
M c a s
M MccM Maasstteerr U Un niivveerrssiittyy D Diivviissiio on no off O Op ph htth haallm mo ollo og gyy R Reessiid deen ntt M Maan nu uaall Contents The specialty of Ophthalmology is concerned with the screening, diagnosis, prevention and management of optical, medical, and surgical disorders of the eye. Upon completion of the Ophthalmology Resident Program, a resident is expected to be a competent Ophthalmologist capable of assuming a consultant’s role in the specialty. The resident must acquire a working knowledge of the theoretical basis of the specialty, including its foundations in the basic medical sciences and research. The Ophthalmologist must possess a sound knowledge of the general principles of surgery and medicine. Ophthalmology embraces some aspects of neurology, pathology, plastic surgery, dermatology, microbiology, and other specialties, and the graduate must have knowledge in these fields as they relate to Ophthalmology. (RCPSC) This Resident manual provides a complete orientation to the Ophthalmology residency program at McMaster University. Faculty & Staff Dr. John Harvey Professor Oculoplastics Academic Division Head, Division of Ophthalmology Director of Oculoplastic, Reconstructive, Lacrimal and Orbital Service Contact Information: For inquiries please contact Joanne Verboom, Administrative Assistant Phone: 905-573-7777 x38095 Fax: 905-573-4826 Email: verboom@mcmaster.ca Dr. Nina Ahuja Associate Clinical Professor Ophthalmology Residency Program Director, Division of Ophthalmology Contact Information: Phone: 905-575-7050 Fax: 905-297-7597 Residency Program Coordinator: Julia Smerilli Email: smerilj@mcmaster.ca Phone: 905-573-7777 x38060 Dr. Keith Mann Assistant Clinical Professor Ophthalmology Optics Contact Information: Phone: 905-627-4975 Fax: 905-627-7553 Dr. Amadeo Rodriguez Assistant Professor Neuro-Ophthalmology Contact Information: For inquiries please contact Grace Palumbo, Administrative Assistant Phone: 905-573-7777 x38052 Fax: 905-573-4858 Email: gpalumbo@stjoes.ca Dr. Yasser Khan Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-456-9500 Fax: 905-456-9508 Dr. Varun Chaudhary Assistant Professor Ophthalmology and Vitreoretinal Surgery Contact Information: For all inquiries please contact Sarah Dion, Administrative Assistant Phone: 905-573-7777 x38058 Fax: 905-573-4858 Email: sdion@mcmaster.ca Research Support Staff: Michael Mak Phone: 905-573-7777 x38070 Fax: 905-573-4858 Email: surghrs@mcmaster.ca Dr. Dalia Eino Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-527-4975 Fax: 905-627-7553 Dr. Patricia Harvey Assistant Professor Retina Contact Information: For inquiries please contact Joanne Verboom, Administrative Assistant Phone: 905-573-7777 x38095 Fax: 905-573-4826 Email: verboom@mcmaster.ca Dr. Enitan Sogbesan Assistant Professor Ophthalmology- Glaucoma Contact Information: For inquiries please contact Sarah Boers, Administrative Assistant Phone: 905-573-7777 x38311 Fax: 905-573-4858 Email: boerss@mcmaster.ca Dr. Gloria Isaza Associate Clinical Professor Pediatric Ophthalmology Contact Information: For all inquiries please contact Chara Adema, Administrative Assistant Phone: 905-521-2100 x76662 Clinic: 905-521-2100 x72400 Fax: 905-521-2332 Email: cadema@mcmaster.ca Dr. Kourosh Sabri Assistant Professor Pediatric Ophthalmology Contact Information: For all inquiries please contact Ashley Warwick, Administrative Assistant Phone: 905-521-2100 x73509 Fax: 905-570-8968 Email: warwick@mcmaster.ca Dr. Anne Beattie Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-525-7907 Fax: 905-525-9186 Dr. James Csordas Assistant Clinical Professor Contact Information: Phone: 905-525-7907 Fax: 905-525-9186 Dr. Frederick Inch Associate Professor Dr. Lawrence Kobetz Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905- 574-4666 Dr. Jeffrey Sher Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-318-5338 Fax: 905-318-5313 Dr. Robert Adam Assistant Clinical Professor (Adjunct) Ophthalmology Dr. Narendra Armogan Assistant Clinical Professor (Adjunct) Ophthalmology Contact Information: For all inquiries please contact Allison Majeed, Administrative Assistant Phone: 905-212-9482 x311 Dr. Steve Arshinoff Assistant Clinical Professor (Adjunct) Ophthalmology Dr. George Beiko Assistant Clinical Professor (Adjunct) Ophthalmology Dr. Rajiv Bindlish Assistant Clinical Professor (Adjunct) Ophthalmology Dr. James Martin Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-522-3563 Dr. Khalid Hasanee Assistant Clinical Professor (Adjunct) Ophthalmology Contact Information: Phone: 905-469-6666 Fax: 905-469-3171 Dr. Wesley Nash Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-527-5559 Fax: 905-527-3883 Dr. Yasser Khan Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-456-9500 Fax: 905-456-9508 Dr. Aaron Rifkind Assistant Clinical Professor Ophthalmology Contact Information: Phone: 905-549-6123 Fax: 905-548-0770 Dr. Navdeep Nijhawan Assistant Clinical Professor (Adjunct), Section Heads by Subspecialty Dr. Dr. Dr. Dr. Dr. Dr. Dr. Dr. Dr. Dr. John Harvey Varun Chaudhary Dalia Eino Pat Harvey Khalid Hasanee Gloria Isaza Yasser Khan Keith Mann Amadeo Rodriquez Jeffrey Sher Division head, Department Chief Retina Comprehensive, Cataract/IOL theory Resident Research Glaucoma Pediatrc Ophthalmology Oculoplastics Optics Neuro-Ophthalmology Cornea and External Disease Residents Dr. Joshua Teichman PGY5 Email: josh.teichman@utoronto.ca Dr. Gamal Seif PGY4 Email: gamal.seif@medportal.ca Dr. Vasudha Gupta PGY3 Email: vasudha.gupta@medportal.ca Dr. Manreet Alangh PGY2 Email: manreet.alangh@medportal.ca Dr. Brian Chan PGY1 Email: brian.chan@medportal.ca Dr. Christopher McLaughlin PGY1 Email: christopher.mclaughlin@medportal.ca Program Overview The PGY1 year offers a broad range of clinical experiences prior to beginning core training in ophthalmology in PGY2. Specific attention is given to those areas of medicine and surgery that relate most to ophthalmology, including endocrinology, neurology, neuroradiology, dermatology, rheumatology, and plastic surgery. The PGY2 thru PGY5 years constitute the four core years of ophthalmology training. The fortyeight months are divided into three sixteen-month cycles, each cycle consisting of eight twomonths rotations. Each two-month rotation is subspecialty service based, with learning sites ranging from private offices, hospital clinics and ORs. Residents are exposed to each subspecialty in each of the three cycles, thereby allowing graduated learning and acquisition of skills appropriate for resident level of training. Objectives of Training in Ophthalmology The four core years of training in ophthalmology are designed to meet the objectives and specific requirements of training established by the Royal College, in CanMEDS format: The role of "Medical Expert" is imparted through clinical, didactic, and self-study programs that include periodic review and evaluation by faculty. During the PGY2 & 3 years, each resident independently studies the thirteen sections of the Basic & Clinical Science Course given by the American Academy of Ophthalmology. At the end of the PGY2 year towards the beginning of PGY3, each resident attends a formalized Basic and Clinical Science Course in ophthalmology, taught by leading experts at either Lancaster or Stanford University, USA. During the PGY4 year, each resident attends an Ophthalmology Board Exam review course at a leading academic center for ophthalmic training and research. In the PGY5 year, each resident attends the Annual Meeting of the American Academy of Ophthalmology. There are several hundreds of courses are offered at this meeting, allowing ample opportunity to pursue specific interests and to enhance special skills. In addition to the various courses listed above, our on-site academic program consists of weekly grand rounds alternating with clinical rounds (September to June) to discuss interesting cases, ethical issues, and research presentations; a visiting professor program with presentation to the department, followed by an academic half-day session with the residents; bimonthly journal clubs (September to June) to develop critical thinking skills and establish evidence-based practice patterns; and an academic half-day series of lectures given on a two-year cycle, to ensure up-todate and comprehensive acquisition of knowledge in each subspeciality. Attendance at local and surrounding area academic events are also encouraged, including Stringer Day (Hamilton), Sally Letson (Ottawa), Walter Wright (Toronto), and Jack Crawford Day (Toronto). Competency in the use and interpretation of various diagnostic modalities is attained during clinical rotations throughout residency training in a progressive manner. Laser and other surgical skills are acquired using a planned and graduated approach, with progressive involvement and increasing responsibility beginning early in the core years of the program. Skills in acute care and trauma are acquired through emergency call, and clinics in the various rotations. Skills in longterm care of patients are also acquired and developed through clinics in the various rotations. In- patient consultation for patients on other medical and surgical services are provided by residents, commencing in their PGY2 year. Formal evaluation of knowledge is carried out internally with faculty involvement by mock written examination administered each winter, mock oral examination administered each spring, and evaluation following each of the two-monthly rotations based on rotation-specific goals and objectives in CanMEDS format. Formal evaluation is also carried out externally by the standardized multiple-choice examination administered annually to all residents in Ophthalmology in the United States and Canada (Ophthalmic Knowledge Assessment Program (OKAP)), serving to rank resident knowledge across several domains relative to fellow residents in the same level of training. The Program Director meets with residents every six months to review and discuss the sum of evaluations. "Communication" and "Collaboration" skills are nurtured and evaluated during clinical and surgical rotations to ensure that each resident is able to communicate and appropriately collaborate with patients, patients’ families, fellow students and colleagues (including medical students, residents, clinical fellows, referring and consultant physicians), and other members of the health care team (including nurses, social workers, orthoptists, ophthalmic technicians, Eye Bank personnel, and workers from the Canadian National Institute for the Blind). "Management" skills are taught during clinical and surgical rotations, with our program having the added benefit of exposure to various practice patterns and management styles as residents learn at various teaching sites, each with its own unique structure. Participation in external courses such as "Future Focus" offered by the Canadian Ophthalmologic Society are also encouraged, to provide further insight into patient and practice management issues. Dedicated computer resources for residents are also available, to allow easy access to electronic information technology. "Health Advocate" skills are acquired through caring for individual patients while identifying and actively addressing needs unique to each patient. Modeling by faculty, case discussions at rounds and journal clubs, and participation in interest groups further encourage understanding of the physician’s role as one who provides excellent medical and surgical care of disease, while treating the person by identifying and offering appropriate resources as required, eg access to low vision services. In addition to the various elements of our academic program, "Scholarship" is fostered through resident attendance and participation at meetings and conferences held by our national and international specialty societies. Each resident is also required conduct original research leading to presentation and publication. "Professionalism" is developed through modeling by faculty, and by discussion of various elements of behavior with residents as examples arise in aspects of patient care, interactions with colleagues, practice management, and professional development. Self-assessment and the ability to recognize and acknowledge one’s limitations are emphasized. Residents are observed in daily interactions to ensure behaviors are in keeping with the ethical standards and responsibilities of a professional physician. Research During the course of residency training, residents are required to conduct at least one original randomized controlled trial for presentation at local, national, or international meetings, with subsequent publication in the literature. PGY1 – General Goals & Objectives Learning Objectives for PGY-1 Ophthalmology Residents – BCT Year Rotations Learning objectives in general are those of each individual service/clinic that you attend, but overall learning objectives may be stated as follows. Medical expert 1. Residents will see patients in various settings and learn to conduct a relevant and concise history and physical examination, develop a management plan appropriate to the service/clinical setting a. Residents will function at a level of independence appropriate to PGY-1 b. Managing multiple patient issues/complaints within a clinic environment where time is limited c. All patients seen will be reviewed by the attending physician 2. Longitudinal care should be emphasized – where possible residents should have the opportunity to see patients more the once to see the results of their management plan 3. Residents will learn to access and apply relevant medical information in a timely manner within the constraints of the practice a. This includes the ability to pose an appropriate patient-related question, execute a systematic search for evidence, and critically evaluate medical literature and other evidence all within the time and resource constraints of the practice b. Residents will be taught how evidence based medicine principles can be applied in a service/clinical setting Communicator 1. Residents will learn to communicate diagnoses and management plans with patients in a service/clinical setting a. This includes “giving bad news” and prompting end of life discussions where appropriate in a service/clinical setting b. This includes the ability to counsel patients in regards to his/her own illness(es), especially in complex medical issues, health promotion and advocacy (eg. smoking cessation) 2. Residents will learn how to establish a therapeutic relationship with patients within a situation where “face time” is episodic and short, but recurring a. This includes the ability to establish and maintain rapport and fostering an environment characterized by understanding, trust, empathy and confidentiality. b. Managing patients with multiple issues/complaints 3. Elicit and synthesize relevant information from families, and/or community. This implies the ability to explore patient’s beliefs, concerns, and expectations about the origin, nature, and management his/her illness. Specialists need to be able to assess the impact of such factors as age, gender, ethno cultural background, social support, and emotional influences on a patient’s illness. Collaborator 1. Residents will learn to dictate letters to consulting physicians and other health care providers as part of the clinic management process a. Residents will learn to dictate succinctly and clearly, emphasizing their professional opinions and conclusions b. Residents will state clearly what the management plans are, and to communicate who is responsible for executing that plan c. Residents will learn to use the consultation letter as a education tool for referring doctors in professional and collegial way, where appropriate 2. Effectively consult with other physicians a. Residents will learn how to develop investigations, treatment and continuing care plans in partnership with the patient and other care providers b. Learn to recognize of personal expertise, understand the roles and expertise of the other individuals involved 3. Learn the role of the multidisciplinary team within the service/clinical setting a. learn the roles and skills of service/clinic nurses in the service/clinic and how to work effectively with the nursing team to benefit patient care b. learn the role of dieticians, physiotherapists, chiropdists, etc. in the community who can help manage physicians to patients c. Learn the role to inform and involve the patient and his/her family in decision-making, and explicitly integrate the opinions of the patient and caregivers into management plans. Manager 1. Utilize time and resources effectively in order to balance patient care, earning needs, outside activities, and personal life. This implies the ability to employ effective time management and self-assessment skills to formulate realistic expectations and a balanced lifestyle. 2. Needs to include fundamental knowledge of the financing of the Ontario/Canadian health care system. 3. Effectively utilize information technology to optimize patient care, continued self-learning and other activities. This implies the ability to: use patient related databases, access computerbased information, and understand the fundamental of medical informatics. Scholar 1. Residents will familiarize themselves with continuing professional development as per the Maintenance of Certification Program from the Royal College of Physicians and Surgeons of Canada a. Residents will learn how to develop and complete a Structured Learning Project (or Personal Learning Project) as per Section 4 of the Maintenance of Certification program from the Royal College of Physicians and Surgeons of Canada. b. The question generated will be based on at least one clinical encounter during the service block c. Residents may elect to register as a resident under the program Professionalism 1. Staff physicians will model the highest quality of care, and conduct themselves with integrity, honesty and compassion. a. Residents will learn professionalism through an apprenticeship model b. Staff will discuss how to incorporate ethic, gender, cultural and societal issues into practice c. Staff will ensure there is proper supervision and adequate teaching during the service/clinic experience 2. Residents will attend each scheduled clinic on time, and inform staff ahead of time when he/she is not able to attend a clinic Health Advocate 1. Appreciate patient autonomy and the religious, ethnic, and psychosocial factors which influence the physician/patient relationship and to take these factors into account when pursing problems and understanding patient decisions. Identify and utilize appropriate interventions to treat the patient Goals & Objectives by Sub-specialty Cornea/External Disease and Uveitis Medical Expert: An ophthalmologist’s training must include an excellent foundation in the diagnosis, investigation and treatment of corneal and external diseases of the eye. This area includes common problems areas encountered in general ophthalmologic practice such as ocular surface infections as well as rarely encountered inherited and acquired corneal disorders. The ophthalmologist in training should acquire the skills of diagnosis, pathogenesis and treatment of corneal and external diseases, but also the skill of a critical and inquiring approach to diseases of the eye that will serve the trainee throughout their future career in ophthalmology. The diagnosis of external disease problems of the eye frequently requires a team approach, with the ophthalmologist working closely with the clinical microbiology lab technician, other specialists in infectious diseases, and specialists in internal medicine, particularly in the field of rheumatology. The primary objective for the cornea and external disease rotation is to allow the resident to diagnose, understand and manage common diseases of the cornea and the ocular surface. It is expected that much exposure of the resident with be during general out-patient clinics where most of these patients are seen, but that also there will be regular and punctual attendance at cornea and external disease clinics, both in the hospital out-patient clinics and in the attending physician’s private offices, where appropriate. In addition, attendance at Journal Clubs, special lectures, cornea and external disease teaching sessions is expected. The residents are advised to read, understand and use the knowledge in the American Academy of Ophthalmology Basic Clinical Science Course, Section 7. Residents are also expected to review the current ophthalmic literature and other informational resources. Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with 1. Patient’s and Their Families a. Explain general surgical disease processes b. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians a. Family physician b. Clinical microbiologist c. Lab technicians d. Internal Medicine Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • • • • • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for Cornea/External Disease and Uveitis, and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) F.1 Clinical (i) generate a clinical question (ii) identify his/her own knowledge and recognize deficits in knowledge about the question (iii) develop a plan to remedy the deficit by a) conducting an appropriate literature search (iv) (v) (vi) (vii) F.2 F.3 b) assimilating and critically evaluating the literature c) consulting other physicians and health care professionals propose a solution to the clinical question implement this solution in her/his practice evaluate the outcome of this solution generate new clinical questions... Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) develop a proposal to answer the research question by a) conducting an appropriate literature search b) assimilating and critically evaluate the literature c) identify, consult and collaborate with appropriate experts to undertake the research proposal (iii) propose appropriate methods for conducting the research (iv) undertake the proposed research (v) propose a solution to the clinical question (vi) disseminate and defend the results of the research (vii) identify future research opportunities and questions that arise from the results Education (i) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others (ii) demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. McMaster SPECIFIC EDUCATIONAL OBJECTIVES Retina Retina Medical Expert: Become proficient with appropriate examination techniques, including - slit lamp biomicroscopy with 78 and 90 D lenses and contact lenses - indirect ophthalmoscopy - direct ophthalmoscopy - scleral depression - retinal drawing - A and B scan ultrasonography Assist in Vitreoretinal surgery Knowledge of normal retinal anatomy and histology, and variations of fundus appearance related to race and age. Knowledge of pathophysiology, diagnosis and management of: - diabetic retinopathy - arteriosclerosis and hypertension retinopathy - macroaneurism - BRVO,CRVO, BRAO, CRAO - Maculopathies including ARMD,CSR, OHS, pathologic myopia, angioid streaks - Peripheral retinal degenerations - Retinal detachment Ability - to perform retinal photocoagulation therapy (PRP and treatment of retinal tears) periocular injections AC paracentesis Understands indications and techniques of: - pneumatic retinopexy - scleral buckling - vitrectomy Understands approach to postoperative endophthalmitis and can perform appropriate AC and vitreous taps and injection of intravitreal antibiotics Knowledge of Pathophysiology, diagnosis and management of: - retinopathy of prematurity - inflammatory/infectious conditions including sarcoidosis, toxoplasmosis, syphilis, TB, endogenous endophthalmitis, AIDS retinopathy, CMV retinitis, and other HIV related conditions, serpigenous choroiditis, white dot syndromes - traumatic retinal conditions (commotio retinae, Purtscher’s retinopathy, valsalva retinopathy, choroidal rupture. McMaster SPECIFIC EDUCATIONAL OBJECTIVES Retina Able to independently manage post operative vitreoretinal patients including knowledge of potential side effects and complication of intraocular gas tamponade and silicone oil Knowledge of pathophysiology, diagnosis and management of - hereditary and degenerative retinal conditions (retinoschisis, retinitis, pigmentosa, choroideremia, gyrate atrophy, etc) - neoplastic diseases – choroidal melanoma, choroidal metastases, hamartomas, retinoblastoma Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with 1. Patient’s and Their Families c. Explain general surgical disease processes d. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians e. Family physician f. Clinical microbiologist g. Lab technicians h. Internal Medicine Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. McMaster SPECIFIC EDUCATIONAL OBJECTIVES Retina • • • Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for Retina, and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) F.1 Clinical (i) generate a clinical question (ii) identify her/his own knowledge and recognize deficits in knowledge about the question (iii) (iv) (v) (vi) (vii) F.2 develop a plan to remedy the deficit by a) conducting an appropriate literature search b) assimilating and critically evaluating the literature c) consulting other physicians and health care professionals propose a solution to the clinical question implement this solution in her/his practice evaluate the outcome of this solution generate new clinical questions... Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) develop a proposal to answer the research question by a) conducting an appropriate literature search b) assimilating and critically evaluate the literature c) identify, consult and collaborate with appropriate experts to undertake the research proposal (iii) propose appropriate methods for conducting the research (iv) undertake the proposed research (v) propose a solution to the clinical question (vi) disseminate and defend the results of the research (vii) identify future research opportunities and questions that arise from the results McMaster SPECIFIC EDUCATIONAL OBJECTIVES Retina F.3 Education (i) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others (ii) demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma Glaucoma Medical Expert: In general, our goal in training ophthalmologists is: 1. to provide excellent teaching of ophthalmology. 2. to provide skillful care to patients with ophthalmic disorders. 3. to nurture a critical and inquiring approach to investigating the unsolved problems of eye diseases. It is critical to understand the chronic slow progression of glaucoma and differentiate it from other eye disorders. A good understanding of the definition of glaucoma in particular intraocular pressure being a risk factor is very important. Detailed history and examination key in differentiating primary open angle glaucoma (POAG) from low tension glaucoma (LTG), secondary open angle glaucoma (2◦ OAG), and traumatic inflammatory or other type of glaucoma. The primary objective for the glaucoma rotation is to be familiar with diagnosing and managing common glaucoma disorders. It is expected that there will be regular and punctual attendance at glaucoma clinics and rounds. In addition, attendance at Journal Clubs and special lectures is strongly encouraged. Each resident is also encouraged to initiate a research project that can be presented at a scientific meeting. The residents are advised to read the American Academy of Ophthalmology Basic and Clinical Science Course (BCSC), Section 10: Glaucoma. Other relevant BCSC Sections should also be reviewed. Review of the current medical literature (through information technology, literature searches, etc.) is also important. Stratified Objectives for Post-Graduate Year 1) to demonstrate knowledge of the pathogenesis of the primary and secondary glaucomas (open and closed angle) and the natural history of each including low tension glaucoma and ocular hypertension; 2) to demonstrate knowledge of primary and secondary glaucomas in the newborn and in children; 3) to identify the pediatric glaucoma patient; 4) to describe the effects of raised intraocular pressure on the optic nerve head and discuss theories of mechanism of damage in glaucoma; 5) to demonstrate an understanding of the significance of the term “glaucoma suspect”; 6) to take a history appropriate to the glaucoma patient with special reference to risk factors; Page 19 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma 7) to begin to correctly interpret features of the anterior segment in the glaucoma patient including chamber depth, gonioscopy and any indicators of secondary glaucoma; 8) to begin to describe and to differentiate the optic nerve head in normal and in glaucoma patients; 9) to begin to understand the operating principles of visual fields machines; 10) To describe the appearance and evolution of visual field defects in glaucoma; 11) To identify and interpret visual fields defects in glaucoma patients and to differentiate them from defects due to other causes; 12) To demonstrate understanding of intraocular pressure – its control, its measurement and its variability; 13) To assess and to interpret intraocular pressure data and the effects of therapy; 14) To identify and interpret any co-morbidity in the eyes of glaucoma patients; 15) To demonstrate an understanding of pharmacology of systemic and topical antiglaucoma medications; 16) To apply that knowledge in any management of glaucoma patients; 17) Establish trusting relationship with patients and their families; 18) Discuss appropriate information with patients and their families; 19) Consult effectively with other physicians and health care professionals; 20) Contribute to Grand Rounds, Journal Clubs, etc. 21) Begin to utilize resources effectively to balance patient care, learning needs, and outside activities; 22) Utilize information technology to optimize patient care and life-long learning; 23) Identify important determinants of health affecting patients (i.e., age, sex, lifestyle, poverty, culture, ethnicity, religion, etc.); 24) Recognize the need for appropriate support and referral (i.e., low vision clinic, CNIB, other community-based resources/agencies, opticians, and optometrists); 25) Develop a personal education strategy; 26) Be punctual and responsible; 27) Be organized, tidy, and well dressed; 28) Keep accurate records; 29) Recognize one’s own limitations; Page 20 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma 30) Seek appropriate assistance when necessary; 31) Exhibit appropriate behavior and attitude. 32) be proficient in slit lamp biomicroscopy with 78D and 90D lenses, gonioscopy, indirect and direct ophthalmoscopy; 33) To refract and to measure visual acuity taking into account pupil size; 34) To demonstrate an understanding of the principles of ophthalmic lasers and their application in the treatment of glaucomas; 35) To begin to perform argon laser trabeculoplasty, iridoplasty, iridotomy and transcleral cycloablation using ophthalmic lasers; 36) In the care of surgical patients: a) to demonstrate an understanding of the levels of disability induced by glaucoma before operative interference is deemed advisable; b) to perform regional and periocular retrobulbar injection techniques; c) to be introduced to intraocular surgery with the beginning hands on experience; d) to be proficient in the handling of surgical ocular instruments in the laboratory; e) to demonstrate suture placement and knot tying in the laboratory; 37) Surgery: a) to demonstrate an understanding of the mechanism and application of operating room instruments and machines, including the operating microscope, lens fragmentation and aspiration instruments and vitreous suction cutters; b) to take measurements and assess the findings and to calculate lens power in patients needing intraocular lenses including axial length determination, keratometry, lens power calculation and endothelial cell appearance; c) to perform to the satisfaction of the surgical tutors the following glaucoma procedures including the management of intraoperative and postoperative complications. These procedures include: -trabeculectomy; -trabeculectomy combined with cataract removal; -iridectomy; -revision of drainage blebs; and -the use of wound modulating drugs. d) to perform to the satisfaction of the surgical tutors and following additional procedures: diagnostic and therapeutic paracentesis of the anterior and posterior segments. e) to perform retrobulbar and regional anesthesia. The student will be evaluated by an on-going process and deficiencies will be brought to their attention as soon as one is recognized. Unsatisfactory evaluations will be addressed on an individual basis. It is expected that the student will also critically evaluate the preceptor so as to help he/she improve their ability to teach more effectively. The resident’s evaluation of the instructor will in no way affect the final evaluation they are to receive. Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with Page 21 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma 1. Patient’s and Their Families e. Explain general surgical disease processes f. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians i. Family physician j. Clinical microbiologist k. Lab technicians l. Internal Medicine Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • • • • • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for Glaucoma and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Page 22 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) F.1 Clinical (i) Generate a clinical question (ii) Identify her/his own knowledge and recognize deficits in knowledge about the question (iii) (iv) (v) (vi) (vii) F.2 F.3 Develop a plan to remedy the deficit by a) Conducting an appropriate literature search b) Assimilating and critically evaluating the literature c) Consulting other physicians and health care professionals Propose a solution to the clinical question Implement this solution in her/his practice Evaluate the outcome of this solution Generate new clinical questions... Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) Develop a proposal to answer the research question by a) Conducting an appropriate literature search b) Assimilating and critically evaluate the literature c) Identify, consult and collaborate with appropriate experts to Undertake the research proposal (iii) Propose appropriate methods for conducting the research (iv) Undertake the proposed research (v) Propose a solution to the clinical question (vi) Disseminate and defend the results of the research (vii) Identify future research opportunities and questions that arise from the results Education (i) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others (ii) Demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Page 23 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Glaucoma Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. Page 24 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Pediatric Ophthalmology & Adult Strabismus Pediatric Ophthalmology & Adult Strabismus Medical Expert: Obtain & synthesize relevant general & ophthalmic history from patients/families/others Obtain appropriate visual assessment, including: fixation preference recognition visual acuity understand forced preferential looking Recognize the causes of amblyopia, and understand its treatment including occlusion, pharmacological agents and optical methods Start refraction of children, including performing cycloplegic retinoscopy Measure motor eye alignment with such tests as cover, cover-uncover, alternate cover-uncover, simultaneous prism & cover, ocular versions and ocular ductions Understand, test and accurately assess sensory status with such tests as stereoacuity, Worth 4dot, Maddox rod & double rod, synoptophore and Bagnolini lenses Perform & properly interpret other components (i.e. non-motility) of pediatric eye exam Start to understand the diagnosis of strabismus, including classification & syndromes Start to understand other (i.e. non-strabismus) diseases & syndromes involving the pediatric eye e.g. nasolacrimal obstruction, dacryocystitis, amniotocele, congenital & infantile cataracts, ptosis Establish therapeutic relationship with patients/families Discuss appropriate information with patients/families/health care team Consult effectively with other physicians & health care professionals, including orthoptists and ophthalmic assistants Contribute to grand rounds, journal clubs, etc. Start to utilize resources effectively to balance patient care, learning needs and outside activities Utilize information technology to optimize patient care and life-long learning Identify important determinants of health affecting patients Appropriate support & referral to low vision clinics, the CNIB, other community agencies, opticians and optometrists Develop a personal education strategy Be punctual & responsible Accurate record keeping Recognize one’s own limitations Seek appropriate assistance when necessary Exhibit appropriate behavior/attitudes Perform strabismus surgery including postoperative adjustment if adjustable sutures used Perform nasolacrimal duct probing Be able to initiate & follow anti-amblyopia therapy, recognizing the limitations of each method, endpoints and failure Understand the treatment of amblyopia in complicated situations such as glaucoma, cataract and trauma Perform accurate refraction of children, including accurate cycloplegic retinoscopy Accurately measure motor eye alignment Understand the mechanisms involved in sensory responses such as diplopia, visual confusion, suppression, and abnormal retinal correspondence Synthesize the history & physical findings into a differential diagnosis, formulate and carry out a treatment plan, with appropriate follow up Understand the diagnosis & classification of strabismus, such as the various esodeviations, esodeviations, vertical deviations, and A & V patterns, as well as syndromes such as Duane’s, Browns, Moebius, double elevator palsy, and conditions such as myasthenia, Page 25 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Pediatric Ophthalmology & Adult Strabismus dysthyroid, post-traumatic including blowout fractures, cranial nerve palsies and ocular & non-ocular causes of abnormal head posturing Understand the medical pediatric diseases with ocular manifestations, such as juvenile rheumatoid arthritis, ophthalmia neonatorum, Downs, fetal alcohol syndrome & shaken baby syndrome Be able to perform an adequate examination for retinopathy of prematurity, properly assessing its status & necessity for treatment Understand the indications for the various pediatric eye surgeries such as strabismus, nasolacrimal obstruction including silicone intubation of the nasolacrimal system, ptosis & congenital cataract, and be able to obtain informed consent Understand the various forms & causes of nystagmus Understand pediatric neurophysiology, including cortical visual inattention/blindness, and the role of electrophysiological testing (e.g. ERG, VEP, EOG) Continue a personal education strategy Be able to diagnose and treat the more complicated medical & surgical pediatric eye diseases including anterior segment dysgenesis, ectopia lentis, optic nerve and retinal disorders, visual system disorders causing visual impairment as well as adult strabismus Be able to establish a strong therapeutic relationship with patients and families, utilizing consultations and other health care professionals in an appropriate manner Contribute effectively to grand rounds, journal clubs, and teaching to other health care professionals Have an effective personal education strategy Be inquisitive Be an appropriate and effective patient advocate Deliver quality care with integrity, honesty & compassion Practice medicine ethically consistent with the obligations of a physician METHODS: Regular & punctual attendance at clinics Regular & punctual attendance at surgery Completion of relevant sections of the AAO BCSC Relevant sections of the Lancaster Basic Science Course in Ophthalmology Attendance in Orthoptics Cadaveric orbital dissection Lectures Journal Clubs Journals, books Scientific meetings, courses (as possible) Communicator The resident will demonstrate the ability to establish an appropriate rapport with the patient and family. This includes the ability to adjust tasks to patient’s level of ability/development as well as able to counsel patients and family members. Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Page 26 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Pediatric Ophthalmology & Adult Strabismus Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager The resident should be able to apply knowledge of the clinical and basic sciences to clinical practice: Gather appropriate clinical information to perform a strabismus consultation and follow-up assessment. Recognize the pertinent features of a strabismus case study. Formulate a reasonable plan of investigation. Interpret the investigations in the patient’s context. Formulate an appropriate treatment approach. Understand the goals of treatment and likely outcomes. Manage amblyopia, diplopia and vergence weakness within professional guidelines Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for Pediatric Ophthalmology & Adult Strabismus and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar The resident accepts and acts on constructive feedback. Takes initiative to research and review patient cases and takes an evidence-based approach to management problems. It should be noted that not all objectives will be met on each 1-month rotation, but will be accumulated over several rotations in the orthoptic clinic. Further learning takes place during related rotations, supervised clinic time, seminars and independent study. Professional The resident will practice orthoptics ethically: with integrity, honesty and compassion, always demonstrating respect for others. Maintains composure when interacting with patients, colleagues and supervisors. Is punctual. Appropriate attire and grooming in the work situation. Page 27 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Neuro-Ophthalmology Neuro-Ophthalmology Medical Expert: In general, our goal in training ophthalmologists is: 1. to provide excellent teaching of ophthalmology. 2. to provide skillful care to patients with ophthalmic disorders. 3. to nurture a critical and inquiring approach to investigating the unsolved problems of eye diseases. The evaluation of patients with neuro-ophthalmic disorders is often a time-consuming task. It is important to understand that all neuro-ophthalmic disorders require a detailed history and chronology of events. Often, this may require the resident to contact other physicians or optometrists for old records or visual fields. In addition, since we are often dealing with a patient who have disorders of the visual pathways, neuro-imaging is an important step in the evaluation process. It is mandatory to personally review all previous imaging studies. This is how one becomes comfortable in viewing CTs and MRIs with confidence. In addition to a detailed history and examination, the resident should familiarize themselves with ‘typical’ case presentations in neuro-ophthalmic conditions. This aids the physician in the management of the patient’s complaints. Of course, some patients may be ‘atypical’ in the presentation of disease, but this will only serve to have the resident review the current literature for similar case reports. The primary objective for the neuro-ophthalmology rotation is to be familiar with diagnosing and managing common neuro-ophthalmic disorders. It is expected that there will be regular and punctual attendance at neuro-ophthalmology clinics and rounds. In addition, attendance at Orthoptics Clinic, Journal Clubs, special lectures, neuroscience rounds, and neuroradiology rounds is strongly encouraged. Each resident is also encouraged to initiate a research project that can be presented at a scientific meeting. The residents are advised to read the American Academy of Ophthalmology Basic and Clinical Science Course (BCSC), Section 5: Neuro-Ophthalmology. Other relevant BCSC Sections should also be reviewed. Review of the current medical literature (through information technology, literature searches, etc.) is also important. Stratified Objectives Cycle 1 - - obtain and synthesize relevant and general and ophthalmic history from patients obtain appropriate visual assessment, including - critical analysis of sensory afferent visual function - critical analysis of sensory and motor efferent visual function - gathering ‘additional’ information (old charts, collateral history, old photographs, previous visual acuities and visual fields, previous neuro-imaging, etc.) recognize causes of unexplained loss of vision recognize causes of diplopia recognize causes of papillary inequality recognize causes of visual disturbances recognize causes of visual field defects Page 28 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Neuro-Ophthalmology - - recognize causes of headaches and eye pain recognize neuro-ophthalmic manifestations of systemic (and neurologic) disease begin to understand the natural history of common neuro-ophthalmic problems begin to understand the various tests of sensory afferent and efferent visual function begin to understand the various types and interpretation of visual field tests (perimetry) begin to understand the indications for and interpretation of neuro-imaging begin to understand neuroanatomy as it relates to neuro-ophthalmology begin to understand the need for diagnostic procedures such as tangent screen evaluation, forced duction testing, temporal artery biopsy, conjunctival biopsies, Tensilon/Prostigmine testing, cerebrospinal fluid analysis begin to perform tangent screen evaluation, forced duction testing, temporal artery biopsy, conjunctival biopsies, Tensilon/Prostigmine testing establish trusting relationship with patients and their families discuss appropriate information with patients and their families consult effectively with other physicians and health care professionals contribute to Grand Rounds, Journal Clubs, etc. begin to utilize resources effectively to balance patient care, learning needs, and outside activities utilize information technology to optimize patient care and life-long learning identify important determinants of health affecting patients (i.e., age, sex, lifestyle, poverty, culture, ethnicity, religion, etc.) recognize the need for appropriate support and referral (i.e., low vision clinic, CNIB, other community-based resources/agencies, opticians, and optometrists) develop a personal education strategy be punctual and responsible be organized, tidy, and well dressed keep accurate records recognize one’s own limitations seek appropriate assistance when necessary Cycle 2 - - - - all of the above apply plus: be able to critically analyze the various components of sensory afferent and efferent visual function be able to thoroughly analyze and interpret various causes of unexplained loss of vision, diplopia, pupillary inequality, visual disturbances, visual field defects, and headaches and eye pain be able to discuss the neuro-ophthalmic manifestations of systemic (neurologic) diseases be able to thoroughly analyze and interpret various types of visual field tests be able to thoroughly analyze and interpret neuroimaging studies be able to thoroughly understand the natural history of common neuro-ophthalmic problems be able to thoroughly understand neuroanatomy as it relates to neuro-ophthalmology be able to thoroughly understand the need for diagnostic procedures such as tangent screen evaluation, forced duction testing, temporal artery biopsy, conjunctival biopsies, Tensilon/Prostigmine testing, cerebrospinal fluid analysis to be able to competently perform tangent screen evaluation, forced duction testing, temporal artery biopsy, conjunctival biopsies, Tensilon/Prostigmine testing to understand the indications for and interpretation of ancillary tests such as orbital echography, electrophysiologic tests (VEP, ERG, EOG, etc.), fluorescein angiography, color vision tests, and diagnostic pupillary drop testing continue a personal education strategy Page 29 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Neuro-Ophthalmology Cycle 3 - all of the above apply plus: be able to diagnose and manage complex neuro-ophthalmic conditions be able to establish a strong diagnostic and therapeutic relationship with patients, utilizing consultations and other health care professionals in an appropriate manner contribute effectively to Grand Rounds, Journal Clubs, and teaching to other health care professionals have an effective personal education strategy be inquisitive be an appropriate and effective patient advocate delivery quality care with integrity, honesty, and compassion practice medicine ethically consistent with the obligations of a physician The student will be evaluated by an on-going process and deficiencies will be brought to their attention as soon as one is recognized. Unsatisfactory evaluations will be addressed on an individual basis. It is expected that the student will also critically evaluate the preceptor so as to help he/she improve their ability to teach more effectively. The resident’s evaluation of the instructor will in no way affect the final evaluation they are to receive. Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with 1. Patient’s and Their Families a. Explain general surgical disease processes b. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians a. Family physician b. Clinical microbiologist c. Lab technicians d. Internal Medicine Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Page 30 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Neuro-Ophthalmology Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • • • • • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for Neuro-Ophthalmology, and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) F.1 Clinical (i) generate a clinical question (ii) identify her/his own knowledge and recognize deficits in knowledge about the question (iii) (iv) (v) (vi) (vii) F.2 develop a plan to remedy the deficit by a) conducting an appropriate literature search b) assimilating and critically evaluating the literature c) consulting other physicians and health care professionals propose a solution to the clinical question implement this solution in her/his practice evaluate the outcome of this solution generate new clinical questions... Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) develop a proposal to answer the research question by a) conducting an appropriate literature search b) assimilating and critically evaluate the literature c) identify, consult and collaborate with appropriate experts to Page 31 of 47 McMaster SPECIFIC EDUCATIONAL OBJECTIVES Neuro-Ophthalmology (iii) (iv) (v) (vi) (vii) F.3 undertake the research proposal propose appropriate methods for conducting the research undertake the proposed research propose a solution to the clinical question disseminate and defend the results of the research identify future research opportunities and questions that arise from the results Education (i) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others (ii) demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. Page 32 of 47 General Ophthalmology and Cataract Medical Expert: Obtain & synthesize relevant ophthalmic & general history from patients/families/others Perform appropriate visual assessment, including visual acuity, visual fields, external examination, slit lamp examination & tonometry, and ophthalmoscopy, understanding proper use & care of instruments Start performing refractions Comes to a reasonable differential diagnosis for level, and starts formulation of an appropriate treatment plan Establish therapeutic relationship with patients/families Discuss appropriate information with patients/families/health care team Consult effectively with other physicians & health care professionals, including orthoptists and ophthalmic assistants Contribute to grand rounds, journal clubs, etc. Start to utilize resources effectively to balance patient care, learning needs and outside activities Utilize information technology to optimize patient care and life-long learning Identify important determinants of health affecting patients Appropriate support & referral to low vision clinics, the CNIB, other community agencies, opticians and optometrists Develop a personal education strategy Be punctual & responsible Accurate record keeping Recognize one’s own limitations Seek appropriate assistance when necessary Exhibit appropriate behavior/attitudes Start to participate in extraocular surgery, as appropriate and under supervision, and participate in postoperative care Start the first half of the American Academy of Ophthalmology Basic & Clinical Science Home Study Course Attend the Stanford or Lancaster Basic Science Course Complete the Stanford or Lancaster Basic Science Course Complete the entire American Academy of Ophthalmology Basic & Clinical Science Home Study Course Synthesize history & physical findings into a differential diagnosis, formulate and carry out a treatment plan, with appropriate follow-up, particularly with ambulatory & ward consultations Continue to participate in extraocular surgery as appropriate under supervision, and participate in postoperative care Continue a personal education strategy Be able to diagnose and plan treatment for the more complicated medical & surgical eye diseases Participate in intraocular surgery Attend the Armed Forces Institute of Pathology course in Ocular Pathology Be able to establish a strong therapeutic relationship with patients and families, utilizing consultations and other health care professionals in an appropriate manner Contribute effectively and plan grand rounds, journal clubs, and teaching to other health care professionals Have an effective personal education strategy Be inquisitive Be an appropriate and effective patient advocate Deliver quality care with integrity, honesty & compassion Practice medicine ethically consistent with the obligations of a physician Attend the Future Focus course preferably in PGY 4 (given biannually) Page 33 of 47 Attend the Annual Meeting of the American Academy of Ophthalmology in PGY 5 METHODS: Regular & punctual attendance at clinics Regular & punctual attendance at surgery Attendance in Orthoptics Completion of relevant sections of the AAO BCSC Attend the Stanford or Lancaster Basic Science Course in Ophthalmology Lectures Journal Clubs Journals, books Attendance at scientific meetings, courses (as possible) Participate in a research project Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with 1. Patient’s and Their Families c. Explain general surgical disease processes d. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians e. Family physician f. Clinical microbiologist g. Lab technicians h. Internal Medicine Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Page 34 of 47 • • • • • Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for General Ophthalmology and Cataract, and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) F.1 Clinical (i) generate a clinical question (ii) identify her/his own knowledge and recognize deficits in knowledge about the question (iii) (iv) (v) (vi) (vii) develop a plan to remedy the deficit by a) conducting an appropriate literature search b) assimilating and critically evaluating the literature c) consulting other physicians and health care professionals propose a solution to the clinical question implement this solution in her/his practice evaluate the outcome of this solution generate new clinical questions... F.2 Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) develop a proposal to answer the research question by a) conducting an appropriate literature search b) assimilating and critically evaluate the literature c) identify, consult and collaborate with appropriate experts to undertake the research proposal (iii) propose appropriate methods for conducting the research (iv) undertake the proposed research (v) propose a solution to the clinical question (vi) disseminate and defend the results of the research (vii) identify future research opportunities and questions that arise from the results F.3 Education Page 35 of 47 (i) (ii) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. Page 36 of 47 Lacrimal, Lids & Orbits Medical Expert: The resident will demonstrate knowledge of: Orbit Orbital Anatomy & Physiology Bony orbit Bony apertures Orbital soft tissues Periorbital structures Cranial cavity Sinus cavities Nasal cavity Evaluation of orbital disorders Pain Proptosis Palpation Pulsaton Physical Exam and laboratory tests Inspection Palpation Auscultation Exophthalmometry Radiology Investigation CT MRI Ultrasound Plain X-Rays Venography Arteriography Orbital Pathology Classification & Management of orbital disorders Orbital disorders in children Congenital anomalies Infections & inflammations Tumours Orbital disorders in adults Infections & inflammations Tumours Thyroid eye disease Orbital surgery Surgical spaces Anterior orbitotomy Lateral orbitotomy Orbital decompression Pre and Post operative care Complications of orbital surgery Orbital trauma Orbital fractures Le Fort fractures Page 37 of 47 Orbital roof and rim fractures Blow-out fractures Orbital foreign bodies Orbital hemorrhage The anophthalmic socket Enucleation Evisceration Socket reconstruction Exenteration Lid Eyelid anatomy Skin & subcutaneous tissue Protractors Retractors Orbital septum & fat Tarsus Conjunctiva Eyelashes Meibomian glands Vascular supply Nerve supply Classification & Management of eyelid disorders Congenital anomalies Eyelid inflammation Eyelid trauma & burns Ectropion Entropion Symblepharon Trichiasis Ptosis Eyelid retraction Tumours Aging lid changes Eyelid and Canthal surgery Benign essential blepharospasm Lacrimal System Anatomy Secretory system Excretory system Physiology of tear production & out flow Evaluation of the tearing patient Structural tests Irrigation Probing Dacryocystography CT Functional test Dye disappearance Jones tests Scintigraphy Page 38 of 47 Tear film & lacrimal secretion Management of outflow disorders Punctal disorders Canalicular disorders Lacrimal sac disorders Nasolacrimal duct disorders Surgical techniques Punctoplasty Probing & irrigation Silicone intubation Dacryocystorhinostomy Canaliculo- Dacryocystorhinostomy Conjunctivo- Dacryocystorhinostomy Progression of Responsibility in Oculoplastic, Reconstructive, Orbital and Lacrimal Rotations Procedure Cycle 1 Cycle 2 Cycle 3 Evaluation of orbital disorders Interpret Radiology Investigation Management of orbital disorders Lateral orbitotomy Orbital decompression Orbital fracture repair Enucleation Evisceration Socket reconstruction Exenteration O,A,P O,A,P P P T T O,A P P,T O O O O,A O,A O,A O,A A A A A,P A,P A,P A A,P A,P A,P P,T P,T P,T A,P Evaluation of lid disorders Ectropion repair Entropion repair Trichiasis repair Ptosis repair Tumours excision Benign essential Blepharospasm-Botox O,A,P O,A O,A O,A O,A O,A O,A P A,P A,P A,P A,P A,P P T P,T P,T P,T P,T P,T T Evaluation of the tearing patient Punctoplasty Probing & irrigation Silicone intubation Dacryocystorhinostomy O,A,P P T O,A,P O,A,P O,A,P O,A P P P P T T T P O=Observe Page 39 of 47 A=Assist P=Perform major part (or whole) of the surgery under supervision T=Teach to more junior residents Communicator: Resident is expected to demonstrate communication skills in both verbal and written manner with 1. Patient’s and Their Families a. Explain general surgical disease processes b. Obtain informed consent related to surgical procedures 2. Health Care Professionals including Physicians a. Family physician b. Clinical microbiologist c. Lab technicians d. Internal Medicine e. Medical students 3. Nurses 4. Other specialist in infectious disease Collaborator: Be willing to participate in interdisciplinary teams, considering and respecting the opinions of other team members and contributing expertise as an Ophthalmologist. Identify and understand the roles, expertise and limitations of all members of an interdisciplinary team working to achieve a goal related to patient care, an educational program, a research project or an administrative activity. Work with the other members of the interdisciplinary team to develop a plan for an ophthalmology patient; this may include preoperative and postoperative investigations, treatments and continuing care both in hospital and in ambulatory settings. Manager: To achieve these competencies, upon of an ophthalmology rotation the resident will: • • • • • Realize appropriate resource allocation Share tasks on the ward with other residents and clinical clerks Design an appropriate method of communicating with other team members to assure smooth operation of the clinical team and avoid duplication and errors. Ensure that chart notes document important points in the patient’s course, treatment options, expectations and plans for care. Organize the workload appropriately to ensure that team members are able to participate in the rounds, in the operating room and in clinics as benefits the individuals. Page 40 of 47 • • Know the principle of Quality Assurance in clinical practice Give due attention to details Health Advocate: Be able to identify operative risk factors in individual patients. Identify risk factors for General Ophthalmology and Cataract, and factors that deleteriously affect operative risk factors and counsel patients on these risk factors. Scholar: While on the Ophthalmology service the resident should be starting to assess clinical problems by (under the following headings) 1 Clinical (i) generate a clinical question (ii) identify her/his own knowledge and recognize deficits in knowledge about the question (iii) (iv) (v) (vi) (vii) develop a plan to remedy the deficit by a) conducting an appropriate literature search b) assimilating and critically evaluating the literature c) consulting other physicians and health care professionals propose a solution to the clinical question implement this solution in her/his practice evaluate the outcome of this solution generate new clinical questions... 2 Research (i) start the process of generating a research question (basic science, clinical, population health or some combination) (ii) develop a proposal to answer the research question by a) conducting an appropriate literature search b) assimilating and critically evaluate the literature c) identify, consult and collaborate with appropriate experts to undertake the research proposal (iii) propose appropriate methods for conducting the research (iv) undertake the proposed research (v) propose a solution to the clinical question (vi) disseminate and defend the results of the research (vii) identify future research opportunities and questions that arise from the results 3 Education (i) demonstrate an understanding of the concepts of adult learning (in addition to the application) with respect to herself/himself and others Page 41 of 47 (ii) demonstrate an understanding of preferred learning methods in working with colleagues, residents, medical and nursing students and other health professionals Review texts, recommended reading and review articles in preparation for OR cases. Be able to critically review and appraise information as it relates to ophthalmology. Read around consults seen in the ER, clinics, and on the ward. Professional: Interact with patients, families, nurses and other health care personnel in a professional manner with appropriate attitudes. Work to maintain and advance professional competence. Respect all opinions of health care workers as well as the patient and their family. Provide care in an ethical manner. Examine and resolve interpersonal difficulties in professional relationships. Strive to balance personal and professional roles and responsibilities, and to demonstrate ways to resolve conflicts in these areas. Constantly evaluate her/his knowledge, skills and abilities, and recognize the limits of her/his professional competence. Page 42 of 47 External Courses proposed for Residents Although McMaster’s half day program is rigorous and complete. We firmly believe in sending residents to supplement their education with exposure to highly rated external courses. Each year of the residency will involve at least one main external course and the following have been proposed. PGY1 — Toronto Ophthalmology Residency Introductory Course (TORIC) — This course provides a basis for incoming PGY2 residents. It is a comprehensive basic science course taught over six weeks by leading educators and clinicians from across Canada. PGY2 — Surgical “Boot Camp” — This dynamic new course is a 3 day intensive one-on-one introduction to surgical procedures in Ophthalmology with Dr. Guillermo Rocha in Brandon, Manitoba. PGY2/3 - Lancaster/Stanford — basic science course over a 7 or 8 weeks time frame at the end of PGY2 & beginning of PGY3 years. PGY4 — American Academy of Ophthalmology — The residents will attend the Annual conference at least once during residence, typically in PGY4. PGY5 — San Antonio Review Course, or equivalent — This is a one week intensive review course in preparation for the Fellowship exam that is very popular with residents across North America The residents will also attend the Canadian Ophthalmological Society (COS) Annual Conference (rotating locations) Local Annual Conferences and Academic Days — Southern Ontario is home to 5 of Canada’s 11 Ophthalmology residency program and attendance at the local continuing education clinical conference days will be encouraged. These include Sally Letson (Ottawa), Walter Wright (Toronto), Jack Crawford (Toronto), Paul Stringer (Hamilton), University of Western Ontario Clinical Day in Ophthalmology Local Research Days — Each University also hosts an annual research day for residents and faculty to present work in lecture and in poster format. Page 43 of 47 Research Dr. P Harvey – Resident Research Coordinator Commensurate with the goals of the program, residents are expected to engage in research during their years in training. The experience of conceiving a research idea and seeing it through the multiple stages involved in arriving at publication is an invaluable learning experience. This is an active way of learning the skills of critical review, ethics in research, collaboration, statistics, and scientific writing. A minimum of one peer reviewed publication with presentation at COS or internationally is required during residency. Residents keen on pursuing more research will be encouraged to do so, and the department will always strive to accommodate their needs in these endeavours. There are many active clinical projects at McMaster in most subspecialty fields. Furthermore, our proximity to several other residency programs as well as the only Optometry school in Ontario provides for ample opportunity for multi-centered work and collaboration with colleagues. Source McMaster Surgical Associates Research Advisory Committee Medical Council of Canada McMaster Centre for Leadership in Learning (Large Grants) Funding Sources- Education Research Deadline Amount Eligibility Restrictions Early Jan yearly ON HOLD Feb1/12 (not updated for 2013 yet) Feb 1st Yearly Up to $30K 7500k/resident/p roject/year $37 500/1 yr $10K McMaster Centre for Leadership in Learning (Small Grants) Feb 1st, July 1st, Nov1st, Yearly $1K RCPSC (Medical Education Research Grant) Mar 2/12 (not updated for 2013 yet) $25K/yr for 3 years, up to maximum of $50K RCPSC (Royal College/AMS CanMEDS Research and Development Grant) Mar 2/12 (not updated for 2013 yet) $25K/2yrs -applicant must be a member -application information emailed out -resident -medical assessment research -Pl may be faculty, staff or graduate students of a Canadian Medical Facility -proposed project should improve quality of students’ learning -priority given to projects that benefit large #s learners, have application to other courses, optimize use of existing resources, involve collaboration -proposed project should improve quality of students’ learning -priority given to projects that benefit large #s learners, have application to other courses, optimize use of existing resources, involve collaboration -curriculum design and implementation, instructional methods, assessment, program evaluation, continuing education, professional development, and faculty development -applicants must be involved in teaching and/or medical education research in Canada, Fellow must contribute -supports research, development, and/or implementation of projects to enhance specialty education in the promotion of the key roles for specialists as defined by CanMEDS, includes faculty development, course development and/or medical education research Page 44 of 47 RCPSC (Faculty Development Grant) Mar 2/12 (not updated for 2013 yet) $5K/1yr Association for Surgical Education CESERT Grants June 1st, Yearly $25K/1-2 yrs Source McMaster Surgical Associates Research Advisory Committee PSI Foundation (Health Research) -applicants must be involved in teaching and/or medical education research in Canada, Fellow must contribute -supports creation, promotion, and evaluation of, and/or research on, new and innovative methods of faculty development to foster the training of quality teachers -applicants must be involved in teaching and/or medical education research in Canada, Fellow must contribute -innovation in surgical education -ASE member or non-member working with a member Funding Sources- Ophthalmology Deadline Amount Eligibility/Restrictions Early Jan Yearly ON HOLD Dec 6th 2012, Mar 7th, June 6th 2013 Up to $30K $7500K/resident/pr oject/year $85K/year (clinical research) for 2 years with possibility of renewal for 1 further year $20K for 1 year PSI Foundation (Resident Research) Dec 6th 2012, Mar 7th, June 6th 2013 CNIB (Baker Applied Research Fund) Jan 15th Yearly (opens in Nov) $35K/1yr CNIB (Baker New Researcher Fund) Jan 15th Yearly $35K/1yr CNIB (Baker Fellowship Fund) Jan 15th Yearly Max $30K/year McWork.-summer employment Jan 30th Yearly Subsidy for minimum wage Glaucoma Research Society of Canada (Seed Funding) Jan 20/12 (not updated for 2013) $20K/1yr -applicant must be a member -application information emailed out -resident -PI is practicing physician with academic appt -no cancer, heart and stroke or mental health projects -animal work only if animals are immediate patient surrogate -resident must be supervised by faculty member: supervisor is applicant, resident is PI -may apply for cancer, heart/stroke and mental health projects -social, educational, cultural and rehab needs of persons living with vision loss -new investigator or senior researcher developing program of applied research -equip costs not covered except if matched by host facility, travel/pub cost not to exceed $2K -PI within 5yrs of MD or PhD -seed money for bigger grants -equip costs not covered except if matched by host facility, travel/pub costs not to exceed $2K -recipients must begin or return to an academic posting in Canada within three years of completing their training, or return to an area of need as supported by a letter from the Medical Director of the community. -funding for McMaster students yrs 1-3 -Contact- Anne Lancaster -Surgeons must apply through Surgery HR and must have funds available to cover the cost of the student -basic and clinical research into all aspects of glaucoma -PI must have Canadian university of academic hospital appointment -MSc or PhD students if supervised by a Page 45 of 47 HHS New Investigator Fund Mar 31st, Oct 1st Yearly Seed grant of $50K for 12-18 months PSI/CSCI Prizes for Resident Research Canadian Glaucoma Clinical Research Council (CNIB-CGCRS Award) American Health Assistance Foundation (Macular Degeneration Research Award Program) Glaucoma Research Foundation (Shaffer Grants) May 31st yearly 5 $2000 prizes, top paper additional $1000 $5K-$25K for Pls>5yrs Training or practice Up to $5K for pls<5yrs $120K/2yrs June 30/12 (not updated for 2013) LOl July 10/12 Full app (invite) Nov 9/12 Prelim app July 31st Full App (invite) Sept 30th, Yearly $40K/1yr RMA Scholarship (Postgrad Med Education) Aug 31st Yearly Glaucoma Foundation Sept 1/12 (not updated for 2013) $7500 Travel costs of up to $1000 within 2yrs of completion to present $40K/1yr Renewal of up to $50K Foundation Fighting Blindness (Operating Grant) LOI- Nov 15/12 Full app- Jan 31/13 $50-100K/yr for 2yrs American Health Assistance Foundation (Glaucoma Research Award Program) HAHSO Innovation Grant Nov2/12 $100K/2yrs Nov 5/12 $100K/2yrs preceptor -PI must be HHS medical staff, within 5 years of either 1st faculty appt as PI or 1st 5 years of performing own research -must have experienced researcher as mentor, who is Co-I on grant, who is HHS staff and who has received peer rev funding- residents are eligible if research occurs at HHS site -PD must nominate resident -only completed research eligible -improve patient outcomes through understanding of treatment and progress of glaucoma -encourage collaboration -pilot study grants -no duplicate funding -basic science and/or clinical research collaborations -high impact basic/epidemiological/clinical-based research -strategic goals: protect/restore optic nerve, detect/monitor progress, genetics, intraocular pressure/treatments, risk factors using systematic outcomes data -resident must be PI-new project, not added to an existing project -PI must have fulltime faculty appointment -expert in glaucoma or collaborating with one -special interest in: Optic Nerve Rescue and Restoration, Molecular Genetics, and Nanotechnology -origin, detection, prevention, treatment and cur of retinitis pigmentosa, macular degeneration and related blinding retinal diseases -pilot study grants -no duplicate funding -basic science and/or clinical research collaborations -development of new and innovative practices fin healthcare delivery and support leadership and dissemination of knowledge across the healthcare system. Page 46 of 47 Chief Resident Role The Chief Resident is a senior resident, in his/her fourth year of residency. Primary Roles: Representation of the Resident body within Departmental meetings Organizing the call schedule on a monthly basis Planning vacation times based on resident requests and availability within the schedule Organize morning rounds Relaying resident concerns to the Program Director Helpful Tips for PGY1 Residents Contact the Postgrad office and stay on top of CPSO and CMPA membership paperwork BEFORE July 1st Parking at SJH Stoney Creek site — contact Maria ext 4816 regarding tokens (site is not covered by the parking transponder) Remember to register for AAO and COS, will get free subscription to journals and other perks Get a T2200 tax form — talk to payroll about it For various support mechanisms for your time here at McMaster University, please refer to the Postgraduate Medical Education Office’s “Resident Wellness Support Systems” booklet. Always keep in mind that the Program Director is here to help support and guide you through our residency program. Page 47 of 47



















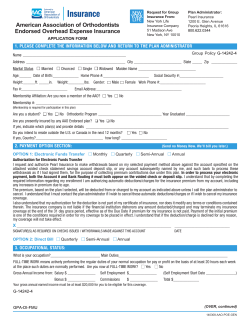

© Copyright 2025