (since 2002), there was only one other case of vaccine failure. 29 50. Fish-eye disease 51. A.S.B. Conijn-Mensink, J.G. Schrama Spaarne Hospital, Department of Internal Medicine, Spaarnepoort 1, 2134 TM HOOFDDORP, the Netherlands, e-mail: mensinkannemarie@hotmail.com Introduction: Fish-eye disease (FED) is a rare genetic disease (homozygous defect of the LCAT gene) clinically characterized by the presence of corneal opacities, markedly decreased plasma concentrations of high-density lipoprotein (HDL) cholesterol and normal renal function. We report a patient with corneal opacities and a low HDL cholesterol, who was diagnosed with FED. Case report: A 55-year-old man was seen on the outpatients’ department because of a low HDL cholesterol. He had no coronary heart diseases and he did not use any drugs. Physical examination showed a non acutely ill man with a cornea opacification of both eyes. He indicated that he has had this opacification since he was 20 years old. His brother had the same eye problem. Blood pressure was 136/90 mmHg. Examination of cor, pulmones and abdomen was normal. Laboratory tests showed a normal haematology, normal renal function, normal glucose, normal liver enzymes and normal thyroid function. He had a low HDL cholesterol of 0,1 mmol/l (normal range 0,9-1,7 mmol/l) with a normal low-density lipoprotein (LDL) cholesterol and triglyceride concentration. Urinalysis showed no protein. The lecithin-cholesterol acyltransferase (LCAT) enzyme activity was decreased to 0.75 nmol/ml x hour (normal limit > 12,6 nmol/ml x hour). The genotype analysis detected a homozygous defect of the LCAT gene. His brother had the same defect. Patient and his brother were diagnosed with FED. Discussion: Because of a low HDL cholesterol and cornea opacification, LCAT deficiency was considered in this patient. Several mutations have been described in the LCAT gene and classified as FED or as familial LCAT deficiency (FLD). Mutations in the LCAT gene associated with partial LCAT deficiency lead to FED, whereas complete absence or very low plasma LCAT activity leads to FLD. In FED, LCAT is unable to esterify cholesterol in the HDL molecule, while it retains its activity in very low density lipoprotein (VLDL) and LDL. In FLD, plasma LCAT activity is nearly absent, and plasma HDL and cholesteryl esters levels are very low. Clinical manifestations include anaemia, corneal opacities and renal disease with proteinuria. Conclusion: In FED, the enzyme LCAT is unable to esterify cholesterol in the HDL molecule. This leads to very low HDL cholesterol and corneal opacities. FED is distinguishable from familial LCAT deficiency by a normal renal function and a partial LCAT deficiency. 30 Isolated elevated aspartate aminotransferase (ASAT), a surprising outcome for clinicians 52. Hyperhemolysis syndrome in a patient with anemia caused by a gastric ulcer R.R.L. Wener, F.J. Loupatty, W.E.M. Schouten Onze Lieve Vrouwe Gasthuis, Department of Internal Medicine, Oosterpark 9, 1091 AC AMSTERDAM, the Netherlands, e-mail: r.r.l.wener@olvg.nl H. Ytredal, H.J. Adriaansen, G.S. Madretsma, C.G. Schaar Gelre Hospital Apeldoorn, Department of Internal Medicine, Nieuwravenstraat 11, 3522 RK UTRECHT, the Netherlands, e-mail: h.ytredal@gmail.com Case report: A 34-year-old Polish woman, gravida 2, para 0, who was 34 weeks pregnant, was presented to the gynecologist with pain in the right upper abdomen. Her medical history revealed a severe trauma with abdominal and pelvic injury, nephrolithiasis, benign ovarian cyst, hematocolpos and pregnancy after Intracytoplasmatic Sperm Injection procedure. In the past, she had seen a doctor in Poland because of abdominal pain with elevated liver enzymes. The gynecologist observed a normal pregnancy and did not find a cause for the abdominal pain. However, laboratory examination demonstrated a solitarily elevated ASAT (397 IU/l, reference values ASAT < 30 IU/l). Consequently, the internist was consulted. The patient had no other complaints, i.e. no jaundice or fever. She used no medication, except an antacid. Physical examination revealed no abnormalities. Acute viral hepatitis was excluded by serological measurements for hepatitis A, B, C, EBV and CMV. An abdominal ultrasound showed completely normal results. There was no evidence for other sources of ASAT, such as myocardial disease, skeletal muscle disorders, pancreatic disease or hemolysis. The presence of macro-ASAT was suggested by the clinical chemist and subsequently confirmed by means of a polyethylene glycol precipitation assay. Discussion: Acro-enzymes are enzymes in plasma that have formed high-molecular-mass complexes, either by self-polymerization or by association with plasma components such as immunoglobulins. This benign phenomenon is well characterized for macro-amylase and macro-CK, but todate only 32 cases of macro-ASAT have been reported in literature. The absence of pathology over a long period of follow-up argues for the benign nature of this phenomenon. Macro-enzymes are effectively detected with a polyethylene glycol precipitation technique. Considering the presence of macro-enzymes is important to avoid diagnostic confusion and unnecessary investigations, as illustrated by our case. Hence, it is important to record this information in patient’s notes. Conclusion: Consider macro-enzymes in the differential diagnosis of single elevated serum enzyme activity without any evidence of disease. Introduction: Hyperhemolysis syndrome is a well described phenomenon in patients with sickle cell disease, however, in patients without a hemoglobinopathy, it is rare. A 64-year-old woman was admitted with a microcytic anemia (hemoglobin 3.6 mmol/l) caused by a gastric ulcer. She was treated with cross-matched red blood cell concentrates (RBC) and a proton pump inhibitor. Ten days later she was readmitted with jaundice and dyspnea. Laboratory findings showed severe hemolysis (hemoglobin 2.4 mmol/l, haptoglobulin < 0.08 g/l) and newly present anti-Jk(a) and anti-Kell antibodies, which were not detectable at the pre-test screening before transfusion. Despite nine compatible RBC’s and high dose corticosteroids the hemoglobin level did not increase further than 3.1 mmol/l. In combination with progressive signs of hemolysis a hyperhemolysis syndrome was diagnosed. After addition of intravenous immunoglobulins (0.4 g/kg) the hemoglobin level increased to 5.1 mmol/l and corticosteroids were tapered. The latest antibody screening conducted eights months after admission revealed only anti-Kell antibodies. Discussion: Hyperhemolysis can be a life threatening disease and early recognition is important. Patients with hyperhemolysis have developed alloantibodies during earlier RBC transfusion or pregnancy. This patient without any previous RBC transfusions most likely developed antibodies during one of her four pregnancies. However, the titer of the alloantibodies decline and can become undetectable, as is shown in this case with the anti-Jk(a) antibodies. In patients without known hemoglobinopathy, as far as we know, hyperhemolysis has only been described in three cases. The cause of hyperhemolysis is still unknown. Hemoglobinopathy itself and the high level of alloantibodies are suggested as a trigger. ‘Bystander hemolysis’ triggered by complement activation as well as inflammation with macrophage activation have been presumed as causes of hemolysis. Furthermore suppression of the erytropoiesis is being described with a decreased number of reticulocytes or reticulopenia. Treatment with prednisone is sufficient in some cases, whereas intravenous immunoglobins have shown additional effect. Conclusion: Hyperhemolysis is a rare life threatening transfusion reaction, mostly seen 5-10 days after transfusion, with hemolysis of the transfused compatible erythrocytes as well as the patient’s own cells. The pathogenesis remains unclear and includes alloantibody mediated hemolysis, ‘bystander hemolysis’’, and suppressed erytropoiesis. This case confirms the importance of always considering the pre-transfusion history of the patient, although alloantibodies could be undetectable. There is no standardized treatment. In this case immunoglobulins were successful. 53. A patient with ‘Coombs-negative’ auto-immune mediated hemolytic anemia A. de Haar-Holleman, L.A. Boven, S.K. Klein Meander Medical Centre, Department of Internal Medicine, PO Box 1502, 3800 BM Amersfoort, the Netherlands, e-mail: a.de.haar@meandermc.nl Case report: A 26-year-old male presented at our emergency department with a 2-day history of fever, jaundice, and hematuria. His history was blank. Physical examination was notable for icterus and pallor. Laboratory investigations revealed hemoglobin of 3.0 mmol/l, which further decreased to 2.3 mmol/l within 2 hours. The MCV was 109, erythroblasts 39/100 WBC and reticulocyte count was at 0,18 * 1012/l. LDH could not be determined due to extensive hemolysis. Blood smear examination showed clear spherocytosis. Blood cultures as well as serology were negative. Auto-immune hemolytic anemia (AIHA) was suspected, but the direct Coomb’s test was negative. Routine antiglobulin test (DAT) uses anti-human IgG and C3d reagents. Therefore, the test was repeated using anti-IgG, anti-complement and, additionally, anti-IgA. The test with IgA was strongly positive, indicating a rare IgA-mediated autoimmune hemolytic anemia. The IgA antibodies were eluted from the red blood cells and further characterized to determine specifity. Surprisingly, the antibodies showed a clear and strong specificity for the rhesus antigen e. Discussion: AIHA is characterized by the destruction of red blood cells (RBCs) associated with the presence of IgG, IgM or IgA, and/or components of the complement system on the RBC cell membrane. More than 70% of cases of warm AIHA are caused by IgG. AIHA caused solely by IgA, however, is very rare, i.e. 0.8-2.5% of cases. IgA autoantibodies are usually warm-reacting. The proposed mechanism of RBC destruction in IgA-mediated AIHA appears to be trapping and subsequent sequestration of agglutinated RBCs in the spleen rather than complement activation or deposition or phagocytosis by monocytes. Which makes our patient even more unique is the fact that the IgA antibodies were directed against rhesus antigen e, which is very uncommon as most AIHA with IgA 31 antibodies are directed against an antigen present on all cells rather than blood type antigens. The patient required multiple transfusions with matched e-negative typed red cell concentrates. As therapy with high dose steroids and gamma globulins were not successful, splenectomy was performed. Relief of fever and jaundice followed and the hemoglobin rose to 6 mmol/l. After discharge, the steroid was tapered off and was discontinued 2 months later. Conclusion:This case demonstrates the importance of performing a monospecific antiglobulin test if there is a strong suspicion of AIHA in apparently ‘Coombs-negative’ AIHA. Splenectomy and not steroids are curative in IgA-mediated hemolysis. 54. our patient, however, analysis of the pro-virus and genes of the HTLV-1 in the skin has not been performed. A strongly considered differential diagnosis was Sézary syndrome, a leukemic variant of a cutaneous T-cell lymphoma, which has marked similarities with ATLL but no association with HTLV-1. Although this retrovirus is not sufficient to induce T-cell leukemia on its own, it drives cell growth of latentlyinfected cells through the expression of the pro-virus coded oncoprotein TAX, which affects a variety of cellular signalling pathways leading to transcriptional activation, proliferation and transformation. Prognosis is ruled by the clinical subtype; the chronic or smoldering subtypes are considered indolent, whereas the acute subtype has a worse overall survival. Conclusion: We described a unique case of an ATLL associated with HTLV-1 presenting as mammary swelling and pruritic skin rash. Apart from clonally integration of the virus, immunophenotyping and a peripheral blood smear are useful in differentiating from Sézary syndrom Adult T-cell leukemia-lymphoma presenting as a mammary swelling G.J. Tack, J.J. Hoefnagel, C.E.H. Siegert, W.L.E. Vasmel Sint Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: g.tack@slaz.nl 55. Introduction: Mammary swelling is commonly caused by malignancy or infection of the mammary gland. We report an interesting case of a rare cutaneous T-cell lymphoma presenting as a mammary swelling. Case: A 82-year-old black woman was admitted because of tiredness, swelling of the left mamma and a pruritic generalized rash. Medical history revealed type II diabetes mellitus, hypertension, chronic renal insufficiency and a pacemaker because of an atrioventricular block. Physical examination showed diffuse swelling of the left mamma and erythemateous lesions without papules or plaques, mainly located on the arms, buttocks, left mamma and lower back. Laboratory tests revealed an increased LDH, normocalciemia, lymphocytosis with so called flower-cells in the peripheral blood smear. Immunophenotyping displayed CD25+T-cells, based on the ex-pression of various T-cell lineage markers (CD3, CD4, CD5 and T-cell receptor alpha/beta), without CD7 and CD8 positivity. In addition, a positive western-blot for HTLV-1 was found. CT-scaning showed axillary and inguinal lymphadenopathy without hepatosplenomegaly. Mammography and ultrasound in-vestigations excluded mamma carcinoma. A skin biopsy demonstrated dermal perivascular infiltration and epidermal microabscesses. Diagnosis: A diagnosis of adult T-cell leukemia-lymphoma (ATLL) was made, an aggressive peripheral T-cell lymphoma strongly associated with the human T-cell leukemia virus-1 (HTLV-1). This rare disorder is characterized by lymphadenopathy, pathognomic flower cells and CD4+/CD8-/CD7-CD25+ T-cell immunophenotype. Skin involvement occurs in more than half of the cases. In Walnut induced thrombocytopenia R. Achterbergh, C. Daemen, H.J. Vermeer, S. Lobatto Tergooi Hospitals Hilversum, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: rachterbergh@tergooiziekenhuizen.nl Introduction: Drug-induced thrombocytopenia, due to antibodies binding to platelets in the presence of a drug, is a well known phenomenon. Only a few case reports have been published with a convincing level of evidence for a causal relationship between thrombocytopenia and food or beverage consumption, like tahin and cranberry juice. We describe a case of thrombocytopenia as an adverse effect of walnut consumption. Case: A 70-year-old male was sent to the hospital because after one night of nausea, vomiting and fever, a blood count showed a platelet count of 32 x 109/l. He had no history of bleeding disorder or low platelets. Four days later, in the hospital, the count was normal (212 x 109/l) and it was concluded that the initial low platelet count was probably due to an incorrect test result. However, a few months later, the same symptoms occurred and again a low platelet count (37 x 109/l) was measured. The platelet count recovered in a few days. The patient recalled eating nuts before both events and suspected a relation between his illness and eating walnuts. He did not take quinine containing beverages and did not use thrombocytopenia inducing medicines. We decided to perform an in hospital walnut provocation challenge. The platelet count before was 233 x 109/l. The patient ate 100 grams of walnuts at 5.00 p.m. and 32 after 4 hours developed a fever (38.7 °C) and nausea and vomiting. No other physical or systemic symptoms were seen, especially no rash, angioedema or low blood pressure. The nausea and fever gradually disappeared during the next 8 hours, but the platelet count, measured 15 hours after walnut ingestion was 4 x 109/l and the patient showed bleeding from an existing small wound and large hematomas at venapuncture sites. Other laboratory results, including specific IgE levels against tree nuts, were normal. After four days the platelet count spontaneously recovered to normal. Discussion: Although walnut-induced thrombocytopenia has never been described before, this case is very convincing. Exposure to walnuts resulted in acute thrombocytopenia that recovered to normal in a few days, in absence of other thrombocytopenia inducing agents or causes. This phenomenon was confirmed by an in hospital provocation challenge. Further serological investigations have been started and seem to confirm the presence of specific walnut dependent IgG platelet antibodies in our patients’ serum. Conclusion: Transient thrombocytopenia might be induced by consumption of walnuts. 56. bleeds. Laboratory examination showed a PT-INR of 1.0. Her aPTT, however, was 96 seconds. As mixing tests only showed partial correction, we suspected a factor VIII (fVIII) inhibitor. Indeed, fVIII activity was 1% and an fVIII inhibitor of 64 BU/ml was established. A lupus anticoagulant was excluded. Interestingly, patient had a normal factor IX and factor XI, while factor XII was significantly reduced to 43%. As 50% of patients with acquired hemophilia have comorbidities or underlying conditions (e.g. post-partum, co-existing autoimmune diseases, malignancy), we performed extensive laboratory testing and a computed tomography of chest and abdomen. All returned negative. Treatment consisted of recombinant factor VIIa for her muscle bleeds and high dose prednisone. Subsequently, her aPTT shortened and fVIII activity slowly increased. Discussion: Acquired hemophilia A typically occurs in elderly patients and may be masked by treatment with vitamin K antagonists. Although anticoagulant therapy is usually monitored using PT-INR, we recommend the determination of aPTT and PT in patients with disproportional or unexplained subcutaneous bleeds. First-line bleeding control consists of a bypassing agent (recombinant fVIIa or activated prothrombin complex concentrate) with an efficacy of 90%. Eradication of fVIII inhibitor may be achieved using regimens of corticosteroids alone or in combination with cyclophosphamide. In case of failure, Rituximab (anti-CD20 antibodies) may be considered. After achievement of remission, prolonged follow-up is indicated as relapse occurs in 20% of patients. A patient with a prolonged aPTT: to bleed or not to bleed G. Labots, F.J.S.H. Woei-A-Jin, P.F. Ypma Haga Teaching Hospital, Department of Hematology, Leyweg 275, 2545 CH THE HAGUE, the Netherlands, e-mail: g.labots@hagaHospital.nl 57. Introduction: Acquired hemophilia A is a rare, but potentially life-threatening bleeding condition due to formation of inhibitory antibodies against factor VIII (mortality 9-22%). Unfortunately, diagnosis is frequently delayed and bleedings undertreated. In this abstract, we present an elderly patient, whose hemophiliac condition was mistaken for a bleeding complication due to treatment with vitamin K antagonists. Case report: A 69-year-old female presented with impressive subcutaneous bruising and right femoral nerve palsy due to an iliopsoas hematoma. Her history consisted of diabetes type 2 and atrial fibrillation, for which she used vitamin K antagonists. Initially, domestic abuse was suspected. Her husband, however, was wheelchair dependent and both patient and spouse denied battering. Prior to admission, patient had severe nose bleeds ultimately resulting in a hemoglobin level of 3.6 mmol/l. As her PT-INR was 4.3, patient was treated with vitamin K. Shortly hereafter, patient was discharged from the hospital with a PT-INR of 1.0. It was not long before patient was readmitted because of generalized hematomas and muscle Dancing eye syndrome W.J. Wiersinga, J.M. Prins, D. van de Beek Academic Medical Centre, Department of Infectious Diseases, Tropical Medicine and AIDS, Meibergdreef 9, 1105 AZ AMSTERDAM, the Netherlands, e-mail: w.j.wiersinga@amc.uva.nl Introduction: Chaotic eye movements and myoclonus are key features of the dancing eye syndrome, sometimes referred to as the opsoclonus-myoclonus syndrome. The etiology may be inflammatory and it can occur in many settings, most notably paraneoplastic, in association with autoimmune diseases, infectious diseases or drug toxicity. Here we describe a unique case of therapy resistant opsoclonus-myoclonus syndrome presenting in a patient with HIV-1 de novo. Case (including video presentation): A 27-year-old previously healthy woman presented with a 3-week history of uncontrolled eye movements with disabling oscillopsia (see videotape registration). The complaints started after a short flu-like illness. Vision was normal. 33 showed markedly elevated uptake of heat-damaged red blood cells in the intraperitoneal and retroperitoneal masses depicted on lowdose CT, corresponding to the lesions visualised on ultrasonography and MRI and confirming the diagnosis abdominal splenosis. Indeed, a peripheral blood smear revealed no Howell-Jolly bodies. Abdominal splenosis (AS) is a condition in which autotransplantation of splenic tissue occurs after iatrogenic/traumatic rupture of the spleen. AS differs from accessory spleens that arise during embryogenesis. In AS, depending on the amount of splenic pulpa that is spread throughout the abdominal cavity, several to hundreds of foci can be indentified. In addition, intrathoracal and even intracerebral splenosis have been described. It is estimated to arise in 65% of traumatic splenic ruptures although usually not diagnosed until 10 years after splenectomy. The borne again spleen can be functional as has been suggested by mouse and human studies. AS is often asymptomatic and is diagnosed by coincidence. However, infarction, bleeding or obstruction can lead to a symptomatic presentation. Usually AS requires no treatment, but the diagnosis is warranted to exclude metastasised malignancy and to assess splenic function. Physical examination was notable for uncontrolled eye movements which were constantly present both at rest and after fixation. Brain MRI, CT of thorax, abdomen and pelvis, and examination of cerebrospinal fluid were normal. However, nine months after presentation, she was tested HIV-1 positive with a plasma HIV-1 RNA load of 9971 copies per ml and CD4 count of 500 cells per mm3. The diagnosis of HIV-associated opsoclonus-myoclonus syndrome was made and she was started on combination antiretroviral therapy (cART). Two years after presentation the clinical picture remains unchanged despite treatment with antiretroviral therapy, immunoglobulines, steroids and gabapentin. Because of her complaints she is unable to carry out her previous duties in the supermarket where she worked. Conclusion: In conclusion, we present a patient with the dancing eye syndrome as a rare manifestation of HIV infection at the time of seroconversion who does not respond to treatment. The pathogenesis of this debilitating syndrome remains a mystery. The absence of clinical improvement after initiation of therapy that target the underlying disorder (cART) or the immune system (immunoglobulines, steroids or gabapentin) has not been described before. New insights are urgently needed for this debilitating condition. 59. 58. An unexpected cause of renal failure in a patient with myelofibrosis The borne again spleen H.G. Jongsma-van Netten, M.B. Rookmaaker University Medical Centre Utrecht, Department of Department of Nephrology and Hypertension, Heidelberglaan 100, 3584 CX UTRECHT, the Netherlands, e-mail: hnetten@umcutrecht.nl J.W.R. Hovius1, H.J. Verberne1, R.J. Bennink1, W.L. Blok2 1 Academic Medical Centre, Department of Internal Medicine, Bilderdijkkade 31 II, 1053 VH AMSTERDAM, the Netherlands, e-mail: j.w.hovius@amc.uva.nl, 2Onze Lieve Vrouwe Gasthuis, AMSTERDAM, the Netherlands Case report: A 68-year-old woman was admitted because of progressive renal failure and general weakness. Her history comprised polycytemia vera 43 years ago, which had been treated with splenic irradiation, busulphan, hydroxyurea and phlebotomies and eventually transformed to myelofibrosis. She had recently been evaluated for renal masses for which a kidney biopsy was performed. The pathology report concluded ‘chronic inflammation’. On physical examination her blood pressure was 172/90 mmHg, she had crackles over her lungs and peripheral edema. Laboratory investigation showed a microcytic anemia (Hb 7.8mmol/l), leukocytosis (39.7 x 109/l), increased circulating erythroblasts (25,8 x 109/l) and mild thrombocytopenia (106 x 109/l). Her plasma creatinine had suddenly increased from 253 umol/l to 410 umol/l in one month. A renal ultrasound showed bilateral hydronephrosis. CT scanning confirmed the hydronephrosis and revealed solid masses in the pyelum and perirenal spaces of both kidneys. A nephrostomy was inserted after which renal function improved slighty. A 48-year-old man was referred to the outpatient clinic with markedly elevated liver enzymes. His medical history included splenectomy due to a car accident at the age of 5 years old and a gastric ulcer. Furthermore, he had a habit of excessive alcohol abuse. Upon physical examination an enlarged liver was observed. Blood tests were compatible with alcoholic liver disease and alpha-fetoprotein levels were marginally elevated. The patient was suspected of alcoholic liver cirrhosis. Further work-up included an ultrasound of the upper abdomen, which revealed hepatomegaly and suggested a central mass in the liver. MRI of the abdomen did not show a hepatic mass, but revealed multiple (> 20) intraperitoneal and retroperitoneal structures with a maximum diameter of 3 cm. The differential diagnosis included metastasised malignancy and, with a medical history of traumatic splenectomy, abdominal splenosis. A single photon emission computed tomography (SPECT) with 99mTc-labelled heat-denatured autologous red blood cells 34 Unfortunately, soon after admission, the patient died of sepsis. Autopsy showed extensive extramedullary hematopoiesis (EMH) in the liver and spleen, but also in the renal parenchyma, pelvis and perirenal region. Revision of the renal biopsy material also revealed renal EMH. Discussion: EMH is the compensatory response to insufficient hematopoiesis in the bone marrow and can be found in myelofibrosis, chronic myelogenous leukemia and chronic hemolytic states. EMH is typically located in spleen and liver, but can occur in almost any organ including the kidneys. Renal EMH is often asymptomatic, but can present with abdominal discomfort. It is mostly bilateral and can cause renal failure due to either infiltration of the renal parenchyma, or urinary obstruction through intrapelvic or perirenal masses. On ultrasonography, renal EMH presents as increased echogenicity of the parenchyma or solid hypoechogenic masses in or around the kidneys. On CT, renal EMH appears as welldefined soft tissue, moderately enhanced with intravenous contrast. The differential diagnosis of bilateral renal masses includes lymphomas, metastases, abcesses and granulomatous diseases. The diagnosis renal EMH is made by biopsy which shows hematopoiesis in all lineages and can easily be confused with inflammatory tissue. Treatment should be initiated in case of renal failure or symptomatic EMH. Therapeutic options are chemotherapy (i.e. busulfan, hydroxyurea) and high dose corticosteroids aimed at the underlying condition or local radiotherapy of the renal masses. Conclusion: In patients with myelofibrosis and renal failure, renal extramedullary hematopoiesis should be considered as a cause of renal failure. 60. HIV and hepatitis were negative and no M-proteine could be detected. Chest X-ray and ultrasound of the abdomen were normal, blood and stool cultures for parasites were all negative. Bone marrow biopsy showed 32% eosinophils, with normal maturation of eosinophils. Chromosome studies revealed no abnormalities; the RT-PCR was negatieve for FIP1L/PDGRF a and ß mutations. A percutaneous kidney biopsy specimen disclosed a dense tubular infiltrate predominated by eosinophils and normal glomeruli. Immunofluorescence was negative. Based upon these findings, he was diagnosed with marked central and peripheral eosinophilia most likely due to an allergic reaction to mesalazine, as was supported by the high levels of IgE. Concurrently, a nephrotic syndrome was diagnosed whereas the kidney biopsy only showed interstitial nephritis. The latter only results in non-nephrotic range proteinuria and cannot account for the observed nephrotic syndrome. Based on the pathological data we speculate that in addition to the mesalazine-induced interstitial nephritis, mesalazine induced a minimal change nephropathy as well, resulting in nephrotic-range proteinuria. He was treated with 1 gr Methylprednisolone for three days, followed by 60 mg of oral prednisone, which quickly resolved his symptoms and resulted in complete remission of the nephrotic syndrome and reversal of the eosinophilia. Allergic reactions to 5-ASA compounds are well known. However, the combination of marked eosinophilia with acute kidney failure with nephrotic range proteinuria has been rarely described. Since these compounds are frequently prescribed for prolonged periods, awareness for these side-effects is important for the internist, nephrologist, haematologist and last but not least the gastroenterologist. A young man with a bloated feeling W.M. van der Deure, M.B.L. Leys, I.J.A.M. Verberk-Jonkers Maasstad Hospital, Department of Internal Medicine, Groene Hilledijk 315, 3075 EA ROTTERDAM, the Netherlands, e-mail: wendyvanderdeure@hotmail.com 61. Hypocalciuric hypercalcemia caused by chronic lithium use, successfully treated with cinacalcet A.E.C.A.B. Willemsen, A.G. Lieverse Máxima Medical Centre, Department of Internal Medicine, De run 4600, 5504 DB VELDHOVEN, the Netherlands, e-mail: anneliekewillemsen@hotmail.com A 21-year-old man presented with a bloated feeling, nausea and vomiting since 2 weeks. He had a history of ulcerative colitis, for which he used mesalazine since 10 years. Except for peripheral edema, physical examination was unremarkable. Laboratory data showed marked eosinophilia (76,1%), with IgE levels higher than 2000 kU/l. Blood results showed an increased creatinine (160 mmol/l), a reduced albumin (14 g/l), whereas urinalysis showed nephrotic-range proteinuria (15 gr/24 hrs) without microscopic hematuria. Anti-nuclear antibodies, anti-double stranded DNA and ANCA were negative. C3 and C4, immunoglobulin A, M and G levels were within normal range, whereas serology for CMV, EBV, Case: A 73-year-old woman was admitted to the psychiatric ward with exacerbation of depression, anxiety and confusion. She had a history of depression and anxiety, for which she uses lithium for over 15 years. During admission she developed nausea, vomiting and constipation. On physical examination there was nonspecific tenderness in the lower abdomen. Laboratory examination showed a corrected hypercalcemia of 2.68 mmol/l, phosphate 1.00 mmol/l, albumin 47 g/l and an impaired 35 tration of plasma cells, fibrosis and increased serum IgG4 levels. A frequent described form is auto-immune pancreatitis, but a wide variety of tissues and organs can be involved. Case report: A 83-year-old man suffered from weight loss, fatigue and decline in physical performance. He did not have night-sweats or fever. Physical examination was unremarkable except for a right-sided 1 cm large supraclavicular lymph node. Laboratory findings were normal except for a normocytic anemia (Hb 6.8 mmol/l), renal insufficiency (serum creatinin 273 ug/l) without proteinuria and hematuria and high serum total protein (106 g/dl). Chest X-ray showed multiple densities suspected for malignancy. PET and CT scan revealed multiple hot spots, corresponding with pulmonary nodes and extensive lymphadenopathy. Bronchoscopy showed no abnormalities, cytologic examination showed inflammatory changes. Culture showed no growth of microbial organisms, culture and PCR for tuberculosis were negative. Radiological guided transbronchial biopsy of nodular lesions showed acute inflammation and fibrosis with a polyclonal plasma cell infiltrate. Plasmacells were predominant IgG4 positive. Microscopy of the resected supraclavicular lymph node showed inflammation and plasma cells with IgG4-positive staining (> 30%). Renal biopsy revealed diffuse tubulointerstitial nephritis with infiltrate dominated by plasma cells of which many were IgG4 positive. Serum IgG4 levels were high (52.5 g/l, normal < 1.35 g/l), with concomitant increase in IgG1 and IgG3. The diagnosis IgG4-related disease with systemic manifestations, acute phase response, lymphadenopathy, nodular pulmonary infiltrates and renal manifestations was made. Treatment was started with prednisolone 60 mg/day with a reduction of serum creatinin to baseline value (112 umol/l) after 4 weeks. In addition, the clinical condition strongly improved, the patient gained bodyweight and lymphadenopathy and pulmonary nodules resolved. Conclusion: This case report describes a patient who presented with abnormalities suspected for a disseminated malignancy and acute renal failure. All abnormalities could be attributed to pulmonary, nodal and renal involvement of systemic IgG4-related disease. This disease is also known as IgG4-related autoimmune disease and pancreatitis, IgG4-related plasmocytic disease or IgG4-positive multi-organ lymphoproliferative syndrome and often responds well to therapy with corticosteroids. This systemic disease needs to be considered in patients with focal infiltrating and fibrotic lesions and/or diffuse organ involvement and malaise with elevated serum IgG4 levels and in whom histological examination shows infiltration with plasma cells. The diagnosis can be made by demonstrating a large fraction (> 30%) of IgG4-positive plasma cells by specific staining. renal function with a creatinine of 110 mmol/l, MDRD 42 ml/min/1.73m2. Further testing showed a parathyroid hormone (PTH) of 6.8 pmol/l, 25-OH-vitamine D3 48 nmol/l and a decreased calcium urinary excretion of 0.8mmol/day. The urine calcium/creatinine clearance ratio was low with 0.0078 mmol/mmol. Discussion: In conclusion our patient has hypercalcemia with a slightly elevated PTH, hypocalciuria and normal vitamin D. Primary hyperparathyroidism was unlikely considering the hypocalciuria. Hypocalciuria can be caused by thiazide diuretics, milk-alkali syndrome or by an inactivation of the calcium-sensing receptor (CaSR). The patient did use thiazide diuretics, but the hypocalciuria did not resolve after discontinuation of this drug and milk-alkali syndrome was ruled out. Therefore an inactivation of the CaSR was the most likely cause. Inactivation of the CaSR results in decreased calcium sensing and therefore inappropriate PTH release with respect to the serum calcium concentration. This inactivation can be caused by multiple mechanisms. There can be a mutation in the gene of the CaSR, as is the case in familial hypocalciuric hypercalcemia, auto-antibodies against the CaSR can develop and chronic use of lithium can cause a deactivation of the CaSR. The family history was not contributory and since auto-antibodies against the CaSR are very rare, in this patient the chronic lithium use was most likely the cause. Uncorrected, persistent hypercalcemia may exacerbate psychiatric dysfunction, so there was an indication for treatment. In some cases hypercalcemia resolves after discontinuation of lithium, but considering her current psychiatric problems discontinuation was contra-indicated. A few case reports describe successful treatment of lithium-induced hypocalciuria with cinacalcet. Cinacalcet is a class II calcimetic agent that acts as an allosteric modulator of the CaSR in the parathyroid glands. It restores the calcium sensitivity of the CaSR. We started our patient on cinacalcet 30 mg once daily and the serum calcium successfully decreased to 2.41 mmol/l and the PTH to 2.6 pmol/l. This case illustrates how lithium-induced hypocalciuria was successfully treated with cinacalcet. 62. Tubulo-interstitial nephritis as part of systemic IgG4-related disease A.B. Kramer, C.A. Stegeman University Medical Centre Groningen, Department of Nephrology, Hanzeplein 1, 9713 GZ GRONINGEN, the Netherlands, e-mail: a.b.kramer@int.umcg.nl Introduction: IgG4-related systemic disease is characterized by tissue and organ inflammation with infil- 36 63. Pro-active intoxication of a dialysis patient? intake. At admission she was comatose (Glasgow Coma Scale E1M4V2) and had normal sinusrythm of 102 beats/min, blood pressure was 150/71 mmHg and respiratory rate was 30 breaths/min. Laboratory results included pH 7.28, pCO2 2.2 kPa, HCO3- 7.4 mmol/l, lactate 0.7 mmol/l, sodium 133 mmol/l, potassium 4.2 mmol/l, chloride 105 mmol/l, glucose 4.1 mmol/l, albumin 33 g/l, osmol 281 mOsm/kg and urine ketones were positive. Anion gap was 20.6 mmol/l, where 4.8 was expected in view of albumin level. Strong ion difference was 32 mEq/l, which is decreased. Osmolgap was normal. Toxicology screening, analysis of liquor and computed tomography of the brain showed no abnormalities. Electroencephalography showed persistent epileptic activity. Nonconvulsive status epilepticus was diagnosed, for which the patient was treated with diphantoïn. This metabolic acidosis was diagnosed as a ketoacidosis and treated by dextrose infusions. Acidosis resolved within 3 days without substantially increase in serum glucose during therapy. Conclusion: This is a case of ketoacidosis due to starvation in a pregnant woman with seizures the days before admission and coma due to a non-convulsive status epilepticus at presentation. Starvation leads to a decline in insuline secretion, caused by an increase of sympathetic drive, induced by dehydration. Furthermore, there is low hepatic storage of glycogen due to an increased demand. This will worsen the lipolysis and generate an excess of acetyl coenzyme A, resulting in ketoacidosis. In case of unexplained metabolic (keto)acidosis starvation is an uncommon finding and clinicians should be aware of this cause. Treatment consists of stimulating endogenous insulin by dextrose infusion. Severe metabolic acidosis as a consequence of acute starvation in pregnancy has been described in the literature and is believed to be due to frequent vomiting and an altered glucose metabolism. In our patient the inadequate oral intake due to the seizures and coma led to the ketoacidosis. M.J.M.M. van der Steen, B. Veldman, S. Luderer Canisius Wilhelmina Hospital, Department of Internal Medicine, PO Box 9015, 6500 GS NIJMEGEN, the Netherlands, e-mail: m.vandersteen@live.nl A good medical history is essential for every patient. A 67-years-old hemodialysis-patient presented himself at the emergency room after a sudden collapse with paralysis of his legs. Electrocardiogram showed typical changes of peaking of the T-wave, prolongation of the PR-interval, loss of the P-wave amplitude and widening of the QRS complex. Laboratory investigations revealed a hyperkalemia of 9,3 mmol/l. The patient was treated with calcium, insulin and glucose and resonium. An acute dialysis was arranged. Soon after treatment was initiated symptoms resolved and the electrocardiogram normalized. A thorough analysis took place of what could be the cause of this life threatening hyperkalemia. The patient was aware of potassium rich products and was compliant to his dietary rules. The only recent change in his diet was the addition of ‘Becel-Pro-Activ® voor de bloeddruk’. This is a low-sodium margarine in which sodium is replaced by potassiumgluconate. By measuring the weight of a slice of bread before and after addition of the margarine we calculated an extra potassium intake of 40 mmol a day. It seemed that this was the cause of the hyperkalemia. No other cause of the sudden increase of potassium could be identified. After discontinuation of the Becel Pro-activ, no excessive potassiumlevels were measured. With this case report we would like to draw attention to the importance of history taking in the patient with a hyperkalemia and the emergency treatment of hyperkalemia. Low-sodium products can be a hidden source of potassium. 64. Severe ketoacidosis caused by starvation during pregnancy: a case report 65. M. Kok, N.X. de Rijk, H. Endeman Diakonessenhuis Utrecht, Department of Intensive Care, Bosboomstraat 1, 3582 KE UTRECHT, the Netherlands, e-mail: m_kok_@hotmail.com Middle aortic syndrome, a rare cause of severe hypertension in a young adult R.W. Andriessen, C.E.H. Siegert St. Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: r.andriessen@slaz.nl Introduction: Diabetic dysregulation is the most common cause of ketoacidosis. This is a case of an uncommon cause of ketoacidosis: starvation. Case: A 37-year-old 34-weeks pregnant woman was admitted to our intensive care unit because of unexplained loss of consciousness. Medical history revealed epilepsy since more than seven years, for which she was treated with carbamazepin. She had suffered from several seizures the days before presentation, which had led to a reduced oral Case report: A 24-year-old man presented with severe hypertension, chest pain, headache, and dizziness. The patient was a non-smoker with no significant medical or family history. Physical examination revealed a high blood pressure 200/117 mmHg, measured in both arms, and a pulse rate of 100 bpm. Besides the high blood pressure, the physical examination was completely normal, with strong and symmetric peripheral pulses. 37 Introduction: Intravascular lymphoma is a rare diagnosis, most often diagnosed by autopsy. The disease is characterized by proliferation of clonal lymphocytes within the lumen of small vessels, with little involvement of surrounding tissue. Noteworthy is that intravascular tumor cells are seldom identified in peripheral blood smear in contrast to leukemia and other lymphomas. Diagnosis is almost exclusively made by biopsies of a suspected site of involvement. Clinical presentations are various; but have a predilection to involve brain and skin. We describe a patient diagnosed with intravascular lymphoma ante-mortem. Case-report: A 73-year-old man, with a history of polycythaemia vera, presented himself with fever and abdominal pain. On physical examination he had pain in his right upper abdomen and petechiae on his legs. Laboratory tests revealed a normal hemoglobin, leukocytosis 14,8 * 109/l, thrombocytopenia 38 * 109/l, c-reactive protein 67 mg/l and elevated lactate dehydrogenasis (LDH) 15530 IU/l. The patient was admitted with the differential diagnosis of sepsis or hematologic malignancy. X-rays did not show a focus and CT-scan of the abdomen showed nothing but splenomegaly. During his stay, he became hypotensive and anuric despite antiobiotic therapy. Analyses were extended by CT-scan of the thorax, showing some pleural effusion and bone marrow examination with no morphological changes in the aspirate. Because of rapid deterioration of the patient’s condition, antibiotics were changed and hydrocortisone was started. Within two days he became better and LDH decreased. In the mean time bone marrow immunophenotyping showed evidence of a monoclonal B-cell population suggesting lymphoma. But surprisingly PET-CTscan showed no FDG-uptake, nor any lymphadenopathy. As the patient became better and no lymphoma could be located, hydrocortisone was discontinued, with a worsening condition of the patient and rapidly raising LDH-levels as result. At that time the histo-pathological examination of the crista biopt revealed myelofibrosis due to a myeloproliferative syndrome and intravascular, atypical proliferation of B-cells, as did skin biopsy. The diagnosis of intravascular lymphoma was confirmed. We started reversed R-CHOP treatment being afraid of tumorlysis. The patient became clinical better and LDH decreased rapidly. Unfortunately the patient deceased a few days later due to peri- and epidural hemorrage caused by a lumbal puncture. Conclusion: Intravascular lymphoma is a rare diagnosis in life, as the clinical presentation is heterogeneous and rapidly progressive. Diagnosis is confirmed with biopsy, with intravascular tumor cells and little involvement of surrounding tissue. Treatment consists of standard lymphoma treatment (like R-CHOP) supplemented with intrathecal chemotherapy. Initial laboratory tests showed a hypokalemia (3.3 mmol/l; normal range 3.5-4.5 mmol/l), the other results, including complete blood count, esr, electrolytes, renal function, thyroid profile and troponin, were normal. The urinalysis showed no protein-uria. Additional tests showed an elevated aldosteron level (1.41 nmol/l;normal range 0.11-0.87 nmol/l) and plasma renin level (79 pg/ml; normal range 5.1-38.7 pg/ml), with normal A/R ratio (6.4), which suggested the presence of secondary hyperalostero-nism due to renovascular disease. Because of the severe chest pain and hypertension a computed tomography was made and excluded an aortic dissection. The CT did demonstrate a severe narrowing (diameter of 9mm) of the distal abdominal aorta, with signs of bilateral renal artery stenosis and celiac artery stenosis. Aortography confirmed abdominal aortic narrowing with a significant bilateral stenosis of the renal arteries and narrowing of the superior mesenteric artery. Renography showed asymmetric renal function (left:right =27:73%). The patients blood pressure was controlled with aggressive antihypertensive therapy (labetolol, enalapril and nifedipine). Serum potassium normalised and his headache and thoracic pains disappeared. The patient was furthermore initially treated with PTA of the right renal artery, and finally with aorticbypass surgery. Discussion: Middle aortic syndrome (MAS) is a vascular condition characterized by progressive segmental narrowing of the abdominal or distal thoracic aorta. The etiol-ogy has been described as congenital, acquired, inflammatory or infectious. MAS can be found most frequently in children and young adults, with no sex predilection. Symptoms typically occur within the first three decades of life and include hyperten-sion, lower extremity claudication, and mesenteric ischemia. The condition may be considered as a life-threatening emergency as a result of the complications associ-ated with severe hypertension. Aortography remains the gold standard for diagnosis. The timing of intervention is controversial and difficult to decide. Hypertension refrac-tory to antihypertensive treatment and severe ischemic symptoms are major indica-tions in proceeding to intervention. When multiple arteries appear to be involved in a young patient with a new diagnosis of hypertension, the middle aortic syndrome should be considered in the differential diagnosis. 66. The almost invisible lymphoma R.L. de Jager, K.L. van Rooijen, E.J.M. Ahsmann, E.G. van Lochem, S.K. Klein Meander Medical Centre, Department of Internal Medicine, Utrechtseweg 160, 3800 BM AMERSFOORT, the Netherlands, e-mail: dejager.rosa@gmail.com 38 67. A rare cause of heparin-induced thrombocytopenia complicated by venous pulmonary thromboembolism and adrenal hemorrhagic insufficiency haemorhagic adrenal infarction with – a probably transient – acute adrenal insufficiency has never been described after HIT. M.J.R. Quanjel, E. Beeldman, C.R.G.M. Daemen-Gubbels, J.J.J. de Sonnaville Tergooi Hospitals Hilversum, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: marianquanjel@hotmail.com 68. Bone lesions are not always what they seem to be J.M. Sprangers, F.E. D. de Jongh, F. Croon-de Boer, A. Dees Ikazia Hospital Rotterdam, Department of Internal Medicine, Montessoriweg 1, 3083 AN ROTTERDAM, the Netherlands, e-mail: melanie_sprangers@hotmail.com Introduction: Heparin-induced thrombocytopenia (HIT) is a well recognized disorder with severe thrombo-embolic complications with a mortality rate of 25%, usually because of venous thrombo-embolism, myocardial ischemia or mesenterial infarction. HIT is caused by platelet-activating antibodies that recognize complexes of platelet factor four and heparin, resulting in activation of the coagulation cascade leading to thrombin generation and induction of vascular endothelial thrombogenic effects. The usual cause of HIT is treatment with heparin or low molecular weight heparin. We describe a patient with heparin-induced thrombocytopenia linked to Fondaparinux prophylaxis after elective knee surgery, complicated by venous thrombo -embolism and bilateral adrenal hemorrhagic infarction. Case report: A 67-year-old woman presented with back pain, subfebrile temperature and vomiting eleven days after a elective and uncomplicated total knee replacement. She received Fondaparinux to prevent venous thromboembolic complications according to protocol. Physical examination showed a slightly dyspneic women with a temperature of 38,9 °C and blood pressure of 130/85 mmHg. Besides epigastric tenderness and a slightly swollen knee further examination was unremarkable. A CTA (after a normal X-ray of the chest) showed bilateral pulmonary thrombo-embolism, and also bilateral enlargement of the adrenal glands with peri-adrenal infiltration. Blood tests showed a progressive thrombocytopenia (nadir 18 x 109/l) and hyponatremia (nadir 127 mmol/l) and the Solid-Phase Enzyme Immunoassay for HIT was positive, upon which treatment with fondaparinux was discontinued and replaced by Danaparoïd and acenocoumarol. The persistence of vomiting, malaise and subfebrile temperatures, associated with enlarged adrenals and a decrease of sodium levels led to a possible diagnosis of Addison’s disease which was confirmed by a Synacten test (baseline, 30’, 60’ cortisol of 0.11, 0.11, 0.12 mmol/l, with a baseline ACTH of 559 pg/ml). After initiation of Hydrocortisone treatment the patient showed remarkable clinical improvement. CT-scan of chest and abdomen showed no signs of malignancy. Replacement therapy with hydrocortisone was required. Conclusion: This previously healthy patient showed an extremely unusual cause of HIT, namely Fondaparinux, with severe thromboembolic complications. A bilateral Introduction: In hemato-oncology many patients present with extensive bone lesions, which can be caused by many different diseases, but mostly by metastatic carcinoma or multiple myeloma. Case: A 65-year-old woman presented at the surgical emergency department with a (pathological) fracture of the proximal humerus for which she had surgery. Internal medicine was consulted because of abnormal laboratory findings. On physical examination we found a supraclavicular mass on the left side, 6 cm in length together with scalp lesions. Further examination revealed no other abnormalities. Laboratory findings showed a hypercalciemia (3.80 mmol/l), hemoglobin 7.5 mmol/l, ESR 112 mm/h, LDH 213 IU/l, AF 269 IU/l and GGT 170 IU/l. M-protein was detectable, IgG type lambda, 0.6 g/l. Further investigation revealed numerous osseous lesions in both humeri, the sternum, thoracic spine, femora and multiple ribs. CT scan showed no signs of abdominal or intra-pulmonary pathology or lymphadenopathy. Bone marrow aspiration and biopsy was performed, which showed no signs of multiple myeloma, carcinoma or melanoma. In addition, biopsies of the supraclavicular mass and the scalp lesions were analyzed and showed a CD30+ anaplastic large cell T-cell lymphoma, ALK-negative (ALCL). Our patient was treated with radiotherapy of the humerus followed by chemotherapy (CHOP + G-CSF) resulting in a partial response after 3 cycles. However, a few weeks later she presented with progressive tetraparesis. MRI of the spine showed diffuse infiltration of the spinal cord and extensive leptomeningeal involvement. Despite treatment with dexamethasone and radiotherapy her condition progressively worsened and she died within several weeks. ALK-negative ALCL counts for 2% of the Non-Hodgkin lymphomas, typically have an aggressive behavior and a rather poor prognosis. They often present in stage III or IV with painless lymph node masses, anemia and high lactate dehydrogenase. However, extranodal lesions as described above in our patient are also reported. Summary: We presented a middle age women with a pathological fracture, hypercalciemia and bone masses. Multiple 39 myeloma and metastatic carcinoma were excluded. Biopsies of the supraclavicular mass and the skin lesions revealed an anaplastic large cell T-cell lymphoma (ALCL). Conclusion: We described an unusual presentation of malignant lymphoma with extensive bone lesions, but without involvement of blood, bone marrow and lymphoid tissues. 69. disease due to talcum inhalation have not been reported it is not inconceivable. Discussion: When analysing a patient with iron deficiency it is important to ask for unusual cravings in order to detect the pica syndrome, which has an incidence up to forty percent in non pregnant iron deficient adults. Furthermore, such behaviour may be copied by relatives as well. An unusual craving! 70. E.G. Gerrits1, J.B. Schnog2 1 University Medical Centre Groningen, Department of Internal Medicine, Hanzeplein 1, 9713 GZ GRONINGEN, the Netherlands, e-mail: e.g.gerrits@int.umcg.nl, 2St. Elisabeth Hospitaal, CURACAO, the Netherlands Antilles New oral direct thrombin inhibitors: a coming treatment option for paraneoplastic thrombotic disease? H.T. van der Boog, A. Goosens, A.C. Ogilvie ’t Lange Land Hospital, Department of Internal Medicine, Toneellaan 1, 2725 NA ZOETERMEER, the Netherlands, e-mail: ac.ogilvie@xs4all.nl Introduction: Pica refers to an abnormal appetite for both edible and non-edible substances usually occuring in children with developmental disability or brain injury. However, it is also associated with the iron deficiency state, most often presenting with a craving for ice (pagophagia), but substances like rubber, lemon peals and toothpicks have been reported as well. The craving mostly rapidly reverses with iron repletion. Here we present a case of craving for Johnsons’ baby powder. Case report: A 41-year-old woman was referred to the outpatient clinic because of severe iron deficiency anemia. She was supposed to take iron tablets because of anemia caused by frequent epistaxis due to hereditary hemorrhagic telangiectasia. Upon physical examination she had characteristic mucocutaneous telangiectasiae. In the past, pulmonary and cerebral blood vessel abnormalities were excluded elsewhere. She had discontinued her iron pills for eight months. Laboratory results revealed severe iron deficiency anemia. During the consult she asked whether it was normal to consume one bottle of Johnsons’ baby powder dayly, a behaviour subsequently picked up by her 11-year-old daughter. She was diagnosed with pica syndrome secondary to severe iron deficiency anemia. After four weeks of iron supplementation she felt no more craving and completely stopped its consumption. Her general practitioner was informed and immediately intervened pertaining to her daughter, in whom iron deficiency was excluded. Johnsons’ baby powder or talcum powder contains hydroxylated magnesium silicate and zinc oxide, minerals that inhibit iron absorption. Talcum powder craving associated with iron deficiency has not previously been described. Pica for this powder might be harmful for a patient ‘s health. As both mother and daughter consumed the powder straight from its bottle it is very likely that significant amounts have also been inhaled. Acute respiratory problems secondary to talcum inhalation have been described. Even though chronic lung Introduction: Cancer patients are at increased risk of developing venous thromboembolism (VTE). The occurrence of VTE predicts worse prognosis in cancer patients: whereas the 1-year survival in cancer patients free of thrombosis is 36%, in patients with diagnosed VTE it is 12%. The management of VTE in cancer patients is challenging because the anticoagulant treatment in these patients can be less effective and carry considerable morbidity. Case report: A 66-year-old woman was diagnosed with a stadium IV ovarian cancer. She was on fenprocoumon treatment after a deep venous thrombosis and a portal vein thrombosis. During her Carboplatin Paclitaxel chemotherapy she developed a hematopericard and a deep venous thrombosis, despite having a prolonged prothrombin time (> 7,0 INR). During salvage treatment with subcutaneous Enoxiparin the thrombotic proces progressed and a thrombopenia developted, due heparin-induced thrombocytopenia (confirmed by heparin-platelet factor 4 antibody testing). Treatment with intravenous Argatroban was initiated as a subsequent treatment and led to suppresion of the ongoing thrombosis proces. After stabilisation the treatment was switched to subcutaneous Fondaparinux, in order to make it possible to discharge her. However, the deep venous thrombosis progressed and intravenous Argatroban had to be administered. During subsequentely subcutaneous Danaparoid treatment she developed again thrombopenia. She responded when intravenous Argatroban was given as salvage treatment. The thrombopenia resolved. Unfortunately, her cancer progressed and it was decided to stop the chemotherapy and to give supportive care only. Because of the demonstration of the clinical efficay of treatment with Argatroban, it was decided to administer off-label Dabigatran, another direct thrombin inhibitor with an oral formulation. Unexpectedly, 40 approximately 1 year later, she was in a much better clinical condition and it was decided to start second line Carboplatin Liposomal-Doxyrubicin treatment when documented disease progression developed, while the Dabigatran treatment was continued. No new thrombotic event occurred. Conclusion: This extra ordinary case suggests that direct thrombin inhibitors may play also an important role in the treatment VT-PE in cancer patients, reflecting the positive results of recent clinical studies of oral direct thrombin inhibitors as thromboprophylaxis after elective hip or knee replacement surgery. 71. thalassemia major) and much less pronounced in heterozygotes (ie beta thalassemia minor). On electrophoresis in patients with beta-thalassemia minor, over 90% of the hemoglobin will be hemoglobin A along with an elevation in the hemoglobin A2 value, sometimes as high as 7%, and an increase in HbF in about 50% of patients. However, some forms of beta-thalassemia are not associated with elevated hemoglobin A2. This may be the result of the presence of coinherited deltathalassemia from one of the common structural mutants of the d gene or from mild beta-thalassemia mutations. Therefore, a high-normal concentration of HbA2 does not rule out the presence of beta-thalassemia trait, as shown in our patient. Anemia with persistent, unexplained low MCV with normal Hb-electrophoresis and high-normal HbA2 prompts further evaluation of thalassemias. The microcytic anemia in our patient does not have clinical relevance. Because this hemoglobinopathy is hereditary, it is an indication for screening of relatives to avoid the risk of beta-thalassemia major in offspring of our index patient or his relatives. Unusual cause of beta-thalassemia minor I.J.H. Vriens1, R.H. Olie1, Y. Kluiters1, C.L. Harteveld2, L.V. Beerepoot1 1 St. Elisabeth Hospital, Department of Internal Medicine, Hilvarenbeekseweg 60, 5022GC TILBURG, the Netherlands, e-mail: ingeborgvriens@hotmail.com, 2Leiden University Medical Centre, LEIDEN, the Netherlands A 30-year-old kaukasian man without a medical history was referred to our clinic because of fatigue. Physical examination was unremarkable. Laboratory investigations showed microcytic anemia (Haemoglobin 8.1 mmol/l (8.5-11.0), MCV 71 fl (80-100), MCH 1,46 fmol/l (1.702.10)). Ferritin value was 51 mg/l (16-165). Serum iron level was 10 mmol/l (11-28), total iron-binding capacity 59 mmol/l (45-75) and transferrin saturation 17% (18-38), but our patient was taking iron supplements at that time. We advised the patient to stop the iron supplements and decided to evaluate the digestive tract for blood loss. The results of evaluation by esophagogastroduodenoscopy, colonoscopy, and videocapsule endoscopy were normal. Biopsies taken from the duodenum didn’t show signs of celiac disease. After cessation of the iron supplements, haemoglobin, MCV and ferritin values didn’t further decline. Iron deficiency hereby definitely wasn’t the cause of the microcytic anemia. Hb-electrophoresis performed in our clinic showed normal amounts of HbA2 (3,1%, ref 2.5-3.5%), concluding that there were no signs of betathalassemia. No common mutations were found in the alpha-globin chain, grossly ruling out alpha-thalassemia. Further investigation on hemoglobinopathies however, showed a heterozygous mutation in the HBB-gene and HbA2 was high-normal (3,2%). Our patient therefore has beta-thalassemia-minor. Beta-thalassemia is due to impaired production of beta-globin chains, leading to a relative excess of alphaglobin chains. The degree of alpha-globin chain excess determines the severity of subsequent clinical manifestations, which are profound in homozygous patients (ie beta 72. Recurrent vomiting stopped by taking a hot shower W.A.G. van der Meijden, T.C. Minderhoud, E.F.H. van Bommel, W. Lesterhuis Albert Schweitzer Hospital, Department of Internal Medicine/Gastroenterology, Albert Schweitzerplaats 25, 3318 AT DORDRECHT, the Netherlands, e-mail: wagvdmeijden@kliksafe.nl Case report: A 24-year-old male visited our emergency department for the second time in three months with hematemesis. His medical history included diabetes mellitus type-I and depression. Three months ago a grade-B-refluxoesophagitis was diagnosed. The patient reported frequent vomiting with traces of blood since one day and colicky abdominal pain. Meleana was not reported. Physical examination showed a skinny patient. Blood pressure was 145/75 mmHg, pulse rate 93 beats/ min. Abdominal examination revealed no abnormalities. Laboratory investigation included haemoglobin level of 8,1 mmol/l; white-blood-cell count of 19,2 * 109/l and C-reactive protein level of 21 mg/l. Serum creatinine amounted to 71 mmol/l, urea 6,2 mmol/l, amylase 4 IU/l, glucose 15,3 mmol/l. Serum electrolytes and venous bloodgas were within the normal range. Chest X-ray showed no evidence of pneumomediastinum or pneumoperitoneum. The patient was hospitalized for observation and to perform duodenoscopy. The next morning, nurses were amazed about the patient’s behaviour, because he spent the whole night in the 41 bathroom taking many hot showers. Vomiting was not reported over the night. Duodenoscopy revealed gradeD-(reflux)oesphagitis and prolaps by vomiting, no hiatal hernia. His recurrent periods of severe vomiting and frequently taking hot showers made us suspect the ‘cannabinoid-hyperemesis-syndrome’. When asked, the patient confirmed using cannabis for many years. Subsequently his partner mentioned daily cannabis use and many hospital admissions the last two years because of dehydration by vomiting. Discussion: ‘Cannaboid-hyperemesis-syndrome’ has been described only recently in 2004. Patients with a history of several years of cannabis abuse prior to the onset of hyperemesis acquire cyclical vomiting illness. Cannaboids have an anti-emetic effect. The paradoxical effects in ‘cannaboid-hyperemesis-syndrome’ are not understood. Proposed mechanisms of cannabinoid hyperemesis include toxicity due to marijuana’s long half-life, fat solubility, delayed gastric emptying, and thermoregulatory and autonomic disequilibrium via the limbic system. Effects of cannabinoids on the limbic system might be the underlying mechanism for the compulsive hot bathing behaviour. Warm water improved the symptoms. Cessation of cannabis stops the cyclic vomiting. Essential for the diagnosis is a history of regular use of cannabis for years. Major clinical features of this syndrome are: severe nausea and vomiting; vomiting that recurs in a cyclic pattern over months; resolution of symptoms after stopping cannabis use. Supportive features are: compulsive hot baths with symptom relief; colicky abdominal pain; no evidence of gall bladder or pancreatic inflammation. Conclusion: If patients presenting with cyclic severe vomiting, accompanied by colicky abdominal pain and compulsive hot bathing, the diagnosis of ‘cannabinoidhyperemesis-syndrome’ should be considered. 73. before final diagnosis is made. We describe a patient with submandibular and mediastinal lymphadenopathy associated with AIP. Case report: A 62-year-old male was analyzed for non-painful submandibular lymphadenopathy since 2007. At presentation, he reported a rapid development of unilateral submandibular nodule in the absence of fever, weight loss or nightly perspiration. Physical examination was further unremarkable. Laboratory assessment of blood chemistry, infection serological and bone marrow tests were normal. Initial Computerised tomography (CT) revealed no other localisation of pathological lymphoma. Cytologic and histologic findings of submanidibular lesion revealed inflammatory changes without evidence of malignancy. Three years later, patient presented with painless obstructive jaundice. Physical examination showed jaundice and firm swollen submandibular nodes. Blood chemistry revealed elevated bilirubin 130 umol/l (n: 0-17 umol/l), AF 542 U/l (n:40-125 U/l), GGT 910 U/l (n:0-55 U/l), ALAT 840 U/l (n:0-45 U/l) and ASAT 467 U/l (n:0-35 U/l). CT revealed a mass in the pancreatic head, mesenteric peripancreatic and mediastinal lymfeadenopathy. Endoscopic retrograde cholangiopancreatography (ERCP) with insertion of an endoprosthesis was performed and showed distal stenosis of the common bile duct. Brush cytology of the stenosis showed no malignancy. Endoscopic ultrasound revealed diffuse oedematous pancreas, more prominent in the pancreatic head and fine needle aspiration was again negative for malignancy. Autoimmune serology, such as antinuclear antibody(ANA), Anti-neutrophil cytoplasmic antibody (ANCA) was negative. IgG4 was elevated (20.7 g/l; n:0.08-1.4 g/l), highly suggestive of AIP. Treatment was started with 20 mg of prednisolone. After 2 weeks follow-up CT showed resolution of pancreatic mass, mediastinal, peripancreatic lymphadenopathy and IgG4 level dropped. Azathioprine 50mg was started and prednisolon was tapered slowly. Complete resolution of submandibular lymphadenopathy was noted after 6 weeks of treatment. Conclusion: AIP should be considered in every patient who presents with unexplained systemic disease in combination with pancreatic abnormalities. Diagnosis is based on a combination of diagnostic criteria based on histology, imaging, serology and organ involvement. Since AIP often mimics pancreatic or biliary cancer and in general shows excellent response to corticosteroids, accurate diagnosis is important. Consequently, it may prevent unnecessary surgical intervention and potential morbidity and mortality. Sounds from the abdomen of cervical lymphadenopathy heralding autoimmune pancreatitis F.M.F. Alidjan, J.W.J. van Esser, M.J. van Heerde Amphia Hospital, Department of Internal Medicine, Molengracht 21, 4800 RK BREDA, the Netherlands, e-mail: falidjan@amphia.nl Introduction: Autoimmune pancreatitis (AIP) is a rare benign disorder of presumed autoimmune etiology that is associated with characteristic clinical, histologic, imaging and serum marker findings. AIP may occur as a primary pancreatic disorder, but is often associated with other autoimmune disorders. Most often the diagnosis is made in case of overt pancreatic disease. However, extrapancreatic manifestations may predominate clinical symptoms, even years 42 74. Case: A 66-year-old woman was admitted for dyspnoea and aching on the right side of the chest. She complained of a gradual weight loss and an elevated temperature. She has a history of pulmonary tuberculosis and visited our out-patient clinic for several years because of lymfoplasmocellular lymphoma (Waldenström disease). Previous treatment with chlorambucil leaded to sustained remission. One year before admission she experienced a painful volume increase of her right breast. Excision biopsy showed lymfoplasmocellular lymphoma. During follow up these complaints faded. At presentation a moderately ill woman was seen. Temperature was 37,3 °C, pulse 98/min, oxygen saturation 92% breathing ambient air. The axillary skin and lateral side of the right breast were purple-red and felt hardened on palpation. No palpable lymph nodes were found. Chest examination revealed diminished breathing sounds and dullness on percussion, notably on the right side of the chest. Laboratory results showed elevated CRP (218 mg/l) and BSE (89 mm/h), without leukocytosis (8,9 * 109), anaemia with normal cell indices. Viscosity was 2,5 mPascal/sec. and IgM 18,1 g/l, stable compared to previous measurements. Chest X-ray revealed pleural fluid predominantly on the right side. Antibiotics and furosemide had no effect on dyspnoea, fever or CRP. Multiple thoracic drainages were performed, without lasting improvement. Pleural fluid was characterised as an exudate, no monoclonal cell population was detected, cultures and PCR for tuberculosis were negative. On CT scanning of the thorax we found an axillary lymphoma, eleven cm in diameter and bilateral pleural fluid. Histologic examination showed lymphoplasmocellular lymphoma without evidence for evolution to a high grade lymphoma. Systemic chemotherapeutic treatment with rituximab, cyclophosphamide, vincristine and prednisone was started. Sclerotherapy with talc and subsequently with bleomycin failed to decrease the massive production of pleural fluid. However instillation of 50 mg of rituximab through the thoracic tube resulted in an immediate decline in production. A second instillation of rituximab in the pleural cavity was not possible. Now, two years later, the patient is doing well without recurrence of the pleural fluid. Discussion: Rituximab is a chimeric monoclonal antibody selectively binding to CD20 positive cells leading to cell destruction. It is widely used for the systemic treatment of CD20 positive non Hodgkin lymphoma. Only 2 case histories describe the pleural instillation of rituximab. Conclusion: In cases of therapy resistant pleural fluid associated with CD20 positive lymphomatous pleuritis, intrapleural rituximab is a possible treatment option. Myelodysplastic syndrome and myelofibrosis in a patient with multiple sclerosis treated with natalizumab M.A.E. Rab, P.C. De Bruin, S.T.F.M. Frequin, H.R. Koene St. Antonius Hospital, Department of Hematology, Koekoekslaan 1, 3435 CM NIEUWEGEIN, the Netherlands, e-mail: minkerab@hotmail.com Introduction: Multiple sclerosis (MS) is an auto-immune disorder with limited therapeutic options. Natalizumab, an anti-alpha4 integrin antibody, has shown effectivity as second line treatment of relapsing-remitting MS. Although the exact mechanism of this antibody remains unclear, the most likely mechanism is thought to be the prevention of leukocyte adhesion to vascular endothelium, thus preventing migration of immune cells in the central nervous system. Besides the positive results of natalizumab on MS disease activity, severe adverse effects have been reported. Case report: A 32-year-old patient with MS visited our outpatient clinic because of severe, transfusion-dependent anemia. At presentation, he was being treated with natalizumab for 15 months. Laboratory investigation revealed no clear cause of the anemia. Bone marrow investigation showed only mild dysplasia, cytogenetic analysis revealed no abnormalities. Although anemia was not a know adverse effect of natalizumab use, we discontinued the treatment. Six months after discontinuation, the anemia resolved spontaneously to Hb-concentrations of 9 mmol/l. Because MS disease activity increased again, natalizumab was reintroduced 14 months later. Unfortunately, the anemia recurred. This time it did not improve after cessation of natalizumab therapy. Trephine biopsy showed severe dysplasia and fibrosis. Cytogenetic analysis was again normal. Myelodysplasia and/or myelofibrosis has not been reported as a side effect of natalizumab in the literature, although two concisely described cases were found in the online drug library DrugLib (www. druglib.com). Conclusion: Treatment with natalizumab is associated with bone marrow dysplasia and fibrosis. Therapy should immediately be discontinued upon occurrence of unexplained anemia. 75. Intrapleural rituximab for sclerotherapy resistant pleural fluid in lymfoplasmocellular lymphoma J.D. Sriram, W.G. Meijer Westfries Gasthuis, Department of Internal Medicine, Westfries Gasthuis, 1624 NP HOORN, the Netherlands, e-mail: jd.sriram@gmail.com 43 76. Kill two birds with one stone: rituximab as treatment of refractory polymyositis associated with B-cell chronic lymphocytic leukemia prednisone was tapered, and completely withdrawn after 6 months. A few months later the patient is still doing well. Conclusion: This case illustrates the rare co-occurrence of myositis and B-CLL in which remission of both refractory polymyositis and B-CLL was achieved after treatment with rituximab. Despite the absence of histological confirmation, the parallel course of the diseases suggests an association. D. Boumans, B.W. Schot, H.J. Bernelot Moens ZGT Hospital Almelo, Department of Internal Medicine, Zilvermeeuw 1, 7609 PP ALMELO, the Netherlands, e-mail: d.boumans@gmail.com Introduction: Polymyositis is an uncommon skeletal muscle disease belonging to the idiopathic inflammatory myopathies. It is associated with the occurrence of solid malignancies and in rare cases with B-cell chronic lymphocytic leukemia (B-CLL). Patients generally present with subacute progressive bilateral proximal muscle weakness. Several therapeutic options are available if corticosteroid treatment fails. Rituximab, an anti-CD20 antibody, is successfully used for treating both hematologic malignancies and rheumatic disorders. A number of case reports suggest that treatment with rituximab is effective and safe in patients with refractory polymyositis. Unfortunately, clinical trials are lacking. We describe a patient in which prednisone refractory polymyositis is probably associated with B-CLL and successfully treated with rituximab. Case report: A 70-year-old woman presented with subacute progressive symmetrical proximal muscle weakness of legs and arms. Physical examination was unremarkable except for muscle weakness (MRC 4/5). Skin abnormalities, lymphadenopathy and splenomegaly were absent. Medical history reported diabetes for which she used glimepiride and metformin. Laboratory investigation revealed a remarkable increase of creatinine kinase (CK) (6329 U/l), abnormal liver biochemistry (LDH 864 U/l, AST 161 U/l, ALT 331 U/l) and monoclonal B-cell lymphocytosis (leukocytes 16 x 109/l). ANA and ENA-screening were negative. Electromyography including needle examination showed polyneuropathy with neuropathic and myopathic changes. Treatment with prednisone was initiated (1 mg/ kg) as polymyositis was suspected. Three weeks later the CK level decreased with 50%, but the muscle strength did not improve. The leukocyte count increased up to 36 x 109/l and the patient met the criteria for B-CLL (RAI stage 0) for which, however, treatment was not warranted. Prednisone was tapered after eight weeks as the CK level had decreased further. This was not accompanied with an increase in muscle strength, which led to our conclusion that the patient was refractive to prednisone. Due to the synchronous development of B-CLL we suspected an association with the myositis. To target both diseases we started treatment with rituximab (four times 375 mg/m2/ month) and chlorambucil. Remission of both myositis and B-CLL was achieved after a three month period. Subsequently, rituximab and chlorambucil were ceased and 77. Acquired recurrent angioedema in systematic lupus erythematodes N. Mehra, V.R. van der Pas, A.C. Venhuizen, E. Ton University Medical Centre Utrecht, Department of Internal Medicine, Rijnlaan 75-D, 3522 BD UTRECHT, the Netherlands, e-mail: n.mehra@umcutrecht.nl Introduction:Acquired angioedema (AAE), also called deficiency of C1 inhibitor, is a rare syndrome of recurrent episodes of angioedema. AAE is kinin-mediated, and in contrast to mast-cell degranulation, characterised by angioedema without urticaria or signs of anafylaxis. C1 inhibitor (C1-INH) acts by irreversible binding to activated C1-subcompenents C1r and C1s. Deficiency leads to high complement consumption and production of C2-kinin. Furthermore C1-INH stimulates bradykinin release. Activation of the kinin pathway increase endothelial permeability via mechanisms involving nitric oxide, cyclic GMP, and other effector molecules. In systemic lupus erythematodus (SLE) auto-antibodies have been described directed against C1-INH but also against C1q, leading to AAE. Case report: We present a female Caucasian patient who was admitted to the Rheumatology ward for reconstructive hand and foot surgery. She had previously been diagnosed with Sjogren’s disease and SLE with deformities to the extremities (knees, hands). She had suffered from pleuropericarditis, osteomyelitis, spondylodiscitis, interstitial lung disease and lungembolus. She was known with allergies to antibiotics (clindamycin and cotrimoxazol). Furthermore she had five previous post-operative episodes of angioedema. The first three episodes she had manifest swelling of the tongue, oral cavity, larynx and neck, but without urticaria or signs of bronchoconstriction and hypotension. Thereafter she had been thoroughly examined for allergic responses to peri-operatively used medication, of which all tested were negative, other than the known allergies. Afterwards she was treated pre-operatively before planned operations with a cocktail of dexamethasone and tavegil, and post-operatively 3 consecutive days with xyzal. Still, there were mild episodes of angioedema with pre-and postmedication, the third of these episodes following reconstruction of the extensor 44 digitorum communis of the right hand and amputation of her small toe. She had a nerve-block with local anesthesia, found safe by earlier analyses. She was using no other known medication that could cause bradykinin-induced angioedema, such as ACE-inhibitiors or etanercept. Investigation demonstrated normal tryptase, IgE and C3/ C4 levels, ruling out mast-cell induced angioedema and hypocomplementaemia. Therefore we tested for C1-INH serum levels, C1-INH function, C1q and C4. We found low C1-INH function, demonstrating evidence for acquired angioedema. If an future adverse event takes place, C1 inhibitor concentrate will be tested at an initial dose of 20 units/kg. Conclusion: Angioedema in SLE can be caused by autoantibodies directed against inhibitors of the complement pathway, leading to activation of the kinin-pathway, increased vascular permeability and subsequent edema of the skin, gastro-intestinal tract and upper airway. resonance imaging of the brain showed symmetric multifocal areas of white matter demyelination suggestive for progressive multifocal leukoencephalopathy (PML). Polymerase chain reaction for JC virus in the cerebrospinal fluid was positive. In the meantime, she developed fever, progressive dyspnea and coughing. Despite administration of antibiotics, patient deteriorated clinically and died under the suspicion of pneumonia. At autopsy, the differential diagnosis of inflammatory myopathy with PML was confirmed. Discussion: PML is a severe demyelinating disease of the central nervous system caused by reactivation of JC virus, but is seldom reported in patients without immunodeficiencies. The disease course of PML is poor and usually progressive and fatal. The present case underscores the intriguing possibility that PML may not only occur in patients with immunodeficiencies, but also in auto-immune disorders (polymyositis). 78. 79. A woman with dysphagia, muscle weakness, and cognitive impairment J.L. Peters1 , L.D. Felius1, S.A. Danner 1, F. Stam 2 , J.M. Rozemuller1, A.W. Lemstra1, A.E. Voskuyl1 1 VU University Medical Centre, Department of Internal Medicine, PO Box 7057, 1007 MB AMSTERDAM, the Netherlands, e-mail: mjl.peters@vumc.nl, 2Medical Centre Alkmaar, ALKMAAR, the Netherlands A man with an ‘invisible’ primary tumor and adenohypopituitarism S.A.F. Streukens, J.P.W. van den Bergh, P.W.L. Thimister, W.H.M. van Kuijk Viecuri Medical Centre, Department of Internal Medicine, Tegelseweg 210, 5912 BL VENLO, the Netherlands, e-mail: bstreukens@me.com Introduction: We describe a patient with severe endocrine abnormalities in combination with liver metastasis, but without signs of a primary tumor despite extensive diagnostic testing. Case: A 70-year-old male with a medical history of an ischemic CVA, atrial fibrillation and type 2 diabetes, was admitted because of progressive edema, dyspnea, tiredness and marked hypertension. His medication consisted of ramipril, atorvastatin, metformin and acenocoumarol. Laboratory testing showed severe hypokalemia with metabolic alkalosis, hyperglycemia and liver enzyme abnormalities. The cardiologist ruled out cardiac decompensation. Abdominal ultrasonography showed multiple hepatic lesions suggestive of metastasis. Additional laboratory testing showed marked hypercortisolism (plasma cortisol 4.7 umol/l, 24h-urine cortisol excretion 20.000 nmol) combined with increased ACTH (49.1 pmol/l) and adenohypopituitarism. There was no suppression of cortisol after (high dose) dexamethason. Plasma aldosterone and renin levels and 24h-urine (nor) metanephrine excretion were normal. Glucose concentration was constantly between 15-30 mmol/l. Abdominal and thoracic CT-scans confirmed multiple liver metastasis with slight bilateral adrenal hyperplasia but no signs of a primary tumor. Liver biopsy showed a poorly differen- Casus: A 65-year-old patient was admitted to the hospital with a 6-month history of progressive dysphagia, muscle weakness, and cognitive impairment. During this period she lost 10kg of weight. She also noticed muscle weakness of the upper and lower extremities with gradual worsening over the last period and gait ataxia. Her family reported cognitive changes including an altered mental status, impaired awareness and memory. The patient did not have fever, nigh sweats, cough, skin lesions, or headaches. She had previously been well, retired, lived alone, drank alcohol socially, and smoked 10-15 cigarettes a day. On examination, the patient was tired and had a lack of attention complicating cognitive testing. There was muscle atrophy and weakness of the hands and lower extremities. No skin lesions were observed. The complete blood count (with differential count), erythrocyte sedimentation rate, C-reactive protein, serum levels of electrolytes, and tests for renal and liver functions were normal. Serum levels of creatine kinase were increased (2690 U/l), and the test for antinuclear antibody (ANA) was positive, but additional testing for specific antibodies was negative. Nailfold capillaroscopy demonstrated a ‘scleroderma’ spectrum with mega-capillaries. Tissue (skin and muscle) biopsy of the upper leg revealed an inflammatory myopathie. Magnetic 45 tiated carcinoma with neuroendocrine differentiation. MRI showed no hypothalamic or pituitary abnormalities. Based on these findings this patient was diagnosed with multiple liver metastasis from an unknown ACTHor CRH-producing primary tumor with secondary hyperglycemia, hypertension, hypokalemic metabolic alkalosis and adenohypopituitarism due to extreme hypercortisolism. Our differential diagnosis regarding the primary tumor was: carcinoma of the lung (small cell (SCLC) or bronchial), thyroid, pancreas, stomach or a carcinoid. Gastroscopy and colonoscopy were both normal. A PET-CT-scan now showed marked bilateral adrenal hyperplasia but no signs of FDG capturing metastasis or a primary tumor. An additional octreotide scan was planned. However the patient’s physical condition worsened and he died before further diagnostic testing. Autopsy showed extensive myocardial ischemia and a SCLC of the right lower lobe (diameter 3.5cm) with pleural carcinomatosis and extensive metastasis in the left lung, liver, pancreas, adrenal glands, prostate and bone marrow. Reassessment of both PET and CT-scan still did not reveal the metastasis or the primary tumor. Conclusion: SCLC is a known cause of ectopic ACTH-secretion with clinical presentation of Cushing’s syndrome. The present case has two distinctive characteristics. Firstly the adenohypopituitarism (without signs of a pituitary mass) probably caused by suppression of pituitary hormones due to the extreme hypercortisolism. Secondly the ‘invisibility’ of the primary tumor on both the PET and CT-scan despite its size at autopsy. Possibly it was not FDG capturing due to the hypercortisolism-induced hyperglycemia. 80. of severe insulin resistance. In our outpatient clinic, she had persistent hyperglycemias despite usage of a total amount of insulin of about 250 units a day. In the past three years her insulin necessity had been doubled. Besides sporadic vaginal blood loss, she reported no abnormalities. During admission she needed 440 units of insulin per day. Laboratory testing showed an increased level of estradiol and inhibin B. An additional CT scan of the abdomen showed a solid tumor of the left ovary. A bilateral salpingo-oophorectomy was performed, with removal of the tumor. Pathological examination of the left ovary showed a thecoma, a benign, solid, fibromatous tumor. Postoperatively, the need for insulin dramatically decreased. Glycosylated hemoglobin decreased from 12.6 to 6.7% in a few months. In this patient, severe insulin resistance was caused by a thecoma. Thecomas are usually confined to a single ovary and occur predominantly in postmenopausal females. They may produce estradiol and up to 20 percent of patients present with synchronous endometrial cancer. These tumors have a yellowish appearance from accumulated lipid and can become very large (up to 40 cm). Histologically, they are primarily composed of theca cells, but may also contain granulosa cell components. The most common symptom of thecomas is abnormal vaginal blood loss as a result of endometrial stimulation from estroadiol produced by theca cells. Conclusion: Although ovarial stromal hyperthecosis and PCOS are known to cause insulin resistance, no literature exists on an association between a thecoma and insulin resistance. Little is known about the pathophysiology of insulin resistance in ovarial stromal hyperthecosis and PCOS. Future studies might clarify a common pathway of insulin resistance in ovarial stromal hyperthecosis, PCOS and thecoma. A thecoma as a cause of severe insulin resistance: a case report N.L. Verbeet, M.O. van Aken Haga Hospital, Department of Internal Medicine, Leyweg 275, 2545 CH THE HAGUE, the Netherlands, e-mail: nicoletteverbeet@yahoo.com 81. A rare cause of hypophosphatemic osteomalacia A.C. van de Ven, A.R. Hermus Radboud University Medical Centre, Nijmegen, Department of Endocrinology, Geert Grooteplein 10, 6525 GA NIJMEGEN, the Netherlands, e-mail: ac.ven@aig.umcn.nl Introduction: Insulin resistance is caused by several diseases, some in which pathophysiology is known, such as obesity and rare inherited diseases, like leprechaunism and Rabson-Mendenhall syndrome, some in which the mechanism remains unclear, such as polycystic ovary syndrome (PCOS). In this report, we present a patient with a thecoma causing severe insulin resistance. An association which has not been reported previously in the literature. Case report: A 77-year-old female, known with type 2 Diabetes Mellitus, ischemic dilated cardiomyopathy and atrial fibrillation, was admitted at our hospital because A 38-year-old woman was referred to our outpatient clinic by the rheumatologist. For the past 3 years, she had suffered from progressive pain in the muscles and bones. Due to the pain, she was sitting in a wheelchair and she needed help with daily activities. She was using Lynestrenol because of endometriosis and Fumaric Acid because of psoriasis. On physical examination, no signs of arthritis or other abnormalities were noticed. Initial laboratory analyses showed a severe hypophosphatemia (0.28 mmol/l, normal 46 value: 0.80-1.40 mmol/l) and a hypokalemia (2.9 mmol/l, normal value: 3.5-4.7 mmol/l). Calcium, magnesium, creatinin, vitamin D and parathyroid hormone were normal. X-rays, already performed by the rheumatologist, showed a decalcified aspect of the pelvis and revealed a fracture of the third left metatarsal. Whole body scintigraphy showed a generally increased radiotracer uptake and multiple foci of increased uptake in the rib cage (rosary sign), tibia and feet. The diagnosis hypophosphatemic osteomalacia was made and further investigations were performed in order to assess the cause of the hypophosphatemia. Analysis of the urine showed a glucosuria and proteinuria. The fractional phosphate excretion was inappropriately high, suggestive for renal loss of phosphate. Also, a generalized aminoaciduria was found. Serum uric acid and bicarbonate were low. This combination of abnormalities is consistent with Fanconi syndrome, a defect localized in the proximal renal tubule. Several diseases can cause Fanconi syndrome. Monoclonal gammopathy, Wilson’s disease and cystinosis were ruled out. A Pubmed search yielded 3 case reports of middle aged German women who developed a Fanconi syndrome with osteomalacia during the use of Fumaric Acid. Fumaric Acid is an occasionally prescribed medicine for the treatment of psoriasis in the Netherlands, although it is not registered for this purpose. We stopped the Fumaric Acid immediately and started with phosphate supplementation. Later on, vitamin D was added. Within a few days, the patient noticed a decline of muscle pain. She was able to walk all day, without the use of the wheelchair. At this moment, 6 months after stopping the Fumaric Acid, she has no complaints at all. Unfortunately, the Fanconi syndrome is still present and the patient needs to take daily high doses of a phosphate mixture in order to keep the serum phosphate sufficient. Diagnosis: hypophosphatemic osteomalacia due to Fanconi syndrome, caused by Fumaric Acid use. 82. there were no other people with osteoporosis. Physical examination showed no abnormalities. The bone mineral density measurement (using DXA) showed a T score of -4.1 SD for the lumbar spine and T -2.5 SD for the femoral neck. The X-ray of the spine showed a fracture of Th 12. Further evaluation for a secondary cause of his osteoporosis showed no abnormalities besides an elevated serum tryptase level (44.5 mg/l, normal value < 11.4 mg/l.). In the bone biopsy several mast cells were seen. There was a weak signal of the c-kit D816V mutation measurable. It was concluded that the patient had osteoporosis and a vertebral fracture because of systemic mastocytosis. He was treated with peginferferon a, a bisfosfonate, cetirizine and ranitidine. The results of one year of treatment and some background information will be presented. 83. Ain’t no sunshine when she’s gone… C.R. van Rooijen, F. Stam, M.B. Kok Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 21, 1815 JD ALKMAAR, the Netherlands, e-mail: cleovanrooijen@gmail.com Introduction: Serum calcium levels are hormonally controlled, with a key role for parathyroid hormone (PTH) and vitamin D. We present a patient with extremely low calcium levels and an unusual disorder in calcium metabolism. Case report: An 18-year-old negroid woman presented with progressive cramps in both hands for 2 days. She was born in Jamaica and had moved to the Netherlands 8 months ago. She had no relevant medical history. On physical examination, we found her fingers to be cramped as well as a positive Trousseau’s sign. No other abnormalities were noticed. Laboratory analysis showed severe hypocalcaemia (1.17 mmol/l) and hyperphosphatemia (2.0 mmol/l), with normal blood levels of albumin (36 g/l), creatinin (61 mmol/l) and alkaline phosphatase (96 U/l). Urinary excretion of both calcium (0.8 mmol/day) and phosphate (5 mmol/day) was low. We found this to be consistent with hypoparathyroidism. However, the PTH level was increased (22.1 pmol/l), whereas 25-(OH)-vitamin D was low (31 nmol/l). An Ellsworth-Howard test was performed, measuring urinary phosphate excretion after administration of synthetic PTH. This showed only a fivefold increase in phosphate excretion, thereby supporting the diagnosis of pseudohypoparathyroidism (PHP). Upon treatment with calcium supplementation and 1a-(OH)vitamin D (alfacalcidol), her symptoms disappeared. Serum calcium levels however remained in the low range, as did her calcium excretion. Discussion: Pseudohypoparathyroidism (PHP) is a rare hereditary disorder with features resembling hypoparathy- An unusual ca(u)se of osteoporosis L.I. Arwert, P. Lips VU University Medical Centre, Department of Endocrinology, PO Box 7057, 1007 MB AMSTERDAM, the Netherlands, e-mail: l.arwert@vumc.nl This is a case report of a 46-year-old man who was seen for evaluation of osteoporosis. He had a recent vertebral fracture (Th12) after putting his motorbike in the upright position. Thereafter he had back pain, but no other complaints. In his history he had a wrist fracture at the age of 9. In the last years he lost 5 centimetres of length. He had no skin signs or abdominal problems. In his family 47 roidism, although plasma PTH levels are elevated. PHP is caused by alterations in the PTH receptor, inducing target tissue resistance to PTH. Normally, PTH increases serum calcium levels by stimulating bone resorption and renal calcium reabsorption and converting 25-(OH)-vitamin D to the metabolic active 1,25-(OH)2-vitamin D (calcitriol). PTH and calcitriol interact to increase intestinal calcium and phosphate absorption, whereas PTH also stimulates renal phosphate excretion. In PHP, tissue resistance to PTH results in hypocalcaemia and hyperphosphatemia in the presence of elevated PTH levels. The biochemical abnormalities of PHP can be associated with Albright’s hereditary osteodystrophy, which was not the case with our patient. The diagnosis of PHP is confirmed by the EllsworthHoward test. In hypoparathyroidism, administration of synthetic PTH will cause a 100-fold increase in phosphate excretion. Treatment is lifelong supplementation of both calcium and alfacalcidol. In our patient, symptoms were probably evoked by the lack of sunlight in Dutch winter, decreasing vitamin D levels and thereby aggravating hypocalcaemia. Conclusion: Hypocalcaemia and hyperphosphatemia in the presence of high PTH levels can be caused by alterations in the PTH-receptor. 84. treatment with a GLP-1 RA, primarily because of the associated weight loss. At presentation she used insulin aspart 8-12 IU with each meal, insulin glargine 22 IU and metformin 850 mg bid. She weighed 100 kg (BMI 34.6 kg/m2) and her HbA1c was 69 mmol/mol (8.5%). We decided to treat her with liraglutide at an initial dose of 0.6 mg per day. She was instructed to stop insulin after taking 11 IU of insulin glargine at bedtime prior to starting liraglutide the next morning. Results: Thirty-six hours after starting liraglutide, she reported severe nausea and vomiting, with glucose values between 12 and 20 mmol/l. At presentation in our emergency department she had an acetone smell, arterial pH of 7.29, bicarbonate level of 12.8 mmol/l, and tested positive for ketones in her urine. She was treated for diabetic ketoacidosis, and subsequently her insulin regimen was restarted. Anti-GAD was positive (30 U/l). She is now considered to have type 1 diabetes mellitus, and she was instructed to never stop insulin again. Conclusion: Our case shows that adequate classification of diabetes is crucial before insulin is switched to GLP-1 RA. Diabetic ketoacidosis in a patient falsely classified as having diabetes mellitus type 2 should be considered as an alternative explanation for nausea and vomiting after initiation of a GLP-1 RA. Diabetic ketoacidosis after switching from insulin to a glucagon like peptide-1 receptor agonist T.M. Vriesendorp, F. Holleman, J.H. de Vries Academic Medical Centre, Department of Internal Medicine, 1105 AZ AMSTERDAM, the Netherlands, e-mail: t.m.vriesendorp@amc.nl Introduction: Glucagon like peptide-1 receptor agonists (GLP-1 RA), a new class of glucose lowering agents, are associated with weight loss. Their main mechanism of action is glucose-dependent stimulation of insulin secretion, but GLP-1 RA also inhibit gastric emptying and promote satiety. The main side effects of GLP-1 RA are nausea and vomiting. Currently, the combined use of insulin and GLP-1 RA therapy is not approved. Aim: To report a case of diabetic ketoacidosis after switching from insulin to a GLP-1 RA Materials and methods: A 34-year-old Caucasian female visited our outpatient department for a second opinion. Seven years before she had been diagnosed with type 2 diabetes mellitus, complicating her obesity with a BMI of 41.5 kg/m2. After 4 months she started insulin because of poor control on oral agents. In the past year she had participated in an intensive weight loss program and had lost 20 kg of weight. Recently, her weight had stabilised and her HbA1c had gone up after an initial fall. She proposed III. ENDOCRINOLOGY RESEARCH 85. LHRH-antagonist cetrorelix may reduce postmenopausal flushing P.M. van Gastel, M. van der Zanden, D. Telting, M. Filius, L. Bansci, H. de Boer Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: petrivangastel@hotmail.com Introduction: Estrogen replacement therapy is the most effective treatment for postmenopausal (PMP) flushing, but its use is often contraindicated. An effective and safe alternative is urgently needed. Aim: To explore the effects of the LHRH receptor antagonist cetrorelix in women with severe PMP flushing who have a mean daily flush score > 15. Materials and methods: Open-label treatment with cetrorelix 250 g twice a day in 9 women with severe PMP flushing, for a period of 4-6 weeks. The response to treatment was evaluated by monitoring serum gonadotropin levels, flush scores, and quality of life. 48 Results: 254 of 395 patients agreed to participate. The results in this abstract are based on the patients that participated in the period April 2009 until June 2011 (n=170). The response to the questionnaire at baseline was 100%. 106 patients completed the follow-up period of which 81 patients returned the follow-up questionnaire (76,5%). One third of the patients had primary and two third secondary adrenal insufficiency. Conclusion: Glucocorticoid-education meetings could help to improve patients’ knowledge and self-management of illnesses and proper use of glucocorticoid stress doses. Results: At baseline, the mean daily flush score was 35.9±2.0 (range 29-44). All subjects demonstrated a decrease in serum LH and FSH during treatment, but premenopausal levels of both gonadotropins were reached in only 2 subjects. The mean daily flush score decreased by 39.6±8.4% (p<0.005). This was caused by a decrease in flush frequency of 25.4±7.1%, and a decrease in flush severity of 17.3±7.5%. Conclusion: Severe PMP flushing can be reduced by LHRH receptor blockade. The data suggest that a longer treatment period is required to capture the maximal effect. 86. Knowledge and self-management of patients on replacement therapy with glucocorticoids 87. The role of Techneticum-99m methoxyisobutylisonitrile scanning in diagnostic imaging of patients with primary hyperparathyroidism J.W.J. Repping-Wuts, M.M.L. Stikkelbroeck, M.F. Kerstens, M. vanTeeffelen-Lourens, A.R.M.M. Hermus Radboud University Medical Centre, Department of Internal Medicine, 6500 HB NIJMEGEN, the Netherlands, e-mail: j.repping-wuts@reuma.umcn.nl M. Maas, E.J. Postema, P.H.M. Reemst, H.R Haak Máxima Medical Centre, PO Box 7777, 5500 MB Veldhoven, the Netherlands, e-mail: M.Maas@mmc.nl Objectives: To assess the knowledge and selfmanagement in patients receiving replacement therapy with glucocorticoids before and 6 months after glucocorticoid-education-meetings. Method and design: A longitudinal questionnairebased survey at the Radboud University Medical Centre Nijmegen. Participants: 395 patients with primary or secondary adrenal insufficiency on glucocorticoid replacement therapy, received an invitation letter from their endocrinologist, to attend to a glucocorticoid-education-meeting. Patients were invited to bring along a partner or a close friend. Intervention: The three-hour glucocorticoid-educationmeeting (12-14 patients per meeting) consisted of a lecture about the disease, the treatment and specific stress education. The nursing education consisted of instructions how to inject hydrocortisone i.m.. Supervised by the nurse, all patients and their guests could practice this action during the meeting. Furthermore, during the meeting patients could talk with other patients. Measurement: Two weeks before, and 6 months after the meeting, patients were invited to fill in a questionnaire. This questionnaire (1), had been adapted and translated into the Dutch language. Besides patients characteristics, the questionnaire consisted of six hypothetical conditions of illness and the patients were asked what action they would take. Furthermore, patients were asked if they had the glucocorticoid instruction leaflet and ampoules of hydrocortisone at home. They were also asked about the symptoms of an Addison crisis and if they had practiced the intramuscular injection. Objective: The aim of this study was to assess the radiologic and nuclear diagnostic methods prior to surgery in patients with primary hyperparathyroidism in Máxima Medical Centre. Methods: Between January 2005 and October 2010, sixty-six patients with hyperparathyroidism underwent a parathyroidectomy. Of these, we analysed fourty-six patients with primary hyperparathyroidism who had a first time parathyroidectomy with proven parathyroid adenoma or hyperplasia. Primary hyperparathyroidism was defined as having a serum PTH > 5.2 pmol/l, a serum calcium > 2.55 mmol/l and a serum phosphate of < 0.80 mmol/l. The forty-six patients were analysed retrospectively for the used diagnostic method (ultrasound, MIBI, CT), the sensitivity of these diagnostics for correctly predicting the quadrant of the adenoma location and the obtained short and long term remission. Results: In thirty-four of the forty-six patients (74%) with a proven parathyroid adenoma or hyperplasia, the MIBI scan predicted the localisation of the adenoma correctly. Of these thirty-four patients, twenty-five had additional diagnostic procedures. In two of the remaining twelve patients, the MIBI scan predicted the right side, but the wrong quadrant. One of these two patients had a CT scan that was normal, the other had an ultrasound which did not show anything either. Both patients underwent a minimally invasive parathyroidectomy (MIP) and had normal serum calcium a year post-surgery. Nine of the twelve patients (75%) with a negative MIBI scan also had a CT scan, an ultrasound, or both. Only in 2 of these nine patients, the additional diagnostic method predicted the quadrant of the adenoma location correctly. 49 Conclusion: Our data indicate that a MIBI scan is a reliable diagnostic method to predict the localisation of a parathyroid adenoma or parathyroid hyperplasia. Therefore, it should be the pre-operative diagnostic method of first choice. There is very limited value of additional diagnostic procedures. Based on our study we would advise the following pre-operative algorithm: Patients with a serum confirmed PHP should first have a MIBI scan. If the MIBI scan shows a parathyroid adenoma, the patients is eligible for having a MIP. In case of a negative scan, the patients should undergo an ultrasound of the neck. If the ultrasound shows an adenoma in the neck, the patient is eligible for an MIP. If this ultrasound is negative, the patient should have a bilateral neck exploration. 88. was within the normal range (NR 0.4-4.0 mE/l) in 93.2% of cases, and in 91.8% of controls, respectively (p>0.05). Mean TSH level did not differ significantly between groups (cases: 2.0±1.7 mE/l vs. controls: 2.3±1.0 pmol/l; p>0.05). Mean FT4 level was significantly lower in cases than in controls (15.9±2.9 pmol/l vs. 17.7±3.2 pmol/l; p<0.001), but there was no difference between the frequency of within normal range FT4 levels (NR 9-24 pmol/l) between groups (cases: 100% vs. controls: 98.6%; p>0.05). Frequency of anti-TPO antibody positivity (i.e., anti-TPO titer >35 kIU/l) was similar in both groups (cases: 8/73 [10.9%] vs. controls: 6/73 [8.2%]; p>0.05). Three iRPF patients and two control patients had subclinical hypothyroidism (TSH >4 mE/l and normal range FT4 level) associated with anti-TPO antibody positivity (p>0.05). Three iRPF patients and two control patients were positive for both ANA en anti-TPO antibody (p>0.05). The overall frequency of ANA positivity did not differ between groups (cases: 15/73 [20.54%] vs. controls: 13/73 [17.8%]; p>0.05). Conclusion: In this unique case-control study we found no association between iRPF and Hashimoto’s thyroiditis. Our findings do not support the concept of iRPF being a systemic autoimmune disorder. Hashimoto’s thyroiditis and anti-thyroid peroxidase antibody associated with idiopathic retroperitoneal fibrosis: case-control study C.E. Andreescu, E.F.H. van Bommel Albert Schweitze Hospital, Department of Internal Medicine, Albert Schweitzerplaats 25, 3318 AT DORDRECHT, the Netherlands, e-mail: corina_andreescu@hotmail.com Background: Idiopathic retroperitoneal fibrosis (iRPF) is a rare disease of unknown origin, characterized by an inflammatory proliferative fibrosing process occurring in the retroperitoneum. Some case-reports suggest an association of iRPF with Hashimoto’s thyroiditis, which should support the hypothesis of an autoimmune pathogenesis of iRPF. Our objective was to investigate the frequency of Hashimoto’s thyroiditis, anti-thyroid peroxidase antibody (anti-TPO) and antinuclear antibody (ANA) positivity in iRPF patients. Methods: In a case-control study, we evaluated prospectively 73 patients with a diagnosis of iRPF from April 1998 through October 2010 in our tertiary care referral Centre. Controls were 73 randomly selected patients, followed at the same outpatient department of internal medicine, who volunteered to take part in the study. Controls were not known with a history of iRPF and had no evidence of iRPF by radiological examination. Groups were matched for age and sex. In all patients, clinical (including history regarding thyroid diseases and iRPF) and physical examination were performed. In both groups, we determined the presence of anti-TPO antibodies, ANA, as well as thyroid hormone (FT4) and thyroid stimulating hormone (TSH) levels. Results: Demographic characteristics did not differ between groups, including mean age (cases: 62.5±11.1year vs. controls: 61.7±14.0 year) and percentage male sex (cases: 73.9% vs. controls: 72.6%; both p>0.05). TSH level IV. ENDOCRINOLOGY CASE REPORTS 89. Unexpected severe hypercortisolism leading to ethical discussions at an intensive care unit I.J.A. de Bruin 1 , A.J.C. Rokx 1, J.J. Weenink 2 , H.H. van Ojik1, W.A. Oranje1 1 TweeSteden Hospital, Department of Internal Medicine, Dr. Deelenlaan 5, 5042 AD TILBURG, the Netherlands, e-mail: idbruin@tsz.nl, 2Spaarne Hospital, HOOFDDORP, the Netherlands Case report: A 30-year-old man was referred to our rheumatology department because of pain in both hands. The patient was known with triple A syndrome and used hydrocortisone replacement therapy, he used no other medication. His mental capacities are limited, probably in relation to the triple A syndrome. On physical examination no signs of arthritis were found and further laboratory analysis was performed. Inflammation parameters were normal but there was a hypothyroidism (f T4 7,4 pmol/l, TSH 94,2 mU/l). Only 4 months earlier his TSH had been in the normal range (4.5 mU/l). On further evaluation TPO antibodies were negative and the patient did not have a goiter. He had never had radioiodine treatment and had never had amiodaron, lithium or other drugs that might interfere with thyroid function. Levothyroxine as replacement therapy was initiated and after 4 months of treatment he was euthyroid and free of pain in his hands. Discussion: There are different mutations known in the AAAS gene resulting in a heterogeneity of clinical symptoms among patients. Often exhibited symptoms (except for the alacrima, achalasia, adrenal insufficiency and microcephaly) are abnormalities of pupils and cranial nerves, optic atrophy and autonomic neuropathy. A literature search revealed no known cases of patients with triple A syndrome and hypothyroidism. The dysfunctional protein caused by mutations in the AAAS gene is normally part of the WD repeat protein family which has a wide functional diversity. Possibly the mutation in this patient is also responsible for the development of hypothyroidism through still unknown mechanisms, because all features of the syndrome appear to be neuro-endocrine in nature. Our hypothesis is supported by the fact that no other causes of hypothyroidism were identified. Conclusion: Primary hypothyroidism diagnosed in a 30-year-old male patient known with triple A syndrome, possibly because of a linked gene defect. workup revealed renal rather than intestinal potassium loss. This prompted us to investigate the possibility of hyperaldosteronism or cortisol excess. No stigmata of Cushings disease had been noticed. Serum ACTH was 356,7 ng/l and cortisol was 3,11 umol/l. A CT-scan showed an intrapulmonary laesion and hepatic metastases. A liver biopsy confirmed extensive small cell lung carcinoma (SCLC). Ectopic ACTH overproduction from SCLC was diagnosed. We discussed extensively whether we should continue treatment. However SCLC can be treated with chemotherapy with a high chance of durable responses. So treatment was continued. First the high cortisol had to be lowered. There are several possibilities: high dose ketoconazol, metyrapone, mifepristone, etomidate, a bilateral adrenalectomy or chemotherapy. Because the condition of the patient deteriorated and he had to be intubated, we choose for etomidate as a sedative and therapeutic drug. Immediately after intubation we started with substitution therapy with hydrocortison. Broad antibiotic coverage including prophylaxis with trimethoprim-sulfamethoxazol and fluconazol was started in this immunocompromised patient. Serum levels of both ACTH and cortisol dramatically fell within 8 hours. After the patient’s condition stabilized he was transferred to a tertiary centre for a bilateral adrenalectomy. There the patient was successfully weaned from the ventilator and etomidate was substituted for ketoconazol orally with good response. Finally no bilateral adrenalectomy was performed since chemotherapy can induce rapid responses. The condition of the patient stabilized so there could be started with Cisplatin and Etoposide. Initially the patient seemed to improve clinically. Unfortunately he died from neutropenic sepsis. Conclusion: This case illustrates the endocrine emergency of malignant ectopic ACTH production leading to ethical discussions at an ICU and different methods to treat it. 91. Introduction: Severe hypercortisolism caused by malignant ectopic ACTH production is a rare cause of hypokalaemia and metabolic alkalosis and is difficult to treat. Treatment options depend on the condition of the patient. Case: A 66-year-old man with chronic diarrhoea and recent onset diabetes and hypertension was referred to the emergency department with general oedema and suspicion of decompensated heart failure. Lately his diabetes was difficult to manage. He experienced progressive loss of muscular strength and despite the oedema there was a weight loss of 10 kg. No other features of heart failure were found. Blood analysis revealed serum levels of: potassium 1,6 mmol/l, sodium 141 mmol/l, bicarbonate 40 mmol/l and arterial pH 7,59. He was admitted to the ICU for treatment of hypokalaemia and alkalosis. The diagnostic 50 90. Hypothyroidism in a patient with triple A syndrome, due to the same gene defect? Hypoglycaemia leading to a diagnosis of Non-Hodgkin Lymphoma F.J.C. Cuperus, R. Komdeur, D. Telting, H. de Boer Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: franscuperus@gmail.com L.E. van der Wagen1, P.C. de Jong1, G.D. Valk2 1 St. Antonius Hospital, Department of Internal Medicine, Koekoekslaan 1, 3435 CM NIEUWEGEIN, the Netherlands, e-mail: lotte_vd_wagen@hotmail.com, 2University Medical Centre Utrecht, UTRECHT, the Netherlands Introduction: Hypoglycaemia is uncommon in non-diabetic subjects. Its etiology can be established by appropriate blood tests during prolonged diagnostic fasting. This report describes a patient presenting with hypoglycemia as the key symptom leading to a diagnosis of Non-Hodgkin Lymphoma. Case: A 72-year-old female was presented at the emergency ward with a hypoglycemic coma (blood glucose 1.3 mmol/l), Introduction: Triple A syndrome (‘Allgrove syndrome’) is a rare autosomal recessive genetic disorder. Patients have mutations in the AAAS (Alacrima Achalasia Adrenal insufficiency syndrome) gene located on chromosome 12q13. They present with the above symptoms and also a wide range of neurologic abnormalities. 51 which rapidly resolved after intravenous administration of glucose 50%. Retrospectively, hypoglycemic episodes had been present for 3 months. Medical history was unremarkable, and the patient did not use any medication. Night sweats, weight loss, or fever were not reported. Physical examination and a general laboratory screening were normal. Five hours after the start of a standardized fasting procedure she developed hypoglycaemic symptoms (blood glucose 2.3 mmol/l), upon which samples for the measurement of glucoregulatory hormones were taken. Plasma C-peptide, insulin, pro-insulin, insulin antibodies, cortisol, and IGF-BP3 were within the normal range. Plasma IGF-I and IGF-II were 279 (normal range 56-165) and 706 (normal range 280-610), respectively. Plasma E-peptide, a surrogate marker for pro-IGF-II, was within normal range. Treatment with R-COP (rituximab, cyclophosphamide, doxorubicin, prednisolone) resulted in a normalisation of glucose metabolism and plasma IGF-I and IGF-II levels within one month. Discussion: Malignancy-induced hypoglycaemia is very rare, but should not be forgotten in the differential diagnosis of non-hyperinsulinemic hypoglycemia. The most common cause is tumoral overproduction of pro-IGF-II, a precursor of IGF-II that stimulates the insulin receptors and enhances glucose uptake. Less frequent causes associated with malignant disease include tumoral IGF-I or IGF-II production, tumoral insulin auto-antibody production, and extensive destruction of the liver by malignant cells. In our case no clear etiological agent was found; E-peptide was within the normal range and IGF-I and IGF-II were only mildly elevated. Conclusion: A structured approach allows a rapid diagnosis of non-islet cell tumor hypoglycaemia, finding the etiological agent appears to be the major challenge. 92. having any shortness of breath, coughing, oedema or nycturia. Fevers and nocturnal transpiration were absent and the patient followed a normal diet without gastrointestinal complaints.At physical examination, vital signs were normal, and examination of the heart and lungs did not reveal any abnormalities. Of note, the thoracic pain was inducible by compression of the ribs of the left hemithorax. No axial pain or pressure pain was present in the extremities. Routine laboratory analysis, including a complete blood cell count, renal function, and liver enzymes, was normal.Chest X-ray and additional oblique rib films were normal. A bone scintigram demonstrated focal accumulation of activity in the left ribs and diffusely elevated uptake in the mandible and cannon bones, evidencing osteomalacia. Additional laboratory investigations revealed hypocalcaemia (1.72 mmol/l) with a normal serum albumin (44 g/l) and a low-normal serum phosphate (0.87 mmol/l). Serum 25-hydroxyvitamine (vitamin D) level was 53 nmol/l (reference level 50-100 nmol/l), with a significantly elevated parathyroid hormone (75 pmol/l). This was interpreted as secondary hyperparathyroidism as a result of a vitamin D deficiency, since there was no evidence of malabsorption or osteoblastic disease.After 2 months of oral calcium and vitamin D suppletion, thoracic pain and facial spasms had resolved, and serum calcium and phosphate levels were normalized. Importantly, serum parathyroid hormone level had decreased to 51 pmol/l after 2 months, and further to 6 pmol/l after 9 months of treatment. Serum vitamin D level increased to 82 nmol/l after 9 months.In conclusion, this patient was diagnosed with isolated hypocalcaemia with secondary hyperparathyroidism and osteomalacia as a result of vitamin D deficiency, whereas vitamin D levels did not suggest severe vitamin D deficiency.The minimum value of serum vitamin D has been subject of debate for several years. However, most experts agree that a serum vitamin D level < 50 nmol/l may be considered deficient. Nonetheless, the current case demonstrates that serum vitamin D levels must be interpreted in the in the clinical context of each patient. Hypocalcaemia and osteomalacia in a patient with a normal vitamin D level J. van Ramshorst, M.J.F.M. Janssen, C.F.A. EustatiaRutten, H. Dik, F. Smit, A.M. Schrander-van der Meer, G.J.P.M. Jonkers Rijnland Hospital, Department of Internal Medicine, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: j.van_ramshorst@lumc.nl 93. Post-partum hypopituitarism and a sellar mass: not always a Sheehan’s syndrome S.M. Platvoet-Sijtsma, B.G. Ziedses des Plantes, B.L.J. Kanen Zaans Medical Centre, Department of Internal Medicine, PO Box 210, 1500 EE ZAANDAM,, the Netherlands, e-mail: smsijtsma@gmail.com Case report: A 28-year-old women of Somalian origin presented to the pulmonologist with thoracic pain. Her medical history included treated pulmonary tuberculosis 10 years ago. She complained of a stinging, non-radiating pain on the left hemithorax which worsened with breathing, but was not radiating to the shoulder, upper extremity or cheeks. Furthermore, the patient complained of facial tingling sensations and spasms. She denied 94. She had recently given birth to a healthy child. During labour there was aproximately 500 cc bloodloss. In the following days, lactation was difficult and had been stopped. One month later, our patient visited a neurologist because of headaches. The analysis, including a computed tomography scan of the brain, showed no explanation. In the months following, our patient became anorectic and nausious. She had fainted several times. Physical examination was unremarkable, except for a blood pressure of 105/78 mmHg, with evident orthostasis. Laboratory findings include normal haemoglobin, kidney and liverfunction. Cortisol (< 0.01 mmol/l) and ACTH (2.0 pmol/l) were compatible with secundary adrenal insufficiency, but other pituitary functions seemed intact. The prolactine level was normal (139 ml IU/l). Magnetic resonance imaging (MRI) of the brain showed a sellar mass iso-intense to brain tissue with homogeneous gadolineum-contrast uptake which therefore was not compatible with pituitary apoplexy as in Sheehan’s syndrome. The diagnosis lymphocytic hypophysitis was suspected and since there was no optic chiasm compression, treatment with high dose glucocorticoids was started. Recovery was quick and hydrocortison in a substitution dose was continued. Pituitary gland- and alpha-enolase autoantibodies all came back negative. One month later, MRI showed a decrease in size of the adenoma, supporting our diagnosis. Discussion: Lymphocytic hypophysitis (LYH) is a very rare disorder; the incidence is unknown. LYH typically occurs during the third trimester of a pregnancy, or shortly after pregnancy. It can be mistaken for a pituitary adenoma due to its mass effect which can also result in optic chiasm compression. It is characterized by lymphocytic infiltration and destruction of the pituitary and typically results in hypopituitarism. Usually the pituitary-adrenal axis is the first to be affected, followed by the pituitary-thyoidal-axis. The few cases reported describe disease courses from complete recovery to permanent panhypopituitarism. Few reports mention the presence of pituitary autoantbodies, especially anti-alpha-enolase, but the clinical and etiological relevance is unclear. A confirmed diagnosis can only be made with a biopsy of the pituitary. Treatment with high-dose glucocorticosteroids is advocated, but due to it’s rarity evidence is lacking. Conclusion: When hypopituitarism is diagnosed in a post-partum patient with a sellar mass, one should consider lymphocytic hypophysits as a possible cause other than Sheehan’s syndrome. Treatment with glucocorticoids could be beneficial in preserving or recovering of pituitary function. H.M. de Wit, A.H. Mudde Slingeland Hospital, Department of Internal Medicine, PO Box 169, 7000 AD DOETINCHEM, the Netherlands, e-mail: hmdewit@gmail.com Introduction: MIDD and MELAS are both associated with a 3,243 A>G mutation in mitochondrial DNA, which is transmitted by maternal inheritance. MIDD patients often present with progressive hearing loss, followed by diabetes at 30-40 years of age. MELAS is characterized by stroke-like episodes, encephalopathy causing seizures or dementia and blood or cerebral spinal fluid lactic acidosis, often presenting before 20 years of age. Both diseases are characterized by a broad spectrum of other symptoms including renal, cardiovascular, neuromuscular and psychiatric disease. We report on clinical details of the members of a Dutch family with the 3,243 A>G mutation to make a contribution to the phenotypic description of this mutation. Family history: The mtDNA 3,243 A>G mutation was discovered in 2002 in 2 generations of a family with a high penetration of diabetes mellitus and deafness. The mother of this family, who was positive for the mutation (heteroplasmy 2,5%), was diagnosed as type 2 diabetes at 53 years. She became insulin dependent 15 years later and deafness became apparent at 79 years. Her husband, negative for the mutation, had type 2 diabetes. Four of their 5 children developed diabetes and progressive hearing loss, with heteroplasmy levels in leukocytes varying between 15 and 23%. In the course of their diseases remarkable observations in these subjects were made. Firstly, extreme insulin resistance gradually developed, which is unusual in MIDD. The role of the paternally inherited diabetes, superimposed on the mtDNA mutation is discussed. Secondly, the youngest brother (heteroplasmy in leukocytes and in muscle 20% and 84%, respectively), showed a striking deterioration of symptoms in time. He was diagnosed with MIDD based on classical symptoms. Later in time he seems to meet the criteria for MELAS, with stroke-like episodes, declining cognitive function, blood lactic acidosis and severe exercise intolerance, which we demonstrated in a 6 minute walking test. His sister has recurrent depressions and cerebral spinal fluid lactic acidosis. Muscle biopsies in both patients showed abnormalities consistent with MELAS, however no ragged red fibers were found. Conclusion: This family history illustrates that MELAS and MIDD could be regarded as two phenotypical expressions of the same disease. The first may emerge from the second in time. Moreover, extreme insulin resistance may be a feature of the clinical picture. Case report: A 28-year-old woman, with a history of subfertility, was admitted to our hospital because of fainting and hypotension. 52 From MIDD (maternally inherited diabetes mellitus and deafness) to MELAS (mitochondrial encephalomyopathy with lactic acidosis and stroke-like episodes): two expressions of the same disease? 53 95. Hypokalemic paralysis in a 22-year-old man compartment, which leads to hyperpolarization of the muscle membrane and inactivity of muscle fibres. The paralysis may occur within an few hours-days usually affecting lower extremities more than upper extremities. Besides potassium suppletion, treatment aims for an euthyroid state and antagonization of beta adrenergic stimulation. M.L. op de Weegh, H.E. van der Wiel IJsselland Hospital, Department of Internal Medicine, Spangesekade 75G, 3027 GK ROTTERDAM, the Netherlands, e-mail: marlous33@hotmail.com Introduction: Acute paralysis is usually reported in neurologic, inflammatory, toxic, metabolic or endocrinological diseases. We present a patient with an acute paralysis and a low serum potassium. Case: A 22-year-old negroid man was referred to the emergency ward with a symmetric paralysis of both legs, and decreased strength in both arms. Additional symptoms were nausea and vomiting. The day before admission he had undergone an arthroscopy without complications. His medical history yielded acute liver failure of unknown origin, aplastic anemia and thrombocytopenia. The patient denied using illicit drugs, but was using NSAIDs and pantoprazole. Physical examination revealed an athletic male with symmetric paralysis of both legs, and decreased strength in both arms with diminished reflexes. Laboratory results showed an extreme low serum potassium (K 1.2 mmol/l), low TSH (0.020 m IU/l), high FT4 (55.7 pmol/l), high TSI (111 IU/l) and urinary potassium excretion was 20 mmol/l. The arterial blood gas and serum renine activity were normal. Serum aldosteron was slightly decreased (0.10 nmol/l). The ECG showed U-waves. The MRI of the spinal cord showed no abnormalities. After treatment with strumazol, propanolol and intravenous potassium, the serum potassium normalized within hours with complete recovery of his paralysis. An ultrasound of the thyroid gland was performed, which showed a small inhomogeneous deviation of the left lobe of the thyroid gland. Discussion: This patient presented a thyrotoxic hypokalemic periodic paralysis (TPP). Graves disease is the underlying disorder in most cases of TPP. Thyrotoxic hypokalemic periodic paralysis can be precipitated by carbohydrate load, exercise or stress (in this case the arthroscopy). TPP predominantly occurs in the early morning. In most cases the paralysis is reversible. The incidence of TPP is highest in Asian men. In non-Asian populations the incidence of TPP is estimated to be 0.1-0.2%, mostly within the age of 20-40 years. Our patient was from Caribbean origin in which TTP is rare. It’s hypothesized that paralysis could occur because thyroid hormone increases tissue responsiveness to beta adrenergic stimulation. This response increases sodium-potassium ATPase pump activity on the skeletal muscle membrane. This is followed by a sudden shift of potassium from the extracellular into the intracellular 96. A harmless injection? M.M. Oosterwerff, P. Lips, W. de Ronde VU University Medical Centre, Department of Endocrinology, De Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: m.oosterwerff@vumc.nl Introduction: Intra-articular corticosteroid injections are well-known treatment modalities in rheumatic conditions. Locally administered corticosteroid injections only sporadically evoke adverse effects. In this case report we present a women with iatrogenic Cushing syndrome after two intraarticular injections with triamcinolon acetonide (TCA, Kenacort®). Case: A 31-year-old female was seen in the outpatient clinic with a gradually developing moon face. Because of chronic pain in the right shoulder, an injection with 40 mg TCA was administered intra-articularly by her general practitioner four and two weeks prior to presentation. Her medical history revealed a dilated cardiomyopathy with tromboembolism and amputation of both legs caused by a pheochromocytoma in the right adrenal gland in 2000. The right adrenal gland was resected. In 2006 there was a clinical and biochemical suspicion for a relapse of pheochromocytoma close to the liver, which was resected, but microscopic examination showed no abnormalities and she had a good recovery. At presentation, our patient complained of rapid weight gain, hypertension, headache, irregular menses and backache. Clinical examination showed a moon face, high blood pressure 170/102 mmHg and multiple purple striae. A 24-hour urine collection showed free cortisol excretion of < 18 and < 14 nmol/24 hr. Morning plasma cortisol and ACTH concentrations were very low at < 30 nmol/l and 2 pmol/l, respectively. A diagnosis of iatrogenic Cushing’s syndrome was made. Our patient was treated with metoprolol 50 mg once daily, hydrocortisone in case of stress to avoid secondary adrenal insufficiency, no replacement therapy in the abcence of severe symptoms. In about five months symptoms and signs gradually regressed and spontaneous recovery of HPA-axis was observed. Conclusion: Supraphysiological amounts of exogenous glucocorticoids are a cause of Cushing’s syndrome. In this case report a iatrogenic Cushing’s syndrome is described after two injections of TCA, which is an exceptional event. 54 Furthermore, exogenous corticosteroids can suppress the HPA-axis and subsequently induce secondary adrenal failure. 97. due to takotsubo cardiomyopathy, which is a ventricular dysfunction that is usually reversible. Treatment consists of supportive care and resection of the adrenal tumor. Conclusion: Takotsubo cardiomyopathy as initial presentation of a pheochromocytoma. Cardiomyopathy and an adrenal mass C.L. Boot, P. Lips VU University Medical Centre, Department of Internal Medicine, De Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: c.boot@vumc.nl 98. Successful treatment of insulinoma with endoscopic ultrasound-guided alcohol ablation M. Weijmans1 , F.P. Vleggaar2 , B.T. Rövekamp1, E.A. bij de Vaate1 1 Zuwe Hofpoort Hospital Woerden, Department of Internal Medicine, Polanerbaan 2, 3447 GN WOERDEN, the Netherlands, e-mail: liez7@hotmail.com, 2University Medical Centre Utrecht, Department of Gastroenterology, UTRECHT, the Netherlands Introduction: Most of the patients with a pheochromocytoma have hypertension. We present a case of a patient with hypotension instead of hypertension as result of a pheochromocytoma. Case report: The patient is a 58-years-old woman, who once had an episode of chest pain, without a clear diagnosis. Since then she uses acetylsalicylic acid, bisoprolol and simvastatin. Further medical history was unremarkable. Since a couple of months before presentation she suffered from heavy perspiration. She has had no hypertension, headaches, palpitations or weight loss. Because of chest pain and ST-elevations in leads V1, V2 and V3 on ECG the patient was transferred from a hospital abroad to our academic clinic to undergo a percutaneous coronary intervention. However, at the initial cardiac angiography no abnormalities of the coronary arteries were seen. Because blood pressure had fallen down, the patient needed haemodynamic support. A transthoracic echocardiogram showed a dilated left ventricle with akinetic segments suggesting takotsubo cardiomyopathy. Ultrasonography of the abdomen showed an adrenal mass at the right side of 6 cm, which was also seen on the CT-scan. In the urine an excessive excretion of catecholamines was found, even after stopping haemodynamic support. On the MIBG-scan intense uptake was seen in the right adrenal mass, without any uptake elsewhere. After a short period of time the patient became normotensive. Metyrosine was given to reduce the production of catecholamines. After starting doxazosine as a-blocking drug followed by atenolol as ß-blocking drug to prevent hypertension during operation a successful laparoscopic adrenal extirpation was performed. Pathologic examination showed a pheochromocytoma of 7 cm. Postoperatively no complications were seen and within a week the patient was sent home in good clinical condition and with normal blood pressure. After some weeks she was seen at the outpatient department. Her sweats were gone, and blood pressure, catecholamine excretion and echocardiogram were all normal. Discussion: Pheochromocytoma is a rare diagnosis which often presents with episodic haedache, sweating and hypertension. As we show in this case, sometimes the initial presentation is chest pain combined with hypotension Introduction: We present a case of a patient with recurrent symptomatic episodes of insulinoma-induced hypoglycemia. Insulinoma is a rare beta-cell neoplasm of the pancreatic islet that oversecretes insulin. Instead of standard surgical therapy we performed EUS-guided alcohol ablation. Case report: In September 2010 an 82-year-old woman was admitted to our hospital with a history of recurrent episodes of hypoglycemia for more than one year. She had no history of diabetes mellitus, did not use any medication to regulate blood glucose levels, nor did she have underlying liver failure. A fasting evaluation test was performed and showed a spontaneous episode of hypoglycemia. An inappropriately high serum insulin concentration of 60.8 mU/l was measured during a hypoglycemia of 2.5 mmol/l. This indicated excess insulin and insulinoma was suspected. The preferred initial tests, a transabdominal ultrasonography and a CT-pancreas, were performed and showed no presence of a tumorous lesion in the pancreas. The subsequent endoscopic ultrasonography showed a neuroendocrine tumor of 10 mm size in the corpus of the pancreas. Because of the patient’s age, general condition and the small size of the tumor, an EUS-guided alcohol ablation instead of surgery was performed. There were no complications and a total of 3 ml 96% ethanol was injected into the tumor. A histological biopsy taken during the procedure showed a neuroendocrine tumor, which conformed the diagnosis of insulinoma. Currently, the patient is feeling well and has not experienced any recurrence of hypoglycemia. Conclusion: The standard therapy for patients with a benign, solitary insulinoma is surgical excision of the tumor. Only two cases1,2 of endoscopic ultrasound-guided alcohol ablation of insulinoma have been reported. In our patient the treatment showed good results: there was no 55 recurrence of hypoglycemia. Endoscopic ultrasound-guided alcohol ablation is minimally invasive and appears to be suitable for patients with a poor general condition and a small insulinoma. 99. may be often seen. The most frequent benign cause of a recurrent laryngeal nerve paralysis is a multinodular goitre. Thyroiditis causing recurrent laryngeal nerve paralysis is extremely rare. Fortunately with modern imaging techniques one rarely has to resort to surgery to exclude a malignant cause. Conclusion.: Recurrent nerve palsy when caused by thyroid disease may be transient and have a benign cause, especially when there is no apparent thyroid enlargement. A rare cause of recurrent laryngeal nerve palsy in thyroid disease M. Sandovici1, C. Halma1, H. van den Berge2 1 Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: maria.sandovici@znb.nl, 2Department of Otorhynolaringolog, Medical Centre Leeuwarden, LEEUWARDEN, the Netherlands 100. Abdominal pain as the presenting symptom of panhypopituitarism S.H. Binnenmars, A.J.J. Woittiez Hospital Group Twente, Department of Internal Medicine, Zilvermeeuw 1, 7600 SZ ALMELO, the Netherlands, e-mail: H.Binnenmars@zgt.nl Introduction: Paralysis of a recurrent laryngeal nerve in thyroid disease is classically associated with an enlargement of the thyroid gland due to a malignant process. Case: A 60-year-old female with osteoporosis and Civatte’s poikilodermia, presented with hoarseness. Six weeks before, while on holiday in France, she got a sore throat and fever up to 39.2 °C. She was initially treated with Tragitol en strepsils and thereafter with Klacid and possibly Prednison. At the moment of presentation the patient still had a sore throat, a subfebrile temperature, night sweating and fatigue. On physical examination a light dysphonia, a slightly enlarged, painful thyroid gland without any nodules and a heart rate of 85/min were found. Blood analysis revealed an elevated sedimentation rate (> 9 0 mm/h) and CRP (107 mg/l), a normocytic anaemia (Hb 6.7 mmol/l), normal white blood cell counts, a slightly decreased TSH (0.21 mU/l) and a normal FT4 (21.5 pmol/l), and a negative anti-TPO. Flexible laryngoscopy showed a palsy of the left vocal cord. A CT of the neck and thorax showed signs of inflammation of the thyroid gland and glottis, some reactive lymph nodes and no pathology in the aortic-pulmonary window. A diagnosis of recurrent laryngeal nerve palsy accompanying a subacute thyroiditis was made. Ten days later the hoarseness subsided and the pain clearly diminished. Four weeks later the CRP normalized, the sedimentation rate decreased to 18 mm/h, the anemia had spontaneously resolved and patient became hypothyroid. A MRI showed a normal thyroid gland and no signs of pathology along the left recurrent nerve. Discussion: Paralysis of a recurrent laryngeal nerve is only rarely associated with a benign thyroid disease. The mechanisms involved herein are compression of the nerve against the cervical spine or the trachea, stretching of the nerve over an enlarged thyroid (such as in a goitre, thyroid nodule or thyroiditis), inflammation of the nerve itself, oedema or thrombosis of the minute arterial supply. In the chronic phase, perineural fibrosis or calcifications therapy was started. Almost one year after diagnosis the patient is doing well. Discussion: Abdominal pain is a well-known sign of adrenal insufficiency. To the best of our knowledge the underlying pathofysiological mechanism is poorly understood. Abdominal pain is more often seen in primary adrenal insufficiency than in secondary (or tertiary) insufficiency. For this reason the pain is probably due to mineralocorticoid deficiency rather than glucocorticoid deficiency. This case illustrates that abdominal pain can also be the presenting symptom in secondary adrenal insufficiency. Conclusion: It is important to look for other signs and symptoms of primary adrenal insufficiency, as well as secondary adrenal insufficiency in patients with unexplained abdominal pain. extensive investigation for the presence of endocrine function disorders and neoplasia was performed. Blood levels of TSH, prolactin, IGF-1,calcitonin, several tumor markers, as well as urinary excretion of cortisol,and (nor) metanefrine and 17-ketosteroids, were within the normal range. A 1 mg dexamethasone overnight suppression test was normal. However, the plasma level of chromogranine A level was elevated (239 nmol/l; normal range 0-100). Ultrasonography of the thyroid, magnetic resonance imaging of the spine and pituitary gland, colonoscopy, cystoscopy and gynaecological examination revealed no signs of a malignancy. Genetic analysis for the regulatory type I-a (RIa) subunit of protein kinase A (PRKAR1A) tumor suppressor gene, characteristic for the Carney complex, is still pending. Conclusion: Carney complex should be suspected in case of (multiple) neoplasias (mucocutaneous, cardiac, adrenal, neural) in combination with endocrine overactivity and/ or pigmented mucocutaneous lesions. Early recognition of the Carney complex may avert life-threatening embolic complications of cardiac myxomas, which otherwise can be the first manifestation. Any patient suspected of having the Carney complex should be evaluated for the presence of endocrine abnormalities and malignancies. When confirmed, first degree relatives should also be screened. 101. Carney complex Case: A 75-year-old man was admitted to our hospital because of abdominal pain. His medical history included benign prostatic hypertrophy, hypertension and polyarthrosis. His medications consisted of tamsulosin, losartan potassium, furosemide and piroxicam with pantoprazole. Besides a continuous chained pain around his upper abdomen, the patient suffered from anorexia, nausea, vomiting and lethargy since three months. On physical examination the patient was pale with a blood pressure of 111/65 mmHg. Auscultation of heart and lungs was normal. Moderate tenderness was noted over the epigastric area. Laboratory results revealed a mild normocytic anaemia (7.2 mmol/l) and hyponatremia (129 mmol/l). Renal function and potassium were normal. At first, symptoms were assigned to gastric pathology. However, gastroscopic examination revealed no abnormalities. Abdominal ultrasound was normal except for liver steatosis. Because of the combination of abdominal pain with hypotension and hyponatremia, adrenal insufficiency was suspected. A serum cortisol of 0.04 umol/l confirmed this diagnosis. ACTH-level was 2.6 pmol/l, suggestive of secondary (or tertiary) adrenal insufficiency. All other hypothalamic-pituitary-endocrine axes were suppressed. TSH level was 1.9 mU/l and FT4 level was 9.5 pmol/l. Testosterone level was 4.06 nmol/l with low LH and FSH levels (2.2 and 2.9 U/l). Prolactin level was slightly elevated (23.8 ug/l) and IGF-1 level was just normal considering the patient’s age (68 ug/l). Magnetic resonance imaging of the cerebrum showed a cystic pituitary tumor extending to the right and to the optic chiasm, presumably an adenoma with cystic degeneration, grade II to III-B/E according to Hardy’s classification of pituitary adenomas. The patient had no visual field deficits. He was started on hydrocortisone and in a few days his abdominal pain was dissolved. Levothyroxin and testosterone replacement 56 Z.A. Choudhry, J.J.M. van der Hoeven, S. Simsek, F. Stam Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 12, 1815 JD ALKMAAR, the Netherlands, e-mail: zichoudhry@hotmail.com Introduction: Carney complex is a rare multiple neoplasia syndrome assiociated with a variety of pigmented mucocutaneous lesions. Carney complex is inherited as an autosomal dominant trait. We describe a case in which the manifestations were an atrial myxoma, facial lentigines and bilateral nodular masses. Case report: A 63-year-old woman presented at our outpatient department with a progressive inguinal swelling. Her medical history consisted of a resected atrial myxoma five years before, diabetes mellitus type 2 and hypertension On physical examination, the patient was obese (body mass index 36,4 kg/m2) with a centripetal distribution of body fat. Investigation of the skin showed facial lentigines and blue naevi in the trunk. In the right groin a painless, hard mass of 5 cm was felt. Further physical examination was remarkless. A complete blood count, chemistry profile, liver and kidney functions were normal. Positron emission tomography (PET) with computed tomography demonstrated enlargement of lymph nodes in the left para-iliac region with F18-fluorodeoxyglucose (FDG) uptake. Furthermore, bilateral adrenal nodularity without uptake of FDG was seen, suggestive for primary pigmented adrenocortical disease (PPNAD). Histopathological examination of the inguinal lymph node revealed a poorly differentiated neuro-endocrine carcinoma. The coincidence of a neuro-endocrine carcinoma, atrial myxoma (in the history), lentigines, blue naevi and possible PPNAD, was suggestive for a Carney complex. Therefore, 102. Case report: uncommon cause of infertility J.P.H. van Wijk1, W.L. de Ranitz-Greven1, F.A. Groenman2, C. Kimmel2, E.W.M.T. ter Braak1 1 University Medical Centre Utrecht, Department of Internal Medicine, Heidelberglaan 100, 3508 GA UTRECHT, the Netherlands, e-mail: jwijk3@hotmail.com, 2FlevoHospital, ALMERE, the Netherlands We report a case of ovarian hyperstimulation syndrome related to FSH secreting pituitary adenoma in a 21-year-old female. The patient was referred to our hospital with a 2 year history of amenorrhea, abdominal pain, weight gain and headache. On examination, she was obese, and horizontally disposed striae were located on the breast, abdomen and legs. Furthermore, there was a large mass in the lower abdomen. Laboratory evaluation revealed extremely high estradiol (23501 pmol/l, normal for follicular phase: 180-600 pmol/l) with suppressed LH (< 0,5 IU/l, normal for follicular phase: 2-11 IU/l) and inappropriately high FSH (27 IU/l, normal for follicular phase: 3-12 IU/l). Pelvic ultrasound showed bilateral enlarged ovaries containing multiple giant cysts: the right ovary measured 10 x 18 cm and the left ovary 10 x 13 cm. The presence of an endogenous ovarian hyperstimulation syndrome was suspected. Subsequent MRI revealed pituitary macroadenoma with optic chiasm compression. Consultation of 57 the ophthalmologist confirmed bitemporal hemianopsia. Transsphenoidal resection of the macro-adenoma was performed, with an uneventful postoperative course. Immunohistologic examination showed staining for FSH, consistent with the diagnosis FSH secreting pituitary adenoma. After surgery, laboratory values normalized and the patient resumed regular menstrual cycles. Three months after surgery, the MRI showed tumour disappearance. Pelvic ultrasound showed marked involution of the ovarian masses. Within 6 months after surgery, the patient conceived spontaneously. The pregnancy course was uneventful. Recently, she gave birth to a healthy daughter. In conclusion, ovarian hyperstimulation syndrome due to a FSH secreting pituitary adenoma is a very rare medical condition. Our patient resumed regular menstrual cycles and conceived spontaneously after successful transsphenoidal resection of the adenoma. V. controlled trials (RCTs) using the total symptom score (TSS) as the outcome measure were selected and assessed for their methodological quality. A random-effect model was used for pooling in case of heterogeneity, a fixed-effect model in the absence of heterogeneity. Subgroup analyses for intravenous and oral administration of alpha lipoic acid versus placebo were conducted. Results: The search yielded 242 publications. Six RCTs met our inclusion criteria. Four RCTs were of good quality and included for statistical pooling. Overall, the pooled standardized mean difference estimated from all trials revealed a reduction in TSS scores of -2.26 (CI: -3.12 to -1.41; p=0.00001) in favour of alpha lipoic acid administration. Subgroup analyses of oral administration (-1.78 CI: -2.45 to -1.10; p=0.00001) and intravenous administration (-2.81 CI: -4.16 to -1.46; p=0.0001) confirmed the robustness of the overall result. Conclusion: Based on the currently available evidence, when given intravenously at a dosage of 600 mg once daily over a period of 3 weeks, alpha lipoic acid leads to a significant and clinically relevant reduction in neuropathic pain (grade of recommendation A). The significant improvements seen after 3-5 weeks of oral administration at a dosage of <u>></ u> 600 mg daily are not clinically relevant. DIABETES MELLITUS RESEARCH 103. Alpha lipoic acid for neuropathic pain in patients with diabetes: a meta-analysis of randomised controlled trials 104. Defining, measuring and improving perioperative diabetes care G.S. Mijnhout1, B.J. Kollen2, A. Alkhalaf1, N. Kleefstra3, H.J.G Bilo1 1 Isala Clinics, Department of Internal Medicine, Dr. van Heesweg 2, 8025 AB ZWOLLE, the Netherlands, e-mail: g.s.mijnhout@isala.nl, 2University Medical Centre Groningen, GRONINGEN, the Netherlands, 3Diabetes Centre and Langerhans Medical Research Group, ZWOLLE, the Netherlands I. Hommel, M.E.J.L. Hulscher, P.J.M. van Gurp Radboud University Medical Centre, Department of Iq Healthcare, Geert Grooteplein 21, route 114, 6500 HB NIJMEGEN, the Netherlands, e-mail: i.hommel@iq.umcn.nl Introduction: Optimal glycaemic control in surgical patients reduces mortality, rate of infections and length of stay. Guidelines and literature provide various recommendations on perioperative diabetes care. Optimal perioperative diabetes care, however, is often not achieved. This probably reflects the difficulty of implementing best practice recommendations into a complex multiprofessional setting. Aim: To define and measure perioperative diabetes care in terms of optimal professional, organizational and patientoriented quality, in order to guide development of an improvement program. Methods: To define optimal perioperative diabetes care, a systematic RAND-modified Delphi method was used to develop a set of key recommendations. Experts appraised 79 recommendations on perioperative diabetes care, extracted from international guidelines and literature, resulting in 17 indicators on professional performance, 9 indicators on organizational structure, and 4 indicators on patient outcome. Twelve additional indicators on patient- Background: Neuropathic pain is difficult to treat. The medications currently used mainly include antidepressants, antiepileptics and opioids. These medications are limited in their effectiveness, have considerable side effects, and have no effect on the processes by which hyperglycemia leads to cell damage. Alpha lipoic acid is a potent antioxidant, reported to reduce diabetic micro- and macrovacular complications in animal models. Aim: We performed a systematic review and meta-analysis of the literature in which the effectiveness of alpha lipoic acid as a treatment for neuropathic pain in patients with diabetes was evaluated. The aim of this meta-analysis was to evaluate the effects of intravenous as well as oral administration of alpha lipoic acid versus placebo. Methods: The databases MEDLINE and EMBASE were searched using the key words ‘lipoic acid’’, ‘thioctic acid’, ‘diabet * ’, and the medical subject headings (MeSH) ‘thioctic acid‘ and ‘diabetes mellitus’. Randomised placebo- 58 metformin and a sulfonylurea. To evaluated from these data if there is enough reason to conduct a prospective study. Patients and methods: 19 Overweight diabetic patients of our outpatient clinic, whose therapy with a combination of insulin and metformin was changed to the combination of incretin mimetic, metformin and sulfonylurea (new treatment), were evaluated in a retrospective study after six months of the new treatment. HbA1c and weight were measured in the beginning and after 6 months of the new therapy. The patients were asked also about their quality of life feelings after the six months of therapy. Results: 6 Patients could not be evaluated, because two patients were lost by failing and stopping the new therapy during the six months treatment and four patients were lost by lacking data. At the beginning of the new treatment the remaining 13 patients had a body mass index higher than 35.0 kg/m2, a mean HbA1c of 10.0% and a mean weight of 116.1 kilograms. Six months after the start of the new treatment the mean HbA1c was decreased to a mean of 8.6%, and the mean weight to 111.0 kilograms. Only two patients had an increase in HbA1c and only 1 patient gained weight. All the patients said to feel a better quality of life with the new treatment, than with the insulin treatment. Conclusion: In this retrospective evaluation of a small group of patients we showed in most patients a reduction in HbA1c and weight and a better quality of life with a treatment of incretin mimetics, metformin and sulfonylurea in stead of insulin and metformin. We recommend a prospective study to confirm these results and to assess which overweight diabetic patients treated with insulin can benefit from incretin mimetics. oriented quality were derived from an interview with an expert panel of diabetic patients who underwent surgery in the recent past. To measure current perioperative diabetes care, in 6 Dutch hospitals, 400 diabetic patients were identified based on the use of diabetic medication during hospitalization for a major surgical procedure. Diabetic patients who had abdominal surgery during general anesthesia, heart surgery or large joint orthopedic surgery with a minimum operative time of one hour in the period march 2009-march 2010 were included. Selected patients were approached by mail and by telephone to request permission for a medical record search on professional performance, and to complete a questionnaire on patient-oriented items. Hospital organizational structure was assessed by questionnaire. Results: Preliminary results showed that there is ample room for improvement regarding many of the indicators. For example, medical records revealed information on preoperative glycemic control in only 42% of patients. Protocols on perioperative diabetes care were present in all 6 hospitals; multiprofessional involvement in establishing and supporting adherence to these protocols varied, however, considerable. Regarding patient-oriented quality, 17% of patients received complete information on perioperative diabetes management prior to surgery. Conclusion: To improve perioperative diabetes care, we are currently performing interviews with the various professionals involved, revealing among others problems in knowledge, insight into own performance and organizational problems like a lack of agreement on mutual responsibilities. Education, feedback on professional performance, and a multiprofessionally established protocol will be part of the improvement program. Patient-oriented care will receive special attention to promote continuation of self care of diabetes patients in hospital. 106. Vildagliptin improves endothelium-dependent vasodilatation in subjects with type 2 diabetes P.C.M. van Poppel, P. Smits, C.J. Tack Radboud University Medical Centre, Department of Internal Medicine, PO Box 9101, huispost 463, 6500 HB NIJMEGEN, the Netherlands, e-mail: pleunvp@hotmail.com 105. Are incretin mimetics useful in obese insulin treated diabetic patients? C.M.L. Driessen, P.F.M.J. Spooren TweeSteden Hospital Tilburg, Department of Internal Medicine, Dr. Deelenlaan 5, 5042 AD TILBURG, the Netherlands, e-mail: chantal_driessen@hotmail.com Introduction: Cardiovascular complications are the leading cause of morbidity and mortality associated with type 2 diabetes mellitus. Endothelial dysfunction is a marker of and often precedes these vascular complications. Ideally, pharmacotherapy for type 2 diabetes not only lowers blood glucose levels but also has beneficial cardiovascular effects. Recently, incretin-based therapy has become available for the treatment of type 2 diabetes mellitus. Dipeptidyl peptidase-4 (DPP-4) inhibits the breakdown of incretin hormones including glucagon-like peptide-1 (GLP-1). GLP-1 improves endothelial function in both animals and humans. Introduction: Incretin mimetics (or GLP-1 analogs) are approved for the treatment of type 2 diabetic patients. They cause a significant reduction in HbA1c and in weight in comparison to placebo. Aim: To establish that poorly regulated obese type 2 diabetic patients using large quantities of insulin and metformin are treated more effectively and show a better quality of life with a combination of an incretin mimetic, 59 Aim: To determine the effect of the DPP-4 inhibitor vildagliptin on endothelial function in patients with type 2 diabetes. Materials and methods: 16 subjects with type 2 diabetes (age 59.8±6.8year, BMI 29.1±4.8 kg/m2, HbA1c 6.97±0.61) on oral blood glucose lowering treatment were included. Participants received vildagliptin 50 mg bid or acarbose 100 mg tid for 4 consecutive weeks in a randomised, double blind, cross-over design. At the end of each treatment period we measured forearm vasodilator responses (plethysmography) to intra-arterially administered acetylcholine (endothelium-dependent vasodilator) and sodium nitroprusside (endothelium-independent vasodilator). Results: Baseline forearm blood flow (FBF) was higher during vildagliptin treatment than during acarbose (exper imental arm 3.3 ±0.3 vs.2.5±0.2 ml.dl1.min1, p=0.02). Corresponding values in the non experimental arm were 2.7±0.3 and 2.2±0.3 ml.dl1.min1 (p=0.07). Infusion of acetylcholine induced a dose-dependent increase in FBF in the experimental arm, which was higher during vildagliptin (3.1±0.7, 7.9±1.1 and 12.6±1.4 ml.dl1.min1 in response to acetylcholine 0.5, 2.0 and 8.0 mg.dl-1. min-1) than during acarbose (2.0±0.7, 5.0± 1.2 and 11.7± 1.6 ml.dl1.min1 respectively, p=0.01 by two-way ANOVA). Treatment with vildagliptin did not significantly change the vascular responses to sodium nitroprusside. Conclusion: Vildagliptin improves endothelium-dependent vasodilator responses in type 2 diabetic subjects on oral treatment, while endothelium-independent responses are unaffected. This effect might have favourable cardiovascular implications. widespread access to the EU market, exposing large groups of patients. This makes it of crucial importance to identify safety concerns as soon as possible. Relevant safety signals in the EU are regularly communicated in so-called ‘Direct Healthcare Professional Communication’ (DHPC) or European Medicines Authority (EMA) press releases. It is unknown whether such safety signals effectively influence prescribing and dispensing of drugs. Aim: To analyse trends in dispensing patterns of rosiglitazone and pioglitazone following DHPCs and EMA press releases in the EU member state the Netherlands. Methods: Data for this study were obtained from the PHARMO Record Linking System which includes, among other issues, drug dispensing records from community pharmacies of approximately 2.5 million individuals in the Netherlands. We used linear regression analysis with dispensing volume as the outcome and time as determinant to assess the variance in dispensing volume over time. Hypothesizing that this variance would not change, the beta’s of this model were used as the outcome in a subsequent linear regression. In this second model the DHPC letters or EMA press releases were used as determinants to assess the impact of these safety communications. Adjustments were made for publication of certain relevant literature. Results: 6,165,341 million prescriptions with an ATC code for drugs used in diabetes mellitus (A10) were dispensed to 158,599 participants during the period 1998-2008. After applying exclusion criteria, 3,579,810 (58.1%) dispensed prescriptions for 112,105 (70.7%) participants were left for the analysis. The volume of rosiglitazone dispensings decreased significantly after publication of DHPCs and EMA press releases. This effect was more pronounced for dispensings prescribed by specialists than for those prescribed by general practitioners. Similar observations were made for pioglitazone. However, adjustment for certain relevant literature reduced the effect of the communicated safety issues on the proportion of dispensings. Conclusion: Although it is difficult to disentangle the effect of DHPCs and EMA press releases from the effect of reports published in the literature, our results suggest that prescribers also react to such safety communications. 107. Trends in dispensing patterns of rosiglitazone and pioglitazone in the Netherlands following safety signals during the period 1998-2008 R. Ruiter 1 , E. Visser 1, M.P.P. van Herk Sukel 2 , P.H. Geelhoed-Duivestijn3, S. de Bie1, S.M.J.M. Straus4, P.G.M. Mol5 , S.A. Romio1, R.M.C. Herings2 , B.H.Ch. Stricker1 1 Erasmus Medical Centre, Department of Epidemiology, PO Box 2040, 3000 CA ROTTERDAM, the Netherlands, e-mail: r.ruiter@erasmusmc.nl, 2PHARMO Institute for Drug Outcomes Research, UTRECHT, the Netherlands, 3 Medical Centre Haaglanden, THE HAGUE, the Netherlands, 4 College ter Beoordeling van Geneesmiddelen, THE HAGUE, the Netherlands, 5University Medical Centre Groningen, GRONINGEN, the Netherlands 108. The association between body fat and serum C3 levels is largely explained by low-grade inflammation and insulin resistance: the CODAM study N. Wlazlo1 , M. Greevenbroek 2 , I. Ferreira 2 , C.J.H. van der Kallen2, C. Schalkwijk 2, B. Bravenboer1, C.D.A. Stehouwer2 1 Catharina Hospital, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: nick.wlazlo@cze.nl, 2Maastricht University Medical Centre, MAASTRICHT, the Netherlands Introduction: In the European Union (EU), the European Medicines Agency (EMA) coordinates the centralised authorisation procedure for medicinal products. Approval through a centralized procedure facilitates a swift and 60 VI. Introduction: Serum complement factor 3 (C3) is an emerging risk marker for cardiovascular and metabolic diseases. C3 levels are closely related to body fat, but the underlying mechanisms explaining this association are still unknown. We investigated the association between several adiposity measurements and C3 and examined the role of low-grade inflammation and insulin resistance herein, since both are known correlates of adiposity and C3. Methods: Body mass index (BMI), sum of 4 skinfolds (subscapular, suprailiacal, biceps, triceps), waist circumference (WC), hip circumference (HC), waist-to-hip ratio (WHR), sagittal diameter, serum C3, homeostastis model assessment – insulin resistance (HOMA2-IR) and markers of inflammation (high sensitivity C-reactive protein, interleukin-6, serum amyloid A, haptoglobin, ceruloplasmin, soluble inter-cellular adhesion molecule-1) were determined in the Cohort on Diabetes and Atherosclerosis Maastricht (CODAM) study population (n=535; 62% men, age 59±6.9 years, BMI 28.5±4.3 kg/m2, WC 99.3±11.8 cm). The markers of inflammation were standardized and compiled into an average inflammation score. We used linear regression analysis to examine the associations of individual adiposity measurements with C3, adjusting for age, sex, type 2-diabetes mellitus, cardiovascular disease, smoking, alcohol intake and medication. Multiple mediation analyses were performed to ascertain whether, and the extent to which, these associations were independently explained by inflammation and HOMA2-IR. Results: After adjustment for covariates, all adiposity measurements were significantly and positively associated with C3 levels, with the strongest associations found for sagittal diameter (standardized regression coefficient ß=0.451; 95% CI 0.374-0.528) and WC (ß=0.422; 95% 0.342-0.502). Further adjustments for inflammation and HOMA2-IR attenuated these associations to ß=0.187 and ß=0.135 respectively. The independent mediation (expressed as standardized ß) by inflammation in the relation between WC and C3 was 0.097 (95% CI 0.0660.135), representing 23% of the total association between WC and C3 (0.097/0.422 * 100%). Additionally, the mediation by HOMA2-IR was 0.190 (95% CI 0.138-0.248), which was 45% of the total association. For all adiposity measures, 20-25% of the association with C3 was explained by low-grade inflammation, and 40-55% by HOMA2-IR, independently of one another. Conclusion: Systemic low-grade inflammation and insulin resistance may represent two independent pathways by which body fat leads to elevated C3. Increases in serum C3 may be due to changes at the level of C3 transcription in response to e.g. increased (local) concentrations of inflammatory cytokines, or loss of inhibitory effect of insulin. Moreover, decreased fatty acid storage in insulin-resistant adipocytes may provide another potential stimulus for C3 production in fat. DIABETES MELLITUS CASE REPORTS 109. Reversible loss of vision due to atorvastatin W.J. Lammers, A.F.G. Jansen, A.A.M. Zandbergen, A. Dees Ikazia Hospital, Department of Internal Medicine, Willem van Hillegaersbergstraat 12b, 3051 RJ ROTTERDAM, the Netherlands, e-mail: w.j.lammers@gmail.com Introduction: Atorvastatin is worldwide one of the most used cholesterol lowering drugs, which blocks the HMG-CoA-reductase, an important enzyme in the biosynthesis of cholesterol. A number of side effects have been reported such as myalgia, nausea, constipation, diarrhea and headache. Not much is known about visual loss as major side effect. Here we describe a patient with the onset of visual acuity problems after years of atorvastatin use. Case report: A 60-year-old patient had been followed up for many years at the Outpatient Clinic because of his metabolic syndrome. His medical history comprised hypertension, diabetes mellitus, hypercholesterolemia, adipositas, atypical thoracic pain without evidence of coronary artery disease, psychosocial problems and epicondylitis lateralis. The treatment regimen consisted of losartan, aliskiren, metoprolol, metformin and insulin, four times daily. He had been treated with atorvastatin for more than ten years. The patient was known with hypermetropia, his visual acuity after correction was 20/20. He underwent regular ophthalmologic checks, without any significant signs of diabetic retinopathy and with a first appearance of cataract of the left eye. Despite these findings a slowly progressive complaint of blurred vision of both eyes developed within 10 months. The ophthalmologist found that his visual acuity decreased to 20/40. No other new ophthalmic abnormalities were noticed. The patient lost his driver licence. Thinking of medicine-induced vision problems, the atorvastatin has been switched to simvastatin. After the switch a dramatic clinical improvement occurred and the blurred vision resolved slowly. Discussion: Atorvastatin is a widely used drug with some well-known side effects. However, ophthalmologic problems have only been reported sporadically. Also, the Dutch databank of medicine side effects, called Lareb, reports three other cases of transient blurred vision due to atorvastatin. There is nothing known about the pathophysiology of these ophthalmologic complications. Possibly, opticus neuropathy is involved. Conclusively, in patients who are on statin treatment for instance atorvastatin, drug side effects must be considered when visual loss occurs, even after many years of use. 61 110. Mastopathy: a rare complication in a young patient with type 1 diabetes VII. HAEMATOLOGY RESEARCH N.C. de Clercq, M.E.M. Rentinck Tergooi Hospitals, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: nicoliendeclercq@gmail.com 111. Increased numbers of microparticles and microparticle specific thrombin generation in patients with myeloproliferative disease M.C. van Aalderen 1 , M.C. Trappenburg 1 , M. van Schilfgaarde1, P.J. Molenaar 1, H. ten Cate2, A. Leyte1, W.E. Terpstra1 1 Onze Lieve Vrouwe Gasthuis, Department of Internal Medicine, Oosterpark 9, 1090 HM AMSTERDAM, the Netherlands, e-mail: m.c.vanaalderen@olvg.nl, 2Maastricht University, MAASTRICHT, the Netherlands Case: A 29-year-old woman was seen at the outpatient clinic with a painless mass in the right breast. Her medical history revealed type 1 diabetes mellitus from the age of 12, with secondary complications of retinopathy and nephropathy. The patient had noticed the mass 2 months before, without signs of nipple discharge or retraction. She had an aunt who died of breast cancer. Physical examination of the breast showed a tumor behind the right nipple, measuring approximately 2 cm. The left breast was normal; no enlarged axillary lymph nodes were present. Mammography showed dense fibroglandular tissue in the central part of the right breast; no discrete lesions or pathological microcalcifications were found. Acoustic shadowing was seen on ultrasound at the site of the palpable mass, measuring 3,6 by 2,1 cm. Cytology of the tumor was nonconclusive. Histological biopsy under ultrasound guidance was performed. Pathology demonstrated lymphoplasmocellular infiltration around the acini and lobuli. No signs of malignancy were seen. The clinical profile in combination with these pathologic features was characteristic of diabetic mastopathy. Discussion: Diabetic mastopathy is an unusual and often not recognized complication of diabetes. Characteristic are lymphocytic mastitis and stromal fibrosis that presents in premenopausal women with long-standing type 1 diabetes mellitus with multiple microvascular complications. Clinicopathological features include the development of irregular breast masses, which tend to be recurrent and bilateral. Clinical distinction from a malignancy can be difficult. However, the benign nature of this lesion is easily recognized by histopathological examination. Microscopy shows stromal fibrosis with signs of ductitis, lobulitis and vasculitis. Although the pathogenesis is still unknown, several mechanisms have been suggested. Possibly these lesions are due to an auto-immune reaction to the accumulation of abnormal matrix induced by hyperglycemia. After surgical excision, diabetic mastopathy tends to recur in the same location and involves more breast tissue than the preceding lesion; therefore surgical procedures should not be considered unless neoplasia has not been ruled out. Conclusion: The association between mastopathy and type 1 diabetes has been reported, but this clinical condition is poorly recognized since breast examination is not routinely performed in young diabetic patients. Recognition of this complication in patients with long-standing type 1 diabetes is important as it might save patients with documented diabetic mastopathy from being subjected to repeated breast biopsies. Introduction: Essential Thrombocythemia (ET) and Polycythemia Vera (PV) are both myeloproliferative neoplasms associated with an ill-understood high risk of thromboembolic events. In a previous study we showed elevated levels of platelet, endothelium and leukocyte related microparticles (MPs) in ET. Aim: To compare MP phenotypic profiles and MP-dependent thrombin generation of ET and PV patients to healthy controls to further explore the putative role of MPs in myeloprolific thrombophilia. Materials and methods: In plasma samples from 18 ET patients, 24 PV patients and 20 controls, levels and cellular origin of MPs were determined by flowcytometric analysis and MP-dependent thrombin generation by our adaptation of the Siemens ETP assay. Results: ET patients had significantly higher numbers of platelet derived MPs (CD41+) than PV patients and controls (median: ET 9000, PV 5970, controls 4100 x 106/l; p<0.001). MPs expressing the endothelial marker CD62E were highly abundant in ET and moderately increased in PV compared with controls (median ET 2975, PV 324, controls 80 x 106/l; p<0.001 and p=0.02). Leukocyte derived (CD45+) MP numbers were small but elevated in all patients (median: ET 77, PV 112, controls 21 x 106/l; p<0.001; p<0.001) and correlated with leukocyte count (p<0.001). In line with their MP numbers, ET patients had a higher MP-dependent endogenous thrombin potential (ETP) than controls (median ET 278, PV 212, controls 147 milliAbsorbance; p<0.01). Conclusion: ET and PV patients had elevated numbers of MP with phenotypic profiles reflecting different degrees of platelet, endothelium and leukocyte ancestry. MP specific thrombin generation, which was highest for ET patients, appeared equally proportional to ET, PV and control MP numbers suggesting similar procoagulant properties. VIII. HAEMATOLOGY CASE REPORTS 113. Cholestasis as presenting symptom of Hodgkin lymphoma K. Boslooper1 , M. Hoogendoorn1, K. van der Linde1, R.E. Kibbelaar2 1 Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: boslooperk@gmail.com, 2Pathologie Friesland, LEEUWARDEN, the Netherlands 112. A woman with smoking Buttocks?! N.A.F. Verheijden, T. Ermens, J.W.J. van Esser Amphia Hospital Breda, Department of Internal Medicine, Molengracht 21, 4818 CK BREDA, the Netherlands, e-mail: NVerheijden@amphia.nl Paraneoplastic features are frequently observed in patients with Hodgkin lymphoma. These phenomena can mislead clinicians and delay the diagnostic process. We describe a case of a previously healthy 76-year-old men presenting with fatigue, transient diarrhea and a skin rash in combination with laboratory tests showing severe cholestasis. Extensive diagnostic work-up including endoscopy, CT scan and liver biopsy, performed by the hepatologist, did not reveal the diagnosis. Several months later the patient was admitted to our hospital with fever, weight loss and night sweats. A FGD-PET/CT showed diffuse PET positive lymphadenopathy. Lymph node and bone marrow biopsy showed Hodgkin lymphoma, stage IV-B. The patient was successfully treated with systemic chemotherapy consisted of adriamycin, bleomycin, vinblastin and dacarbazin (ABVD) and achieved complete remission after six cycles of chemotherapy. The liver function test nearly normalized after finalizing the treatment. Liver involvement can be detected in Hodgkin lymphoma. It has a variable etiology, including hepatic infiltration of lymphoma, extrahepatic obstruction by enlarged lymph nodes, hemolysis or concurrent infectious hepatitis. However, jaundice and severe cholestasis as the first presenting symptom is rare. This may be due to a paraneoplastic phenomenon, which is defined as vanishing bile duct syndrome or idiopathic cholestasis. The pathogenesis of these entities is largely unknown, but among the different hypotheses cytokine release by lymphoma cells is frequently postulated. The cholestasis may be fully reversible after successful treatment of the disease. These paraneoplastic phenomena should therefore be considered in cholestasis of unknown cause. Case history: A 42-year-old woman, with a history of epilepsy, had a routine visit to her neurologist. Laboratory check up showed an abnormal leukocyte count and the patient was referred. She had a smoking history of 30 pack years and used no alcohol. Her father was known with a non Hodgkin lymphoma and bladder carcinoma. Physical examination was normal, especially no lymphadenopathy or hepatosplenomegaly were present. Laboratory assessment showed: Hb 8.2 mmol/l (7.5-10.0 mmol/l), leukocytes 16.5 x 109/l (4-10 x 109/l), leukocyte differentiation; lymphocytes 11.7, monocytes 0.7 and granulocytes 4,1 and a thrombocyte count of 198 x 109/l (150-400 x 109/l). The peripheral blood smear showed ‘Buttock cells’. Flowcytometry of peripheral blood revealed a polyclonal increase of mature B-lymphocytes. A diagnosis of persistent polyclonal B-cell lymphocytosis (PPBL) due to nicotine abuse was made. Discussion: Persistent polyclonal B-cell lymphocytosis is a benign disease, characterized by the presence of typical binucleated lymphocytes on peripheral blood smear. These ‘Buttock cells’ are lymphoid cells with a cleft and prominent nucleolus. PPBL is predominantly seen in females and is associated with nicotine abuse. The pathophysiology of PPBL is unknown, but its association with HLA DR 7 suggests a genetic predisposition. Flowcytometry is mandatory to differentiate PPBL from monoclonal B cell proliferation as in chronic lymphatic leukaemia and other lymphoproliferative diseases. Reviewing the literature, three patients diagnosed with PPBL, developed a non Hodgkin lymphoma. In all other cases PPBL had a benign cause. Quit smoking should be the therapy of choice. Conclusion: Persistent polyclonal B-cell lymphocytosis is a benign disease in which peripheral blood smear shows binucleated lymphocytes (Buttock cells). PPBL is associated with nicotine abuse, but there also seems to be a genetic predisposition. To prevent extensive work-up, knowledge of this disease entity is mandatory. 114. ‘Copycat’ D.G.J. Robbrecht, A.A.M. Ermens, R.S. Boersma, J.W.J. van Esser Amphia Hospital, Department of Internal Medicine, Molengracht 21, 4818 CK BREDA, the Netherlands, e-mail: DRobbrecht@amphia.nl Introduction: We present two patients that illustrate how a difficult but intriguing diagnostic process ultimately lead to the diagnosis angioimmunoblastic T-cell Lymphoma (AITL). 62 63 Case report: Case 1: a 51-year-old male was referred because of progressive red spots on both legs since 1 day. Preceding referral he complained of malaise, pain in his wrists and ankles, shortness of breath, and nocturnal transpiration without fever, weight loss or itching. There was no history of unsafe sex, blood transfusion, visits to foreign countries nor did he use any medication. On physical examination purpura were seen on both legs, furthermore multiple enlarged lymph nodes and splenomegaly were present. He had a normocytic anemia, kreatinin 102 umol/l (n: 59-104 umol/l, LDH 436 U/l (n: max. 250 U/l) and urinary screening was unremarkable. Auto-immune serology was negative, viral serology showed positive IgM for cytomegalovirus and parvovirus. Serum elektrophoreses showed polyclonal hypergammaglobulinemia and complement profile was decreased. Skin biopsy revealed leukocytoclastic vasculitis. Differential diagnosis consisted of viral infection, auto immune disease or lymphoma. Lymph node and bone marrow examination revealed AITL and chemotherapy was initiated subsequently. Case 2: a 63-year-old male presented with fever and rash. On physical examination a palpable liver, generalised rash and ankle edema were found. Laboratory examination showed leukocytosis with marked eosinophilia and liverfunction abnormalities. Chest X ray was normal and ultrasound of the abdomen showed a homogenously enlarged liver. Liver biopsy and bone marrow examination showed marked eosinophilia. Differential diagnosis consisted of (drug) allergy, auto-immune disease, parasitic infection, or hyper eosinophilic syndrome. A few days later patient was readmitted because of a normocytic anemia of 4,2 mmol/l and reticulocytopenia, auto anti D and aspecific cold and warmth auto antibodies were present. Computed tomography showed lymphadenopathy and an enlarged liver. Lymph node histology showed a reactive process consisting of plasmacells, lymphocytes and eosinophils, bone marrow examination showed a hypercellular marrow with mature eosinophilia. Unfortunately patient died secondary to a myocardial infarction. T cell receptor rearrangement analysis showed monoclonal T cells. A retrospective diagnosis of AITL was made. Discussion: Cytokine production in AITL causes, amongst others, polyclonal B-cell stimulation and a myriad of symptoms mimicking infection, auto-immune disease, allergy etc. Knowledge of this entity may prevent unnecessary delay and initiation of treatment. 115. Introduction: Portal vein thrombosis (PVT) is a rare thrombosis that can be associated with Philadelphianegative myeloproliferative diseases (MPD). Diagnosing MPD in patients with PVT can be difficult because of the effects of portal hypertension, such as hypersplenism, gastrointestinal bleeding and haemodilution. Since the mutation in the Januskinase2 gene (JAK2 V617F) is present in the majority of patients with MPD, testing is an important diagnostic tool in recognizing atypical or latent MPD. To illustrate the difficulties in the diagnostic workup, we present a patient with thrombosis of the splanchnic system as the presenting symptom of a latent MPD. Case: We saw a 68-year-old man, complaining of sub-acute onset upper left quadrant abdominal pain, nausea and fever. An abdominal CT-scan showed extensive portal vein thrombosis along with splenic and superior mesenteric vein thrombosis, as well as splenic infarction in an enlarged spleen. Also, ascites and a thickened mesenterium were observed. Laboratory tests at presentation showed the following: haemoglobin 7.8 mmol/l (8.0-10.6), haematocrit 40%, MCV 76 fl (81-96) Leukocyte count 20.8 * 109/l (4.0-11.08 * 109), mainly neutrophils, CRP 142 mmol/l (<10.0). Kidney function and electrolytes were unremarkable, liver enzymes were slightly elevated. The initial thrombocyte count was 622 * 109/l and ranged from 318 to 682 x 109/l (150-400 * 109) during his stay in hospital. Endoscopic studies revealed no gastrointestinal pathology. Blood cultures were positive with bacteroides fragilis indicating a concurrent peritonitis. We started treatment with anticoagulants and antibiotics. Screening for thrombophilia revealed a lupus anticoagulans. Additional testing for JAK-2 mutation was positive. Bone marrow biopsy was consistent with MPD essential thrombocytemia. However, in one year follow-up, no treatment targeting the essential trombocytemia was initiated because of completely normal blood cell counts, including the platelets. Discussion: In this case report we demonstrate pitfalls in the diagnostic workup of patient with PVT. Concurrently with extensive thrombosis of the splanchnic system, our patient was diagnosed with splenic infarction and peritonitis. In the setting of unreliable clinical and haematological parameters, the identification of JAK-2 mutation can be pivotal in diagnosing latent MPD. Furthermore, follow-up of our case with persistent normal blood cell counts, illustrates that finding MPD underlying a PVT does not inherently warrant initiating MPD treatment. Whether the JAK mutation itself has intrinsic prothrombotic capacity remains to be illuminated. Pitfalls in diagnosing myeloproliferative disease in the presence of portal vein thrombosis G. Douma, M. Hoogendoorn Medical Centre Leeuwarden, Department of Internal Medicine, H. Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: gea.douma@znb.nl 64 116. Right ventricular failure due to chloroma as initial presentation of a patient with acute myeloid leukemia syndrome with multilineage dysplasia. Two weeks later she presented with progressive fatigue and pancytopenia. Another bone marrow puncture demonstrated progression to MDS-RAEB type 2. Chromosomal analysis revealed complex cytogenetic abnormalities. Due to her young age doubt rose about the diagnosis and we investigated whether the patient, despite her normal physical appearance, suffered from Fanconi’s anemia. A chromosome breakage test with mitomycine confirmed this diagnosis Discussion: Fanconi’s Anemia (FA) is a rare autosomal recessive disorder typically diagnosed at young age. Patients have characteristic physical anomalies, including short stature, café-au-lait spots and abnormalities of thumb, radius and genitourinary tract. Bone marrow failure typically develops during the first decade of life. In addition, they have increased risk of developing malignancy, acute myelogenous leukemia being the most frequent. Ear, nose and throat tumors and gynecological malignancies are much more prevalent as well. There are 13 genes involved in FA, all of which cooperate in a common DNA-repair pathway. The mutation in the FANCC gene is the most abundant FA mutation occurring in the Netherlands. This mutation is associated with a relatively mild phenotype. Bone marrow transplantation is the only curative option for these patients. Our patient will receive treatment with azacitidine to reduce blast count followed by hematopoietic stem-cell transplantation with myeloablative conditioning. Conclusion: Fanconi’s anemia is a rare cause of pancytopenia which should be considered in young adults presenting with pancytopenia. M.L. Wumkes, W. Deenik Tergooi Hospitals, Department of Internal Medicine, Nachtegaalstraat 5c, 3581 AA UTRECHT, the Netherlands, e-mail: mlwumkes@live.nl Chloromas (granulocytic sarcomas) occur in 3-5% of patients with acute myeloid leukemia (AML). A few patients with chloroma involving cardiac structures have been reported in literature so far. We describe a 78-year-old female who presented with dyspnoe, coughing, fatigue and weight loss. Her medical history was besides ear problems unremarkable. At physical examination she was dyspnoeic with signs of right ventricular failure. Electrocardiography showed atrial fibrillation without signs of cardiac ischemia. Chest X-ray revealed interstitial edema and pleural effusion. The patient was diagnosed with cardiac failure caused by atrial fibrillation and was treated with diuretics, digitalization and anticoagulants. Transthoracic echocardiography revealed right ventricular hypertrophy and a mass in the right atrium. Peripheral blood revealed 5.2 x 109 leukocytes with 35% blasts in the differential count. Flowcytometry of the blasts in the peripheral blood showed CD11c, CD13, CD33, CD34, CD117 and MPO positivity, consistent with myeloid blasts. Analysis of the pleural effusion revealed myeloblasts with identical immunophenotypic features. Palliative radiotherapy of the right ventricle was scheduled, because the patient was not a candidate for intensive chemotherapy. However, the patient diseased shortly after diagnoses due to cardiac failure before she received radiation therapy. Right ventricular failure is a very rare initial presentation of a patient with AML. 117. 118. Löffler endocarditis, a rare complication of a rare disease N.D. Niemeijer1 , P.L.A. van Daele1, O.J.L. Loosveld 2, B.J.M. van der Meer2 1 Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: ndniemeijer@gmail.com, 2 Amphia Hospital, BREDA, the Netherlands A rare cause pancytopenia in an adult patient A. de Haar-Holleman, S.K. Klein Meander Medical Centre, Department of Internal Medicine, PO Box 1502, 3800 BM Amersfoort, the Netherlands, e-mail: a.de.haar@meandermc.nl Introduction: The hypereosinophilic syndromes (HES) are a rare group of disorders marked by the sustained overproduction of eosinophils. It is defined by an eosinophil count of more than 1500 cells per microliter for at least 6 months, in addition to damage to target organs, such as the heart and lungs. Eosinophilic myocarditis is a major cause of morbidity en mortality among patients with HES. We present a patient with idiopathic hypereosinophilic syndrome and cardiac involvement. Case report: A 37-year-old man presented to the emergency department with one month of fatigue and five days of progressive dyspnoea. Three months earlier he had been Case report: A 24-year-old female presented at our emergency department with deep anemia (hemoglobin 3.9 mmol/l). Her history was blank. Besides pallor, we found no abnormalities with physical examination. Laboratory investigations showed pancytopenia (leukocytes 1.5 * 109/l, thrombocytes 51 * 109/l). Thinking of acute leukemia a bone marrow examination was performed showing elevated cellularity and major abnormalities in all three lineages consistent with myelodysplastic 65 Case: A 70-year-old man presented with normocytic anemia (Hb 6.2 mmol/l) and progressive pain in the pelvic girdle. Physical examination was normal. Laboratory investigation didn’t show any signs of hemolysis or deficiencies, there were no signs of plasmaceldyscrasia, autoimmune diseases or infections. Repeated X-rays and ultrasounds were normal. A bone marrow examination did not reveal any aberrations besides minor dysplasia, too little for any diagnosis. One year later myalgia worsened and ESR rose to 119mm/ hr; but a PET-CT scan yielded no abnormalities and a temporal artery biopsy did not show giant cell artritis. Therefore polymyalgia rheumatica was suspected and prednisone 15mg was started. Symptoms vanished promptly. But four months later, the patient was admitted because of severe intermittent bone pain of the shoulder and pelvic girdle and hence an elevated lactate dehydrogenase (LDH) of 1059 IU/l, without hemolysis. MRI showed diffuse infiltration of the bone marrow and a skeletscintigraphy showed multiple hot spots suggesting metastases. Again bone marrow aspiration was performed, showing normal morphology, but cytogenetic testing showed 46 XY, add(12). Immunophenotyping revealed that 9% of cells were large blast-like cells. One week later a third bone marrow aspirate was performed in an affected region and a monotonous cell population, without classic hematopoietic features was seen with blue/grey cytoplasm and round to oval nuclei without nucleoli. Immunophenotyping showed 74% aberrant leukocytes (weak CD45+/CD13+/CD15/CD16+/CD117/CD34-/partially MPO positive), suggesting immature myeloid cells with some degree of maturation. Bone biopsy revealed immature myeloid cells. Finally, the diagnosis myeloid sarcoma was made based on the cytogenetic testing, the positive markers CD13, MPO and negative CD34 and the remarkable findings on MRI and skeletscintigraphy. The patient was treated with daunarubicin and cytarabine, giving relieve of all complaints. Unfortunately he passed away a few weeks later because of ileus and cardial weakness. Discussion: Myeloid sarcoma (MS) is an extramedullary tumor composed of immature myeloid cells, which is rarely diagnosed. Most of them occur with concurrent bone marrow or blood involvement by a myelodysplastic syndrome of a myeloproliferative disorder like acute myeloid leukemia. MS is often associated with distinctive cytogenetic and molecular abnormalities. It can be treated like AML, but survival rates are low. MS is an elusive disease, which may present in many different forms and locations with subsequently a high variety of clinical signs and symptoms. diagnosed with severe eosinophilia. Extensive diagnostic evaluation at that time revealed no cause of secondary eosinophilia. High dose corticosteroids were prescribed but later stopped because of ineffectiveness. On admission we saw an ill-looking, dyspnoeic man, temperature 38.1 °C with signs of shock. Laboratory evaluation revealed a high number of eosinophils of 84.2 x 109/l. Chest X-ray showed pulmonary congestion. On the electrocardiogram ST-elevations in V1-V3 and ST-depressions in various leads were found. Transthoracic echocardiography revealed a large mass in the left ventricle. In the intensive care unit, the trachea was intubated and the patient mechanically ventilated because of respiratory insufficiency. Cardiac magnetic resonance imaging showed endomyocardial fibrosis and necrosis and a large thrombus in the left ventricle. Löffler endocarditis was diagnosed. Therapy was initiated with diuretics, methylprednisolone and anti-coagulation. Because of ineffectiveness interferon alpha and hydroxycarbamide were added. After this the eosinophils declined gradually. Recovery was complicated by bone marrow depression with anemia and thrombocytopenia and haemoptysis with bilateral pulmonary consolidations, possibly eosinophilic consolidations. Discussion: Idiopathic hypereosinophilic syndrome is a rare systemic disease defined by the combination of prolonged eosinophilia, evidence of organ involvement and no evidence for other known causes of eosinophilia. It affects mostly men between 20 and 50 years of age, with a peak in the 4th decade of life. Cardiac involvement is frequently found. The damage to the heart ranges from early necrosis to subsequent thrombosis and fibrosis. It is believed that eosinophils are directly cytotoxic and release toxic substances like enzymes, reactive oxygen species, pro-inflammatory cytokines and arachidonic acidderived factors. Prednisone and hydroxyurea constitute the first-line therapy. In therapy-resistant cases interferon alpha, which inhibits degranulation of eosinophils, is a possibility. Besides this, routine cardiac therapy with diuretics, afterload reduction and anticoagulation is necessary. The prognosis is poor, and death is usually due to congestive heart failure. 119. Myeloid sarcoma; a rare diagnosis after a challenging diagnostic process H.A. Polinder-Bos, N. Josephus Jitta, L.A. van Boven, S.K. Klein Meander Medical Centre, Department of Internal Medicine, Postbus 1502, 3800 BM AMERSFOORT, the Netherlands, e-mail: h.a.polinder@meandermc.nl Introduction: Anemia is frequently seen, sometimes it hides special diagnosis. 66 120. Dialysis using a Theralite filter in addition to chemotherapeutical treatment of multiple myeloma with acute renal failure: a multidisciplinary approach. Case report showed a significant decrease compared to the pre-dialysis level. In between dialysis, levels rose but an overall reduction in sFLC levels was achieved. Conclusion: The addition of intense dialysis using the Theralite filter to chemotherapeutical treatment with bortezomib/dexamethasone might be a very effective approach to the treatment of patients with acute renal failure due to multiple myeloma induced cast nephropathy. E. Verweij, J.J. Beutler, R.M.J. Hoedemakers, H.A.M. Sinnige Jeroen Bosch Hospital, Department of Hematology/ Nephrology, Tolbrugstraat 11, 5211 RW ’s-HERTOGENBOSCH, the Netherlands, e-mail: mail@evaverweij.net 121. ITP and CMV: to treat, or not to treat? Introduction: In September 2010 our patient was diagnosed with multiple myeloma stage III B according to Durie and Salmon (stage III according to the New International Staging System) based on serum Free Light Chain levels (sFLC, type Lambda) of 13300 mg/l. Other laboratory abnormalities included a creatinin of 808 umol/l, Hb 4,4 mmol/l, calcium 3,33 mmol/l (normal albumin) and B2-microglobulin 33,30 mg/l. Upon diagnosis patient had 44% monoclonal plasma cells in the bone marrow aspirate and multiple osteolytic lesions. Renal biopsy confirmed cast nephropathy combined with deposition of free light chains. Methods: Treatment with bortezomib 1,3 mg/m2 (day 1, 4, 8 and 11) and dexamethasone 20 mg (day 1, 2, 4, 5, 8, 9, 11 and 12) was started. On day 8, dialysis using a Gambro Theralite filter started (daily the first week with one non-dialysis day, followed by dialysis every other day). sFLC levels were determined before and immediately after dialysis. The Gambro Theralite filter consists of a membrane designed to target free light chains and other proteins up to 15-65 kD. Regular filters are not permeable because of much smaller pores. Theoretically the filter removes more sFLC than plasma exchange (which is more expensive and has not been proven effective). During dialysis, frequent measurements of electrolytes (phosphate, magnesium and calcium in particular) and albumin are necessary to prevent (potentially severe) deficiencies. Bortezomib is a small molecule and concentrations may be reduced during dialysis. However it has a short half-life (?20 minutes). Therefore, determination of plasma levels is not useful. Administering doses immediately after dialysis or administration of bortezomib on non-dialysis days is adequate. Results: Bortezomib and dexamethasone treatment started on day 1. On day 8, sFLC levels remained stable at 13300 mg/l and patient underwent the first dialysis with the Theralite filter. sFLC level measurement immediately after dialysis showed a spectacular decrease (of 78% to 2880 mg/l). Unfortunately levels rose within 24 hours after dialysis. Patient underwent dialysis on day 9, 10, 12-15, 17, 18, 20, 22 and 25. Every sFLC level post-dialysis M.L. Nijland, A.M. de Kreuk Sint Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: m.nijland@slaz.nl Introduction: Immune thrombocytopenic purpura (ITP) is a common cause of acquired thrombocytopenia. ITP is often considered to be idiopathic, but in some cases ITP is associated with viral infections. In daily practice, results of serological tests and/or viral load-assays only become available after a few days. Management of CMV-associated ITP may become a challenge if platelet counts do not recover promptly after initial treatment. Cases: We review two cases of CMV associated thrombocytopenia with a different clinical course. Patient 1: A 63-year-old woman on adjuvant chemotherapy for breast cancer, presented with large haematomas and a febrile temperature. Physical examination showed multiple large haematomas and petechiae. She had no signs of hepatosplenomegaly or lymphadenopathy. Patient 2: A 50-year-old man presented with petechiae and gingival and rectal bleeding. He had complaints of tiredness since a few months. Physical examination showed petechiae but no other abnormalities. In both cases, the initial laboratory tests showed a platelet count of 2 x 109 IU/l, a mild lymphocytosis with atypical lymphocytes, and a mild elevation of liver enzymes, leading to the hypothesis of ITP, possibly induced by CMV. Initially, we treated both patients with intravenous immunoglobulins (IVIG) and a platelet transfusion, in combination with methylprednisolone 1000mg/day for 3 days in patient 1 and with 40 mg prednisone/day in patient 2. In patient 1, CMV IgM was positive, and the viral load at diagnosis was 10100 DNA-copies/ml. After 1 week the platelet count was 177 and she received no further treatment. In patient 2, CMV IgM was also positive, and the viral load was 61110 DNA-copies/ml. His platelet count remained < 10 x 109 IU/l, and his bleeding only responded partially to tranexaminic acid treat-ment. Subsequently, we started prednisone (1mg/kg per day) treatment, however still 67 day, followed by oral prednisolone (1 mg/kg/day). Because no universal guidelines were available, we decided to treat the WM pragmatically as low-grade lymphoma with chloorambucil and rituximab from July until December 2010. Renal function improved but remained moderately impaired (creatinine 127 mmol/l; eGFR 38 ml/min). IgM levels decreased and Hb increased to normal ranges (IgM 1.81 g/l; Hb 7.8 mmol/l). Corticosteroids were tapered and stopped. Discussion: WM is a lymphoplasmocytic proliferation leading to the secretion of monoclonal IgM. Renal complications in WM are rare, and most often the result of membranoproliferative type glomerulonephritis due to intracapillary IgM deposition with or without the detection of cryoglobulinaemia. However, AL-amyloidosis, cast nephropathy and Fanconi’s syndrome have also been described. Most reports describe complete recovery of renal failure after steroid treatment. This case showed that renal failure can be the only presentation of WM, and that restoration of renal function can at least partially be obtained with appropriate treatment. without response. Treatment with valganciclovir resulted in a decrease of CMV DNA, but not in improvement of the platelet count. Only when prednisone was tapered and discontinued under valganciclovir treatment, the platelet count finally increased. After two months, CMV DNA was negative and the platelet count was 51 x 109 IU/l. Discussion: CMV infection can cause ITP, possibly through molecular mimicry or immune dysregulation. CMV may also directly infect megakaryocytes leading to diminished platelet production. In this situation, immunosuppression could actually worsen or prolong thrombocytopenia, as probably happened in case 2. We recommend considering non-immunosuppressive therapies for the initial treatment of ITP in all cases where an underlying CMV-infection is suspected. 122. A rare case of renal failure R.B. Takkenberg, H.P. van den Berg, J.J. Weening Tergooi Hospitals Blaricum, Department of Internal Medicine, Rijksstraatweg 1, 1261 AN BLARICUM, the Netherlands, e-mail: btakkenberg@tergooiziekenhuizen.nl ymphoma and performed an additional liver biopsy. This biopsy showed sinusoidal infiltration of atypical T-cells; immunophenotyping confirmed the diagnosis of liver involvement of the T-LGL. T-LGL usually is an indolent non-Hodgkin lymphoma. It is a clonal disease of large granular lymphocytes. The pathogenesis is unknown but the disease is often associated with Human T-lymphotropic virus, cytokine disregulation and impaired apoptosis. Clinicians should consider T-LGL in patients with recurrent neutropenia without an other reasonable explanation or recurrent infections. Seventy percent of the patients do need treatment with methotrexate, or cyclophosphamide, or cyclosporin A because of symptomatic disease. Combination chemotherapy can be started in case of more severe disease activity. Because of the extreme weight loss, our patient was treated with a combination of cyclophosphamide, vincristine and prednisone every three weeks. After four cycles of CVP-chemotherapy a CT-scan showed a significant decrease in hepatosplenomegaly compatible with a partial remission. Conclusion: T-LGL-leukemia is an indolent T-cell malignancy that should be considered in case of unexplained neutropenia. More aggressive variants should be treated with combination chemotherapy. colon. She underwent an extended right hemicolectomy with ileodescendostomy. Histology showed no signs of ischemia, but suggested a medication induced colitis. Differential diagnosis suggested thalidomide or NSAID’s as a possible initiating agent. Postoperatively the patient was admitted to the intensive care unit. During this admission she developed pneumocystis carinii pneumonia and Adult Respiratory Distress Syndrome, anastomotic leakage followed by relaparotomy and ascites infected with candida albicans. She died 37 days after presentation. No postmortem examination was performed. Conclusion: In this case report a bowel perforation following thalidomide treatment was described. There is one literature report of four cases of thalidomide associated bowel perforation in one hospital suggesting that it is highly improbable that this is a co-incidental finding. More reports of this possible side effect of thalidomide can possibly contribute to unraveling its causative mechanisms. 124. T-cell large granular lymphocyte leukemia; not always indolent 123. Thalidomide and bowel perforation: a case report Introduction: Waldenström’s macroglobulinaemia (WM) or lymphoplasmocytic lymphoma is a rare lymphoid neoplasia, accounting for 2% of all hematological malignancies, with only 75 new cases per year in the Netherlands. Renal function impairment can be found and is most often the result from immunological light chain nephrotoxicity. We describe a patient with renal failure, based on a rare presentation of WM. Case report: A 75-year-old woman presented with progressive fatigue, shortness of breath on exercise and weight loss. Her medical history revealed hypothyroidism and M. Sjögren since 2008. Physical examination showed a blood pressure of 90/45 mmHg with a pulse of 80/min. There was no pitting edema on the extremities. Laboratory investigations revealed an erythrocyte sedimentation rate (ESR) of 40 mm/h, hemoglobin (Hb) 6.3 mmol/l with a mean cell volume (MCV) of 85 fl, leukocytes of 6.2 x 109/l and platelets of 336 x 109/l, creatinine of 235 mmol/l (eGFR 19 ml/min), with a urea of 13.7 mmol/l. Total serum protein was 90 g/l, and electrophoresis revealed a monoclonal IgM level of 22.1 g/l. Urine analysis showed no abnormalities except for a high micro protein albumin of 120 mg/24 hours. A renal biopsy showed a profound interstitial cellular infiltrate composed of CD20+/IgM+ lymphoplasmocytic cells. Cytology and histology of bone marrow showed no infiltration. The diagnosis WM with diffuse renal infiltration and renal failure was established. The anemia was interpreted as caused by renal impairment. Because renal function deteriorated rapidly, she was treated with three pulses of methylprednisolon 500mg/ F.M. van Haalen, I. van Dijk, F.H.M. Cluitmans, A.M. Schrander-van der Meer Rijnland Hospital, Department of Internal Medicine and Intensive Care, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: f.v.haalen@rijnland.nl Introduction: Thalidomide is an oral agent with immunomodulatory and antiangiogenic properties. Besides its teratogenic side effects, thalidomide possesses other important toxicities including constipation, peripheral neuropathy, sedation, fatigue, thromboembolism, rash and pruritus. Bowel perforation is not a frequent side effect of thalidomide. In the literature speculations are found that thalidomide may contribute to bowel perforation by a number of mechanisms. Bowel perforation following thalidomide has been previously described in only a few cases. Case-report: A 58-year-old female recently diagnosed with multiple vertebral compression fractures presented to the emergency room with hypercalcaemia. Bone marrow cytology showed multiple myeloma. One week after starting therapy with dexamethason 40 mg a day, thalidomide 100mg a day and pamidronate (APD), she became progressively dyspnoeic, developed peripheral edema, clouding of consciousness and diarrhea with rectal loss of blood. Computed tomography showed free air formation intra-abdominal suspect of stomach or proximal duodenal perforation. Subsequent surgery demonstrated multiple perforated lesions in the transverse 68 M.C. Telgen1, J. Slomp1, J. van Baarlen2, W.M. Smit1 1 Medical Spectrum Twente, Department of Internal Medicine, Ariensplein 1, 7511 JX ENSCHEDE, the Netherlands, e-mail: m.telgen@mst.nl, 2Laboratorium Pathologie Oost, ENSCHEDE, the Netherlands 125. A testicular tumor which turned out to be AML R. Wester, V. Mattijssen Rijnstate Hospital, Department of Internal Medicine, Weurtseweg 69, 6541 AN NIJMEGEN, the Netherlands, e-mail: westerruth@gmail.com Case report: A formerly healthy 54-year-old woman was referred to our outpatient clinic with a two months history of an altered defecation pattern, night sweats and weight loss of thirteen kilograms. Physical examination revealed a hepatomegaly and an anal process. Although a gastrointestinal malignancy was the most probable diagnosis, a colonoscopy did not show abnormalities. The anal process appeared to be a thrombotic hemorrhoid. Laboratory results showed a LDH 232 U/l, hemoglobin 5,8 mmol/l, thrombocytes 331 109/l, leukocytes 6,6 109/l, with an absolute neurophil count of 0,41 109/l. The differentiation of the peripheral blood showed atypical lymphocytes with granules. Immunophenotypic there was an abnormal T-cell population (CD 3+, CD 8+, CD 57+, CD16weak, TCR-AB+ and diminished expression of CD7 and loss of expression of CD5) suggestive for T-cell large granular lymphocyte leukemia (T-LGL). Additional T-cell gene rearrangement showed a monoclonal population. A bone marrow aspiration and biopsy confirmed this diagnosis. Although T-LGL mostly has an indolent course, our patient had an aggressive disease with B-symptoms and hepatosplenomegaly on CT-scan. Therefore we wanted to exclude a more aggressive lymphoma that could also fit the phenotype, such as an alphabeta positive hepatosplenicl- Introduction: Myeloid sarcoma is a rare manifestation of acute myeloid leukemia (AML), characterized by the occurrence of myeloid masses at an extramedullary site. Despite the curiosity, it is important to recognize this entity because of the fast clinical deterioration and the important therapeutic consequences. That myeloid sarcoma may occur at any site of the body is demonstrated with this patient with AML, presenting as a testicular tumor. Case: A 65-year-old man presented at the urology department with a growing mass in his right testicle. Testicular cancer was suspected, and an orchidectomy was performed. Serum tumor markers were normal. Histological evaluation revealed a malignancy which could not be classified. Two weeks later, the consulting internist discovered pathologically enlarged lymph nodes in the neck, and an elevated LDH. Malignant lymphoma was suspected. Peripheral blood counts and bone marrow examination at that moment were normal. A lymph 69 node biopsy was performed. Waiting for the results the patient became progressively ill, with dyspnoea and nausea. He developed pleural effusion. Four weeks after the orchidectomy, the laboratorium results deteriorated, with blasts appearing in his peripheral blood smear, trombocytopenia, diffuse intravascular coagulation, and renal failure. Another bone marrow biopsy revealed more than 50% myelo-monoblasts. In the mean time the pathologist concluded, that the malignant cells in the testis and the lymph node were young monoblasts (myeloid sarcoma). The combination of these results led to the diagnosis of AML with extensive extramedullar localisation, complicated by disseminated intravascular coagulation and renal failure. The patient’s condition deteriorated very quickly, and remission induction chemotherapy for AML (ICE; Idarubicine, Cytarabine and Etoposide) was started. Very soon there was improvement in condition and in renal function. Although it resulted in a complete remission of bone marrow, lymph nodes and pleural effusion, we had to refrain from further chemotherapy because of weak general condition and a very small chance of curation, because of the detrimental presentation of the AML in combination with age of the patient. Conclusion: We demonstrate a patient with AML who presented with a tumor in his right testicle and lymphadenopathy. Differential diagnostic considerations included testis carcinoma and non-Hodgkin-lymphoma. However, occasionally patients with AML present with extramedullary disease. It may precede overt bone marrow disease, as in our patient. Because of the fast clinical deterioration, and the therapeutic consequences, being intensive chemotherapy with curative intent, it is of the utmost importance to recognize myeloid sarcoma. as were two PCR’s for Borrelia DNA. The patient was treated with adjuvant radiotherapy and received two weeks of doxycycline 100 mg once daily. He is in complete remission for 2 years now. PCMZL are indolent, extranodal lymphomas, classified as marginal zone lymphomas (MZL’s) according to the WHO-EORTC. MZL’s arise as extranodal acquisition of lymphatic tissue at sites of chronic inflammation. MZL’s are clearly associated with infectious, antigenic stimuli that precede the transformation into a lymphoid malignancy. The most common type of MZL is mucosaassociated lymphoid tissue (MALT)-lymphoma of the stomach, which is associated with Helicobacter pylori gastritis. Remarkably, in Helicobacter pylori associated MALT-lymphoma of the stomach, the B-cell tumour clone is not selected against a bacterial epitope, but carries autoreactive rheumatoid factor-immunoglobulins that undergo somatic hypermutation. They develop as a secondary lymphoid response to chronic inflammation. When typical API2/MALT1 fusion cytogenic abnormalities are absent, certain MALT-lymphomas have been known to show complete histological remission after antibiotic eradication therapy. PCMZL has been associated with Borrelia Burgdorferi infection, i.e. Lyme’s disease. There is a striking geographical variation in the association between Borrelia burgdorferi and PCMZL. While a clear association has been seen in Europe, this association could not be demonstrated in the United States and Asia-Pacific. The geographical variation is interesting with regards to the fact that different genotypes of spirochetes are responsible for Lyme’s disease in Europe and the United States. Furthermore the vector that transmits the spirochete to humans differs from the one in Europe and studies within the Ixodes ticks have demonstrated an influence of the tick’s saliva on the differentiation of T-cells into either Th1 or Th2 lineage commitment. The association between PCMZL and infection with Borrelia Burgdorferi could have important clinical implications since, if the B-cell tumor clone is antigenically driven, its progression into malignant lymphoma could be arrested by antibiotic therapy or, at least, delayed to prevent more aggressive therapies such as radiotherapy and chemotherapy. 126. Primary cutaneous marginal zone lymphoma in the presence of occult Borrelia infection. P.G.N.J. Mutsaers, H.P.J. Visser Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 12, 1815 JD ALKMAAR, the Netherlands, e-mail: mutsaersp@gmail.com A 54-year-old man presented with a solitary subcutaneous tumour on the lateral side of the right leg present for six months. Excision biopsy showed a primary cutaneous marginal zone lymphoma (PCMZL), which was excised with free margins. Dissemination examination did not reveal metastatic disease. Although the medical history was negative for a tick bite, the Borrelia serology was strongly positive. Additional blood investigation showed presence of rheumatoid factor. Direct staining of the excision tissue for Borellia burgdoferi was negative, 127. Is early stage chronic lymfatic leukemia a risk factor for severe cytomegalovirus infection? E.H.C.J. Buster, E.F.S. van Velsen, D. Cheung, J. Keijman, J.A. Riedl, M-D. Levin Albert Schweitzer Hospital, Department of Internal Medicine, Albert Schweitzerplaats 25, 3018 AT DORDRECHT, the Netherlands, e-mail: e.buster@asz.nl 70 The second patient is a seventy-eight years old man who was seen in the outpatient clinic because of a IgG kappa, stage I multiple myeloma. One year after the first presentation he progressed into stage IIIB for which he was treated with VAD-chemotherapy (vincristine, adriamycine, dexamethason). Evaluation after three cycles showed a markedly regression. After the fourth course the patient complained of a light discomfort in the abdomen. After the fifth course he was admitted to the hospital because of progressive abdominal pain. At physical examination a mass was palpable. A diagnostic CT of the abdomen showed a very-large mass with encasement of the right renal artery, vena cava inferior and the right ureter. A biopsy revealed malignant plasma cells compatible with an extra-medullary localization of the multiple myeloma. Therapy was switched to bortezomib with dexamethason. After two cycles patient developed slight back pain and progressive lymphedema of the right leg. A new CT-abdomen showed progression of the tumor mass. Given that first and second line chemotherapy was not successful, we switched to palliative treatment. We showed two cases with an extraordinarily course of a multiple myeloma. The first patient presented with an extensive extra-medullary localization and the second developed such during treatment. In both cases a rapidly progressive course was observed. A 56-year-old male with early stage chronic lymphocytic leukemia (CLL) and COPD was admitted after five days of high fever and chills without specific complaints indicating a cause of the fever. The fever persisted for 18 days while the patient was receiving broad-spectrum antibiotic therapy and prednisone. During the hospital stay dyspnea progressively worsened and the patient underwent a bronchoscopy. Bronchoalveolar lavage showed evidence of CMV pneumonitis. Treatment with ganciclovir was initiated and the patient’s body temperature gradually declined and normalized, and dyspnea gradually resolved. Bone marrow aspiration biopsy and CT-scan confirmed early stage CLL (Rai stage 0, Binet stage A). There were no sign of secondary immunoglobulin deficiency, paraprotein or transformation to diffuse large B-cell lymphoma. CMV pneumonitis is a rare presentation of CMV infection in patients without evidence of immunodeficiency. 128. Two patients with an extraordinary course of a multiple myeloma I.H.A. Zegers Catharina Hospital, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: ingrid_zegers@hotmail.com We present two cases with an extraordinary course of multiple myeloma. The first patient is a seventy-nine years old man who presented himself with abdominal pain, difficulties with urinating and a swollen left leg. Laboratory investigation showed an acute renal insufficiency. Computer-tomography scanning (CT-scan) of the abdomen showed widespread lymphadenopathy with encasement of the ureters, arteria abdominalis, vena cava inferior and both iliacofemoral arteries. On PositronEmission-Tomography (PET)scan there was widespread metabolic active lymphadenopathy in the abdomen, pelvic cavity and multiple small bone metastasis. Pathological examination of a lymphnode revealed a multiple myeloma, monoclonal for IgG lambda with blastair features. The patient received three times CHOP-chemotherapy (cyclofosfamide, vincristine, doxorubicine, prednisone). Evaluation by means of CT-thorax/abdomen and PET-CT showed a markedly reduced tumoractivity. After another three cycles of CHOP-chemotherapy a new CT-scan was performed. Except for a local laesion at the right urether no abnormalities were found. However on a PET-CT accomplished four days later, widespread lymphadenopathy in the abdomen with hydronephrosis of the right kidney, bone metastasis and pleural effusion were seen. The patient was admitted in the hospital but deteriorated very fast and died ten days later. IX. ONCOLOGY RESEARCH 129. Screening for DPYD * 2A mutations: preventing severe 5-fluorouracil related toxicity in Meander Medical Centre M.C. van der Goes, J.M. van Dodewaard, M. van Wijnen, M.M. Malingre, H.J. Bloemendal, C.J. Rodenburg Meander Medical Centre, Department of Internal Medicine, Utrechtseweg 160, 3818 ES AMERSFOORT, the Netherlands, e-mail: mc.vander.goes@meandermc.nl Background: Capecitabine, an oral prodrug of 5-fluorouracil (5-FU), and 5-FU are frequently used chemotherapeutic agents and are catabolized by the enzyme dihydropyrimidine dehydrogenase (DPD). Numerous genetic mutations have been identified in the DPD gene locus (DPYD). Few mutations, among which the DPYD * 2A with prevalence of 1.8 percent in the Dutch population, result in decreased enzymatic activity and increase the risk of severe toxicity. We screened patients planned for treatment with 5-FU/capecitabine for the presence of the DPYD * 2A mutation in order to prevent severe toxicity. 71 Methods: In the period from march 2009 until october 2010 259 cancer patients were screened for the presence of the DPYD * 2A mutation prior to receiving chemotherapy. All patients required treatment with monotherapy capecitabine or combination chemotherapy including 5-FU/capecitabine. A high-throughput real-time PCR test was used. Results: In total 259 patients were screened. The mean age was 62 years and 62% of the patients were female. Of the 259 patients 58% had colorectal cancer, 30% breast cancer and 12% had other cancers (e.g. gastric and oesophageal cancer). Fourty-eight percent of the patients were treated in the adjuvant setting, 38% in the palliative setting and 14% in the neo-adjuvant setting. Monotherapy with capecitabine was given in 26% of the cases, combination therapy including 5-FU/capecitabine in 74%. Two patients were found to be DPYD * 2A heterozygote and one was homozygote. In the homozygote patient, no enzymatic activity was detected in the mononuclear cells and chemotherapy was withheld. In one of the heterozygote patients capecitabine was given with a 50% dose reduction, which resulted in minor toxicity. Chemotherapy was withheld in the other patient. Of the 256 patients without a DPYD * 2A mutation, still 8 percent required hospital admission because of severe 5FU/capecitabine related toxicity. Conclusions: Screening for DPYD * 2A mutations presumably prevented severe or even lethal toxicity in three patients. On the other hand, severe toxicity requiring hospital admission developed in 8 percent of patients. A possible explanation could be that these patients have another mutation and/or have diminished DPD enzymatic activity. Further analysis is in progress whether this is the case and to see if screening for DPD deficiency is useful in the clinic. and cyclophosphamide in clinical studies, which is most frequently performed in selected patients. However, the frequency of cardiotoxicity of trastuzumab in non-selected patients in clinical practice is unknown. Here we describe the cardiotoxicity in a retrospective study of breastcancer patients treated with trastuzumab. Materials and methods: In a retrospective single centre study we considered all HER2Neu-receptor positive breast cancer patients who underwent treatment with trastuzumab from March 2001 until August 2010. Trastuzumab was prescribed in two different settings: adjuvant and palliative. In the adjuvant setting trastuzumab was preceded by antracycline containing treatment regiments. After this, trastuzumab was administered in combination with Paclitaxel, followed by trastuzumab monotherapy for one year. Whereas in the palliative setting trastuzumab was administered as initial treatment in combination with Paclitaxel. Afterwards trastuzumab was continued until relapse in the latter patient population. Left ventricular ejection fraction (LVEF) was assessed by MUGA-scan or 2 or 3D-echocardiography. Results: In total 215 woman received treatment with trastuzumab and had received follow-up by MUGA-scan or echocardiography. Two hundred (93%) were treated with trastuzumab after an anthracycline containing regimen and fifteen (7%) received trastuzumab without previous treatment with anthracyclines. Sixty-seven of all patients (31%) had a decline in LVEF of moren than 10%. Of these patients 18 demonstrated a decline of 10 to 14% and 49 demonstrated a decline of more than 15%. Seven of the 15 patients treated only with trastuzumab had a decline in LVEF of more than 10%, of which six had a decline of > 15%. Of the patients with a decline in LVEF two patients received angiotensin-converting enzyme inhibitor because of asymptomatic decreased LVEF. Forty-five of the forty-nine patients who had a decline of > 15% recovered to an LVEF > 45% during and after treatment with trastuzumab. Conclusion: Cardiac follow-up is of critical importance in the treament of patients with trastuzumab because of the high incidence of cardiotoxicity. 130. Incidence of cardiotoxicity of trastuzumab in Her2Neu positive breast cancer patients: a retrospective cohort study C. Liesting, M.J.M. Kofflard, M-D. Levin Albert Schweitzer Hospital, Department of Internal Medicine, 3318 AT DORDRECHT, the Netherlands, e-mail: c.liesting@asz.nl Introduction: Chemotherapy has been proven to be a helpful and efficient modality in the treatment of breast cancer patients both in adjuvant and palliative settings. HER2neu-receptor blocking agents, such as trastuzumab, have evolved as promising agent in the treatment of breast cancer with overexpression of the human epidermal growth factor receptor 2 protein (HER2). A well-known downside of treatment with trastuzumab is the increased incidence of cardiotoxicity. The incidence of cardiotoxic effects of trastuzumab varies from 2-5% when used as a single agent to 25% when combined with anthracyclines X. ONCOLOGY CASE REPORTS 131. Bevacizumab associated caecal perforation in a patient with advanced breast cancer: a bitter pill to swallow Introduction: Vascular endothelial growth factor (VEGF) is a potent angiogenic factor that is overexpressed in many human tumours and associated with tumour progression and poor prognosis. Bevacizumab (Avastin®) is a humanized monoclonal antibody that recognizes and blocks VEGF-A. In clinical setting it has been shown to be effective in the treatment of patients with advanced colorectal, lung, renal, and breast cancer. Case report: A 60-year-old female patient presented to our emergency department with abdominal pain and fever. Her medical history revealed advanced breast cancer with bone and liver metastases for which she recently received 2 courses of paclitaxel and bevacizumab as first line palliative chemotherapy (paclitaxel 90 mg/m2 i.v. on days 1, 8, and 15, and bevacizumab 10 mg/kg i.v. on days 1, and 15 of a 4 weekly cycle) On physical examination her abdomen was tender, but neither signs of peritonitis nor ileus were found. Extensive laboratory testing and abdominal CT revealed no focus for her symptoms, which were then attributed to chemotherapy-induced mucosal toxicity. Despite increasing doses of morphine and antibiotic treatment (cefuroxim and gentamicin), abdominal pain progressed during the subsequent 2 days, with abdominal rigidity and rebound tenderness. At that time intraperitoneal free air was shown on a repeated CT scan. At emergency surgery, fecal peritonitis caused by a hand-size proximal caecal perforation was noted, for which ileocecal resection was performed. Pathological examination of the resected specimen showed extensive necrosis due to vascular ischemia; no evidence for thrombosis or malignancy was found. After surgery, the patient had a complicated 5 weeks lasting postoperative course attributable to poor wound healing, pneumonia and an infected central venous access device. Discussion: GI-perforation is a rare complication of bevacizumab with an estimated incidence of 0-15%. Its’ pathophysiology is not completely understood, but potential mechanisms are ischemic perforation by inducing regression of normal blood vessels in the GI tract, regression and necrotisation of GI located tumours, and inhibition of normal healing of ulcers and surgical wounds. Risk factors mentioned in the literature are recent bowel surgery, bowel obstruction, high doses of bevacizumab, and treatment of patients with colorectal and renal cell carcinoma. The mortality rate of this complication is reported to be as high as 50%. Conclusion: We report the complicated clinical course of a patient suffering from bevacizumab associated GI-perforation, which should be suspected in all patients treated with this agent and presenting with acute abdominal pain. 132. Bone metastases from a granulosa cell tumour of the ovary C.J. Compaijen, M. Bierhoff, R.W. ten Kate, P.W.G. van der Linden, M.I. Grootscholten Kennemer Gasthuis, Department of Internal Medicine, Boerhaavelaan 22, 2035 RC HAARLEM, the Netherlands, e-mail: c.compaijen@kg.nl Introduction: A granulosa cell tumour is a sex cord stroma cell tumour. In general, granulosa cell tumours from the ovary do not metastasise. They usually have a relatively good prognosis and primary treatment is surgical excision. Metastases are predominantly abdominal, whereas bone metastases are extremely rare. Case: A 63-year-old woman presented with back pain, tingling of the abdominal skin and bladder dysfunction. Her medical history showed a granulosa cell tumour in 1988 for which total extirpation was performed. In 2007 a recurrence was treated with debulking and chemotherapy (3 cycles of BEP). A new a recurrence 2 years later was again treated with chemotherapy (6 cycles of carboplatin/palcitaxel) with a good response (inhibin B from 2083 to 159 ng/l). Physical examination showed paresis of both legs and dysesthaesia from the xyphoid downwards. Laboratory analysis showed an increase of inhibin A and inhibin B levels. A magnetic resonance imaging scan of the spine was performed and showed a pathological fracture of the first thoracal vertebra, with a tumour mass and compression of the myelum. Further there where diffuse bone metastases. Computer tomography of the thorax and abdomen confirmed the bone metastases, besides growth of pulmonary and lymph node metastases with a new mass in the pelvis. Because it is extremely rare for a granulosa cell tumour to metastasise to the bone, a biopsy was performed to exclude other causes of bone disease. The biopsy showed granulosa cells, which were inhibin positive. There were no more therapeutic options for our patient with extended metastatic disease of a granulosa cell tumour and a high risk of a transverse myelitis. She was transferred to a hospice for palliative care and died several weeks later. Conclusion: Metastases of a granulosa tumour may rarely present with symptomatic bone lesions. 133. Paraneoplastic hypoglycemia in a patient with gastrointestinal stromal tumour on palliative imatinib treatment H. Visser, C.E.H. Siegert, W.L.E. Vasmel Sint Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: h.visser@slaz.nl F.A. Klok, L.T. Vlasveld, N.I. Weijl Bronovo Hospital,Bronovolaan 5, 2579 AX THE HAGUE, the Netherlands, e-mail: f.a.klok@lumc.nl 72 73 Introduction: Non-islet cell tumor induced hypoglycemia (NICTH) is a rare paraneoplastic syndrome characterized by recurrent fasting hypoglycemia in non diabetic patients. Recently NICTH was de-scribed in patients with gastrointestinal stromal tumours (GIST), with and without imatinib treat-ment. Case: A 84-year-old woman was admitted to our hospital because of drowsiness. Her medical history revealed a GIST of the stomach four years previously, for which she underwent partial gastric resec-tion. Unfortunately, two months before presentation, extensive intraperitoneal and hepatogenic metastases of GIST were diagnosed. She started imatinib (400 mg daily) treatment. One week before admission her family noted she frequently seemed to lose consciousness. Her drowsiness appeared to be related to hypoglycemia’s. Her fasting glucose was 1.6 mmol/l, although she did not use any antidiabetics. Additional laboratory findings showed low levels of C peptide (0,18, nmol/l; normal range 0.30-2.35 nmol/l) and insulin (< 0,2 U/l; normal range 6-27 mU/l). Also, IGF-I (36 ng/l; normal range 52-165 ng/l)) and IGFBP-3 (0,84 mg/l; normal range 1.40-3.20 mg/l)) were decreased, while IGF-II (511 ng/l; normal range 280-610 ng/l) was normal. She was treated with glucose infusions and imatinib was discontinued. After a few days she was euglycemic and could be discharged with dietary advises. Discussion: GIST are the most common type of mesenchymal malignant tumour of the gastrointesti-nal tract. Patients with metastatic or unresectable GIST are successfully treated with imatinib. Since 2003 occurrence of NICTH in patients with GIST has been reported. In contrast to patients with hy-perinsulinemic hypoglycemia, these patients have low serum insuline and C-peptide concentrations during hypoglycemia. Hypoglycemia is induced by overproduction of proinsuline like growth factor II (pro-IGF II) which stimulate insulin receptors. IGF’s circulate in the blood bound to IGF-binding pro-teins (IGFBP). In patients who suffer NICTH, serum concentrations of IGF II are normal, altough IGF-I and IGFBP-3 are found to be reduced. Unfortunately pro-IGF II was not measured in our patient, but other laboratory findings are compatible with the diagnosis NICTH. Some case reports mention pa-tients with GIST on imatinib treatment. The specific pathogenetic role of imatinib in patients with GIST and NICTH remains to be resolved. Conclusion: Hypoglycemia due to NICTH in patients with GIST is a very rare phenomenon. It has been described even as the first symptom of GIST. Moreover, hypoglycemic episodes can be trig-gered by imatinib treatment, as was the case in our patient. 134. Incidental pulmonary embolism in oncology patients; a frequent finding with unknown prognosis M. van der Veer, A.P. Hamberg, W.E.J.J. Hanselaar Sint Franciscus Gasthuis,Department of Internal Medicine, Kleiweg 500, 3045 PM ROTTERDAM, the Netherlands, e-mail: m.vanderveer@sfg.nl Introduction: The association between cancer and venous thromboembolism (VTE), compromising deep venous thrombosis (DVT) and pulmonary embolism (PE) is well known. Next to the malignancy, the presence of metastases and anti-cancer therapy have a contributable risk for VTE. Recently, there have been literature reports concerning PE found by incidence in oncology patients. We describe the occurrence of incidental PE in two patients with cancer and summarize the data available on prevalence, risk factors and prognosis of incidental PE. Cases: The first case is a 40-year-old female who was diagnosed with stage IV non small cell lung cancer. Therefore she received Cisplatin and Gemcitabine. After two cycles of these cytotoxic agents, a CT scan showed tumorprogression and PE. Low molecular weight heparin (LMWH) in a full therapeutic dose was applied. The following months her malignancy was progressive and four months after diagnosis she died of respiratory failure. The second case is a 64-year-old male diagnosed with a progressive castrate refractory prostate cancer and he recently received radiation therapy because of painful bone metastases. A CT scan was performed as baseline scan before the commencement of first-line cytotoxic therapy showing incidental PE. Treatment with LMWH was initiated. He currently is receiving docetaxel as first-line cytotoxic treatment. Discussion: Incidental PE is a common finding in patients suffering from cancer.Multiple studies show a prevalenco of 6% incidental PE in inpatients and a 3-3.8% prevalence in ambulatory patients. These studies also note that 75% of the incidental PE was undetected at the initial CT image interpretation, suggesting many cases are not diagnosed in daily practice. Incidental PE is frequently observed in patients with gynaecological, lung, genitourinary, ovarian and pancreatic cancer. This matches the malignancies associated with symptomatic PE. Metastatic disease, high leukocyte count, platin-based chemotherapy and recent diagnosis of cancer increase the risk for incidental PE. One study showed a high mortality rate after asymptomatic proximal DVT in patients with an acute medical illness, including cancer. No specific data about the survival after incidental PE in oncology patients alone are available. Conclusion: Incidental PE in oncology patients is a common finding and thus a part of daily practice of those caring for these patients. The risk factors for incidental PE in patients with cancer match those for symptomatic PE. 74 The survival after an incidental PE in oncology patients remains unclear. Further research is needed to establish the prognosis after incidental PE. immediate therapy was started with high-dose cortico steroids and after broncho-alveolar lavage, broad spectrum antibiotics were added. Within 24 hours symptoms and radiologic findings diminished and oxygen requirement decraesed. Antibiotics were stopped after two days of therapy. Both patients recovered fully from their gemcitabine induced severe acute lung injury and corticosteroids could be tapered out. Conclusion: We describe two cases of pancreatic cancer which both developed severe acute lung injury after treatment with gemcitabine. Early recognition of the gemcitabine induced pulmonary toxicity is vital as this pneumonitis is rapidly progressive and with early adequate treatment the condition can fully recover. 135. Gemcitabine induced pulmonary toxicity in two patients with pancreatic cancer J.W.T. van Enschot, G.J. Creemers Catharina Hospital, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: joris.v.enschot@cze.nl Introduction: Gemcitabine-associated acute lung injury is a rare cause of dyspnea after treatment with gemcitabine. The clinical symptoms are aspecific. Diffuse crackles can be heard during auscultation of the lungs. The symptoms may occur days to months after administration. Computed tomography may show bilateral diffuse ground-glass opacities. Discontinuation of the drug, administration of corticosteroids and pulmonary support is the mainstay of treatment. The mechanism of toxicity in gemcitabineinduced lung toxicity remains unclear. Case 1: A 50-year-old man with a pT3N0Mx adenocarcinoma of the pancreas was treated adjuvantly with gemcitabine (Gemcitabine 1000 mg/m2 day 1, 8, 14 every 4 weeks x6). After his fourth course of chemotherapy he presented himself at the emergency department with complaints of fever and dyspnea. Except from dyspnea, physical examination revealed no abnormalities. Laboratory investigation showed a C-reactive protein of 33 mg/l (normal 0-10 mg/l) and leukocyte count of 8.7 x 109/l (normal 4-10 x 109/l). Arterial blood gas analyses showed a PaO2 of 88 mmHg (normal 80-100 mmHg). X-ray showed minimal consolidations in the right upper lobe. Treatment was started with broad-spectrum antibiotics. Despite this therapy the condition of the patient deteriorated rapidly with a PaO2 of 56 mmHg and the X ray showed diffuse bilateral interstitial markings. Gemcitabine induced pneumonitis was considered and high dose corticosteroids were started. Within 24 hours the patient had less dyspnea and during the next days radiographic findings improved dramatically. Case 2: A 56-year-old man diagnosed with a cT3N1M1 adenocarcinoma of the pancreas was treated palliatively with gemcitabine. After his third course of chemotherapy he complained of dry cough, high fever and severe dyspnea. Arterial blood gas analyses showed severe hypoxemia with a PaO2 of 56 mmHg. C-reactive protein was 140mg/l and leukocyte count was 7 x 109/l. Chest radiography showed bilateral interstitial opacities and computed tomography showed evident bilateral central perihilar areas with ground-glass configuration. Given the high suspicion of gemcitabine induced pneumonitis 136. Large bowel metastasis in metastatic renal cell carcinoma 21 years after immunother S.M. van Dorp, G.J.P.M. Jonkers, F.H.M. Cluitmans, A.M. Schrander-van der Meer, M.J.F.M. Janssen Rijnland Hospital, Department of Internal Medicine, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: s.v.dorp@rijnland.nl Introduction: A man with rectal blood loss turned out to have a late colonic metastasis of metastatic RCC with an unique disease free interval of 21 years after treatment with adoptive immunotherapy. Case report: A 73-year-old man -transferred from the regional academic centre- presented with rectal blood loss without other symptoms. In 1989 he was diagnosed with RCC with osseous and pulmonary metastasis. He had a nephrectomy and extraction of the metacarpus I. In addition, he was treated by intravenous interleukine-2 and LAK-cell therapy. He attained complete remission, until January 2010. Because pulmonary embolism, the patient was treated with warfarin. In August 2010 he noticed rectal blood loss. Colonoscopy revealed a polypoid tumor in the colon transversum. Pathologic examination disclosed a localization of RCC, positive on S-100 marker. CT scanning of chest and abdomen showed no signs of metastatic disease. Because of obstruction he underwent resection of the transverse colon. Discussion: In 1985, S.A. Rosenberg reported his observations on the systemic administration of LAK cells and recombinant interleukin-2 to patients with metastatic cancer. During this treatment, referred to as adoptive immunotherapy, lymphocytes from patients with advanced metastatic cancer where obtained by repeated leucapheresis and incubated in interleukine-2 to generate lymphokine-activated killer cells (LAK cells). These LAK cells were reinfused in combination with the intravenous 75 administration of interleukine-2. In a study population of 25 patients, 11 patients showed tumor regression and 1 patient showed complete remission. In 1987 these results were confirmed in a population of 157 patients, of whom 36 patients with advanced RCC. In the latter 11% reached complete remission. Unfortunately most patients with complete remission relapsed later on. Because of the severe toxic side effects due to capillary leakage, with a mortality of 2,7%, its limited effectiveness and high financial burden this treatment has been abandoned. In the Netherlands only few patients have been treated according to this method of which results are unknown. The latest Cochrane review about immunotherapy for advanced RCC in 2005, concluded that treatment with interferon-a complementary to nephrectomy has proven to be the most effective form of immunotherapy. The combination with interleukine-2 gives no additional effect. Conclusion: This case report describes a late colonic metastasis of metastatic RCC after treatment with adoptive immunotherapy. Although gastrointestinal metastasis are known and tend to occur later than metastasis at the usual sites, the disease free interval of 21 years is exceptional. of doxorubicin and cyclophophamide and 12 weekly cycles of trastuzumab and paclitaxel the LVEF was 72%. Four days after the 1st 3-weekly course of trastuzumab, she was admitted to the hospital for rhythm observation on account of recurrent syncopal episodes. A nine-seconds cardiac arrest with sinoatrial block was observed at rest, followed by a slow nodal escape rhythm. After pacemaker implantation trastuzumab monotherapy was continued. Conclusion: This is the first reported case of asytole after trastuzumab treatment. As the sinoatrial node does not express HER2, there is no clear explanation for this complication. 138. Long lasting pruritus as manifestation of a growing colonic polyp A. Wennemers, R. Heijligenberg, H.K. van Halteren Gelderse Vallei Hospital, Department of Internal Medicine, Willy Brandtlaan 10, 6716 RP EDE, the Netherlands, e-mail: halterenh@zgv.nl Introduction: Pruritus can be an epiphenomenon of malignant disease, either because of skin infiltration by tumor cells, or due to (epi)dermal autoimmune inflammation. We describe a case with an exceptionally long interval between onset of pruritus and cancer diagnosis. Case report: A 69-year-old male was referred for colonoscopy because of iron-deficiency anemia. For the past 4 years he had suffered from continuous burning pruritus, which increased during hot showers and had led to sleepless nights. The dermatologist had refrained from skin biopsy, because the skin appeared macroscopically normal. The pruritus was refractory to treatment with hydoxyzin, acrivastatin, desloratadin, lidocain ointment and UV-light therapy. Colonoscopy revealed an adenocarcinoma of the coecum. A laparoscopic right hemicolectomy was performed and a pT3N1 adenocarcinoma was recovered. After the operation the pruritus disappeared completely. Conclusion: The temporal relation between hemicolectomy and disappearance of pruritus strongly suggests that pruritus onset was caused by a growing colonic polyp. The immunogenicity of colonic polyps makes this hypothesis plausible. 137. Asystole as complication of trastuzumab treatment H.K. van Halteren, A. Wennemers, R. Walhout, D. Agterhuis, R. Heijligenberg Gelderse Vallei Hospital, Department of Internal Medicine, Willy Brandtlaan 10, 6716 RP EDE, the Netherlands, e-mail: halterenh@zgv.nl Introduction: Trastuzumab is a monoclonal antibody directed against the human epidermal growth factor receptor 2 (HER2). It has proven to be highly effective in the adjuvant/palliative treatment of breast cancers with HER2 overexpression. Trastuzumab also binds to HER2-expressing cardiomyocytes and treatment has been shown to decrease left ventricle contractility in up to 25% of patients. In contrast with anthracyclins, trastuzumab cardiotoxocity does not appear to be cumulative and has shown to be reversible with treatment discontinuation. Rechallenge with trastuzumab may be well-tolerated. There are no reports on trastuzumab treatment-related arrythmias. Case-report: A 65-year-old woman with no previous history of cardiopulmonary events underwent a radical mastectomy because of a pT1N1M0 infiltrating ductal carcinoma of the left breast. Since the tumor appeared HER2-positive, but hormone receptor-negative, she was referred for chemoimmunotherapy with trastuzumab. Before initiation of treatment the left ventricular ejection fraction (LVEF), as estimated by means of Multi Gated Acquisition Scanning, was 70%. After four 3-weekly cycles 139. Central nervous system involvement of multiple myeloma Introduction: Multiple myeloma (MM) is a clonal B-cell malignancy, characterized by the presence of neoplastic proliferating plasma cells. Primary MM is mainly located in the bone marrow, but may invade other tissues and organs, leading to an atypical clinical presentation as is demonstrated in our case. Case-report: A 71-year-old woman was presented to the neurology department with unilateral sensory loss of the face which had developed in several days. Her medical history included MM, with an IgA lambda M-protein level of 49 g/l at onset, one year before presentation. The MM was treated with melphalan, thalidomide and prednisolone, and became in complete remission five months before presentation. On physical examination she had an unilateral sensory loss of the face, without other abnormalities. MRI of the brain and spine revealed a mass close to the left nervus trigeminus, suggestive for a schwannoma or a meningeoma. However, analysis of the cerebrospinal fluid (CSF) showed an elevated protein level of 950 mg/l with a monoclonal plasma cell population with lambda-expression. The diagnosis of central nervous system (CNS) involvement of MM was made. Despite the start of intrathecal chemotherapy (cytarabine) the patient died several days after the diagnosis due to progressive neurologic symptoms and signs. Discussion: CNS involvement in MM is a rare complication with an estimated incidence of approximately 1%. It is defined by the presence of monoclonal plasma cells in the CSF. Evidence of monoclonality is mandatory, as plasma cells can be seen in several infectious and non-infectious conditions. The exact etiology remains unknown. Several hypotheses are (1) direct continuous spread of osteolytic skull lesions, (2) haematogenous spread of plasma cells seen in plasma cell leukemia, or the spread of lymphoid cells, progenitors of plasma cells, and (3) continuous growth of plasma cells in the CNS during the course and treatment of MM, while the drugs used in MM cannot pass the blood-brain barrier. The clinical presentation covers a diffuse array of neurological symptoms and signs. Treatment options include combinations of systemic chemotherapy, intrathecal chemotherapy and cranial irradiation. Despite treatment, CNS involvement of MM has a poor prognosis with a median survival of two months. Conclusion: The presented case demonstrates a patient with CNS involvement of MM after complete remission. Although it is a rare manifestation, unexplained neurologic signs and symptoms in a patient with MM, even when in apparent remission, should prompt to look for monoclonal plasma cells in the CSF. 140. Pleural and peritoneal effusion and an ovarian tumour. Not always malignant M.L. Wumkes, H.P. van den Berg Tergooi Hospitals, Department of Internal Medicine, Nachtegaalstraat 5c, 3581 AA UTRECHT, the Netherlands, e-mail: mlwumkes@live.nl The combination of a pelvic tumour, pleural effusion and ascites has been known since the late 19th century. The features of the disease were described by Meigs and Cass in 1937. Today, Meigs’ syndrome is defined as the co-existence of benign ovarian fibroma, pleural effusion and ascites. We describe a 55-year-old postmenopausal woman who presented with dyspnea and recent abdominal pain. Her medical history revealed hypertension, appendectomy, cholecystectomy and melanoma. Examination of the lungs revealed decreased respiratory sound and attenuation at the right side. There was also an abdominal mass just above the pubic bone. Laboratory investigation, except CA-125 (300 kU/l), was unremarkable. Computed tomography revealed right sided pleural effusion, ascites and a large solid ovarian tumour of 11 x 10 x 8 cm as well as an enlarged uterus. Cytologic examination of the pleural effusion and ascites was negative for malignant cells. Histologic analysis of the ovarian tumour biopsy revealed fibroma. Shortly afterwards patient presented with increasing abdominal pain caused by the tumour. During surgery both ovaries including the tumour and uterus were resected. Final histology revealed a fibrothecoma originating from the left adnex, without signs of malignancy. She recovered uneventful. There’s no indication for further treatment. The trias of non-malignant pleural effusion, ascites and a benign ovarian tumour is also known as Meigs’ Syndrome. Fluid accumulation like pleural effusion and ascites is related to substances like vascular endothelial growth factor (VEGF) that raise capillary permeability. Resection of the tumour results in elimination of ascites and pleural effusion. Several cases of Meigs’ syndrome have been reported in association with raised serum CA 125 levels. Thus, neither ascites or pleural effusion, nor an elevated CA 125 is necessarily indicative of an epithelial ovarian cancer in a woman with a pelvic tumour. 141. Asystole as a complication of trastuzumab treatment D.E. Agterhuis, M. Wennemers, H.K. van Halteren, R.J. Walhout Gelderse Vallei Hospital, Department of Internal Medicine, Willy Brandtlaan 10, 6716 RP EDE, the Netherlands, e-mail: Dinetteagterhuis@gmail.com Y.H.M. Poel, H.P.J. Visser, W.A.T. Slieker Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 12, 1815 JD ALKMAAR, the Netherlands, e-mail: yvonne_poel@hotmail.com 76 77 Introduction: Trastuzumab is a monoclonal antibody directed against the human epidermal growth factor receptor 2 (HER2). It has proven to be highly effective in the adjuvant/palliative treatment of breast cancers with HER2 overexpression. Trastuzumab also binds to HER2-expressing cardiomyocytes and treatment has been shown to decrease left ventricle contractility in up to 25% of patients. In contrast with anthracyclins, trastuzumab cardiotoxocity does not appear to be cumulative and has shown to be reversible with treatment discontinuation. Rechallenge with trastuzumab may be well-tolerated. There are no reports on trastuzumab treatment-related arrythmias. Case-report: A 65-year-old woman without cardiopulmonary history underwent a radical mastectomy because of a pT1N1M0 infiltrating ductal carcinoma of the left breast. Since the tumor appeared hormone receptornegative but HER2-positive, she was referred for chemoimmunotherapy with trastuzumab. Before initiation of treatment the left ventricular ejection fraction (LVEF), as estimated by means of Multi Gated Acquisition Scanning, was 70%. After four 3-weekly cycles of doxorubicin and cyclophophamide and 12 weekly cycles of trastuzumab and paclitaxel, the LVEF was 72%. Four days after the 1st 3-weekly course of trastuzumab, she was admitted to the hospital for rhythm observation on account of recurrent syncopal episodes. Routine ECG and laboratory tests were normal. A nine second cardiac arrest with sinoatrial block was observed at rest, consequently followed by a slow nodal escape rhythm. After pacemaker implantation trastuzumab monotherapy was continued. Conclusion: This is the first reported case of asystole after trastuzumab treatment. As the sinoatrial node does not express HER2, there is no clear explanation for this complication. high aniongap (AG) metabolic acidosis (pH 7.38, pCO2 2.9kPa, pO2 14kPa, HCO3- 12.4 mmol/l, BE -10.6mmol/l, albumin corrected AG 30.5 mmol/l) with elevated lactate (20mmol/l), considerably elevated liver function tests (LD 2496 U/l, ASAT 352 U/l, ALAT 320 U/l, GGT 1850 U/l, AF 464 U/l and Bilirubin 30mmol/l) and elevated albumin corrected calcium (3.02 mmol/l). Contrast-enhanced CT of chest and abdomen demonstrated a tumorous process in the left hilus with mediastinal lymphadenopathy and extensive hepatic and adrenal metastases. Histopathological examination of a biopsy obtained from the liver confirmed small cell lung carcinoma. Despite normal circulatory dynamics following volume resuscitation, lactate levels remained high. Respiratory distress syndrome ensued compelling buffering with sodium bicarbonate. Nevertheless the patient died 3 days after admission. Conclusion: Lactate has evolved into an important biological marker for critical ill patients, lactic acidosis being associated with a poor clinical outcome, in consideration of the fact that the underlying causes are often difficult to manage. The disorder is related to a broad range of possible etiological factors, a thorough knowledge of which may assist clinicians in improving patient management. The classification of Cohen and Woods differentiates between type A en type B lactic acidosis: the first one being related to hypoxia as in shock, the latter being irrespective of the level of oxygenation and associated with diseases like liver or renal insufficiency, malignancy, pharmacological side effects or adverse reactions and genetic defects. In our patient lactic acidosis was caused by metastatic malignancy. The fact that cancer cells predominantly produce energy by high rate of glycolysis with subsequently lactic acid fermentation even in an aerobic situation is described as the Warburg effect. The pathophysiological mechanisms have been gradually unravelled and are applied in PET scanning. Furthermore, pharmacological manipulation of intracellular lactate handling opens novel therapeutic options. Recent studies have demonstrated that dichloracetic acid may induce selective apoptosis by mitochondrial toxicity in brain tumors, opening new perspective in cancer treatment. 142. Type B lactic acidosis as severe complication of lung cancer – review of pathophysiological mechanisms may open new ways of cancer treatment A. Hana, P.L. Rensma, L.V. Beerepoot St. Elizabeth Hospital, Department of Internal Medicine, Hilvarenbeekseweg 60, 5022 GC TILBURG, the Netherlands, e-mail: a.hana@elisabeth.nl 143. No guts no glory: lifelong bevacizumab maintenance therapy, an ethical dilemma in colon cancer? Case report: A 72-year-old man with unremarkable medical history besides nicotine abuse presented with progressive dyspnoea, coughing, abdominal pain and anorexia leading to a weight loss of 7 kg. Before admission he had been given antibiotics because of a presumed pneumonia, without clinical improvement. Physical examination showed an ill and dehydrated patient with Kussmaul breathing, tachycardia and hypotension. Laboratory evaluation revealed respiratory compensated A.C. Ogilvie, J.M. de Koning-Gans ’t Lange Land Hospital, Department of Internal Medicine, Toneellaan 1, 2725 NA ZOETERMEER, the Netherlands, e-mail: ac.ogilvie@xs4all.nl Introduction: Due to the addition of tageted treatments as bevacizumab to classic chemotherapy for metastatic colon 78 Background: After completion of a standard clinical work up in patients with cancer, in less than 5% a ‘truly’ unknown primary cancer (UPC) is diagnosed. The pathologic approach to UPC uses the clinical context, morphology, and, where necessary, additional immunohistochemistry (IHC), electron microscopy and molecular genetic testing like PCR. In female patients the IHC panel includes staining for ER, PR, CK7 and CK20. IHC should also include Her-2 staining, as is stated by standard oncology textbooks. Case: In 2008 a 44-year-old woman came to the emergency department with abdominal pain, fatique, itching, dyspnoea and jaundice. At physical examination the cardinal findings were a WHO-PS of 4 and an enlarged liver, there were no lymph node nor breast abnormalities. Additional studies showed: elevated liver function tests, liver lesions at ultrasound and biopsy of a metastatic adenocarcinoma in the liver. Serum levels of CEA, CA-15.3 and CA-125 were elevated. However, additional studies including CT scanning, Mammography and Sigmoidscopy failed to identify a primary tumor site. She was diagnosed as having a ‘locally advanced cholangiocarcinoma’ - which was confirmed during a second opinion -, and treated with gemcitabine and oxaliplatin. After her first treatment cycle, when additional IHC demonstrated Her-2 positivity, it was decided to add trastuzumab therapy. Her clinical condition improved gradually thereafter, she gained a good clinical remission and became free of symptoms. A year later, during at the initiation of second line paclitaxel with trastuzmab therapy because of progressive disease (liver and the development of skeletal metastasis), she presented with a mass in the right breast and a right axillar palpable lymph node. After resection, it appeared that this was a primary Her-2 negative breast cancer. A second liver biopsy again demonstrated the Her-2 positivity of the metastases. Due to disease progression, third-line vinorelbin and trastuzumab treatment was initated early in 2011. Discussion: This case highlights the clinical importance of IHC staining studies in women suspected of having UPC or a cholangiocarcinoma, as well as the high activity of systemic chemotherapy regimes which inclcude trastuzumab in this group of women with metastatic Her-2 positive adenocarcinoma, even when they appear clinically to have entered the terminal stage of their illness. cancer, response rates, progression-free and even overall survival are improving. However, some times better than anticipated responses leads to untill now an unknown ethical dilemma: how to make good clinical decisions without the guidance of the results evidence-based clinical tests. Case report: In 2006, a 64-year-old man presented with abdominal pain, due to an obstructing sigmoid carcinoma. After a sigmoid resection, additional studies showed supraclavicular, para iliac and mesentery lymph node as well as liver and lungs metastases; of which the supraclavicular site was cytologically proven. This patient was treated with the experimental treatment arm of the Dutch CAIRO-2 study, consisting of capecitabine, oxaliplatin, bevacizumab and cetuximab. Despite severe cutaneous toxicity grade III which lead to the dose-reduction and discontinuation of cetuximab and reduction of the capecitabine dose by 50%, he gained a complete remission after the 6th treatment cycle. Thereafter, in december 2006 he continued with the study maintenance treatment untill disease progression (according to the studyprotocol) consisting of capecitabine and bevacuzimab. Capecitabine caused invalidating grade III toxicity, including Pseudomonas A. infection of the toe nail beds, which regressed after its discontinuation and local antibiotic treatment. Thereafter the only remaining toxicities were: hypertension (treated with enalapril), hypothyriodism (with Thyroxine), the other asymptomatic toxicities (mild hyponatremia and proteinuria) did not needed treatment. The WHO-PS was 0, the patient led a completely normal life. After the seond year of therapy the question of the optimal treatment duration was dicussed yearly with the patient and his family, after gaining expert consultation from the regional comprehensive cancer Centre and advice from the study investigators. Untill now, both patient and his doctor has decided in every occasion to continue bevacizumab untill progression, presumably because they aim at the intuitive 5-year landmark of complete remission duration. Discussion: Given the absence of objective clinical assessment instruments of the possibly persisting colon cancer cells in our patient, such a good treatment outcome results in tough ethical questions. Decisions regarding treatment duration of bevacizumab maintenance can – to our best knowledge – be only based on clinical judgment, while eagerly awaiting further clinical research results. 145. Veno-occlusive disease (VOD) of the liver after oxaliplatin treatment 144. Remember the Her-2 staining in woman with an unknown primary cancer H. Wolzak, M.P.J. Lolkema, A. Baars University Medical Centre Utrecht, Department of Medical Oncology, PO Box 85500, 3508 GA UTRECHT, the Netherlands, e-mail: h.wolzak@gmail.com A.C. Ogilvie, N. Buurma ’t Lange Land Hospital, Department of Internal Medicine, Toneellaan 1, 2725 NA ZOETERMEER, the Netherlands, e-mail: ac.ogilvie@xs4all.nl 79 XI. Introduction: Veno-occlusive disease (VOD) of the liver is a condition in which small veins in the liver are blocked, which is causing liver failure. It is mainly observed in relation to high dose chemotherapy followed by stem cell transplantation, but incidentally occurs after regularly dosed chemotherapy as well. VOD is thought to result from injury to the endothelium of the liver veins causing obstruction of the hepatic sinusoidal and centrolobular venous outflow resulting in congestion of the liver. Clinical signs include jaundice, weight gain caused by fluid retention, hepatomegaly and spontanous hematoma. In the medical literature seven other cases have been described in which patients develop liver failure after oxaliplatin therapy of whom 3 died due to progressive liver failure. In this case report we present a patient with VOD of the liver after oxaliplatin treatment that died from complications of the VOD. Case report: A 30 -year-old male patient with metastatic extragonadal non-seminoma was treated with third line chemotherapy consisting oxaliplatin and gemcitabine. The first two cycles of gemcitibine and oxaliplatin were uneventful, but four days after start of cycle three epistaxis and dyspnea developed. The patient was dyspnoic and had a distended abdomen. On physical examination his liver was enlarged and ascites was present. Initial laboratory results showed a severe thrombocytopenia as well as elevated liver enzymes and hyperbilirubineamia of 205 umol/l. There was no sign of hemolysis. Abdominal ultrasound showed ascites, hepatomegaly and absence of portal vein thrombosis. Viral hepatitis was ruled out. Veno-occlusive disease of the liver was suspected and the patient was admitted to the intensive care unit for thrombolysis with alteplase and i.v. heparin through a femoralis catheter. Platelet transfusion was given. After thirty hours alteplase had to be discontinued because of severe blood loss at the beginning of the central line. During 10 days heparin treatment was continued. Although transaminases slightly improved the bilirubin steadily rose from 40 to 300 umol/l, hepatic encephalopathy developed and need for infusion of trombocytes persisted. The clinical and neurological condition of the patient gradually worsened without further treatment options. A few days later he died. Autopsy was not performed. VOD of the liver after oxalipaltin is a very rare complication and can be fatal. Treatment mainly consists of supportive care including diuretic treatment, paracentesis as clinically indicated, correction of coagulopathy and stopping hepatotoxic medication. VASCULAR MEDICINE RESEARCH 146. Mannose binding lectin as cardiovascular risk factor: a cohort study B. Klop, A. Alipour, A. Westzaan, E. Birnie, G.J.M. van de Geijn, T. Njo, J.W. Janssen, N. van der Meulen, J.W.F. Elte, A.P. Rietveld, M. Castro Cabezas Sint Franciscus Gasthuis, Department of Internal medicine, PO Box 10900, 3004 BA ROTTERDAM, the Netherlands, e-mail: b.klop@sfg.nl Background: Mannose binding lectin (MBL) is linked to atherosclerosis and both high and low levels have been reported as risk factor. We measured MBL as part of our standard cardiovascular risk (CVR) program and followed patients prospectively. Methods: MBL deficiency was established 0.8 mg/l. Cardiovascular disease (CVD) was defined by coronary artery disease (CAD), cerebrovascular disease (CVA) or peripheral vascular disease (PVD) after initial MBL measurement. Results: 478 patients were analyzed. The prevalence of MBL deficiency was 44.4%. The median follow-up was 24.0 months (range 2.0-60.0 months). Age, gender and medical history of CVD were comparable between patients with and without MBL deficiency. Type 2 diabetes mellitus (T2DM) was less prevalent in patients with MBL deficiency (17.1% vs. 25.6%; p=0.016) in contrast to heterozygous familial hypercholesterolemia (FH) (10.4% vs. 3.4%; p=0.002). MBL deficient patients showed an incidence per 1000 person-years of 4.7 for CAD, 4.7 for CVA, 11.9 for PVD and 21.3 for all CVD events combined. In patients with MBL sufficiency, incidence density rates were respectively 16.2 for CAD, 9.0 for CVA, 16.2 for PVD and 41.3 for CVD. The relative risk of MBL deficiency for CAD was 0.29 (95% CI 0.06-1.36), CVA 0.53 (95% CI 0.32-2.72), PVD 0.73 (95% CI 0.38-2.19) and for any CVD event 0.52 (95% CI 0.24-1.12). Conclusion: MBL deficiency was unexpectedly prevalent in our cohort. T2DM was less prevalent in MBL deficient patients, but FH was more prevalent. Overall, our study suggests a trend towards a protective effect of MBL deficiency for atherosclerosis. 147. Variability of diurnal triglyceride levels in men and women B. Klop1, A.J.H.H.M. van Oostrom2, J.P.H. van Wijk3, A. Alipour 1, E. Birnie1, J.W.F. Elte1, J.S. Cohn 4 , M. Castro Cabezas1 1 Sint Franciscus Gasthuis, Department of Internal medicine, PO Box 10900, 3004 BA ROTTERDAM, the Netherlands, 80 e-mail: b.klop@sfg.nl, 2St. Antonius Hospital, NIEUWEGEIN, the Netherlands, 3University Medical Centre Utrecht, UTRECHT, the Netherlands, 4Heart Research Institute, CAMPERDOWN, Australia Aim: We assessed whether cardiovascular risk for these individuals differs from that of hypercholesterolemic FH heterozygotes and unaffected relatives. Materials and methods: Individuals between 18-55 years were recruited within 18 months after genetic screening. Three groups were eligible: i.e. subjects with a molecular diagnosis of FH and LDL-C levels at genetic screening below the 75th percentile (FH-low), subjects with genetic FH and an LDL-C level above the 90th percentile (FH-high) and subjects without FH (No-FH). We measured carotid intima-media thickness (IMT) by ultrasonography. Differences in carotid IMT between the groups were assessed using multivariate linear regression analyses. Results: Mean carotid IMT of 114 subjects in the FH-low group (0.623 mm 95% CI: 0.609 to 0.638 mm) was significantly smaller than that of 162 subjects in the FH-high group (0.664 mm 95%CI: 0.648 to 0.679 mm; p<0.001) and did not significantly differ from the mean carotid IMT in 145 individuals in the No-FH group (0.628 mm 95% CI: 0.613 to 0.642 mm; <i>p</i>=0.67). Conclusion: Our findings suggest that the risk of cardiovascular disease in patients with FH is to a large extent related to LDL-C levels and not to the presence of a mutation per se. Consequently, this study cautiously suggests that individuals with an FH genotype without expression of hypercholesterolemia may not require a pharmaceutical intervention that is as aggressive as the standard for subjects with FH. Objective: Both increased fasting and non-fasting triglycerides (TG) predict cardiovascular events. However, TG vary largely in the fasting state and possibly even more postprandially. Only limited data are available on the intraindividual variability of non-fasting TG. Methods: Capillary triglycerides (cTG) of 272 subjects were measured in a free living situation at six standardized time points (fasting, before lunch, after lunch, before dinner, after dinner and at bedtime) for three days. Coefficients of variation (CV) for cTG were calculated for each time-point. Subjects were divided into tertiles based on their three-day average fasting cTG. Results: The CV for cTG gradually increased during the day with a median ranging from 19.2% (IQR 10.2-33.4) to 25.0% (IQR 13.2-40.4). CVfasting was significantly lower compared to CVafter dinner and CVbedtime (p<0.05), but CVbefore lunch, CVafter lunch and CVbefore dinner did not differ significantly with other time-points including CVfasting. Subjects from the first tertile showed a significantly lower CVfasting and CVbefore lunch compared to subjects from the second and third tertile (p<0.001). Within the second and third tertile there were no significant differences in CV between the different time-points. Average CV was increased with 20.2% in men compared to women for fasting and non-fasting time-points (p<0.05). Conclusions: Men show a higher intra-individual variability of fasting and non-fasting TG than women. Variability of non-fasting TG compared to fasting TG is similar and only slightly higher during the evening. Measuring non-fasting TG instead of fasting TG could be easier for patients and help in cardiovascular risk assessment. 149. Skin autofluorescence, a marker of tissue Advanced Glycation Endproducts accumulation, is increased in patients with carotid artery stenosis and peripheral artery disease D.J. Mulder1, M.J. Noordzij1, E. Loeffen1, B.R. Saleem1, R. Meerwaldt2, H.L. Lutgers1, A.J. Smit1, C.J. Zeebregts1, J.D. Lefrandt1 1 University Medical Centre Groningen, Department of Internal Medicine, PO Box 30001, 9700 RB GRONINGEN, the Netherlands, e-mail: udomulder@gmail.com, 2Medical Spectrum Twente, ENSCHEDE, the Netherlands 148. Assessment of carotid atherosclerosis in normocholesterolemic individuals with proven mutations in the LDL-receptor or apolipoprotein B genes R. Huijgen1 , B.A. Hutten 2 , I. Kindt 3 , M.D. Trip2 , E. de Groot2, J.J.P. Kastelein2, M.N. Vissers2 1 Rode Kruis Hospital, Department of Internal Medicine, Vondellaan 13, 1942 LE BEVERWIJK, the Netherlands, e-mail: r.huijgen@amc.uva.nl, 2 Academic Medical Centre, AMSTERDAM, the Netherlands, 3Stichting Opsporing Erfelijke Hypercholesterolemie, AMSTERDAM, the Netherlands Introduction: Advanced Glycation Endproducts (AGEs) play an important role in development and progression of atherosclerosis. Skin autofluorescence (SAF), a non-invasive marker of tissue AGE accumulation, has been shown to be a strong predictor of incident cardiovascular morbidity and mortality in patients with acute myocardial infarction, diabetes mellitus, and kidney failure, independent of classical risk factors. Aim: We evaluated whether SAF is elevated in patients with carotid artery stenosis (CAS) with and without coexisting peripheral artery occlusive disease (PAOD). Introduction: Genetic cascade screening for heterozygous familial hypercholesterolemia (FH) revealed that fifteen percent of diagnosed individuals do not exhibit elevated low-density lipoprotein cholesterol (LDL-C) levels. 81 Materials and methods: SAF was measured using the AGE Reader in 56 patients with CAS and in 56 age- and sex-matched healthy controls without diabetes, renal dysfunction, or known atherosclerotic disease. Results: SAF was higher in patients with carotid artery stenosis compared with controls: mean 2.81 versus 2.46 arbitrary units (AU) (p=0.002), especially in the younger age group of 50 to 60 years old: mean 2.82 versus 1.94 AU (p<0.001). Patients with CAS and PAOD proved to have an even higher SAF than patients with CAS only: mean 3.28 versus 2.66 AU (p=0.003). Backward linear regression analysis showed that age, smoking, diabetes mellitus, renal function and the presence of PAOD were independent determinants of SAF, whereas CAS alone was not. Conclusion: SAF, a non-invasive marker of tissue AGE accumulation, is increased in patients with CAS and even more in those who also suffer from PAOD. It is associated with established risk factors, including age, smoking, diabetes, and renal insufficiency. The observation that SAF increases with the extent of cardiovascular disease suggests that it may be an indicator of the burden of atherosclerosis and may potentially serve as a risk indicator in patients with cardiovascular disease. Using the Spacelabs oscillometer daytime MAP was 102±8,9 mmHg, i.e. 34,1±3,4% of PP above DBP. MAPPWA was 103,8±11,4 mmHg; 38,8±4,4% above DBP. This difference was significant (p<0,01). Conclusion: MAP displayed by the Watch BP office and the Spacelabs oscillometer, are too imprecise to be used for calibration purposes. We suggest that devices should not display MAP unless their accuracy is tested. 151. Aldosterone-receptor antagonists lead to prolonged blood pressure reduction in uncontrolled hypertension: a retrospective analysis P.M. Jansen1, K. Verdonk1, B.P.M. Imholz2, A.H.J. Danser1, A.H. van den Meiracker1 1 Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: jansen.pm@gmail.com, 2Twee Steden Hospital, WAALWIJK, the Netherlands Introduction: Aldosterone-receptor antagonists (ARAs) have been shown to effectively reduce blood pressure (BP) in patients with uncontrolled hypertension. However, the long-term efficacy of ARAs as add-on treatment in uncontrolled hypertension has not yet been reported. Methods: Data from 123 patients (21 with primary aldosteronism, 102 with essential hypertension) with difficultto-treat hypertension who received an ARA between May 2005 and September 2009 were analyzed retrospectively for their effect on blood pressure (BP) and biochemistry at first follow-up after start with ARA and the last follow-up available. Possible predictors for a better BP response were subsequently tested in a multivariate regression model. Results: Systolic BP decreased by 22±20 and diastolic BP by 9.4±12 mmHg after a median treatment duration of 25 months. In patients that received treatment > 5 years, SBP was 33±20 and DBP 16±13 mmHg lower than at baseline. Changes in BP were not significantly different for PA and EH patients. Serum potassium increased from 4.0 to 4.4 mmol/l (p<0.001) in EH and from 3.4 to 4.3 mmol/l (p<0.001) in PA patients. In addition, serum creatinine showed a significant rise upon ARA treatment (85 to 94 mmol/l (p<0.001) in EH, and 86 to 96 mmol/l (p=0.01) in PA). The total defined daily dose (DDD) of antihypertensive drugs remained unchanged (5 at baseline versus 4.5 at end of follow-up, p=0.459). Multivariate analysis revealed that baseline BP and follow-up duration were positively correlated with BP response. Conclusion: Add-on ARA treatment in difficult-to-treat hypertension results in a profound and sustained BP reduction. 150. Inaccuracy in determining mean arterial pressure with oscillometric blood pressure techniques J. Vos1, H.H. Vincent1, M.C. Verhaar2, W.J.W. Bos1 1 St. Antonius Hospital Nieuwegein, Department of Internal Medicine, Koekoekslaan 1, 3435 CM NIEUWEGEIN, the Netherlands, e-mail: jornvos@hotmail.com, University Medical Centre Utrecht, UTRECHT, the Netherlands Objective: Accurate determination of MAP is important in the calibration of pressure waveforms to calculate central blood pressure. Currently a precise, individualized measurement of mean arterial pressure (MAP) can only be obtained with intra-arterial BP measurements or with applanation tonometry. Objective was to investigate whether easy to use oscillometric devices validated for systolic and diastolic pressure measurements (BHS protocol) give accurate determinations of MAP. Methods: MAP measurements obtained with the WatchBP Office oscillometric (Microlife) monitor (n=102) or with the Spacelabs 90207 oscillometer (n=52) were compared with MAP, assessed by pulse wave analysis (PWA) (SphygmoCor). Results: Average oscillometric MAPMicrolife was 97±12,5 mmHg (mean±SD), i.e. 23,6±9,1% of pulse pressure (PP) above diastolic pressure (DBP). MAPPWA was 106±14,6 mmHg (p<0,01), 37,7±3,9% of PP above DBP. In simultaneous measurements on both arms with Microlife we observed individual left-right differences. 82 XII. VASCULAR MEDICINE CASE REPORTS rare. Furthermore, TA commonly affects young Asian females, rarely occurring after age 40. Our case involves a Caucasian woman, who was diagnosed with TA at age 49. Conclusively, we here described a patient with concurrent occurrence of RA and late onset TA. This association is very rare and remains to be clarified. 152. Late onset Takayasu arteritis diagnosed in a patient with rheumatoid arthritis K.E. Verweij, J.G.J. Jonkman, A.A.M. Zandbergen, A. Dees Ikazia Hospital, Department of Internal Medicine, Montessoriweg 1, 3083 AN ROTTERDAM, the Netherlands, e-mail: evelyneverweij@gmail.com 153. An unusual intrathoracal sharply defined mass B. Tomlow, A. Boersma Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 12, 1815 JD ALKMAAR, the Netherlands, e-mail: 1000702@mca.nl Introduction: Takayasu arteritis (TA) is a rare, chronic vasculitis of unknown etiology that most frequently involves the aorta and its branches. The highest incidence is in Asians. In Europe the incidence is 1-3 per million per year. TA mainly affects young women, with an age at onset usually between 10 and 40 years. Rheumatoid arthritis (RA) is characterized by chronic, systemic inflammation of unknown etiology that primarily involves joints. It can occur at any age with a peak onset between 30 and 55 years. Case report: A 48-year-old Caucasian woman with pain and swelling in left knee and small joints in her hands was diagnosed as having anti-CCP-positive rheumatoid arthritis in October 2009. Treatment was started with prednisolon (15 mg/day) and methotrexate (15 mg/week), which improved her clinical condition. A year later, she presented at the outpatient clinic with fatigue in both upper extremities while in use. She did not experience weight loss or low-grade fever. Upon physical examination, a blood pressure difference between the left and the right arm was noted, respectively 109/71 mmHg and 93/71 mmHg. Furthermore, a murmur was noticed over the left carotid artery. Pulsations of both radial arteries were reduced. Laboratory tests were unremarkable, except for a slight leukocytosis (15 x 109/l). Subsequent MRA showed occlusion of the right truncus brachiocephalicus at its origin from the aortic arch and a slight irregularity of the aortic arch. There was also stenosis of the left subclavian artery. PET-CT demonstrated increased FDG uptake along both brachial arteries, suggestive of active vasculitis. According to the ACR classification criteria the patient was diagnosed with TA. The treatment she already used for RA was continued. Within two months, the fatigue in both arms improved, but the reduced pulsations and blood pressure difference remained. Conclusion: TA is a rare disease of which the pathogenesis remains to be clarified. It has been suggested that the vasculitis may deteriorate via an autoimmune mechanism. Several studies have reported an association between TA and systemic lupus erythematosus (SLE) or systemic sclerosis, but the concurrent presence of TA and RA is Introduction: If a sharply defined mass is found intrathoracal a CT thorax-abdomen should be performed to differentiate between the diagnosis of an infection, an empyema, a vascular problem, malignancy (mesotheloma, pleuritis carcinomatos, lymphoma), tuberculosis or a haemathorax. In case of a mycotic aneurysma the in-hospital mortality rate lies around 35%. A possible explanation for this can be that operations are usually performed on an emergency basis while patients are in a state of sepsis or shock and at hightened risk of an aneurysmal rupture. Case report: In July, 2010 a 79-year-old woman was presented to our emergency department with fever, fatigue and pain on the left side of the abdomen. Her medical history revealed diabetes mellitus type 2, severe vascular disease, and a smoking history of 30 pack years. Vital signs revealed a body temperature of 38.5 °C, blood pressure of 188/117 mmHg, heart rate of 95 /min and a respiratory rate of 18/min with a SO2 of 98% without supplemental oxygen. Physical examination showed symmetrical normal breathing with minor increase in vocal fremitus. The left area of the abdomen showed tenderness, painful at palpation, without muscular defence. Laboratory results indicated an elevated C-reactive protein level of 279 mg/l (normal values: 0 to 10 mg/l), White blood cell count of 12.7. * 109/l (normal values: 3.5 to10.0 * 109/l) and a hemoglobin level of 5.5 mmol/l (normal values: 7.5-9.5 mmol/l) with a mean corpuscular volume of 86.0 fl (normal values: 80 to 100 fl). The chest x-ray showed a sharply defined intrathoracal mass most prominent on the lateral view. A thoracentesis was performed which showed a green-brown gelatinous fluid with a pH of 7.4, LDH of 1987 U/l, total protein of 39 g/l and a hemoglobin level of 0.4 mmol/l. A CT thorax-abdomen which showed a giant aneurysmata - 13 cm diameter – in the intra-thoracal (TAA) as well as in the intra-abdominal aortic arch (AAA), most likely a mycotic aneurysma which is a localized, irreversible arterial dilatation caused by an infectious destruction of the vessel wall. This is a serious condition leading to significant morbidity and mortality rate which 83 and can trigger life-threatening ventricular arrhythmias. A hypothesis is that calcium is also increased in the pulmonary smooth muscle cells and can cause pulmonary arterial vasoconstriction and in this manner genetic susceptibility for developing pulmonary arterial hypertension in this patient. So a RYR-2 mutation is possibly a new genetic risk factor. The risk for developing pulmonary arterial hypertension is then further increased when a patient uses amphetamines or cocaine. Conclusion: Chronic use of amphetamines, cocaine and appetite suppressants can cause severe pulmonary hypertension. Genetic susceptibility can play an important role. can develop when a new aneurysm is produced by infection of the arterial wall or when a pre-existing aneurysm becomes infected. In spite of its name, which refers to the appearance, like ‘fresh fungus vegetations’, the majority of mycotic aneurysms are caused by bacteria. 154. Pulmonary arterial hypertension caused by chronic use of amphetamines and cocaine M. Ezzahti, N. Masalha Amphia Hospital, Department of Internal Medicine, Molengracht 21, 4818 CK BREDA, the Netherlands, e-mail: ezzahti00@hotmail.com 155. Acute myocardial infarction in a young woman: how a critical appraisal of the blood count led to a treatable cause Case: A 28-year-old woman diagnosed with catecholaminergic polymorphic ventricular tachycardia (CPVT) complained of progressive exertional dyspneu and fatigue over two years. She had no chest pain and there was no syncopal episode. The patient had used for more than 13 years amphetamines and cocaine. She had also used for 3 months pseudoephedrine and caffeine for appetite suppression. On physical examination the blood pressure was 109/69 mmHg, her heart rate was 84 beats/min and the oxygen saturation was 95% without use of oxygen. Auscultation of the heart showed a split second heart sound. Further physical examination was unremarkable. Electrocardiography revealed signs of right ventricular hypertrophy and a chest radiograph showed large central pulmonary arteries. Echocardiography showed dilatation of the right ventricle and right atrium, an estimated pulmonary pressure of 105 mmHg, tricuspid regurgitation grade 2 and a normal left and right ventricular function. Right cardiac catheterization revealed findings consistent with pulmonary hypertension: pulmonary arterial systolic pressure of 101 mmHg, mean right atrial pressure of 8 mmHg and a cardiac output of 4,1 liter/ min. Pulmonary function testing was normal. Ventilation perfusion scanning and a CT angiogram of the chest revealed also no abnormalities. Lab results showed normal liver function tests, negative ANA and ANCA and negative HIV serology. The cause of pulmonary hypertension in this patient was the chronic use of amphetamines, cocaine and possibly appetite suppressants. Other causes were excluded. The patient was treated with ambrisentan, an endothelin receptor antagonist. Discussion: Amphetamines may lead to pulmonary arterial hypertension due to the release of serotonin, which causes pulmonary vasoconstriction and the proliferation of smooth muscle cells. Cocaine can cause endothelial dysfunction and also proliferation of pulmonary smooth muscle cells. The patient has a p.Val2178IIe mutation in the RYR2-gen, which causes CPVT. The RYR2 mutation increases calcium release in the muscle cells of the heart D.J. Mulder, E.J. Houwerzijl, J.D. Lefrandt, M.M.J.B.G. Beckers, A.J. Smit, K. Meijer University Medical Centre Groningen, Department of Internal Medicine, PO Box 30001, 9700 RB GRONINGEN, the Netherlands, e-mail: udomulder@gmail.com Introduction: Although acute myocardial infarction (AMI) mainly occurs in elderly patients, young individuals can also be affected. In young patients, most cases are still explained by classical risk factors. However, in the absence of risk factors, exceptional causes should never be overlooked. Case report: At the age of 34, a previously healthy woman was admitted to our hospital in cardiac arrest. Angiography revealed a proximal 90% occlusion of the left main coronary artery for which a drug eluting stent was placed. The remaining coronary arteries did not show luminal stenosis or apparent dissection, without signs of atherosclerosis on CT-scan. Patient was treated according to protocol after which she rapidly recovered. The usual secondary prevention, including acetylsalicylic acid, was started. Classical risk factors were absent, she had never smoked, was athletic and not overweight, had no family history of premature atherosclerosis, no hypertension, no diabetes, and a normal lipid profile. Two months earlier, she had had a short period of chest pain on exertion. In retrospection, her hemoglobin and platelet levels appeared to be relative high for a young woman. At the age of 27, her haemoglobin was 9.7 (7.5-9.9) mmol/l with platelets of 377 (150-350) x 109 IU/l and at admission haemoglobin was 9.9 mmol/l, platelets were 394 x 109 IU/l, and leukocytes were 12.7 x 109 IU/l, with maximum values of 10.3 mmol/l, 467 and 18.6 x 109 IU/l. Four years later, during regular follow-up, platelets had increased to 575 109 IU/l. We considered the possibility of an underlying myeloproliferative disorder (MPD), and a JAK2 V617F mutation was detected. Bone marrow aspiration demonstrated a low iron depot and panmyelosis, 84 matching the diagnosis MPD, without signs of primary myelofibrosis of chronic myeloid leukemia. Based on the 2008 WHO criteria, i.e. Hb > 10.2 for women and JAK2 V617F mutation, polycythaemia vera was the most appropriate diagnosis. Conclusion: Our patient’s fulminant presentation of AMI was almost certainly a thrombotic event following a previously unrecognized MPD, already present many years earlier. These are clonal marrow neoplasms that are associated with arterial or venous thromboses, with AMI being a rare complication. Untreated recurrence rates of thrombotic events may be up to 60%. Cytoreductive therapy is very effective in protecting against recurrent events, particularly after AMI. Therefore, in young patients with arterial thrombosis, blood counts that are mildly but consistently elevated should raise suspicion of MPD. This opportunity to decrease the risk of recurrence should not be missed. dehydrogenase (LDH, 971 U/l). A contrast-computed tomography showed a left renal infarction. Cocaine metabolites were found in a later performed drug screening. It is generally accepted that cocaine has potent vasoconstrictive effects on vascular smooth muscle. The release of vasoactive substances is influenced by cocaine, for example the inhibition of vasodilatative nitric oxide. It also blocks the re-uptake of catecholamines in sympathetically innervated tissues, thereby leading to sympathetic discharge. Extreme vasoconstriction causes damage to the endothelial surface, resulting in platelet activation and possibly formation of thrombi. Beside the cardiac effects, renal injury is the most described side effect of cocaine use. This involves renal failure and infarction, mostly due to severe vasoconstriction. Less often mentioned are gastrointestinal complications, despite a mortality rate of almost 30%. Blocking the re-uptake of norepinephrine may lead to mesenteric ischemia and focal tissue ischemia, which may lead to perforation. Conclusion: This case report shows renal and gastrointestinal side effects of cocaine use. It is important not to underestimate these effects, as mortality rate can be high. 156. Unusual complications of cocaine J.M. Hillen, F.H. Bosch Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6800 TA ARNHEM, the Netherlands, e-mail: judithhillen@gmail.com 157. A life-threatening presentation of Wegener’s granulomatosis Introduction: The cardiac effects of cocaine are well known. We report on two cases in which unusual effects of cocaine are shown, induced by cocaine related vasoconstriction. Case report: The first patient, a 45-year-old male, presented at the emergency department with abdominal pain, vomiting and absence of defecation since 5 days. Medical history revealed cocaine and marihuana abuse. Laboratory results showed a serum creatinine of 542 mmol/l with a blood urea nitrogen of 19.8 mmol/l. Liver enzymes were slightly elevated and cocaine metabolites were found in the urine. ECG showed negative T’s in II, III, V4-V6 but cardiac enzymes were not elevated. Two days after admittance patient detoriated and developed acute gastrointestinal complaints. Laparotomy showed ischemia of the mesentery and necrosis of the sigmoid. He was admitted to the ICU, but died in five days because of an abdominal sepsis with multi organ failure. Autopsy showed recent myocardial infarction, as well as liver infarction and extensive ischemia of the small intestine, colon and omentum. In the left kidney, multiple older infarcts were seen, all matching cocaine use. Our second patient, a 36-year-old male, presented with sudden pain in the left lower abdomen, characterized as sharp and radiating to his left lower back. Physical examination revealed a tenderness with percussion on the left costovertebral angle. Laboratory analysis revealed no abnormalities, except a remarkable increased lactate J.A.J. Douma, F. Stam Medical Centre Alkmaar, Department of Internal Medicine, Wilhelminalaan 12, 1815 JD ALKMAAR, the Netherlands, e-mail: joeridouma@gmail.com Case report: A 64-year-old man presented at our emergency department with symptoms of malaise. His complaints consisted of loss of appetite, sensation of fever, night sweats, painful legs and rhinorrhea since two weeks. In addition, he had crusts in his nose for two years, with periods of nose bleeding. The medical history included schizophrenia, with three times a psychosis, and ankylosing spondylitis, for which he received treatment with etoricoxib. Physical examination showed a body temperature of 38.1 °C, crustae in the nose and an oral fetid odour. Laboratory investigation revealed an elevated C-reactive protein (340 mg/l), thrombocytosis (1028 x 109/l), leukocytosis (20.1 x 109/l), and slight liver enzymes disturbances. In addition, marked renal insufficiency (serum creatinine 591 mmol/l) with proteinuria (1.1 g/l) and dysmorphic erythrocyturia was demonstrated. A chest X-ray showed a pulmonary infiltrate, whereas computed tomography revealed mucosal swelling of the maxillary and ethomidic sinuses, with partial destruction of the nasal septum. A few days after presentation, the patient developed acute pain on the left side of the abdomen with a computed tomography showing subtotal splenic infarction. 85 Aim: Determine complaints in correlation with the use of acid suppressive therapy ten years after diagnosis. Materials and methods: 672 patients with oesophagitis between 1998 and 2000 were reviewed to identify patients suitable for this investigation. A total of 262 patients were excluded because of pre-defined exclusion criteria (ie. chronic cardiopulmonary disease, or treatment of cancer), leaving a study population of 410 subjects. Patients received a questionnaire regarding their use of acid suppressive therapy, dosage, compliance and patient satisfaction. In addition, use of ™ or gen was assessed. Presence of reflux complaints was assessed via a validated questionnaire, and a symptom score was calculated using a 5-point Likert scale. Results: A total of 208 patients returned the questionnaire (51%), 161 (78%) of them used acid suppressive therapy. Of the patients still on acid suppressive therapy 72% (116 patients, group 1) had reflux complaints, while the remaining 45 patients (28%, group 2) were in complete clinical remission. There was no difference in gender, age or severity of the initially diagnosed reflux oesophagitis between both groups. An equal number of patients in both groups received the prescription from their general practitioner. Patients in group 1 were significantly less compliant and satisfied compared to patients from group 2, 73% vs. 96% and 83% vs. 100% (p<0,001) respectively. An equal number of patients in both groups used ™ or gen (p=ns). Presence of reflux complaints as well as symptom score (although rather low) showed no difference between users of ™ or gen. The majority of patients always uses the prescribed dosage. Conclusion: It is concluded that more than 10 years after the diagnosis of reflux oesophagitis 22% of patients stopped using acid suppressive therapy. From the patients still on medication only a minority (28%) is in complete clinical remission associated with significantly higher patient satisfaction and compliance to therapy as compared to their symptomatic counterparts. There appears to be no difference in effect and usage of ™ versus gen preparations. Another few days later the patient became dyspnoeic, due to congestive heart failure as result of a non-ST-elevation myocardial infarct. At that time, an obvious purple-red discolouration of some parts of the fingers was noticed. Cultures of blood and urine were negative. Given the wide range of signs and symptoms in combination with the participation of the upper airways a systemic disease, like Wegener’s granulomatosis, was suspected. Immunological investigation, showed a strongly positive C-ANCA titre, as was the case for antiproteinase3-ANCA. This confirmed the diagnosis Wegener’s granulomatosis. Pathological investigation of tissue biopsy of the nose displayed only necrosis, without granulomas. Electromyography of the legs showed a mixed neuropathy with degradation of both the motoric and sensory nerves. After starting intravenous treatment with high doses of prednisolone and cyclophosphamide the condition of the patient improved. However, the patient needed to undergo temporary haemodialysis because of renal failure and some necrotic fingers needed to be amputated. Eight weeks after admittances the patient could be discharged in good general condition. Conclusion: Wegener’s granulomatosis is a potential lifethreatening disease, that can affect multiple organ systems. Our case represents the dramatic impact, when the disease progresses without the correct diagnosis. When a patient presents with signs and symptoms of multiple organs, especially when combined with upper airway symptoms, Wegener’s granulomatosis should always be considered. XIII. GASTRO-ENTEROLOGY RESEARCH 158. Use of acid suppressive drugs, trademark versus generic, more than 10 years after the endoscopical diagnosis of reflux oesophagitis 159. Complaints in patients with reflux oesophagitis more than 10 years after the diagnosis G.M.H.E. Dackus, S.M.L.A. Loffeld, R.J.L.F. Loffeld Zaans Medical Centre, Department of Internal Medicine, PO Box 210, 1500 EE ZAANDAM, the Netherlands, e-mail: loffeld.r@zaansmc.nl S.M.L.A. Loffeld, G.M.H.E. Dackus, R.J.L.F. Loffeld Zaans Medical Centre, PO Box 210, 1500 EE ZAANDAM, the Netherlands, e-mail: loffeld.r@zaansmc.nl Introduction: Reflux oesophagitis needs maintenance therapy with acid suppressive drugs. Since generic preparations (gen) became available, clinicians made the observation that these drugs are probably less effective. Most studies on the efficacy of acid suppressive therapy report on short term follow-up after treatment with trademark (™). Little data exist on the long term follow-up of patients with reflux oesophagitis. Data on comparison between these ™ and gen are not available. Introduction: Treatment of reflux oesophagitis with acid suppressive therapy is effective. Data on long term follow-up are lacking. Aim: A study was done in patients in order to assess complaints more than 10 years after the endoscopic diagnosis. Material and methods: All patients diagnosed in the years 1998, 1999 and 2000 were studied. Exclusion criteria were chronic cardio-pulmonary disease, active treatment for any 86 collected. The cause and localisation of perforation was determined. The cause was therapeutic (polypectomy or coagulation), barotraumatic (the inflated air) or mechanical (direct trauma). Results: In the period of 1992-2010 22376 consecutive procedures were done. Perforation of the colon occurred in 29 patients (0.12%) (10 men, 19 women, mean age 74.9 years, SD 10.3, median 76, range 33-89). In 15 cases (52%) the cause of perforation was mechanical, in 9 (31%) barotraumatic (cecal blow-out), and in four cases (13%) it was due to coagulation or polypectomy. In one patient data was not available. Two sites were prone to perforation: the sigmoid and the cecum. Cecal blow-out occurred significantly more often as the result of barotrauma, while perforation of the sigmoid was more often the result of direct mechanical trauma. This occurred more often in cases of diverticuli in the sigmoid. Three perforations in patients with polyps were not the direct result of a polypectomy or biopsy, two patients also had diverticuli and one patient had a stenotic anastomosis. Diverticuli are the most common diagnosis in relation to mechanical trauma. Two patients had a mechanical perforation of an otherwise normal sigmoid. Both patients used high dosages of corticosteroids during a longer period of time. One perforation of the sigmoid occurred during the dilatation of a stenotic anastomosis, because the guide wire perforated a diverticulum 20 cm proximal to the stenosis. One patient with overt bleeding due to active colitis was treated with coagulation and had a sigmoid perforation one day later. Successful cecal intubation was achieved in 14 out of these 29 patients with perforations (48%). In case of successful cecal intubation the perforation was located in the sigmoid in 7 cases, in the transverse colon in one case and in the cecum in 4 cases. This was 10, 0, and 6 respectively in case the cecum was not reached during the procedure. The majority of perforations were diagnosed within the first 24 hours. Conclusion: It is concluded that the risk of perforation is rather low. Mechanical trauma in cases of diverticuli and barotrauma due to inflated air are very important causes. Patients with a higher risk are those with diverticuli in the sigmoid. cancer, immigrants, Alzheimers, mental disability, and psychiatric illnesses. All patients received a questionnaire by mail. The questionnaire comprised four different, validated lists of questions. A general questionnaire consisted of 20 questions on reflux complaints. Severity as well as frequency was scored on a five and six point Likert scale respectively (scores ranged from 0-40 and 0-60). The GerdQ list, a symptom activity index (SAI), and the gastrointestinal symptom rating scale (GSRS) were used as well. Results: In a period of three years 672 patients were diagnosed with reflux oesophagitis. After exclusions the study population comprised of 410 patients. Of these 208 questionnaires (51%) were available for evaluation. Complaints were reported by 130 patients (63%). The majority of these, 115 (88%), use acid suppressive therapy. Only 78 patients were in clinical remission, with or without therapy. The respondents with complaints were divided into two groups. Group 1: all patients with reflux complaints and using acid suppressive therapy. Group 2: all patients with complaints without medication. Patients in group 1 were significantly older at time of the endoscopic diagnosis compared with patients of group 2. Patients in group 1 had significantly more often a hiatal hernia (p<0.001). There was no difference in overall symptom or frequency score per patient between both groups, mean 5.97 versus 6.8 and 13.4 versus 13.8 respectively. However, heartburn, nausea, acid regurgitation, epigastric pain, dysphagia, and nocturnal complaints showed a significant higher prevalence in patients of group 2. Scores for specific complaints were significantly lower in group 2. There was no difference between the GERD-Q, SAI and GSRS. Conclusion: Despite effective therapy only a 37% of patients is in complete remission. However, the symptom score per patient is rather low. Patients without medication have more often reflux complaints but lower severity scores, being a possible reason for not taking medication. Hence it is to be expected that these patients regarded their complaints very mild not necessitating therapy. Patients who still had complaints and used medication had significantly more often a hiatal hernia. 160. Perforations after colonoscopy. Incidence and causes 161. Clinical and microbiological evaluation of liver abscesses: 15-year single-centre experience in the Netherlands R.J.L.F. Loffeld, A. Engel, P.E.P. Dekkers Zaans Medical Centre, Department of Internal Medicine, PO Box 210, 1500 EE ZAANDAM, the Netherlands, e-mail: loffeld.r@zaansmc.nl I.L. Holster, A.C. de Vries, P. de Man, A.J.P. van Tilburg Sint Franciscus Gasthuis, Department of Gastroenterology and Hepatology, Kleiweg 500, 3045 PM ROTTERDAM, the Netherlands, e-mail: i.holster@erasmusmc.nl Introduction: The causes of perforations after colonoscopy are largely unknown. Aim: Study the causes leading to perforation. Materials and methods: Data on sex, age, endoscopic diagnosis, therapeutic actions, and cecal intubation were Background: Liver abscesses are diagnosed infrequently in the Western world. Escherichia coli, Streptococcus and 87 Case: A 64-year-old woman was admitted to our department because of a 1-day history of diffuse abdominal pain. She had no other complaints. The medical history comprised limited cutaneous systemic sclerosis with sclerodactyly, digital ulcers, calcinosis cutis and Raynaud phenomenon, and GERD. At physical examination, the abdomen was diffusely tender. Laboratory examination showed a leukocyte count of 16,0 x 109/l and C-reactive protein of 89 mg/l. Shortly after admission the patient developed diarrhea, abdominal distension and high-pitched borborygmi at auscultation. Contrast enhanced abdominal CT revealed distention of the small intestine and diffuse thickening of the colonic wall with an intact splanchnic circulation. At sigmoidoscopy, there was a moderate to severe ischemic colitis of the sigmoid and descending colon. Repeated faecal cultures were negative for SSYC and Clostridium difficile. The patient was treated with a nasogastric tube, TPN and analgesics. One week after admission, abdominal pain declined and auscultation revealed normalized bowel sounds, but diarrhea persisted, with bowel movements up to ten times per 24 hours. Sigmoidoscopy was repeated and showed an unchanged endoscopic picture suggestive for severe ischemic colitis. Two days later, the patient developed an acute abdomen. Abdominal CT was repeated and showed diffuse intestinal distention, pneumatosis coli of the sigmoid and descending colon and free intra-abdominal air. An emergency subtotal colectomy was indicated. However, the patient refused surgical intervention and died two days later. Autopsy revealed a perforation of 3 centimeters at the splenic flexure. Discussion: Systemic sclerosis (SSc) is a chronic systemic disorder of unknown etiology characterized by thickened, hard skin (scleroderma) and distinctive involvement of multiple internal organs, most notably the lungs, heart, kidneys and gastrointestinal tract. The pathologic hallmark of SSc is diffuse obliterative vasculopathy of small arteries and arterioles and fibrosis in the skin and internal organs. Nearly 90 procent of patients with SSc have some degree of gastrointestinal (GI) involvement. Because of neuropathy, smooth muscle atrophy and fibrosis, there is reduced peristalsis throughout the gastrointestinal tract. GERD and gastroparesis are frequently reported symptoms. Sever GI problems, including bacterial overgrowth, malabsorption and intestinal pseudo-obstruction, are much less common, affecting less than 10 procent of patients. Pneumatosis coli, that is the presence of air in the bowel wall, is a very rare complication and a poor prognostic sign. Although successful conservative treatment has been described, the risk of colonic infarction and spontaneous perforation with concomitant mortality is high, as seen in our patient. Staphylococcus species are the most recovered microorganisms in Europe, while Klebsiella pneumoniae is predominant in puss cultures of pyogenic liver abscesses in Southeast Asia and North America. In this report an overview is provided on clinical presentation, etiology and recovered microorganisms of liver abscesses in a general hospital in the Netherlands. Methods: All patients with a microbiologically proven liver abscess during the period from December 1994 until December 2009 were included. Clinical, laboratory, radiological, and microbiological data were systemically collected and analyzed. Results: A total of 35 patients (median age 69.5year; 63% male) with an aspirated liver abscess (32 pyogenic (91%), 3 amoebic (9%)) were included. Frequently reported symptoms in patients with pyogenic liver abscess at presentation were fever or chills (72%) and abdominal pain (66%). Twenty-one abscesses (60%) were solitary and 13 patients (40%) had multiple abscesses. The majority of abscesses was right sided (43%), followed by multilocular (37%) and left sided (11%). The median size of the largest abscess per patient was 7 cm (IQR 6-9 cm). The most common etiologies of the abscesses were biliary (31%) and diverticulitis (17%), while in 26% of cases etiology remained unknown. Streptococcus species and Escherichia coli were most frequently cultured, both in pure cultures (resp. in 22% and 16% of patients), as well as in mixed cultures (in 32% of patients). Resistance of microorganisms to amoxicillin clavunalate was found in cultures of four patients (12%) and to combination treatment of cefuroxime/metronidazole in three patients (9%) (two of them were extensively pretreated with antibiotics). Conclusion: Liver abscesses show large heterogeneity in clinical presentation and microbiological culture results. Streptococcus species and Escherichia coli are the most common causative microorganisms in the setting of general Dutch hospitals. In addition to drainage of the abscess, empiric antibiotic treatment with cefuroxime/metronidazole seems an appropriate strategy, while resistance occurs infrequently. These data support current Dutch antibiotic guidelines for initial therapy of liver abscesses. XIV. GASTRO-ENTEROLOGY CASE REPORTS 162. Systemic sclerosis complicated by pneumatosis coli and intestinal perforation M.C. van Veen, S.D. Kuiken Sint Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: merkvanveen@hotmail.com 88 163. Amiodarone-induced hepatotoxicity eight years after initation of therapy Conclusion: Late hepatotoxity is a rare complication of chronic amiodarone therapy. Regular liver enzyme function testing remains warranted, even after years of treatment. J.G.P. Reijnders, S. Indhirajanti, A. Dees Ikazia Hospital Rotterdam, Department of Internal Medicine, Montessoriweg 1, 3083 AN ROTTERDAM, the Netherlands, e-mail: jgp.reijnders@gmail.com 164. Pulmonary embolism in a patient with inflammatory bowel disease (IBD), receiving adequate thrombosis prophylaxis Introduction: Hepatotoxicity is a relatively uncommon side effect of amiodarone chlorhydrate, and, although asymptomatic elevation of aminotransferases is reported in up to a fourth of all patients, symptomatic hepatic dysfunction occurs in less than 1% of the patients on chronic amiodarone therapy. Case: A 77-year-old man was referred for analysis of slowly, progressive abnormal liver tests, which had started 15 months before. Medical history included mitral valve plasty, and paroxysmal atrial fibrillation, which was managed with initiation of fenprocoumaron and oral amiodaron 200mg eight years before presentation. The latter therapy had been complicated by type 2 painless thyroiditis and persistent hypothyreoidy. There were only complaints of long-term dyspepsia. He had no history of jaundice, dark urine of pale stools, and denied alcohol abuse or using any herbal or over-the-counter drugs. He was a lean man without a family history of liver disease. He had not received any blood transfusions. On physical examination there were no signs of chronic liver disease. Liver chemistries were abnormal: AST 171 U/l, ALT 191 U/l, alkaline phosphatase 115 U/l, GGT 259 U/l, bilirubin 9 mg/l, albumin 37 g/l, INR 3.7. Hepatitis B and C serologies were negative, as were auto-immune serologies. Serum Ig levels, ferritin, ceruloplasmin, and a-1 antitrypsin were normal. Computed tomography of the liver demonstrated no signs of liver cirrhosis or portal hypertension, and no focal lesions, yet revealed a bright texture of the liver, suggestive of diffuse liver fatty infiltration. Drug-induced hepatotoxicity with amiodarone was considered as a possibility in view of the temporal association of development of abnormal liver test values after initiation of amiodarone, and the exclusion of other causes of liver disease. Amiodarone was stopped, and resulted in complete normalization of liver chemistries six months after discontinuation of amiodarone. Discussion: Amiodarone is a strong lipophilic compound, which accumulates in tissue with high adipose content, such as the liver. The latent period before aminotransferase elevations develop, may vary from a few weeks to several years, and probably reflects the time needed for drug accumulation in the hepatocytes. Vice versa, because of its long half life and huge volume of distribution, amiodarone can persist in the liver for long periods after the drug is stopped, and liver damage can thus progress despite drug discontinuation. L.H.A. Bonnie, A.J.G.H. Bindels, A.N. Roos Catharina Hospital Eindhoven, Department of Intensive Care Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: linda.bonnie@CZE.nl Introduction: IBD patients are at increased risk for a thrombo-embolic event, which should be prevented by thrombosis prophylaxis. We describe an IBD patient dying from a pulmonary embolism, despite adequate prophylaxis. Case report: A 68-year-old male was presented because of fever, malaise and confusion. He had a medical history of diabetes mellitus type 2, obesity and IBD, treated with prednisone and methotrexate. Physical examination showed a confused, dyspneic man with an oxygen saturation of 90% without oxygen. Laboratory findings were normal, except for signs of inflammation (leukocytes 8.0 * 109/l (4,0-10,0 * 109/l), CRP 110mg/l (< 6 mg/l)) and an elevated LDH (370 U/l (150-300U/l)). Blood gas analysis showed a respiratory acidosis with hypoxemia. A chest-X-ray showed bilateral infiltrates. CT-angiography revealed diffuse alveolar infiltrates without pulmonary embolism. Patient was admitted to the ward; co-trimoxazole was started under suspicion of a pneumocystis cariniipneumonia. The diagnosis was confirmed by a lavage and cultures. Three days later, patient’s condition deteriorated; he was progressively confused, had low blood pressure, and was respiratory insufficient. He was admitted to the ICU for respiratory and hemodynamic support, antibiotics were continued and standard ICU-care including prophylactic dalteparine was started. During the following days, patient slightly improved; inotropes were reduced and he was weaned from the ventilator. Eleven days after admission, CRP level and lactate concentration were increasing, without a clear clinical explanation. The next day, the clinical situation deteriorated progressively; patient had a high fever (40.7 °C) and was hypotensive with poor peripheral circulation. Fluid challenges were given and inotropes restarted. Unfortunately, he remained hypotensive and bradycard, and after all resuscitation had to be started. Despite prolonged resuscitation, patient passed away. 89 treatment for recurrent cystitis. Discontinuation of the drug caused an immediate fall in liver enzyme levels. This major improvement after discontinuation of the drug underlines the role of nitrofurantoine in the pathogenesis of autoimmune hepatitis in this patient. We therefore decided to refrain from corticosteroid treatment, taking into account the posible side effects of long term immunosuppressive treatment. Our patient showed normalization of liver values within three months after withdrawal of nitrofurantoin. Discussion: Nitrofurantoin is a commonly used antibiotic in the treatment and prevention of urinary tract infections. Although it is generally considered as a safe drug, hepatotoxicity occurs in 0.0003% of cases during long term use. Different patterns of hepatotoxicity have been described, including autoimmune hepatitis. It is postulated that drug metabolites bind to cellular proteins which are susequently recognized as neo antigens by the immune system. Although corticosteroids are often used, withdrawal from the drug alone can reverse the hepatic damage. Conclusion: Nitrofurantoin induced autoimmune hepatitis may resolve without immunosuppressive therapy. The sudden clinical deterioration without overt explanation gave reason to an autopsy; a massive pulmonary embolism as the cause of death was found. Discussion: Presence of IBD is associated with an increased incidence of thrombo-embolic events, compared to healthy subjects. The exact mechanism remains unknown, but there is evidence of an altered haemostatic situation. Also, it seems that tissue damage may lead to simultaneous activation of both coagulation and inflammation. It is believed that factor Xa plays an important role in this process. Inhibiting factor Xa may thus both reduce the inflammatory response and the risk of thrombosis. Literature is not informative about the incidence of thrombo-embolic events in IBD patients using prophylaxis, such as factor Xa-inhibitors. Therefore, it is difficult to identify the optimal dose of thrombosis prophylaxis in patients with IBD. 165. Autoimmune hepatitis triggered by nitrofurantoin; recovery without immunosuppression E.C. Gootjes, J.J.M. van Meyel, J. Veenstra St Lucas Andreas Hospital, Department of Internal Medicine and Gastroenterology, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: e.gootjes@slaz.nl 166. A clinical manifestation of the Hepatopulmonary Syndrome Introduction: Autoimmune hepatitis is diagnosed based on the presence of auto antibodies, total IgG levels and characteristic histopathological changes in the absence of viral hepatitis. Immunosuppression is the first line of therapy. Rarely, a toxic agent can be identified to be causative. We present a case of autoimmune hepatitis, induced by long term use of nitrofurantoin. Case report: A 71-year-old woman was referred with complaints of malaise, a raised erythrocyte sedimentation rate (80 mm in first hour) and mildly elevated AST (82 u/l) and ALT (90 u/l). Previously she was diagnosed with arthrosis, Raynaud syndrome and Sjögrens syndrome and she was recently treated for cystitis. Besides eye drops, she used esomeprazole and losartan/hydrochlorothiazide. She denied the use of alcohol. On physical examination there were no diagnostic clues. Elaborate laboratory testing did not show evidence of viral hepatitis or storage disease. Autoimmune serology showed a positive ANA (previously negative), but anti SMA, anti LKM and anti SLA were negative. Levels of total IgG were elevated (18 g/l). Imaging of the liver showed no abnormalities of the liver parenchyma. As the liver enzyme levels further increased (AST 252 u/l, ALT 274 u/l), a liver biopsy was performed. The biopsy showed interface activity and confluent necrosis compatible with autoimmune hepatitis. Meanwhile, repeated careful questioning of the patient revealed long term use of nitrofurantoin as prophylactic S.M.C.H. Langenberg, D.M. Oude Hergelink, M.J. Kerbert-Dreteler Medical Spectrum Twente, Department of Internal Medicine, Ariënsplein 1, 7511 JX ENSCHEDE, the Netherlands, e-mail: s.langenberg@mst.nl Introduction: There are no specific signs or symptoms for the Hepatopulmonary Syndrome (HPS), although abnormal oxygenation with dyspnea at rest and on exertion, digital clubbing, spider naevi and cyanosis are strongly suggestive for HPS. Diagnostic criteria for HPS are liver disease with portal hypertension and/or cirrhosis, pulmonary vascular dilatation (diameter 15-100 mm; normal range 8-15 mm) and an oxygenation defect. Studies show that, when diagnosed with HPS, the median survival is 24 months and the 5-years survival rate is 23%. Liver transplantation is the only treatment and shows a 5-years survival rate of 76%. Case report: a 70-years-old female with alcohol induced liver cirrhosis was admitted because of hematemesis due to esophageal varices grade 2. She also suffered from dyspnea, especially in an upright position and on exertion. Arterial blood gas analysis, breathing ambient air, showed a severe oxygenation defect with a partial pressure of oxygen of 56 mmHg (7.3 kPa) and an A-a gradient of 57 mmHg (7.4 kPa). X-ray computed tomography showed no intrapulmonary abnormalities. Based on the history of 90 the patient, HPS was considered. In case of HPS, cut-off values of abnormal oxygenation are a partial pressure of oxygen < 80 mmHg (10.7 kPa) or an alveolar-arterial oxygen gradient (A-a gradient) =15 mmHg (2.0 kPa) breathing ambient air. The most practical and sensitive way to detect pulmonary vascular dilatations and to a lesser extend arteriovenous communications (shunts) is contrastenhanced echocardiography with agitated saline (shaken to produce microbubbles > 10mm). In case of pulmonary vascular dilatation, microbubbles opacification in the left atrium occurs after three to six hearth beats. Contrastenhanced echocardiography in this case was positive after five to six hearth beats. Administration of oxygen relieved dyspnea and resulted in adequate oxygenation. A classification of severity is vital because the severity of HPS influences survival and is useful in determining timing and risks of liver transplantation. Transplantation in this case was considered and rejected, because of the combination of severity of abnormal oxygenation, general condition and age of the patient. Conclusion: Although dyspnea in patients with portal hypertension and/or cirrhosis can be due to other causes such as anaemia, ascites, muscle wasting, hepatic hydrothorax and/or chronic obstructive pulmonary disease, HPS must be considered because of the consequences for treatment. be hepatic abscesses. An additional CT-scan showed two liver abscesses of 8 cm and 3 cm in diameter, as well as a thickened mucosa of the terminal ileum and the suggestion of a Meckels diverticulitis. A Meckel-scan showed no ectopic gastric acid production, which made a Meckels diverticulum unlikely. A colonoscopy was performed which showed an ileitis of (at least) the last 30 cm with ulcerations, and skip lesions matching Crohn’s disease. Biopsies showed an active inflammation with ulceration likely to be Crohn’s disease. Blood cultures showed a Streptococcus intermedius. Faecal cultures showed absence of protozoa and other bacteria. Treatment consisted of antibiotics (Ceftriaxon and metronidazol) initially intravenously and later on Ciproxin orally. At that time no immune suppressive therapy was administrated. The abscess size declined and the clinical condition of the patient improved. After six weeks of antibiotic therapy there was no evidence for an active infection and treatment of Crohn´s disease was started with budesonide 9 mg and Puri-Nethol 125 mg daily. Conclusion: A liver abscess is a rare complication of Crohn’s disease and it is even more seldom described as the presenting symptom. The hypothesis of underlying pathology is bacterial translocation across damaged intestinal mucosa in Crohn’s disease followed by portal bacteraemia. 167. A rare first presentation of Crohn’s disease 168. Freak of nature J.W.G.M. Schreurs, M.E. Bartelink, M.A. van Herwaarden Deventer Hospital, Department of Internal Medicine, Jan van Arkelstraat 28, 8266 CN KAMPEN, the Netherlands, e-mail: schreursjohn@live.nl S. Boudewijns, C.M. Schweitzer, F.H.J. Wolfhagen TweeSteden Hospital, Department of Internal Medicine, Dr. Deelenlaan 5, 5042 AD TILBURG, the Netherlands, e-mail: steve_boudewijns@hotmail.com Introduction: A liver abscess is either an amoebic abscess or an pyogenic abscess. However, only 7% of the pyogenic liver abscesses are due to portal bacteraemia. A hepatic abscess is a rare complication of Crohn’s disease, and has to our knowledge only 3 times been described as the presenting symptom in the last decades. Case report: A previously healthy 43-year-old, male with a history of two gastric bleedings was admitted to the gastro-enterology ward with abdominal pain in the right upper quadrant, fever, chills and anorexia for 3 days. There were no symptoms of nausea, vomiting or changed bowel habits. On physical examination temperature was 39.60C and there was slight tenderness in the upper abdominal region without organomegaly. Laboratory examination showed leukocytes of 33.5/nl, C-reactive protein of 237 mg/l, normal electrolytes and renal function, bilirubin 35/17 umol/l, Alkaline Phosphatase 208 U/l, GGT 93 U/l, ASAT 40 U/l, ALAT 57 U/l, LDH 236 U/l. Ultrasound examination showed two lesions suspect to Introduction: Dysphagia is a frequently reported complaint and has different causes. A thorough analysis is necessary to achieve a correct diagnosis and appropriate therapy. We report on a young woman with dysphagia and weight loss. Case report: A 23-year-old woman, with a history of ADHD and morbus Osgood-Schlatter, presented with dysphagia and twelve kilograms loss of weight. She had trouble swallowing food since a couple of months. Liquids had not been a problem. She had been using methylphenidate since 6 months. Physical examination was unremarkable except for extreme nausea during palpation of the neck. Laboratory results were all within the normal range and an esophagogastroduodenoscopy was normal. At first a barium swallow showed no pathology of the oesophagus or stomach. Manometry of the oesophagus showed a high-pressure zone with pulsations in the proximal part of the oesophagus. This raised the suspicion of compression of the oesophagus by an arteria lusoria, which was confirmed by CT-scan. So, most likely the patient 91 deficiency. The test results for lysosomal storage diseases were inconclusive. Histological examination of a liver biopsy identified a normal liver. Finally, extensive revision of the sagittal and coronal images of the CT scan revealed a marked enlargment of the right liver lobe typical for a Riedel’s lobe. Riedel’s lobe is a tongue-shaped projection of the liver from the inferior surface of the right lobe. It is a normal anatomical variant and seen most frequently in women. The lobe may be quite large, sometimes extending into the right iliac fossa, and so, can be easily mistaken for pathological enlargement of the liver. suffered from dysphagia lusoria. In retrospect the barium swallow showed a possible compression of the proximal oesophagus. Because of her severe complaints the patient was presented to a vascular surgeon for reconstruction of the vascular anatomy. Discussion: Dysphagia secondary to extrinsic esophageal compression by an aberrant right subclavian artery (arteria lusoria) is known as dysphagia lusoria. David Bayford first described it in 1794, and called it ‘lusus naturae’, meaning ‘freak of nature’. The aberrant right subclavian artery arises from the dorsal part of the aortic arch. It is a relatively common congenital anomaly, with a prevalence of up to 1,8%. This may be asymptomatic, but symptoms varying from mild to severe dysphagia have been reported. Usually a barium swallow reveals the abnormality and sometimes it is seen with endoscopy. Diagnosis is confirmed by CT-thorax or MR angiography. Therapy depends on the severity of the symptoms. In some cases dietary changes are sufficient, whereas in more severe cases surgical transposition of the aberrant artery is necessary. The results of surgical intervention are good with relief of symptoms in nearly all patients. Conclusion: An arteria lusoria as most likely cause of dysphagia is described. Usually, an arteria lusoria is discovered by a barium swallow investigation, but in this case it was detected by manometry of the oesophagus. Manometry may reveal unexpected and uncommon causes of dysphagia. 2 mm skin biopsies from the eschars of all four patients. Results were known within one week, where as positive serology was not obtained until several weeks after patients had completely recovered. Conclusions: ATBF should be considered in travellers returning from South Africa with (sub)febrile illness and multiple skin lesions. The diagnosis can be confirmed by (paired) serology, however PCR and sequencing on skin biopsies could be a (better) alternative confirmatory test. This will have to be validated in larger studies. Advantages of molecular methods over serology are exact determination of the infectious agent and the timeframe within which the diagnosis can be confirmed. weeks with good clinical response. He was switched to oral maintenance therapy with itraconazole and highly active antiretroviral treatment was initiated. Discussion: Sporotrichosis is caused by the dimorphic fungus Sporothrix schenckii and is a rare invasive mycosis. The fungus usually grows in decaying material, soil, or hay. History usually reveals trauma to the skin, which causes direct inoculation of the conidia (spores) into the wound. Ulcerative nodules in the draining lymph-tract are usually seen, but in immunocompromised patients hematogenic dissemination can occur with meningeal, osteoarticular, pulmonary, visceral, and rarely other organ involvement. Presumably our patient also had laryngeal infiltration. Diagnosis is based on culture and microscopy of material obtained from involved tissue sites. Histopathologic examination of tissue biopsies is not sensitive nor specific, but can help to rule out other pathology. There are no randomised studies addressing treatment of disseminated sporotrichosis. Guidelines recommend to start with lipid formulations of intravenous amphotericin b and switch to oral itraconazole for long-term maintenance therapy. In patients with persisting immunosuppression, lifelong suppressive therapy with itraconazole is advocated. XV. INFECTIOUS DISEASES RESEARCH XVI. INFECTIOUS DISEASES CASE REPORTS 170. Diagnosis of African tick-bite fever infection in travellers returning from South-Africa J.W.R. Hovius1 , R.W. Wieten 1, E. Tijsse-Klasen 2 , H. Sprong2, M.C. Beersma3, M.P. Grobusch1 1 Academic Medical Centre, Department of Internal Medicine, Bilderdijkkade 31 II, 1053 VH AMSTERDAM, the Netherlands, e-mail: j.w.hovius@amc.uva.nl, 2RIVM, BILTHOVEN, the Netherlands, 3Erasmus Medical Centrum, ROTTERDAM, the Netherlands 169. Too large but normal – Riedel’s lobe Introduction: African tick-bite fever (ATBF) is frequently diagnosed in travellers returning from South Africa. It is the only tick-transmitted rickettsiosis in which several inoculation eschars are observed in a high proportion of cases. AFTB is caused by Rickettsia africae, a gramnegative bacterium, belonging to the spotted fever group of Rickettsiae. The principal vectors for ATBF in southern Africa are Amblyomma hebraeum ticks. The diagnosis is based on the travel history and clinical presentation, but is confirmed by detecting antibodies in serum against Rickettsiae of the spotted fever group. However, these serological tests have major shortcomings. Antibodies typically occur late in the course of the disease and early antibiotic treatment or a mild course of the disease can diminish antibody production. Methods and results: Here, we describe four male travellers that presented with (sub)febrile temperature and multiple skin lesions several days after returning from SouthAfrica. They were suspected of having contracted African tick-bite fever. As we expected initial immunofluorescence assays yielded no IgM/IgG antibodies directed against Spotted Fever Rickettsiae. However, Rickettsia africae DNA, using two independent polymerase chain reactions (PCRs, i.e. and confirmed by sequencing, was amplified from M. Kok, S. Lobatto, S.A. Luykx-de Bakker Tergooi Hospitals, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: kokmarleen@hotmail.com Case: A 61-year-old woman without a significant medical history was referred to our outpatient department with hepatomegaly. The hepatomegaly was discovered over ten years ago during a routine check-up. Besides a chronic vague abdominal pain in the right upper quadrant, the patient reported no medical problems. There was no history of alcohol abuse and she did not take any medication or supplement. On physical examination the liver was palpable over 5 cm under the costal margin. No icterus, stigmata of liver disease or signs of splenomegaly or heart failure were present. Laboratory investigations showed mildly elevated transaminases and gammaglutamyltransferase. Abdominal ultrasound and CT-scan showed an enlarged liver extending into the right pelvis but no further abnormalities. Additional biochemical investigation excluded viral and auto-immune causes, as well as Wilson’s disease, hemochromatosis, alpha-1-antitrypsin- 92 171. Full of fungi J.C. Dutilh1, E. de Barra2, J.J. Taljaard3 1 University Medical Centre Utrecht, Department of Internal Medicine, Heidelberglaan 100, 3584 CX UTRECHT, the Netherlands, e-mail: j.c.dutilh@umcutrecht.nl, 2Galway University Hospital, GALWAY, Ireland, 3Tygerberg Academic Hospital, KAAPSTAD, South Africa 172. Als de kat van huis is… M.M.C. Lambregts, P.H. Rothbarth, M.B. Crijns, S. Anten, N.M. Delfos Rijnland Hospital, Department of Internal Medicine, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: merel_lambregts@hotmail.com Introduction: Sporotrichosis is an invasive mycosis caused by Sporothrix schenckii and is endemic in large parts of Central- and South America and Africa. In severely immunocompromised patients it can cause disseminated disease. Case: A 31-year-old HIV-positive man was referred to Tygerberg Academic Hospital (Cape Town, South-Africa) by a primary care facility with skin lesions. His CD4 count was 18 cells per cubic millimeter. He worked as a construction worker and had been receiving antituberculous therapy for several months for pulmonary tuberculosis. The skin lesions had developed over a period of three months. There were multiple painless, ulcerative, and nodular lesions in the face, on the trunk, and on the extremities. Three weeks prior to admission he developed dysphonia. At presentation he was afebrile and not acutely ill. On examination a swollen proximal interphalangeal joint was noted on his right middle finger. X-ray of this finger showed a lytic lesion with interruption of the cortex. Laryngoscopy revealed ulcerating granulomas on the vocal cords. A skin biopsy showed granulomatous inflammation. A Ziehl-Neelsen-stain was negative and PAS-stain with diastasis sporadically showed fungal conidia. Culture of the skin biopsy grew Sporothrix schenckii. The patient was treated with amphotericin b intravenously for two Case: A 35-year-old woman presented with fever and a crusting ulcer on her chest. The lesion occurred a few weeks earlier when a vesicular eruption developed and progressed to a brownish crusting ulcer with vesicles on the borders followed by cellulitis and painful axillary lymfadenopathy. Recently, she had bought kittens at a nearby flowerfarm and had frequently held them to her chest, petting them. Since one of the kittens had contracted a skin disease, she consulted a veterinarian. The cat was successfully treated for a presumed bacterial and fungal infection, without further testing. Other animal contacts were not reported. Gram-stain and culture of the lesion were negative, probably due to prior antibiotic treatment. While awaiting further results the cellulitis improved on a regimen of amoxicillin/clavunalate and ciprofloxacin for suspected secondary bacterial infection or cat scratch disease. Eventually cowpox virus was cultured from the lesion, and confirmed by polymerase chain reaction (PCR). We concluded that the patient was infected with the cowpox 93 virus by her kitten leading to a single skin lesion followed by a secondary infection with common cellulitis. Discussion: Cowpox virus is a DNA virus, part of the orthopoxvirus family, as is smallpox. The name cowpox historically originates from dairymaids getting infected through infected teats of cows, which ultimately led to the smallpox vaccine. Today, cowpox is a rare disease in humans. However, the Netherlands have a relatively high and rising prevalence, mainly affecting young people. This can probably be attributed to the fact that routine smallpox vaccination was abandoned in 1976 because of global smallpox eradication. Despite the name, most cowpox-infections are transmitted by domesticated cats and mice. Rodents, but not cows, are the reservoir hosts of cowpox virus. The kitten in this case probably got infected by hunting voles. The incubation period is 10-14 days, starting with localized vesicolopustular lesions at the site of contact, mostly the hands and lower arms. After days to weeks the lesions ulcerate and a crust develops. Secondary bacterial infection with local lymphadenopathy is common. The combination of a typical history and skinlesion should raise suspicion of cowpox virus. However, other zoonotic infections, particularly other orthopoxvirussen, parapoxvirussen and catscratch disease, may produce resembling lesions. The disease is self-limiting in otherwise healthy individuals. However, secondary lesions and generalized eruption may occur in immunocompromised patients and in patients with skin diseases. Discussion: Rat bite fever, caused by Streptobacillus moniliformis, is characterized by fever, polyarthralgias and a rash. The rash may appear petechial, purpuric or maculopapular, sometimes with hemorrhagic vesicles. The rash is seen on the extremities, especially the hands and feet. Rat bite fever typically follows a rat bite, but can also occur after the ingestion of food or water that has been contaminated with rat excrement. S. monilliformis is a Gram-negative bacillus and is almost the exclusive cause of rat bite fever in the United States and Europe. Spirillum minus can also cause rat bite fever and accounts for most cases in Asia. The incubation period of S. moniliformis-associated rat bite fever ranges from 3 days to over 3 weeks, but is in most cases less than 7 days. The mortality rate is 13% when untreated and causes of death include endocarditis, pneumonia and overwhelming sepsis. The differential diagnosis include Lyme disease, Rickettsial infections, Leptospirosis, secondary Syphilis, Meningococcemia and sepsis from Staphylococcus aureus and Streptococcus pyogenes. Diagnosis is made by culture of blood or synovial fluid. Streptobaccillus requires culturing on enriched media. Penicillin is the treatment of choice for 14 days. For penicillin-allergic patients tetracyclines are also effective. Conclusion: Rat bite fever should be considered in any patient with a clinical triad of fever, arthralgias and a rash, especially patients who are exposured to rats. 173. Rat bite fever N. Josephus Jitta, B.M. van der Oord Meander Medical Centre, Department of Intensive Care Unit, Utrechtseweg 160, 3818 ES AMERSFOORT, the Netherlands, e-mail: n.josephusjitta@gmail.com 174. A skin infection in an immunocompromised patient – don’t miss odd pathogens! M. Ezzahti, A.J.W. Kluytmans, I.M. Kuijpers, J.B. Heijns Amphiahospital, Department of Internal Medicine, Molengracht 21, 4818 CK BREDA, the Netherlands, e-mail: ezzahti00@hotmail.com Introduction: We present an immunocompromised patient with a skin infection: a common combination, but caused by an uncommon pathogen. Case: A 79-year-old man was admitted to our ICU, after initial presentation at the emergency ward. His medical history included COPD and chronic kidney disease stage 3. Under suspicion of polymyalgia rheumatica, he had been using steroids (prednisone 15 mg daily) for over five years. A few hours before presentation he developed pain in his left leg, later he noticed some redness. During the next hours the pain increased and redness expanded. At presentation the patient was clearly in pain, his hemodynamics were stable and his temperature was 37 °C. We noticed a sharply demarcated rash, covering his left leg and the calf of his right leg. During his stay at the emergency ward, the redness rapidly expanded and the patient became somnolent. He was treated with cefuroxim and gentamycin (local protocol for sepsis of unknown origin), which was Case: A 48-year-old man with no medical history presented with a two-day history of fever, arthralgias and a pustular rash. The man was bitten two weeks before by his pet rat on his left thumb. On physical examination the blood pressure was 136/80 mmHg, his heart rate was 108 beats/ min and the temperature was 38,6 °C. The patient had a pustular rash on his palms of his hands and soles of his feet. Further physical examination was unremarkable. Lab results showed a CRP of 248 mg/l, leukocytes of 16,2 x 109/l and a normal renal function. Blood cultures were negative. Streptobacillis moniliformis was identified from a culture of a pustule on his left hand. A diagnosis of rat bite fever was made. The patient was treated with amoxicillin/ clavulinic acid 1 week intravenously and 1 week orally. The patient recovered completely. 94 shortly followed by penicillin and flucloxacillin (local protocol for erysipelas). The patient was admitted to our ICU. We continued penicillin and started clindamycin. Under suspicion of necrotizing fasciitis, we performed a biopsy of the fascia of his left calf. Surprisingly, Gram stain was negative. During the next hours he patient’s condition improved and the rash didn’t expand anymore. After being stable for 24 hours, the rash expanded again till it covered all four limbs, but the patient remained otherwise stable. Blood cultures were negative. After 36 hours the biopsy showed grow of Pseudomonas Aeruginosa. Pathological examination of the biopsy wasn’t typical of fasciitis, but was more consistent with cellulitis. Ceftazidim was started, combined with clindamycin, because we couldn’t exclude coinfection with S. Pyogenes. The rash gradually improved. The patient slowly recovered. He was discharged from the hospital after one month. Discussion: We present a 79-year-old immunocompromised patient with a severe cellulitis, caused by P. Aeruginosa. P. Aeruginosa is an aerobic, Gram negative bacillus. It is a common pathogen in immunocompromised patient. P. Aeruginosa usually causes infections of the respiratory or urinary tract, or infections of the eyes or ears. Both fasciitis and cellulitis are rare. Cellulitis, caused bij P. Aeruginosa usually presents with necrotic skin ulcerations. In our patient, we saw a very painful, sharply demarcated rash on both legs, which rapidly progressed, and seemed to be more consistent with necrotizing fasciitis. not disinfected. Five days later, the patient developed fever and progressive pain and swelling of the right shoulder, which she could barely move. At hospital admission, the patient was febrile (39.0 °C). Blood pressure was 124/65 mmHg, heart rate 106 beats per minute and respiratory rate 28 breaths per minute. Physical examination revealed no heart murmurs, abnormal lung sounds or petechiae. Her right shoulder was swollen without redness, tender to palpation and extremely painful to all active and passive movements. The dorsal side of her right foot showed a small lesion that, according to the patient, had been caused by the recent acupuncture treatment. Laboratory investigation showed a markedly raised C-reactive protein level (304 mg/l), without leukocytosis. X-ray and ultrasound examination of the right shoulder showed no abnormalities. A shoulder punctate showed clear synovial fluid. After taking blood cultures, the patient was treated with cefuroxim intravenously. Two days later, she developed hypoxia. A chest-CT showed large bilateral infiltrates. The presence of hematogenic pneumonia was considered. At that time, Staphylococcus aureus grew in multiple blood cultures and the culture of the shoulder punctate. Thereupon, the antibiotic regimen was switched to flucloxacillin intravenously for three weeks. Ultrasound investigation of the heart showed no signs of endocarditis. She recovered gradually. The right shoulder improved slowly with physical therapy. Two months later, she had still not regained full function of her right arm. Conclusion: Sepsis is a rare, but potentially fatal complication of acupuncture. The effectiveness of acupuncture for the treatment of CFS is not proven. 175. An uncommon cause of Staphylococcus aureus sepsis 176. An abdominal emergency M.L. Maas, P.C. Wever, A.W. Plat, E.K. Hoogeveen Jeroen Bosch Hospital, ’s-Hertogenbosch, Department of Internal Medicine, Tolbrugstraat 11, 5211 RW ’s-HERTOGENBOSCH, the Netherlands, e-mail: m.maas@jbz.nl C.S. Ootjers, M.J.F.M. Janssen, A.M. Schrander-van de Meer, M.K. Vu Rijnland Hospital, Department of Internal Medicine, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: claudia.ootjers@gmail.com Introduction: Acupuncture is increasingly used to treat a variety of conditions such as chronic fatigue syndrome (CFS), for which there is no proof of effectiveness. Therefore, it is important to establish whether its potential benefits outweigh its risks. The risk of a serious adverse event with acupuncture is estimated to be 0.05 per 10.000 treatments. We report a case of Staphylococcus aureus sepsis due to acupuncture. Case: A previously healthy 48-year-old woman was admitted to hospital because of fever and severe pain of the right shoulder since two days. A week before admission, she had received acupuncture treatment for CFS. Sterile needles had been inserted into the skin of her head, shoulders and feet. With standard acupuncture, the skin is Introduction: Atraumatic splenic rupture is a rare event that has been associated with several infectious disease processes and that requires immediate diagnosis and prompt surgical treatment to ensure patient’s survival. Case report: A previously healthy 55-year-old male presented to the emergency department with fever and chills since 5 days, without localizing signs. He collapsed during his visit to the general physician earlier that evening. Examination demonstrated beside fever and hemodynamic instability minimal tenderness to palpation over the left lower quadrant of the abdomen without rebound or guarding. The remainder of his physical 95 fever. The pain was sharp and worsened on mobilization. He had no diarrhea, and the stools appeared normal. No family members were sick and there was no history of a recent travel. He had a slightly productive cough with white mucus. We saw an ill looking patient with a temperature of 39 °C and a heart rate of 100/min. There was a normal peristalsis and defense musculaire especially around McBurney, with direct and rebound tenderness. Laboratory findings: leukocytes 19.6 x 109/l and CRP 181 mg/l, normal liver and kidney functions. Ultrasound was inconclusive. Because of clinically high suspicion on appendicitis, an exploratory laparoscopy was performed. A normal appendix was found. Further exploration of the abdomen did not reveal another cause for the pain. After surgery fever continued and an abdominal abscess was suspected. On abdominal CT scan no abscess was found, however, in the upper slice an empyema in the right lower pulmonary lobe was seen. Culture of the pus was positive for Staphylococcus aureus sensitive for flucloxacilline. After drainage and antibiotic treatment the patient fully recovered and was released one month after admittance. Discussion: Although on physical examination an acute abdomen was apparent, the relatively high levels of infection parameters, temperature and the cough were a clue that something else could be wrong. A chest X-ray should have been made. Then adequate therapy could have been started sooner, without an unnecessary operation. Conclusion: Although every physician should know that abdominal pain and fever may have a thoracic origin, this case illustrates that in clinical practice there is not always attention for this relationship. It can not be stressed enough that especially pneumonia and pleural empyema may present as an acute abdominal problem. examination was unremarkable. Laboratory investigation revealed pancytopenia (hemoglobin 6.9 mmol/l, leucocytes 3.9 mmol/l with 40% immature neutrophils; Platelet count 82 x 109/l) and increased C-reactive protein of 65. Chest radiography and urine analysis were normal. Because hemodynamic instability remained, despite adequate resuscitation measures taken in the emergency department, the patient was taken to the Intensive Care Unit (ICU) for optimal support. Cefuroxime, gentamicin and metronidazole was started on empirical base. During his stay on the ICU the hemodynamic instability remained and his abdominal pain increased with signs of peritonitis. An abdominal focus of sepsis seemed most likely and a CT-scan of the abdomen was performed on which a diagnosis of atraumatic splenic rupture was ultimately suspected. After exploratory laparotomy with confirmation of multiple ruptures, splenectomy was performed, and the patient made a full, uneventful recovery. Histopathologic examination revealed increase of neutrophilic granulocytes (consistent with sepsis), with bleeding and multiple ruptures of the capsule. Results for serologic testing over the patient’s hospital course and after discharge were negative. Conclusion: Atraumatic splenic rupture is a rare event that may lead to life-threatening hemorrhage if not diagnosed and treated quickly. Although the infectious organism which caused the sepsis of the patient’s case remains unknown, atraumatic splenic rupture has been associated with a variety of infectious diseases. Increased awareness of atraumatic splenic rupture as a possible complication of various infectious disease processes can enhance early diagnosis and effective treatment. 177. Acute abdomen; not always appendicitis J.E.M. Mellema, V. Mattijssen Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815AD ARNHEM, the Netherlands, e-mail: liesbeth.mellema@hotmail.com 178. Abiotrophia defectiva: a very rare cause of spondylodiscitis J.B. van der Net, A.P. Rietveld, M. Castro Cabezas, R.G. Wintermans, P. de Man1 Sint Franciscus Gasthuis, Department of Internal Medicine, Zestienhovensekade 501, 3043 KT ROTTERDAM, the Netherlands, e-mail: j.vandernet@sfg.nl Introduction: Appendicitis is the most common cause for acute abdomen. About 10-20% of patients operated because of appendicitis eventually, are diagnosed otherwise. False positive results are acceptable because of the severe complications of a perforated appendix, compared to the low morbidity and mortality of an appendectomy. Anamnesis and physical examination are as always, the cornerstones of evaluating a patient. The next case report illustrates one of the pitfalls in evaluating a patient with abdominal pain. Case report: A 43-year-old man with no known medical history was admitted to the emergency department with abdominal pain which started about five days before, located in the right lower quadrant and umbilical region. He also had cold chills, nausea, vomiting, anorexia and Introduction: Spondylodiscitis (or vertebral osteoarthritis) is an infection of the spinal vertebrae and the adjacent intravertebral disc space. In developed countries Staphylococcus aureus is the main cause. Here, we report a very rare cause of spondylodiscitis. Case report: A 46-year-old man with a history of hypertension was admitted to our hospital because of lower back pain and abdominal pain in the lower left quadrant, which had existed for three days and was worse at night. The pain began gradually and progressively worsened. Because of the 96 back pain he had been bedridden for two days. There were no signs of urinary tract infection. His stool was normal en he did not have fever. There was no muscle weakness or sensory change. On physical examination, there were no remarkable findings, apart from local tenderness in the lower left abdomen. There was no tenderness with palpation or percussion of the spine. Laboratory results showed an elevated C-reactive protein and an elevated leukocyte count with immature bands. CT-scanning of the abdomen showed no remarkable intra-abdominal findings, but did show a degenerative aspect of the lumbar spine. An MRI of the lumbar spine showed spondylodiscitis of L2-L3. The gram stain of blood cultures showed gram-positive pleomorphic bacterial growth, both coccoid and rod shaped. Some of the rod-shaped forms had a central bulb. In expectation of the definitive determination, our patient was treated with amoxicillin intravenously. Aerobic and anaerobic growth was very slow and poor. Biochemical identification with the VITEK system (Biomerieux) revealed Abiotrophia, a finding consistent with the gram stain, and poor growth. Later, 16S rRNA sequencing confirmed that our isolate was an Abiotrophia defectiva (A. defectiva) strain. Therapy was switched to oral rifampicin and clindamycin for a total of six weeks. There was considerable destruction of the lumbar spine. Therefore, a brace was prescribed to reduce the pain and stabilize the spine. Repeated transesophageal echocardiography did not reveal any sign of endocarditis. Discussion: A. defectiva is part of the normal flora of the intestinal and urogenital tract and is a very rare cause of endocarditis. There are only a few case reports in literature showing spondylodiscitis caused by A. defectiva, but all secondary to endocarditis. To our knowledge, this case report is the first to show spondylodiscitis caused by A. defectiva, without signs of endocarditis. pain and progressively loss of memory since three months. Physical examination upon admission showed a man normal habitus with a weight of 55 kg. His blood pressure was 130/65 mmHg, pulse rate 70 beats/min and body temperature 36.5 °C. There were no enlarged palpable lymph nodes in the neck, supraclavicular, axillar or inguinal. Auscultation of lungs and heart was normal. Palpation of the abdomen revealed no abnormalities. Neurological examination was normal. Laboratory investigation showed a microcytic anaemia with reduced serum iron, transferrin and ferritin. Electrolytes, renal function and liver tests were within the normal limits. Faecal fat analysis demonstrated steatorrhoea: 5.4 g/24 h stools and stool culture was normal. Chest X-ray showed mild pleural effusion without other abnormalities. Abdominal CT showed enlarged lipoid mass along the mesenteric veins. Gastroduodenoscopy showed macroscopic duodenitis and duodenal biopsies showed increased histocytic macrophages laden with PAS-positive globulin, without signs of malignancy or mycobacterial infection. Cerebrospinal fluid obtained by lumbar puncture showed a elevated protein level (0.46 g/l). Examinations of cell pellets obtained by cytocentrifugation of CSF samples were positive for PAS staining. Polymerase chain reaction testing of the CSF was positive for Tropheryma whipplei resulting in strong evidence of neuro-WD. Brain magnetic-resonance imaging showed minimal loss of cerebral and cerebellum tissue. Our patient was treated with intravenous ceftriaxone (2 g daily) for two weeks and followed by oral co-trimoxazole (trimethoprim plus sulphamethoxazole, 960 mg twice per day) for at least one year. During antibiotics therapy patient showed complete resolution of complaints together with reversibility of cognitive impairment. Conclusion: WD should be considered in any patient with, diarrhoea, fever, malabsorption, weight loss, abdominal pain or lymphadenopathy. CNS involvement may occur and the prognosis for patients with neurological signs remains poor. If the diagnosis is considered, this condition can be readily diagnosed and shows good clinical response with long-term antibiotics. 179. A patient with Neuro-Whipple’s disease F.M.F. Alidjan, T. Seerden, B. Veldhuijzen Amphia Hospital, Department of Internal Medicine, Molengracht 21, 4800 RK BREDA, the Netherlands, e-mail: falidjan@amphia.nl 180. The great pretender strikes again Introduction: Whipple’s disease (WD) is a systemic disease caused by a gram-positive bacterium, Tropheryma whippelii. Although the first descriptions of the disorder described a malabsorption syndrome with small intestine involvement, the disease also affects the joints, cardiovascular system, and central nervous system(CNS). CNS involvement may be silent and its clinical expericience is sparsely reported. We report a 68-year-old male with WD with involvement of the CNS. Case: A 68-year-old man without a medical history was admitted at our hospital with nonbloody diarrhoea, loss of appetite, weight loss of ten kilogram, diffuse abdominal Y. Eling, A.I.M. Hoepelman, D.J. Hijnen, V. Sigurdsson, J.E. Arends Utrecht University Medical Centre,Department of Internal Medicine and Infectious Diseases, PO Box 85500, 3508 GA UTRECHT, the Netherlands, e-mail: y_eling@hotmail.com Introduction: Syphilis is a sexually transmitted disease caused by the spirochete Treponema pallidum often seen in men who have sex with men and shows a high rate of HIV co-infection. We describe a patient with a very rare 97 Case: A 72-year-old female patient suffered from arthralgias and arthritis for ten years. Analysis by rheumatologist, neurologist and internist did not led to a definite diagnosis. Due to anaemia, increased ESR and substantial weight loss multiple gastroduodenoscopies and colonoscopies were performed, but no explanatory macroscopic abnormalities were observed. During these procedures mucosal biopsy specimens were harvested, which did not reveal histologic abnormalities. As part of a scientific study in the analysis of intestinal microbiota, mucosal biopsy specimens were subjected to a specific real-time qPCR targeting an exclusive, repetitive sequence of T. whipplei. Periodic acid schiff (PAS) staining of stored mucosal biopsy specimens from both duodenum and colon showed purple-stained foamy macrophages in the lamina propria. Subsequently, patient underwent gastroduodenoscopy with harvesting of mucosal biopsy specimens from the duodenum. No histological abnormalities were observed, with PAS-staining being negative. Nonetheless, qPCR was positive for T. whipplei DNA. In addition, due to low back pain for years with radiation to the right leg, suspicion of infectious spondylodiscitis aroused. Therefore, an MRI of the spinal column was performed which showed signs of discitis localized at L2-L3. Bone biopsy from L2 was harvested, in which no histological abnormalities were present including negative PAS-staining. However, T. whipplei DNA was detected by qPCR. To exclude presence of T. whipplei in the cerebrospinal fluid, lumbal puncture was performed, and proved to be negative for T. whipplei DNA. Since convincing evidence for Whipple’s disease was present, including an infectious (spondylo)discitis but without central nervous system involvement, patient received intravenous ceftriaxone for two weeks, followed by trimethoprim-sulfamethoxazole twice daily for a year. Currently, situation of the patient has clinically improved significantly with weight gain of 15 kg in five months and absence of arthralgias. However, radiating pain persisted because of which she is currently being treated by a neurosurgeon. Obviously, not only CNS involvement could lead to irreversible damage, but also the consequences of spondylodiscitis due to T. whipplei infection. In this case the coincident diagnosis of T.whipplei infection as part of a scientific study led to accurate treatment of this potentially lethal disease. manifestation of syphilis which was initially misdiagnosed. The incidence is increasing in the Netherlands from 250 cases in 2005 to 512 diagnoses in 2009 in STD clinics. Case: A 34 year old homosexual man diagnosed with HIV in 2009 and a normal CD4 count and no current cART developed multiple nodular and ulcerative skin lesions in a course of two weeks. Several weeks before developing the lesions he experienced an episode of fever in combination with chills. Shortly afterwards several purple nodules appeared that progressed into well demarcated ulcerations some covered by a dark crust and others with necrotic material. His general physician suspected a bacterial infection and started a course of flucloxacillin, though promptly hereafter new lesions formed. Laboratory studies revealed a slight normocytic anemia and normal white blood cell counts with a normal differentiation. The erythrocyte sedimentation rate was 75 mm/hour and C-reactive protein was 18 mg/L. Liver and renal functions were normal. A skin biopsy taken from the inside of the left thigh showed hyperkeratosis of the epidermal layer. The upper dermal layer revealed an increased vascularisation and the lower dermal layer was characterized by leucocytoclasia and lymphohistiocytic infiltration, suggesting an infectious etiology. Immunohistochemistry for HHV8 and spirochetes were however negative as were bacterial cultures and PCR’s for Bartonella and mycobacteria. The serum VDRL was positive (1:64) as was the CLIA for Treponema pallidum and confirmation via Trepnonema pallidum immunoblot having previously tested negative. The diagnosis of secondary syphilis in the form of a nodulo-ulcerative syphilis was made and the patient was administered intramuscular penicillin-G. At a subsequent visit one month later the patient showed significant clinical improvement. Discussion: Nodulo-ulcerative syphilis or lues maligna is a form of secondary syphilis characterised by papules, plaques as well as nodules which tend to ulcerate. Typically the face is involved and contrary to other forms of secondary syphilis the palms and soles are spared. Although this is a rare presentation of a well known disease, due to the ever increasing incidence of syphilis especially in the MSM population it is yet again an entity to be reckoned with by a disease known as the great pretender. 181. Science saved her life: diagnosis of severe T.whipplei infection by coincidence 182. Acute abdominal pain as first sign of severe varicella zoster in the immunocompromized patient M.E. Grasman, A.M. Pettersson, N. Rabelink, P.H.M. Savelkoul, A.A. van Bodegraven, E.A. bij de Vaate VU Medical Centre, Department of MDL, De Boelelaan 1118, 1081 HV AMSTERDAM, the Netherlands, e-mail: thijsgrasman@hotmail.com A.H.W. Bruns, H.J. Bloemendal, R. Fijnheer Meander Medical Centre, Utrechtseweg 160, 3818 ES AMERSFOORT, the Netherlands, e-mail: ahw.bruns@meandermc.nl 98 Introduction: Tuberculosis is a chronic disease caused by Mycobacterium tuberculosis. It usually infects the lungs but may effect any part of the body. Most infected individuals harbor the tuberculosis bacterium without symptoms, but may later on develop active disease. Diagnosing tuberculosis may be very difficult. Case: A 68-year-old Turkish woman, living in the Netherlands, presented with fever, cold shivers, night sweats, and abdominal pain. Her medical history revealed Parkinson’s disease. On physical examination she had high fever (40.7 °C) and abdominal tenderness. Her laboratory results showed progressive anemia and thrombocytopenia, with normal leukocyte counts, elevated C-reactive protein levels (63 mg/l), elevated liver enzymes, and diffuse intravascular coagulation. CT scans showed thoracic para-aortal lymphadenopathy. Extended microbiological evaluation including blood and urine cultures, viral hepatitis, HIV, EBV, CMV, malaria, brucellosis, and leishmaniasis remained negative. The IGRA test (Interferon Gamma Release Assay) was positive, and active tuberculosis was suspected. A bone marrow puncture and biopsy were performed, for pathological examination and culture on tuberculosis. There were no granulomas nor acid-fast rods in the bone marrow biopsy. Remarkable was the presence of increased numbers of T lymphocytes in the peripheral blood and bone-marrow. Immunophenotyping of the peripheral blood showed that this concerned a CD1a, CD4, aßTCR, CD56 restricted T-cel population with loss of CD7 expression. This was the reason to seriously consider a T cell lymfoproliferative disease in the differential diagnosis. Meanwhile, the patient had become very ill, and 13 days after admission treatment for tuberculosis was started. Four days later she died of multi-organ failure. Afterwards the bone marrow culture on tuberculosis became positive. Conclusion: This patient was admitted with high fever. Tuberculosis was suspected because of her Turkish origin and positive IGRA test, and ultimately proven in the bone marrow culture. The remaining question was: how to explain the pathological T cells in blood and bone marrow? The immune response elicited after Mycobacterium tuberculosis infection is critically dependent on CD4+ T cells during both acute and chronic infection. In addition to CD4+ T cells, other T cell subsets such as gd, CD8+ and CD1-restricted T cells have roles in the immune response to M. tuberculosis. A diverse T cell response allows the host to recognize a wider range of mycobacterial antigens presented by different families of antigen-presenting molecules, and thus greater ability to detect the pathogen. Case report: A 63-year-old women was admitted with nausea and acute onset of severe epigastric pain referring to her back. She successfully had undergone an autologous stem cell transplantation (SCT) for high risk plasmacell leukemia one year ago. On admission, physical examination revealed abdominal tenderness localized to the epigastric region. She had no fever, skin or mucosa lesions. Initial laboratory results showed leucopenia (WBC 2.3 * 109/l) and thrombocytopenia (50 * 109/l). The biochemistry levels including, liver enzymes, bilirubin, amylase and C-reactive protein were in the normal ranges. Chest radiography appeared normal. Abdominal ultrasound showed prominent intra-hepatic bile ducts and a distended ductus choledochus up to 1 cm without concrements. During admission her pain rapidly worsened, requiring intravenous morphine. Because of the intensity of the pain, the dilation of bile ducts and slightly raised bilirubin levels (18 umol/l) she underwent on the second day of admission an ERCP, which except of a dilated ductus choledochus turned out to be normal. On day four, she developed fever and a disseminated vesicular erythematous rash on her trunk, face and scalp and treatment with acyclovir intravenous was initiated. PCR of vesicular fluid turned out to be positive for varicella zoster virus (VZV) and serology of VZV IgG was positive. After initiating acyclovir she recovered within one week. Discussion: Reactivation of varicella zoster virus (VZV) is a common event after SCT. Visceral presentation of generalized VZV infection is uncommon, although probably an under-diagnosed event in post-SCT patients. The interval from onset of abdominal pain to the development of skin eruptions may delay the initiation of specific antiviral therapy and symptoms may be incorrectly diagnosed as gastro-intestinal or surgical disease. Therefore, varicella zoster should be considered in the differential diagnosis of abdominal pain in all immunocompromized patients, particularly when the cause is not obvious. Acyclovir therapy should be started as soon as the clinical picture shows the typical manifestation of the disease. Conclusion: Recognizing severe abdominal pain as primary sign of varicella zoster is of major importance, since it allows prompt treatment of the infection and prevents for invasive procedures. 183. Pathological T-cells in a patient with unexplained fever: malignant lymphoma or tuberculosis? S.N. Huttjes, E.J.M Mattijssen, J. Ruinemans-Koerts Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: sannehuttjes@hotmail.com 99 184. Brucellosis: an unpleasant travel companion 185. The balcony of death W. Yassi, Dr. Zwart, A. van Tellingen Zaandam Medical Centre, Department of Internal Medicine, Koningin Julianaplein 58, 1502 DV Zaandam, the Netherlands, e-mail: wisamyassi@yahoo.com M.C. van Boreen1, J. Buijs2 1 Atrium Medical Centre Heerlen, Department of internal medicine, Henri Dunantstraat 5, 6419 PC HEERLEN, the Netherlands, e-mail: maritvanboreen@hotmail.com, 2 Atrium Medical Centre, HEERLEN, the Netherlands Case: A 67-year-old woman of Turkish origin, is admitted to our internal medicine department for analysis of longstanding fever. Her medical history includes, end-stage renal failure, due to malignant hypertension, for which she recieves hemodialysis therapy. One and a half month before admission, she was treated for suspected urinary tract infection with amoxicillin, but without effect. On further questioning she has a swinging fever, with peaks in the evening. The patient is also depressed and has a decreased appetite. On physical examination she has a temperature of 39.8 °C, stable hemodynamics, flank pain and an intense lower back pain increasing with movement. She has tenderness over the lower lumbar vertebrae at the location of the sacroiliac joint. Other physical examination is not contributing, especially no heart murmurs. Blood test shows a CRP of 171 mg/l and WBC of 8.0 x 109/l. Urine analysis shows > 40 leukocytes per high powered field. Under the suspicion of pyelonephritis, patient is treated with amoxicillin /clavulanic acid intravenously, again without effect. Ultrasonography shows no hydronephrosis or abcesses. Chest and abdomen CT shows pathologically enlarged mediastinal lymph nodes and a spondylodiscitis L3-L4. Urine culture remains negative, however we switched to cefuroxime and ciprofloxacin, guided by positive blood cultures for gram-negative bacilli. The gram-negative bacilli are hard to identify biochemically. Considering the undulating temperature pattern, the ethnicity of the patient and spondylodiscitis, brucellosis is highly probable in our differential diagnosis. The Bang reaction in the serum is markedly elevated. The complement-binding reaction revealed a fourfold increase in three weeks. PCR and 16S RNA sequencing of the blood culture colony give a 99% identification as Brucella, on species level. Further identification to species level is not possible by molecular microbiology. Patient was treated with doxycyclin and rifampicin for 6 weeks with good clinical respons also, follow up CT after 6 weeks of therapy no longer shows mediastinal lymphadenopathy, and a marked reduction in spondylodiscitis. In the outpatient clinic, the patient has no recurrence of fever nor lower back pain. Discussion: In the Netherlands Brucellosis is a rare cause of fever of unknown origin. The incidence is 3 per 10 million inhabitants. The typical undulating fever, the country of origin and contact with animals may give the clue for the diagnosis. Brucellosis is a disease which should be reported to disease control authorities. Combination therapy is chosen to reduce the risk of recurrence. Case: A 73-year-old woman presented at the emergency department with nausea, fatigue and melena. One month earlier, analysis of anemia and inflammation revealed a normal gastroscopy and colonoscopy. FDG-PET-CT-scan showed abnormal metabolic activity in the upper abdomen and a small aortic aneurysm. Her further medical history was unremarkable. We saw a pale patient with normal vital signs and a pulsating abdominal mass. Laboratory tests demonstrated: hemoglobin 4.3 mmol/l, leukocytes 20.7 x 109/l. CT-angiography showed no signs of a leaking aneurysm. After admission, repeated gastroscopy because of haematemesis and hypotension revealed active duodenal bleeding. CT showed an increased aneurysm size and thrombus formation around the calcified aorta. Under suspicion of aortaduodenal fistula patient underwent immediate prosthesis-surgery. Bacterial cultures of blood and the native aneurysm remained negative. The postoperative period was complicated by recurrent infectious and ischemic problems, needing surgical closure of a duodenal perforation, resection of necrotic jejunum, gall bladder, right-sided colon and repair of multiple enterocutaneous fistulae. Due to a recent regional outbreak of acute Q-fever, serology was determined, although there was no documented primary infection. Serologic titers were 1:2048 and 1:1024 for phase 1- and 2-IgG, respectively. Despite of intensive medical and surgical treatment patient died after 5 months of hospitalization due to respiratory insufficiency and exhaustion. Q-fever, a zoonosis caused by Coxiella burnetii, affects various hosts, including humans, ruminants and pets. This Gram-negative microorganism is very resistant to environmental influences and may survive for months outside the host. Moreover, only a small inhalated inoculum may lead to infection. Dry climate and direction of the wind are closely related to human infection rate. In 2007/2008 the Netherlands was faced with the largest epidemic of acute Q-fever ever reported worldwide. In 3-5% of cases, chronic Q-fever ensues, leading to vascular complications like endocarditis and infected aneurysms or vascular prostheses. Retrospectively, the patient did not recollect having any contact with animals, nor did she live in the neighbourhood of an infected farm. The only clue was the fact that she spent many hours on her balcony in the city, 6 kilometers east-ward to the rural region of Voerendaal, the hot-spot of the Q-fever epidemic in the south of the 100 Netherlands. With the prevailing western winds, we speculate that this may have caused transmission. This dramatic case illustrates the importance of suspecting chronic Q-fever in endemic regions, even when there is no history of acute Q-fever or direct contact with infected animals. 187. Fulminant hepatitis with coagulopathy due to HSV-1 in an immunocompetent man 186. Lemierre’s syndrome Introduction: Herpes simplex infection (HSV-1) is a common and most often a benign, self-limiting disease presented with mucocutaneous lesions and mild viremia. Systemic herpes simplex infection with acute hepatitis is a rare complication of HSV-1 infection, especially in immunocompetent patients. The diagnosis is often missed due to the absence of specific signs or symptoms. Clinical manifestations are nonspecific which include flu-like illness, fever and abdominal discomfort. Fulminant HSV-1 hepatitis is usually marked by significant elevations in transaminases (ASAT higher than ALAT), and a mild or absent hyperbilirubinemia. The course of the disease is often rapid and frequently fatal. The mortality rates vary between 50 percent and 90 percent, mainly because of delayed diagnosing and treatment with antiviral therapy. We describe a patient with systemic HSV-1 infection with a fulminant hepatitis and severe coagulopathy without liver failure. Case report: A 57-year-old man, with a history of recurrent nephrolithiasis, was admitted to our hospital with fever and chills after his return from Gambia. He had his vaccinations, and used malaria-prophylaxis. Two days before presentation our patient had noticed itchy skin lesions in the neck. On physical examination he had a fever of 38.5 °C. We saw a few vesicles in the neck. Laboratory assessment revealed a low platelet count (102 x 109/l) and elevated transaminases (ASAT 1348 U/l, ALAT 852 U/l). A tropical associated disease was suspected. Because of progressive fever intravenous amoxicillin/clavulanic acid was started. Skin lesions suspected a disseminated varicella zoster virus infection and acyclovir was added. Patient’s condition worsened with the development of a severe hepatitis (maximum levels of ASAT 4530 U/l, ALAT 1978 U/l, bilirubin 12 mmol/l). There were signs of disseminated intravascular coagulation with gastrointestinal and urinary tract haemorrhages and respiratory failure with pleural effusion. PCR of serum and from a biopsy of the affected skin revealed herpes simplex virus type I (HSV-1). CT scan, thoracentesis and gastroscopy did not reveal other pathology. Antibiotics were stopped and acyclovir was continuated. On day 7 of acyclovir use patient started to improve until full recovery, including full recovery of hepatic enzymes. Laboratory testing showed no signs of immunodeficiency. Patient told he never experienced cold sores before; his wife L.J.N. Wind, F.W. Folkert, M.N. Gerding Deventer Hospital, Departement of Internal Medicine, Nico Bolkesteinlaan 75, 7416 SE DEVENTER, the Netherlands, e-mail: LJNWind@hotmail.com N.P. Barlo, A.J. Meinders, B.M. de Jongh St. Antonius Hospital, Department of Internal Medicine, Koekoekslaan 1, 3435 CM NIEUWEGEIN, the Netherlands, e-mail: n.barlo@antoniusHospital.nl Introduction: Lemierre’s syndrome is a form of thrombophlebitis caused by Fusobacterium necrophorum. Patients present with a sore throat caused by a streptococcus infection, accompanied by a peritonsillar abcess. Anaerobic bacteria like Fusobacterium grow inside the abcess and penetrate into the jugular vein and cause thrombosis and bacteremia. Fusobacterium bacteremia is uncommon, accounting for less than 1% of positive blood cultures. The majority of patients with positive blood cultures for Fusobacterium present as Lemierre´s syndrome. Case: A 27-year-old man with a blank medical history presented at the emergency department with a sore throat, vomiting and diarrhoea since 5 days. Two weeks earlier he returned from a journey to Gambia and Liberia, where he stayed for two months and did not experience any symptoms. He presented with severe hypotension, tachycardia en fever. On clinical examination he had a red pharynx, painful cervical lymphadenopathy and a diffuse painful abdomen on palpation. Laboratory tests showed thrombocytopenia, abnormal liver and kidney function tests and an increased lactate level and CRP. He was admitted at the ICU and treated with cefuroxime and gentamicin pending culture results. Extensive diagnostic research was performed for tropical diseases. Blood cultures revealed a Streptococcus milleri and Fusobacterium species. This combination of bacteria led to the clue of Lemierre’s syndrome. On CT scan there was indeed a parapharyngeal abcess and thrombosis of the left internal jugular vein. Furthermore, there were bibasilar pulmonary infiltrates, which may be explained as septic emboli from the thrombophlebitis. His travel history could not explain this disease. He was treated with penicillin and recovered well. Conclusion: Lemierre’s syndrome is a rare disease, classically presenting in otherwise healthy young adults following a pharyngitis. Blood cultures showing Fusobacterium species should point into the direction of Lemierre´s syndrome and encourage further analysis for a pharyngeal abcess, jugular vein thrombosis and metastatic spread of septic emboli. 101 and daughter experienced cold sores a few weeks before hospital admission. Conclusion: This case illustrates that awareness of HSV hepatitis, though extremely rare in immunocompetent patients, is important, since timely recognition and early initiation of antiviral therapy improves prognosis. arthritis in the acute phase of hepatitis C infection has to our knowledge never been described. our case. When a complicated infection is suspected, it is important to localize potential extraintestinal foci because drainage is usually indicated, combined with prolonged antimicrobial therapy. with an increased risk of fulminant bacterial infections, especially with encapsulated bacteria. Congenital asplenia is usually seen in the context of recognised syndromes with abnormalities in other organs, primarily cardiac abnormalities. Isolated congenital asplenia is rare. It is a condition that is difficult to diagnose in the absence of other indicators, and often diagnosed only after the patient has had a serious, often fatal infection. Morphologic anomalies of peripheral blood erythrocytes, such as Howell-Jolly Bodies, may be the only evidence of a non-functional spleen. It is not clear whether further investigation is warranted if at a routine abdominal ultrasound the spleen is not visualised. 189. Persistent shiver due to Salmonella F.J. Voogd, A. Al Moujahid, M.D. Themmen Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: fia.voogd@znb.nl 188. Arthritis and elevated liver enzymes in a patient with HIV-infection: A rare presentation of acute Hepatitis C Introduction: Many primary enteric infections are mild, selflimiting and not microbiologically diagnosed. Case: Since four days, a 27-year-old male with no medical history had a fever up to 40 °C with vomiting and diarrhoea. Two weeks before admission to our hospital he came back from a holiday in Turkey. On admission, we saw an ill patient with fever and minimal abdominal complaints without any other abnormity by physical examination. Blood analysis showed a raised C-reactive protein (171 mg/l), a normal white blood cell count and elevated liver enzymes. Blood cultures showed Salmonella oranienburg. Serological test for HIV was negative. Despite adequately given antibiotic therapy with ciprofloxacin intravenously there was persistent fever with signs of relapsing bacteremia. Computer tomography (CT) showed splenomegaly with splenic abscesses. After ultrasound-guided percutaneous drainage was performed the clinical findings quickly improved. Punctate showed Salmonella oranienburg. After treatment with ciprofloxacin during four weeks the abscesses completely resolved. Discussion: Bacteremia with splenic abscesses are serious complications of nontyphoidal Salmonella infection which may not be suspected in the setting of mild primary infection. The incidence of bacteremia is affected by Salmonella serotype, geographic location, time of year and host factors. Host risk factors include extremes of age and any immunosuppressing condition. In series of adults with nontyphoidal Salmonella bacteremia over 90 percent of patients had an underlying medical illness. Salmonella oranienburg is a foodborne pathogen and the incidence of infections seems to be low overall, but specific data are lacking. Infection is hardly complicated by abscesses and mostly comparable with a Salmonella enteritidis infection which hardly leads to bacteremia but can behave like an opportunist in patients with any immunosuppressing condition leading to infection at any site. In this case our patient was young without any predisposing comorbidities. HIV infection specifically was excluded. Conclusion: Primary enteric infections with nontyphoidal Salmonella may be mild but can have serious complications unexpectedly, even in otherwise healthy persons as in S. Slavenburg, E.H. Elzinga, R.W. ten Kate, B.L. Herpers, R. Soetekouw Kennemer Gasthuis,Department of Internal Medicine, Boerhaavelaan 22, 2035 RC HAARLEM, the Netherlands, e-mail: s.slavenburg@kg.nl Introduction: The incidence of acute hepatitis C infection (HCV) in HIV-positive men who have sex with men (MSM) has increased. Symptoms in the acute phase of HCV infection are usually mild and aspecific such as fatique, nausea, loss of apetite, flu-like symptoms or jaundice. Herein we describe a HIV-positive patient with oligoarthritis of both knees as a manifestation of acute HCV infection. Case report: The patient is a 63-year-old HIV-positive man who was successfully treated with combination antiretroviral therapy (c-ART) consisting of atazanavir/ritonavir, emtricitabine and tenofovir. The viral load was undetectable and the CD-4 count was stable around 400 x 109/l. There was no previous co-infection with hepatitis B or C. He was admitted with arthritis of both knees and was found to have abnormal liver function tests (bilirubin 72 mmol/l, AF 108 U/l, YGT 65 IU/l, ALAT 132 U/l, ASAT 130 U/l) consistent with acute HCV infection. Antibodies against HCV were negative but the HCV-RNA assay in plasma was positive (genotype 1A, viral load 4,5 x 106 cop/ ml). The rheumatoid factor was < 3.0. The anti-nucleair factor (ANF) was not measurable and anti-cyclic citrullinated peptide antibody (anti-CCP) was 2.7 kU/l. The joint radiograph showed osteoarthritis of both medial compartments. Crystals could not be identified in the synovial fluid and bacterial cultures were negative. However, HCV-RNA was demonstrable in the synovial fluid. In the course of several weeks the arthritis resolved spontaneously. Twelve weeks after presentation, HCV-RNA was still detectable in plasma and treatment with peginterferon and ribavirin was initiated. A rapid viral response was noted with undetectable HCV-RNA after 4 weeks of therapy. Discussion: Arthritis, and indeed musculoskeletal symptoms, are well known extrahepatic manifestations of chronic hepatitis C virus infection. However, a self-limiting 102 190. Fulminant pneumococcal sepsis in a patient with congenital asplenia L.N. van den Hende1, F.G.C. Heilmann 2, T. Meys1, Th.F. Veneman1 1 ZGT Hospital, Department of Internal Medicine, PO Box 7600, 7600 SZ ALMELO, the Netherlands, e-mail: L.vdHende@zgt.nl, 2Laboratorium Microbiologie Twente Achterhoek, ENSCHEDE, the Netherlands 191. Varicella zoster virus induced paraparesis – a case report Case report: A 48-year-old woman was referred to our emergency department because of flu-like symptoms since three days, with dyspnoe and fever developing in the last day. Her medical history revealed a laparoscopic cholecystectomy. On physical examination she appeared moderately ill, with a blood pressure of 130/80 mmHg, regular pulse rate of 131 BPM, body temperature of 39.2 °C, oxygen saturation 99% (3 l O2). Auscultation revealed normal breathing sounds bilaterally, without adventitious sounds. Laboratory examination revealed CRP 305 mg/l, leukocytosis 11.6 * 109/l, thrombocytopenia 90 * 109/l, serumcreatinin 200 mmol/l and lactate 13.8 mmol/l. Chest X-ray showed dubious infiltrates in both lower fields. Under suspicion of pneumosepsis, intravenous broad-spectrum antibiotics (amoxicillin/clavulanic acid and ciprofloxacin) were administered. During her stay at the emergency department her condition deteriorated rapidly. She was transferred to our ICU for mechanical ventilation and hemodynamic support. At that point she also developed reddish/purple skin lesions diffusely on her body. A CT scan of abdomen and thorax was made to rule out any other focus of infection. Again, infiltrates were seen in both lower lung fields. Surprisingly, near-complete absence of the spleen was discovered. In hindsight an abdominal ultrasound had been made a few years prior at which her spleen was not visualised. The next day blood cultures grew Streptococcus pneumonia for which Benzylpenicillin was started.. During the following period our patient developed a fulminant sepsis, with multi-organ failure. Severe thrombopenia on account of DIC, inotropydependency and renal failure with the need for dialysis developed. In blood smears Howell-Jolly Bodies were seen. Furthermore the skin lesions progressed, with necrosis of fingers and toes. She was eventually referred to a university hospital for amputation of lower legs and fingers and further treatment. Conclusion: Asplenia is an uncommon condition that may be acquired, functional or congenital. It is associated J. Branger, J. Kliffen, J. van de Vlekkert, E. Bierdrager Flevo Hospital,, Department of Internal Medicine, Hospitaalweg 1, 1315 RA ALMERE, the Netherlands, e-mail: jbranger@flevoHospital.nl Introduction: Varicella zoster virus (VZV) is the well known cause of shingles and herpes zoster infections. However, in immunocompromised patients, such as in HIV-infection, VZV can cause serious neurological disease with permanent impairment, as illustrated in the case report below. Case report: A 37-year-old male presented with progressive weakness of the right leg, numbness of the left leg, and inability to urinate. Three months earlier, he was diagnosed with toxoplasmosis encephalitis and an advanced HIV-1 infection (CD4-count 80/ml). Both infections were treated according to the current guidelines. Two weeks before admission, the patient experienced cramps and dysesthesia in his right leg. Since one week, he developed loss of strength in his right leg and urine retention. He reported no other symptoms, in particular no fever or recent skin abnormalities. On examination we saw an alert, a febrile male, hemodynamically stable. Neurological examination showed a bilaterally disrupted vital sensibility from the level Th8 downwards; gnostic sensibility was intact. Furthermore, there was loss of strength in the lower limbs, right more pronounced than left, without hyperreflexia. Babinski’s reflex was present on both lower extremities. Further physical examination was uneventful. Laboratory tests showed a mild leucopenia with 110 CD4-cells per ml. Biochemistry, including C-reactive protein was normal. A MRI scan of the spine was performed showing a diffuse myelopathy from C5 to Th12 with thickening and/or swelling of the myelum and gadolinium enhancement, suggestive of myelitis. Our differential diagnosis comprised viral (herpesviridae, HIV), 103 fungal and parasitic infections. Furthermore, syphilis and tuberculosis were considered. Finally, acute disseminated encephalo-myelitis (ADEM) was thought of. Liquor examination showed 96 mononuclear cells/ml, an elevated total protein level (1.32 g/l), and a normal glucose concentration of 2.9 mmol/l. A broad spectrum of microbiological tests was performed, showing a positive PCR and IgG antibodies for Varicella Zoster Virus in the liquor. The diagnosis incomplete spinal cord lesion caused by Varicella zoster myelitis was made. The patient was treated with acyclovir and corticosteroids, with little clinical improvement. Six months later, he is largely wheelchair dependent and uses self catheterization. Discussion and conclusion: In immunocompromised patients, reactivation of VZV often occurs. This may cause neurological sequelae including cranial nerve palsy, meningo-encephalitis and myelitis. As in our patient, herpes zoster may be absent: ‘zoster sine herpete’. Unfortunately, VZV myelitis in HIV patients is often progressive and frequently causes irreversible damage to the CNS. When suspected, treatment should be started without delay. Twelve hours later he became respiratory insufficient and was transferred to the intensive care unit, where he was intubated and mechanically ventilated, eventually in prone position. H1N1-infection was confirmed by PCR analysis, serology for HIV was negative. His renal function deteriorated, levels of CK and LDH decreased in the following 4 days and the patient is slowly recovering. Discussion: Pneumonia, complicated by rhabdomyolysis, is primarily associated with legionella or influenza infection. It was reported that 10% of the patients with influenza pneumonia suffered from rhabdomyolysis and the 2009-H1N1-serotype may even have a greater propensity for muscular inflammation than other seasonal influenza serotypes. Mild to moderate CK elevation is seen in 62% of patients with H1N1-pneumonia with respiratory failure. Mechanisms underlying its pathogenesis remain unclear and may include viral invasion, viral toxin, cytokines or hypoxemia. Conclusion: Physicians should be aware that rhabdomyolysis may present as a complication in a critically ill patient with influenza A(H1N1)-induced respiratory failure. 193. Souvenir from Indonesia: an ameboma 192. A patient with pneumonia and rhabdomyolysis M.J.T. Crobach, E.D. Beishuizen, J.W. van ’t Wout Bronovo Hospital, Department of Internal Medicine, Bronovolaan 5, 2597 AX THE HAGUE, the Netherlands, e-mail: moniquecrobach@hotmail.com A.D. Cornet, A.J. Kooter VU Medical Centre, Department of Internal Medicine, De Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: cornet@vumc.nl Introduction: Amebic infection is a rare cause of traveler’s disease. Its clinical presentation is variable. An ameboma, a mass of granulation tissue caused by localized amebic infection, is one of the unusual presentations of amebic infection. We present a patient with an ameboma after a trip to Indonesia. Case report: A 60-year-old woman was admitted with malaise, fever and pain in the right lower abdomen. These complaints started 3 days after a trip through Indonesia (Java and Bali). Past medical history included gastroesophageal reflux disease and irritable bowel syndrome. She was born in Indonesia. Before the trip, she had received all recommended vaccinations. On admission, physical examination showed a febrile patient with a tender right lower abdomen at palpation. Laboratory results and chest X-ray showed no abnormalities. Abdominal ultrasound showed an ileocecitis. A preliminary diagnosis of bacterial ileocecitis was considered and therapy with ceftriaxon IV was initiated. A tuberculin skin test was positive but was considered non-diagnostic as she was born in Indonesia. On therapy, the patient recovered quickly and was discharged some days later. Case: A 56-year-old man, without a relevant medical history, presented to the Emergency Department because of shortness of breath, dry cough and a mild fever. He used paracetamol because of myalgia and had been treated with doxycylin for 3 days prior to presentation, but his condition deteriorated. He had not traveled recently, did not smoke or have pets. None of his relatives were ill and he had not been vaccinated for seasonal flu. At presentation we saw an obese man in respiratory distress, with a respiratory rate of 38/min, cyanosis was absent using supplemental oxygen with a nonrebreathing mask. His temperature was 37.6 oC, pulse 92/min and blood pressure 125/75 mmHg. Breath sounds were bilaterally attenuated with fine crackles up until the scapula. Laboratory results showed a CRP of 106 mg/l, leukocytes 5.0 x 109/l (10% lymphocytes) and a normal renal function. Remarkable were the elevated levels of both LDH (950 U/l) and CK (3080 U/l). Blood gas analysis was as follows: pH 7.46, pCO2 37 mmHg, BE +1 mmol/l, pO2 37 mmHg (room air) and urinalysis demonstrated myoglobin. The chest X-ray showed bilateral infiltrates. Amoxicillin-clavulanic acid and erythromycin were started. The rhabdomyolysis raised the suspicion of (H1N1-)influenza pneumonia and oseltamivir was started. 104 However, after this episode, the patient presented in the outpatient clinic with persisting symptoms of right lower abdominal pain, initially accompanied with fever. CT scanning of the abdomen revealed slight inflammation around the cecum and distal ileum. A colonoscopy revealed no abnormalities, Auramine and Ziehl-Neelsen stains were negative. One month later a CT scan showed localized inflammation in the ileocecal region with accompanying lymphadenopathy, findings which might also be suggestive of an underlying tumour mass. At a second colonoscopy, there were signs of inflammation in the ileocecal region, biopsies showed amebic trophozoites. Amebic serology and amebic PCR on feces were positive. We concluded that our patient suffered from an ameboma. She was treated with metronidazol and paromomycin. On a follow-up visit four months later, she was asymptomatic. The CT scan of the abdomen showed a nearly normalized ileocecal region. Discussion: Amebic infection has a variable clinical presentation. Many conditions, including colon cancer, inflammatory bowel disease and tuberculosis, may have overlapping clinical features. Not recognizing amebic infection may have deleterious consequences, as patients may for example be treated with steroids on suspicion of inflammatory bowel disease. Given the present situation with extensive foreign travel, amebic colitis and ameboma must be included in the differential diagnosis of all patients who present with colitis or a colonic mass after travelling to the developing world. and rifampicin. Patient started treatment with isoniazid, rifampicine and moxifloxacin. In retrospect the abdominal aneurysm, for which an EVAR was perfomed in 2009, had shown some signs of a mycotic aneurysm. This diagnosis was rejected because of the absense of fever and inflammatory parameters The psoas abcess was drained twice but recurred. Therefore it was decided to replace the EVAR for a graft of the great saphenous vein. Up until now patient is doing well. He has to continue tuberculostatics for six months after surgery. A recent MRI showed no signs of activity in the spine In international literature there are about 16 reported cases of mycotic aneurysms due to M. bovis and several cases of spondylodiscitis after BCG-immunotherapy. The route of infection in our patient is most likely haemotogenous because the localisation in the spine is not related to the psoas abces and the aorta. This case shows that in doubt of a mycotic aneurysm or in case of an unexpected osteoporosis in a patient with previous BCG installation a low grade chronic infection like M. bovis must be suspected. 195. A healthy female with Rhodococcus erythropolis septicemia J.M. van Hattem, S.A. Luykx-de Bakker, S. Lobatto Tergooi Hospitals Hilversum, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: jarne.vanhattem@gmail.com 194. Spondylodiscitis and a mycotic aneurysm: complications of intravesical BCG (bacillus Calmette-Guérin)-immunotherapy Case: A 46-year-old female with a history of an appendectomy presented with stabbing pain in the left lower abdomen of 2 weeks duration and fever (temperature 39.9 °C) since one day. An IUD for birth control was placed 6 years before. On physical examination a non-ill woman, with a painful left lower abdominal quadrant without rebound tenderness was seen. Laboratory examination showed an elevated CRP (70 mg/l, a day later 146 mg/l) and elevated leukocytes (13.4 x 109/l, a day later 16.6 x 109/l). Ultrasound showed a mass in the left lower abdomen, possibly infiltrated fat tissue with abscesses. A CT-scan was performed showing a para-iliac mass with a diameter of 5 cm with central calcification, most likely an ovarian abscess. She was initially treated with oral amoxicillin/clavulanic acid on an out-patient basis but was readmitted the next day because of fever. Transvaginal drainage of the ovarian abscess was performed and her IUD was removed. Blood cultures identified a Rhodococcus species, further determined by matrix assisted laser desorption/ionisation (MALDI) as Rhodococcus erythropolis, penicillin sensitive and trimethoprim-sulfamethoxazole resistant. Genital swab cultures, PCR for Chlamydia trachomatis and B. Santbergen, M.E.E. van Kasteren, P.H.W.E. Vriens St. Elisabeth Hospital, Department of Internal Medicine, Hilvarenbeekseweg 60, 5022 GC TILBURG, the Netherlands, e-mail: bart_santbergen@hotmail.com We report a case of a 58-year-old man with persisting back pain after a vertebroplasty of vertebra Th8-Th9 because of osteoporosis. Previous medical history included intravesical BCG-immunotherapy 3 years earlier for minimal invasive bladder carcinoma and an EVAR for an abdominal aneurysm 1 year earlier. Last months patient complained of weight loss. A new MRI of the spine showed signs of a low-grade spondylodiscitis at Th8-Th9 and a CT-guided bone puncture was performed. Pathological analysis showed necrotizing granuloma and microbiological cultures grew Mycobacterium bovis. CT abdomen showed a swelling around the EVAR and an abscess of the left psoas muscle. A puncture of the psoas abscess also showed acid fast bacilli and PCR for Mycobacterium complex was positive. Culture grew M. bovis sensitive to isoniazid 105 Neisseria gonorrhoeae as well as culture of puss from the abscess were all negative. The patient was treated with penicillin intravenously and could be discharged after a week. Rhodococcus is a gram-positive pleomorphic organism that appears coccoid on solid media but forms long rods or short filaments in liquid media. The organism is an occasional cause of disease in cattle and can cause severe lung infections in foals. Most human infections have been associated with immune system dysfunction. Pulmonary infections are the most common form of human disease. Little is known about the pathogenic potential of Rhodococci other than R. equi. We found two case reports of R. erythropolis septicemia: a 79-year-old man with esophageal cancer who had been treated with radiotherapy followed by chemotherapy and a 7-year-old child treated with chemotherapy for acute lymphocytic leukemia. We know that colonization and pelvic infections with Actinomyces are associated with IUD use, especially prolonged IUD use. We could not find any literature about the association between Rhodococcus and IUD use. Conclusion: This is the third case report of Rhodococcus erythropolis septicemia and the first in an immunocompetent woman. It has been suggested that non-equi Rhodococcus species may be of more importance in human disease than previously thought. An association between Rhodoccus infection and prolonged IUD use is very well possible. above described skinlesions on the body and a conjunctivitis. He was hemodynamically stable, had a normal temperature and a oxygen saturation of 95% with 5 liter O2. On chest examination there were crackles at the right lung base. Laboratory results showed elevated CRP 125 (< 10 mg/l) and a mild leukocyte count of 12.2 (< 10 x 109/l). Chest X-ray showed a para-cardial infiltrate. With the suspicion of a Stevens-Johnson Syndrome triggered by a pneumonia, ciprofloxacin was started, amoxicilin was continued without clavulanic acid and aciclovir was added to cover a possible herpes simplex co-infection. Initially he became septic en developed high temperature. After a few days he recovered clinically and the skin lesions resolved. Blood cultures were negative, urine analysis for Legionella pneumophila was negative, HIV serology was negative but sputum culture and serology were positive for M. pneumoniae. Antibiotics were switched to oral clarithromycin. Histologic findings of the skin appeared evident for a Stevens Johnson syndrome. The patient recovered quickly. Laboratory findings and chest X-ray normalized after a couple of weeks. Conclusion: One should keep in mind that when a patient presents with symptoms suspected for a Stevens Johnsons Syndrome, serology for M. pneumoniae should be obtained. If there are respiratory symptoms, appropriate antibiotics should be started covering M. pneumoniae prior to any test results. of an ischaemic cerebral infarction. His medical history further comprised multiple airway infections, a myocardial infarction and an endovascular reconstruction for an asymptomatic aortic aneurysm. His cardiovascular risk factors included smoking, dyslipidemia, age and a positive family history. Despite of risk factor reduction, the patient experienced a series of strokes in the three years after his first stroke, leaving him severely disabled. No other causes for these recurrent events were found. During follow-up at the internal medicine department the patient complained of malaise and nightsweats without fever. Several blood tests showed abnormalities: a slow rise of the ESR to 97 mm/h and a slowly developing anaemia of chronic disease (Hb 7.0 mmol/l). Also, levels of all IgG subclasses were now raised, as well as the IgA and IgM levels (previously normal). Based on the clinical presentation and the labarotory tests a non-athesclerotic endovasculitis was suspected. Serologic analysis showed high phase 1 and phase 2 IgG and IgM antibody titers to C. Burnetii (1:16000). At last, the patients clinical condition could be explained by chronic Q-fever infection, which was confirmed by high antibody titers and biochemical signs of chronic infection. Echocardiography showed no abnormalities, the patients condition improved after treatment with doxycycline and hydroxychloroquine. Conclusion: 1. In this patient the diagnosis of chronic Q-fever infection was delayed, due to the misrecognition of the infectious cause of the vascular complications and the lack of symptoms accompanying the acute phase of the infection. 2. Possibly, the dysfunction of the cellular immunity contributed to sustained infection. 3. In patients with multiple vascular events and chronically increased inflammatory parameters, a chronic bacterial infection should be suspected as a cause. encephalitis for which intravenous acyclovir was started. Computed tomography of the brain showed asymmetric edema mainly in the left temporal lobe. Cerebrospinal fluid (CSF) analysis showed lymphocytosis (1540 cells per ul), elevated protein (1.72 g/l) and a normal glucose concentration (2.8 mmol/l). Polymerase chain reaction (PCR) of CSF revealed herpes simplex virus type 1 (HSV-1). The patient recovered quickly and was discharged home ten days later. The non-fluent aphasia did not resolve completely for which she received speech therapy. Discussion: Herpes simplex encephalitis (HSE) is the most common cause of sporadic viral encephalitis. It usually affects the temporal and frontal lobes. In most cases HSV-1 is responsible for the disease, herpes simplex type 2 virus (HSV-2) is involved in 4-6% of cases. Characteristically, patients have behavioral changes, fever, confusion, speech disturbances and, less frequently, seizures. MRI of the brain is the preferred imaging study and may show changes in the temporal and/or frontal lobe. Polymerase chain reaction (PCR) of the CSF is the diagnostic method of choice. Mortality rates reach 70% in the absence of therapy and only a minority of individuals return to normal function. Conclusion: Herpes encephalitis must be suspected in case of fever, confusion and focal neurological deficit. In this patient the key to the diagnosis lay in recognizing the reported ‘confusion’ as aphasia. Plasma leukocytosis and raised CRP, common signs of infection, were conspicuously absent. 197. A patient with herpes encephalitis 196. Rare presentation of a very common pneumonia L.J.N. Wind, M. Ghiti, D.Q. Ngo, M.J.M. Diekman Deventer Hospital, Departement of Internal Medicine, Nico Bolkesteinlaan 75, 7416 SE DEVENTER, the Netherlands, e-mail: LJNWind@hotmail.com M.I. Ilik ZGT Hospital, location Almelo, Department of Internal Medicine, Zilvermeeuw 1, 7609 PP ALMELO, the Netherlands, e-mail: m.ilik@zgt.nl 198. Late recognition of chronic Q-fever in an immunodeficient patient with multiple vascular complications M.C. Buis1, G.J. Kootstra1, R. Klont2, Chr.H.H. ten Napel1 Medical Spectrum Twente, Department of Internal Medicine, Ariënsplein 1, 7511 JX ENSCHEDE, the Netherlands, e-mail: m.buis@mst.nl, 2Laboratorium Microbiologie Twente en Achterhoek, ENSCHEDE, the Netherlands 1 Case report: A 58-year-old previously healthy women, presented with fever, chills and vomiting since five days. She had headaches, muscle pain and her family members reported ‘confusion’ since two days. She used no alcohol or illicit substances. On physical examination she had fever of 38.9 °C, blood pressure of 126/68 mmHg and a pulse of 73 bpm. Further physical examination was unremarkable. On neurological examination she was cooperative. She seemed to respond adequately but was not fully oriented with respect to time and place. There were no further neurological signs. Laboratory analysis showed normal C reactive protein (CRP), leukocyte count and leukocyte differential. Apart from a normocytic anemia (Hb 7.1 mmol/l) and mild hyponatremia (133 mmol/l) electrolytes, glucose, liver enzymes and renal function were normal as were urine analysis and a chest X ray. The consulted neurologist recognized the disorder in comprehension as a sign of non-fluent aphasia and diagnosed clinically herpes Introduction: Pneumonia due to Mycoplasma pneumoniae are frequently found in young adults. Our patient had a very rare presentation of a M. pneumoniae! Case report: A 19-year-old male with no relevant medical history presented with a nine days history of malaise, cold chills, nausea and since three days diarrhea and dyspnoea. Six days after his initial symptoms of cold chills and nausea he developed blisters and erosions on his lips and oral mucosa. He also developed erythematous and purpuric macules with vesicles and bullae, which started on his palms and symmetrically spread to the rest of the body. His general physician had started with amoxicillin/ clavulanic acid orally two days before presentation. Despite antibiotics the patients developed purulent coughing and became more dyspnoeic. He had not used any medication prior to his illness, worked as a gardener and had not been bitten by insects, nor had he been abroad recently. Physical examination showed the 106 199. A young healthy man with repeated episodes of pericarditis Introduction: Q-fever, a zoonosis caused bij Coxiella burnetii, is a disease with a high morbidity but low mortality. While acute Q-fever often presents with mild non-specific symptoms and is a self-limiting condition, the infection can become chronic and -when untreated- cause endovasculitis with major vascular complications. Due to lack of specific symptoms the diagnosis remains a clinical challenge. We would like to present the case of an immunodeficient patient with a complicated chronic Q-fever infection, which was only recognised after multiple vascular events. Case report: A 78-year-old male, with a medical history of chronic oesophageal candidiasis after which he was diagnosed with T-cell dysfunction in vitro, mannosebinding lectine deficiency en IgG-subclass deficiency (low IgG1 and IgG3), was admitted to the hospital because A.M.T. Huijben, S.J. van den Boogerd, J.M.G.H. van Riel St. Elisabeth Hospital, Department of Internal Medicine, Tilburg, the Netherlands, e-mail: aukehuijben@hotmail.com Case: A 36-year-old non-smoking and previously healthy male presented at the Emergency Room with fever, dyspnoea and malaise. Psychical examination showed fever (38.8 °C) and tachypnea. Laboratory investigation showed an inflammatory response with elevated CRP and leukocytes, and slightly elevated liver enzymes. Urine analysis was normal. Chest-X-ray and abdominal ultrasound at presentation were normal. Treatment was started with amoxicillin and tobramycin with the suspicion of fever with pulmonal or abdominal origin. 107 After 48 hours antibiotics fever persisted and patient became oxygen dependent. As a consequence a CT-A was performed showing bilateral pneumonia with atelectasis and no lung embolism. Coincidental a pericardial cyst was seen, suggested congenital. Electrocardiogram showed atypical depolarization and heart enzymes were elevated. With the suspicion of an acute coronary syndrome patient was transmitted to the CCU. Echocardiography was normal at that moment. Next day on cardiac examination pericardial rub was heard and the diagnosis of pericarditis secondary to pneumonia was hypothesized. Treatment with high dose acetylsalicylic acid was started with initial improvement. After seven days of decreasing inflammatory markers and absence of fever, antibiotics were discontinued. Meanwhile microbiological analysis did not show pathogens and there was no evidence for autoimmune disease. However, patient’s clinical situation worsened and he developed thoracic pain. Repeated CT showed pericardial effusion without signs of tamponade. Since patient was hemodymanic stable, a pericardial punction was not performed. One week later pericardium effusion progressed and patient became hemodynamic instable with clinical signs of a tamponade like pulsus paradoxus, hypotension and elevated CVP. Patient underwent chirurgical intervention with drainage of 800 cc haemorrhagic fluid. Microbiological analysis of the pericardium fluid and all the blood cultivates did not show any bacterial or viral agent. After all this, patient developed again a pneumonia, which was treated with ciproxin, and also a pericarditis, confirmed with CT, and colchicine was added to the acetylsalicylic acid. The pericardium cyst, described as congenital before, was not seen at this CT. Discussion: Acute pericarditis is a common, not always primary mentioned, disorder in several clinical settings. Our patient had relapsing pericarditis due to a presumed viral pneumonia. This case shows how pericarditis can cause life-threatening clinical condition, even in a young man without co-morbidity. However, retrospective we can also hypothesize that there was an infected pericardial cyst which is also described in literature. resistance) is generally regarded to have a favorable safety profile. We report on two cases of severe cutaneous adverse reactions following repeated exposure to this widely used drug. To the best of our knowledge, Stevens-Johnson syndrome (SJS) has now been reported as an adverse reaction to proguanil – atovaquone in three published cases. Our patients (1 M, 1 F) - both healthy subjects with no known history of apparent drug allergy had been exposed to proguanil-atovaquone before. One of them on more than ten occasions. Both patients were severely ill with generalized involvement of skin and mucosal membranes. Following withdrawal of all possibly offending drugs treatment with steroids was initiated. Cutaneous adverse events are frequent following the use of pharmaceutical agents. The majority are caused by NSAIDs, anticonvulsants, and antimicrobials. SJS typically affects 10% of the skin surface, but dermal detachment may progress and overlap with the more severe and extensive form of the disease, toxic epidermal necrolysis (TEN). The incidence of SJS is 1-2 cases per million population per year with a low mortality rate. In TEN it raises upto 15%-75%. SJS is characterized an erythematous rash with macules, and, occasionally, vesicles and bullae that may coalesce and erode and mucous membrane lesions that involve the oral cavity, anogenital regions, and conjunctivae. SJS can be confused with erythema exudativum multiforme (EEM) but EEM is typically limited to the extensor surfaces of the extremities and the mucosal epithelium. Our patients developed their symptoms while still on the drug with first appearance on the palate, gums and trunk region. In the next 72 hours erythematous macules on the trunk, proximal extremities and erosions in the genital region appeared. Prednisone (60 mg) was started and virtually no new lesions developed since. The diagnosis of SJS was supported by the histopathological findings. As single agents both proguanil and atovaquone have been rarely reported to provoke skin rashes with JSJ mainly caused by atovaquone. We conclude that proguanil – atovaquone were the causative agents of SJS in our patients. There have been no relapses or persisting complaints. Obviously (re)challenge is thought to be unethical. This report should alert physicians to add proguanil – atovaquone to the list of drugs that can cause SJS. 200. SCAR ‘severe cutaneous adverse reactions’ following the use of proguanil-atovaquone (Malarone®) malaria prophylaxis P.J. Wismans, M. van Kats, D. Overbosch, P.J.J. van Genderen Haven Hospital and Institute for Tropical Diseases, Department of Internal Medicine, Haringvliet 2, 3011 TD ROTTERDAM, the Netherlands, e-mail: pjwismans@planet.nl 201. Neuroschistosomiasis C.R. Boeddha1, M. van Wolfswinkel1, J.J. van Hellemond2, S. Rosso1, P.J.J. van Genderen1, P.J. Wismans1 The highly effective combination proguanil – atovaquone to prevent malaria (even in areas of high level chloroquine 108 1 XVII.NEPHROLOGY RESEARCH Haven Hospital and Institute for Tropical Diseases, Department of Internal Medicine, Haringvliet 2, 3011 TD ROTTERDAM, the Netherlands, e-mail: c_boeddha888@hotmail.com, 2Erasmus Medical Centre, ROTTERDAM, the Netherlands 202. Improving medication safety in patients with renal impairment; enhancing collaboration between pharmacists and physicians Introduction: Schistosomiasis (Bilharzia) is a parasitic disease, caused by infection with a trematode of the Schistosoma species. S. haematobium, S mansoni and S. Japonicum are the most important pathogens. Humans are infected by penetration of the skin by larval schistosomes in snail infested water in specific regions. Chronic disease occurs when adult worm pairs produce eggs, evoking an inflammatory response. Neuroschistosomiasis is rare complication, caused by migration of schistosoma eggs to the central nervous system. We describe a case of neuroschistosomiasis that was recently seen in our hospital Case report: A 41-year-old man with a history of hepatitis, malaria and schistosomiasis, for which he was treated adequately in 2006, presented with chest pain and a numbed feeling of his abdomen en legs for the past 3 weeks. He also reported muscle weakness and urinary hesitancy. From 1985-1990 he had worked in Liberia and since 1990 he lived in Guinea. His vital signs were normal. Neurological examination showed a decreased sensibility from level Th 2 and the abdominal reflex was absent. Decreased muscular strength of the legs and bilateral Babinski’s sign were found. Magnetic resonance imaging showed a transverse myelitis involving C4-Th7. Laboratory results showed eosinophilia but were otherwise unremarkable. A lumbar puncture was not be performed in view of the swelling of the myeloma. HIV screening was negative. Stool microscopy revealed living S. Mansoni eggs. Schistosoma serology titers had increased. A diagnosis of neuroschistosomiasis was made and the patient was started on praziquantel 60 mg/kg for 3 days and prednisone 60 mg once daily. He soon noted improvement of the neurological symptoms and made a virtually complete recovery. After one month, repeated MRI scanning showed normalisation of the abnormalities and a lumbar puncture was performed which revealed positive schistosoma serology, confirming the diagnosis. Discussion: This patient presented with neurological symptoms while suffering from schistosomiasis. A detailed travel history is of utmost importance. To locate the patients signs an accurate physical examination is required. Other infectious causes such as TB, HIV, neurocysticercose etc. need to be excluded. An accurate approach is needed to prevent persisting neurological damage. Conclusion: The diagnosis of schistosomiasis should be considered in any traveller from an endemic area with a history of exposure to surface water. Eosinophilia, schistosomiasias serology and parasitological examination in stools and urine supports the diagnosis. Praziquantel is the drug treatment of choice. J.M.H. Joosten1, I. Drion2, C.J. Boogerd3, E. van der Pijl3, R.J. Slingerland 4, T.J. Jansen5, O. Schwantje5, J.P.J. Slaets6, R.O.B. Gans7, H.J.G. Bilo2 1 Universitary Medical Centre Groningen, Department of Internal Medicine, Hanzeplein 1, 9700 RB GRONINGEN, the Netherlands, e-mail: j.m.h.joosten@int.umcg.nl, 2Diabetes Centre, Isala Clinics, ZWOLLE, the Netherlands, 3Pharmacy Boogerd-Kluin, ZWOLLE, the Netherlands, 4Isala Clinics, ZWOLLE, the Netherlands, 5General Practitioner, ZWOLLE, the Netherlands, 6Deparment of Geriatric Medicine, University Medical Centre Groningen, GRONINGEN, the Netherlands, 7 Department of Internal Medicine, University Medical Centre Groningen, GRONINGEN, the Netherlands Introduction: Guidelines stress the importance of monitoring prescriptions to prevent adverse drug events (ADEs), especially in patients with polypharmacy or comorbidities like CKD. The Dutch HARM-study estimated an incidence of 41.000 medication-related admissions in the Netherlands (of which 19.000 possibly preventable). Renal failure appeared an important risk factor, but is often not recognized. More effective use of routinely collected data from electronic patient records (like eGFR) was suggested to improve medication monitoring. Aim: To address medication errors from a preventive perspective by linking laboratory data on eGFR to pharmacy records and by introducing medication alerts for renal impairment. Materials and methods: Prospective intervention study conducted between February 2009 and January 2010 in Zwolle. All community pharmacies (n=11) and GP practices (n=24) in Zwolle participated. The regional laboratory consecutively reported all (newly) identified adults with an eGFR =40 ml/min/1.73 m2 towards participating pharmacies. Community pharmacists checked the patients’ actual drug regimen on current contra-indications with regard to eGFR and, if necessary, proposed an intervention in the drug regimen towards the prescribing physician. Subsequently a low-eGFR-alert was activated at the pharmacy record to warn for low eGFR in future presciptions. Besides patients’ characteristics, all proposed interventions, potential ADEs and ADEs were recorded. Results: During the study period 1368 subjects with an eGFR 40 ml/min/1.73m2 were identified. Median [IQR] age was 78 years and median [IQR] eGFR 34 ml/min/1.73 m2. Polypharmacy was present in 73% (n=993); the mean 109 number of drugs was 7 (range 0-21). Overall, 342 drug errors triggered an intervention in 211 subjects (15%); this mainly concerning diuretics (22%), antibiotics (21%) and anti-gout therapy (15%). Subjects needing an intervention had a significantly lower eGFR (median [IQR] 34 versus 29 ml/min/1.73 m2, p<0.001) and a higher polypharmacy rate (89 versus 70%, p<0.001) versus those without. Overall, 88% (n=300) of all drug errors were regarded as potential ADEs. These potential ADEs were mainly judged as significant or serious. Physicians complied with 67% of the proposed interventions. In 21 cases an ADE occurred after not implementing the proposed intervention. Conclusion: After introducing low-eGFR-alerts in pharmacies, intensified collaboration between community pharmacists and physicians resulted in 229 drug adjustments aiming to improve drug safety. Extending the availability of renal function data revealed that 1.2% of our city inhabitants is at risk for ADEs due to renal impairment. Awareness of this risk factor is especially relevant in elderly and subjects with polypharmacy. 136.9(2.0) and 137.3(1.7), NaISE 135.9(3.0), 135.4(1.9) and 135.3(1.7), KF 4.8(0.7), 3.9(0.4) and 3.7(0.3), KDSE 4.7(0.7), 3.9(0.5) and 3.6(0.3), KISE 4.7(0.7), 3.9(0.5) and 3.6(0.3) mmol/l respectively. NaC was lower after HD and was always higher than NaF, NaDSE or NaISE. NaF was stable during HD. NaF was always higher than NaISE but than NaDSE only after HD. NaDSE was stable during HD and always higher than NaISE. NaISE was stable during HD. K declined during HD. KF was always higher than KISE and KDSE. KDSE was slightly higher than KISE after HD. NaC before HD was best explained (r2=0.72) by NaDSE, KDSE, TP and TG. Conclusion: NaC is strongly affected by HD. An increasing difference between NaDSE and NaISE suggests at least a change in PW during HD. It is unknown whether changes in other ions beside Na and K are relevant for NaC since they were not measured. NaC is higher than NaDSE and NaISE at any moment. This may be relevant to HD practice. NaF and KF are structurally higher then Na- and KDSE and -ISE. This can be explained by the fact that flame photometry measures total Na and K whereas DSE and ISE measure active Na and K. 203. Differences between methods for determining [na+] and [k+] in hemodialysis patients at different times during dialysis 204. Vitamin D levels in a cohort of patients on hemodialysis A.L.H.J. Aarnoudse, J.A. Riedl, G.M.T. de Jong Albert Schweitzer Hospital, Department of Internal Medicine, PO Box 444, 3300 AK DORDRECHT, the Netherlands, e-mail: a.j.aarnoudse@asz.nl E.R. van de Wal-Visscher, H. Bogers, B. Bravenboer, C.J.A.M. Konings Catharina Hospital Eindhoven, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: e.vandewal@alumni.maastrichtuniversity.nl Introduction: Na and K can be measured with a flame photometer (NaF, KF), direct ion-selective electrode (NaDSE, KDSE) and indirect ion-selective electrode (NaISE, KISE). Na represents the majority of electrolytes in blood. This enables the AK200 ULTRA S (Gambro) dialysis machine to derive a Na-concentration from the conductivity of blood (NaC). Hemodialysis (HD) may change plasma water (PW) as well as it does plasma Na and K. The different methods are differently affected by these changes. Aim: To compare the different methods for measuring NA and K during dialysis. Methods: In 45 HD-patients (M/F 28/27) blood was drawn and NaC was registered before, halfway and after a HD-session. Blood was analyzed for Na, K, hematocrit, total protein (TP), albumin, cholesterol, triglycerides (TG) and urea. Mean Na and K were compared between methods and between sampling times using paired tests. A backward stepwise linear regression model was used to explain NaC from NaF, NaDSE, NaISE and measured variables. All statistics were performed using SPSS for Windows. Results: Mean(SD) concentrations at start, during and after HD were for NaC 141.2(2.6), 140.2(1.8), and 139.4(1.3), NaF 136.6(2.6), 136.8(1.7) and 136.2(1.7), NaDSE 136.9(2.8), Introduction: Vitamin D deficiency in hemodialysis patients is associated with a higher incidence of cardiovascular diseases, metabolic abnormalities and mortality. Vitamin D deficiency has been linked to various problems next to renal osteodystrophy, an alteration of bone morphology, and as such it has been ignored as a source of morbidity in the western world. Aim: The purpose of this study is to identify vitamin D deficiency in a large cohort of patients on hemodialysis in one dialysis Centre, Catharina-hospital Eindhoven. Patients and methods: Levels of 25 (OH)-vitamin D3, Ca, PO4 and PTH were measured in 81 hemodialysis patients in the Catharina-hospital Eindhoven, the Netherlands in 2008. All patients received standard state of the art counselling by qualified dieticians. Results: The patients were tested in winter. The mean vitamin D3 in 81 patients was 23.4 nmol/l +/- 13.2 nmol/l. 80 Patients (98.8%) had a level of vitamin D (25-hydroxyvitamin-D levels) below 75 nmol/l. Only one patient had a normal vitamin D level. The mean calcium level 110 was 2.3 mmol/l +/- 0.2 mmol/l, mean PO4 level was 1.6 mmol/l, +/- 0.4 mmol/l. Calcium levels were higher than 2.54 mmol/l in 10 patients (13%) and 38 patients (46.9%) had a phosphate level between 1.13-1.78 mmol/l. The mean PTH concentration was 30.3 pmol/l, +/- 22.3 pmol/l. 40 Patients (49.4%) had a PTH level in the normal range. Conclusions: There is a very high prevalence of vitamin D3 deficiency in hemodialysis patients. It is necessary to screen on vitamin D3 dialysis patients and review standard dietary care of dialysis patients and supply deficits to avoid vitamin D3 deficiency and subsequent morbidity and possible mortality. Further research must indicate whether suppletion should lead to a lower mortality and morbidity in dialysis patients. result of ACE-inhibition, we concluded that the most likely diagnosis was a stenosis in the remaining renal artery. A CT-angiography showed a 98% renal artery stenosis, due to five misplaced surgical clips. The cortex of the kidney was still enhanced by contrast. Two months after the initial nefrectomy, an uncomplicated hepato-renal bypass was created. Diuresis started immediately after surgery. Three weeks later the blood pressure had normalized, urinary production was more than 2 liters/24 hrs and the creatinine had stabilized on 197 mmol/l (2.2 mg/dl) (MDRD clearance 23 ml/min). To our knowledge, there has never been a report of a successful renal revascularization procedure after two months of reduced blood flow. It is known from abdominal aortic surgery and kidney transplantation that the maximum time the kidney can be deprived of blood is fifty minutes. However, in this case report, occlusion of the blood flow was incomplete, which resulted in revivability of the kidney two months after reduction of the blood flow. In conclusion we describe a patient with an iatrogenic, incomplete renal artery stenosis, where a successful revascularization procedure was performed two months after the initial event. XVIII. NEPHROLOGY CASE REPORTS 205. A different kind of stenosis K.J. Woittiez, M. van Buren HAGA Hospital, Department of Internal Medicine/ Nephrology, Leyweg 275, 2545 CH THE HAGUE, the Netherlands, e-mail: kwoittiez@hotmail.com 206. Primary focal and segmental glomerulosclerosis successfully treated with immunosuppression and plasmapheresis A 54-year-old woman complained of back pain and weight loss. A CT-scan revealed a mass in the left kidney, suggestive of renal cell cancer with pulmonary and bone metastases. She was immediately referred to the urologist for a palliative nephrectomy. Pre-operatively our patient had an excellent renal function, with a creatinine of 53 mmol/l (clearance MDRD 104 ml/min). Surgery was complicated by hypotensive episodes due to an estimated blood loss of 18 liters. To compensate, our patient received multiple transfusions with washed erythrocytes, fresh frozen plasma and voluven®. After the operation, the patient produced no urine. An ultrasound of the remaining kidney showed no signs of hydronephrosis. It was concluded that the patient most likely suffered from acute tubular necrosis, due to low blood pressure during surgery, in combination with possible nefrotoxicity due to the large amount of infused voluven®. After four days, hemodialysis became necessary. Several days later, the patient developed hypertension and blurred vision. The ophthalmologist diagnosed hypertensive retinopathy grade 3. Calcium antagonist and efforts to raise the ultrafiltration rate during dialysis were unsuccessful. Eventually, ACE-inhibition was started, which resulted in lowering of the blood pressure. After adding up the acute anuric kidney failure after nephrectomy, the symptomatic hypertension and the good D.A. Geerse1, C.J.A.M. Konings1, J.F.M. Wetzels2 1 Catharina Hospital, Department of Internal Medicine, Michelangelollaan 2, 5623 ER EINDHOVEN, the Netherlands, e-mail: dgeerse@hotmail.com, 2Radboud University Medical Centrum, NIJMEGEN, the Netherlands Introduction: primary focal and segmental glomerulosclerosis (FSGS) is a frequent cause of the nephrotic syndrome in adults and is usually treated with immunosuppressive drugs. Plasmapheresis is generally reserved for recurrence of FSGS in renal transplants. Case report: A 40-year-old man was admitted with severe ischemic ulcers of both legs. He had peripheral arterial disease with no surgical options for revascularization and was diagnosed with nephrotic syndrome a year earlier. Renal biopsy was compatible with FSGS and high dose prednisolon was started. Three months before his hospital admission he was admitted for exacerbation of nephrotic syndrome due to bad treatment compliance. Treatment with prednisolone (60 mg daily) was resumed. The patient had ischemic ulcers on both legs with digital necrosis. Amputation of the left lower leg was performed several days later. Two weeks later, he developed a lung abscess in the right upper lobe, multiple liver abscesses and an acalculous cholecystitis. Cultures were drawn 111 and treatment was started with cefuroxim, metronidazol and gentamycin. The prednisolone dose was decreased. Subsequently, his nephrotic syndrome exacerbated and he developed acute renal failure, for which hemodialysis was started. He developed respiratory insufficiency and was transferred to the Intensive Care Unit. A bronchoalveolar lavage (BAL) fluid was obtained for culture. All cultures remained negative. A sputum culture drawn three weeks earlier showed aspergillus fumigatus. Echocardiography showed no vegetations. There were no signs of osteomyelitis on X-ray. The patient was transferred to a tertiary care hospital one day after starting hemodialysis. Another renal biopsy was performed to evaluate disease reversibility; active FSGS was found without scarring. High dose prednisolone was resumed, resulting in sufficient improvement to stop hemodialysis. There was still massive proteinuria though, requiring additional treatment. Because of the lung abscess, no cyclophosphamide was given. Instead, plasmapheresis was started, resulting in a significant improvement of proteinuria. Meanwhile, his lung abscess progressed to a cavitating lesion with characteristics of an aspergilloma. Ultimately, a lobectomy was performed. Pathologic examination confirmed an aspergilloma. Postoperatively, the patient remained in partial remission, with stable proteinuria. In attempt to obtain complete remission, tacrolimus and ciclosporin were given, but both were discontinued because of gastrointestinal sideeffects. Two years afterwards though, complete remission was achieved, and the prednisolone dose was gradually lowered. He is currently taking 5 mg daily, with proteinuria of 140 mg/day. Conclusions: We strongly suspect that plasmapheresis had an important role in inducing remission of primary FSGS in our patient. in improving outcome of transplantation. Meta-analyses have demonstrated superior effectiveness of bariatric surgery when compared with conventional therapy in achieving sustained weight loss in obese patients. Yet, further analysis shows higher postoperative mortality rates after bariatric surgery in patients with renal failure than in the general population. Aim: To assess the feasibility of bariatric surgery prior to renal transplantation in patients with ESRD. Materials and methods: We report 2 female patients (patient 1: age 28; patient 2: age 65), initially rejected for renal transplantation because of morbid obesity, who underwent a laparoscopic bariatric procedure followed by kidney transplantation. Both patients had hypertension, patient 1 suffered from insulin-dependent diabetes mellitus and hypercholesterolemia, patient 2 suffered from severe tapetoretinal degeneration. Patient 1 had diffuse glomerulosclerosis, probably caused by hypertension, as cause of ESRD and patient 2 had diabetic nephropathy. Results: Laparoscopic gastric banding was performed in patient 1 in 2008, 20 months prior to kidney transplantation, patient 2 underwent laparoscopic sleeve gastrectomy in 2009, 7 months prior to kidney transplantation. BMI values decreased from 46 to 36 kg/m2 in patient 1 and from 41 to 31 kg/m2 in patient 2 after bariatric surgery prior to transplantation. Complications developed in patient 2: after the sleeve gastrectomy, the patient developed respiratory failure probably based on opiate intoxication, and was treated in the ICU for 14 days. However, both patients recovered well and mean total weight loss was 22%. Subsequently, live donor kidney transplantation was performed successfully in both patients. Conclusions: Laparoscopic bariatric surgery is a viable treatment option in morbidly obese patients with ESRD to achieve sufficient weight loss prior to successful renal transplantation. Larger prospective studies are necessary to further investigate the potential risks and benefits of bariatric surgery in patients with ESRD. 207. The feasibility of bariatric surgery prior to kidney transplantation in two morbidly obese patients with ESRD Introduction: Preclinical studies have shown that the endogenous nucleoside adenosine is able to modulate inflammation and to prevent associated organ injury. Dipyridamole, an adenosine reuptake inhibitor, increases extracellular adenosine concentrations during unfavourable conditions, e.g. inflammation, and as such may attenuate the inflammatory response and subsequent organ injury. Aim: To examine the effects of oral dipyridamole treatment on innate immunity and organ injury during human experimental endotoxemia. Material and methods: In a randomized double-blind placebo-controlled study, 20 healthy male subjects received 2 ng/kg E. Coli endotoxin intravenously following seven day pretreatment with dipyridamole, 200 mg retard twice daily, or placebo. Results: Nucleoside transporter activity was significantly reduced by dipyridamole with 89±2% (p<0.0001), which resulted in significantly augmented endogenous adenosine levels at the start of the experiment. Experimental endotoxemia induced flu-like symptoms and increased concentrations of circulating cytokines. Dipyridamole concentrations correlated with the peak adenosine concentration, 2 hours after LPS administration (r=0.82, p=0.0038). Moreover, this dipyridamole-induced increase in adenosine concentrations resulted in an enhanced IL-10 response (r=0.82; p=0.0035). IL-10 peak concentrations correlated with a more pronounced decline in TNF-a (Pearson r=0.54, p=0.018), a phenomenon known as negative feedback. Furthermore, dipyridamole treatment resulted in less endotoxin-induced circulating plasma markers of endothelial activation; intercellular adhesion molecule (ICAM) and vascular cell adhesion molecule (VCAM) (p=0.07 and p=0.018), and partial recovery of vascular sensitivity to norepinephrine. No effect of dipyridamole on the endotoxin-induced increased urinary excretion of markers of renal tubular damage, nor on oxidative stress was observed. Conclusions: Dipyridamole treatment augments the antiinflammatory response associated with a faster decline in TNF-a, during human experimental endotoxemia. These actions of dipyridamole are mediated by increased adenosine concentrations. Dipyridamole did not affect LPS-induced end-organ damage. our dialysis unit with renal failure. There was no evidence of a pre- or post-renal cause, but ultrasound imaging did show a large mass involving the right kidney. Dialysis was commenced but was not tolerated due to severe hypotension 30 minutes after starting a dialysis session. Further history, physical examination and initial laboratory studies did not reveal a clear cause of the renal failure or the dialysisinduced hypotension. Microscopic examination of the blood film showed monocytosis and blasts. Eventually a bone marrow biopsy in combination with the presence of a c-kit mutation and elevated serum tryptase levels confirmed a diagnosis of systemic mastocytosis. Unfortunately, renal biopsy to further evaluate the renal mass was not possible due to a persistent coagulopathy, possibly due to mast-cell heparin release. The acute renal failure was believed to be multifactorial with mast cell infiltration of the kidney and periods of mastocytosis-associated hypotension as contributing factors. We hypothesised that the hypotensive episodes were due to mast cell degranulation induced by the haemodialysis and this was confirmed by increases in serum mast cell tryptase during the first hour of dialysis which returned to baseline after dialysis. To protect against the effects of mast cell degranulation during dialysis premedication with anti-histamines and hydrocortisone was commenced resulting in an improved dialysis tolerance. Unfortunately, the systemic mastocytosis transformed into a secondary acute leukaemia and despite treatment and eventually the decision was made to withdraw dialysis. She died several days later. Discussion: Systemic mastocytosis is a rare disorder characterised by pathological mast cell accumulation in extracutaneous organs. Symptoms occur due to release of mast cell mediators, such as histamine or tryptase, the effects of local infiltration of mast cells. Triggers of mast cell mediator release include infections, surgical procedures and various drugs resulting in symptoms including pruritis and systemic vasodilation. We show that dialysis can trigger mast cell degranulation and that symptoms coincide with mast cell mediator release. 208. An unusual cause of dialysis-induced hypotension M. Jalving1, D.J. Meredith2, G.P. Collins2, E. Sharples2 1 University Medical Centre Groningen, Department of Internal medicine, PO Box 30.000, 9700 RB GRONINGEN, the Netherlands, e-mail: m.jalving@int.umcg.nl, 2Oxford Radcliffe Hospitals NHS Trust, OXFORD, United Kingdom M. Zijlstra, B. Bravenboer, C. Konings Catharina Hospital Eindhoven, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: myrte.zijlstra@gmail.com Introduction: Obesity is a major contributing factor in the aetiology of chronic renal failure, since end-stage renal disease (ESRD) is most commonly caused by obesity-related diseases. Survival rates in obese patients are higher after renal transplantation than on dialysis. However, obesity is associated with increased peri- and postrenal transplantation morbidity and mortality, and therefore is considered a (relative) contraindication for transplantation. Weight loss may play a key role Introduction: A symptomatic reduction in blood pressure occurs in up to 50% of dialysis sessions. Causes include rapid fluid removal and cardiac compromise. We describe a patient with severe dialysis-induced hypotension and an unusual underlying cause. Case: A 68-year-old woman, being analysed for leukocytosis at the haematology department, was transferred to 112 XIX. INTENSIVE CARE RESEARCH 209. Dipyridamole modulates the innate immune response during human endotoxemia. 210. Assessing small bowel function in ICU patients with multiple organ dysfunction syndrome using the citrulline generation test B.P.C. Ramakers, N.P. Riksen, T.H. Stal, S. Heemskerk, P. van den Broek, J.G. van der Hoeven, P. Smits, P. Pickkers Radboud University Medical Centre, Department of Intensive Care, Geert Grooteplein 10, 6500 HB NIJMEGEN, the Netherlands, e-mail: b.ramakers@ic.umcn.nl M.B. Keur1, J.H. Peters2, N. Wierdsma3, A.R. Girbes3, A.A. van Bodegraven3, A. Beishuizen3 1 VU University Medical Centre, Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: 113 martijnkeur@gmail.com, 2Rode Kruis Hospital, BEVERWIJK, the Netherlands , 3VU University Medical Centre, AMSTERDAM, the Netherlands 211. Causes and consequences of extremely low blood glucose levels not caused by insulin L.R. Woittiez1, M. Hoekstra2, R.F.M. Oude Elferink1, M.W.N. Nijsten2, K. Hoogenberg1 1 Martini Hospital Groningen, Department of Internal Medicine, Van Swietenplein 1, 9728 NT GRONINGEN, the Netherlands, e-mail: lyckewoittiez@gmail.com, 2University Medical Centre, GRONINGEN, the Netherlands Introduction: Small bowel dysfunction is believed to be an under diagnosed condition but it is difficult to diagnose because there is no validated bed side test. However, it is of high importance since small bowel dysfunction can possibly lead to malabsorption, sepsis and multiple organ dysfunction syndrome (MODS). Recently a novel functional test was developed, the citrulline generation test (CGT) which is suggested to quantify enterocyte function and mass, making it an interesting test to assess small bowel function. The aim of this study was to elaborate the feasibility of the CGT in a group of ICU patients with MODS and to compare results with a control group of stable ICU patients. Materials and methods: The CGT was performed in 19 ICU patients with MODS (= 2 failing organs) and in a control group of 16 stable ICU patients who were mechanically ventilated but had no other organ support. Median age and APACHE II score were respectively 69 years (64-76) and 28 (20-34) in the MODS group and 63 years (53-68) and 25 (20-27) in the control group. SOFA score was higher in MODS patients when compared to the control group, 10 (8-14) vs. 4 (3-5) (p<0.001). The CGT was performed after a 5 hour fast, after which 20 mg of glutamine-alanine was administered intravenously. Subsequently, arterial plasma was sampled at fixed time points to measure plasma citrulline levels using HPLC. Small bowel function was defined by both the slope and the incremental area under the curve of citrulline at T=75 (iAUCT75). The slope was calculated from baseline and peak citrulline levels. Results: Fasting citrulline plasma concentration was 37 mmol/l (23-45) in the MODS group and 31 mmol/l (25-38) in the control group (p=0.5), respectively. Peak citrulline concentration was 46 mmol/l (32-65) in MODS and 52 mmol/l (37-59) in controls (p=0.8). The slope in MODS patients was 0.17 mmol/l.min (0.1-0.25) versus 0.22 mmol/l.min (0.19-0.3) in the control group, p<0.05. The iAUCT75 was also lower in the MODS group, 461 mmol/l.min (289-726) vs.691 mmol/l/min (564-781) in the control group (p<0.05). Conclusion: Identifying patients with small bowel dysfunction is of great concern, however no validated tests existed until recently. The novel CGT is a test which is able to quantify small bowel function in ICU patients with MODS, being more sensitive than single fasting citrulline determination. Future studies will further elaborate feasibility and accuracy of the CGT for daily clinical practice. Introduction: The adverse effects of insulin-induced hypoglycaemia have been repeatedly described, both in diabetics and in patients in the intensive care unit (ICU). Systematic evaluation of extremely low glucose levels not caused by insulin has, to our knowledge, not been performed before. Thus we examined our hospital records for patients with extremely low blood glucose levels. Aim: Determine the causes and consequences of blood glucose levels ≤ 0.5 mmol/l in patients who did not receive insulin. Materials and methods: Glucoses from all patients admitted over a 4 year period to our hospital were evaluated. Patients with glucose levels of 0.5 mmol/l or less who did not receive insuline were included in this study. These patients were analyzed for organ failure and other factors known to contribute to hypoglycaemia and mortality rate. Results: We identified 8 patients displaying glucose levels of 0.5 mmol/l or less. All patients died during the same hospital admission, 7 of them within one day. Analysis of the patient histories demonstrated severe multiple organ failure in all patients. With respect to the potential mechanism involved in extremely low glucose levels, two factors were present in all patients. Firstly, all patients had severe disease existing for several days and thus compatible with full exhaustion of glycogen supplies. Secondly, all patients demonstrated significant laboratory signs of liver failure, indicating impaired hepatic gluconeogenesis. Conclusion: Very low blood glucose levels that are not caused by insulin administration carry poor short-term prognosis. This appears to be due primarily to exhaustion of glycogen supplies and failing gluconeogenesis. As hypoglycemia itself may contribute to the adverse outcome timely intravenous administration of concentrated glucose is warranted in patients at risk for hypoglycemia. We are currently conducting a dual Centre study to confirm the current findings and identify potentially protective factors. 114 XX. INTENSIVE CARE CASE REPORTS third trimester pregnancy. It is important to have a local protocol for this rare event. 212. Cardiac arrest in pregnancy 213. Reversal of severe tricyclic antidepressant-induced cardiovascular toxicity with sodium bicarbonate in two cases V.H. van Waning, P.M.L.H. Vencken, P.W. de Feiter, A.J.B.W. Brouwers Sint Franciscus Gasthuis, Department of Internal Medicine, Kleiweg 500, 3062 KW ROTTERDAM, the Netherlands, e-mail: v.vanwaning@sfg.nl P. Bijlstra, A.A.K. Jahn, P. van Driel, J.A.H. van Oers St. Elisabeth Hospital, Department of Intensive Care Unit, Hilvarenbeekseweg 60, 5022 GC TILBURG, the Netherlands, e-mail: p.bijlstra@elisabeth.nl Introduction: Cardiopulmonary arrest in pregnancy is a rare event. However it is important for emergency physicians to be familiar with the indications for performing a perimortem caesarean section (PMCS). We report 2 cases of PMCS performed during CPR. Cases: The first case, a 37-year-old female, G1P0, had a medical history of epilepsy. Her pregnancy was complicated at 30 weeks gestation by a single uncomplicated grandmal seizure as a result of a low valproate level. After doseadjustment no more seizures occurred. Two days after admission for hypertension, at 35 weeks gestation, she was found unresponsive. Basic life support was initiated. Upon arrival of the resuscitation team she had pulseless electrical activity. She was treated according to the standard advanced cardiac life support protocol. After 8 minutes she was still pulseless, so we decided to perform PMCS in the operating theatre. Two days postoperatively she was still unresponsive, with absent pupillary and cornea reflexes. A somato sensory evoked potential (SSEP) showed bilateral absence of N20 signals, confirming the diagnosis of severe postanoxic encephalopathy. Because of poor prognosis treatment was withdrawn. The male infant, with a birth weight of 2300 grams, had an initial Apgar score of 0/6/7 and had seizures. The baby was resuscitated and intubated. The baby survived, and follow-up 12 months after delivery showed normal growth and neurologic development. The second case, a 35-year-old patient, G3 P1, had an uneventful medical history and was referred to the hospital for induction of labour at 41 weeks and 3 days duration of pregnancy. Half an hour after spontaneous rupture of membranes the patient suffered from dyspnoea, hypotension, bradycardia and cyanosis. Upon arrival of the resuscitation team the patient had pulseless electrical activity. Three minutes after cardiopulmonary resuscitation the patient was still pulseless and PMCS was performed in the delivery room, resulting in the birth of a girl of 3450 grams with Apgar scores of 2/6/7. Two weeks after the PMCS both mother and daughter were discharged without any neurological or other abnormalities. Conclusion: Timely use of PMCS is critical for obtaining improved maternal and fetal outcomes in cardiac arrest in Introduction: We present two cases of complete reversal of serious tricyclic antidepressant (TCA) intoxication. Case 1: A 51-year-old man was admitted to the ER 1 hour after ingestion of 300 tablets Imipramine of 25 mg and 200 tablets Nortriptyline of 25 mg. BP 90/50 mmHg, pulse rate 120/min. Within a few minutes he lost consciousness, was intubated and mechanical ventilation was started. He underwent gastric lavage and was given charcoal. Crystalloid infusion and vasopressic drugs were started. His ECG showed a sinus tachycardia at a rate of 120/min and a QRS of 180ms, QTc of 561 ms and a right bundle branch block. Laboratory studies showed no abnormalities. No TCA plasma concentration was determined. Sodium bicarbonate infusion was started. 200 ml sodium bicarbonate 8.4% as bolus infusion, followed by 2 litres of sodium bicarbonate 1.4% intravenously per day. This resulted in pH values in the target range of 7.45 to 7.55. QRS time normalized within 6 hours and the right bundle branch block configuration disappeared. The patient was discharged from the ICU after 6 days. Case 2: A 20-year-old man was admitted to the ER after ingestion of 150 tablets of Tryptizol 50 mg, 30 tablets of Tryptizol 25 mg, 10 tablets Alprazolam 1 mg, 10 tablets Alprazolam 0.25 mg and 10 tablets Tranxene 5 mg. Time of intake was unknown. At arrival BP was 80/60, pulse 30/ min and Glascow Coma Scale 3. The patient was intubated on site and transported to the ER. Because of the delayed arrival no gastric lavage was performed, charcoal therapy was started. Arterial bloodgas analysis showed a pH of 7.26 and 100 cc bolus sodium bicarbonate 8,4% was given and 2 times repeated until pH range was 7.45-7.55. At arrival the QRS width was 138 ms and QTc was 541 ms. Both normalized in 12 hours. Plasma concentration of TCA was elevated. The patient was discharged from the ICU after 6 days. Discussion: TCA induced cardiotoxicity is predominantly due to blockade of cardiac fast sodium channels in the His-Purkinje system and ventricular muscle, resulting in conduction defects and decreased inotropy. Within 2 hours after ingestion gastric lavage is useful. Blood alkalization with Bicarbonate is the therapy of choice. The exact 115 mechanism is unresolved, suggested mechanisms being both pH change and sodium loading. Because of the large volume distribution and protein binding, dialysis cannot help in disposition of TCA. occur. Our patients required aggressive treatment with high doses of sedatives, which lead to prolonged ventilation and ICU stay. In the second case we considered administration of medical GHB as treatment. 214. Prolonged mechanical ventilation and ICU stay due to GHB withdrawal syndrome in two cases 215. Relationship between Staphylococcus aureus sepsis, orchidodynia and retroperitoneal disease: knowledge of simple anatomy P. Bijlstra, Q.L.M. Habes, J. van Rosmalen, J.A.H. van Oers St. Elisabeth Hospital, Department of Intensive Care Unit, Hilvarenbeekseweg 60, 5022 GC TILBURG, the Netherlands, e-mail: p.bijlstra@elisabeth.nl Y.M. Ahmed-Ousenkova 1 , H.J. van Leeuwen 2 , V. Mattijssen1 1 Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: youlia-ahmed@hotmail.com, 2Rijnstate Hospital, 2Department of Intensive Care, ARNHEM, the Netherlands Introduction: We present two cases of mechanically ventilated patients with Gamma-Hydroxybutyrate (GHB) withdrawal syndrome. Case 1: A 28-year-old man, with a history of alcohol and cocaine abuse, presented to the ER with confusion and agitation. Blood pressure 110/60 mmHg, pulse rate 110 beats/min, Glasgow Coma Scale Score of 9. Further examination was without abnormalities. Because of his fierce agitation he had to be intubated and sedated. A cerebral CT, liquor analysis, laboratory studies and EEG showed no abnormalities. At the ICU he became unmanageably aggressive, despite high doses of propofol 2.3 mg/ kg/h. Intravenous midazolam 1.5 mg/kg/h for 94 hours and oral lorazepam 32 doses of 4 mg in 7 days had to be added, with little improvement. The second day after admission the patient’s family reported that he used an unknown amount of street GHB 4 times every day. Therefore intravenous clonidine (average 0.6 mg/kg/h) was given for 77 hours, after which was switched to oral clonidine 3 x 200 mg/day. Finally, on day 7, his agitation resolved and he could be detubated. The patient was discharged to the psychiatric department with oral clonidine 3 x 200 mg/day and lorazepam 6 x 4 mg/day at day 8. Case 2: A 34-year-old man was admitted to the ICU after a high-energy trauma with multiple rib fractures, left side pneumothorax, pulmonary contusion and fractures of cervical vertebrae C2-C6. Cerebral CT was without abnormalities. Due to a history of amphetamine and GHB abuse he was treated with intravenous clonidine 0.59 mg/kg/h for 273 hours and 0,47 mg/kg/h for 335 hours, propofol 2,4 mg/kg/h for 61 hours and 1,6 mg/kg/h for 546 hours and midazolam average 0,1 mg/kg/h for 562 hours. Due to more agitation on the third day lorazepam was added to the regime (total 142 doses of 4 mg in 24 days),. Due to the regime of sedatives he required prolonged mechanical ventilation (26 days). The patient was discharged with lorazepam 6 times 4 mg and clonidine 6 times 150 mg at day 27. Discussion: GHB is an increasingly popular drug of abuse. These cases highlight that after sudden cessation of GHB use, a severe withdrawal syndrome with agitation may Introduction: The incidence of Staphylococcus aureus sepsis has significantly increased in the last twenty years. Twenty percent of patients develop metastatic complications, such as endocarditis, spondylodiscitis, metastatic abscess formation and meningitis. The presenting symptoms can sometimes be atypical, as is demonstrated in this case. Case report: A 64-year-old man with a long history of chronic lumbago and type 2 diabetes mellitus was referred to the emergency department because of sudden behavioural changes, worsening of back pain and pain in the left testicle. Three days before admission, he had consulted his general practitioner for worsening back pain, and received increased pain medication. On physical examination Glasgow Coma Score was 9. Vital signs were: temperature 35 °C, blood pressure 171/96 mmHg, and a pulse rate of 126 beats/min. Apart from a painful lower spine on palpation, physical examination did not show any abnormalities, especially inspection and palpation of the testicles. The results of blood tests showed leukocytes 3.0 x 10/l, thrombocytes of 41 x 10/l, high lactate of 10,3 mmol/l and CRP 485 mg/l. Chest X-ray and urine analysis showed no abnormalities. Liquor was clear, and mixed with blood. The patient was admitted at the Intensive Care Unit and treated according to local protocol for sepsis of unknown origin with cefuroxim. The pain in the testicle at first could not be explained. CT scans of chest and abdomen showed spondylodiscitis L3-L4 with abscess formation and spread into the left psoas muscle. Next day he was operated and the psoas abscess was drained. From blood, cerebrospinal fluid and psoas abcess Staphylococcus aureus was isolated. High dose flucloxacillin was started. Transthoracic echocardiography showed vegetations on the tricuspide valve. Four days after admission, he died due to multiple organ failure. Conclusion: We describe a patient who presented with orchidodynia and lumbago and who proved to have severe Staphyloccus aureus sepsis based on spondylodiscitis with 116 a psoas abscess. The orchidodynia can be explained as referred pain from the retroperitoneal lumbar region. This is due to the innervation of the testicle by the ilioinguinal and genitofemoral nerves, which descend from level L1, partly along the psoas, to the testicle. Diagnosis of spondylodiscitis is difficult in old patients because they present with a wide variety of symptoms and signs. Orchidodynia, without abnormalities of the testicle at physical examination, should focus on the retroperitoneal region, and in this patient might have revealed the psoas abscess related to spondylodiscitis earlier. was performed. All were negative. An osmol gap of 63,5 mOsm/kg is calculated (measured serum osmol 352 mOsm/kg minus calculated osmol 288,5 mOsm/ kg). This osmol gap is explained by the ethanol intoxication. Ethanol explains the osmoles, but is no acid. An osmol gap of 63,5 mOsm/kg corresponds with an ethanol intoxication of 2,9 ‰ (63,5 x 0,046). The measurement of serum ethanol was 2 hours later performed. With this case we tried to focus attention on the fact that a high anion gap metabolic acidosis with an osmol gap is not always the result of an intoxication with known intoxications as methanol, ethylene glycol, aspirin or toluene (all acids). 216. High anion gap metabolic acidosis with osmol gap is not always due to ingestion of known toxins 217. Use of terlipressin in amitriptyline overdose P. Bijlstra, M. Samuels, J.A.H. van Oers St. Elisabeth Hospital, Department of Intensive Care Unit, Hilvarenbeekseweg 60, 5022 GC TILBURG, the Netherlands, e-mail: p.bijlstra@elisabeth.nl D.L.J. Moolenaar, A. Manten, B.M. van der Oord Meander Medical Centre, Department of Internal Medicine, Utrechtseweg 160, 3818 ES AMERSFOORT, the Netherlands, e-mail: davidmoolenaar@gmail.com Introduction: We present a case of a patient with a mixed high anion gap metabolic acidosis with a osmol gap. Case: A 29-year-old man, with a history of alcohol abuse, presented to the ER after a fall from the stairs with a short period of loss of consciousness and seizures. Due to further loss of consciousness he had to be intubated and artificial ventilation was started. A cerebral CT scan showed bone fractures and a intracerebral haemorrhage with blood in the ventricles. He was transported to the ICU. Again seizures were observed and levetiracetam was started intravenously. Blood pressure 100/60, pulse rate 111 beats/min, respiratory rate breaths 20/ min, temperature 36,4 °C, SaO2 93%, fully sedated. Except for a haematoma on the skin of his scull no further abnormalities on examination. Laboratory studies included: Na+ 140 mmol/l; K+4,3 mmol/l; CL - 106 mmol/l; ureum 1,8 mmol/l; glucose 6,7 mmol/l; ABG pH 7,33; HCO3- 19,3 mmol/l; lactate 5,3 mmol/l; measured serum osmol 352 mOsm /kg H2O. Urine analysis revealed no ketones. Measured serum ethanol 1,7 ‰. Serum analysis for methanol, ethylene glycol, aspirin and toluene were negative. Calculated anion gap 19mmol/l, (Na+ + K+ Cl- - HCO3-) [N 8-16 mmol/l], calculated osmol (2 x Na+ + glucose + ureum) 288,5 mOsm/kg. Discussion: With an ethanol intoxication our patient fell from the stairs and developed a traumatic subarchnoid haemorrhage (SAH) The seizures are a result from the SAH or ethanol intoxication and explain the high serum lactate, which is released from the muscles. There were no signs of sepsis or tissue hypoperfusion due to shock. The lactate acidosis explains his high anion gap. Under the suspicion of an intoxication serum analysis for known toxins as methanol, ethylene glycol, aspirin and toluene Introduction: Amitriptyline is an important member of the tricyclic antidepressants and it is a commonly used drug in intentional overdose. Case: A patient is presented with severe hypotension due to amitriptyline intoxication not responding to volumesuppletion, sodiumbicarbonate administration and high dose vasopressive therapy. A very good response was elicited by administering 2 mg of terlipressin leading to a quick and uneventful recovery in the next hours. Conclusion: We report a case of acute tricyclic-intoxication, complicated by severe vasodilatory hypotension refractory to volume and vasopressive therapy, successfully and safely treated by terlipressin. XXI RHEUMATOLOGY RESEARCH 218. Lymphocytopenia as a riskfactor for Pneumocystic jiroveci pneumonia in dermatomyositis: two case reports, a review and profylaxis recommendations D.G. Beekman1, M.D. Kruif2, I. van Groenigen3, K. Saito4, Y. Tanaka 4 , A. Voskuyl3, M. van Agtmael3, C. Slagt1, B. Kanen1 1 Zaans Medical Centre, Department of Internal Medicine, PO Box 210, 1500 EE AMSTERDAM, the Netherlands, e-mail: djoekegonne@hotmail.com, 2 Academic Medical Centre, AMSTERDAM, the Netherlands, 3VU University Medical Centre, AMSTERDAM, the Netherlands, 4School of Medicine, KITAKYUSHU, Japan 117 Introduction: We present two cases of DM, one fatal of Pneumocystis jiroveci pneumonia in patients with dermatomyositis. No consistent guidelines were found for PCP-profylaxis in this patient group. We collected expert opinions and we pooled data from previous studies, in order to construct new, simple recommendations for PCP-profylaxis in these patients. Methods: Literature was reviewed using PubMed database and references. Authors were contacted for sharing original data, which were pooled in order to calculate incidence figures of PCP, mortality rates and prognostic factors. Results: Two cases from our hospital are presented, one of them was fatal. In literature, 13 relevant case series were found. Pooled incidence for PCP were 1% for all patients with connective tissue disease (CTD) and 4.3% (p<0,001) for the subset of patients with dermatomyositis and/or polymyositis (DM/PM). Mortality in both groups was high but not significantly different (45% vs. 55%). We found a relation between a low lymphocyte count (< 1.5 x 109/l) based on clinical parameters. Conclusion: Based upon pooled data from 12 prospectiveen retrospective studies as well as 2 case-reports, we recommend PCP-profylaxis for all patients diagnosed with DM/PM with a low lymphocyte count (< 1.5 x 109/l) at diagnosis. joints. Blood investigation revealed a CRP of 141 mg/l, ESR 114 mm/h, leukocyte count of 17.7 x 109/l and normal renal and liver function tests. Diclofenac treatment was started without success. Serologic examination for Borrelia, Q-fever, Rubella, CMV and EBV as well as rheumatoid factor were negative. Ferritin level was 3687 ug/l. At this point AOSD was considered. Three months after initial complaints, the patient developed acute liver test abnormalities with a total bilirubin level of 303 umol/l, AF 512 U/l, gGT 330 U/l, ASAT 1659 U/l, ALAT 1591 U/l and a ferritin level of 7639 ug/l. Hepatitis A,B,C,E serology was negative and she had no anti nuclear or anti mitochondrial antibodies. Within a month her liver function returned to normal. However, fever and arthralgia persisted and the liver enzymes increased again. Definite diagnosis of AOSD was made and prednisone was started which resulted in a remarkable improvement. Eight months after her initial complaints, the patient is nearly in remission. Discussion: AOSD is an inflammatory disorder with unknown etiology, characterized by fevers, arthritis, skin rash and markedly elevated levels of serum ferritin. There is no specific test to confirm the diagnosis. Therefore, a combination of criteria, termed the Yamaguchi criteria, have to be met. Liver involvement is one of the minor criteria, but only a few cases describe extreme liver test abnormalities. In this case, drug sensitivity for amoxicillin cannot be completely ruled out but is considered unlikely because of relapse of liver function disturbance and the fact that development of liver test abnormalities was entirely in line with the development of extreme levels of serum ferritin. Conclusion: AOSD is often difficult to diagnose and can lead to severe and long-lasting complaints. XXII.RHEUMATOLOGY CASE REPORTS 219. Adult-onset Still’s Disease as a cause of extreme liver test abnormalities 220. Painless joint deformities in a patient with renal disease and diabetic polyneuropathy P.M. van Gastel, C. Richter Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: petrivangastel@hotmail.com J.J.M. Geelhoed, I.C. van Riemsdijk-van Overbeeke, A. Dees Ikazia Hospital, Department of Internal Medicine, Scheepmakerskade 73, 3011 VX ROTTERDAM, the Netherlands, e-mail: mgeelhoed@hotmail.com Background: Adult onset Still’s Disease (AOSD) is a well characterized rheumatoid disorder in which the liver is frequently involved. This is generally asymptomatic, but severe hepatic failure has occasionally been reported. We describe a case of a woman who developed severe liver test abnormalities three months after presenting symptoms of AOSD. Case-Report: A 52-year-old woman with a history of endometrial carcinoma was referred to our outpatient clinic because of fever. Complaints started five weeks earlier, with fever, diffuse rash and a sore throat. Amoxicillin therapy had been started two weeks before, without remission. On examination she had erythema on upper legs and red and swollen metacarpophalangeal Introduction: Limited surgery of fingers or toes sometimes is inevitable in diabetic and rheumatic patients, usually due to persistent microvascular or infectious disease. Underlying crystal arthropathies however, such as longstanding gout, may mislead the pathologist and clinician. Case: A 79-year-old male was sent to the nephrologist in case of chronic kidney disease stage III. On admission, marked, painless joint lesions of all fingers were noticed. He had a history of TBC, hypertension, polyneuropathy, type II diabetes mellitus, atrium flutter, and congestive heart failure. Physical examination showed red and swollen joint lesions 118 of his fingers with yellow-white deposits (tophus lesions). He missed his left digit V, which had been amputated. The patient, who feared new surgery, told that the other fingers had become worse since five months. The case was reconsidered: digit V had been amputated some years before, because of persistent ulceration. The pathological diagnosis was rheumatoid arthritis. X-ray imaging of the hands had shown reactive changes with extensive erosions in nearly all fingers. Because of the dramatic radiologic and microscopic results, a diagnosis of rheumatic arthritis had been made. Therapy with methotrexate and prednisone was started, leading to an improvement of the clinical picture. Moreover, older patient data revealed that at first, the lesions were thought to be pseudo-gout caused by renal insufficiency. However, in the past he had been diagnosed with gout flares of his big toe and feet, accompanied by characteristic gout pain and treated with Colchicine. Combining these contradicting data a new smear of the deposits was taken, showing (surprisingly) massive uric acid crystals. Retrospectively, the pathologist changed result of the amputated tissue from rheumatoid arthritis to gout. Discussion: Gout is a very painful urate crystal deposit disease of the joints. Most often it presents as an acute mono-arthritis with predilection for lower extremities, especially the big toe. Longstanding progressive tophus disease may present as low grade chronic poly-arthritis, resembling rheumatoid arthritis. The diagnosis of gout is confirmed by the presence of uric acid crystals in the joint fluid or tophi. In our patient, doctors were misled by the lack of pain, the pathological diagnosis of rheumatoid arthritis and his renal insufficiency. Conclusion: It illustrates that serious joint deformities do not necessary lead to joint pain. In this atypical patient, his diabetic polyneuropathy may have masked the pain and thereby delayed the diagnosis. muscle pain and muscle weakness. Laboratory results at that time revealed no abnormalities, except for an increased sedimentation rate (85 mm/h) and a leucopenia (3.1 x 109/l), although creatininekinase was not determined. Blood cultures were repeatedly negative. On examination at our hospital the patient had severe proximal muscleweakness and could hardly walk, showed proximal muscle atrophy and most importantly a heliotrope rash and Gottron’s plaques. Based on these clinical observations, the most likely diagnosis was dermatomyositis. The diagnosis was confirmed by the presence of increased serum creatinekinase levels (1880 IU/l) and abnormalities shown in the skinbiopsy (chronic perivascular and interstitial dermatitis with vacuolar changes, edema and mucine depositions) and in the muscle biopsy (lymphocytic infiltrates in muscle, no specific abnormalities). Additional imaging analysis revealed no signs of malignancy and immunoserology showed positive antinuclear antibodies with antibodies against SS-A but not against Jo-1. The patient was treated with corticosteroids. Dermatomyositis is a rare inflammatory myopathy. Both male and female of all ages may be affected. Symmetric and proximal muscle weakness as well as characteristic skin findings as heliotrope rash, shawl’s sign and Gottron’s plaques are the typical symptoms. Systemic complaints such as fatigue, fever, weight loss or non-erosive inflammatory polyarthritis may develop, especially as the disease progresses. Interstitial lung disease develops in at least ten percent of the cases and can rapidly lead to respiratory failure and even death. Furthermore patients with dermatomyositis have an increased risk of malignancies, especially adenocarcinomas of the cervix, lung, ovaries, pancreas, bladder and stomach. The treatment of choice are glucocorticoids and if needed glucocorticoid-sparing medications such as azathioprine or methotrexate. In every patient with skin abnormalities on handjoints in combination with muscle weakness the diagnosis dermatomyositis should be suspected. 221. Red fist without strength I.K. van Groeningen1 , J. Arnoldus2 , D. Beekman 2 , M. van Agtmael1, A.E. Voskuyl1 1 VU University Medical Centre, Department of Internal Medicine, De Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: i.vangroeningen@vumc.nl, 2Zaans Medical Centre, ZAANDAM, the Netherlands 222. Takayasu arteritis mimicking malignancy A.E. Pulles, G.J.M. Herder, E.J. ter Borg, W.J.W. Bos St. Antonius Hospital, Department of Internal Medicine, Koekoekslaan 1, 3435 CM NIEUWEGEIN, the Netherlands, e-mail: a.pulles@antoniusHospital.nl Case: In July 2010, a 64-year-old man was presented to our hospital for a diagnostic problem consisting fever, skin lesions and musclepain. Six weeks before he presented himself at another hospital with a submental swelling and high fever and was treated with antibiotics on suspicion of erysipelas. A week later skinlesions developed on the metacarpophalangeal and proximal carpophalangeal joints hands, nose and eyes. His mobility was impaired due to Case report: A 69-year-old woman of Indonesian descent was diagnosed with Takayasu arteritis in 2005 and is regularly controlled in our outpatient department. For the last couple of years there were no signs of disease activity; blood pressure difference between both arms was stable. Recently, she was evaluated because of weight loss. 119 Three weeks prior to presentation she was admitted to a hospital in Bali (Indonesia) because of a suspected pneumonia. The radiology report of the X-thorax described a density in the left inferior lobe and possibly in the right inferior lobe as well. She was treated with antibiotics and her pulmonary symptoms disappeared completely. A follow-up X-thorax in our clinic revealed a small density in the right inferior lobe. Further analysis by CT disclosed three nodules in the right inferior lobe, of which the largest diameter was 1 cm. The lesions were suspect for malignancy; therefore a PET-CT was made. However, on PET-CT only one of the three nodules was visible and barely active. Furthermore, there were no signs of active metabolism in the large arteries. At that moment, CRP (1 mg/l) en ESR (21 mm/h) were low. Subsequently a bronchoscopy was performed. Cytology obtained by lavage demonstrated no malignant cells and the cultures did not grow any pathogenic micro-organisms. Since malignancy could not be excluded, video-assisted thoracoscopic surgery with a wedge resection of the right inferior lobe was performed. Histopathological examination of the obtained tissue showed mainly necrotic tissue surrounded by some granulomatous inflammation. There were no malignant features or signs of an active vasculitis. Stains for acid-fast bacteria, fungi and other micro-organisms were negative. The pathologist considered an old infarction to be the most likely interpretation of this specimen. Discussion: Takayasu arteritis primarily affects the aorta and its main branches. In approximately 50 percent of patients pulmonary arteries are involved as well, but pulmonary symptoms occur less often. Pulmonary infarction as the initial presentation of Takayasu disease is well documented. However, to our knowledge pulmonary infarction mimicking pulmonary malignancy in Takayasu arteritis has not been described previously. Conclusion: This case report illustrates that pulmonary infarction due to Takayasu arteritis can mimic malignancy. is thought to reduce morbidity and mortality. Early warning systems (EWS) are based on this hypothesis. In our hospital an EWS based on level of consciousness, respiratory rate, heart rate, systolic blood pressure and oxygen saturation was introduced. Aim: To assess characteristics and outcome of patients with clinical deterioration according to our EWS. Methods: We performed a retrospective analysis of the reports of the EWS during a ten-month period in 2009 and 2010 on a medical ward in a teaching hospital in the Netherlands. Only first reports were included. Primary endpoints were hospital mortality and adverse events in the 24 hours after the report. Results: During the study period there were 53 reports. Two were not included because of incomplete data, 14 reports were excluded because they were second or third reports. From the 37 reports which were analysed 59.5% of the patients were male, the median age was 78 year (range 44-91). 94.6% of the admissions were not planned. Most frequent reasons for admission were suspicion of infectious disease (45.9%), dyspnoea and kidney failure (both 10.8%). In 56.8% there were no limitations on treatment preceding the report. The parameter that was most frequent changed was the respiratory rate (RR >25/min, 26 times), followed by oxygen saturation (oxygen saturation < 92%, 25 times) and changed level of consciousness (decrease of GCS =2 points, 11 times). The decline was in most cases thought to be due to a primary problem in the circulation (37.8%) or to sepsis/infection (37.8%). Medication and supportive care were started 28 times. In 9 cases there was consultation of an intensive care specialist; 4 patients were transferred to the ICU, in the other 5 cases a treatment limitation was adjusted. Two other patients got a treatment limitation following the report. Three patients (8.1%) died within 24 hours of the report. All three of them had a treatment limitation and their deaths were expected. Total hospital mortality was 32.4%. No cases of cardiopulmonary resuscitation were found in the observed group. Conclusion: In our study we found the respiratory rate as most frequent reported changed physiological parameter, as is previously described in other studies. The most frequent causes for decline were circulatory problems and sepsis/infection. It is notable that in almost 1 in 5 patients a treatment limitation was arranged following the report. XXIII. GENERAL INTERNAL MEDICINE RESEARCH 223. Early warning system on a medical ward; patient characteristics and clinical outcome C. Bethlehem, W.P. Kingma Medical Centre Leeuwarden, Department of Internal Medicine, Henri Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: carina.bethlehem@znb.nl 224. The safety of winetasting: the Bac(chus) experiment D.L.J. Moolenaar, A. van de Wiel, J.P.M. Wielders Meander Medical Centre, Department of Internal Medicine, Utrechtseweg 160, 3818 ES AMERSFOORT, the Netherlands, e-mail: davidmoolenaar@gmail.com Introduction: Clinical deterioration is often preceded by changes in physiological parameters; early intervention 120 Introduction: During the last two decades wine has become very popular even in non-wine growing countries and winetasting sessions are organized regularly as part of this social phenomenon. Although the wine is not consumed, the contact of the wine with the buccal mucosa may lead to alcohol absorption. In this experiment blood alcohol concentrations (BAC’s) were measured after such a winetasting session. Methods: Ten healthy volunteers, five men and five women, ages ranging from 30-60 years, participated in the experiment. They tasted ten wines, five white and five red ones, with alcohol percentages ranging from 11.5-13.5% during 50 minutes. They were requested to hold fifteen cc of each wine in the mouth during two periods of 15 seconds with an interval of one minute. The wine was spat out to prevent gastro-intestinal uptake. The mouth was washed with water before the next wine was tasted three minutes later. Ten minutes after the last wine, so one hour after the start of the experiment blood samples were taken for BAC analysis by an enzymatic method on a Beckman Counter Analyzer. Results: In only one of the individuals, a woman of small size, the alcohol concentration found (0.06 g/l) was above the detection limit of 0.05 g/l. For the whole group concentrations ranged from 0.01-0.06 g/l, mean 0.025 g/l for both men and women, well below the legal Dutch limit for driving permission (0.5 g/l). Conclusion: The tasting of ten wines during a one hour period does not result in blood alcohol concentrations that interfere with driving ability or daily activities. in the Netherlands from May 2007-August 2007 were studied. 2000 consecutive admissions were studied: 576 (29%, 26-32%) were classified as possibly iatrogenic; out of these 380 (19%, 17-22%) as definitely iatrogenic, out of whom 229 (12%, 10-14%) had already been classified as iatrogenic by the admitting physicians. Patients with cardiac disease, hypertension, gastrointestinal conditions, anticoagulant treatment and use of NSAIDs were, particularly, at risk of iatrogenic admission with percentages of 22 (16-24), 13 (11-18), 12 (9-15), and 7 (5-11)%. An independent predictor of iatrogenic admissions was age with an odds ratio of 1.27 per 10 years (p=0.0001). 1. At least 19% of admissions to the departments of internal medicine/cardiology/pulmonology, and, maybe, even percentages up to 29% were due to adverse drug effects. 2. A large difference between the numbers of iatrogenic admission according to the physicians in charge of admission and the investigators, 229 versus 380 patients, was observed. 3. Most often iatrogenic admissions were observed with cardiac disease, hypertension, gastrointestinal conditions, anticoagulant treatment, and use of NSAIDs. 226. Meta-analysis of recent studies on patients admitted to hospital due to adverse drug effects R. Atiqi1 , E.H.F. van Bommel1, A.M.J. Cleophas1, A.H. Zwinderman2 1 Albert Schweitzer Hospital, Department of Internal Medicine, Albert Schweitzerplaats 25, 3300 AK DORDRECHT, the Netherlands, e-mail: r.atiqi@live.nl, 2 Academic Medical Centre, AMSTERDAM, the Netherlands 225. Prevalence of iatrogenic admissions to the departments of medicine/cardiology/pulmonology in a 1250 beds general hospital 1 1 In the past decade the use of drugs has expanded. Earlier studies on patients admitted for adverse drugs effects (ADEs) were heterogeneous. The objectives were to assess recent numbers of admissions to hospital due to ADEs, to assess heterogeneity of recent studies. Prospective studies published in the past decade were pooled and compared to the pooled results from earlier studies. The pooled overall percentage of the recent studies (n=20) was 5.4% (5.0-5.8) and did not significantly differ from that of the earlier studies (n=21, pooled percentage 4.7%, 3.1-6.2). The studies were clinically very heterogeneous with percentages of ADEs between 3.4 and 33.2%. The type of study group could be held largely responsible for the clinical heterogeneity observed. 1 R. Atiqi , E.H.F. van Bommel , A.M.J Cleophas , A.H. Zwinderman2 1 Albert Schweitzer Hospital, Department of Internal Medicine, Albert Schweitzerplaats 25, 3300 AK DORDRECHT, the Netherlands, e-mail: r.atiqi@live.nl, 2 Academic Medical Centre, AMSTERDAM, the Netherlands A recent meta-analysis in this journal showed incidences between 3.4 and 33.9%. Studies performed by pharmacists and epidemiologists produced lower incidences than internists’ studies. We reassessed the prevalence of iatrogenic admissions in a study of internists. Iatrogenic disease was defined as adverse drug reactions according to the World Health Organisation Definition and complications induced by non-drug medical interventions. Subsequent admissions at the departments of medicine/ cardiology/pulmonology in a 1250 beds general hospital 121 227. Anemia and its consequences in the LifeLines cohort study than 65 years. Less than half of the participants who were informed contacted their GP. Among these patients several serious diagnoses were found needing therapy. There was no relationship between anemia and HR-QOL. M.M. van der Klauw, H. van der Valk, L.J. van Pelt, B.H.R. Wolffenbuttel University Medical Centre Groningen, Department of Endocrinology, PO Box 30001, 9700 RB GRONINGEN, the Netherlands, e-mail: m.m.van.der.klauw@int.umcg.nl 228. Analyzing completion times in an academic emergency department: decision making is the weakest link Introduction: Anemia is a common problem and is associated with increased morbidity, mortality and a decrease in quality of life. Aim: To assess the prevalence of anemia in southwest Friesland and East Groningen, and the diagnoses established, and to compare the quality of life in participants with anemia with that of participants without anemia. Materials and methods: Case-control study within the Dutch adult population who participated in the LifeLines-cohort from November 2006 until June 2010. We measured Hb, Ht and erythrocytes, and HR-QOL (RAND-36 item Health Survey) in 11645 Caucasian participants, 4870 men and 6775 women (mean age 43.89, SD 11.44, range 18-89 years). Anemia was defined as a Hb value of =0.5 mmol/l below the lower limit of the reference interval of the University Medical Centre Groningen laboratory (women < 7.0, men < 8.2 mmol/l). Both the general practitioner (GP) and the participant were informed of the finding. Of these participants, a chart survey was performed in 41 general practices. The control group consisted of a random selection of LifeLines participants, matched for age and gender. Results: Prevalence of anemia was 2.2% among men and 2.1% among women. Among 644 participants older than 65 years, the prevalence in men was 8.4%, and in women only 0.3%. Patient charts were checked in 196 anemia cases. Only 96 (49%) participants contacted their GP for further evaluation, 64 women and 32 men. Additional examinations were performed in 68 participants, 22 received therapy directly, in 6 no analysis was performed and no therapy started. 54 Participants had a known anemia, and in 21 upon further analysis the anemia had resolved. 4 Participants had recently donated blood, 32 had hypermenorrhea, 3 vitamin B12 deficiency, 2 hemorrhoids, 1 nose bleeds, 1 a Barrett oesophagus, 3 thalassemia (of which 2 were known), 1 oesophageal varices, and 5 were found to have a carcinoma (1 renal cell, 1 stomach, 1 pancreatic and 2 coloncarcinomas). The % of participants contacting their GP was larger if the Hb was lower. No relationship between the participants with anemia and the control group regarding HR-QOL could be found. Conclusions: The prevalence of anemia in this population was 2.1%, and higher among male participants older I.L. Vegting, M.C. Visser, M.H.H. Kramer, G.M. Koole, E. van de Walle, P.W.B. Nanayakkara VU University Medical Centre, PO Box 7057, 1007 MB AMSTERDAM, the Netherlands, e-mail: p.nanayakkara@vumc.nl Introdcution: Although, congestion with long waiting times are frequently noticed in some emergency departments (ED) in the Netherlands, no target for completion time is defined or enforced. In our opinion, it is preferable to keep the length of stay at the ED short, so that patients can be transferred to a stable and a safe environment as soon as possible. It has been demonstrated that the length of stay in the ED is associated with the length of stay in the hospital and even mortality Aim: Investigating completion times in an academic emergency department (ED) and the factors contributing to long completion times. Material and methods: Data of ED patients presenting at VU university medical centre, was prospectively collected during 4 weeks in February 2010. Presentation time, referrer, discharge destination, and medical specialties involved were registered. Additional detailed data about relevant time-steps were collected from patients with triage category Emergency Severity Index (ESI) 3. The Pearson’s chi-square test and the Mann-Whitney test were used for statistical analysis. Results: 13% of patients had a completion time longer than four hours (average 2:23 hours). In ESI 3 patients, 24% had a completion time longer than four hours (p<0.001). Internal medicine had most patients exceeding the four hour target (37%), followed by neurology (29%). Undergoing a CT scan and hospital admission were associated with exceeding the four hour target (p<0.001). No association between arrival time on the ED and completion time was found. The elapsed time between receiving the results of all diagnostic tests and admission/ discharge had the most influence on the completion time (p<0.001). Conclusions: A significant percentage of vulnerable and sick patients exceeded the four hour completion time in our ED. The biggest contributor to this delay was the process of decision making after completion of all diagnostics on the ED. Improving the direct supervision 122 of junior colleagues will, in our opinion, speed up the decision making process and lead to shortening of completion times in many patients. significant reduction in the diagnostic costs in the department of internal medicine. Extending these measures to the entire hospital and even entire country will in our opinion lead to significant reduction in the health care costs. 229. Increasing the awareness among the doctors lead to a significant reduction in the costs spend on the diagnostics 230. Risk factors influencing the outcome of community acquired pneumonia I.L. Vegting, M. van Beneden, M.H.H. Kramer, A Thijs, P.W.B. Nanayakkara VU University Medical Centre, PO Box 7057, 1007 MB AMSTERDAM, the Netherlands, e-mail: p.nanayakkara@vumc.nl L.M.A. Klieverik, R. So, D. Cheung, M.D. Levin Albert Schweitzer Hospital, Department of Internal Medicine, PO Box 444, 3300 AK DORDRECHT, the Netherlands, e-mail: l.klieverik@asz.nl Introduction: The burden of health care expenditure on national budgets have increased dramatically over the past decade. Hospital care consumes one of the largest portion of the total healthcare costs. In hospitals a large portion of the money is spent on diagnostic tools such as laboratory and radiological tests. A pilot study performed in our hospital demonstrated that unnecessary diagnostic tests were performed frequently. Aim: Reducing the costs of unnecessary diagnostic tests in internal medicine patients Materials and methods: In December 2008, a management consultant evaluated all cost of all the diagnostics (laboratory, radiology, nuclear medicine, pathology, microbiology) performed in the department of internal medicine between 2006 and 2008. Doctors were then informed of these findings. A target was set to reduce the costs spent on diagnostics in the internal medicine department by 7,5% in 2009 compared to 2008. In 2009 multiple interventions were introduced to improve awareness of unnecessary diagnostic costs among physicians. This included: introduction of posters and pocket cards detailing the costs of diagnostic tests, six weekly feedback on the diagnostics costs, mentorship of junior doctors, unbundling panel tests and increasing protocol adherence. Main outcome measures were reduction in the total diagnostic costs and the total number of laboratory tests performed in the internal medicine department in 2009. Results: The department of internal medicine spent 2.80 million euro and 2.45 million euro on the diagnostic tests in 2008 and 2009 respectively (13% decline) and thereby saved 350.000 euro in 2009. The largest reduction was achieved by reducing the number of laboratory tests performed.). In the rest of the hospital (internal medicine department excluded), the total costs spent on the diagnostics were 32,94 million euro in 2008 which declined to 32,13 million euro in 2009, saving 389.000 euro in 2009 (2.4% reduction). Conclusions: Introduction of a few simple measures to improve awareness among the physicians led to a Introduction: Community acquired pneumonia (CAP) has worldwide high morbidity and mortality. In the literature the mortality varies from 10% to 25%. In het Albert Schweitzer Hospital in Dordrecht, the Netherlands the morbidity and mortality are quite high as well. Aim: The question remains what the underlying cause is for these high numbers of hospital mortality. Materials and methods: Between 01-2005 and 01-2010 2508 consecutive patients were admitted in our hospital with a CAP. We evaluated patient characteristics, early and late morbidity and mortality and predictors of adverse outcome. Also the pneumonia severity index (PSI) en de CURB-653 were used to predict mortality. Furthermore we compared our outcome to the Dutch HSMR (Hospital Standardized Mortality Ratio). Results and conclusions are currently analyzed and will be completed before the annual meeting of the Dutch College of Physicians. 231. Physicians report barriers to deliver best practice care for asplenic patients A.J.J. Lammers, J.B.L. Hoekstra, P. Speelman, M.J.M.H. Lombarts Academic Medical Centre, Amsterdam, Department of Internal Medicine, Meibergdreef 9, 1105 AZ AMSTERDAM, the Netherlands, e-mail: a.j.lammers@amc.uva.nl Introduction: Current management of asplenic patients in the Netherlands is not in compliance with best practice standards as defined by the British Committee for Standards in Haematology. To improve quality of care, factors inhibiting best practice care delivery need to be identified first. Aim: To identify and quantify physicians’ barriers to adhere to best practice management of asplenic patients. Materials and methods: A cross-sectional survey was performed, preceded by multiple focus group discussions. 123 Dutch physicians responsible for prevention of infections in asplenic patients, including internists, surgeons and general practitioners (GPs) participated. Results: Forty seven GPs and seventy three specialists returned the questionnaire, yielding response rates of 47% and 36,5% respectively. Physicians reported several barriers to deliver best practice. For both GPs and specialists, the most frequently listed barriers were: poor patient knowledge (> 80% of specialists and GPs) and lack of clarity about which physician is responsible for the management of asplenic patients (50% of internists, 46% of surgeons, 55% of GPs). Both GPs and specialists expressed to experience a lack of mutual trust: specialists were uncertain whether the GP would follow their advice given on patient discharge (33-59%), whereas half of GPs was not convinced that specialists’ discharge letters contained the correct recommendations. Almost all physicians (> 90%) indicated that availability of a national guideline would improve adherence to best practice, especially if accessible online. Conclusion: This study showed that care delivery for asplenic patients in the Netherlands is suboptimal. We identified and quantified perceived barriers by physicians that prevent adherence to post-splenectomy guidelines. Better transmural collaboration and better informed patients are likely to improve the quality of care of the asplenic patient population. sation. The anion gap was elevated: 21 mmol/l. Presuming a diagnosis of urosepsis, sodium bicarbonate was given and the gynecologist decided to perform a Caesarean delivery which passed uneventfully. Two girls were born, one needing short cardiac massage and mechanical ventilation. The next day both newborns were doing well and no permanent disabilities were foreseen. Pathological examination revealed no abnormalities of the placentae. Lactate levels, measured shortly before caesarian section were within normal range. A urine keton value of more than 7,8 mmol/l was demonstrated (normal < 0.5 mmol/l). Her husband stated that she had barely eaten for a week previously and that she had been vomiting for two days prior to admission. He confirmed her statement that she had not taken salicylates, other medication or ingested alcohol. She had no access to antifreeze. Toxicological tests revealed a salicylate level of < 5 mg/l, an acetaminophen level < 1 mg/l, and an acetone level of 300 mg/l (reference 5-20 mg/l), Methanol and ethanol tests were both negative. No signs of renal disease or diabetes were present. The metabolic acidosis resolved fully after glucose 5% infusion. Her vital parameters remained normal and she was discharged to the obstetric ward the following day. A non-diabetic starvation keto-acidosis in pregnancies has been reported only in a few case reports. Pregnancy is a high insulin resistant state, especially in third trimester, accentuated in this case by obesity and a gemelli pregnancy. The combination of (mild) starvation and a state of insulin resistance may easily lead to metabolism based on alternative sources, leading to overproduction of ketons, and consequently ketoacidosis. Acute acidosis in pregnancy is a risk for intra-uterine death and may lead to abnormal neurological development. Treatment is glucose and often delivery. XXIV.GENERAL INTERNAL MEDICINE CASE REPORTS 232. A case of non-diabetic keto-acidosis in pregnancy 233. Rhabdomyolysis after dying hair with paraphenyl diamine-containing hair dye J.B.J. Scholte, W.E. Boer Atrium Medical Centre Parkstad, Department of Internal Medicine-IC, Henri Dunantstraat 5, 6419 PC HEERLEN, the Netherlands, e-mail: Janscholte@hotmail.com M. Ezzahti1, P. Biezen2 1 Amphia Hospital, Department of Internal Medicine, Molengracht 21, 4818 CK BREDA, the Netherlands, e-mail: ezzahti00@hotmail.com, 2Erasmus Medical Centre Rotterdam, ROTTERDAM, the Netherlands Case: A 26-year-old patient presented with progressive dyspnoea. She was pregnant with a dicorial, diamniotic gemelli (35 weeks and 4 days). Initially (for one day) she was treated with amoxicillin for a presumed lower urinary tract infection. Physical examination revealed no abnormalities except a body mass index of 39 kg/m2. Cardiotocography revealed both normal and reactive heart rates and no contractions. Chest X ray and electrocardiography showed no abnormalities. She was admitted for further observation with a presumed diagnosis of chronic hyperventilation and an unexplained mild elevation of CRP (32 mg/l). The second day a new blood gas analysis revealed a metabolic acidosis with respiratory compen- Case-report: A 34-year-old female without medical history was admitted to the hospital because of generalised muscle pain and dysphagia. At physical examination there was oedema of the face, no fever, the blood pressure was 120/80 mmHg and respiratory rate 12/min. On examination her hands were coloured deeply black. Laboratory results showed a normal renal function, normal CRP, CK 84446 U/l, ASAT 2619 U/l, ALAT 463 U/l and lactate dehydrogenase of 6051 U/l. The urine was 124 Case presentation: An eighty-seven-year-old caucasian woman presented with progressive fatigue and weakness in the proximal extremity muscles. Because of an elevated risk for cardiovascular events she used a statin. Medical evaluation included high serum levels of creatine phosphokinase (CK) and lactate dehydrogenase (LD). Extensive evaluations for underlying malignancies, cardiac and interstitial pulmonary disease were unremarkable. Differential diagnosis included statin-induced myositis. She was treated by prednisone and discontinuing the statin. The laboratory results improved, but the muscle weakness did not. An electromyogram (EMG) showed axonal polyneuropathy with clues for an anterior horn disease. A muscle biopsy revealed a necrotising myopathy. Conclusion: Side-effects of statin use can follow a serious course with muscle complaints, myositis, rhabdomyolysis, and statin-induced myositis. One should always think of such side-effects if a patient presents with muscle complaints. Also, be aware of a possible underlying (muscle) disease. Cessation of statin and monitoring CK levels are important goals in treatment of statin-induced myositis. very dark and contained myoglobin. A chest radiograph showed bilateral infiltrative shadows. The patient had a combination of rhabdomyolysis, oedema of the face and pneumonia. The patient used no medication or drugs. There was no trauma or extreme physical exercise. There were none electrolyte disturbances. The cause of her black coloured hands was that she applicated with no gloves traditional hair dye (Takawath) in combination with Henna on her hair four hours before she got complaints. She boiled the Takawath and this caused damps which she inhaled. The Takawath contains paraphenyldiamine (PPD). The urine of the patient was analysed qualitatively for PPD and the result was positive. The patient was treated with a high amount of 0.9% sodium chloride solution with addition of bicarbonate. The renal function stayed normal and CK decreased very rapidly. The complaints of dysphagia and muscle pain disappeared in a couple of days. After three days the chest radiograph showed spontaneous reduction of the infiltrative shadows. The patient was advised not to use PPD-containing hair dye anymore. Discussion: Paraphenyldiamine is used very often in hair dye and as an additive to Henna to give Henna a black tattoo-like appearance. In Northern Africa and India hair dye ingestion is a common problem. The ingestion of PPD-containing hair dye is used to commit suicide and can produce rhabdomyolysis, renal failure and severe laryncheal oedema. The pathogenesis of renal failure is through rhabdomyolysis and because of a direct toxic effect of PPD in the tubules. Because the mechanism in which PPD causes rhabdomyolysis is not known, we performed in this patient a biopsy of the muscle of the right upper leg. This showed a myositis with an allergic component because of a great amount of eosinifolic granulocytes. Conclusion: This case illustrates that paraphenyldiaminecontaining hair dye can cause rhabdomyolysis, oedema of the face and a chemical pneumonia possibly through an allergic mechanism. Every clinician should be aware that this association exist. 235. A patient with back pain and inflammatory changes on MRI due to polymyalgia rheumatica N. Wlazlo, B. Bravenboer, H. Pijpers, M.C. de Rijk Catharina Hospital, Department of Internal Medicine, Michelangelolaan 2, 5623 EJ EINDHOVEN, the Netherlands, e-mail: nick.wlazlo@cze.nl Introduction: Polymyalgia rheumatica (PMR) is often diagnosed by its typical presentation of pain and stiffness in proximal joints. We present an atypical case of a man with low back pain, in which imaging studies were eventually helpful in establishing a diagnosis of PMR. Case: A 64-year-old male was admitted to our hospital with increasing low back pain, radiating to his upper legs. Analgesics and physical therapy had not improved his symptoms. In the past 5 months, he had visited our emergency department twice with these complaints, but no diagnosis had been established and the pain proved to be self-limiting. The patient’s history showed type 2 diabetes mellitus and several cardiovascular events. The patient was not febrile and showed no abnormalities on physical and neurological examination. Laboratory investigation (reference values between parentheses) showed an elevated erythrocyte sedimentation rate of 74 mm/h (0-20 mm/h) and a C-reactive protein of 74 mg/l (0-6 mg/l). Our differential diagnosis included spondylodiscitis, epidural abscess, rheumatoid arthritis (RA), unknown infection, spondylarthropathy, malignancy (especially multiple myeloma), or auto-immune disease. 234. Statin-induced myositis I.C. Kouwenberg, M.M.C. Hovens Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: ikouwenberg@alysis.nl Introduction: Statins (HMG-CoA (3-hydroxy-3-methylglutaryl-coenzyme A) reductase inhibitor) are often used to reduce the risk of cardiovascular events. Side effects of statins can consist of muscle pain and remarkably elevated serum creatine phosphokinase (CK) levels, or rhabdomyolysis, and can be life threatening. 125 unremarkable except for hypotension (BP 90/60 mmHg) and a bradycardia of 45 beats/min. Electrocardiography showed a sinus bradycardia of 50 beats/min with a first degree atrioventricular block. Laboratory investigations showed no abnormalities. Supportive treatment resulted in rapid recovery in this case, too. Discussion: We describe two patients that recently presented at our emergency room with poisoning by wild honey. Both patients had obtained the substance in Turkey, where it is used as a complementary medicine for gastrointestinal and cardiovascular symptoms. Wild honey is made by bees from flowers of rhododendron species, the most common being Rhododendron ponticum and Rhododendron flavum. These rhododendrons can be found in Turkey, Japan, Nepal, Brazil, and some parts of North America and Europe. Grayanotoxins are believed to be the toxic substances of these plants, and are found in its leaves, flowers and nectar. Grayanotoxins in the honey may cause the negative chronotropic effects. A possible mechanism of action is binding of the toxin to sodium channels in the cell membrane, resulting in a constant state of depolarization. This results in a decreased action potential, causing dysfunction of the sinoatrial and atrioventricular nodes. Another mechanism might be stimulation of the vagus nerve. Both modes of action result in bradycardia and hypotension. No deaths due to wild honey poisoning have been documented so far. Supportive treatment, consisting of infusion of normal saline and positive chronotropic agents if needed, commonly facilitates recovery within 24 hours. Conclusion: Although rare, wild honey poisoning should be considered as a potential cause of hypotension and bradycardia. MRI of the lumbar spine was performed because of the suspicion of spondylodiscitis, and showed inflammatory changes dorsal of vertebrae L3-L5 with a small pocket at L5. The patient was treated with i.v. flucloxacilline for 6 weeks, but did not recover. Several blood cultures and a needle biopsy of the pocket at L5 showed no bacterial agent. Auto-immune antibodies, rheumatoid factor and anti-citrulline antibodies were all negative. Subsequently, he developed pain at his neck and right shoulder. A malignancy was ruled out by shoulder X-ray and bone scintigraphy. We performed a FDG-PET-computed tomography study in order to find a systemic inflammatory disease or infectious focus. This showed enhanced FDG-uptake in shoulders, back and hips. This pattern has been described in patients with polymyalgia rheumatica, and so we started treatment with prednisone. The pain decreased in 2 days and inflammatory markers declined. Three months later the inflammatory changes on MRI had disappeared as well. Conclusion: Typical PMR is a clinical diagnosis after exclusion of other disorders. When patients do not present with the typical features, imaging studies like MRI or PET-CT may be helpful in making a diagnosis by excluding other possibilities, as in our case. Moreover, interspinal bursitis on MRI and increased FDG-uptake in shoulders, back and hips on FDG-PET-CT might be suggestive of PMR in these patients. 236. Wild honey: not so sweet after all? M. Wester, R. van Eijk, R.J. Walhout, J. Zeelenberg Gelderse Vallei Hospital, Department of Internal Medicine, Willy Brandtlaan 10, 6716 RP EDE, the Netherlands, e-mail: westermaarten@gmail.com was acetylsalicylic acid because of PTCA 10 years before. There were no other complaints than fever and arthralgias, particularly of both feet, but the hands en knees were involved as well. On the first day of presentation he had fever of 38.7 degrees centigrade, and a non-pruritic rash on both legs, no obvious signs of arthritis. Laboratory examination revealed a raised CRP, and a mild proteinuria. Serological tests for ANA, ANCA, and reumatoid arthritis remained negative. Further analysis, which included blood cultures, an ultrasound of the abdomen, an X-ray of the chest, an analysis of a urine specimen and testing for multiple myeloma, revealed no abnormalities. A performed skin biopsy showed a leukocytoclastic vasculitis with the presence of C3 within the walls of small capillaries. No antibiotics were administered, as our patient did not appear very ill and did not fulfill the SIRS criteria. During his hospital stay his daughter told us that a family trip to Suriname was planned and that they had received DTP and hepatitis A vaccination 10 days before. As other causes for the clinical presentation were ruled out, we concluded that the patient most probably suffered from a severe serum sickness reaction against his recent vaccinations. Because of the severely painful arthritis he had developed during his hospital stay, oral corticosteroids were started. A few days later the pain and arthritic pain resolved. Unfortunately, their family vacation had to be skipped. Conclusion: We present a man with a classic serum sickness reaction with arthralgias, arthrititis and fever after a vaccination against Hepatitis A and DTP. This case shows that an extensive history is an important tool for making this clinical diagnosis. Serum sickness is a known, but rare complication of vaccinations. change. Papilledema was not present. We were consulted to evaluate for possible underlying internal causes of the hydrocephalus. Chest imaging showed bihilar lymfadenopathy and histology of a mediastinal lymph node revealed non-caseating granulomas, compatible with sarcoidosis. At 37-weeks of gestation she delivered a healthy daughter. After delivery, her neurologic complaints progressed. Ventriculostomy did not reduce the symptoms. However, prednisolone 1mg/kg resulted in rapid disappearance of symptoms. MRI showed complete resolution of the hydrocephalus within 3 weeks after the start of prednisolone. Literature review. Many internal diseases can cause a hydrocephalus. Particularly infections, tumours and autoimmune disorders must be considered. Hydrocephalus is a rare manifestation of sarcoidosis (0,25% of cases). Sarcoidosis presenting with a hydrocephalus is even rarer and poses a substantial diagnostic dilemma. Sarcoidosis can cause an obstructive hydrocephalus by fourth ventricular outflow obstruction or a communicative hydrocephalus due to reduced absorption of liquor in the basal cisterns. Of all manifestations of neurosacoidosis, hydrocephalus has the worst long-term prognosis with a mortality rate of 75%. Diagnostic criteria for neurosarcoidosis have been proposed by Zajicek et al. who define possible, probable and definite neurosarcoidosis. A nervous system biopsy is necessary to establish a diagnosis of ‘definite’ neurosarcoidosis, however this is not always feasible. Our patient met the criteria for ‘probable’ neurosarcoidosis. High-dose corticosteroids are widely accepted as the first line of treatment. Conclusion: Hydrocephalus can be the presenting manifestation of sarcoidosis. An acquired hydrocephalus in adults can have many non-neurological causes. The internist can play an important role in the differential diagnosis of hydrocephalus. Adequate diagnosis of the underlying disease requires a multidisciplinary approach. Treatment of hydrocephalus due to neurosarcoidosis consists of high dose steroids and on demand ventriculostomy. 238. Hydrocephalus, a rare manifestation of sarcoidosis 237. Serum sickness: vacation of vaccination? Case report: Patient A is a 36-year-old male who presented with palpitations, nausea, vomiting and sweating. He had no relevant medical history and was not using any medication. The symptoms occurred a few hours after ingestion of wild honey for gastrointestinal symptoms. Physical examination was unremarkable except for hypotension (BP 98/48 mmHg) and a severe bradycardia of 37 beats/min. Electrocardiography showed a sinus bradycardia of 40 beats/min with normal conduction times. Haematological and biochemical laboratory investigations were normal. Treatment consisted of normal saline intravenously only. Within a few hours blood pressure and pulse returned to normal values. Patient B is a 42-year-old male who was referred because of weakness, sweating, dizziness, nausea and vomiting. He had no relevant medical history and did not use any medication. His complaints started two hours after eating yoghurt with wild honey. Physical examination once more was M.J. Cruijsen, C. Richter, M.M.C. Hovens Rijnstate Hospital,Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: mcruijsen@alysis.nl Introduction: Classic serum sickness describes the syndrome of a ‘type III’ of immune complex- mediated hypersensitivity disease. The most common symptoms are rash, fever, malaise, and polyarthralgias or polyarthritis. They are caused by immunization of the host by heterologous (non-human) serum proteins, developing one to two weeks after first exposure to the responsible agent. Diagnosis is often delayed, as this syndrome resembles more common infectious diseases Case report: A 76-year-old man was presented to the emergency ward because of fever, chills, and extremely painful feet since 10 days. The only medication he used 126 G.S. Mijnhout, J.M. van Rooijen, T.T.A. Aalders Isala Clinics, Department of Internal Medicine, Dr. van Heesweg 2, 8025 AB ZWOLLE, the Netherlands, e-mail: g.s.mijnhout@isala.nl 239. The unidentified angel W. Vercoutere, J. Buijs, C. van Deursen Atrium Medical Centre Parkstad, Department of Internal Medicine, H. Dunantstraat 5, 6419 PC HEERLEN, the Netherlands, e-mail: wardvercoutere@yahoo.com Introduction: Sarcoidosis is a multisystem granulomatous disorder of unknown origin typically affecting young adults. The organs most commonly involved are the lungs, skin and lymph nodes. Involvement of the nervous system occurs in 5% of patients with sarcoidosis. We present a patient with a hydrocephalus as the presenting manifestation of sarcoidosis. To our knowledge only few cases have been reported. Aim: Case report and review of the literature. Case report: A 36 weeks pregnant woman developed a symptomatic non-communicating hydrocephalus. She had a 6-week history of progressive nausea, vomiting, dizziness, diplopia and headache precipitated by position Introduction: A 61-year-old man was referred to the hospital with nausea, vomiting and watery diarrhoea. One day before admission he received a present of his friend, consisting of a collection of freshly picked mushrooms. Being a connaisseur of mushrooms, he prepared himself a meal consisting of Boletus edulis (penny bun), Cantharellus cibarius (golden chanterelle) and two unidentifiable mushrooms. 127 Introduction: Worldwide, proton pump inhibitors (PPI’s) are one of the most frequently prescribed drugs. Although considered safe, the following case-report demonstrates a rare but life-threatening skin-disease that can occur as an adverse reaction to omeprazole. Case report: A 50-year-old female presented to her general practitioner with stinging eyes and a rash on her chest. Four weeks earlier she had been started on omeprazole for abdominal complaints. Since a toxic dermatitis was suspected, omeprazole was terminated immediately. 48 hours later however the rash had worsened and the patient was referred to our hospital. On examination a generalized rash with erythematous macules and dusky centres was noticed. She also had extensive oral and genital ulcerations, conjunctivitis and blepharitis. Urine sediment analysis showed signs of a cystitis. The most likely diagnosis was erythema multiforme major (EMM) caused by an urinary tract infection. The patient was admitted and received antibiotics. Within the next 24 hours the rash became confluent and desquamative, with multiple vesicles growing into bullae followed by erosion of the skin and mucous membranes, eventually affecting more than 40% of her body-surface area (BSA). The clinical picture and extensiveness of the BSA involved were now concomitant with toxic epidermal necrolysis (TEN). A skin biopsy revealed chronic inflammation suiting a diagnosis of either TEN or EMM. Urine and blood cultures remained negative. With the absence of other recently initiated drugs and no sign of infection, TEN was attributed to omeprazole. Treatment was initiated with high dose prednisolone, hydration and nutritional support. Because of the specialized wound care that was required the patient was transferred to a dermatological ward in an academic hospital. Shortly after her transfer the skin condition stabilized and the steroids were weaned. Subsequently the denuded skin re-epithelialized. After two weeks she could be discharged with a lifelong absolute contraindication for PPI’s. Conclusion: Considering the incidence of 1 per one million people annually and a mortality rate of 35%, TEN is a rare but life-threatening adverse drug reaction. Although TEN is mostly related to specific types of drugs (allopurinol, penicillins, carbamazepine and NSAID’s), many other agents have been implicated in a smaller number of cases. So far only five cases of TEN caused by omeprazole have been reported in literature. This case report illustrates that even commonly prescribed drugs like PPI’s can cause severe adverse drug reactions. Early recognition is important and clinicians should be aware of the possibility of TEN. Case report: On examination in the hospital he showed normal vital signs and slight tenderness of the abdomen. Serum alanine-aminotransferases were slightly elevated (84 U/l), alkaline-phosphatase, bilirubin and coagulation tests were normal. C-reactive protein and creatinine were 31 mg/l and 120 mmol/l, respectively. Given the history and symptoms, amatoxin poisoning was suspected. Silibinin (milk thistle, Silybum marianum) and acetylcysteine were started as antidotum. The next days he remained clinically stable, although laboratory tests revealed increasing transaminases and declining liver synthesis parameters. On day 4 he suffered from hemorrhagic diarrhoea, hypotension, anuria, high-anion gap metabolic acidosis and severe impairment of liver function (albumin 25.9 g/l, APTT 64 sec, INR 6.38, bilirubin 73.8 umol/l, LDH 5000 U/l, transaminases > 3000 U/l). He was referred to an academic hospital and underwent an immediate liver transplantation. Nevertheless, he died after surgery. Pathological examination of the native liver showed massive cellular necrosis. Discussion: This case illustrates the clinical course of a lethal mushroom poisoning, caused by amatoxin (Amanita phalloides, ‘death angel’). The LD50 of amatoxin is very low, i.e. 0.1 mg/kg body weight, reflecting the weight of only one mushroom. Amatoxin interacts with RNA polymerase-II, leading to decreasing mRNA-concentrations, deficient protein synthesis and cell death. Intestinal mucosa, liver and kidneys are the most susceptible organs. Silibinin inhibits the enterohepatic cycle of amatoxin. N-acetylcysteïne impairs toxicity by reducing glutathione in hepatocytes. Amatoxin poisoning is classically divided into four phases. After a latency period of 8-12 hours, gastrointestinal symptoms start. Since non-hepatotoxic mushrooms induce gastrointestinal symptoms 1-2 h after ingestion, amatoxin intoxication should be considered when a longer latency-period occurs. In the second phase, oliguria, electrolyte/acid-base disturbances and renal failure occur. In the third phase, diarrhoea ceases, leading to clinical improvement. However, after 36-48 h signs of liver involvement may appear, ranging from asymptomatic increase of transaminases to full-blown acute liver failure. Conclusion: The incidence of mushroom poisoning varies over the world, depending on local traditions, life-style and occurrence of wild mushrooms. Although the incidence of mushroom intoxications is low in the Netherlands, patients and clinicians should be aware of the hazardous consequences. 240. A rare side effect of a common drug J. van der Kraan, S. Anten Rijnland Hospital, Department of Internal Medicine, Simon Smitweg 1, 2353 GA LEIDERDORP, the Netherlands, e-mail: j.vd.kraan@rijnland.nl 241. First degree atrioventricular block due to acute ethanol intoxication D.A. Geerse, G.J. Creemers 128 with fever. Twenty hours before presentation, the father had attempted to remove a colony of greenish Zoanthids (soft corals) from a rock in his tropical sea aquarium by putting the rock in a bucket of boiling tapwater. This produced an offensive odour, which was inhaled by all four family members. Immediately after touching the corals, the man experienced paresthesias and pruritus in his right arm lasting about ten minutes. A few hours later, the man started to feel unwell. He reported a metallic taste in his mouth, nausea, headache, shivering and severe muscle cramps. On physical examination, he had a blood pressure of 100/60 mmHg, pulse rate 100/min and temperature 38 °C. Further physical examination revealed no abnormalities. Blood analysis showed leukocytosis (22.9 * 109/l) and elevated CRP (174 mg/l). His wife and children had similar – but less severe – symptoms and signs, all three had fever > 38.5 °C. Based on the clinical history in combination with the description of the soft coral, a clinical diagnosis of palytoxin-intoxication secondary to (dermal and) inhalational exposure was made. All family members fully recovered within 48 hours with supportive therapy. Discussion: Palytoxin (PITX, PTX) is a very potent marine toxin that converts the membrane sodium-potassium pumps, responsible for maintaining ionic gradients critical to cellular function (Na+/K+-ATPase), into nonspecific ion channels. PTX has been found mainly in certain tropical soft corals (Zoanthid) and bentic dinoflagellates (Ostreopsis sp.). Cases of severe intoxication after ingestion of tropical sea fish containing palytoxin (derived from eating these corals/plankton) have been described, with symptoms ranging from paresthesias, fever, dysguesia, myalgia and nausea, to more severe with rhabdomyolysis, myocardial damage and death. In the literature, two cases of toxicity after dermal contact with Zoanthids from home sea aquaria and two case reports describing intoxication after inhaling a foul odour liberated by pouring boiling water on Zoanthids from home aquaria were identified. There is no antidote known for this toxin, supportive care is recommended. Conclusion: Due to improved home marine aquarium techniques, aquarians are potentially exposed to (un) known sickening entities such as palytoxin. Aquarians and their healthcare providers should be aware of these potential risks. Catharina Hospital, Department of Internal Medicine, Michelangelollaan 2, 5623 ER EINDHOVEN, the Netherlands, e-mail: dgeerse@hotmail.com Introduction: Ethanol intoxication can lead to cardiac conduction disturbances such as prolongation of the QTc interval, possibly leading to lethal arrhythmias. It has also been shown to increase the PR-interval in healthy individuals. Few case reports exist of atrioventricular (AV) block caused by acute ethanol intoxication. Case report: A 26-year-old man was brought into the emergency room with an acute ethanol intoxication. He was found comatose after drinking large amounts of liquor. On arrival of the ambulance, he was unresponsive to pain. He regularly drank large amounts of alcohol, he did not use illicit drugs and was otherwise healthy. On physical examination he had an ethanol foetor and was somnolent. Blood pressure was 120/75 mmHg, with a regular pulse of 86/min. He had a snoring respiration with a frequency of 12/min, with a SpO2 of 96% while breathing ambient air. His core temperature was 34.7 °C and he had cold extremities. Further examination showed no abnormalities. Laboratory evaluation showed normal serum potassium, sodium and calcium values. No other abnormalities were found. An electrocardiogram showed a sinus rhythm with a frequency of 88/min and a markedly prolonged PR-interval of 300 msec. The QTc was 464 msec. There were no other abnormalities and no second degree AV block on continuous monitoring during the first hour in the emergency room. After this hour, his consciousness improved and he was able to answer questions. He was given intravenous fluids and was admitted to the ward for further observation. An electrocardiogram was repeated 8 hours later; this showed normalization of the PR-interval to 172 msec. He was feeling well at this time and was discharged. Discussion: This case describes a transient first degree AV block in a patient with ethanol intoxication. Ethanol has a direct inhibitory action on the cardiac conduction system and may cause prolongation of the PR-interval, and even third degree AV block. Clinicians should be aware of this possibility when confronted with patients with ethanol intoxication. 242. A febrile family after handling soft corals from a marine aquarium 243. How fast does an atrial myxoma grow? L.L. Snoeks, J. Veenstra Sint Lucas Andreas Hospital, Department of Internal Medicine, Jan Tooropstraat 164, 1061 AE AMSTERDAM, the Netherlands, e-mail: l.snoeks@slaz.nl J.M.J.B. Walpot 1 , B. Shivalkar2 , J. van Zwienen 1, W.H. Pasteuning1 1 Admiraal De Ruyter Hospital, Department of Cardiology, Koudekerkseweg 88, 4380 DD VLISSINGEN, the Netherlands, e-mail: j.walpot@adrz.nl, 2University Hospital Antwerp, EDEGEM-ANTWERP, Belgium Case report: A family of four (father 37, mother 35, twins 10 years old) presented simultaneously to the emergency room 129 Introduction: The growth rate of atrial myxoma in humans is not known, as the diagnosis of such lesions implies surgical excision to prevent embolic events. Reports with documented growth rate are very rare. Case presentation: We report the case of a 65-year-old woman, in whom a left atrial mass of 4.5 x 3.2 cm was seen on a routine transthoracic echocardiogram. She was in follow-up for mixed aortic valve disease. A year earlier, the transthoracic echocardiogram could not document an atrial mass.Histology diagnosed a myxoma. The calculated growth rate was 0.375 cm/month. The growth rate of cardiac myxoma is not known. We performed a search in the medical literature and added one new case. A Med-line search with the terms ’myxoma and tumor growth’ was done. All case reports with a documented growth rate were selected. Cases with recurrent myxomas were excluded. Twelve case studies were found. The calculated growth rate was 0.49 cm (rang 0-1.36 cm) per month. Conclusion: Reports with documented growth rate of cardiac myxomas are very rare. These reports suggest the growth rate of these lesions may be faster than we think. was noticed that she had polyuria. Afterwards the patient reported having polyuria and – polydipsia for three years. A diagnosis of sarcoidosis was considered. Further analysis with CT scan of the chest and MRI of the pituitary showed small hilar and intrapulmonal lymphnodules, a thickened aorta, and a mass in the pituitary gland. PET-CT showed increased hilar and intrapulmonary tracer uptake, and intense uptake in the aorta, suggesting aortitis. Histologic examination of the extramedullary tumour revealed a granulomatous inflammation. Auramine staining, PCR and culture showed no mycobacteriae. In conclusion, our patient had a rare presentation of a combination of neurosarcoidosis with spinal as well as pituitary localisations, and systemic sarcoidosis complicated by aortitis. The patient was treated with prednisolone, desmopressin and anticoagulants. During therapy recovery of polyuria and -dipsia and mild improvement of the neurologic symptoms occured. Discussion: Sarcoidosis is an inflammatory disease of unknown aetiology characterised by the presence of noncaseating granulomas. Mycobacterial and fungal infections as well as malignancy should be ruled out. Sarcoidosis can effect any organ, most commonly lymph nodes, lung, liver, skin and eye. On rare occasions the nervous system and (large) blood vessels may be involved in the disease process. Cornerstone in the treatment of sarcoidosis are corticosteroids. 244. A woman with rare manifestations of a common disease J.P. Post, H.M.A. Hofstee VU University Mmedical Centre, Department of Internal Medicine, Boelelaan 1117, 1081 HV AMSTERDAM, the Netherlands, e-mail: jp.post@vumc.nl 245. A rare case of dyspnea due to bisacodyl abuse I.M. Dijkstra, H.R. Koene, V.H.M. Deneer, I.A. Eland, I.M.M.J. Wakelkamp St. Antonius Hospital, Department of Clinical Chemistry, PO Box 2500, 3430 EM NIEUWEGEIN, the Netherlands, e-mail: info@congresservice.nl Case: A 58-year-old woman was admitted to the hospital with a 3-month history of progressive muscle weakness, sensory loss, and unsteady walk, eventually progressing to paraplegia. Her past medical history included type 2 diabetes mellitus, hypertension, chronic obstructive pulmonary disease, and pulmonary nodules that had not changed in size for two years. The patient’s father died of morbus Wegener. On physical examination the patient had paralysed lower extremities, hypesthesia and hypalgesia below the dermatome corresponding with the 6th thoracic vertebra, bilateral Babinski’s response, and absent patellar and achilles reflexes. Also there was swelling and redness of the left leg. No other abnormalities were observed, especially no lymphadenopathy, masses, skin changes, hepatosplenomegaly, or swelling of the joints. MRI of the spine showed a large epidural mass extending from the 2nd to the 6th and a smaller mass near the dorsal corpus of the 10th thoracic vertebra. Compression ultrasonography showed a deep vein thrombosis of the left vena poplitea. After the insertion of a vena cava filter, a decompressive and diagnostic laminectomy was performed. At the postoperative ward the patient developed hypernatremia, and it Introduction: Bisacodyl, a contact laxative, can be obtained without prescription. Adverse side effects of (excessive) bisacodyl use are kidney stones, dehydration, hypovolemia and secondary hyperaldosteronism. Aim: We here present bisacodyl abuse as an explanation for most clinical symptoms in a patient with a history of a JAK2-V617F-negative thrombo- and erythrocytosis and a recently discovered adrenal incidentaloma. Case history: A 41-year-old woman was seen at our emergency room with dyspnea, polydipsia and polyuria. The medical history reported kidney stones and thromboand erythrocytosis most likely due to a myeloproliferative disorder. However, no significant bone marrow abnormalities were observed and JAK-2 (V617F) mutation analysis was negative. Three years earlier, a pulmonary embolism was diagnosed and she was treated with fenprocoumon, hydroxyureum, and occasional phlebotomy. 130 Physical examination revealed no abnormalities and normal blood pressure (116/81 mmHg). Arterial blood gas analysis showed a respiratory compensated metabolic acidosis (pH 7.42, pO2: 14.2 kPa, pCO2: 3.8 kPa, HCO3: 18.4mmol/l, BE: -4.9). Besides hyponatremia (128 mmol/l), elevated creatinin (94 mmol/l) and known erythro- and thrombocytosis, no abnormalities were found in the lab. No evidence of pulmonary embolism was seen on the CT scan. However, an enlarged left adrenal gland was observed. Hormonal evaluation excluded pheochromocytoma and Cushing’s syndrome, but showed secondary hyperaldosteronism (plasma renin activity (PRA): 28,000 fmol/l/sec, 16x upper reference limit (URL)) and aldosteron: 40000 pmol/l, 47x URL). Although saline infusion markedly decreased PRA (3500 fmol/l/sec, 5x URL) and aldosteron (5000 pmol/l, 11x URL) levels, they remained significantly elevated. The patient repeatedly denied use of laxatives or diuretics and reported normal stools and no excessive sweating. A salt loading test was performed for 5 consecutive days during which she was asked to ingest 6 grams of salt per day, collect urine and register fluid intake. Blood, urine, weight and blood pressure were analysed daily. Average daily fluid intake was 3.5 litres, while urine production was 1.2 litres. Her weight remained 59 kg and blood pressure stayed normal. Because of persistent low bicarbonate levels, screening for laxative in urine was eventually conducted. All urine samples contained bisacodyl metabolites. Conclusion: Bisacodyl use was demonstrated in a patient presenting with dyspnea, polydipsia, polyuria and adrenal incidentaloma. Laxative abuse and subsequent dehydration explains the electrolyte disturbances, metabolic acidosis, shortness of breath and secondary hyperaldosteronism, most probably causing adrenal hyperplasia. Also, the haematological abnormalities and previously reported kidney stones are possibly due to dehydration. started in 2009, but no other actual complaints. On examination a bradycardia of 46 beats per minute and a relative hypotension of 106/54 mmHg were noted without other abnormalities. EKG registration demonstrated an AV-nodal rhythm without signs of ischemia. Hematology and clinical chemistry were unremarkable. Within several hours after admission, spontaneous recovery of sinus rhythm and blood pressure was observed. Discharge without a definite diagnosis followed. Both the Holter registration and the exercise EKG subsequently performed in the outpatient clinic appeared normal. Strikingly, it turned out that the roommate of our patient experienced a similar faintness during the admittance of our patient. Though much milder in character, this roommate too reported self-limiting symptoms that had developed shortly after breakfast. As both our patient and his roommate had consumed wild honey of Nepalese origin, a suspicion on a food related toxic origin was raised. With hindsight, the symptoms of both subjects seemed highly characteristic for Mad Honey Poisoning. Chemical analysis of the honey by the Dutch food authority confirmed the presence grayanotoxin, the causative toxin. Yet in Antiquity, the toxicity of honey and even its military exploitation were reported. Currently, small amounts of wild honey are being advocated as an alternative medicine for gastrointestinal discomfort and sexual dysfunction. The clinical picture of mad honey poisoning is grossly cholinergic consisting of bradycardia, hypotension, perspiration, salivation, blurred vision, lightheadedness and even loss of consciousness. Symptoms arise through blockade of sodium channels by grayanotoxins originating from Rhododendron nectar. Symptoms develop within minutes to hours after ingestion, are rarely fatal and generally last for no more than 24 hours. Treatment is mainly supportive, consisting of atropine for symptomatic bradycardia and intravenous administration of fluids in case of hypotension. Conclusion: Symptomatic bradycardia may be due to atherosclerotic disease, especially in the presence of cardiovascular risk factors. The differential diagnosis is nevertheless extensive and includes food related toxins. Given the increasing number of worldwide travelers in addition, clinicians should be attentive to exotic causes of intoxication. 246. A sweet surprise D. Dekker1, P. Mulder2, R.F. van Es3, P. Smits1 1 Radboud University Medical Centrem, Department of Farmacology/Toxicology, PO Box 9101, 6500 HB NIJMEGEN, the Netherlands, e-mail: douwedekker@hotmail.com, 2Voedsel en Waren Autoriteit, WAGENINGEN, the Netherlands, 3 Hospital Bethesda, HOOGEVEEN, the Netherlands 247. Rhabdomyolysis as complication of the new designer drug MDPV Case: a 64-year-old male presented at the emergency department with a sudden faintness consisting of lightheadedness, perspiration and nausea which occurred shortly after breakfast. Several days before, he returned from a holiday in Nepal. The medical history revealed obesity, systolic hypertension and thrombosis of the central retinal vein of the left eye for which aspirin was T.T.H. Nguyen, S.C.E. Klein Nagelvoort-Schuit, A. Govers Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: hien277@hotmail.com 131 Introduction: In the fall of 2009 the health authorities decided to start mass vaccination for the H1N1 virus because of the ongoing pandemic in an attempt to prevent excess deaths caused by infection by this new influenza virus. Although the expected rate and morbidity of side effects of the vaccine are very low, rapid mass vaccination in groups at risk can lead to a wide range of problems. The possibility of serious mistakes should at least be a matter of consideration when rapid mass vaccination is initiated. Safety protocols should be available and in routine use wherever parenteral medication is administered. Case report: A few weeks after the start of the H1N1-vaccination campaign, 11 patients from a nursing home were admitted to the emergency-department. During the vaccination procedure in the nursing home 50 Units of Insulin Glargine were mistakenly administered to all 11 patients instead of the H1N1 vaccine. In the emergency department all patients were rapidly treated with intravenous administration of glucose. In two patients a single episode of hypoglycaemia was treated successfully. Four other patients developed hypoglycaemia which persisted for 24 hours despite glucose infusion. One of these four patients died during admission, possibly of heart failure. Conclusion: In the Netherlands drug-related physical complaints lead to an estimated 19.000 admissions a year and 1200 deaths. The number of cases of in-hospital drug-related harm may rise up to 30.000 a year. We report a serious and possibly very harmful mistake in the administration of H1N1 vaccine which caused hospitalization in 11 patients, severe hypoglycaemia in at least four patients and one death. Although the indication for influenza vaccination in patients at risk is valid, as any medical procedure, mass vaccination can lead to mistakes, which can have very serious consequences. Especially in patients with underlying morbidity, such as the population in nursing homes, safety procedures should be followed to prevent health damage. Introductions: The use of psycho stimulant drugs have been greatly increased since the last two decades. ‘Designer drugs‘ are new drugs, which are created to avoid the current drug laws, and/or to enhance the psychoactive effect of existing drugs, usually by modifying the molecular structures. Methylenedioxypyrovalerone (MDPV) is a new designer drug; this recreational drug is not as innocent as being said, as the next case illustrates. Case report: A 21-year-old male, with a history of drugsinduced psychosis and possible schizophreniform disorder, was seen in the Emergency Department because of an auto-intoxication. Anamnestic evaluation reveals that he used MDPV since 5 months, but now he has taken a much larger dose than normal, the exactly amount was unclear. At the Emergency Department he was anxious, agitated and extremely paranoid, with hyperkinesia. His blood pressure was 150/100 mmHg, with a pulse of 132 bpm, the rest of the physical examination was unremarkablel. Laboratory assessment revealed a creatinine of 214 umol/l, urea 11 mmol/l, creatininekinase 13.508 U/l, WBC 39 x 109/l, CRP 12 mg/l. At the Emergency Department he refused urine examination. An ultrasound of the kidneys didn’t show any abnormalities. The diagnosis was rhabdomyolysis due to MDPV-abuse and also a MDPV-induced psychosis. The leukocytosis was attributed to extreme stress; there were no signs of infection. Treatment consisted of proper rehydration according to the guidelines for rhabdomyolysis, and Haloperidol for the psychosis. After a few days the laboratory findings were fully normalized and he was transferred to the psychiatric ward. Discussion: MDPV is a new psychoactive drug chemically related to Methylphenidate (but more potent), Pyrovalerone (PV) and Methylenedioxymethamphetamine (MDMA). It is assumed that it behaves as a norepinephrine-dopamine reuptake inhibitor, and to a lesser extent as a serotonin reuptake inhibitor. The acute physical effects include hypertension and tachycardia; the mental effects are euphoria, increased awareness and arousal, anxiety and agitation. On the internet forums high doses have been reported to give prolonged panic attacks and even psychosis. Side effects are presumed to be similar to PV and MDMA, long term effects and toxic dose are not known yet. Conclusion: Using the recreational drug MDPV is not always without consequences, beware of adverse events such as rhabdomyolysis and drugs induced psychosis. transurethral resection of the prostate. This so called TUR syndrome occurs in up to 20% of prostate operations. The major risk factor for hyponatremia is the volume of irrigant that is absorbed. Procedural risk factors for excess fluid absorption during endoscopic procedures include the type of procedure, introduction of fluid at high pressure, visceral perforation, prolonged duration of the procedure and type of anesthesia. Case: A 45-year-old woman, with a history of hypertension was admitted to the hospital for hysteroscopic resection of fibroids. Medication consisted of amlodipine, valsartan, hydrochlorothiazide and amitryptilline. At preoperative screening all laboratory results, including the sodium level were normal. During hysteroscopy 6 liters of non-conductive (non-electrolyte) distension fluids (1.5% glycine) were used, of which 500 ml fluid was absorbed during the procedure. During postoperative recovery the patient complained of nausea and malaise. Laboratory findings showed a hyponatremia of 119 mmol/l. She was treated with hypertonic saline and a furosemide. Her serum sodium level increased to 124 mmol/l. With an 0.9% saline infusion, her sodium level returned to normal, 140 mmol/l, by which time she was asymptomatic. Hyponatremia in this patient occurred shortly after hysteroscopic surgery, during which she absorbed 500 ml of glycine irrigant. Hyponatremia is most likely due to the absorption syndrome. It has been described that symptomatic hyponatremia associated with glycine irrigation requires fluid absorption of at least 1000 ml. However this case shows that it is also possible to develop symptomatic hyponatremia with less fluid absorbed during hysteroscopic procedure. Conclusion: Hyponatremia should be suspected whenever large volumes of nonconductive irrigation fluids have been used or when patients develop new neurologic symptoms during postoperative recovery, like nausea. This case underlines the importance of monitoring the amount of fluid absorbed during surgery so that patients at risk for severe hyponatremia can be detected. Tracheal compression may simulate asthma and warrants further investigation. Case-report: A 23-year-old woman was seen at our hospital because of dyspnea and difficult swallowing. Physical examination showed no stridor. Hemodynamics and examination of heart and lungs were normal. Laboratory results including arterial blood gas analysis was normal. Chest X-ray showed possible compression of the trachea. CT-thorax revealed a right sided aortic arch associated with an aberrant left subclavian artery (LSA) originating from a Kommerell’s diverticulum. The trachea and esophagus were being compressed. Pulmonary function test showed a flattened inspiratory pattern. The bronchoscopic examination showed stenosis of the lower part of the trachea with a remaining lumen of 50%. A barium esophageogram revealed extrinsic compression of the esophagus. No congenital cardial abnormalities were found. Because of her symptoms and the risk of rupture of aneurysmal dilatation of the diverticulum surgical treatment was indicated. A left lateral thoracotomy was performed. The fibrous ligamentum arteriosum between the left pulmonary artery and the inferior edge of diverticulum of Kommerell squeezed the trachea and esophagus on their left lateral face against the retrotracheo-esophageal subclavian artery in the back and the ascending aorta on the right. The ligamentum arteriosum was cleaved and the diverticulum of Kommerell was reefed. She recoverd quickly and dyspnea and dysphagia disappeared. Discussion: A right sided aortic arch is a rare congenital defect of the aorta. The frequency is about 0.1%. In 50% there is an aberrant LSA. In 1936 Dr. Kommerell first reported an aberrant right subclavian artery (RSA) originating from the left descending thoracic aorta and associated with persistence of a remnant of the right dorsal aorta: a diverticulum from which the aberrant RSA originated. In contrast to the anomaly of a left aortic arch with an aberrant RSA patients with an right aortic arch with aberrant LSA are symptomatic because the trachea and esophagus are encircled by vascular structures. 5-10% have also cardial congenital abnormalities. Surgical intervention is recommended in symptomatic patients or asymptomatic patients with a large diverticulum. There is an increased risk of rupture with large diverticuli and there is an increased risk of thrombosis. Conclusion: It is necessary for physicians to recognize that the combination of tracheal or esophageal symptoms could be caused by an vascular anomaly. 249. Hyponatremia following hysteroscopic surgery I. Walhout, C.R.G.M. Daemen-Gubbels Tergooi Hospitals, Department of Internal Medicine, Van Riebeeckweg 212, 1213 XZ HILVERSUM, the Netherlands, e-mail: iwalhout@tergooiziekenhuizen.nl Introduction: Hysteroscopic procedures utilize large volumes of irrigating solutions. The use of these nonconductive (non-electrolyte) containing fluids has been associated with a number of complications including heart failure and volume overload. Hyponatremia is an uncommon complication following hysteroscopy. Severe symptomatic hyponatremia occurs in 0.06 to 0.2 percent of women. It is a well known complication after 248. An unexpected side effect of vaccination against the H1N1 virus. Safety first ! B. Flameling, W. de Graaff, M.H. Silbermann Tergooi Hospitals Blaricum, Department of Internal Medicine, PO Box 10016, 1201 DA HILVERSUM, the Netherlands, e-mail: bflameling@tergooiziekenhuizen.nl 132 250. Don’t forget a congenital vascular anomaly in the combination dyspnea and dysphagia E.A.J.E. Braam1, J.C. Antons2 1 Rijnstate Hospital, Department of Internal Medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: evelienbraam@gmail.com, 2Radboud University Medical Centre, NIJMEGEN, the Netherlands 251. Giant cell arteritis: when to PET and when not to PET? Introduction: Developmental abnormalities of the aortic arch affect approximately 3% of the general population. Clinical manifestations are uncommon. Symptoms usually occur because of compression of the trachea or esophagus. N.L.H. Bekkali1 , K.D.F. Lensen 2 , C.E.H. Siegert 3 , E.H. van der Poest Clement1, J. Bosma1 133 1 St.Lucas Andreas Hospital, Department of Internal Medicine-MDL, Jan Tooropstraat 164, 1061 DE AMSTERDAM, the Netherlands, e-mail: noorbekkali@hotmail.com 2VUmc, AMSTERDAM, the Netherlands Conclusion: The 18-FDG PET-CT should be considered in patients with high clinical suspicion for GCA despite negative ultrasonography and biopsy. Introduction: Early recognition of Giant cell arteritis (GCA) and instant treatment with glucocorticosteroids are essential to prevent severe organ dysfunction, blindness in particular. While temporal artery biopsy is considered the gold standard in diagnosing GCA, PET-CT is also gaining a more important role in diagnosing GCA. Here we present a patient who was diagnosed with GCA by PET-CT after negative results from both, biopsy and ultrasonography. Case report: A 50-year-old woman presented with a 2-weeks history of fever, fatigue, chest pain and a dry cough. The week prior to presentation she was treated with amoxicilline-clavulanic acid by her general practioner for bronchitis. Her medical history revealed asthma. She also reported right-sided headache, fever with cold chills and night sweats. After one week no infectious cause was found for the fever. Thereafter the patient started complaining of jaw claudication as well as painful shoulders. Biochemical tests showed an ESR of 117 mm/h with a CRP level of 70 mg/l and mild normocytic anaemia (haemoglobin level 6.7 mmol/l). Repeated blood cultures were negative. Serological testing was positive for ANA and negative for anti-dsDNA. Infectious serological testing, including HIV, was negative. Tested M-protein was negative. After one week, given the new complaints amongst which jaw claudication, GCA was considered. Therefore, a bilateral temporal artery ultrasonography was performed revealing no abnormalities. Also, a unilateral (right) temporal artery biopsy showed no signs of inflammation. Despite these negative findings, yet with significant clinical suspicion for GCA, a 18-FDG PET-CT scan was performed. The PET-CT revealed large-artery vasculitis, showing increased FDG-uptake in the proximal branches of the aortic root and entire aorta. MRA of the thorax was performed to exclude Takayasu’s arteritis. No signs of vascular narrowing or obstruction could be shown on MRA. Treatment with high doses of prednisone was started with direct symptom relief and temperature normalisation. Discussion: In this patient the combination of clinical features and positive results obtained by PET-CT-scanning were compatible with GCA. The presented patient demonstrates that negative temporal artery ultrasonography and biopsy does not necessarily exclude the diagnosis of temporal arteritis (Brack 1999 A&R, Janssen 2008 J Vasc Surg). In cases of a strong suspicion of this classical syndrome in internal medicine a 18-FDG PET-CT may be a valuable new gold standard to diagnosis. 252. An unusual cause of post-renal kidney failure P.J.E.J. van de Berg, V.C. Harris, P.S. van Dam Onze Lieve Vrouwe Gasthuis, Department of Internal Medicine, Oosterpark 9, 1091 AC AMSTERDAM, the Netherlands, e-mail: p.j.e.j.vandeberg@olvg.nl Introduction: In an elderly woman, the combination of unintentional weight loss, loss of appetite, general weakness and a retroperitoneal para-aortal mass leading to obstructive kidney failure is highly suggestive for malignancy. In the present case, however, an unusual non-malignant condition was responsible for the development of similar symptoms. Case: A 74-year-old woman was admitted to the hospital with generalized weakness, unintentional weight loss and loss of appetite. Two months previously, she had undergone bilateral angioplasty of the common iliac arteries. Physical examination was significant for a solitary solid mass that was palpable at the left sub-mandibular angle, which had features suggesting a malignant lymph node with ultrasound examination. Laboratory analysis of blood and urine revealed renal insufficiency, which was subsequently explained by the presence of a para-aortal mass obstructing both ureters. Suspecting a malignant lymphoma, an initial biopsy of the sub-mandibular lymph node was performed, however pathology results revealed a benign salivary gland tumor (Warthin tumor). Consequently, biopsy of the para-aortal mass was performed and revealed chronic fibrosing inflammation, consistent with retroperitoneal fibrosis. To regain urinary flow, pyelo-vesicular catheters were placed in both ureters. This intervention relieved the patient’s malaise and loss of appetite, and partly restored her kidney function (estimated GFR 55 ml/min). The retroperitoneal fibrosis was treated with high dose prednisolone for six weeks, slowly tapering the dose hereafter to 10mg per day. After three months of treatment, there was only a slight reduction in the size of the retroperitoneal fibrosis. Our intention is to treat the patient with prednisolone for the coming 1.5 years. During this time, bilateral pyelo-vesicular catheters will assure adequate urinary flow. Discussion: This case demonstrates an unusual cause of obstructive renal failure with a prevalence of 1.3 per 100.00 inhabitants. Although benign, the consequences of retroperitoneal fibrosis can be severe and treatment requires long-term glucocorticoid treatment. The insidious onset of the disease makes a quick diagnosis difficult. Interestingly, this patient underwent a percutaneous procedure of the 134 Conclusion: This case shows an impressive presentation of starvation causing hypotension, hypoglycemia and metabolic acidosis. The starvation being caused by a combination of reduced intake, gastric banding and pregnancy. The complaint of popping ears caused by tuba atrofy underlined her marked loss of fat supplies. Gastrical banding is increasingly used as treatment for obesity, many of these patients are women in a fertile age. This case stresses the importance of monitoring their nutritional state during pregnancy. iliac arteries two months prior to when the retroperitoneal fibrosis became clinically apparent. Perhaps the mechanical manipulation of the aorta and large arteries resulted in the ‘periaortitis’ which is thought to play a role in the pathogenesis of this disease. 253. A young woman with hypoglycemia, metabolic acidosis and popping ears M. Krikke, M. ten Wolde, N. Smit Flevo Hospital, Department of Internal Medicine, Hospitaalweg 1, 1315 RA ALMERE, the Netherlands, e-mail: nsmit@flevoHospital.nl 254. Unusual use of nutmeg C.G. Krol1, M.J.F.M. Janssen2 Leiden University Medical Centre, Department of Internal Medicine, Albinusdreef 2, 2333 ZA LEIDEN, the Netherlands, e-mail: cgkrol@hotmail.com, 2Rijnland Hospital, LEIDERDORP, the Netherlands 1 Case report: A 35-year-old woman presented at the emergency room with hypotension, nausea and vomiting. She had consulted her doctor days before with dizzy spells and general malaise. Four weeks earlier she had given birth to her second child, the pregnancy and birth had been without complications. Her symptoms started in the last term of the pregnancy. In addition she lost over 15 kilograms of weight in the last month and had complaints of popping ears, closing and opening continuously. Her past medical history only notes a gastrical band placing in 2000 due to obesity. Tachycardia, low blood pressure and tachypneau were seen on physical examination. Laboratory analysis showed a hypoglycemia of 2.7 mmol/l, metabolic acidosis with inadequate respiratory compensation and increased aniongap and ketonuria. The differential diagnosis considered M. Addison, insulinoma, M. Sheehan, gastroenteritis, infection, starvation, intoxication. Empiric hydrocortisone and fluids were started and further analysis was requested; cortisol levels, thyroid function, ACTH levels, all were within normal range. Cultures of blood and urine were also negative. The general condition of our patient improved. Further blood analysis revealed electrolyte imbalances; hypomagnemesia, hypofosfatiemia, hypokaliemia. When deepening the history patient confesses to low intake during her pregnancy. Also she notes that she did not adjust her gastric band as instructed during a pregnancy. This has resulted in starvation during pregnancy and the breastfeeding period, afterwards depleting her of her supplies. The starvation resulted in a higher keton production, causing a metabolic acidosis and her other symptoms and electrolyte imbalances. The hypoglycemia is caused by insufficient substrate for gluconeogenesis and glycogenolysis due to glycogen depletion. The ENT doctor was consulted. Her ears were clean of wax on examination and the eardrum showed no signs of pathology. Due to the loss of fat usually present in the tuba, atrophy of the tuba is seen causing the tuba to collapse causing a pressure difference resulting in popping ears. Introduction: Nutmeg is a spice, frequently used in Dutch and Asian cooking. Relatively unknown are the hallucinogenic and euphoric effects of nutmeg, and the adverse effects in case of nutmeg intoxication. Case: A 20-year-old woman with borderline personality disorder was referred to the emergency department by a psychiatric clinic. Her medical history included several hospital admissions because of intoxications with analgesics. On the day of the referral, she felt ‘down’ and searched the internet for a drug for self-harm when she read about nutmeg, which she bought at a local supermarket. After taking 10 g of nutmeg she complained of stomach ache and dizziness. A physical examination showed mild hypothermia and sinus tachycardia. She was admitted for observation and discharged after 24 h to the psychiatric clinic without sequelae. Discussion: Nutmeg is a frequently used spice, of which low quantity is generally enough to add flavour. In higher dosage, nutmeg has hallucinogenic and euphoric effects for which it is used mainly by drug abusers and students because of its low costs and availability. Due to its strong flavour and unpredictable and mild effects, wide-spread usage has not been reported. Symptoms appear 6 h after ingestion of at least 10 g of nutmeg and are related to its effects on the central nervous system, leading to agitation and lethargia. Anxiety, feelings of ‘doom’ and psychosis are reported, accompanied by visual hallucinations. Dry mouth, nausea and dizziness may also occur. Physical examination may show hypothermia, tachycardia or hypertension or, in rarer cases, hypotension and shock. Laboratory tests are usually unremarkable, and nutmeg intoxication cannot be biochemically confirmed. There is debate about the mechanism of toxicity. The symptoms are probably caused by myristicine, which is metabolized 135 to amphetamine- like substance leading symptoms similar to LSD intoxication. Symptoms disappear without sequelae after 24-48 h. Death due to nutmeg intoxication has not been described. Treatment consists of supportive measures, including fluid infusion and anti-emetics. In case of severe delirium, benzodiazepine treatment may be considered. In the event of haemodynamic instability, cardiovascular monitoring is indicated and other intoxications should be considered. Conclusion: The course of nutmeg intoxication is generally mild with disappearance of symptoms without sequelae within 24-48 hours. Treatment is mainly supportive. (75%) with SB lesions and in one (17%) without SB lesions. Serum levels of TNF-a, IL1ß and IL-10 were also elevated in one patient. Conclusion: DBE is a valuable and safe tool to evaluate the involvement of the entire gastrointestinal tract in BD patients possibly leading to a change in therapy. Inflammatory cytokines are involved, however no clear Th1 or Th17 profile was observed. XXV. IMMUNOLOGY/ALLERGOLOGY RESEARCH 256. DRESS syndrome; a case-report XXVI. IMMUNOLOGY/ALLERGOLOGY CASE REPORT M. Janssen, G.S. Bleumink Rijnstate Hospital, Department of Internal medicine, Wagnerlaan 55, 6815 AD ARNHEM, the Netherlands, e-mail: m3janssen@alysis.nl 255. Clinical use of small bowel evaluation by double balloon enteroscopy in Behçet’s patients with abdominal complaints Case: A 48-year-old man presented at the emergency department with fever, rash and diarrhea of one week duration. He also complained of headache and loss of appetite. Five weeks earlier he had switched his antiepileptic medication from levetiracetam to carbamazepine. He stopped using carbamazepine since start of the rash. On physical examination the patient had a temperature of 39.2 °C, blood pressure of 125/87 mmHG and pulse of 108 bpm. Exanthema, impressing as toxicodermia, was seen all over his body Laboratory results showed an increased white blood cell count of 19.8 x 109/l, high C-reactive protein (96 mg/l), acute renal failure, increased liver enzymes and prolonged coagulation tests, suggesting hepatic insufficiency. Because of suspicion of sepsis, our patient was started on cefuroxime and i.v. fluids. The rash was thought to be caused by an allergic reaction to carbamazepine. Post renal obstruction was excluded as a cause of renal failure. During follow-up despite administration of i.v. fluids his kidney function did not improve. Also, liverfunction tests, fever and rash did not improve after antibiotics. Hence the patient was started on methylprednison because of suspicion of interstitial nephritis by DRESS syndrome caused by carbamazepine. Eosinophils were determined in the blood count and were elevated. During his stay in the hospital repeated blood cultures stayed negative. Shortly after the start of corticosteroids his kidney function improved as did the other laboratory abnormalities. After cessation of glucocorticoid treatment, his symptoms recurred, therefore prednisone was started after another infusion of solu-medrol, which again led to improvement of laboratory abnormalities and clinical improvement. J.H. Kappen, J.A.M. Laar, P.B.F. Mensink, W.A. Dik, H. Hooijkaas, S. Lachman, P.L.A. Daele, P.M. Hagen Erasmus Medical Centre, Department of Internal Medicine, ’s-Gravendijkwal 230, 3015 CE ROTTERDAM, the Netherlands, e-mail: j.kappen@erasmusmc.nl Introduction: Gastrointestinal symptoms are often present in patients with Behçet’s disease (BD), but objective gastrointestinal inflammation occurs infrequently. Double balloon enteroscopy (DBE) enables visualization of the entire small bowel (SB) together with tissue sampling and thus enhances the yield of gastroentestinal investigations of BD patients with abdominal complaints. Evaluation of Th1 and Th17 skewed key BD-cytokines might improve the understanding of the pathophysiological processes in this systemic vasculitis. Aim: Evaluate small intestine involvement in BD using DBE. Patients and methods: 10 BD patients with therapy resistant abdominal complaints were evaluated with DBE. Serum cytokine profiles and lymphocyte subsets were analyzed. Results: SB lesions were identified in four (40%) patients. The SB lesions were located in the distal ileum in three, and distal jejunum and terminal ileum in one patient. In all patients the SB lesions were out of reach for conventional gastroduodeno- or ileocolonoscopy. No complications occurred during or after the DBE procedure. In two of the patients with SB lesion (50%) the serum C-reactive protein (CRP) was elevated, while one patient without SB lesions (17%) had an elevated CRP level. Serum IFN-y levels were elevated (> 10 pg/ml) in three patients 136 Background: DRESS syndrome stands for Drug Rash (or Reaction) with Eosinophilia and Systemic Symptoms. Symptoms can be severe and include exanthema, fever and involvement of one or more organs, including liver, kidneys and lungs. Mortality is about 10%. Classically it develops 1 to 8 weeks after start of the causative drug. Anti-epileptics are the most common drugs described as causing DRESS syndrome. It is hypothesized that hypersensitivity is induced as a result of abnormalities in production and detoxification of active metabolites of the causative drug. Treatment consists of discontinuing the causative drug. Often high-dose corticosteroids are given, but there is no evidence in medical literature that this influences the duration of symptoms or mortality of the DRESS syndrome. In our case glucocorticoids seemed to be effective in treating the DRESS syndrome, especially because of recurrence of symptoms after cessation of therapy. the pharmacist reviewed the data and contacted the prescribing physician, if necessary. Results: During the study period, the computer reported 271 times that the drug dose needed correction because of the renal function. However, in 210 cases the dose turned out to be correct (or too low !) and no further action was needed. In 36 cases improved renal function was a reason not to contact the physician. In 25 cases the pharmacist contacted the physician for advice. Drugs most frequently reported were: low molecular weight heparin (LMWH), various antibiotics, ACE inhibitors, metformin, pregabalin, allopurinol and amantadin. The most important was overdosage of LMWH in patients with renal failure, which may cause serious bleeding. Conclusion: In 60 days there were 246 reports, this would be approximately 1650 reports in a year, but only 25 phone calls were necessary (152 calls/year). However, very few serious problems were seen. Apparently, when prescribing drugs, most doctors take renal function into account. Still, drug surveillance such as described here, may prevent morbidity and mortality, and should therefore be continued. However, our system certainly needs improvement in view of the many unnecessary computer reports. XXVII. OTHER RESEARCH 257. Improving safety in prescribing drugs in patients with impaired renal function 258. Sarcopenia: can it be defined? F.H. Woudstra, C. Halma, D. Vogel Medical Centre Leeuwarden,Department of Internal Medicine, Henry Dunantweg 2, 8934 AD LEEUWARDEN, the Netherlands, e-mail: f hwoudstra@hotmail.com A.Y. Bijlsma, C.G.M. Meskers, R.G.J. Westendorp, A.B. Maier Leiden University Medical Centre, Department of Ouderengeneeskunde, Albinusdreef 2, 2333 ZA LEIDEN, the Netherlands, e-mail: a.y.bijlsma@lumc.nl Introduction: Because many drugs are excreted by the kidneys, renal failure may cause accumulation and unwanted drug toxicity. In hospitalized patients it is possible to combine the pharmacy drug data base and clinical data base (renal function) in order to track down inappropriately dosed drugs. By contacting the prescribing physician dosages may be adjusted and morbidity may be prevented. Aim: We examined retrospectively our programme to detect inappropriately dosed drugs in our hospital. Materials and methods: During a period of sixty days all patients admitted to the Medical Centre Leeuwarden (657 beds/28.700 admittances a year) were screened on appropriateness of dosing according to the KNMP Kennisbank ‘verminderde nierfunctie’. Data from the pharmacy drug database (Zamicom) and clinical database (GLIMS) were combined into an Acces database. The renal function was estimated by eGFR using the Modification of Diet in Renal Disease (MDRD) formula, without correction for body surface area (eGFR is in ml/min/1,73 m2). When the computer indicated that the drug dose needed adjustment, Introduction: Sarcopenia occurs as early as 30 years of age and may result in a loss of about 50% of muscle mass by the age of 80 years. Age related loss of muscle mass is related to detrimental outcome, i.e. functional impairments, falls and increased mortality. Since the term ‘sarcopenia’ was launched in 1988 by Rosenberg, not much progress has been made towards a widely accepted, scientifically and clinically useful definition. The long way from the observation of a phenomenon to a guidance for clinical decision making shows similarities with previous attempts to define the ‘age-related’ phenomenon osteoporosis. Even today physicians remain critical and keep thinking of better strategies to define the term osteoporosis. Aim: To get a firm grip on and explain the status quo of a definition of sarcopenia by a chronological comparison to the development of a definition of osteoporosis. Materials and methods: We first investigated the prevalence of sarcopenia in a large cohort of subjects of the Leiden 137 Longevity Study, emerging from five different existing definitions of sarcopenia using body composition values as measured by bioimpedance analysis. Furthermore, the chronology of the development of definitions for osteoporosis was assessed from subsequent editions of Harrison’s Principles of Internal Medicine and compared to current definitions of sarcopenia. Results: Within the Leiden Longevity study, comprising 311 middle aged women and 320 middle aged men a range of 0-3.6% women and 0-26.4% men fulfilled the criteria for sarcopenia depending on the applied definition. The prevalence of sarcopenia was not related to chronological age, when the five existing definitions were applied. A timeline of milestones of the history of osteoporosis definition development reflected the difficulties in defining sarcopenia during recent years. Conclusion: Prevalence of sarcopenia varies widely depending on used definition or cut-off point. It even can happen that no age-related loss of muscle mass is found at all. Difficulties in definition of sarcopenia are very similar to those of osteoporosis, e.g. in both cases it appeared difficult to discern pathology from inevitable age related decline and in both cases it is difficult to assess the functional consequences on an individual base. electrophoresis, glucose, and Troponin I were within normal limits. Rhythm monitoring was unable to detect arrhythmias or high degree conduction disturbances. Even in the presence of dizziness, the rhythm was normal. Neurological work-up did not show relevant abnormalities. The transthoracic echocardiographic (TTE) study showed mild to moderate left ventricular hypertrophy with preserved systolic function and impaired diastolic relaxation. There was left atrial compression due to the hiatus hernia. A CT scan of the chest documented that the stomach was nearly completely localized above the diaphragm. Left atrial compression was confirmed. TTE was repeated in fasting condition and after a copious meal. After the meal, there was severe compression of the left atrium, which could not be documented in fasting condition. A careful requestioning of the patient confirmed the time relation between the postprandial period and the episodes of dizziness and collapse. The patient was considered to be too aged to be submitted for surgical correction. He was told to use the same amount of calories in more frequent smaller meals. Domperidon was initiated. The conservative management resulted in complete relief of the symptoms. The medical literature on left atrial compression is rather limited. A Med-line search with the term ‘left atrial compression’ showed 271 hits. Only 17 cases, of which 11 with hiatus hernia, of left atrial compression due to structures of the gastrointestinal tract were found. Most of the patients were successfully treated with conservative management. Noteworthy, the median age of these patients was 75 years, suggesting that LAC due to a gastrointestinal structure is a disease of the elderly. Conclusion: We report the case of an 86-year-old man, who suffered from recurrent syncope caused by LAC due to a large hiatus hernia. Reports describing LAC are rare. Echocardiography is a reliable tool to confirm LAC and quantify the severity the compression. XXVIII. OTHER CASE REPORTS 259. A rare cause of syncope: left atrial compression due to a hiatus hernia J.M.J.B. Walpot1, J. van Zwienen1, W.H. Pasteuning1, B. Amsel2 1 Admiraal De Ruyter Hospital, Department of Cardiology, Koudekerkseweg 88, 4380 DD VLISSINGEN, the Netherlands, e-mail: j.walpot@adrz.nl, 2University Hospital Antwerp, EDEGEM-ANTWERP, Belgium Introduction: Symptomatic left atrial compression is a rare clinical condition causing left ventriculair inflow obstruction resulting in low output, with symptoms such as syncope, and retrograde increase in pressure throughout the pulmonary vessels with subsequent dyspnea. Case report: An 86-year-old male, with a medical history of a known asymptomatic hiatus hernia and polyneuropathy of unknown origin, was hospitalized because of a syncope. After a meal, he had briefly lost consciousness. The physical examination was unremarkable. The electrocardiogram showed sinus rhythm without ischemic or hypertrophic changes. A complete blood count, renal an liver function tests, inflammatory parameters, protein 138 I ND E X FIRST AUTHOR Aalderen, van Aarnoudse Achterbergh Agterhuis Ahmed-Ousenkova Alidjan Andreescu Andriessen Arwert Atiqi Barlo Beekman Bekkali Berg, van de Bethlehem Bierhoff Bijlsma Bijlstra Binnenmars Boeddha Bonnie Boog, van der Boot Boreen, van Borst, de Boslooper Boudewijns Boumans Braam Branger Brok, den Brouwers Bruin, de Bruns Buis Buster Choudhry Claessens Clercq, de Compaijen Conijn-Mensink Cornet Crobach Cruijsen Cuperus Dackus De Haar-Holleman Dekker Deure, van der Dijkstra Dorp, van Douma Douma Douma Driessen Drion FIRST AUTHOR ABSTRACT NR M.C. A.L.H.J. R. D.E. Y.M. F.M.F C.E. R.W. L.I. R. N.P. D.G. N.L.H. P.J.E.J. C. M. A.Y P. S.H. C.R. L.H.A. H.T. C.L. M.C. M.H. K. S. D. E.A.J.E J. A.N. M.C.G.J. I.J.A. A.H.W. M.C. E.H.C.J. Z.A. J.J.M. N.C. C.J. A.S.B. A.D. M.J.T. M.J. F.J.C. G.M.H.E. A. D. W.M. I.M. S.M. R.A. G. J.A.J. C.M.L. I. 111 203 55 141 215 73, 179 88 65 82 225, 226 186 218 251 252 43, 223 44 258 213, 214, 216 100 201 164 70 97 185 12 113 168 76 250 191 10 15 89 182 198 127 101 34 110 132 50 192 193 237 91 158 53, 117 246 60 245 136 6 115 157 105 11 Droogendijk Dutilh Eling Enschot, van Ezzahti Flameling Gastel, van Geelhoed Geerse Gerrits Goes, van der Gootjes Grasman Grijsen Groeningen, van Haalen, van Hagen, van Halteren, van Hana Hattem, van Hende, van den Hermans Hermsen Hillen Hofland Holster Hommel Hoogenberg Hovius Huijben Huijgen Huttjes Ilik Jager, de Jalving Jansen Janssen Jongsma-van Netten Jonker Joosten Josephus Jitta Kampschreur Kappen Kappers Keur Klauw, van der Klieverik Klok Klop Kok Kouwenberg Kraan, van der Kramer Kramer Krikke Krol 139 ABSTRACT NR J. J.C. Y. J.W.T. M. B. P.M. J.J.M. D.A. E.G. M.C. E.C. M.E. M.L. I.K. F.M. P.M. H.K. A. J.M. L.N. M.A.W. I.G.C. J.M. J. I.L. I. K. J.W.R. A.M.T. R. S.N. M.I R.L. M. P.M. M. H.G. J.T. J.M.H. N. L.M. J.H. M.H.W. M.B. M.M. L.M.A. F.A. B. M. I.C. J. M. A.B. M. C.G. 5 171 180 135 154, 173, 233 248 85, 219 220 206, 241 69 129 165 181 20 221 123 8 137 142 195 190 18 38 156 37 161 104 27 58, 170 3, 199 148 183 196 66 208 16, 151 23, 256 59 30 202 174 19 255 39 210 227 230 131 146, 147 64, 169 234 240 45 62 253 254 FIRST AUTHOR Laar, van Labots Lambregts Lammers Lammers Langenberg Langenberg Liesting Linde, van der Loffeld Loffeld Logtenberg Maas Maas Meerten, van Mehra Meijden, van der Mellema Mijnhout Moolenaar Mulder Mutsaers Net, van der Nguyen Niemeijer Nijland Ogilvie Oosterwerff Ootjers Peters Platvoet-Sijtsma Poel Polinder- Bos Poppel, van Post Pulles Quanjel Rab Ramakers Ramshorst, van Reijnders Repping-Wuts Robbrecht Rodenburg Rooijen, van Ruiter Sandberg Sandovici Santbergen Scholte Schouten Schreurs Schrijver Schuijt Simkens Slavenburg Sluis, van Snoeks Sprangers ABSTRACT NR J.A.M. G. M.M.C. W.J. A.J.J. M.H.G. S.M.C.H. C. N.A.J. S.M.L.A. R.J.L.F. S.J.J. M. M.L. T. N. W.A.G. J.E.M. G.S. D.L.J. D.J. P.G.N.J. J.B. T.T.H. N.D. M.L. A.C. M.M. C.S. J.L. S.M. Y.H.M. H.A. P.C.M. J.P. A.E. M.J.R. M.A.E. B.P.C. J. J.G.P. J.W.J. D.G.J. E.M. C.R. R. Y. M. B. J.B.J. M. J.W.G.M. E.J.M. T.J. L.H.J. S. G.L. L.L. J.M. FIRST AUTHOR 9 56 172 109 231 35 166 130 17 159 160 28 87 175 2 77 72 177 103, 238 217, 224 149, 155 126 178 247 118 121 143, 144 96 176 78 93 139 119 106 244 222 67 74 209 92 163 86 114 33 83 29, 107 42 99 194 232 25 167 41 24 36 188 49 242 68 Sriram Stassen Steen, van der Streukens Stuijver Tack Takkenberg Telgen Tomlow Tromp Veen, van Veer, van der Vegting Ven, van de Verbeet Vercoutere Vergeer Verheijden Versmissen Verweij Verweij Visser Vondeling Voogd Vos Vriens Vriesendorp Wagen, van der Wal-Visscher, van de Walhout Walpot Waning, van Weegh, op de Weijmans Wener Wennemers Wentholt Wester Wester Wiersinga Wijk, van Wijsman Willemsen Wind Winkel, van de Wismans Wit, de Witmer Wlazlo Woittiez Woittiez Wolzak Woudstra Wumkes Yassi Ytredal Zegers Zijlstra Zondag Zonneveld 140 ABSTRACT NR J.D. P.M. M.J.M.M. S.A.F. D.J.F G.J. R.B. M.C. B. M. M.C. M. I.L. A.C. N.L. W. M. N.A.F. J. E. K.E. H. A.M. F.J. J. I.J.H. T.M. L.E. E.R. I. J.M.J.B. V.H. M.L. M. R.R.L. A. I.M.E. R. M. W.J. J.P.H. C.A. A.E.C.A.B L.J.N. L.M.H P.J. H.M. J.L. N. K.J. L.R. H. F.H. M.L W. H. I.H.A. M. W. A.M. 75 22, 32 63 79 26 54 122 124 153 1 162 134 228, 229 81 80 239 14 112 13 120 152 133 48 189 150 71 84 90 204 249 243, 259 212 95 98 51 138 46 125 236 57 102 31 61 187, 197 47 200 94 40 4, 108, 235 205 211 145 257 116, 140 184 52 128 207 7 21
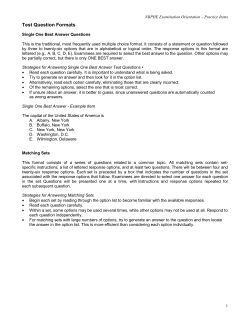








© Copyright 2025