
TABLE OF CONTENTS Section Subject Page #
FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory TABLE OF CONTENTS Section I Subject Page # GENERAL INFORMATION INTRODUCTION VISION STATEMENT MISSION STATEMENT LICENSURE AND ACCREDITATION LABORATORY DEPARTMENTS CONSULTATION SUPPORT STAFF MEDICARE COMPLIANCE What will Medicare cover? Background Medical Necessity Documentation Statutorily Excluded Services Medicare Coverage Limitations Types of Limitations Medicare Coverage Decisions Affecting Lab Testing Medicare Compliance Checking Tool To Check Compliance To Perform a Diagnosis Narrative Search Advance Beneficiary Notice (ABN) Purpose When to ask Medicare beneficiaries to sign an ABN Where to get an ABN Form Steps to obtaining an ABN Disclosure of Medicare Regulations GENETIC TESTING Informed Consent LABORATORY ORDERS Required Patient Information Outpatient Order: Required Information Inpatient Order: Required Information Laboratory Requisitions Outpatient Laboratory Requisition Inpatient Laboratory Requisition: OTHER FORMS Advanced Beneficiary Notice (ABN) Informed Consent for Vermont Informed Consent for New York State Telephone or Fax Laboratory Order Form Laboratory Mailing Request Form Supply Order Form Lead Demographic Form ANONYMOUS PATIENT TESTING 3 3 3 4 5 6 9 9 9 9 9 10 10 10 11 11 12 14 14 14 14 14 16 17 18 19 19 19 19 20 21 21 22 22 22 22 22 22 22 22 23 1 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory TELEPHONE TEST ORDERS ADDING A TEST TO AN EXISTING ORDER STANDING ORDERS REFLEX TESTING LABORATORY TESTS SUBJECT TO REFLEX ANATOMIC PATHOLOGY AND REFLEX TESTING CUSTOM PROFILES BILLING INFORMATION OUTPATIENT BLOOD DRAWING SITES RESULT REPORTING Laboratory Report Devices Cytopathology and Anatomic Pathology Report Print Schedule Clinical Pathology Report Print Schedule Client Report Fax Lab Order Priority Designations STAT Call/Fax Result Routine Critical Values COURIER LABORATORY SUPPLIES STAT LIST CRITICAL VALUES LIST APPENDIX Advanced Beneficiary Notice (ABN) Informed Consent New York State Informed Consent Vermont Laboratory Mailing Request Supply Order From Telephone Laboratory Results Form Telephone/Fax/Standing Order Request Form II SPECIMEN HANDLING III SPECIMEN REQUIREMENTS IV DISEASE MANAGEMENT V SPECIAL INSTRUCTIONS VI FEES 24 24 25 26 27 29 33 34 35 36 36 36 36 39 40 40 40 41 41 42 42 43 46 2 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory INTRODUCTION Fletcher Allen Health Care was formed on January 1, 1995 as the result of a merger between the Medical Center Hospital of Vermont, Fanny Allen Hospital, and the University Health Center, with the University of Vermont as an affiliated partner. DEPARTMENT OF PATHOLOGY AND LABORATORY MEDICINE VISION STATEMENT Pathology and Laboratory Medicine strives to be the best regional, academic Clinical and Anatomic Pathology Laboratory with areas of national and international prominence in Laboratory Services, Education, and Research. MISSION STATEMENT To deliver excellent pathology and laboratory services that support the patient care mission of Fletcher Allen and other regional organizations, support clinically relevant research and education, and provide consultative services within its areas of expertise. 3 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory LICENSURE AND ACCREDITATION Fletcher Allen Health Care Laboratories are accredited by the following agencies. AABB ASHI CAP CLIA88 TJC NYS UNOS ACC Laboratory* 001058 03-1-VT-01-1 1182501 47D0660960 5483 3584-LAP34308 01VTMC Fanny Allen Laboratory** Electron Microscopy Laboratory*** 1182801 1182508 *Ambulatory Care Center (ACC) Laboratory is located at the main hospital, East Pavilion 1 and 2, 111 Colchester Avenue, Burlington VT, 05401. **The Fanny Allen Laboratory is located at the Fanny Allen Campus, 360FA1, 101 College Parkway, Colchester VT, 05446 ***The Electron Microscopy laboratory is located at the University of Vermont, Microscopy Imaging Center, Health Science Research Facility, Room 204, Burlington VT, 05405. AABB: American Association of Blood Banks ASHI: American Society for Histocompatibility & Immunogenetics CAP: College of American Pathologists CLIA88: Clinical Laboratory Improvement Amendments’88 TJC: The Joint Commission on Accreditation (formerly JCAHO) NYS: New York State Department of Health, Clinical Laboratory Permit UNOS: United Network for Organ Sharing 4 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory LABORATORY DEPARTMENTS Pathology Laboratory, Ambulatory Care Center East Pavilion-Level 2 Cytopathology Cytology Cytotechnology School Surgical Pathology Cutting Room Histology Autopsy Clinical Laboratory, Ambulatory Care Center East Pavilion-Level 1 Blood Bank Compatibility Testing Donor Center HLA Immunohematology Stem Cell HLA Testing General Chemistry Blood Gases General Chemistry HIV-Stat Mono Test Pregnancy Test-Urine Urinalysis Hematology Hematopathology Manual Differentials Routine Coagulation Special Hematology Special Chemistry 1 Atomic Adsorption Chromatography ELISA GLC Immunoassay QUAD Marker Special Coagulation Cytogenetics Flow Cytometry Special Chemistry 2 Electrophoresis Nephelometry Microbiology Bacteriology Susceptibility Testing Occult Blood Special Microbiology 1 Mycology Mycobacteriology Parsitology Virology Molecular Testing Antigen Detection 5 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory CONSULTATION SUPPORT STAFF ADMINISTRATION Edwin G. Bovill, M.D., Director and Chairman Thomas S. Wadsworth, MBA, MT (ASCP), SBB, Administrative Director ACC Lab Office, Phone ACC Lab Office Fax 656-2931 847-3933 847-0241 847-3509 ANATOMIC PATHOLOGY Kumarasen Cooper, MBChB, Director Timothy St. John, CT (ASCP), Manager Karen Brown, Coding and Transcription Supervisor Anatomic Pathology Office Anatomic Pathology, Fax 847-9766 847-5134 847-3501 847-3566 847-3509 AUTOPSY SERVICES Masatoshi Kida, M.D., Director Timothy St. John, CT (ASCP), Manager Jude Carpenter, HT, HTL (ASCP), Supervisor Autopsy Office Autopsy Fax 847-9917 847-5134 847-5116 847-3570 847-6443 BLOOD BANK Mark Fung, M.D., Director Chuck Powden, CLLSp (H), Manager Paulette Hammond, MT (ASCP), Supervisor Sharon Bushor, MT (ASCP), Technical Specialist 847-5145 847-5137 847-5147 847-3523 BUSINESS DEVELOPMENT & OUTREACH Lynn Bryan, Manager Eleanor Sinclair, Reimbursement Specialist Colleen Williams, Senior Marketing Specialist Valerie Rogers, Client Relations Specialist Nicole Carney, Client Relations Specialist Lee Stirling, Client Relations Specialist Outreach Fax Billing Fax 847-9540 847-0234 847-9473 847-9472 847-6689 847-7754 847-7418 847-8190 SPECIMEN RECEIVING Ron Bryant, M.D., Director Monica Sullivan, MT (ASCP) Manager Cindy Cruickshank, M (ASCP), Supervisor Elizabeth Manning, MT (ASCP), Charge Technologist John Frost, Evening Charge Technologist Specimen Receiving Fax 847-5139 847-5123 847-5127 847-4763 847-4763 847-2358 CHEMISTRY Greg Sharp, M.D., Director Monica Sullivan, MT (ASCP) Manager Cindy Nelson, MT (ASCP), Supervisor, Special Chemistry Judy Schwenn, MT (ASCP), Supervisor, High Volume Chemistry Jocelyne Stocker MT (ASCP), Technical Specialist Chemistry Fax 847-5115 847-5123 847-5124 847-2714 847-5117 847-6079 6 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory CLINICAL PATHOLOGY Ronald Bryant, M.D., Director Clinical Pathology Hot Seat Clinical Pathology Fax 847-5139 847-3795 847-3987 COAGULATION Edwin Bovill, M.D., Director Chuck Powden, CLLSp (H), Manager Russell Brown, MT (ASCP), Supervisor 656-2931 847-9692 847-1201 COMPLIANCE Compliance Hot Line Janet Schroeter, MT (ASCP), Laboratory Compliance Specialist Kathy Nadeau, MLT (ASCP), Asst. Laboratory Compliance Specialist Compliance Fax 847-9430 847-9435 847-0930 847-7418 CUSTOMER SERVICE Lynn Bryan, Manager Michele Baker, Supervisor Customer Service Customer Service Fax, (ACC East Pavilion 1) 847-9540 847-7131 847-5121 or 1-800-991-2799 847-5905 CYTOGENETICS Mary Tang, M.D., Director Chuck Powden, CLLSp (H), Manager Catherine Buck, MT (ASCP) CLSP (GC), Charge Technologist Cytogenetics Fax 847-2894 847-5137 847-3565 847-3987 CYTOPATHOLOGY Gladwyn Leiman, MBBCh, FRCPath, Director Timothy St. John, CT (ASCP), Manager Carol Colasacco, CT (ASCP), Supervisor Cytopathology Fax 847-5136 847-3921 847-5134 847-6199 847-3632 FANNY ALLEN CAMPUS LAB John Lunde, M.D., Director Chuck Powden, CLLSp (H), Manager Fanny Allen Lab, Fax 847-5135 847-5137 847-6424 HEMATOLOGY John Lunde, M.D., Director Chuck Powden, CLLSp (H), Manager Russell Brown, MT (ASCP), Supervisor Hematology Fax 847-5125 847-3683 847-5137 847-1201 847-3509 7 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory HISTOLOGY Alexandra Kalof, M.D., Director Timothy St. John, CT (ASCP), Manager Jude Carpenter, HT, HTL (ASCP), Supervisor Histology Fax 847-2712 847-6868 847-5134 847-5116 847-3509 FLOW CYTOMETRY John Lunde, M.D., Director Chuck Powden, CLLSp (H), Manager Russell Brown, MT (ASCP), Supervisor Danielle Sartini, MT (ASCP), Technical Specialist 847-3683 847-5137 847-1201 847-5373 INFORMATION SERVICES, PATHOLOGY Information Services Fax Tania Horton, Lead 847-5614 847-6336 MICROBIOLOGY Washington Winn, M.D., MBA, Director Monica Sullivan, MT (ASCP), Manager Fred Westenfeld, MT (ASCP), SM, Supervisor Debra Reardon, MT (ASCP), Technical Specialist Sharon Weisburgh, MT (ASCP), Technical Specialist Microbiology Fax 847-3554 847-5140 847-5123 847-5141 847-5142 847-6584 847-4806 NIGHTS Chuck Powden, CLLSp (H), Manager Christopher Carpenter, MT (ASCP), Supervisor 847-5137 847-3620 PHLEBOTOMY Lynn Bryan, Manager Susan Antell, MT (ASCP), Supervisor, Outpatient Phlebotomy Michele Baker, MT (ASCP), Supervisor, Inpatient Phlebotomy 847-9540 847-1080 847-7131 SATELLITE LABS – POINT OF CARE TESTING (POCT) Lynn Bryan, Manager Sue Antell, MT (ASCP), Supervisor Marie Beede, MT (ASCP), Technical Specialist POCT, Fax 847-9540 847-1080 847-8973 847-3509 SURGICAL PATHOLOGY Donald Weaver, M.D., Director Timothy St. John, CT (ASCP), Manager Jude Carpenter, HT, HTL (ASCP), Supervisor Hot Seat Surgical Pathology Fax 847-3566 847-5928 847-5134 847-5116 847-3795 847-4155 8 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory MEDICARE COMPLIANCE What will Medicare cover? Background Medicare, like private insurers, makes decision about what services will be covered under their program. While both Medicare Part A & Part B cover clinical laboratory testing, not every test in every clinical situation is covered. Services that are generally excluded from coverage include routine health examinations and services that are not reasonable and necessary for the diagnosis or treatment of an illness or injury. Some specific types of screening services such as pap smears for cervical cancer, fecal occult blood for colorectal cancer screening and PSA for prostate cancer screening are specifically covered by statute, but may be subject to frequency limitations. Medical Necessity Documentation Documentation of medical necessity is of utmost importance. Under the Balanced Budget Act of 1997, physicians are required to supply a diagnosis to the laboratory for services provided so the laboratory can be paid. Medicare requires hospital laboratories to submit all the diagnosis information, in the form of ICD-9 codes, provided by the referring physician on claims. Medicare will only pay for testing that meets Medicare’s definition of “medical necessity”. Therefore, a physician may order a laboratory test that they believe is appropriate for the patient, however, Medicare will deny payment unless it meets Medicare’s definition of medical necessity. To determine the correct ICD-9 code to use, please refer to the current version of the International Classification of Diseases, 9th Revision, and Clinical Modification (commonly referred to as the Physician’s ICD-9 CM manual). Please submit the specific diagnosis that describes the patient’s signs and symptoms pertaining to why the laboratory testing was ordered. An ICD-9 code is preferable to a narrative diagnosis. We are happy to help you with ICD-9 coding if needed. Please refer to the Compliance contact list for assistance. Statutorily Excluded Services Medicare has published a list of ICD-9 diagnosis codes that are statutorily excluded from coverage regardless of the service. This means that services (including laboratory testing) submitted to Medicare with only a statutorily excluded diagnosis code will not be covered. A statutorily excluded ICD-9 code may be the most appropriate diagnosis code to use in some cases. If a more specific ICD-9 code or sign/symptom is relevant to the requested testing then it too should be added as diagnosis information on the laboratory requisition. If a statutorily excluded ICD-9 code is the only appropriate ICD-9 diagnosis code, Medicare requires that we, as the billing entity, indicate to Medicare on the claim that it is a non-covered service. Advance Beneficiary Notices (ABN’s) should not be used for services that are statutorily excluded. Please remind patients in this circumstance that Medicare will not pay and that the beneficiary is ultimately responsible for the charges. 9 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Medicare Coverage Limitations Types of Limitations Laboratory testing is subject to the following limitations: 1. Medicare does not cover lab testing considered to be investigational or experimental. 2. Medicare generally does not pay for any tests ordered for screening purposes (usually indicated by V-codes). There are exceptions noted below which are specifically covered by statute, however, the coverage is subject to frequency limits: • • • • • 3. Pap Smear screening for cervical or vaginal cancer PSA for prostate cancer screening Fecal Occult Bloods for colorectal cancer screening Screening for Diabetes Mellitus Cardiovascular Disease Screening Coverage Decisions are predicated on what is considered “medically necessary”. Medicare believes some tests may be over utilized (ex. Urine cultures, CBCs, Glucose, TSH). Their response to the perceived over utilization was to create the coverage decisions which define & limit the circumstances under which the test(s) will be covered. Medicare’s coverage decisions can be at a national or local level. • • National Coverage Decisions (NCD’s) An NCD is a policy developed at the national level that establishes the diagnoses (ICD-9 codes) under which a particular procedure/test will be considered medically necessary and thus reimbursable by Medicare. Local Coverage Decision (LCD’s) A local coverage decision is similar in purpose to an NCD except that it is developed at the local level (ex. VT/NH) either by our Medicare Carrier or Fiscal Intermediary. A local contractor may only continue to issue an LCD if there is no national policy or if they wish to supplement an NCD when it doesn’t address a specific issue, such as frequency. Medicare Coverage Decisions Affecting Lab Testing with Links to View Policy Online If a lab test is ordered and will not be considered medically necessary based on one of the coverage limitations, please obtain an Advance Beneficiary Notice (ABN). Please visit our website http://www.FAHC.org/Pathology/Services/MedicareCompliance for more information. 10 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Medicare Compliance Checking Tool Fletcher Allen Health Care (FAHC) offers access from the web to the Pathline Medicare Compliance Checker. Pathline is a software application that includes a tool to help you work out Medicare Compliance rules. This tool is also useful for looking up ICD-9 codes from a narrative. In the URL Address box enter: http://pathcc.fahc.org for the direct link to the Medicare Compliance Checking for VT and NH (database). You do not need a user name and password to use the compliance checker. To Check Compliance 1. Select Division: From the drop down menu select: LAB Choices: LAB – Laboratory CARD – Cardiology RAD – Radiology Note: Show NCD/LMRP Tests: This option will show all tests for the division selected that have a local or national coverage policy. 2. Entering a Test If you do not know the FAHC test code for the test you are checking on, enter the test name in the box under Procedure/Tests and hit Search. When you find the test, click on the code and it will populate the search field. You can add another test in the Procedure /Test box and hit search to look for another test or enter the test code and press Add. NOTE: If only one test is added to the list box you can press Display Covering Diagnosis and view all ICD-9 codes that are covered for that test. 3. Entering a Diagnosis You can add a narrative to the Diagnosis box and press Search to find the correct ICD-9 code or if you know the correct code, you can enter the code and press Add. 11 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory To Perform a Diagnosis Narrative Search In the Diagnosis search box add the word or words you need the ICD-9 code for. Press Search. The search result will return a list of all possible ICD-9 code matches. Here is a search result for Hypothyroidism. ICD Search Search For (7 Matches) Code 243 244.0 244.1 244.2 244.3 244.8 244.9 Desc Congenital hypothyroidism Postsurgical hypothyroidism Other postablative hypothyroidism Iodine hypothyroidism Other iatrogenic hypothyroidism Other specified acquired hypothyroidism Unspecified hypothyroidism Select the most appropriate code by clicking on the underlined code number. 12 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory You can also look up a diagnosis by entering the ICD-9 code or partial code into the Diagnosis search box and pressing Search. The search result will return all entries with the diagnosis entered. Here is a search result for the partial code V52. ICD Search Search For (7 Matches) Code V52.0 V52.1 V52.2 V52.3 V52.4 V52.8 V52.9 Desc Fitting and adjustment of artificial arm (complete) (partial) Fitting and adjustment of artificial leg (complete) (partial) Fitting and adjustment of artificial eye Fitting and adjustment of dental prosthetic device Fitting and adjustment of breast prosthesis and implant Fitting and adjustment of other specified prosthetic device Fitting and adjustment of unspecified prosthetic device Select the most appropriate code by clicking on the underlined code number. NOTE: If you press the Search button without a code in the search box you will get a listing of all ICD-9 codes in numerical order. 4. When all the tests and codes are entered press Check Compliance. Checker Results Test (CPT) Diagnosis 244.3, TSH(84443) 250.00 244.3, √ LPR(80061) 250.00 PSA(84153) Reason Medically necessary according to NCD-Thyroid titled THYROID TESTING and dated 07/01/2008 Medically necessary according to NCD-Lipids titled LIPIDS and dated 10/01/2006 Medicare does not pay for these items/services for your condition. The following options will display as per Medicare rules based on tests/diagnoses entered: 1. (Green 2. 3. 4. 5. ) a This CPT code is not subject to Medicare coverage policy. b. Medically necessary according to (LCD/NCD titled …..) (Yellow ) Medically necessary according to frequency rules titled….. (Red ) Medicare does not pay for these items/services for your condition. (Yellow/green ) Some test have frequency limitations, if they are not met a message will display stating the frequency limitation. Ex. Fecal Occult Screening covered once a year for persons over 50. (Black -- ) NA – not applicable. If the Compliance Checker labels a test with an X of any color, an ABN must be obtained. 13 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 66.91 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Advance Beneficiary Notice (ABN) Purpose: An Advance Beneficiary Notice (ABN) is a written document used to notify a Medicare patient of the likelihood that Medicare will deny payment for the ordered tests(s) and to indicate the patient’s agreement to accept responsibility for payment if the service is not covered by Medicare. An ABN allows beneficiaries to make informed consumer decisions about receiving items or services for which they may have to pay out-of-pocket and to be more active participants in their own health care treatment decisions. When to ask Medicare beneficiaries to sign an ABN: 1. When ordering any procedure or test that is subject to a National Coverage Decision (NCD) or a Local Coverage Decision (LCD), where the ICD-9 code provided by the physician is not covered as part of the policy. 2. When ordering a screening test that is subject to a frequency limit and the frequency limit is not met. In the lab, the tests included are: • Pap smear for cervical cancer screening • PSA for prostate cancer screening • Fecal occult blood for colorectal cancer screening • Glucose testing as a screen for diabetes • Lipid testing as a screening for cardiovascular disease 3. When ordering a test which is considered experimental or investigational. Where to get an ABN Form: Contact Laboratory Customer Service at (802)847-5121 Steps to obtaining an ABN: 1. The following information must be completed on the ABN form before you present it to the patient to sign: • Patient’s name • Date of Birth • Medical record number • The specific procedure/test(s) you believe is/are likely to be denied by Medicare. • The reason you believe Medicare is likely to deny coverage. Check the most appropriate reason. If multiple tests and reasons are listed, please indicate which reason applies to which test. • Estimated cost 2. Present the ABN to the beneficiary or authorized representative* for review. 14 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory 3. When the beneficiary has read the ABN, ask them to choose an option by checking the appropriate box on the form. Option 1: I want the items and services listed above. You may ask to be paid now, but I also want Medicare billed for an official decision on payment which is sent to me on a Medicare Summary Notice (MSN). Option 2: I want the items or services listed above, but do not bill Medicare. You may ask to be paid now as I am responsible for payment. I cannot appeal if Medicare is not billed. Option 3: I don’t want the items or services listed above. I understand with this choice I am not responsible for payment, and I cannot appeal to see if Medicare would pay. 4. 5. Ask the beneficiary or authorized representative* to sign and date the form. If the beneficiary refuses to sign either option but demands the service, the provider should annotate the ABN, and have the annotation witnessed by a fellow staff member, indicating the circumstances and persons involved. The signature line can be used for the annotation. 6. The ABN is a 3 part form and must be distributed as follows: • Copy given to patient • Copy filed in physician’s office • Copy attached to appropriate clinical requisition Please Note: 1. Do not routinely ask all Medicare patients to sign ABNs. This is considered a “blanket ABN” and is not an acceptable practice. Use the ABN only when you believe Medicare will deny payment for an ordered test for one of the reasons listed on the ABN. Exception: In the case when a service/test provided is subject to a frequency limitation, the physician or supplier may routinely give ABNs to beneficiaries because the physician may not know when or where the patient last had the test performed (i.e. may have been ordered by another physician in a different location). 2. The ABN must be presented before the service is provided or before testing of specimen begins. 3. The beneficiary must be provided with an estimated cost to help them make an informed decision. 1. 2. 3. 4. 5. 6. ***Reminder: A valid ABN must: Be on an approved CMS-R-131 (03/08) form. Clearly identify the test or service. Give the reason why denial is likely to occur. Indicate the option chosen by the beneficiary. Be dated & signed by the beneficiary or authorized representative*. Provide the cost of test/service not meeting medical necessity rules. * An authorized representative is a person who is acting on the beneficiary’s behalf when the beneficiary is temporarily or permanently unable to act for himself/ herself. The authorized person is acting in the beneficiary’s best interests and does not have a conflict of interest with the beneficiary. Examples: spouse, adult child, adult sibling, close adult friend, and public guardian. A representation of the ABN form is located at the back of this section. 15 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Disclosure of Medicare Regulations In an effort to keep our physician clients informed of Medicare regulations as they pertain to the laboratory, we provide the following notice on an annual basis to all physician clients. Please note that Medicare will only pay for tests that meet the Medicare coverage criteria and are reasonable and necessary to treat or diagnose an individual patient. Section 1862(a)(1)(A) of the Social Security Act states, “no payment may be made under Medicare Part A or Part B for any expenses incurred for items or services which are not reasonable and necessary for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body member.” In addition, Medicare has developed coverage policies at both the national and local level. These policies limit and define the diagnosis (ICD-9) codes that will support medical necessity for a particular laboratory test. Medicare can issue or update coverage policies at any time. As we receive these policies we will continue to pass them on to our clients. The importance of an accurate diagnosis being submitted with each laboratory test request cannot be overstated as this is the means by which Medicare justifies medical necessity. Our laboratory offers the organ or disease oriented panels listed: Basic Metabolic Panel, Comprehensive Metabolic Panel, Electrolyte Panel, Lipid Panel, Liver (Hepatic Function) Panel, and Prenatal Panel. On the back of our laboratory requisition we have provided a list of tests included in each panel with the CPT code used for billing. The Specimen Requirements section of our Lab Services Directory also describes what is included in each panel. These panels should only be ordered when all the tests in the panel are medically necessary. Our laboratory requisition provides the option to order as a panel or individually as needed. We are happy to provide the Medicare reimbursement schedule for any clinical laboratory procedure upon request. If this information is desired, please contact a Laboratory Compliance Specialist at (802)847-5121. Please note that Medicaid reimbursement will be equal to or less than the amount of Medicare reimbursement. A complete list of clinical consultants is available (see Telephone Number listing earlier in this section) should any questions arise regarding laboratory test ordering or interpretation of results. 16 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory GENETIC TESTING As defined by Vermont law, genetic testing means a test, examination or analysis that is diagnostic or predictive of a particular heritable disease or disorder and is of a human chromosome or gene; human DNA or RNA; or a human genetically encoded protein. Genetic testing does not include a test, examination or analysis of a human chromosome or gene, of human DNA or RNA, or of a human genetically encoded protein that is diagnostic or predictive of a particular heritable disease or disorder, if, in accordance with generally accepted standards in the medical community, the potential presence or absence of a mutation, alteration or deletion of a gene or chromosome has already manifested itself by causing a disease, disorder or medical condition or by symptoms highly predictive of the disease, disorder or medical condition. State regulations define what is considered genetic testing. Regulations are applied by where the sample is obtained, not the residence of the patient. Examples of Genetic Testing Carrier Identification includes genetic tests used by families with a history of recessive genetic disorders and who are considering having children. Three common tests include those for Cystic Fibrosis, Tay-Sachs disease, and sickle cell trait. Late-onset Disorders include adult diseases such as cancer and heart disease. Genetic tests may indicate a susceptibility or predisposition for these diseases. Examples include Huntington’s disease, Myotonic Dystrophy and other DNA mutations analyses for single gene disorders. Prenatal Screening (Including QUAD Markers) Information from genetic testing can affect the lives of individuals and their families. In addition to personal and family issues, genetic disease or susceptibility may have implications for employment and insurance. Vermont and New York State require an Informed Consent from the patient prior to testing. It is the physician’s responsibility to obtain Informed Consent when ordering Genetic Testing. Guidelines for Informed Consent for Genetic Testing 1. Obtaining Informed Consent is the responsibility of the ordering physician. 2. Informed Consent is not necessary for genetic testing used for diagnosis in a symptomatic patient. 3. Informed Consent is necessary for genetic testing used to determine predisposition to a genetic disorder, carrier status, and screening of asymptomatic patients or family members. 4. We recommend: When in doubt, fill it out. 5. An Informed Consent should include the following information: i. Information about the sensitivity and specificity of the test has been reviewed ii. Test results may become part of the patient’s permanent medical record iii. Test results may impact the patient’s ability to obtain certain insurance benefits iv. Results are reported only to the ordering physician unless written authorization is obtained. 6. Informed Consent should be documented in the patient chart. 17 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Informed Consent An Informed Consent form for samples drawn in Vermont can be obtained at the Fletcher Allen Health Care Laboratory web-site http://www.fahc.org/pathology/ go to Services, Information for Health Care Professionals, Forms or by calling Customer Service at (802)847-5121. A representation of the form is located in the back of this section. Fletcher Allen Health Care Laboratory requisitions include the following reminder with regard to Genetic testing: Informed Consent Certification required for all genetic testing. Submission of an order for any laboratory test constitutes certification to Fletcher Allen Health Care that: 1. The Ordering Provider has obtained the “Informed Consent” of the patient as required by any applicable state or federal laws with respect to each test ordered; and 2. The Ordering Provider has obtained from the patient authorization permitting Fletcher Allen Health Care to report results of each test ordered directly to the ordering physician. 18 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory LABORATORY ORDERS Required Patient Information 1. We strongly discourage the use of prescription pads for laboratory test orders as the laboratory does not usually receive all the required information when orders are requested by this format. 2. In order for the Fletcher Allen Health Care Laboratory to perform the test requested by the physician and bill appropriately for that test, it is essential that the laboratory order be filled out correctly. 3. If you need forms for ordering laboratory testing, please call Customer Service (802)847-5121. Outpatient Order: Required Information 1. 2. 3. 4. 5. Patient’s full name (first and last name) Patient’s date of birth Sex of patient Billing provider (first and last name) If ordering provider different than billing provider, add ordering provider under [Additional Copy To] section (first and last name required). 6. Who should be billed: Electronic billing rules required that we submit the subscriber’s date of birth with each claim. a. If patient’s insurance, fill in lines 1-6 of billing section. b. If patient has no insurance, fill in lines 1 and 2 of billing section. c. To bill your office, supply correct 96 or 97 account number for billing. 7. ICD-9 code/diagnosis information 8. Specimen collection date and time 9. Specimen Type 10. The test(s) requested to be performed. 11. If Pap Smear requested on Medicare patient, whether physician considers it is screening (low or high risk) or diagnostic. See Pap smear guidelines in Section V, Special Instructions. Inpatient Order: Required Information 1. 2. 3. 4. 5. 6. 7. 8. Patient’s full name (first and last name). Patient’s MRN. Ordering Provider (first and last name). Specimen collection date and time. Specimen Type. The test(s) requested to be performed. For Cytology and Surgical Pathology, we need clinical diagnosis, pertinent history, previous lab data. Phone or beeper number for questions (optional but extremely helpful when there are specimen questions or critical lab values). 19 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Laboratory Requisitions The following is a summary of the laboratory order forms that we supply to outside clients. We customize the Account Information area with your practice name and phone number. Below are common fields on all forms. Please be sure to write legibly. We try to customize as much of the form as possible. If there are tests that you need to write in frequently, we can add these tests to your form. Account information: We customize this area with the following: Report Code/Location Code (Code set-up by Lab unique to your practice) Practice Name Phone Number (for patient or sample questions) Provider: In most cases the billing and ordering provider will be the same but in cases where they are different we require both. Please supply the provider(s) first and last name. Patient Information: This area is located on the top right of the form. We will need the patient’s full name along with two identifiers. The date of birth as well as the sex of the patient is required. Please provide the patients FAHC Medical Record Number if available, if not please provide the patient Social Security Number. Client ID: If you have an internal identifier (medical record number or protocol number) that you would like to have associated with this patient you would enter that information here. This identifier will print on the report. Additional Copy to: If you would like us to send another provider a copy of the report, please fill in the Additional Copy to area with the providers first and last name. If the provider is not local, please provide additional information, address and or fax number for report. Billing Information: Billing information is required on outpatients, if you are using this form on an inpatient you can ignore this area. Please let us know who should be billed. If we are to bill an insurance company or Medicare or Medicaid we will need subscriber’s date of birth with each claim, please fill in lines 1-6 in the billing area. If patient has no insurance, we require the name, address, and phone number of the person responsible for payment (lines 1 and 2 of billing section). If your office has an account number and you would like to charge the testing to your office please supply your billing number. 20 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Outpatient Laboratory Requisition: This is the form used to order clinical laboratory testing for Chemistry, Hematology, Microbiology and therapeutic drug levels. You can also order PAP Smears on this form. The form is dark green and white and the form number is 23-014951. Test(s) Requested: This area is located on the bottom half of the form. Tests included are the most commonly ordered tests listed by laboratory department. • Tests shaded green are subject to Medicare coverage policies (See Medicare Compliance in this section). • Tests that have a check (√) mark to the right of the test name are subject to Reflex (See Reflex Testing in this section). • Tests in Italics are available stat. • Specimen codes are listed to the right of the test name, B-blue top, Gn-green top, L-lavender top, S-red top (serum), T-serum separator (sst), U-urine, and X-See Laboratory Services Directory. Other Area: This area is for tests that are not already included on this form but that your office orders frequently. Cytogenetics /Flow/Bone Marrow Exam Lab Requisition: This form should be used for ordering Cytogenetics, Flow Cytometry or when you are requesting a Bone Marrow Exam All relevant diagnosis information should be documented in the Clinical Diagnosis/Pertinent History/Lab Data area located in the middle of this form. This form is maroon and white and the form number is 23-033734. Surgical Pathology/Non GYN-Cytology Requisition: This form is used for submitting tissue and cytology samples. The form is blue and white and the form number is 23-017154. All relevant diagnosis information should be documented in the Clinical Diagnosis/Pertinent History/Lab Data area located in the middle of this form. Genetic & Prenatal Laboratory Requisition: This form is used for submitting QUAD Markers and other prenatal and genetic screening. The form is purple and white and the form number is 23-017153. All relevant diagnosis information should be documented in the Diagnosis Information area located in the middle of this form. The prenatal screening questions must be filled in for result interpretation. Tests shaded are subject to Medicare coverage policies (See Medicare Compliance in this section). Inpatient Laboratory Requisition: Most laboratory orders should be sent through PRISM during computer downtime. Emergency Department Laboratory Requisition: This is the form used by the Emergency Department to order clinical laboratory testing for Chemistry, Hematology, Microbiology and therapeutic drug levels when Pathline is down. The form is black, white, and red and the form number is 23-014591. In-Patient Back-up Requisition: This form is used only on inpatients and only when HISPROD is down. This is the form used to order clinical laboratory testing for Chemistry, Hematology, Microbiology and therapeutic drug levels. This form is black, white, and green and the form number is 23-014667. Surgical Pathology / Non GYN-Cytology Order: This form is used for submitting tissue and cytology samples. The form is Blue and White and the form number is 23-036550. The top copy is the physicians order and is meant to be a part of the patient’s medical record. The back copy follows the sample to the lab. All relevant diagnosis information should be documented in the Clinical Diagnosis/Pertinent History/Lab Data area located in the middle of this form. 21 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory OTHER FORMS These forms are available in the Appendix to this section Advanced Beneficiary Notice (ABN) An ABN is a form that when used properly allows physicians and clinics to bill Medicare patients for services that Medicare deems not “medically necessary.” (See “Medicare Compliance” beginning on page 10) The ABN allows the Medicare beneficiary to make an informed decision about whether to receive a service that may not be deemed medically necessary, or a service that is governed by frequency limitations. Informed Consent for Vermont Informed Consent Certification is required for all genetic testing. Please See “Genetic Testing” beginning on page 18. Informed Consent for New York State Informed Consent Certification is required for all genetic testing. Please See “Genetic Testing” beginning on page 18. Telephone or Fax Laboratory Order Form This form should be used for call-in orders and for standing orders. Other laboratory requisitions do not fax well. Laboratory Mailing Request Form This form is required when you have a request for testing to be performed by a lab other than one we would normally send testing to. Supply Order Form This form lists all the supplies that we will provide for our clients use. Lead Demographic Form Vermont Department of Health collects patient demographic information on all lead testing. This form lists the required information. 22 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory ANONYMOUS PATIENT TESTING The laboratories at Fletcher Allen Health Care are committed to serving clients who need anonymous patient testing. Guidelines have been established to create a system in which this type of sample can flow. 1) The client must complete a Fletcher Allen Laboratory requisition with the following: a) b) c) d) e) Anonymous Name – 7 characters (to be supplied by client) Billing Provider Client location code 96 billing number Testing requested 2) The anonymous name needs to be assigned by the client office. The name is limited to 7 alphanumeric characters. The lab will add ANON,T to the code assigned by the office so the name will appear on the report as ANON,T * (* represents coded name assigned by your office). When the results arrive at the client office the correct person can decode the name and forward the result to the provider. 3) The testing must be billed to a 96 account number, which bills the client office. Since the testing is being done anonymously we cannot submit a bill to the patient’s insurance because we do not know the identity of the patient. 4) The client office will receive a bill for this testing and is responsible for collecting the money from the patient and paying Fletcher Allen Health Care for the testing. 5) If the patient is to be drawn in one of our outpatient drawing centers, all appropriate paperwork must accompany the patient. 6) If some testing will be done anonymously and some done under the patient’s name then two requisitions must accompany the sample and/or the patient. One will list the testing to be done anonymously and all appropriate information (see #1 above) and the other will have the patient’s name and billing information. Please submit a different sample(s) for each requisition, with the appropriate name on the tube. 23 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory TELEPHONE TEST ORDERS Although we prefer patients to present for laboratory testing with an outpatient requisition, Fletcher Allen Health Care Laboratory will accept telephone test orders. There are two types of telephone test orders, those taken as a new test order and those taken as an additional test for an existing order. New test orders can be called to Laboratory Customer Service at (802)847-5121. We will fax you a Telephone or Fax Laboratory Order Form for someone in your office to review, sign and fax back to (802)847-5905. The laboratory will require that a diagnosis be provided for all telephone orders. In addition, as telephone orders are taken, the laboratory staff will ask, “Is the order documented in the patient’s chart?” It is the physician’s responsibility to ensure the test order is documented in the patient’s chart. Federal law states that laboratories must request written documentation as a follow-up to any telephone orders received. You will be asked to verify telephone orders (both new and add-ons to an existing order) with written confirmation. For new orders, a form, the Telephone or Faxed Laboratory Order Form, will be faxed to you for this purpose. For add-ons to an existing order, the lab compliance staff will send you a list of telephone orders received on a biweekly basis. Please verify the information on the form or list is complete and accurate. Confirm your review by providing an authorized signature on the form and fax or mail it back to Fletcher Allen Health Care Laboratory ADDING A TEST TO AN EXISTING ORDER If you would like to add a test to an existing order, call Laboratory Customer Service at (802)847-5121 or 1-800-991-2799. Depending upon sample type we may be able to add testing on to samples previously sent to the lab. Samples are discarded after 5 days. Fax: (802)847-5905 Mail: Fletcher Allen Health Care Pathology and Laboratory Medicine Compliance Office, MP1-107 111 Colchester Avenue Burlington VT 05401 24 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory STANDING ORDERS When initiating a standing order, please fill out a Fletcher Allen Health Care Telephone or Faxed Laboratory Order Form. We will provide these forms to all our clients so that they may be used when a standing order is initiated. If a standing order is phoned into our lab, Customer Service will fill out the Telephone or Faxed Laboratory Order Form with the information we received. All Telephone orders must be followed by written confirmation. See Telephone Orders for information on that process. It is Fletcher Allen Health Care laboratory policy that standing orders be reviewed on at least an annual basis. Standing orders expire at the end of duration stated on original request and/or automatically expire 1 year from date of original request. The lab will send a reminder notice (Standing Order Confirmation) to the ordering physician asking for renewal, revision or cancellation of current standing order on all standing orders with an original duration of one year. The standing order will automatically be cancelled as of the expiration date, either at the expiration date stated on the original order or one year from original order date. We will only accept Standing Orders with a frequency of 4 months or less. A Standing Order for a test requested every 6 months for one year would be treated as a 1 time order six months in the future. 25 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory REFLEX TESTING Reflex testing occurs when initial test results are positive or outside normal parameters indicating that a second related test is medically appropriate for patient care. The Fletcher Allen Health Care Laboratory offers reflex testing in accordance with the Office of Inspector General’s Compliance Program Guidelines for Clinical Laboratories. It is the policy of Fletcher Allen Health Care Laboratory to list tests subject to reflex on the laboratory requisitions and to allow physicians the opportunity to decline the reflex testing if they believe it is not medically necessary. Fletcher Allen Health Care Laboratory will perform reflex tests automatically when the following conditions are met: Physician orders a test listed below and: 1. The initial test result meets the criteria listed below for prompting a reflex test or: 2. The specimen was sent to anatomic pathology and additional studies are needed to complete the evaluation of the case. Please refer to Anatomic Pathology and Reflex Testing on following pages. The physician has the option of declining reflex testing by writing in the name of the test in the box on the front of the laboratory requisition. All reflex testing is reviewed and approved by the laboratory pathologists or their designee on an annual basis. All Fletcher Allen Health Care Laboratory clients will be notified of changes to the reflex policy. Fletcher Allen Health Care bills for the reflex tests it performs using the CPT code listed in the chart. 26 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory LABORATORY TESTS SUBJECT TO REFLEX Initial Test Reflex criteria Reflex Test(s) Additional CPT billed Amphetamine screen, positive result Amphetamine confirmation 82145 urine ______________________________________________________________________________________ Antibody screen positive Antibody ID panel 86870* RBC Antigens 86905* Pretreatment serum 86975 *number of additional charges will vary depending on the # of antibodies and the extent of the work-up. ______________________________________________________________________________________ Anti neutrophil positive at screening dilution Anti neutrophil 86256 Cytoplasmic Ab Cytoplasmic Ab titer ______________________________________________________________________________________ Anti neutrophil positive perinuclear pattern Myeloperoxidase Ab 83520 Cytoplasmic Ab ______________________________________________________________________________________ Antinuclear Ab ANA positive at screening dilution Antinuclear Ab titer 86039 ______________________________________________________________________________________ Centromere Ab positive at screening dilution Centromere titer 86256 ______________________________________________________________________________________ Direct Antiglobulin Test positive DAT IgG 86880 (DAT) DAT complement 86880 ______________________________________________________________________________________ Dilute Russell Result above normal range LA Confirm test 85613 Viper Venom ______________________________________________________________________________________ Electrophoresis suspicious band not Immunofixation 86334 Protein, Serum previously identified ______________________________________________________________________________________ Electrophoresis suspicious band not Immunofixation 86335 Protein, Urine previously identified ______________________________________________________________________________________ Fluid cell count any wbc’s present Differential 89051 ______________________________________________________________________________________ Hemagram & See Lab Services Pathologist’s smear review 85060 Differential Directory & written interpretation ______________________________________________________________________________________ Hepatitis A Antibody positive result Hepatitis A -IgM 86709 Antibody confirmation ______________________________________________________________________________________ Hepatitis C Antibody low level reactivity Hepatitis c RIBA 86804 ______________________________________________________________________________________ Lupus work-up Abnormal PTT PTT 50/50 mix 85732 ______________________________________________________________________________________ Lyme Ab Lyme ELISA of Lyme western Blot 86617 >1.10 Mitochondrial Ab positive at screening dilution Mitochondrial Ab titer 86256 ______________________________________________________________________________________ Parietal Ab positive at screening dilution Parietal Ab titer 86256 ______________________________________________________________________________________ Platelet Function Above normal limit COL/ADD cartridge 85576 Analysis 27 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Initial Reflex Reflex Additional Test Criteria Test(s) CPT billed Prenatal Panel Ab screen positive Antibody ID panel 86870 (up to 3x) Antigen typing 86905 Ig subclass 86975 Ab titer 86886 ______________________________________________________________________________________ PTT 50/50 mix PTT done first, if PTT PTT 85730 nd is abnormal and patient is on PTT (2 ) 85730 heparin-heparin is neutralized Heparin neutralization 85525 and a 2nd PTT is done ______________________________________________________________________________________ RPR positive at screening dilution RPR titer 86593 ______________________________________________________________________________________ RPR Titer reactive RPR at any dilution FTA abs 86781 ______________________________________________________________________________________ Sickledex positive result Hg electrophoresis 83020 ______________________________________________________________________________________ Smooth muscle Ab positive at screening dilution Smooth Muscle Ab titer 86256 ______________________________________________________________________________________ Urinalysis, routine when protein 1+ or Urine microscopic 81001 blood positive or leukocyte esterase positive 28 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory ANATOMIC PATHOLOGY AND REFLEX TESTING In Anatomic Pathology, a specimen is sent to the laboratory with the intent that the pathologist will evaluate the specimen thoroughly enough to make a diagnosis. To this end the pathologist uses their medical judgment in ordering and interpreting additional studies on the material which they feel are necessary to fully evaluate the specimen. In this regard the pathologist is acting as a consultant in the care of the patient. The additional studies are charged only when deemed medically necessary by the pathologist. Such cases would include, but is not limited to, ordering special stains, decalcification of the tissue, immunoperoxidase stains, microbiology cultures on fresh tissue, flow cytometry on certain tumors or products of conception, and electron microscopy as indicated. Providers can also request additional studies on Anatomic Pathology cases, usually following discussion of the case with the pathologist. There are some tests which are often useful for prognosis and diagnosis which are not yet considered routine or standard of care. For these tests, reflex testing procedures have been made so that if a specimen/process meets the reflex criteria then the additional testing will be performed. Providers may decline the reflex testing by completing this box on the Surgical Pathology requisition. The department of Anatomical Pathology will automatically perform reflex testing as outlined in the following page. 29 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory ANATOMIC PATHOLOGY SPECIMENS SUBJECT TO REFLEX _____________________________________________________________________________________ Initial Reflex Reflex Additional Specimen criteria Test(s) CPT billed Breast excision All invasive adenoncarcinomas HercepTest® 88360 for carcinoma _____________________________________________________________________________________ Breast excision HercepTest® with FISH 2x 88271 for carcinoma an indeterminate result (2+) 88274 88291 _____________________________________________________________________________________ Breast biopsy 1st incidence of ER/PR receptor testing 2x 88360 DCIS. 2x 88360.26 _____________________________________________________________________________________ Fatty tumor excision >5 cm Cytogenetics 88233 88264 Renal tumor excision enough tumor to sample. 88291 _____________________________________________________________________________________ Bone tumor excision enough tumor to sample Cytogenetics 88239 88264 Soft tissue excision enough tumor to sample 88291 Additional reflex information: HercepTest® (C-erb-B2 immunoperoxidase stain) Reflex Testing on Breast Cancers C-erb-B2 (Her2/neu) analysis by the Herceptest® will also be performed routinely on all invasive breast carcinomas at the time of the definitive excision with the exception of well-differentiated tumors, which are lymph node negative. The HercepTest® is a FDA approved standardized immunohistochemical assay, which measures the HER2 protein overexpression in tumors. The HercepTest is an excellent first line HER2 assay that is scored as 0-3+ with 0 and 1+ considered a negative result for protein overexpression and 3+ considered as positive for protein overexpression. A 2+ result is considered indeterminate and as such we automatically have Fluorescence in situ hybridization (FISH) performed on these cases to measure whether there is Her2 gene amplification in the tumor. The Division of Surgical Pathology will automatically perform the HercepTest® on invasive breast adenocarcinomas which meet certain reflex testing criteria outlined below. Criteria for reflex performance of the HercepTest® on Breast carcinomas: 1. Tumor present in a resection specimen so that the grade of the tumor can be accurately established (this test will not be performed automatically on core biopsies, unless there is no residual tumor in the resection specimen). 2. All invasive adenocarcinomas are included except well-differentiated tumors (total histologic grading score of 3,4, or 5) that are less than 1 cm (pT1a and pT1b). 30 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Estrogen and Progesterone receptor testing on breast biopsies with ductal carcinoma in situ (DCIS) Recent studies have shown a therapeutic benefit in treating patients with DCIS with tamoxifen. Allred et al.1 presented data at two meetings, which have shown that women with estrogen receptor (ER) positive DCIS treated with tamoxifen have significant reductions in the incidence of ipsilateral and contralateral breast cancer. Their subsequent data showed no benefit for tamoxifen therapy in women with ER negative DCIS. Performance of the PR assay provides additional information on the integrity of the ER receptor axis. As a result of this new data, we now perform reflex testing on breast core biopsies with DCIS alone for estrogen and progesterone receptors. Guidelines for the testing include: 1. All DCIS cases will be tested unless the reflex testing is declined by the provider ordering the test or there is insufficient tissue present for testing; 2. The reflex testing will be performed on the first incidence of DCIS (typically the core biopsy); 3. If invasive tumor is also present in the tissue being tested, the report will reflect the ER/PR results of the invasive tumor only unless the DCIS pattern is significantly different from the invasive tumor; 4. ER/PR testing will be repeated on a subsequent biopsy/ excision which contains an invasive tumor when the original biopsy showed only DCIS. 1 Allred DC, et al. Estrogen receptor status as a predicative marker of the effectiveness of tamoxifen in DCIS: Findings from NSABP Protocol B-24. (Abstract 80) Modern Pathol 2003; 16:21A. Reflex cytogenetic testing on adult renal tumors: Although histologic analysis is the mainstay to the diagnosis of adult renal neoplasms, cytogenetic analysis can provide supportive diagnostic information in many cases. For this reason, Fletcher Allen Health Care has initiated sending portions of renal neoplasms for cytogenetic analysis when we receive a fresh resection specimen, which has enough tumor to sample for cytogenetics. Conventional renal cell carcinomas typically have loss of the genetic material in the long arm of chromosome 3 and chromophobe carcinomas are typically characterized by monosomy of multiple chromosomes and hypodiploidy. Papillary renal cell carcinomas, in contrast, often have a better prognosis than conventional renal cell carcinomas and typically have a distinct cytogenetic profile with trisomy of chromosomes 7, 16 and 17 as well as additional genetic abnormalities. The histomorphologic features of these tumors may overlap in certain cases and thus cytogenetic analysis is felt to be useful in many cases. Reflex cytogenetic testing on fatty tumors: Fatty tumors similarly may be difficult at times to classify on morphologic basis alone and cytogenetics on lesions greater than 5 cm can add additional diagnostic information. Solitary lipomas have been shown to have translocations involving 12q13-15 as well as chromosomal rearrangements of 13q or 6p21-33. Atypical lipomatous tumor/well differentiated liposarcomas, on the other hand, commonly show ring chromosomes and long marker chromosomes from 12q13-15. Dedifferentiated liposarcomas may have additional complex aberrations. Finding specific cytogenetic changes can therefore support the histologic findings. 31 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Reflex cytogenetic testing on soft tissue and bone tumors. In addition to the current reflex policy in surgical pathology for submitting Cytogenetics on renal tumors and fatty tumors, soft tissue tumors and bone tumors including certain pediatric tumors will routinely be submitted for Cytogenetics. More data has emerged on the utility of Cytogenetics as an adjunct to traditional diagnostic methods such as histologic examination with H&E stains as well as immunohistochemical stains. Cytogenetics is considered integral to the diagnosis of some soft tissue and bone tumors, especially in cases which pose histologic challenge. Soft tissue and bone tumors with well known chromosomal translocations and gene rearrangements include Ewing sarcoma/PNET, desmoplastic small round cell tumor, extraskeletal myxoid chrondrosarcoma, synovial sarcoma, alveolar rhabdomyosarcoma, low grade fibromyxoid sarcoma and inflammatory myofibroblastic tumor, to name a few. As with all reflex testing, the ordering provider can choose to decline the reflex testing by checking the selection on the surgical pathology requisition. 32 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory CUSTOM PROFILES Custom profiles permit physicians to establish their own profile consisting of a particular group of tests that they order together frequently. Physicians in certain specialties request such groupings for particular clinical situations. The government recognizes the need to permit custom panels; however, the government expects laboratories that construct custom profiles in response to a physician’s request to provide a disclosure notice to physicians who use the custom panel. This disclosure is called a Physician Acknowledgement of Customized Profile. Our Laboratory will work with physician clients to construct custom profiles to meet specific testing needs. At the time of implementation of any custom profile, and annually thereafter, the physician will be requested to sign a Physician Acknowledgment form. Please contact Laboratory Customer Service (847-5121) and ask to speak to an Outreach Specialist if you would like more information about custom profiles. 33 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory BILLING INFORMATION Fletcher Allen Health Care can bill: • • • • • Your patient Medicare Medicaid Most commercial insurance companies Your office* *A volume discount may be available if we bill your office. Contact Customer Service at (802)847-5121, ask for a Laboratory Outreach Specialist to set up your "96" account. Current legislation requires hospital laboratories to bill Medicare and Medicaid directly for clinical laboratory tests performed for physicians and clinics. Fletcher Allen will submit separate bills for pathologist interpretation of certain tests (e.g. Cytology, Cytogenetics, and Surgical Pathology). This is a federal regulation. These tests are noted on the fee schedule with a "Part B" component. All test orders must be accompanied with up to date billing information. The lab requisition billing information section must be completely filled out. QUESTIONS ABOUT LABORATORY BILLS? Call: 96 Account Billing (Client Billing) ...Lab Reimbursement Specialist: (802)847-0234 Long distance toll free calls: (800) 991-2799 or email: LabMarketing@vtmednet.org Patient Billing (Part A & Part B)……..….Patient Financial Services (PFS) Main Office ACC Building, Main Pavilion, Third Floor 111 Colchester Avenue Burlington, VT 05401 Email CustomerService@vtmednet.org PFS Customer Service Line: (802)847-8000 And Long distance toll free calls: (800)639-2719 Telephone Lines Are Open ................. Monday through Friday, 8:30 a.m. – 4:30 p.m. Office Hours......................................... Monday through Friday, 8:00 a.m. – 4:30 p.m. 34 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory OUTPATIENT BLOOD DRAWING SITES Lactose and glucose tolerance tests must be scheduled in advance by calling laboratory Customer Service ((802)847-5121). For all other testing, no appointment is necessary at any of the phlebotomy areas. Patients are seen in the order in which they arrive. Patients with stat testing, timed tests or patients with special needs will be expedited. Please call Laboratory Customer Service for hours and directions. Medical Center Campus Ambulatory Care Center (ACC) Laboratory Services Level 2 (Orange), Main Pavilion 111 Colchester Avenue Burlington, VT 05401 The primary care site – with four collection stations. Fanny Allen Campus Laboratory 790 College Parkway Colchester, VT 05446 This site has two collection stations. Please plan to stop in the patient registration area before proceeding to the Laboratory OFF-HOURS INFORMATION Routine blood drawing is available Monday through Friday and Saturday morning. If a patient needs to have blood drawn immediately, or if the testing required is a timed draw & not during routine hours, you should instruct the patient to come to the Ambulatory Care Center information desk inside the front entrance on Level 3 (street level) for instructions. After going to registration, a phlebotomist will be paged. 35 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory RESULT REPORTING Individual patient reports are printed every night and distributed by courier or mail the following day. For clients that have Laboratory report devices (fax or printer) in their office, reports print at the same time each day according to a schedule set up when the printer was installed. Each patient report includes the patient's name, date of birth, sex, Fletcher Allen medical record number, laboratory location code, clinician and the date the report was printed in the header. With each test the date/time collected and date/time received will print along with the normal ranges for the tests requested. Any test result that is outside the normal range will be flagged with an "H" for above normal results or "L" for results below normal. Critical values are flagged with a "*". Laboratory Report Devices Types of Report Printers DEVICE CARTRIDGE KIT Printer 6000 (AP, CP & General Lab reports) KIT Printer 6100 (AP, CP & General Lab reports) KIT Printer 8100 (AP, CP & General Lab reports) Brother Fax 2820 (AP, CP & General Lab reports) Toner 12LM-69G8256 Toner 13T0101 or 13T0301 Toner 12LM-4K00198 or 12LM-4K00199 Toner TN-350, Drum DR-350 Cytopathology and Anatomic Pathology Report Print Schedule Reports print in the very early hours of the morning either in your office or at the laboratory and we will forward them to your office. Clinical Pathology Report Print Schedule We provide a written report to the ordering physician and any additional copy to physicians indicated on the order. Laboratory reports will print on a prearranged schedule. Some supplementary reports will be mailed or sent by courier when completed. You will not be called unless a result is a critical value or you have requested that the result be called or faxed. 36 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Report Print Options There are 4 options for printing. Definitions Test: single assay i.e. glucose Battery: A group of assay’s i.e. electrolytes Accession: Test(s) and /or battery(s) that are ordered at the same time. This will vary sometimes with specimen type. Reports are printed by accession. You will get a final report with all test(s) ordered under that accession on a single report. Completed This option allows tests and Accessions batteries to qualify for a report only when an entire accession is Option #1 completed. All accessions that are complete at the scheduled print time will print for any location defined with option #1. Pending Accession Option #2 This option allows tests and batteries to qualify for a printed report when there is any activity on an accession, the entire accession prints each time. Any pending tests or batteries will print as “Pending”. When all tests are complete a report with all the tests ordered for that accession will print completed. Summary - If you order a test that takes longer to report with tests that are usually completed on the same day as received you will not receive a report until the test that takes longer is finalized. Summary - If you order a test that takes longer to complete with tests that are usually completed on the same day you will receive a report at the scheduled print time with the test result that was completed on the same day resulted and the incomplete test reported as “pending”. NOTE: Gram stains that are ordered with a culture will not print until the culture has been resulted. NOTE: Gram stains that are ordered with a culture will print with the next scheduled print after they are completed and the culture will print as pending. 37 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Reports are printed by individual test You may not receive a final report with all tests resulted on a single report. Completed Test & Batteries Option #3 This option qualifies tests and batteries for a printed report when the battery or test is completed. Any battery or test that is complete at the scheduled print time will print. Test and batteries will print only once and you will not see any pending tests or batteries. You will have a printed report for each test and battery but you may not receive a report with the entire accession completed on the same report. Pending Test & Batteries Option #4 This option qualifies tests and batteries for a printed report when there is any activity. Only those tests or batteries that have activity will print. Once a test or battery has printed it will not print again. You will have a printed report for each test and battery but you may not receive a report with the entire order completed on the same report. Summary - If you order a test that takes longer to report with tests that are usually completed on the same day you will receive a report at the scheduled print time with the test result that was completed on the same day resulted, and the test that takes longer as “pending”. Summary - If you order a test that takes longer to result with tests that are usually completed on the same day, you will receive a report at the scheduled print time for tests that are completed, and when a test that takes longer to result is complete you will receive another report for those tests. Previously reported results will not reprint. If there is any new activity on this order a new report will print. New activity could be a pending result, a completed result a corrected result or it could be an updated date/time or something else. NOTE: Gram stains that are ordered with a culture will print with the next scheduled print after they are completed and the culture will print as pending. NOTE: Gram stains that are ordered with a culture will not print until the culture has been resulted. 38 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Client Report Fax For clients that have a report fax in their office please review the following information. Paper Use plain paper only. To avoid paper jams DO NOT USE pre-punched paper or recycled paper or paper with rough or heavily textured surfaces, coated, preprinted, synthetic or thermal paper. The laboratory will supply paper for these report devices. Moving a Device Please contact Fletcher Allen Health Care Lab Customer Service before moving your printer. Index Reports • • • • • Index reports print at the end of each report batch and should be saved for two months. For Pathology Reports, this is a single page detailing the location, ordering physicians, specimen number, report status and patient name in the report batch. For Clinical General Lab Reports, two index reports print, Index of New Activity Event Report Summary By Patient Name and Index of New Activity Event Report Summary By Hospital Number. Always wait until the end of the print to remove the Index Reports from the printer. If the Index Report does not print, call Lab Customer Service at (802)847-5121. Format Errors • Reports should print with a header and footer. • The footer will print approximately 1.5 inches from the bottom of the report. • If the footer prints any further from the bottom of the page, do not use results on any of the reports that have printed in this batch. Call Lab Customer Service at (802)847-5121 to report the problem. Unexpected End of Transmission Error • When did the error occur? This error is normal and expected for KIT 8100, if it occurs after index prints. • For all other printer/fax models, if error occurred before index reports printed – there was an interruption in the transmission. DO NOT use any of the reports that have printed in this batch. • Contact Lab Customer Service at (802)847-5121 to request retransmission of report batch. No Dial Tone Detected: • Check the phone line. Make sure it is securely connected to the wall jack and the printer LINE IN (NOT the FAX OUT) jack. If you reinsert the cable into the printer/fax, turn it off and then back on prior to receiving data. • Plug a standard, single-line phone into the wall jack and listen for a dial tone. If you don't hear a dial tone, the line will need to be tested. Contact Lab Customer Service at (802)847-5121 No Reports Printed Please verify the following: • Printer/fax has power. • Fax box, if applicable has power. (Is the light on?) • Paper is loaded. • No error messages are displayed (on-line/ready status.) **DO NOT turn off the printer unless you are instructed to do so.** 39 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Lab Order Priority Designations To efficiently manage patient care, the following order status designations are offered. DESIGNATION AVAILABILITY TESTING REPORTING Immediately Upon STAT Limited Phone Results Receipt Call Results All Tests Routine Phone Results Routine or ASAP All Tests Routine Phone critical results only STAT Stat testing is defined as laboratory testing required in order to immediately treat a patient. The inappropriate use of requesting Stat testing affects the care of critically ill patients by delaying the turnaround time for Stat testing required to immediately treat them. All tests on the Stat list are completed on the same day the samples are received. Some laboratory testing cannot be offered Stat due to the amount of time it takes to process the sample. Examples are: microbiology cultures, cytogenetics testing, and tests sent out to reference laboratories. STAT requests are given the highest priority at all stages of specimen handling, including collection, processing, testing and reporting. Most STAT tests are reported within sixty minutes of being received in the lab. If you need a test done STAT write STAT on the lab requisition next to the test you want STAT, along with a phone number or beeper number where you can be reached. Also call Customer Service at 847-5121 to let us know a STAT is coming. The STAT result will be called as soon as testing is complete. We perform a limited number of tests STAT. Please see STAT list in this section. Tests not on the STAT list must be approved by a pathologist before testing will be performed. Call/Fax Result Requests for tests to be called or faxed will be treated as routine. Results will be called as soon as they are available. If results are complete after your office hours, we will call the provider on call. Any critical results (see list in this section) will be called immediately. For anatomic and cytopathology, we call all new cancer diagnosis, unexpected malignancy or malignancy in an unusual location, a significant change between a rapid and a final diagnosis, identification of a significant infectious organism, and any case that a pathologists flags. If you need results called or faxed to your office, please fill in the appropriate box on the requisition and supply the phone/fax number. These results will be called or faxed to your office as soon as possible after the completion of the testing. 40 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 Routine Critical Values FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Individual patient reports are printed every night and distributed by printer, courier or mail the following day. Most testing is done within 8 hours of being received in the laboratory. Cultures and some esoteric tests will take longer than 24-hours. Any critical results (see list in this section) will be called immediately. Tests ordered ASAP will be tested as routine. See Lab Services Directory, Section III, Sample Requirements for information on analytical time for specific testing. Critical values will be called to the ordering physician as soon as the results are available. (See the Critical Values list located in this section). A laboratory representative will call and clearly state that the value is critical and requires immediate attention. The laboratory representative will ask the individual who received the result to repeat back the result for confirmation. The call will be recorded in the laboratory information system. The following information must be documented: • Time and date the call was made; • Full name of the individual who received the results; • Name of the individual in the laboratory who communicated the results. Repeat Testing Specimens are generally held for 5 days after test completion. If laboratory results do not match clinical conditions, please call Customer Service 847-5121 to arrange repeat testing. 41 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory COURIER The laboratory operates several courier routes throughout the state of Vermont. For clients outside of our courier area we have various mechanisms in place to handle your specimens. Please contact Laboratory Customer Service, (802) 847-5121, to assist you with this process. STAT Courier Pickups Pickups provided outside the courier’s regular schedule and requiring immediate processing are considered STAT. We are able to provide this service to clients within Chittenden County. Arrangements can be made by calling Customer Service at 8475121. Fletcher Allen Health Care will NOT pay courier pick-up fees for samples brought to the lab by a courier that has not been arranged for by the laboratory. LABORATORY SUPPLIES Collection supplies necessary to forward specimens to our laboratory such as requisitions, transport media, sterile containers, specimen preservatives, needles and vacuum tubes are furnished at no extra charge. Please use the supply order form to order supplies. 42 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory STAT LIST STAT Tests not requiring pathologists approval Blood Bank Blood Group (ABO and Rh Type) Cord Blood Routine Crossmatch of units Transfusion Reaction Workup Type and screen (with or without crossmatch) Chemistry Acetaminophen Acetone Albumin Alkaline Phosphatase Amikacin Ammonia Amylase ALT AST B-type Natiuretic Peptide (BNP) Bilirubin BNP Calcium Calcium, ionized Carbamazepine (Tegretol) Carbon Dioxide Carboxy Hemoglobin Chloride Cholesterol CK CKMB Cortisol (M3, M4, and the ER) Creatinine CRP Creatinine Clearance Digoxin Drug Screen-6 Drug Screen-7 Drug Screen-Agitated Drug Screen-Sedated Electrolytes (Na, K, Cl) Estradiol – In vitro Fertilization Samples (UIVF) Ethanol Ethylene Glycol Fetal Fibronectin Fetal Lung Maturity GGT Gases - PH, PO2, PCO2 43 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory STAT Tests not requiring pathologists approval Gentamicin Glucose HCG Hemoglobin, Plasma HIV-Rapid (7 a.m. to 10 p.m. daily) Iron Iron Binding Capacity Isopropanol - See Volatile Screen Lactic Acid LDH Lipase Lithium Magnesium Methanol - See Volatile Screen Methemoglobin Methotrexate Monospot Osmolality Oxygen Saturation Phenobarbital Phenytoin (Dilantin) Phosphorus Potassium Pregnancy Test, Urine Progesterone – In Vitro Fertilization Samples (UIVF) Protein, Total Salicylate Sodium Theophylline Tobramycin Tricyclic Screen Triglycerides Troponin TSH – ED and Nuclear Medicine Only Urea Nitrogen Uric Acid Urinalysis Urine pH Valproate Vancomycin Volatiles Screen (includes Ethanol, Methanol, and Isopropanol) 44 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Hematology and Coagulation Body Fluid Cell Count Crystals, Joint CSF Cell Count D-Dimer Fibrinogen, plasma Hemagram (CBC) Hemagram and Differential (or any part-WBC HGB, HCT, Platelet) Heparin Level (unfrationated, low molecular weight, fondaparinux) Kleihauer-Betke (approval needed when ordered on evenings, nights and weekend shifts) Partial Thromboplastin Time (PTT) PFA-100 (Platelet Function Analysis) Prothrombin Time Sedimentation Rate Histology Pneumocystis Stain (Pathologist on call must approve before Histology is called in.) Microbiology AFB Smear Fungal Smears (Day only) Gram Smears (on Evening/Night preparation & staining only) Inoculation of bacterial cultures Malarial Smears Parasite Exam, Blood Wet Preps 45 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory CRITICAL VALUES LIST The following is a list of laboratory results that are considered critical values. These results will be called immediately to the ordering provider. Hematology Test Differential Cell Count Hematocrit Hemoglobin Leukocyte Count Critical Value Blast cells greater than 20% Less than 21% Less than 7.0g/dL Less than 1000/µl OR Absolute Neutrophil count <500/µl OR Greater than 50,000/µl Less than 2,000/µl INR greater than 3.8 Over 100 seconds less than 90 mg/dL All Results Greater than 1.5mg/L Greater than 2.0 IU/mL Greater than 1.0 IU/mL Platelet Count Prothrombin Time Partial Thromboplastin Time Fibrinogen Heparin Platelet Ab PF4 ELISA Heparin Level, Fondaparinux Heparin Level, Low Molecular weight Heparin Level, Unfractionated Chemistry Dialysis: The only critical values that must be confirmed and called on samples clearly labeled PreDialysis or PostDialysis are listed below. Use standard call values otherwise: Test Calcium Potassium <6.5 <3. 0 Standard Critical Values Test Acetaminophen Acetone Amikacin Critical Value >14.0 mg/dL >7.0 Meq/L Critical Value >100 ug/mL Any positive result Peak: >36 ug/mL Trough: >6 ug/mL >15 mg/dL <6.5 or >11.5 mg/dL <6.5 or >12.0mg/dL >15 ug/mL >15% >15 mg/dL >5.0 mg/dL with no previous OR 3 times higher than the previous OR >4.0 mg/dL and is more than 2.5 mg/dL higher than previous value >2.0 ng/dL Positive Bilirubin (Children and Adults) Calcium Calcium, (patients 0-28 days old) Carbamazepine (Tegretol) Carboxyhgb Creatinine Delta Creatinine Digoxin Fetal Fibronectin 46 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Test Critical Value Gentamicin Peak: Trough: <50 or <40 or Glucose Glucose (Neonate <1 day) HCG-on Accutane Ionized Calcium Ketones, Urine Lead Lead Lithium Magnesium Methotrexate PH (blood gas) Phenobarbital Phenytoin (Dilantin) Potassium Salicylate Sodium Theophylline Tobramycin <0.8 or 0-18 years Adult <1.0 or <7.00 or <3.0 or <125 or Peak: Trough: Tricyclic screen Valproate Vancomycin Peak: Trough: >12 ug/mL >1.5 ug/mL >500 mg/dL >180 mg/dL >4 mIU/mL >1.60 mmol/L Large >20 ug/dL >40 ug/dL >1.5 mEq/L >4.8 mEq/L >1000 uM/L >7.60 >45 ug/mL >22 ug/mL >6.0. mEq/L >30 mg/dL >155 mEq/L >20 ug/mL >12 ug/mL >1.5 ug/mL >500 ng/mL >150 ug/mL >40 ug/mL >20 ug/mL Microbiology Test Blood cultures CSF specimens Acid-fast bacilli Plasmodium species Group A streptococci - from other than throat Critical Value positive result positive result positive result positive result positive result 47 Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information August 13, 2009 FLETCHER ALLEN HEALTH CARE 2009 Laboratory Services Directory Appendix Advanced Beneficiary Notice (ABN) Informed Consent Vermont Informed Consent New York State Telephone/Fax/Standing Order Request Form Special Send-Out Laboratory Mailing Request Form Laboratory Supply Order Form Lead Demographic Form Customer Service 847-5121 or 1-800-991-2799 http://www.fahc.org/pathology General Information February 16, 2009 FAHC MRN: NAME: DOB: VERMONT STATE INFORMED CONSENT FOR GENETIC TESTING Addressograph Genetic Testing has been recommended for me (or my child). I understand that the genetic testing requires analysis of the chromosomes, Deoxyribonucleic acid (DNA), Ribonucleic acid (RNA), or protein obtained from a sample of blood, skin, cheek brushings or other body tissues. I understand that no other tests than those authorized will be performed and that my biological sample will not be saved without my authorization. I understand the specific test that I (or my child) is having and its accuracy. I understand that the results of this test may be inconclusive or uninformative (not tell me anything). I understand that incorrect information about family relationships may affect the test result. I understand that this test may reveal private information such as non-paternity (someone’s father not being who they think they are) or adoption. I understand that such information, if obtained through this test, will NOT be revealed to me, my child, or to anyone else, under any circumstances. I understand that I am responsible for the costs of genetic testing. If I choose to have my (or my child’s) insurance company pay for the testing, it is my responsibility to contact the company to determine that they cover such testing. I know that if the insurance company pays for the testing they may have a right to learn the test results. I can choose not to have the insurance company pay for the testing, in which case I will pay for the test myself. I understand that in some cases payment is required before the genetic testing is performed. Whether it is the insurance company or me that pays for the testing, the results may become part of my (or my child’s) permanent medical record. Having this information in the medical record may make it more difficult for me (or my child) to get health, disability, long-term care or life insurance. I have also considered the possible financial impact of the test result. I understand that Vermont law gives me certain protections from misuse of genetic information, including the right to sue if such misuse occurs. I have explained to ________________________________ the possible risks, benefits and limitations of the genetic test _________________________________________________________ (name of the test). Provider Signature: ___________________________________________Date:____________________ Institution: _______________________________________Phone number: _______________________ I have read (or had read to me) the above information and received a copy of this page. All of my questions and concerns about genetic testing have been addressed. I know that I can contact the person above if I have additional questions. Patient ______________________________________________ Date: ________________ If patient is a minor: Parent or guardian: _______________________________________ Date: ________________ Witness: _______________________________________________ Form# 036431P Retain in Patient’s Chart 03/2006 Consent Section Date: ________________ Page 1 of 1 FAHC MRN: NAME: DOB: NEW YORK STATE INFORMED CONSENT FOR GENETIC TESTING Addressograph The purpose of this form is to allow you to make an informed decision in regard to whether or not you wish to undergo genetic testing. You may wish to obtain professional genetic counseling before you sign this form. If you do not sign this form, no genetic tests will be performed on your behalf. I understand that the purpose of this test, and its potential benefit, is to obtain the possible diagnosis of an inherited metabolic disease. It may also determine which of my family members may be carriers of the disease. For prenatal diagnosis, it may determine the genetic status of the fetus. I understand that a positive test result is an indication that I (or my child) may be predisposed to or have the specific disease or condition tested for. If I (or my child) receive a positive test result, I understand that I (or my child) may benefit from further independent testing, consultation from my physician, or pursuing genetic counseling. I understand that genetic testing has been recommended for me (or my child). I understand that the genetic testing requires analysis of the chromosomes, Deoxyribonucleic acid (DNA), Ribonucleic acid (RNA), or protein obtained from a sample of blood, skin, cheek brushings or other body tissues. I understand that no other tests than those authorized will be performed and that my biological sample will not be saved without my authorization. I understand that the following diseases or conditions will be tested for: __________________________________ _______________________________________ __________________________________ _______________________________________ I understand that a positive test result for _________________________ disease or condition serves as a ___________ percentage predictor of such disease. Or, in the alternative, as explained to me, no level of certainty has been established for the disease or condition which I am being tested for. I understand the specific test that I (or my child) is having and its accuracy. I understand that the results of this test may be inconclusive or uninformative (not tell me anything). I understand that incorrect information about family relationships may affect the test result. I understand that this test may reveal private information such as non-paternity (someone’s father not being who they think they are) or adoption. I understand that such information, if obtained through this test, will NOT be revealed to me, my child, or to anyone else, under any circumstances. I understand that I am responsible for the costs of genetic testing. If I choose to have my (or my child’s) insurance company pay for the testing, it is my responsibility to contact the company to determine that they cover such testing. I understand that if the insurance company pays for the testing they may have a right to learn the test results. I understand that I can choose not to have the insurance company pay for the testing, in which case I will pay for the test myself. I understand that in some cases payment is required before the genetic testing is performed. Form# 036432P 03/2006 Retain in Patient’s Chart Consent Section Page 1 of 2 I understand that whether it is the insurance company or me that pays for the testing, the results may become part of my (or my child’s) permanent medical record. I understand that having this information in the medical record may make it more difficult for me (or my child) to get health, disability, long-term care or life insurance. I have also considered the possible financial impact of the test result. I understand that my genetic sample will be destroyed at the end of the testing process or not more than sixty days after my sample was taken, unless I authorize a longer period of retention. I authorize the results of this test to be disclosed to the following persons/organizations: ________________________________ _________________________________________ ________________________________ _________________________________________ I have explained to _________________________________________________ the possible risks, benefits and limitations of the genetic test ___________________________________ (name of the test). Provider Signature: _____________________________________________Date: __________________ Institution: _____________________________________Phone number: _______________________ I have read (or had read to me) the above information and received a copy of this form. All of my questions and concerns about genetic testing have been addressed. I understand that I can contact the person listed above if I have additional questions. Patient ______________________________________________ Date: ________________ If patient is a minor: Parent or guardian: _______________________________________ Date: ________________ Witness: _______________________________________________ Date: ________________ I hereby authorize my genetic sample to be retained by the testing organization for a length of time as they see fit, in order that they may use my sample for anonymous research. I understand that this is entirely optional and that my refusal to allow my sample to be used for anonymous research will in no way affect my ability to have my genetic test performed. By signing below, I understand that my sample may be held longer than the sixty day period stated above. Patient ______________________________________________ Date: ________________ If patient is a minor: Parent or guardian: _______________________________________ Date: ________________ Witness: _______________________________________________ Date: ________________ Form# 036432P 03/2006 Retain in Patient’s Chart Consent Section Page 2 of 2 Fletcher Allen Health Care Department of Pathology and Laboratory Medicine 111 Colchester Ave., Burlington, Vermont 05401 Phone: 802-847-5121 or 800-991-2799 TELEPHONE/FAXED LABORATORY ORDER FORM This material is intended for the use of the individual or entity to which it is addressed and may contain information that is privileged, confidential and exempt from disclosure by applicable law. If the reader of this message is not the intended recipient, you are hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. If you received this communication in error, please notify the sender immediately by telephone (collect) and return the original message to the sender listed above. FAX To: Physician fax# __________________________Physician phone _________________________ Outpatient Laboratory Request for Verbal or #Standing Orders Attention _______________________________________________________________________ This form is to be used as follows: 1. For providers who wish to fax in either a one-time or a standing order to the laboratory or 2. By the laboratory for documenting a one time or a standing order received by telephone. If you are faxing in an order, please complete all the information and print legibly. If this form has been faxed to you, please review the telephone order below for completeness and accuracy and confirm this review by providing an authorized signature* below. Fax this form to us at 802-847-5905 or mail it to us at the above address, attention Customer Service. Please return this form to us as promptly as possible. Thank you. ➨Authorized Signature: _________________________________________________________ *An authorized signature is the ordering physician or an authorized person on the physician’s staff. One time Order: Date to be drawn ___________ Standing Order: Frequency ________________________ Duration __________________________ Date Order Requested ____/____/____ Who called? ____________________ Loc Code _________________ Patient Full Name__________________________________________ Date of Birth_____________________ FAHC MRN# or SS#_______________________ Ordering Provider_________________________________ Copy to another physician? Y/N Name_____________________________ Loc Code___________________ Testing Requested _______________________________ ICD-9 Diagnosis Code_______________________ _______________________________ ________________________ _______________________________ ________________________ Order is documented in chart? Y/N Is this a Medicare Patient? Y/N If Medicare: ABN not required_____ Diagnosis not covered, ABN attached_____ Internal Use Only Telephone Order Statement: All Telephone Orders must be followed with written documentation of the Telephone Order within 30 days of the request to comply with federal regulations. The Laboratory has faxed you this form with the telephone order we received and ask that you review the order for completeness and accuracy. We also remind you that the order should be documented in the patient’s chart. Person receiving order _______________ Form # 029402 Database Date/Initials____________ Date faxed _______________ SPECIAL SEND-OUT LABORATORY TEST REQUEST FORM • This form MUST be completed and submitted to Specimen Receiving when the FAHC laboratory is asked to ship any type of specimen to a laboratory that we do not routinely send to (Labs we routinely send-to include: Mayo Medical Laboratory and VT State Lab). • Fax form to 847-2358 and call 847-4763 for confirmation from Specimen receiving Supervisor. • This form MUST accompany a completed laboratory requisition from the performing lab (not an FAHC laboratory requisition). PATIENT INFORMATION Date to be drawn:___________________________ Where patient will be drawn:______________________________________ Patient Full Name:_______________________________________________DOB:_______________ MRN:_________________________ Diagnosis Code(s):__________________________________________________________________________________________ □ Bill Provider: Please provide account number (9____--___________ ) or call 847-5121 to speak to a Marketing Rep. □ Bill Patient or Patient Insurance (Please include insurance information): □ Performing lab listed to bill patient (Include copy of patients insurance card, back and front). Responsible Party Name: _________________________________________________Phone Number: _____________________ Address (Street, Town, State, Zip Code): __________________________________________________________________________________________________________ Medicare No.______________Medicaid No. ______________Managed Care Medicaid No:_________________State:_________ Insurance Name: _____________________________Cert. No. ________________________Group _________________________ Subscriber Name:_______________________________________________DOB______________Relationship________________ Employer__________________________________________________________________________________________________________ YOUR PRACTICE INFORMATION Person Filling Out Form:______________________________________Telephone Number:_________________________ Practice Name:___________________________________________________________________________________________ Address:__________________________________________________________________________________________ Ordering Provider: ___________________________________________Additional Copy To:_______________________________ Physician Signature:_________________________________________________________________________________________ PERFORMING LABORATORY & TESTING INFORMATION You must send Specimen Receiving a completed laboratory requisition from the performing laboratory Specimen Type: ____________________Volume Required:_________________Shipping Temperature:_____________________ Test Name: _____________________________________________________________Test CPT: _____________Test Price: ___________ Performing Lab:_________________________________________________________ CLIA License No:____________________ Lab Address (Street, Town, State, Zip ____________________________________________________________________________________________________________ Lab Phone:______________________________CLIA REQUIRES THAT A COPY OF RESULTS BE SENT TO FAHC LABORATORY In the event that your insurance does not cover these services you will be responsible for the charges. Print name:_____________________________________Signature:____________________________________________________Date:_________________________ Date: _____/_____/_____ Account. Name: __________________________________________________________________ FLETCHER ALLEN HEALTH CARE LABORATORY SUPPLY ORDER FORM Phone Orders: 847-5121 or 1-800-991-2799 Fax Orders: 802-847-5905 Your Name: ______________________________________ Location Code:___________________Phone #:_____________ Items supplied are intended to be used solely for specimens sent to FAHC laboratory. The number of items provided will be monitored to ensure they correlate with the number of tests sent to the lab for processing. Where quantities are listed, we assume you are ordering that number of the quantity listed. For instance, if _3_ Serum separator (SST), 8 ml (box of 50) are ordered we will send you 3 boxes or 150 tubes. Please do not order more items than you will use in 30 days. Items transported and stored at room temperature unless otherwise stated. ®Items transported and stored at 2-8˚c, F items transported 0˚c. TUBES _____ Serum separator(SST), 8 ml (Tray of 50)(031972) _____ Lavender, 4 ml (box of 50) (031974) _____ Lt. Blue, 3.5 ml (box of 50) (031975) _____ Green, 6 ml, (box of 50) (031977) _____ Grey, 4 ml (box of 50) (031978) _____ Yellow, 6 ml (box of 100) (031980) _____ Red, Plain (Serum), 10 ml (box of 100) (031973) PEDI TUBES (Box of 50 or Specify Quantity) _____ Serum separator, Pedi, 4 ml (031982) _____ Lt. Blue, Pedi, 2.0 ml (031981) _____ Green, Pedi, 3 ml (031979) _____ Grey, Pedi, 2 ml (031976) MICROTAINER TUBES (Bag of 50) _____ Gold (serum microtainer) _____ Lavender _____ Green NEEDLES (Box of 100) _____ 21 GA-1 ¼ in. _____ 22 GA-1 ¼ in. (031983) (031984) (031985) (031986) (031988) SPECIMEN COLLECTION & TRANSPORT _____ Special Jumbo Bag (pkg. of 100) (031989) _____ Special Yellow Frozen Bag Sm(Pkg of 50) (035194) _____ Special Pink Refrig Bag Sm (Pkg of 50) (035195) _____ Special White RT Bag Sm (Pkg of 50) (035196) _____ Transport bag (pkg. of 100) (031990) _____ Needle Holder Puncture Guard (BG of 250) (031993) _____ Tourniquet (1 roll) (031997) _____ Coag transfer tube (2 ml, 25 w/caps) (035182) _____ Pour off Tube (pkg of 100) (031994) _____ Transfer Pipet (box of 500) (031995) _____ Container Sterile 100 ml (pkg of 75) (031996) _____ Towelette (031998) _____ Container w/lid, 250 ml (031999) _____ 24 hr. Urine Container Jug #_____ (032000) _____ 24 Hr. Stool Culture Container (032002) _____ Mailing Container Kit, 3 Tube (59182) _____ Mailing Container Kit, 8 Tube (035183) RETURNS: If you return any laboratory supplies please tag the item with a copy of this sheet or add a note explaining where they are being returned from and why so that we can update your location compliance log. Thank you CYTOLOGY/PAP SMEAR SUPPLIES Conventional Pap Supplies _____ Kit(trays of 36 Slides, brushes, scrapers, Sprayfix) (032003) Thin Prep Pap Supplies _____ Vial ( box of 25) (032004) _____ Broom (box of 25) (032005) _____ Brush (box of 25) (034397) _____ Spatula (box of 25) (034399) _____ Brush + Spatula ( box of 25 each) Non-Gyn/Fine Needle Aspiration (032006) _____ CytoLyt Tubes (20 per tray) (034401) SURG PATH/HISTOLOGY _____Formalin, 20ml vial/10ml formalin _____Formalin, 60ml vial/30ml formalin _____Formalin, 120 mL vial/60ml formalin _____Hollandes Filled Cont.,40 ml 24/pk _____Biopsy Filter Paper Circle _____Michel’s Fixative (032026) (032027) (032029) (032028) (032030) (032031) MICROBIOLOGY _____ Blood Culture set, Adult (032033) _____ Blood Culture Set Pedi (032034) _____ Blood Culture Tube, Fungal(Isolator) (59185) _____ Blood Culture Tube, Fungal (Pedi) (59186) _____ Blood Culture Prep Kit II (032149) _____ Blood Culture Chloraprep One-Step (59183) _____ Bone Marrow Tube (SPS) (58852) _____ Anaerobic Transport Vial (032036) ® _____ VCT Transport Media (032037) _____ Genprobe, Unisex (box of 50) (032039) _____ Genprobe, Urine (box of 50) (032038) _____ Ova & Parasite fixative (case of 100) (032040) _____ Stool Culture Vial (box of 20) (032041) _____ Swab (each) (Copan) (59184) F _____ Mycoplasma Transport Media (032042) ®_____ Regan-Lowe (032043) ®_____ Potato Flakes (Mycosel) (032044) ®_____ Jembec Plates (032045) _____ Autoclave Check (032046) CYTOGENETICS ®_____ Bone Marrow Tube (RPMI) (032047) _____ Hanks Solution, Tissue (032048) _____ Sodium HeparinTube,Blood 4ml (green top) (032049) _____ Sodium Heparin Tube, Blood 6ml (green top) (032050) REQUISITIONS/FORMS/OFFICE _____ Outpt Lab Requisition (032007) _____ Genetic & Prenatal Req. (034626) _____ Cytogenetics/Flow Cytometry/ Bone Marrow Exam Req. (032014) _____ Surg Path Non GYN Req. (032013) _____ Lead Demographic Form (25-bound) (Print Shop) (58914) _____ Vet Requisition (032008) _____ Supply Order Form (max 25) (032009) _____ Call Report Form Pad (032016) _____ Advance Beneficiary Notice(ABN) (Max 25) (032022) _____ Telephone/Fax Lab Order Form (032021) PHLEBOTOMY DRAW SITE CARD _____ ACC Cards (50 cards) (032025) _____ Fanny Allen Cards (50 Cards) (56472) _____Acc Card Holder (58853) _____ Fanny Allen Card Holder (58854) PRINTER/FAX LAB REPORT _____ Paper (max 2 reams) (032012) _____Cartridge: Devise Model#______________ Brother Fax 2128 (58856) Kit 6000 (032018) Kit 6100 (032019) Kit 8100 (032020) _____Drum Kit Brother Fax 2128, Every 5th cartridge (58855) _____ Addressograph Cartridge Large (034445) _____ Addressograph Cartridge Small (034446) _____ Labels, Addressograph (032024) _____ Labels, Lab printer (034311) _____ Labels, STAT/Red Hot (034573) FLOW CYTOMETRY/ TISSUE TYPING ®_____ Special Heparin (032051) ®_____ RPMI (For Lymph Nodes) (042119) MISCELLANEOUS SUPPLIES _____ ACD Tube, Sol A (58757) ®_____ Catecholamine Tube (032053) _____ Centrifuge Rubber Cushions (58857) Slide Holders _____ Plastic _____ Cardboard (58913) (032052) Glucose Tolerance Beverage _____ Flavored 75 gr (032055) _____ Flavored 100 gr (032056) _____ Orange 75 gr (032057) _____ Orange 100 gr (032058) LAB SUPPORT USE □ Priority-Scheduled □ Priority-on call □ GMM- Scheduled □ GMM-on call □ U.S. Mail □ ACC □ FAH □ UHC Date Tech Code Order Received: ________________ Order Filled:____________________ #015720B (Rev. 4/24/09) Client LEAD DEMOGRAPHIC FORM Please submit this form when ordering Lead Testing. This form must accompany a laboratory test requisition. PLEASE PRINT CLEARLY Patient Full Name: Street /PO Box City State Guardian Zip Code Full Name: Home Phone: Sample Venous Capillary Check one Date of Collection Race: White (Non-Hispanic) Black (Non-Hispanic) Hispanic Asian/Pacific Islander American Indian/Alaskan Native Other Unknown Check one Insurance: Ordering Provider: Submit to: Private Insurer Medicaid No insurance Unknown Full Name: Practice Name: Street /PO Box City Zip Code Fletcher Allen Health Care Pathology & Laboratory Medicine EP1-100 111 Colchester Avenue Burlington VT 05401 Phone: 847-5121 or 1-800-991-2799 Fax 1-802-847-6079 Form #036447P (Revised 09/01/2006) …Office MCHV/Requisitions/Lead Demographic Form








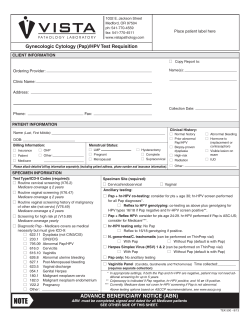



© Copyright 2025