
1 Provider Manual March 2013
Provider Manual
March 2013
Leadership, Partnership, Excellence
1
Table of Contents
Introduction and Overview .........................................................................................................8
Message from the Area Director ..............................................................................................8
Welcome to CoastalCare .........................................................................................................9
Who we are: ..........................................................................................................................10
Description of Expectations/Collaboration Goals ...............................................................10
Mission Statement.................................................................................................................10
Vision Statement ...................................................................................................................11
Value Statement ....................................................................................................................11
The Medicaid Waiver: What is the NC DHHS Health Plan? .....................................................11
About the NC MH/DD/SAS Health Plan ..............................................................................12
About the NC Innovations Waiver ......................................................................................13
CoastalCare Governance and Administration ............................................................................13
Office of the CEO ...................................................................................................................14
Network Management Department.......................................................................................15
Utilization Management ........................................................................................................16
CM Functions .....................................................................................................................16
UR Functions ......................................................................................................................16
Routine Utilization Review .................................................................................................16
Focused Reviews ................................................................................................................17
Appeal Reviews ..................................................................................................................18
Quality Management .............................................................................................................18
Quality Assurance & Quality Improvement ............................................................................19
Corporate Compliance ...........................................................................................................19
Finance and Reimbursement .................................................................................................20
Care Coordination .................................................................................................................20
Customer Services/Call Center ...............................................................................................20
Medical Director ....................................................................................................................21
Operational Committees .......................................................................................................21
Provider Network ......................................................................................................................22
2
Description of Network..........................................................................................................22
Types of Providers ..............................................................................................................22
Quality of Care .......................................................................................................................25
Cultural Competency of the Network: ...................................................................................28
Definition of Cultural Competence ........................................................................................28
What changes should your program make to enhance cultural competence? ....................30
Cultural Competence Goal: ....................................................................................................31
Provider Communication .......................................................................................................31
Provider Council ....................................................................................................................33
Provider Enrollment and Credentialing ..................................................................................33
Performance Monitoring .......................................................................................................37
Gold Star Rating and Monitoring Process ...........................................................................37
Focused Monitoring ...........................................................................................................41
Quantitative Record Review ...............................................................................................41
Mystery Shopping ..............................................................................................................42
Changes in Qualification Status ..............................................................................................42
Applying for Additional Services .........................................................................................43
Implementation Review .....................................................................................................43
Network Development Plan ...................................................................................................44
Access & Availability Monitoring ............................................................................................45
Need/Gap Analysis ................................................................................................................46
CoastalCare Network Development Action Plan ....................................................................47
Contracts ...............................................................................................................................47
Minimum Criteria and Conditions to Participate in the Network ............................................50
Medicaid ............................................................................................................................50
State Funded Network .......................................................................................................50
Training .................................................................................................................................51
Technical Assistance ..............................................................................................................52
Consumer Rights and Empowerment ........................................................................................55
3
Rights of Consumers ..............................................................................................................55
Informed Consent ..................................................................................................................57
Psychiatric Advance Directives (PAD) .....................................................................................57
Confidentiality .......................................................................................................................59
Second Opinion .....................................................................................................................60
Reductions, Denials, Suspensions or Termination of Medicaid Services .................................61
Denial ................................................................................................................................61
Reductions, Suspension, or Termination ............................................................................61
Due Process for Medicaid Decisions ......................................................................................62
Appeal Level I .....................................................................................................................62
Steps to File an Appeal Request .............................................................................................62
Expedited Appeal Review Process ......................................................................................63
Mediation - Level II ............................................................................................................63
Appeal/Hearing - Level III ...................................................................................................64
Final Agency Decision - Level IV ..........................................................................................64
Non-Medicaid Service Appeal Process ...................................................................................65
Non-Medicaid Appeal Request to DHHS .............................................................................66
Receiving Services during the Non-Medicaid Appeal Process .............................................66
Consumer and Family Advisory Committee (CFAC) ................................................................66
Benefit Package.........................................................................................................................68
Eligibility ................................................................................................................................68
Who Is Eligible for the Medicaid Waivers? .............................................................................68
The NC Innovations Waiver (1915 c Waiver): .........................................................................69
Medicaid Waiver Dis-enrollment ...........................................................................................70
Eligibility for State Funded Services .......................................................................................70
Eligibility for Reimbursement by CoastalCare ........................................................................70
Enrollment of Consumers ......................................................................................................71
Service Definitions .................................................................................................................73
Service Array .........................................................................................................................73
4
Hospital Admissions...............................................................................................................73
Medicaid Transportation Services ..........................................................................................73
CoastalCare Clinical Design Plan ................................................................................................74
Access, Enrollment and Authorization of Services .....................................................................74
Accessing Routine Services ....................................................................................................74
Enrollment and Referral Process for Routine Needs ...........................................................74
Accessing Urgent Services......................................................................................................75
Enrollment and Referral Process for Urgent Needs ............................................................75
Accessing Emergent Services .................................................................................................77
Enrollment and Referral Process for Emergent Needs ........................................................78
Electronic Submission of Enrollments by Providers ................................................................80
Registry of Unmet Needs .......................................................................................................81
Care Coordination .....................................................................................................................82
Quality of Care .......................................................................................................................85
CCNC Collaboration ...............................................................................................................85
System of Care (SOC) .............................................................................................................86
System of Care Coordinators .................................................................................................86
Crisis Services ........................................................................................................................87
Innovations and Care Coordination........................................................................................87
Intellectual or other Developmental Disabilities (I/DD) ..........................................................89
Service Definitions and Criteria .................................................................................................90
Service Array .........................................................................................................................90
Medicaid Services ..............................................................................................................90
State Funded Benefit Plan ..................................................................................................91
Claims Information ....................................................................................................................92
Enrollment and Eligibility Process ..........................................................................................92
Eligibility Determination .....................................................................................................92
Enrollment Data .................................................................................................................92
Effective Date of Enrollment ..............................................................................................93
5
Patient ID ...........................................................................................................................93
Coordination of Benefits ........................................................................................................93
Eligibility Determination Process by Provider .....................................................................93
Obligation to Collect ..........................................................................................................94
Reporting of Third Party Payments.....................................................................................94
Process to Modify ..............................................................................................................94
Sliding Fee Schedules .........................................................................................................94
Authorizations Required for Payment ....................................................................................95
System Edits .......................................................................................................................95
Authorization Number & Effective Dates............................................................................95
Units of Service ..................................................................................................................95
Exceptions to Authorization Rule .......................................................................................95
Payment of Claims & Claims Inquiries ....................................................................................95
Clean Claims.......................................................................................................................95
Service Codes & Rates ........................................................................................................96
Standard Codes for Claims Submission ...............................................................................96
Timeframes for Submission of Claims .................................................................................96
NPI (National Provider Identifier) .......................................................................................97
Verification of Receipt of 837 Electronic Billing File ............................................................97
Provider Portal Direct Claims Submission ...........................................................................97
837 Claims Submission .......................................................................................................97
Process for Submission of Paper Claims .............................................................................98
Void and Replacement Claims Processing ..........................................................................98
Clearinghouse Claims Routing ............................................................................................98
Medicare Override Processing............................................................................................98
Claim Denial Inquiries ........................................................................................................98
Non –clinical claims appeals ...............................................................................................99
Response to Claims ................................................................................................................99
835 and Electronic Remittance Advice ...............................................................................99
6
Checkwrite Schedule and EFT Process ................................................................................99
Claims Investigations – Fraud & Abuse ..................................................................................99
Trends of Use & Potential Fraud.........................................................................................99
Audit Process .....................................................................................................................99
Voluntary Repayment of Claims ....................................................................................... 100
Reporting to State & Federal Authorities.......................................................................... 100
Repayment Process/Paybacks ............................................................................................. 100
Standards and Regulatory Compliance .................................................................................... 100
Introduction ........................................................................................................................ 100
Quality Improvement .......................................................................................................... 101
Provider Quality Management Plans ................................................................................ 101
Quality Improvement Projects ......................................................................................... 101
Performance Measurement ................................................................................................. 102
Data Collection and Verification ....................................................................................... 102
Performance Improvement .............................................................................................. 102
Provider Performance Profile ........................................................................................... 102
North Carolina Support Needs Assessment Profile-NC SNAP ............................................ 103
North Carolina Treatment and Outcomes Program Performance System –NC TOPPS....... 106
Performance Monitoring ..................................................................................................... 106
Monitoring of Incidents .................................................................................................... 107
Incident Reporting ........................................................................................................... 108
Additional Reporting to the MCO and DMH/DD/SAS: ....................................................... 109
Restrictive Interventions: ................................................................................................. 109
Where to report incidents: ............................................................................................... 110
Incident Review Process ................................................................................................... 110
Grievances ....................................................................................................................... 111
Perception of Care Surveys .............................................................................................. 112
Medical Record Requirements/Service Record Standards .................................................... 113
State Level Requirements Documents .............................................................................. 113
7
Federal Level Requirements Documents .......................................................................... 114
Corporate Compliance ............................................................................................................ 114
Corporate Compliance Program........................................................................................... 114
Corporate Compliance Plan .............................................................................................. 115
Compliance Committee .................................................................................................... 115
ComplianceHelp Desk ...................................................................................................... 116
Compliance Reporting Tools ............................................................................................. 116
Monitoring and Auditing .................................................................................................. 116
Investigation and Reporting ............................................................................................. 116
Code of Ethics ...................................................................................................................... 116
False Claims Act Education Requirements& Affordable Care Act ......................................... 117
Dispute Resolution Process for Providers ................................................................................ 117
Glossary of Terms.................................................................................................................... 123
Appendices ............................................................................................................................. 143
Official Communication Memos .............................................................................................. 144
Code of Ethics Policy ............................................................................................................... 145
Federal State and Local Requirements .................................................................................... 147
Introduction and Overview
Message from the Area Director
Welcome to the CoastalCare Network! Together, we will develop a comprehensive system of
care for those in our community having a mental illness, an intellectual/developmental
disability or a substance use issue. Our goal is to offer a system that is accessible, responsive
and of the highest quality; all while keep cost reasonable to the taxpayer.
We promise to assist you in overcoming barriers to effectively operate within the CoastalCare
network. We also promise to hold you accountable, as we hold ourselves, to the contract
8
requirements to provide high quality services, and for improving the quality of life for those we
serve. Your membership in the CoastalCare network is regarded as a commitment to partner
with us and others to achieve the goals of the Medicaid Waiver; improve quality of care,
improve access to services and promote cost efficiencies.
Together we can meet the needs of the present with an eye to the future. Good luck and
congratulations on becoming a part of the CoastalCare network.
Sincerely,
Foster Norman
Area Director/CEO
CoastalCare
Welcome to CoastalCare
Welcome to the CoastalCare network of providers! As part of this network, you join a group of
colleagues committed to providing the highest quality of care that meets the needs of citizens
residing in Brunswick, Carteret, New Hanover, Onslow and Pender counties. Thank you for
joining CoastalCare’s mission to improve the quality of life of individuals who have a mental
illness, substance use disorder or intellectual and other developmental disabilities.
The CoastalCare Provider Manual is the most comprehensive source of instructional
information available from CoastalCare to providers. It is intended as a detailed reference to
assist providers in following policies and procedures for CoastalCare. It also details statewide
procedures and regulatory information. It is your responsibility to be familiar with the
information provided in this manual, as well as to adhere to the policies and procedures
outlined. Compliance with this manual is necessary to fulfill contractual obligations as a service
provider with CoastalCare. Your knowledge and practice of this manual will also assist
CoastalCare in providing you with timely service authorizations and claims reimbursement.
CoastalCare is available to answer questions and offer technical assistance Monday through
Friday, 8 a.m. to 5p.m. Please call our Customer Services line at 1-855-250-1539.
9
Thank you for participating in the CoastalCare network and for your dedication to those that
both providers and CoastalCare serve. We look forward to our partnership in serving our
community.
Who we are:
CoastalCare is a local political subdivision of state government established under North Carolina
General Statute 122-C, and has been selected as aMedicaid 1915 (b) (c) Waiver site beginning
January 1, 2013. CoastalCare is the result of a merger between two area authorities, Onslow
Carteret Behavioral Healthcare Services and Southeastern Center for Mental Health,
Developmental Disabilities and Substance Abuse Services. CoastalCare manages a network of
providers that serve individuals with mental health, intellectual/developmental disabilities, and
substance use disorders that reside in Brunswick, Carteret, New Hanover, Onslow, and Pender
Counties.
CoastalCare is nationally accredited by URAC in four functional areas: Claims Processing, Health
Call Center, Health Network Management, and Health Utilization Management. CoastalCare
manages state allocated dollars, federal block grants awarded by the State of North Carolina,
and is one of 11 Medicaid 1915 (b) (c) Waiver sites in North Carolina that manage the Medicaid
funded services through a capitated Pre-paid Inpatient Health Plan (PIHP) beginning January 1,
2013.
Description of Expectations/Collaboration Goals
A self-managed system relies on educated providers who understand and operate intandem
with CoastalCare Clinical Objectives and the Clinical Design Plan. Our goal is todevelop a system
where the structure, requirements and expectations are so well known,that extensive
management and intervention by CoastalCare is not required. This model includesthe
engagement of our Providers in the management of the system and relies on theirinvolvement
in the development of strategies to meet quality and performance goals anddevelop solutions
for systemic problems. Providers participate with CoastalCare through the CoastalCare Provider
Council and the Clinical Advisory. Provider participation in the ongoing operations of the
CoastalCare system is critical in the efficient and effective identification of strategies that
willensure success in achieving our goals. Our joint purpose is to assure easy
access,appropriate,high quality services for consumers, and the elimination of ineffective
andpoor outcome services and practices.
Mission Statement
10
To improve the quality of life of individuals who have mental illness, substance use disorders
and intellectual and other developmental disabilities through efficient management of an
effective care system in our communities.
Vision Statement
To be recognized as a national leader in Public Managed Healthcare.
Value Statement
CoastalCare effectively manages its resources in a fair and equitable manner with efficiency,
accountability, and integrity for the needs of the present, with an eye to the future.
CoastalCare will promote services which are:
Innovative
Accessible
Responsive
Inclusive
Culturally Sensitive
Respectful
Evidence Based
The Medicaid Waiver: What is the NC DHHS Health Plan?
The NC DHHS approved 1915(b)(c) Waiver is a Pre-paid Inpatient Health Plan (PIHP) funded by
Medicaid. All Medicaid MH/DD/SA services are authorized by and provided through the
CoastalCare Provider Network in accordance with the risk contract between the Division of
Medical Assistance/Department of Health and Human Services and CoastalCare. As a prepaid
inpatient health plan, CoastalCare is at financial risk for a discrete set of MH/DD/SA services,
including both NC Medicaid State Plan services and services included in the NC Innovations
waiver.
The NC MH/DD/SAS Health Plan is a combination of two types of waivers: a 1915(b) waiver
generally known as a Managed Care/Freedom of Choice Waiver, and a 1915(c) waiver generally
known as a Home and Community Based Waiver. Through the 1915(b) section of the Social
Security Act, States are permitted to submit a request to waive some Medicaid requirements in
order to provide alternatives to the traditional fee for service system of care. Likewise, through
11
the 1915 (c) section of the Social Security Act, States are permitted to submit a request to waive
some Medicaid requirements in order to provide alternatives to institutional care. Both waivers
are approved under different Federal Medicaid Regulations and require different reporting and
oversight. This type of waiver system is not intended to limit care or choice but to create an
opportunity to work closely with consumers and providers on better coordination and
management of services, resulting in better outcomes for consumers and more efficient use of
resources.
Opportunities that a 1915(b)(c) waiver system presents:
In order to encourage:
Coordination - The waiver allows for better coordination of a system of care for consumers,
families and providers.
Efficient Management of limited public resources - We are able to manage all system
resources so that money can be directed to services most appropriate for identified
consumer needs.
Flexibility in services offered - We have developed a more complete range of services and
supports through Medicaid B-3 authority in order to reduce and redirect reliance on high
cost institutional and hospital care.
About the NC MH/DD/SAS Health Plan
This waiver applies to consumers with Medicaid that reside in any of our counties: Brunswick,
Carteret, New Hanover, Onslow, and Pender.
All Medicaid Clients enrolled in specified eligibility groups will automatically be enrolled into
this plan for their mental health, developmental disability, and substance abuse service needs.
The services that are available will include current NC State Mental Health Plan
Medicaid services including Inpatient Psychiatric care and Intermediate Care Facilities for the
Mentally Retarded (ICF/MR).
CoastalCare has partnered with the state to create additional services that have been identified
as best practices in care, B(3) services.
Under Medicaid B(3) authority, funds that are typically used to serve a person with
intellectual/developmental disabilities in an Intermediate Care Facility for the Mentally
Retarded (ICF-MR), through this waiver can be used to “follow the person” to services outside
of the ICF-MR facility.The CoastalCare Provider Network is qualified to provide best practice
services.Consumers will be able to choose from any provider in CoastalCare’s network that is
contracted and accessible to provide the service they need.Information and education will be
12
provided to consumers to help them choose providers.Access to care is made easier through
CoastalCare’s Call Center (1-866-875-1757)
About the NC Innovations Waiver
The NC Innovations waiver is a Home and Community Based Waiver 1915 (c). This is a waiver of
institutional care.This waiver incorporates the essential elements of Self-Direction, Person
Centered Planning, Individual Budgets, Participant Protections and Quality Assurance. The
waiver supports the development of a stronger continuum of services that enable individuals to
move to more integrated settings. People served and their families have the information and
opportunity to make informed decisions about their health care and services, and exercise
more control over the decisions they make regarding services and supports. The NC Innovations
Waiver has both a Provider Directed and Individual/Family Directed track. In the Provider
Directed track, the services are delivered in a traditional manner with consumers and family
members selecting the providers they believe can best meet their needs. Participants and their
families may choose from two models of Individual /Family Directed services, Employer of
Record or Agency with Choice. In the Employer of Record Model, the staff are hired, directed
and paid by the NC Innovations participant/legally responsible persons with the assistance of a
Community Guide and a Financial Supports Agency. In the Agency with Choice model, the
provider agency is the legal employer but the participant/legally responsible person is the
Managing Employer. The managing employer is responsible for interviewing, training, managing
(with oversight by the agency Qualified Professional) making recommendations to the provider
agency for hiring and firing. A consumer or guardian/family member can choose Provider
Directed, Individual /Family directed or a combination of both options.
CoastalCare Governance and Administration
CoastalCare is a local political subdivision of state government established under North Carolina
General Statute 122-C. The CoastalCare Area Board is a governing body, focused on
establishing and monitoring the goals and objectives of the agency, as well as the development
of public policy. The Chief Executive Officer (CEO) reports to the Area Board, and all other staff
of CoastalCare reports to the CEO.
CoastalCare is nationally accredited by URAC in four functional areas: Claims Processing, Health
Call Center, Health Network Management, and Health Utilization Management. CoastalCare
manages state allocated dollars, and federal block grants awarded by the State of North
Carolina, and is one of 11 Medicaid 1915 (b) (c) Waiver sites in North Carolina. As a Medicaid
13
Waiver site, CoastalCare manages the Medicaid funded services through a capitated Pre-paid
Inpatient Health Plan (PIHP).
Office of the CEO
The Office of the CEO is responsible for the overall management of administrative and clinical
operations for CoastalCare, as well as performance outcomes and achievement of goals. The
Office of the CEO consists of The Chief Executive Officer, Chief Operating Officer, Chief Medical
Director, Medicaid Waiver Project Coordinator, Public Information Officer and Executive
Assistant and Clerk to the Area Board. This unit maintains strong relationships with local and
state partners including provider agencies, public agencies, public and elected officials and
advocacy groups. The Office of the CEO charges the Executive Team with supporting
CoastalCare staff in achieving the goals and objectives of the agency.
CoastalCare is organized into several functional departments shown below. These
departments have been established to perform operational functions that support the mission
of CoastalCare.
Area Board
Office of the CEO
Executive Assistant and Clerk
to the Board
Chief Operating Officer
Medicaid Waiver Project
Coordinator
Public Information Officers
Chief Operating
Officer
Community
Development
Care
Coordination
Customer
Services
CoastalCare
Jacksonville
Office
Corporate
Compliance
Public
Information
Officer
CoastalCare
Corporate
Headquarters
Wilmington, NC
CFAC
Functional
Departments:
Finance
Human Resources
Information Technology
Customer Services
Community
Development
Care Coordination
Corporate Compliance
Network Management
Quality Management
Utilization Management
CoastalCare
Morehead City
Office
Network
Management
Care
Coordination
Customer
Services
Finance
14
Network Management Department
Mission Statement
The Network Management Department shall contract with, monitor and support providers of
behavioral health and developmental disability services to ensure a high quality network
sufficient to meet the prioritized needs of the eligible population.
Network Management Purpose
It is the purpose of the Network Management Department to maintain and manage a provider
network with the capacity and competence to effectively meet the assessed service needs of
the culturally diverse population within the agency’s catchment area.
It is also the purpose of the Network Management Department to implement a comprehensive
provider relations program that includes established mechanisms for assisting providers
regarding network issues, securing provider suggestions and guidance in improving services
delivered to consumers, soliciting provider participation in the review of agency network
management design, function and activities, and mechanisms for ongoing communication with
providers including the provider manual and communication plan.
The department performs essential functions of provider contracting, enrollment,
endorsement, monitoring, application of violations, implementation of corrective actions
and/or sanctions, and network performance assessment, tracking and reporting.
Network Management Department Organization
The Network Management Department has staff organized in a manner to address both
system-wide goals, processes and to be responsive to the needs of individual providers. The
Department Director directly oversees the development staff, including the Network
Development Coordinators, Contract Administrator and Credentialing staff. These positions
assist with network development planning, sufficiency assessment, implementing a qualified
network of providers and reporting.
The department Liaison Supervisor, who reports to the NM Director, oversees the Liaisons who
assist with network management and monitoring activities. The Liaisons are assigned to
specific providers to establish effective and knowledgeable collaboration as they address
provider-specific endorsement, monitoring, technical assistance and support. Communication
is directed at system-wide, disability-specific and individual provider levels.
15
Utilization Management
The Utilization Management (UM) Department includes Care Management (CM) and Utilization
Review (UR) functions.
CM Functions
The Care Managers determine whether a consumer meets and continues to meet
medical necessity criteria and target population requirements for the frequency, intensity and
duration of requested services. Our goal is to ensure that consumers receive the right service,
at the right time, and at the right level of care creating the most effective and efficient
treatment possible. This work is accomplished through consistent and uniform application of
CoastalCare’s Clinical Decision Support Tools for each consumer’s individual clinical needs to
determine the appropriate type of care, service, frequency of services, and intensity of services,
in the appropriate clinical setting. UM Care Managers assist the provider in managing a
consumer’s care needs and identification of appropriate services.
UR Functions
The primary Utilization Review function is to monitor the utilization of mental health,
substance use and intellectual/developmental disability services and review utilization data to
evaluate and ensure that services are being provided appropriately within established
benchmarks and clinical guidelines; that services are consistent with the authorization and
approved Person-Centered Plan (PCP)/Treatment Plan. Our goal is to ensure that consumers
receive the right service; at the right time; at the right level; creating the most effective and
efficient treatment possible.
Utilization review is a post-service review process that involves a pulling a sample from
paid claims. Information from the consumer’s record (assessment information, treatment plan
and progress notes) is evaluated against Medical Necessity Criteria. Indicators will be identified
to select cases for review, such as high utilization of service, frequent hospital admissions, etc.
as well as random sampling of other events. CoastalCare uses both Focused Utilization Review
and a sampling process across Network Providers in its Utilization Review methodologies.
Routine Utilization Review
16
Routine Utilization Review will focus on the efficacy of the clinical processes in cases as
they relate to reaching the goals in the consumer’s PCP / treatment plan. CoastalCare will also
review the appropriateness and accuracy of the service provision in relation to the
authorizations. All providers contracted with CoastalCare who are currently serving CoastalCare
consumers are subject to Utilization Reviews to ensure that clinical standards of care and
medical necessity are being met. A routine UR will be inclusive of, but not limited to:
evaluations of services across the delivery spectrum; evaluations of consumers by diagnostic
category or complexity level; evaluations of providers by capacity, service delivery, and bestpractice guidelines and evaluations of utilization trends.
The criteria used in the Utilization Review processes will be based on the most current
approved guidelines and service manuals utilized under the NC MH/DD/SAS 1915b and c
waivers and processes for NC State services. These documents include, but are not limited to,
the current NC State Plan service definitions with Admission, Continuation, and Discharge
criteria; the CoastalCare approved Clinical Guidelines; the current approved NC DMA Clinical
Coverage policies.
Focused Reviews
A Focused Review will be based on the results of Monitoring Reports that identify
outliers as compared to expected / established service levels or through specific cases
identified in the CoastalCare clinical staffing process to be outside the norm. Focused samples
may include:
High-risk consumers - Examples may include, but are not limited to, consumers who
have been hospitalized more than one time in a 30-day period; developmentally
disabled consumers as identified in the Risk/Support Needs Assessment; children and
youth with multiple agency involvement; or active substance use by a pregnant female.
Under-utilization of services – Examples may include, but are not limited to, consumers
who utilize less than 70% of an authorized service or consumers who have multiple
failed appointments.
Over-utilization of services – Example: consumers who continue to access crisis services
with no engagement in other services.
Services infrequently utilized – Example: an available practice that is not being used.
High-Cost Treatment – Consumers in the top 10% of claims for a particular service
17
Appeal Reviews
An Appeal Review is a local impartial review of CoastalCare’s decision to reduce,
suspend, terminate or deny Medicaid services. A health care professional who has appropriate
clinical expertise in treating the Consumer’s condition or disorder, and who was not previously
involved in CoastalCare’s initial decision, determines the Appeal Decision.
(See Reductions, Denials, Suspensions or Terminations of Medicaid Services for more
information)
Your responsibility as a CoastalCare Contracted Provider is to:
Submit Service Authorization Requests (SAR) with the proper clinical information
to allow UM Care Managers to review for medical necessity; and
Submit Continuing Service Authorization Requests on a timely basis to allow for
Utilization Management activities and authorization prior to beginning services.
Emergency Authorizations are available, but should only be used when necessary to provide for
consumer health and safety.
CoastalCare’s responsibility to Providers is to:
Provide accurate and timely response to Service Authorization Requests and to
ensure that consumers receive services for which they are eligible, and which are
clinically appropriate.
Quality Management
CoastalCare maintains a Quality Management Program which is a comprehensive, proactive
program that provides the structure, process, resources, and expertise necessary to
systematically define, evaluate, monitor and ensure that high-quality, cost-effective care and
service are provided to members. The program is a commitment to continuous quality
improvement principles and requires participation of the Area Board, providers, and staff
members. The Quality Management Program includes a continuous, objective, and systematic
process for: monitoring and evaluation of key indicators of care and service; identification of
opportunities for improvement; development and implementation of interventions to address
the identified opportunities; and for re-measurement to demonstrate effectiveness of program
interventions.
18
Quality Assurance & Quality Improvement
Quality Improvement goes beyond Quality Assurance. Perhaps the defining difference lies in
the fact that in addition to focusing on processes, correcting problems, analyzing data, and
making decisions based on information, QI emphasizes “Improvement”, not mere
“Compliance.” This is a distinct difference that focuses on going beyond standards and
regulations to a passion that believes that improvement is possible and preferable rather than
maintaining the status quo. In North Carolina, this has been a significant paradigm shift for
health care and for mental health, substance abuse, and developmental disabilities services in
particular.
However, Quality Assurance (QA) is much needed set of activities to ensure compliance with
rules, regulations, and requirements. It provides the basic foundation for a quality
improvement model and methodology. Quality Improvement (QI) is a planned, systematic,
organization-wide approach for monitoring, analyzing, and improving organizational and
provider performance. QI promotes the ongoing participation of all staff, consumers, providers,
family members, and other stakeholders in problem-solving efforts across functional and
hierarchal boundaries.
Adding the two elements together produces a comprehensive approach to assuring quality
care: Quality Management; QA + QI = QM.
Corporate Compliance
The purpose of CoastalCare’sCorporate Compliance department is to maintain an effective best
practice compliance program. The department conducts activities to prevent, detect and
correct fraud, waste and abuse to ensure the financial and clinical integrity of the agency. The
department conducts post-payment audits, monitoring and investigations to assure that
payment made to providers for services are rendered in accordance with rules, regulations,
policies and the terms of the provider contract. The departmentreceives allegations of fraud
and abuse from various sources to include, tip-line, complaints, incidents, issues identified by
staff, data mining, detection tools and statistical sampling. The department conducts reviews
of all allegations and if warranted conducts an investigation. The department makes referrals
of suspected fraud and abuse to Division of Medical Assistance-Program Integrity and other
appropriate regulatory bodies. The department maintains the Corporate Compliance Plan.The
department develops and facilitates education and training on prevention, detection and
reporting of fraud, waste and abuse for staff, providers and stakeholders.
19
Finance and Reimbursement
The primary purpose of the Business Management Department is the organization of the fiscal
and budgetary operations of the Area Authority. The department is responsible for sound
financial planning for the area program and for ensuring compliance with all fiscal policies at
the local, state and federal levels. The Business Management department comprises the
following areas: general budget and finance, claims processing and physical plant operations
and maintenance.
Care Coordination
Care Coordination will ensure each consumer identified as having special health care needs
receives a course of treatment, with regular care monitoring that addresses their individualized
needs. Mechanisms used to ensure appropriate treatment planning include; engagement of
the appropriate treatment providers in the Person Centered planning process, review by
community high risk team inclusive of CCNC and primary care providers, referral to appropriate
professionals for additional assessment as needed. The care coordinator will ensure the
development of a treatment plan that meets these conditions.
Customer Services/Call Center
CoastalCare is responsible for publishing two toll free numbers, one to access the Customer
Service Office (1-855-250-1539) and the other to access the Call Center (1-866-875-1757). The
Customer Service Office is staffed with Qualified Professionals whose primary purpose is to
assist consumers, their family members, providers, and other stakeholders to resolve routine
complaints and ensure that accurate and relative information surrounding the MCO, network of
providers, and service availability is accessible. As outlined in the CoastalCare organizational
structure, the office of Customer Service is clearly defined as a separate division with clear
functions from Utilization Review, Finance, Planning and Collaboration, Quality Management
and Network Management to ensure fair and impartial review of issues and actions.
Customer Service Representatives are available by calling the toll-free Customer Services line
listed above or by emailing Customer.Services@coastalcarenc.org. Customer Service
Representatives are available Monday-Friday, 8 a.m. to 5 p.m.
20
CoastalCare is also responsible for ensuring a timely response for consumers accessing mental
health, intellectual/developmental disabilities, and substance abuse services. The Call Center
line is available 24 hours per day, 7 days per week, 365 days per year. It is staffed with licensed
clinicians whose primary purpose is to assess consumers’ needs and offer options based on the
consumers’ preferences and the service needed. Call Center Clinicians also monitor follow-up
to care to ensure consumers have initiated services. Once the consumer has chosen a provider,
Call Center Clinicians will schedule an appointment with that provider through the provider’s
AlphaMCS calendar.
Medical Director
CoastalCare’s Medical Director is the Chief Medical Officer and is responsible for overall clinical
operations at the corporate office. The CoastalCare Medical Director is responsible for the
overall clinical management of services to consumers, including authorization of services,
quality oversight, and utilization management. Other activities include collaboration with
CoastalCare’s network providers, primary care providers in the community, and State and
community hospitals as well as development of preventive health projects for CoastalCare’s
consumers.
Operational Committees
The committee structure of CoastalCare has been revised to include six committees that
revolve around the functions of the organization as a MCO: Quality Management Committee,
Network Development and Management Committee, Utilization Management Committee,
Community Coordination Committee, Claims Processing Committee, and Customer
Services/Call Center Committee. Each committee has oversight for the operations of a
particular function and each department has a designated committee to review its particular
functions. These committees are referred to as content committees. If needed, each
committee can also develop sub-committees for particular areas of interest or projects. There
are additionally two subcommittees of the Quality Management Committee: Corporate
Compliance and Training. The Network Management Committee has a subcommittee as well
known as the Clinical Advisory Committee. This committee serves as an advisory group whose
membership includes various stakeholders (e.g. providers, licensed independent practitioners,
CCNC, DSS, etc.). This sub-committee serves as a formal mechanism for soliciting stakeholder
input regarding clinical processes, work products, etc. for the organization. All committees
report their activities to the Quality Management (QM) Committee.
21
Each committee is responsible for the review of data relative to the functional areas of the
organization. Data identified as outliers within each committee is then reported to the Quality
Management Committee for further analysis and the identification of an action plan. The
established committee structure serves as a formal mechanism for communication and
feedback loops, including data reporting throughout the organization.
Provider Network
Description of Network
CoastalCare is an oversight agency that has written agreements (contracts) with a specialty
network of participating providers to provide outpatient/periodic services, enhanced benefit
services, residential services, and crisis services. These services are available in a variety of
settings including offices, the consumers’ homes, the general community, and in licensed
facilities. CoastalCare is responsible for a five county area in North Carolina. The five counties
are; Brunswick, Carteret, New Hanover, Onslow and Pender.
Types of Providers
Periodic services can be office based or community based. Examples of these services include
direct DD services such as personal assistance, respite and Adult Day Vocational Programs.
Providers of these services have office locations in all five (5) counties and the community
based services are available in all five (5) counties.
Enhanced benefit services can be community based (such as Community Support Team) or
based in a Division of Health Service Regulation (DHSR) licensed facility (such as SAIOP,
Psychosocial Rehabilitation). Providers of enhanced benefit services serve all five counties and
facilitate transportation to facilities when necessary. CoastalCare has identified two enhanced
benefit services for priority monitoring because they are high cost and delivered to priority
consumer populations. These are Assertive Community Treatment Teams (ACTT) and Substance
Abuse Intensive Outpatient (SAIOP) treatment. ACTT is an evidence based practice to meet the
identified needs of recipients who have serious and persistent mental illness and/or cooccurring disorders and the most complex treatment needs. This is a community based service
available to consumers throughout the catchment area. SAIOP is provided in a licensed facility
and is the identified best practice for adult substance abuse consumers according to the ASAM
level of care criteria.
22
Residential services are provided in licensed facilities. There are local group homes & child
residential beds, as well as agreements with out-of-area providers for specialty beds or local
capacity limitations. CoastalCare is able to enter into temporary contractual arrangements, with
providers outside of the geographic area, so that the goals of access can be met for all
consumers who are legal residents of the geographic area.
Clinical Home for Consumers
The state Medicaid Service definitions implemented in March 2006 included the designation of
a Clinical Home for consumers. The role of the Clinical Home is further reinforced by the
development of the Critical Access Behavioral Health Agency model (CABHA). CABHAs are
designed to provide the core clinical services that are needed to ensure consumers receive the
continuity of services that they need. Expected Outcomes for CABHAs and other providers
functioning as Clinical Home Providers:
1. Single point of responsibility to plan, link and coordinate clinical and support services for
consumers.
2. Clinical accountability.
3. First Responder responsibility is clearly assigned.
4. Responsible for development of Crisis Plan or Advance Directive
5. Team approach to planning and monitoring care. Team includes (as appropriate)
psychiatrist, nurse, licensed professional, and peer specialist as well as staff from other
provider agencies serving the person.
6. Development of Person Centered Plans that reflect all consumer needs.
7. Communication with primary healthcare provider.
First Responder
Many of the Medicaid State Plan service definitions approved in 2006 and revised in 2010
include a “first responder” requirement as part of the service definition. This requires that
providers have on-call capacity to respond in the case of a crisis for a consumer that is in their
care. This means that consumers will have the advantage of having someone that knows them
respond when they experience a crisis
Crisis Services for mental health and substance abuse detoxification issues are available
through a local Facility Based Crisis (FBC) provider, a Mobile Crisis Management team and WalkIn Crisis Clinic in multiple locations.
Licensed Practitioners and Professional Practice Groups are Medical Doctors (M.D.),
Practicing Psychologists (Ph.D), Psychologist Associates (Master’s Level Psychologist
[LPA]), Master’s Level Social Workers (LCSW), Licensed Marriage and Family
23
Therapists (LMFT), Licensed Professional Counselors (LPC), Licensed Clinical
Addiction Specialists (LCAS), Advanced Practice Psychiatric Clinical Nurse Specialists,
Psychiatric Nurse Practitioners, and Licensed Physician Assistants who are members of the
Provider Network and bill under their own license. Licensed Practitioners must be credentialed
by CoastalCare. Our enrollment process includes background checks, reference checks, license
verification and other evaluation criteria to make certain the provider meets CoastalCare and
URAC criteria.
Additionally CoastalCare collects information about specific expertise of Licensed Practitioners
(such as Women’s issues, Trauma experience, etc.) in order to help consumers make choices
about providers.
Provisionally Licensed Practitioners are practitioners who are provisionally licensed in NC and
are employed by a Network Provider Agency, Hospital, or Group Practice. Provisionally
Licensed Practitioners may serve Medicaid consumers if they are working for an agency,
hospital, or group practice that is fully contracted with CoastalCare to provide Outpatient
Treatment. Under these circumstances a Provisionally Licensed Practitioner may submit a
CoastalCare Application To Participate as a HealthCare Practitioner. In addition to completing
and submitting the application, the Provisionally Licensed Practitioner must also provide proof
of professional clinical supervision as evidenced by a current supervision contract including the
name and contact information of the clinical supervisor. The clinical supervisor must provide an
attestation stating that the provisionally licensed practitioner is receiving supervision and that
the supervisor has approved the supervision contract. Upon approval by the Credentialing
Committee, the Provisionally Licensed Practitioner will be able to provide Outpatient Treatment
to CoastalCare consumers and submit claims for those services in accordance with the
CoastalCare Provider Contract, the practitioners Licensing body, and/or limitation established
by CoastalCare’s Credentialing Committee.
Out of Area Provider is a contracted Agency or Licensed Independent Practitioner, which
provides specialty services that are not available within the CoastalCare catchment area. Such
providers meet all network requirements and are considered to be full members of the
CoastalCare Network.
Non-Enrolled, Non-Contracted Providers: If a CoastalCare consumer requests services from a
provider who does not wish to apply to become a contracted provider with CoastalCare or is
unable to pass the Enrollment process, the licensed independent practitioner or agency will be
required to transition the consumer to the CoastalCare contracted provider of their choice
within 60 days.
24
If a person receives non-emergency services from a non-enrolled, non-contracted provider,
CoastalCare will not pay for the service. CoastalCare will pay for acute behavioral emergency
care for a CoastalCare Consumer by a non-enrolled, non-contracted provider.
When a consumer enrolled in the NC MH/DD/SA Health Plan resides outside of the CoastalCare
counties, CoastalCare will work collaboratively with the consumer and providers in that area to
ensure that the consumer has access to needed services.
Most services will be available within thirty (30) miles or thirty (30) minutes. However, some
specialty providers may be located outside the person’s county of residence. There may be only
one provider of facility based services, such as Psycho-social Rehabilitation in a county due to
insufficient demand to support two providers and economy of scale factors. CoastalCare
annually evaluates the location of providers and types of services in its Sufficiency Analysis, and
determines the need for additional providers. CoastalCare also maintains geo-maps which allow
us to evaluate location of providers in relation to where consumers live within the catchment
area.
Quality of Care
CoastalCare’s responsibility is to assure the quality of services provided by the CoastalCare
Network of Providers. CoastalCare is accountable to the Division of MH/DD/SA and the Division
of Medical Assistance in the management of both state funded and Medicaid services. In
addition to state requirements, Medicaid waiver quality requirements are extensive and
include:
Health and safety of consumers
Rights protection
Provider qualifications
Consumer satisfaction
Management of complaints
Incident investigation and monitoring
Assessment of outcomes to determine efficacy of care
Management of care of Special Needs Populations
Preventive health care initiatives
Clinical best practice
Coastal Care has numerous quality, satisfaction and financial reporting requirements related to
our agreements with the Division of MH/DD/SA and DMA. An Intra-Departmental Monitoring
Team evaluates CoastalCare’s performance annually. CoastalCare understands the important
role of quality management in protecting consumers and in promoting quality of care.
25
Your responsibilities as a CoastalCare Provider:
Ensure that consumers meet medical necessity requirements for all services that you or
your agency provides.
Provide medically necessary covered services to consumers according to your contract
and as authorized by CoastalCare.
Strive to achieve best practice in every area of service.
Provide culturally competent services and ensure the cultural sensitivity of staff
members. Develop a Cultural Competency Plan and comply with cultural competency
requirements.
Have a clinical backup system in place to respond to crisis/emergencies for consumers
receiving services. Part of this clinical function is to develop crisis plans that are
available to clinicians in your office for consumers, their natural supports and
CoastalCare. The clinical backup system will provide information and directions on how
to seek assistance in a crisis/emergency including coverage for posted office hours,
week-ends, and holidays for all consumers you serve or to serve as first responder as
outlined in the service definition of your contract.
Demonstrate consumer friendly services and attitudes. The Network Provider must
have a system to ensure good communication with consumers and families.
Comply with the policies and procedures outlined in this manual, any applicable
supplements, CoastalCare Communication Memos and in the Provider Contract,
including the General Conditions of the Contract and applicable state and federal laws
and regulations.
Provide services in accordance with all the applicable state and federal laws and
regulations.
Provide services in accordance with access standards and appointment wait time as
noted in the General Conditions of the Provider Contract.
Have a no reject policy for consumers who have been determined to meet medical
necessity for the covered services by the provider or by the Licensed Independent
Practitioner.
CoastalCare Providers must provide their consumers with 24/7/365 telephonic access to
a clinician or qualified professional in the case of an MH/DD/SA crisis or emergency.
This contact may not be 911. This contact may also not be a hospital or mobile crisis
team unless that is the service being provided under contract with CoastalCare.
The contact person must:
o Have the qualification, training and capacity to navigate the range of MH/DD/SA
crisis scenarios a consumer may experience;
o Advise the consumer and assist in the coordination of care during the crisis;
26
o Be available telephonically and may assist in-person if the situation requires;
o Have immediate access to crisis plans for consumers who have crisis plans;
o CABHA’s and other enhanced service providers must also ensure they fully
comply with additional first responder duties outlined in state policies and
service definitions.
Work with CoastalCare to ensure a smooth transition for any consumers that desire to
change providers, or when you need to discharge a consumer because you cannot meet
his/her special needs.
Document all services provided as per Medical Requirements, NC Waiver requirements
and North Carolina State Rules.
Agree to cooperate and participate with all utilization review/management, quality
management, other reviews, and appeal and grievance procedures.
Comply with Credentialing and Endorsement Procedures of CoastalCare that are
outlined in the Enrollment Process to become a Network Provider.
Comply with Authorization and Utilization Management requirements of CoastalCare.
Comply with re-credentialing or re-qualifying procedures of Coastal Care.
Participate in consumer satisfaction surveys, provider satisfaction surveys, clinical
studies, incident reporting, and outcome requirements.
Establish a plan and process for maintenance of personnel and consumer medical
records in accordance with the Records Management and Documentation Manual
(APSM 45-2) records retention schedule
CoastalCare’s Responsibilities to Providers:
Provide assistance twenty-four (24) hours a day, seven (7) days a week to consumers,
and potential consumers including crisis coordination.
Assist providers in understanding and complying with CoastalCare policies and
procedures, applicable policies and procedures of the Department of Health and Human
Services and federal agencies including Centers of Medicare and Medicaid, as well as
the requirements of our accreditation agencies including, but not limited to the
Utilization Review Accreditation Commission (URAC).
Provide technical assistance related to CoastalCare’s contract requirements,
CoastalCare’s Provider Manual requirements, DMA and DMH/DD/SAS requirements of
providers, the development of appropriate clinical services, quality improvement
initiatives, or to assist the provider in locating sources of technical assistance.
CoastalCare is not required to provide technical assistance in areas that would normally
be considered standard operational activities of a provider agency or to providers that
have shown by history not to be able to assimilate previous technical assistance.
27
Make available to providers upon request, the results of its Sufficiency Assessment
which identifies providers that are under or over capacity as well as priorities for
Network Development. CoastalCare is not required to contract with providers beyond
the number necessary to meet the needs of its Consumers.
As a part of the continuous quality improvement process, CoastalCare has a Quality
Management Committee (QMC). The Quality Management Director develops the
Quality Improvement Plan that is reviewed and approved annually by QMC and the
Area Board. The Plan identifies strategies and approaches that are designed and
implemented to identify, track and trend CoastalCare and system wide performance of
outcomes, structures and processes designed by the Area Board, CoastalCare, DHHS,
federal and state guidelines and accreditation standards. The strategies and
approaches shall include performance measures related to access to services,
complaints, satisfaction and others reflective of the scope of URAC accredited
programs. CoastalCare makes information available about it QMC performance to
providers, practitioners, members and stakeholders .
Cultural Competency of the Network:
It is important that the CoastalCare Provider Network is able to adequately meet the needs of
people from all ethnic groups. CoastalCare’s comprehensive process for gathering and
analyzing information identifies needs and gaps in service capacity in the five county geographic
catchment area. This is one mechanism to assess network adequacy and sufficiency. From this
needs and gaps assessment, CoastalCare develops mechanisms to measure and address the
culturally sensitive needs of the consumer population.
Definition of Cultural Competence
Cultural competence refers to an ability to interact effectively with people of different cultures.
Cultural competence is comprised of four components:
Awareness of one's own cultural worldview,
An open attitude towards cultural differences,
Knowledge of different cultural practices and worldviews, and
Cross-cultural skills. Developing cultural competence results in an ability to understand,
communicate with, and effectively interact with people across cultures.
Cultural competence may also be associated with diversity. Diversity must be prevalent and
valued before one may be considered a culturally competent or diversity competent
organization.
28
CoastalCare believes in approaches and interventions that are based on, and targeted to,
person centered results. The agency seeks to maintain an asking stance/partnership with the
community. Methods and services that are culturally congruent and that allow individuals a
voice in the behavioral health services and treatment they receive, are part of our commitment
to our catchment area. CoastalCare leadership is invested and committed to cultural
competence. Cultural competence touches every department of CoastalCare and the Providers
who serve CoastalCare consumers and includes regular cultural competence monitoring.
CoastalCare Network Management, Quality Management, and Quality of Care reviews will
monitor compliance and audits of medical records, administrative files, the physical
environment, and other areas of service including cultural competency reviews.
CoastalCare responsibilities include use of the following mechanisms:
a. Annual needs/gap assessment to measure the cultural and linguistic needs of the
consumer population. The cultural and linguistic composition of the total population
is assessed during this time;
b. Obtains information/reports from the Health Call Center, Utilization Management,
Customer Services, and the Care Coordination Directors related to utilization and
access cases involving linguistics and ethnicity;
c. Obtains reports from the interpreter services with whom CoastalCare contracts; and
d. Expands and promotes cultural diversity activities designed to increase providers’
awareness in their quest to serve our growing, culturally diverse population.
e. Based upon community cultural, racial, and ethnic composition, evaluate (and
document) whether agency's existing location and physical appearance are
respectful and representative of its community members and their culture.
f. Contrast and compare who is currently served, to the population(s) present in the
community. Identify gaps in available community resources, apparent service needs
based upon who is being served, and request feedback from consumers and families
utilizing the services.
g. Consider stigma and its influence on the community to include unique cultural
responses to people with mental illness.
CoastalCare assures the Provider Network’s cultural competency awareness by the use of the
CoastalCare Cultural Competency Plan and mandates that upon implementation of the
CoastalCare Cultural Competency Plan that Providers comply with its direction in provision of
mental health, developmental disability and substance abuse services. The goal is for each
provider to create their own internal Cultural Competence Plan. Providers should set objectives
29
to address and identify mechanisms to renew, enhance, and increase staffs' cultural sensitivity,
cultural awareness, and ability to provide culturally relevant services.
Your responsibility as a CoastalCare Provider is to;
Provide culturally competent services and ensure the cultural sensitivity of staff
members
Actively participate in community collaborative efforts to develop prevention, education
and outreach programs
Actively participate in the education of stakeholders and consumers on system access,
services available, appeals and grievances, advanced directives and the provider
network
Earnestly participate in initiatives to achieve cultural competence
Pursue the acquisition of knowledge relative to cultural competence and the provision
of services in a culturally competent manner.
To be responsive to the cultural and linguistic needs of the consumers your agency
serves
Review your agencies Mission/Vision/Values statements for inclusion of cultural
competence
Adhere to all cultural competence contractual elements
Have access to appropriate self-awareness assessments for their agency
determine the areas that are currently culturally competent
Providers are encouraged to develop an agency specific implementation plan
What changes should your program make to enhance cultural competence?
Help staff learn more about local communities’ service needs and barriers to treatment
Make it easier for consumers to use the services of this program
Have the program’s décor better reflect the heritage of consumers and families using
the facility
Give persons from diverse backgrounds a greater voice in how services are delivered
Other staff added ways to learn about beliefs, customs, norms or values of consumers
and families served – and the diversity within these groups
Help to build diversity of top staff through “in house” promotions
Build contacts with those to whom local religious, ethnic or racial groups turn for
leadership, guidance or aid
Teach staff more about local community helping resources
Attend to concerns of people who differ from the majority in culture or color, i.e., social
justice and quality of life issues such as employment, housing and education
30
Advocate for, begin to use, or use more widely, instruments for consumer diagnosis or
assessment that address cultural concerns.
Send a stronger message that the program will not accept insults towards any race,
religion or ethnic group
Begin to use, or more widely use, or promote treatment that addresses cultural
concerns.
Network Providers will consistently demonstrate efforts to assure that their services eliminate
the effects of any biases based upon individual and cultural factors.
Cultural Competence Goal:
CoastalCare’s Provider Network demonstrates cultural competence with the programs, services
provided to consumers, and is responsive to the cultural, racial and ethnic differences of the
populations served. CoastalCare’s mandate is, in part, that the system will reflect the
uniqueness of our local communities and be shaped by the choices of consumers and their
families. Cultural Competence extends beyond cultural sensitivities into the behaviors,
attitudes, and policies that enable the system to work more effectively in cross-cultural
situations.
Provider Communication
CoastalCare recognizes the vital role that communication plays in stable, productive, and
successful relationships. Listed below are the most notable topics in regard to CoastalCare and
provider communication including avenues for CoastalCare to disseminate information to its
provider network. The CoastalCare Network Communication Plan has been developed to
increase understanding of how providers can obtain needed information from CoastalCare as
well as provide feedback on the various area authority functions.
1. Orientation and Training
2. The Provider Manual
3. Network Management Department
4. CoastalCare Website
5. Communication Memos
6. Local Provider Meeting
7. List Serve
8. Provider Council
9. Clinical Advisory Committee
10. Performance Improvement Teams
31
When CoastalCare implements changes that affect the Provider Network, information about
those changes is communicated through official CoastalCare communication memos.
Communication Memos are posted on the CoastalCare website and notification of the posting
of new memos is relayed to providers via the list serve. All providers are welcome to add their
email addresses to the CoastalCare list serve. The CoastalCare website contains a provider page
with information specifically for providers including upcoming trainings, resources, a library of
forms, details and minutes from the local provider meeting and access to all current and
archived Communication Memos.
Your responsibility as a CoastalCare Network Provider is to:
Keep apprised of current information through the communication offered and provide
services as per the most recent State standards or waiver service definitions;
Attend and participate in Provider meetings in your area
Review the web site for updates on a regular basis;
www.CoastalCareNC.org
Review the State web sites for most up to date information on a regular basis;
www.dhhs.state.nc.us/mhddsas
www.dhhs.state.nc.us/dma
www.cms.gov
Work in conjunction with CoastalCare staff for technical assistance
CoastalCare Wilmington location: (910) 550-2624
CoastalCare Jacksonville location: (910) 459-4816
CoastalCare Morehead City location: (252) 648-3101
CoastalCare’s responsibility to you, the provider, is to:
Offer Provider Meetings in two locations monthly and post the schedule on the
www.CoastalCarenc.orgweb site under the provider tab
Post official CoastalCare Communication Memos on the CoastalCare web page
Send written correspondence via the mail as needed
Assign a Network Management Liaison to each Provider to develop a personal working
relationship and contact who can respond to individual provider needs
Attend meetings with providers as needed to clarify issues or provide technical assistance
Respond to provider inquiries and provide feedback in a timely manner.
32
Provider Council
The Provider Council is one of the key structures of CoastalCare to ensure the perspective of
providers is represented in network management decisions. as such, the council has
responsibility to network providers in representing their interests and challenges, to consumers
and family members and to CoastalCare in responding to standards, key indicators, initiatives
and requirements.
Mission: The CoastalCare Provider Council serves as a fair and impartial representative of all
service providers within the network. The Provider Council shall facilitate open exchange of
ideas, share values, goals, and vision and promote collaboration and mutual accountability
among providers. The Provider Council strives to achieve best practices to empower consumers
within our community to achieve their personal goals.
The objectives for the Provider Council are as follows:
Review and comment on Performance Indicators for network providers.
Review and comment on Plans, Products, Guidelines, related to network management.
Review and comment on provider payment policies or processes.
Review and comment on Needs Assessment and Barriers to services/providers.
Review and respond to Annual Provider Satisfaction Survey
Review and comment on contracting process and provider selection criteria
Review and comment on procedures related to the provider violation mechanism,
sanction criteria and dispute resolution process.
Review and comment on training needs and materials.
Review and comment on QIPs
Membership
The Provider Council membership consists of currently active, Medicaid and state funded
partners that represent the characteristics of the network – consumers served, geographic area
covered and types of services provided.
The Provider Council became operational in the June of 2012 and the current membership and
a schedule of meetings can be accessed on the CoastalCare website under the provider page.
Minutes are posted on the CoastalCare website and are on the provider page.
Provider Enrollment and Credentialing
As a part of the 1915 b/c Medicaid Waiver implementation, the Centers for Medicare and
Medicaid Services (CMS) requires that each Area Authority credential and enroll providers in
33
the network. There are separate application formats, which must be completed and submitted
based on the provider type. Applications are formatted to be typed or hand written.
Licensed Independent Practitioners (LIP)
Agencies
Hospitals
Credentialing
All providers who are directly enrolled with the Division of Medical Assistance to provide
behavioral health services must enroll with CoastalCare. Licensed Independent Practitioners
(LIP) who are required to be credentialed include:
Advanced Practice Psychiatric Clinical Nurse Specialist who is eligible to bill Medicaid
under their North Carolina license
Certified Clinical Supervisor
Licensed Clinical Addiction Specialist (LCAS)
Licensed Clinical Social Worker (LCSW)
Licensed Marriage and Family Therapist (LMFT)
Licensed Professional Counselor (LPC)
Licensed Professional Counselor Supervisor (LPCS)
Licensed Psychologist (PHD Level)
Medical Doctors, who employ clinical staff who bill “incident to” the physician’s
Medicaid Provider Number
Nurse Practitioner
Physician Assistant
Psychiatrists
34
Psychological Associate (LPA)
Provisionally Licensed Clinicians who are employed by an agency
LIP’s who bill Medicaid directly must enroll individually. LIP’s who are employed by an agency
or group practice, must apply for enrollment at the same time (one complete packet) as the
agency to be “associated with” the agency/group practice.
CoastalCare is accepting applications from provisionally licensed practitioners who are
employed by an agency and who bill Medicaid using the agency’s Medicaid Provider Number.
Provisionally licensed clinicians who bill “incident to” a physician within a group practice will not
be credentialed or enrolled at this time; however, the physician overseeing these services must
be credentialed and enrolled with CoastalCare.
Credentialing Application Review
Credentialing Applications will be thoroughly reviewed by credentialing staff within the
Network Management Department. If any information in an application is missing, incorrect, or
inconsistent, providers will be requested to make corrections and/or submit additional
information. As a part of the credentialing process, staff will conduct primary source verification
and an evaluation of good standing status. Also, each credentialing applicant will be presented to
the Credentialing Committee for a determination to approve or disapprove the application.
Providers may request information regarding the status of their application at any time during the
credentialing process. Providers are required to be recredentialed at least every three years.
Primary Source Verification
Primary source verification is defined as “verification based on information obtained directly
from the issuing source of the credential”. Credentialing standards require that CoastalCare
complete primary source verification of licensure. When possible the primary source
verification will be completed through an on line process. When the applicable licensure board
does not complete primary source verification of education, CoastalCare is required to do so.
Boards that do not conduct primary source verification of education are:
Medical Board
NC Substance Abuse Professional Practice Board
35
When CoastalCare is required to conduct primary source verification of education, the LIP is
required to request an official transcript to be submitted directly from the school or university.
Evaluation of Good Standing Status
“Good Standing” status as required for eligibility as a contracted provider is still in the process
of being defined. The determination of “Good Standing” status for providers may be
determined through a variety of means, including but not limited to:
Office of Inspector General’s list of Excluded Individuals and Entities (LEIE) http://exclusions.oig.hhs.gov/
The Data Bank, to include the NPDB and HIPDB- http://www.npdbhipdb.hrsa.gov/index.jsp
The NC Secretary of State Tax Lien databasehttp://www.secretary.state.nc.us/taxliens/filingsearch.aspx
Medicare Exclusion Databases (MED)
Inquiry of state agencies using the standardized Verification of Good Standing form.
Excluded Parties List System (EPLS)- https://www.epls.gov/
Credentialing Committee
CoastalCare’s Medical Director, who is an M.D., is responsible for oversight of the clinical aspects
of the credentialing program and serves as the chair person for the Credentialing Committee. The
Credentialing Committee consists of CoastalCare and provider agency staff that represent the
composition of the network.
The Credentialing Committee may request additional information regarding an applicant.
Although a credentialing applicant can make corrections and submit additional information, the
Committee may choose to factor in inconsistencies with the submitted information when making
credentialing decisions. Only “clean applications” as defined in procedure, will not be individually
reviewed by the committee.
The Credentialing Committee is responsible for the following:
Providing the overall direction of the Credentialing Program including review and approval
of credentialing policies and procedures.
36
Approving or disapproving applications for network participation. The Committee may
delegate authority to the Medical Director for approving clean applications.
Discussing whether providers are meeting reasonable standards of care.
Accessing appropriate clinical peer input when discussing standards of care for a
particular type of provider.
Maintaining Committee Minutes and documenting all actions.
Evaluation and report to CoastalCare’s Management Team on the effectiveness of the
Credentialing Program.
Meeting as often as necessary to fulfill credentialing responsibilities, but no less than
quarterly.
Staff that have access to credentialing information and members of the credentialing committee
will receive training regarding confidentiality of credentialing information. Each credentialing
committee member and any staff that have access to credentialing information will sign a
confidentiality statement. Access to credentialing information will be restricted to authorized
personnel on a need to know basis.
Performance Monitoring
Local monitoring of Mental Health, Intellectual/Developmental Disabilities, and Substance
Abuse provider agencies is one of CoastalCare’s oversight responsibilities. SB 163 monitoring
rules were established to assure monitoring of Category A and B providers of mental health,
Intellectual/Developmental Disabilities, and substance abuse services.
Gold Star Rating and Monitoring Process
The Gold Star Rating and Monitoring Process was adapted to standardize the monitoring
process across the state and is consistent with the 1915 (b)/(c) Medicaid Waiver model and
retains fidelity to that model pursuant to S.L. 2011-264. Specific information regarding provider
monitoring including review tools can be found at:
http://www.ncdhhs.gov/mhddsas/providers/providermonitoring/index.htm .
An overview of the Gold Star Monitoring Process can be reviewed at:
http://www.ncdhhs.gov/mhddsas/providers/providermonitoring/flowchart.pdf .
The Gold Star Rating and Monitoring Process consists of an initial policy and procedure review,
provisional , routine, preferred, exceptional and gold star profiles based on length of time in
service provision within the CoastalCare network and request from the provider to move
beyond the Routine Profile.
37
The Provider Performance Profile Grid gives an over view of the Gold Star requirements for
each level.
DHHS Provider Performance Profile Grid
Noncontract
providers
0 star
Provider
did not
pass
process
Provisional Profile
Routine Profile
(Qualified and/or
Probationary Status 6
months - 1 year)
Preferred Profile
(Commendable)
Exceptional Profile
(Excellent)
Gold Star Profile
(Achievement
Plus)
1 star
2 stars
3 stars
4 stars
5 stars
Review scores are
less than 75% or
significant issues are
identified
Maintain review scores
between 75%-100%
Maintain review
scores between 80%100%
Maintain review
scores between 90%100%
Maintain review
scores between
95%-100%
Review every 6
months
Review Annually
Review every 2nd
year
Review every 3rd year
Review every 3rd
year
Per Qualifying
Committee
recommendation
Provider meets all NC
State Standards and
contractual
requirements
Providers are
required to meet all
previous level
requirements & ALL
items listed below
Providers are
required to meet all
previous level
requirements & ALL
items listed below
Providers are
required to meet
all previous level
requirements &
ALL items listed
below
Serve consumer(s) a
minimum of 90 days
Serve consumer(s) a
minimum of 1 yr
Serve consumer(s) a
minimum of 2 yrs
Serve
consumer(s) a
minimum of 3 yrs
Infrastructure for
implementation of
Independent CQI
process where
information/data is
gathered and
analyzed through CQI
processes. (paper)
Provider has
established formal
self monitoring
quality
management
systems that
generate data
based results that
includes a
functional CQI
process. Submit
reports to
appropriate
committees.
(actual
implementation)
Noncontract
providers
Terminated
contract
providers
Providers new into
system with no
active consumers
Provider completes and
annual satisfaction
survey
Infrastructure for
implementation of
early CQI phases
such as Independent
CQI committee, CRC,
Board of Directors
with different
members on each
committee.
38
Beginning Best Practice
trainings for staff
Agency is beginning
to focus on quality
verses rules to define
quality internally.
Agency is beginning to
identify, document,
and measure
quality/performance
indicators
Data & Outcome
Driven system
with formal goals
and improvement
projects
Pursing National
Accreditation
Person Centered
Service Plan is
developed,
implemented &
includes natural
supports
Coordinated Planning
process includes
creative treatment,
supports, utilizes &
promotes natural
supports
Service Plan is
person centered,
culturally sensitive
and documents
staff training
Provider completes a
consumer
satisfaction survey
annually with results
reviewed by internal
committees.
Agency consumer
satisfaction surveys
completed annually.
Results used in a CQI
process.
Agency consumer
surveys
completed.
Information
analyzed with
implementation
for change.
Provider completes
exit interviews on
staff leaving
company.
Staff surveys are
completed annually.
Agency staff
surveys
completed.
Information
analyzed with
implementation
for change = low
staff turnover per
agency data
Implementing Best
Practice trainings for
staff
Utilizing Best Practices
for agency and has
evidence to
demonstrate
Utilizes research
based Best
Practices in
service delivery
and staff training.
Agency has ability to
produce financial
reports
Infrastructure includes
internal processes for
maintaining financial
balance. Includes
internal audits,
reviews & processes
for paybacks.
Provider reports
regarding financial
processes are
reported to the
agency
committees (CQI,
CRC, Board)
Supervision &
Training are
occurring per agency
requirements.
Supervision occurs
per the individual
plan/contract and
ensures professional
growth. Focus
ensures clinical
management.
Supervision occurs per
an individualized
plan/contract that
encourages and
promotes professional
growth. Focus
ensures clinical
management as well
as education.
Professional
Growth Plans are
developed and
implemented per
staff with goals,
timelines and
strategies.
39
Provider has
sufficient systems in
place to manage
submission of
electronic
information for
billing, data reports,
requests for
authorizations, etc.
Provider has sufficient
systems in place to
manage submission of
electronic information
for billing, data
reports, requests for
authorizations, etc.
Provider has
sufficient systems
in place to
manage
submission of
electronic
information for
billing, data
reports, requests
for authorizations,
etc.
Submission of
Incident Reports,
Restrictive
Interventions and
Level I Quarterly
reports per state
timeframes. Follow
up is minimal and no
POC required.
Provider is beginning
to identify patterns
and trends on the
utilization of
restrictive
intervention.
Interventions are
initiated to reduce
restrictive
intervention
utilization.
Provider is actively
striving to serve
consumers with
"hands-off"
approach. Data
demonstrates a
reduction in
restrictive
intervention
utilization.
Pursuing National
Accreditation
Pursuing National
Accreditation
Nationally
Accredited
Provider has a website
available.
Provider has an
interactive
website for
consumers/family
members to
explore provider
options.
Serve on
LME/MCO or state
committee
promoting reform
&/or best practice
training,
mentoring,…
Serve as
model/mentor for
other providers
Once a Provider has been enrolled into the CoastalCare provider network, a policy and
procedure review is completed. The provider must score 100% on this review and to be placed
on Provisional Profile. After 90 days of service provision, an initial review is completed. The
provider achieves Routine Profile after receiving a minimum score of 75% and stays at Routine
Profile status for up to one year. After one year of service provision, a routine monitoring
occurs. All providers with a Routine Profile are reviewed annually using the Routine Review
40
Tools, Cultural Competency Tool and the Billing Audit tool looking at 30 paid claims. After one
year of service provision and moving forward, a provider may request to increase their profile
level to Preferred, Exceptional or Gold Star Profile. In order to request a higher profile level,
the provider submits a letter of intent and completes the Self-Assessment. Information on Self
Assessments will be added as it becomes available.
Once a provider achieves Preferred Profile, monitoring occurs every two years using the
Preferred Review Tool, Cultural Competency Tool and Billing Audit Tool looking at 20 paid
claims. Once a provider achieves Exceptional Profile, monitoring occurs every three years using
the Exceptional Review Tool, Cultural Competency Tool and Billing Audit Tool looking at 15 paid
claims. Once a provider achieves Gold Star Profile, monitoring occurs every three years using
Gold Star Review Tool, Cultural Competency Tool and Billing Audit Tool looking at 10 paid
claims. After achieving these levels, the next scheduled review consists of the Domain Review
Tool, Billing Audit Tool and Cultural Competency Tool.
Focused Monitoring
Focused Monitoring is monitoring which has a particular area of focus. Focused monitoring
may be initiated based on the following but not limited to: procedural requirements, request
by DHHS, as part of a quality improvement process. Focused monitoring may include staff from
other departments within CoastalCare in conjunction with the Network Management
Departments as well as outside groups such as CFAC, DHHS, etc. Types of targeted monitoring
include but are not limited to:
Monitoring of a particular service or services across providers
Monitoring based on funding source
Follow up monitoring after the addition of a new service
Monitoring that results from a complaint
Monitoring of a particular area of concern, such as First Responder requirements,
consumer rights, incident reporting, quality of care, etc.
Network (State Funded) Provider Monitoring
Quantitative Record Review
Quantitative Record Review (QRR) of a sample of consumer medical and billing records is
completed for each provider. This process is different from the routine monitoring process
described earlier in the manual. The Quantitative Record Review process is required in order to
monitor the provision of public services in the catchment area pursuant to G.S. 122C-11. The
Quantitative Record Review assures that services billed by providers are documented according
41
to the Records Management and Documentation Manual and the Person-Centered Planning
Instruction Manual. These Manuals can be found at the following link:
http://www.ncdhhs.gov/mhddsas/statspublications/Manuals/index.htm.
A standardized review tool is used to determine adherence to requirements. The QRR consists
of a minimum of three percent (3%) of all Medicaid and State Funded (IPRS) paid claims for the
two month period prior to the review date. Other sample sizes and timeframes may be
determined if a request is made for target monitoring.
Mystery Shopping
CoastalCare values the satisfaction of consumers/family members/stakeholders with the
services provided in the CoastalCare Network. CoastalCare has various ways consumer
satisfaction is measured. This includes “mystery shopping”. The goal of this initiative would be
to gather feedback on how various CoastalCare Providers perform during random and
anonymous monitoring. This system is intended to provide information to identify the need for
additional training of Provider staff.
Changes in Qualification Status
In order to link consumers to appropriate care, CoastalCare is diligent in maintaining a provider
database with the current practice information submitted by providers.
Providers shall notify Network Management in writing within one (1) business day of any
changes in their status, including, but not limited to:
Changes in licensure status
Changes in privileging status with other accrediting organizations
Pending citations
Pending malpractice claim, etc.
Providers shall notify Network Management in writing using the PROVIDER ADD/CHANGE
FORM, located on the CoastalCare website within seven (7) days of personnel changes or
information updates. This may include but is not limited to:
Change in ownership
Change in Management
Proposed address changes
Opening of new locations
Changes in capacity
Inability to accept new referrals
Any proposed acquisitions
42
Any mergers
Any pending investigation for Medicaid fraud
Applying for Additional Services
In order for a Provider to be considered for Additional Services:
The Provider must be in “good standing”
CoastalCare has established that there is sufficient need for the service(s) ; and
The provider has submitted a CoastalCare Additional Service or Site Application with all
the required elements to their assigned Network Management Liaison. The application
and all required elements must be received within sixty (60) days of the date the
application is mailed to the provider. If it is not received in this time frame, the
Provider shall have to re-initiate the process.
CoastalCare will:
Provide technical assistance as requested, to providers interested in additional
services/sites.
Determine if there is an established need for the service(s).
Document the date the CoastalCare Additional Services or Site Application was received
and review the information to determine if the application and required documentation
is correct and complete.
Review the performance record of the provider for actions that resulted in suspension
of referrals, findings from other oversight agencies, Provider Performance Profile scores
as well as demonstration of quality and use of best practices.
Network Management will review and render a decision on the completed application
with-in forty-five (45) days.
Implementation Review
CoastalCare Network Management conducts service implementation reviews after the provider
serves CoastalCare consumers for 90 days. During this review, implementation of the newly
contracted service will be assessed. If the review identifies any out of compliance issues, a Plan
of Correction may be required.
43
Network Development Plan
CoastalCare has a formal, comprehensive and ongoing mechanism to ensure network
sufficiency. The Network Sufficiency and Development Plan is developed, reviewed and
approved annually by CoastalCare Network Development and Management Committee. The
CoastalCare Quality Management Committee provides management oversight of the plan and
reviews and approves it annually against larger system goals.
The Network Sufficiency and Development Plan is revised as needed throughout the year when
significant changes to the network occur and as data about the network becomes available.
The plan is developed and implemented based on:
o the defined scope and type of services offered
o the geographic area covered
o the linguistic and culture-based preferences of consumers
o the eligible population served
It includes strategies for developing and managing an array of mental health, substance abuse
and developmental disability services that emphasizes service quality, service access and
availability, best-practice models and maximizes sound use of available funds.
CoastalCare ensures that eligible consumers have timely and easy access to the behavioral
health and developmental disability services offered in CoastalCare geographic area.
CoastalCare also ensures that network providers have availability to meet the needs of
consumers based on intensity of need criteria.
CoastalCare develops access and availability goals using industry standards and measures the
actual performance of the network against these goals. These goals and performance data
contribute to the network sufficiency assessment and plan. CoastalCare assesses the provider
network to ensure that an adequate number of providers are available to meet the behavioral
health and developmental disability needs of eligible consumers.
44
Access & Availability Monitoring
CoastalCare measures actual performance and need for services in comparison to established
access and availability goals. This is accomplished by obtaining, reviewing and analyzing reports
from the following sources on a monthly, quarterly, or annual basis:
1. Call Center Report Emergent, Urgent, and Routine Care: This report is pulled from data
submitted by CoastalCare Call Center. It is reported monthly and includes information
for total number of consumers screened, percent scheduled within the required
timeframe, and percentage compliance with goals for emergent, urgent and routine
appointment benchmarks. The timeframes for each type of appointment are specified
by contract and the Network Sufficiency and Development Plan.
2. Call Center Assessment Appointment Capacity Data: The Call Center Assessment
Appointment Spreadsheet is a “snapshot” of provider appointment availability. The
report is completed monthly, monitoring the calendar for number of daily appointment
slots. The report indicates compliance/non-compliance with urgent and routine
timeframe benchmarks (i.e. 48 hours or 14 days). The reports are trended and reported
monthly to the Network and Development Committee.
3. Initiation and Engagement Measures: This report is pulled from paid claims data to
measure network performance for service initiation (2 services in 14 days) and
engagement (additional 2 services in the next 30 days) against the state minimum
performance measures and CoastalCare established goals.
A Provider Performance Profile is developed on a quarterly basis by the Quality
Management Department. The report includes initiation and engagement data for
individual providers in comparison to the network average and statewide goals. This
report is sent quarterly to each provider by the QM Department. Specific information
regarding Initiation and Engagement timeline requirements is included in the contract
and the Provider Performance Profile.
4. Complaint Data: Complaints involving provider access are reported monthly. This
report gives total number of complaints by provider; total substantiated complaints and
benchmark measures related to number or frequency of substantiated complaints.
5. Paid Claims data: Paid claims reports are generated by the Network Management
Department on a quarterly basis. These reports are used to monitor the total number of
consumers served, as well as the amount and type of services claimed.
45
Need/Gap Analysis
CoastalCare initiates a comprehensive process for gathering and analyzing information that
identifies needs and gaps in service capacity in its five county geographic catchment areas. The
needs/gap assessment serves as one mechanism to assess network adequacy and sufficiency.
The annual needs/gaps assessment process includes:
1. Involving consumers, consumers’ family members, community stakeholders,
CoastalCare Community and Family Advisory Committee (CFAC), CoastalCare Board of
Directors, CoastalCare Management Staff, CoastalCare Provider Council Sub-committee
and provider network participants;
2. Data collection strategies include:
a. The distribution of electronic surveys sent to network providers;
b. Surveys targeting consumers, significant community stakeholders, and CoastalCare’s
Board of Directors;
c. Community meetings where face-to-face discussions occurred; and
d. Needs Assessment forums, with a focus on gathering information from consumers
and stakeholders.
3. Geographic Information Systems to produce geo-access maps to define the service area
and populations served.
4. CoastalCare has developed mechanisms to measure and address the culturally sensitive
needs of the consumer population. CoastalCare uses the following mechanisms:
h. Annual needs/gap assessment to measure the cultural and linguistic needs of the
consumer population. The cultural and linguistic composition of the total population
is assessed during this time;
i. Obtains information/reports related to utilization and access issues which identify
linguistics and ethnicity from the Health Call Center, Utilization Management,
Customer Services, and the Care Coordination Directors;
j. Obtains reports from the interpreter services with whom CoastalCare contracts; and
k. Expands and promotes cultural diversity activities designed to increase providers’
awareness in their quest to serve our growing, culturally diverse population.
5. The assessment takes into consideration at least the following:
a. Population in the catchment area;
b. Identified gaps in the service array;
46
c.
d.
e.
f.
g.
h.
Number and variety of providers for each service;
Access and availability goals;
Service utilization rates;
The cultural and linguistic competency of existing providers;
Provision of evidence based practices and treatments;
Availability of community services to address housing and employment issues;
CoastalCare reports the results of the annual assessment to NC DMH, the Area Board and CFAC.
CoastalCare demonstrates that it is engaged in development efforts to address service gaps and
sufficiency needs identified in the assessment.
CoastalCare Network Development Action Plan
Monthly reports to the NDM Committee are used to develop strategic action plans to address
performance concerns. Once established and finalized, these reports, plans and performance
measures related to the action plan are included as part of the decision making process for the
following:
1. Network development decisions, including Request for Proposal or Request for
Information;
2. Network management decisions ;
3. Increased monitoring of network performance;
4. Contract selection decisions or revision of selection criteria;
5. Network sufficiency decisions regarding expansion or retraction of the network;
6. Revision of the access or availability goals;
7. Recommending a Quality Improvement Project to address the deficient area;
Contracts
CoastalCare must enter into Procurement Contracts with Network Providers before any services
can be authorized or paid. Network Providers are required to have a fully executed CoastalCare
Contract which lists services and approved sites prior to the delivery of services to a
CoastalCare Consumer.
The CoastalCare contract is divided into two sections: a Procurement Contract and a set of
General Conditions.
The Procurement Contract is customized for the following types of providers:
47
• Agency
• Agency: PRTF
• Agency: ICF-MR
• Agency: Innovations
• Agency: Specialized Innovations
• Licensed Independent Practitioner
• Hospital: Inpatient
• Hospital: Inpatient and Outpatient
There are three versions of the General Conditions: One for Agencies, one for Licensed
Independent Practitioners, and one for Hospitals. The General Conditions describe compliance
according to federal and state regulations and CoastalCare’s waiver participation.
All the CoastalCare contract templates have been approved by the Secretary of the Department
of Health and Human Services as required by G.S. 122C 142(a).
CoastalCare will enter into consumer-specific contracts with providers in order to meet the
needs and requirements of consumers. A provider with a consumer specific contract is not
considered to be a full member of the CoastalCare provider network and is not available as a
choice for other consumers.
The CoastalCare Provider Manual is incorporated into the contract by reference. As such, the
policies, procedures and descriptions in the manual are considered a part of the service
contract. (HN-10) Regarding employment agreements, all provider agency subcontractors are
subject to all the provisions of the original contract. The Provider Manual defines the scope of
processes, delineates procedures, provides updated information on network regulations,
benefit plan and claims processing and specifies all URAC required inclusions and exclusions.
CoastalCare excludes any contract language that restricts participating providers from
discussing treatment options and other matters relevant to consumers’ health care, or that
defines “medical necessity” in a manner that emphasizes cost/resource issues above clinical
effectiveness.
Participating Network Provider Contracts and the Provider Manual are issued annually as part
of the annual contracting process. Prior to finalizing of the annual contract, the Network
Management Contract Administrator ensures all required inclusions and exclusions are part of
the binding legal process and documents.
48
Events that may result in the reduction, suspension or termination of network participation
privileges include repeated non-performance of contract obligations without corrective action,
violations of professional standards or the commission of unlawful acts. Examples of the above
may include the following: loss of licensure, loss of credentialing, failure to maintain the
required minimum insurance coverage, substantial failure to meet the contract or service
description requirements, or findings of serious/on-going consumer health and safety
violations.
AGENCY AND LIP CONTRACTS
Provider Agency and LIP responsibilities are to:
• Review the Contract for accuracy and fully execute the Contract and return it to CoastalCare
within thirty (30) days of receipt to assure payment for services.
• Sign and have a fully executed CoastalCare Contract Amendment for any material changes to
the original Contract.
• Submit any required reports or data elements as required in the Contract to remain in good
standing.
• Submit reports as required in attachments and adhere to reporting requirements.
• Understand the obligations and comply with terms of the Contract and all requirements in the
CoastalCare Provider Manual.
• Notify CoastalCare of any prospective changes in sites, ensure that all CoastalCare
requirements are met and that any contract amendments are in place prior to delivery of
contracted services.
• Attempt to first resolve any disputes with other network providers or CoastalCare through
direct contact or mediation.
49
• Notify CoastalCare in advance of any mergers or change in ownership since it may have
implications for contract status.
Minimum Criteria and Conditions to Participate in the Network
Medicaid
All of the following requirements must be met to participate in the CoastalCare Medicaid
network:
1.
2.
3.
4.
5.
6.
7.
8.
be eligible to do business in North Carolina
have a current North Carolina license, if required for the service
have a current accreditation, if required for the service
have insurance coverage with the minimum required coverage limits
have the ability to send & receive electronic claims files
submit a correct and complete application for enrollment
be credentialed by the CoastalCare Credentialing Committee
have a fully executed Medicaid contract with CoastalCare
State Funded Network
To participate in the CoastalCare state funded network, a provider must meet requirements 1-7
above and
1. Meet CoastalCare selection criteria
2. Have a fully executed state funded contract with CoastalCare
Immediate Suspension
CoastalCare has defined the criteria and established clear procedures to utilize in order to
immediately suspend a provider as a result of significant risk to consumer health, welfare and
safety. Any circumstance or concern that may pose a significant risk to consumer health,
welfare or safety is immediately reviewed by the Medical Director. Based on that review, the
Medical Director may immediately suspend a participating provider’s participation in the
network. When suspension occurs an expedited investigation is initiated and the provider is
notified of the suspension. The provider is also notified of their right to access the CoastalCare
dispute process. For additional information, see the Problem Resolution, Disputes & Appeals
section below.
50
Criteria for Suspension based on Significant Risk to Consumer Health, Welfare, Safety
o Health- Maintaining the general condition of well being of the consumer.
o Welfare- Ensuring the physical, social, and financial conditions of the consumer
is maintained satisfactorily while under the providers’ care.
o Safety- Protection from, or not being exposed to, the risk of harm or injury.
o Abuse is:
o Medical Abuse is the improper or excessive use of treatment.
o Psychological Abuse, also referred to as emotional abuse or mental
abuse, is characterized by a person subjecting or exposing another to
behavior that is psychologically harmful.
o Physical Abuse- Injury, or other physical suffering or bodily harm.
o Sexual Abuse is the forcing of unwanted sexual activity by one person on
another, as by the use of threats or coercion or sexual activity that is
deemed improper or harmful, as between an adult and a minor or with a
person of diminished mental capacity.
o Neglect is:
o Disregard: lack of attention and due care to consumer needs, health,
welfare, safety or the requirements of service;
o Negligence: failure to act with the prudence that a reasonable person
would exercise under the same circumstances.
Training
CoastalCare determines what training opportunities are provided based on:
51
Technical assistance needs identified throughout the network in routine monitoring
Training funding availability
Survey Results
Training requests
Training opportunities identified through trending provider requests for information and
technical assistance, through provider survey, and/or through provider complaints and disputes
Assessment of additional training needs is determined every year through the Provider
Satisfaction survey process. The survey is disseminated electronically to the provider network
annually during the first quarter. As part of the survey, providers have an opportunity to
identify training needs. Additionally, providers can submit training requests via the website or
directly to the Training Coordinator, who will submit them to the Training Committee.
Additional assessment of training needs is conducted at the time of the annual training plan. At
this time, the agency solicits input from the monthly provider workgroup about training needs
or request via their completion of a training request form. All information gathered and the
criteria list located above are used as a basis for the development of the CoastalCare annual
training plan. CoastalCare may partner with Southeastern Health Education Center (SEAHEC)
and/or NC Council to negotiate training opportunities for participating providers based on
criteria listed above. CoastalCare Provider Training Opportunities
Technical Assistance
Often providers need guidance or have questions regarding the services they deliver, both
clinical and procedural. CoastalCare’s Network Management department is the avenue through
which communication with providers primarily occurs. Network Management is responsible for
disseminating important information to the provider network as well as being available to
provide technical assistance. The goal of technical assistance is ultimately to teach the provider
how to access the information that they need and occasionally to provide interpretation of
state policies and procedures. The provider community and CoastalCare’s Network
Management department have numerous options to accomplish communication and technical
assistance. Both can occur in groups or on an individual basis. CoastalCare is not required to
provide technical assistance in areas that would normally be considered standard operational
responsibilities of a provider agency or to providers that have shown by history not to be able
to assimilate previous technical assistance provided.
52
Group communication
Group communication methods are used to communicate information that affects the entire
network. They are used by CoastalCare to communicate to multiple providers at a time. They
include:
Website postings
Website postings are used to communicate information to the public at large including the
provider network. Postings can be about various topics from current events and highlights to
job postings. CoastalCare web site (insert link)
Communication Memos
Communication Memos are the specific vehicle that CoastalCare uses to communicate on the
website to the providers. These postings often include policy and procedure changes, benefit
plan information, upcoming trainings, and specific needs of CoastalCare.
Local Provider Meeting
The Local Provider Meeting is held each third Thursday of the month. The location of the
meeting is posted on the CoastalCare website as well as the meeting agenda, associated
handouts, and any training information for the previous month. The Provider Meetings are
usually attended by CoastalCare staff members. The Network Management department often
presents information at the meetings and is available to answer questions. Other departments
from CoastalCare sometimes attend to present information specific to their areas of focus. This
is the best forum for two way communication between CoastalCare and the provider network
as a group.
List Serve
At the Provider meetings, provider agency’s staffs are welcome to add their names to the
CoastalCare provider List Serve. The List Serve is a group of email addresses that CoastalCare
uses to communicate information that may be of interest or benefit to the provider community
such as training information, residential home openings, community collaborative events, and
network development information requests. To be added, contact Wendy Ramsay at
mailto:wendy.ramsay@secmh.org
Provider Orientation
53
CoastalCare provides an annual orientation to all participating providers, prior to the beginning
of the new fiscal year. The CoastalCare Contract Administrator notifies participating providers
by mail of the dates, times and location of the annual orientation opportunities. The annual
orientation opportunities are also posted on the agency website on the “provider’s page” under
training. For flexibility, two dates are scheduled within two weeks of one another. In the event
that a contract is added midyear, the Contract Administrator schedules and notifies the new
provider of an individual orientation opportunity within one month of selection and prior to the
contract begin date. The orientation training curricula includes topics determined to be
necessary for successful utilization of CoastalCare resources as well as information specific to
contracting with participating providers.
Quality Improvement Workgroup
The CoastalCare Quality Management Department facilitates a Quality Improvement
Workgroup monthly that assists providers with questions that they have about the QM
practices at their agencies. The QI workgroup meets the third Friday of every month at a host
provider agency location. Providers are encouraged to attend.
Individualized Communication
CoastalCare communicates one on one with provider agencies as well. CoastalCare assigns all
provider agencies a primary contact person within the Network Management Department. This
person is the agency’s liaison with CoastalCare. A Network Management liaison can provide an
agency with individualized assistance and problem resolution. CoastalCare Network
Management Department Liaisons are available for technical assistance tailored to an agency’s
individual needs. The liaison will make every effort to address questions directly or will
coordinate with other departments to ensure that providers receive comprehensive resolution
to questions. The provider agency’s contact person and the liaison may communicate through
all the usual means of communication such as:
Phone calls
Phone calls are welcome. Liaisons return phone calls within two business days. Provider
agencies are encouraged to direct their calls to their liaisons to best coordinate a resolution.
Emails
Emails are the most frequent form of communication. Providers are encouraged to submit their
questions electronically for a quicker response. Emails are answered within two business days.
54
CoastalCare’s CONFIDENTIAL Email
CONFIDENTIAL email is available for use by provider agencies to communicate with CoastalCare
staff when any protected healthcare information (PHI) is included in an email. CoastalCare
helpdesk will issue a password upon request.
Certified Mail
Certified Mail or receipt mail is used (and often required) by provider agencies and Network
Management. Many of the procedures involved in endorsement require submissions or
responses to be completed within a timeframe. Certified mail allows an outside party to
document receipt/delivery of mail for clear objective initiation of timeframes.
First class mail is also used for letters that do not require timeframes or receipt of delivery.
Consumer Rights and Empowerment
Rights of Consumers
Consumer rights are protected in many ways. The Customer Service Office ensures the basic
rights of consumers receiving mental health, intellectual/developmental disabilities, and
substance abuse services within the catchment area are protected. Consumers shall be
informed of their rights upon initial contact and annually thereafter. It is further the
responsibility of all behavioral healthcare providers to provide training on consumer rights, and
ensure employees are knowledgeable of and adhere to all consumer rights. An overview of
Consumer Rights rules and policies may be found at:
http://www.ncdhhs.gov/mhddsas/services/advocacyandcustomerservice/clientsrightslawrules.
htm
In accordance with 10A NCAC 27D.0201, all behavioral healthcare providers are required to
inform consumers of their rights as follows:
Written summary of consumer rights
Right to contact Disability Rights
Right to contact CoastalCare Customer Services line at 1-855-250-1539
55
Informed of rules expected to follow
Protections regarding disclosure of confidential information
Procedure for obtaining Person Centered Plan
Fee assessment
Complaint procedure
Suspension and expulsion from service
Search and Seizure
Additionally, for the consumer whose treatment/habilitation is likely to include the use of
restrictive interventions, or for consumers in a 24-hour facility whose rights may be restricted,
the consumer/guardian shall be informed of:
Goals and reinforcement structure of any behavior management system
Potential restrictions or potential use of restrictive interventions
Notifications regarding emergency use of restrictive intervention procedures
Notifications after use of restrictive interventions
As a safeguard to ensure that consumers are informed about their rights, one of the goals of
Customer Services is to provide helpful and easy to-understand information about the service
system. The Division of Mental Health, Developmental Disabilities, and Substance Abuse
Services developed the Consumer Handbook to help guide and assist individuals seeking
services and supports from the public mental health, developmental disabilities and substance
abuse service system. It includes information about how to access services, person-centered
planning, crisis services, rights and responsibilities of consumers, and helpful contacts and
resources.
This Division handbook is available via the Division website at:
http://www.ncdhhs.gov/mhddsas/services/consumerhandbook/index.htm
and on the CoastalCare website, along with CoastalCare’s Handbook at:
http://www.CoastalCarenc.org/index.php?content=consumers&catid=35
Both an online and large print version of this handbook is available at the above website.
Effective June 19, 2008, (per Communication bulletin #94) all Local Management Entities (LMEs)
and behavioral healthcare providers are required to make printed versions of the Consumer
Handbook available to consumers, family members and the general public. This handbook is in
PDF format which can easily be printed and distributed locally to ensure that all consumers
receive this information.
56
The Area Board bears the ultimate responsibility of ensuring and protecting the rights of
consumers. The board carries out this responsibility by requiring that the Area Director equally
work toward the objective of safeguarding and ensuring the health, safety, and rights of
consumers. The Area Board has also established a Human Rights Committee, which meets at
least quarterly to review information pertinent to consumer rights. The Office of Customer
Service is responsible for responding to complaints, concerns, and information requests, as well
as promoting education and information to consumers, families, agency staff, and provider
agencies on consumer legal rights.
Informed Consent
Consumers have the right to be informed in advance of the potential risks and benefits of their
treatment options. Upon service initiation, all behavioral healthcare providers are required to
obtain:
Informed written consent for treatment
Informed written consent for planned use of a restrictive intervention [27D .0303(b)]
Written consent granting permission to seek emergency care from a hospital or
physician
Informed written consent for participation in research projects
Written consent to release information [26B .0202 and .0203]
Documentation of written notice given to the individual/legally responsible person upon
admission that disclosure may be made of pertinent confidential information without
his or her expressed consent in accordance with G.S. § 122C-52 through 122C-56.
Consumers also have the right to consent to or refuse any treatment unless:
It is an emergency;
The consumer is under involuntary commitment;
Treatment is court-ordered;
The consumer is under eighteen (18) years of age, has not been emancipated, and the
consumer’s guardian or conservator gives permission for treatment.
Psychiatric Advance Directives (PAD)
In 1997 North Carolina developed a way for mental health treatment consumers to plan ahead
for mental health treatment they might want to receive if they experience a crisis and are
57
unable to communicate for themselves or make voluntary decisions of their own free will. A
statutory form for advance instruction for mental health treatment is provided by § 122C-77 of
the North Carolina General Statutes. An Advance Directive for Mental Health Treatment allows
Consumers to write down treatment preferences or instructions if they had a crisis in the future
and could not make their own mental health treatment decisions. The PAD is not designed for
people who may be experiencing mental health problems associated with aging, such as
Alzheimer’s disease or dementia. To address these issues, a general health care power of
attorney is used.
A Psychiatric Advance Directives Document can include a person’s wishes about medications,
ECT, or admission to a hospital, restraints, and whom to notify in case of hospitalization. The
PAD may include instructions about paying rent or feeding pets while the consumer is in the
hospital. The consumer could also put in an advance instruction “please call my doctor or
clinician and follow his/her instructions.” That way if they are in an emergency room and
unable to speak for themselves or confused, these instructions can be used as a means to help
them at vital moments.
The consumer must sign the Advance Directive for mental health treatment in the presence of
two (2) qualified witnesses. The signatures must be acknowledged before a notary public. The
witnesses may not be the attending physician, the mental health treatment provider, an
employee of the physician or mental health treatment provider, the owner or employee of a
health care facility in which the consumer is a resident, or a person related to the consumer or
the consumer’s spouse. The document becomes effective upon its proper execution and
remains valid unless revoked.
If you are assisting a consumer in completing a Psychiatric Advance Directive, plan on several
meetings to thoroughly think about crisis symptoms, medications, facility preferences,
emergency contacts, and preferences for staff interactions, visitation permission, and other
instructions.
Upon being presented with a Psychiatric Advance Directive, the physician or other provider
must make it a part of the person’s medical record. The attending physician or other mental
health treatment provider must act in accordance with the statements expressed in the
Advance Directive when the person is determined to be incapable, unless compliance is not
consistent with G. S. 122C-74(g). This statute contains the generally accepted practice
standards of treatment to benefit the consumer, availability of the treatments or hospital
requested, treatment in case of an emergency endangering life or health, or when the
consumer is involuntarily committed to a twenty-four (24) hour facility and undergoing
58
treatment as provided by law. If the doctor is unwilling to comply with part or all of the
Advance Directive he or she must notify the consumer and record the reason for
noncompliance in the patient’s medical record.
Consumers can choose someone they trust (like a family member) to make treatment decisions
for them if they cannot make the decisions themselves. This surrogate decision maker has
Health Care Power of Attorney and functions as an Agent to carry out instructions of PAD. If the
consumer does not have a PAD, the health care agent must make mental health decisions
consistent with what the agent, in good faith, believes to be the wishes of the principal. The
health care agent must be competent, at least eighteen (18) years of age, and not providing
health care to the consumer for remuneration. The agent is not subject to criminal prosecution,
civil liability, or professional disciplinary action for any action taken in good faith pursuant to an
advance instruction.
Under the Health Care Power of Attorney a person may appoint a person as their health care
agent to make treatment decisions. The powers granted by this document are broad and
sweeping and cannot be made by a doctor or a treatment provider under NC law.
The Psychiatric Advanced Directive and Health Care Power of Attorney legal forms were
designed by Duke University. They are available electronically at
http://pad.duhs.duke.edu
Confidentiality
The Network Provider is required to ensure and maintain the confidentiality of all medical
record information pertaining to all individuals served by them in the course of business. All
confidential electronic and paper medical record information must be safeguarded and
secured according to the Health Insurance Portability and Accountability Act of 1996 (HIPAA)
and all applicable federal and state confidentiality laws, rules and regulations. This is to
include 45 CFR Part 160 and 164, The Privacy Rule, and 42 CFR, Part 2 the confidentiality of
substance abuse information in medical records. Confidential information should not be
discussed, transmitted, or narrated in any form, except as authorized by the documented
signature of a competent adult being served or the individual’s legally responsible person. A
minor may authorize consent for release of confidential information under specific
circumstances as outlined in APSM 45-1, Confidentiality Rules for Mental Health,
Developmental Disabilities and Substance Abuse Services. Confidential information related to
AIDS or related conditions can only be disclosed according to applicable communicable disease
laws specified in G.S. 130A-143.
59
Secondary records, which contain information about a specific individual or individuals that
can be personally identified, shall be protected with the same safeguards and security as the
original service record. Providers shall be monitored and reviewed to ensure that they
demonstrate through specific evidence their compliance with HIPAA and other federal and
state Confidentiality laws in regard to the security and safeguarding with policy and procedure
in regard to the individual’s served Protected Health Information (PHI).
Second Opinion
Consumers have the right to a second opinion if they do not agree with their diagnosis,
treatment, or the medication prescribed. If a consumer requests a second opinion,
arrangements will be made through CoastalCare’s Clinical Operations.
Consumers are informed of their right to a second opinion in the CoastalCare Consumer
Handbook, which is made available to them at the time of their enrollment.
Your Responsibility As A CoastalCare Contracted Provider Is To:
Respect consumers’ rights at all times
Provide continual education to consumers regarding their rights, as well as support
them in exercising their rights to the fullest extent
Be knowledgeable of, and develop operational procedures to ensure compliance with,
all outlined statutes and regulations regarding consumer rights and the use of restrictive
interventions and protective devices
Maintain an ongoing knowledge of changes to the statutes and regulations and
immediately alter operations to meet changes
Provide information the consumer needs in order to decide among all relevant
treatment options
Provide information to the consumer about the risks, benefits, and consequences of
treatment or non-treatment options
Provide information to the consumer about their right to participate in decisions
regarding their healthcare, including the right to refuse treatment, and to express
preferences about future treatment decisions
Be aware that requesting a second opinion is a right of all consumers and refer the
consumer to contact the toll free CoastalCare Customer Service number if a second
opinion is requested
60
CoastalCare’s Responsibility To Providers Is To:
Develop and disseminate educational material related to accessing services, consumer
rights and protection
Reductions, Denials, Suspensions or Termination of Medicaid Services
It is very important that providers understand the following rights so they may support the
consumer’s request or make the request on the consumer’s behalf (must show written
consent.) If the treating physician/practitioner/provider would like to discuss the case with the
CoastalCare UM care manager or the physician, please call one of the CoastalCare Business
numbers.
There are times when a consumer’s request for services is denied, and there are times when a
current service is changed (i.e. terminated, reduced or suspended) by CoastalCare Utilization
Management.
Denial
A denial could occur if the criteria are not met to support a new authorization request for a
service. Consumer/guardian will receive a letter by US Mail explaining this decision and how to
request a Reconsideration Review. During this time, CoastalCare will not provide the requested
service in dispute.
Reductions, Suspension, or Termination
Services that a Consumer is currently receiving may be reduced, suspended or terminated
based on several different factors including not following clinical guidelines or not continuing to
meet medical necessity for the frequency, amount, or duration of a service. Consumer/guardian
or authorized representative will receive a letter by US Mail at least 10 days before the change
occurs explaining how to request a reconsideration. If consumer/guardian or authorized
representative requests reconsideration by the deadline stated in the letter, the services may
continue through the end of the original authorization.
EXCEPTION: Decisions involving a reduction, termination or suspension of services
In order to continue with existing services during an Appeal review and/or Appeal
Process, the consumer/guardian/authorized representative must request Appeal within
10 days of the date of the Notice of Decision Letter.
61
The services will then continue until the end of the original authorization period as long
as the Consumer remains Medicaid eligible. This right to receive services applies even if
the consumer changes providers.
The service will be provided at the same level the Consumer was receiving the day before
the decision or the level requested by Consumer’s provider, whichever is less. The
services that continue must be based on Consumer’s current condition and must be
provided in accordance with all applicable state and federal statutes and rules and
regulations. (See note on consumer/guardian responsibility for payment if adverse
decision is upheld by DHHS.)
**This does not apply for the denial of an initial service request**
Due Process for Medicaid Decisions
Detailed information about Due Process and Prior Approval Procedures can be accessed via the
Division of Medical Assistance (DMA) website. (See the Resources & Web Links section at the
end of this Manual for website links.)
Appeal Level I
Under The North Carolina MH/DD/SAS Health Plan 1915(b) and NC Innovations Waiver 1915(c)
all persons who do not agree with CoastalCare’s Notice of Decision on a request for Medicaid
services are entitled to Appeal through the CoastalCare Appeal process. To begin the process,
an appeal must be filed within 30 days of the date of the Notice of Decision.
To request an appeal review, the appeal request must be completed and returned by fax, mail
or in person.
Consumer/guardian or authorized representative has the right to review any information used
as part of the Appeal process.
A CoastalCare Appeal Review is a local impartial review of CoastalCare’s decision to reduce,
suspend, terminate or deny Medicaid services. A health care professional who has appropriate
clinical expertise in treating the Consumer’s condition or disorder, and who was not previously
involved in CoastalCare’s initial decision, determines the Appeal Decision.
It can take up to 45 days from the date the Request for Appeal is received for a decision to be
made by the LME.
The consumer/guardian/authorized representative must complete the local appeal process
with CoastalCare before requesting a hearing with the Department of Health and Human
Services (DHHS) and Office of Administrative Hearing (OAH.)
Steps to File an Appeal Request
To request an CoastalCare Appeal, the consumer/guardian/authorized representative and/or
the provider (in making the request on the consumer’s/guardian’s behalf or supporting the
62
consumer’s/guardian’s request with written consent) must complete and return the
CoastalCare Appeal Review Form by one of the following methods:
Calling one of the CoastalCare Business Numbers: 910-550-2600; or toll free 1-855-250-1539
Fax to 910-550-2665
Mail or deliver in person to:
Quality Management
Appeals Specialist
CoastalCare
2023 S. 17th Street
Wilmington, NC 28403
Upon completion of the appeal decision, if the consumer/guardian disagrees with the
CoastalCare appeal decision, the consumer/guardian/authorized representative can then
appeal the decision to both DHHS and OAH by filing a Request for Hearing, also known as the
State Fair Hearing process.
Expedited Appeal Review Process
An Expedited Appeal Review may be requested by the consumer/guardian (or the provider in
making the request on the consumer’s/guardian's behalf or supporting the
consumer’s/guardian's request), if it is indicated that taking the time for a standard Review
could seriously jeopardize the consumer’s life, health or ability to attain, maintain, or regain
maximum function.
If an expedited request is received, it is reviewed to determine if there is sufficient evidence to
support the need for this type of request. If so, an Appeal Review will be completed within 72
hours and the consumer will be notified of the decision.
If there is not sufficient evidence to require an expedited request, the consumer/guardian will
receive verbal notice of the denial of their request for an expedited appeal review and written
notice within 2 days and the process will follow the normal appeal timelines.
Mediation - Level II
Once the Appeal is processed, OAH or The Mediation Network of North Carolina will contact
the consumer/guardian to offer an opportunity to mediate the disputed issues in an effort to
resolve the pending appeal informally. If the consumer/guardian accepts mediation, it must be
completed within 25 days of the request.
63
If the issues are resolved at mediation, the appeal will be dismissed and services will be
provided pursuant the Mediation Agreement. If consumer/guardian does not accept the offer
of mediation or the results of mediation, the case will proceed to a hearing and will be heard by
an Administrative Law Judge with the Office of Administrative Hearings. This is referred to as
the state Fair Hearings process.
Appeal/Hearing - Level III
Consumer/guardian must file an appeal with the NC Office of Administrative Hearings (OAH),
Department of Health and Human Services and CoastalCare within 30 days from the date of the
Appeal decision to the addresses listed on the form.
This state level hearing is conducted by an Administrative Law Judge (ALJ) at the Office of
Administrative Hearings (OAH.) The hearing is scheduled to occur by telephone unless
consumer/guardian requests to attend in person. Consumer/guardian will receive notice of the
date, time and location of the hearing. The hearing will be scheduled at the
consumer’s/guardian’s convenience in a location close to the consumer/guardian.
If there are questions, the consumer/guardian may call the NC Department of Health & Human
Services (DHHS) Division of Medical Assistance Appeals Unit toll-free at 1-800-662-7030 or at
919-855-4260. Ask for the call to be transferred to the DMA Appeals Unit, Clinical Policy and
Programs. To learn more about the appeals process, contact the North Carolina Office of
Administrative Hearings at 919-431-3000.
Final Agency Decision - Level IV
In the past, the North Carolina Department of Health and Human Services reviewed the
administrative law judge’s recommendation and made the final decision. During the last
Session of the General Assembly, legislation was passed that would make the decision of the
Administrative Law Judge the Final Agency Decision. However, that change in law appears to
conflict with federal Medicaid regulations, so the State has asked the federal Centers for
Medicare and Medicaid Services for a ruling. That ruling has not yet been issued, so at the
moment, it is not clear which agency will make the Final Agency decision.
Regardless of which State agency makes the Final Agency Decision, if the consumer/guardian
disagrees with the Final Agency Decision, they may retain an attorney and ask for a judicial
review in Superior Court.
64
If the final resolution of the Appeal is not decided in the consumer’s/guardian’s favor, (meaning
CoastalCare’s or DHHS’s action was upheld), CoastalCare may recover the cost of the services
furnished to the consumer/guardian while the Appeal is pending.
Non-Medicaid Service Appeal Process
Non-Medicaid services are not an entitlement. Non-Medicaid Service Decisions regarding
termination, reduction, suspension or denial of Non- Medicaid services are handled within the
Utilization Management Department. If consumer/ guardian disagree with the Non-Medicaid
Service Decision, s/he or authorized representative may fill out the Non-Medicaid Appeal form
that accompanies the decision and return it to the CoastalCare Quality Management
Department within 15 working days of the date of the non-certified notification letter.
The Clinical Support Department acknowledges receipt of the grievance in writing via a letter to
the appellant dated the next working day following receipt.
The Non-Medicaid Service Appeal process maintained by CoastalCare provides an opportunity
for the consumer, guardian, and authorized representative, ordering/treating provider and/or
facility rendering service to submit information related to the case, including any documents,
records, written comments, or other information that may be helpful in processing the appeal.
Peer Reviewers who process the appeal consider all the information received from the
consumer, guardian, and authorized representative, ordering/treating provider and/or facility
rendering service, regardless of whether the information was presented during the initial
clinical review.
Consumer/guardian/authorized representative will receive a Clinical Review Decision
conducted by a health care professional that has appropriate clinical expertise in treating the
consumer's condition or disorder within appropriate timeframes.
Timeframes for the appeal process, which are in accordance with the requirements of the NC
Division of Mental Health/Developmental Disabilities/Substance Use Services (DMH/DD/SAS)
and URAC--the external accrediting body--are documented in CoastalCare policies and
procedures and are available upon request to any consumer/guardian, provider or facility
rendering service.
65
If the appeal decision is to uphold the original non-certification, the written notification will
explain that there is an opportunity to appeal the decision to the Division’s Non-Medicaid
Appeals Panel, as well as the process for doing so.
Non-Medicaid Appeal Request to DHHS
If consumer/guardian/authorized representative disagrees with the Non-Medicaid Service
Decision, s/he may submit the Non-Medicaid Appeal Request Form to the Division of Mental
Health, Developmental Disabilities and Substance Abuse Services (DMH/DD/SAS.)
The internal CoastalCare Non-Medicaid Service Appeal process must be completed prior to
filing the Appeal Request form with the Division. The DMH/DD/SAS hearing office must receive
the consumer’s appeal within 11 calendar days from the date on the CoastalCare Non-Medicaid
Service Decision Clinical Review Notification Letter [N.C.G.S. 143B-147(a) and 10A NCAC 271
.0600-.0609]. If the 11th day falls on a weekend or holiday, the deadline is the next business
day. A verbal appeal is not acceptable.
The Non-Medicaid Appeal Request is reviewed by a panel of individuals designated by the
Division of Mental Health, Developmental Disabilities, and Substance Abuse Services
(DMH/DD/SAS.) The panel will issue their findings and decisions within 60 days of receipt of the
Appeal Request form to both the consumer/guardian and CoastalCare Executive Director.
Upon receipt of the panel’s findings and decisions, CoastalCare will issue a final decision based
on those recommendations in writing within 10 days. This decision is final and there are no
further appeal rights as set forth in NC GS 143B-147(a)(9). (See first paragraph under Final
Agency Decision - Level IV heading above.)
Receiving Services during the Non-Medicaid Appeal Process
CoastalCare has the option of authorizing other Non-Medicaid Services that are appropriate.
Services may be authorized for the duration of the Appeal Decision process at the discretion of
CoastalCare. Other community resources may also be referred to the consumer for support.
When a consumer/guardian/authorized representative files an Appeal for the denial of a new
service, CoastalCare is under no obligation to provide the requested service during the review
process.
Consumer and Family Advisory Committee (CFAC)
The CoastalCare Consumer & Family Advisory Committee (CFAC) is a committee mandated by
state law and established to review, comment, and make recommendations on the content and
66
delivery of Behavioral Health Services in its own service area. Membership consists of
Consumers and Family Members of Consumers who receive Mental Health, Substance Abuse
and Intellectual/Developmental Disability Services. CFAC members may serve for a maximum of
two (2) consecutive three (3) year terms. The CoastalCare CFAC has twenty-one (21) member
positions and represents all five (5) counties in the CoastalCare service area,in all three (3)
disability areas. The CFAC is a self-governing committee operating under its own by-laws,
membership rules, and Procedures. CFAC serves as an advising committee to the CoastalCare
Board of Directors and CoastalCare’s Executive Administration.
Mission Statement: The Consumer & Family Advisory Committee, which represents and
advocates for all Consumers and Families within the service areas of CoastalCare, has a mission
to ensure that all consumers have access to, and receive, the best available quality services.
Vision Statement: The Consumer/Family Advisory Committee envisions a working and effective
partnership with Coastal Care that will ensure that the voices of Consumers and their Families
will always be heard and considered, forming the basis of decisions made by CoastalCare to
create positive changes and to establish availability of continuing evidence-based practices.
Some of the ways in which CFAC ensures that Consumers and Families remain involved in
oversight, planning, and improvement of services managed by CoastalCare are by:
Membership on, contact with, and monthly reporting to the CoastalCare Board of
Directors.
CFAC representation and input on Coastal Care’s Operational Committees as follows:
o Network Management & Development
o Quality Improvement Committee
o Customer Service & Call Center Committee
o Community Coordination Committee
o Clinical Advisory Committee
As a self-governing committee comprised of Consumers of services and their families,
CoastalCare’s CFAC has been a strong voice at CoastalCare, and in the community. Members
are very active as advocates for higher quality care and are responsible for developing positive
CFAC initiatives, always in close collaboration with CoastalCare staff and key community
stakeholders.
67
CoastalCare has enjoyed a strong and mutually supportive relationship with its CFAC, and has
come to rely upon its recommendations. This ongoing and constructive interaction has often
resulted in important modifications and/or expansions of care in the service array through
input from consumers and family members by means of recommendations identified in a
comprehensive gaps and needs analysis. The CFAC meets every month on the third (3rd)
Tuesday of the month. All meetings are open to consumers, family members, and the general
public. There is time allotted for public comment and questions to the Committee, and all
meeting minutes are recorded, transcribed, and made available on CoastalCare’s Website
athttp://www.CoastalCareNC.org . Any consumer, family member, Provider, or member of the
general public may bring questions or any issues of concern to the CFAC’s attention by
attending any of the monthly CFAC meetings, or by sending an email directly to any individual
CFAC members. Contact may also be made by contacting the CoastalCare CFAC Liaison, at 910459-4840 orJo.Warwick@CoastalCareNC.org .
*If providers know of individual consumers or family members that would like to serve on this
committee, they may advise or assist them by calling the CFAC Liaison, or by visiting
CoastalCare’s Website for access to the application for membership.
Benefit Package
Eligibility
The Provider must not employ any policy or practice that shows discrimination against
enrollees on the basis of race, color, or national origin.
Who Is Eligible for the Medicaid Waivers?
The following must be met for an individual to be eligible for acceptance in the Waiver:
Individuals must have Medicaid in a “covered eligibility group.” Covered eligibility groups
include the following:
Individuals covered under Section 1931 of the Social Security Act (TANF/AFDC)
Optional Categorically and Medically Needy Family and Children not in Medicaid
Deductible Status (MAF)
Blind and Disabled Children and Related Populations (SSI) (MSB)
Blind and Disabled Adults and Related Populations (SSI) (Medicare)
68
Aged and related populations (SSI) (Medicare)
Medicaid for the Aged (MAA)
Medicaid for Pregnant Women (MPW)
Medicaid for Infants and Children (MIC)
Adult Care Home Residents (SAD) (SAA)
Foster Care Children and Adoption
Participants I Community Alternatives Programs (CAP/DA) (NC Innovations) (CAP-C)
(CAP-MR/DD
Medicaid recipients living in ICF-MR facilities
Work First Family Assistance AAF)
Refugee Assistance (MRF) (RRF)
Medicaid County of Residence: Brunswick, Carteret, Onslow, New Hanover, or Pender
Eligibility for individuals meeting the criteria listed above is mandatory and automatic. Children
become eligible the first day of the month following their third birthday for 1915(b) services,
but can be eligible from birth for 1915(c).
The NC Innovations Waiver (1915 c Waiver):
NC Innovations Home and Community Based Waiver 1915 (c) may be enrolled at an earlier age.
A person with mental retardation (intellectual disability) and/or a related developmental
disability may be considered for Innovations funding if all of the following criteria are met:
The individual is eligible for Medicaid benefits based on assets and income of the
applicant whether he/she is a child or an adult
The individual meets the requirements for ICF-MR level of care as determined by the
CoastalCare Utilization Management Department. (Refer to the NC Innovations
Operations Manual for the ICF-MR criteria)
Lives in an ICF-MR facility or is at high risk for placement in an ICF-MR facility
High risk for ICF-MR institutional placement is defined as a reasonable indication that
individual may need such services in the near future (one moth or less) but for the
availability of home and community based services.
The individual’s health, safety, and well-being can be maintained in the community with
waiver support
The individual requires Innovations Waiver services
The individual, his/her family, or guardian desires participation in the Innovations
Waiver program rather than institutional services
69
For the purposes of Medicaid eligibility, the person is a resident of one of the five
counties within the CoastalCare region Brunswick, Carteret, Onslow, New Hanover, and
Pender counties.
The individual will use one Waiver service per month for eligibility to be maintained.
Effective April 1, 2010, new NC Innovations participants must live with private families
or in a living arrangement with six or fewer persons unrelated to the owner of the
facility .
Qualifies for the Innovations Waiver and has been assigned a “Waiver” slot.
Medicaid Waiver Dis-enrollment
When an enrollee changes county of residence for Medicaid eligibility to a county other than
Brunswick, Carteret, New Hanover, Onslow, or Pender; the individual will continue to be
enrolled in The NC MH/DD/SA Health Plan until the disenrollment is processed the by the
Eligibility Enrollment System at the state. Disenrollment due to a change of residence is
effective at midnight on the last day of the month. An enrollee will be automatically disenrolled from the NC MH/DD/SAS Health Plan if the following occurs:
The individual moves to a county other than the CoastalCare counties
The individual is deceased
The individual is admitted to a correctional facility for more than thirty (30) days
The individual no longer qualifies for Medicaid or is enrolled in an eligibility group not
included in the NC MH/DD/SAS Health Plan or NC Innovations 1915 (b) (c) Waivers
The individual is admitted to a state facility with more than sixteen (16) beds
Eligibility for State Funded Services
Enrollees that do not have Medicaid may be eligible for state funded services based on their
County of residence and level of need. A consumer who meets eligibility requirements can be
denied services based on inability to pay. State Funded Services are not an entitlement.
CoastalCare and other LME/MCOs are not required to fund services beyond the resources that
are available to them. There are also some services, including most residential services for
adults that are not reimbursed by Medicaid. Therefore enrollees who receive Medicaid may
also receive state funded services, based on their individual needs and availability of funding.
CoastalCare maintains a Registry of Unmet Needs to track requests for state funding/nonemergency services that have not been met.
Eligibility for Reimbursement by CoastalCare
Consumers who have their services paid for in whole or in part by CoastalCare must be enrolled
in the CoastalCare system. If you have any questions about a consumer’s eligibility, please call
70
the Customer Services line at 1-888-581-9988. Medicaid and state funds should be the payment
of last resort. It is necessary that all other funding options be exhausted first.
Enrollees with a Medicaid card from Brunswick, Carteret, New Hanover, Onslow or Pender
counties are fully enrolled in the Coastal Care system and are eligible to receive Basic Benefit
Services, Basic Augmented Services or Enhanced Benefit Services which have been authorized
by CoastalCare. Medicaid regulations prohibit the use of Medicaid funds to pay for other than
General Hospital Care delivered to inmates of public correctional institutions, and Medicaid
funds may not be used to pay for services provided for enrollees in facilities with more than 16
beds that are classified as Institutions of Mental Diseases (IMD). IMD’s are hospitals such as the
State Facilities because they have more than 16 beds and are not part of a general hospital.
Enrollees with private or group insurance coverage are required to pay the co-pay assigned by
their insurance carrier.
NOTE: Provider contracts specify the funding source available for Provider billing. Providers
should know if they have been contracted for Medicaid, State Services or both. If you have
questions, please contact your assigned Provider Relations Representative.
Enrollment of Consumers
It is important for all providers to assure consumer enrollment data is up-to-date based on the
most current CoastalCare Enrollment Procedures and training. These documents can be found
in the NC MH/DD/SAS Health Plan Operations Manual and/or the CoastalCare website at
http://intranet.secmh.org/. If enrollment data is not complete prior to service provision,
authorizations and claims may be affected. Denial of authorizations requested and/or claims
submitted for reimbursement may result from incomplete enrollment data. (See Section IX
Finance for additional information).
Service Eligibility: Services are divided into multiple service categories:
Basic Services :
The Basic Benefit package includes those services that will be made available to
Medicaid-entitled individuals and, to the extent resources are available, to nonMedicaid individuals. These services are intended to provide brief interventions for
individuals with acute needs. The Basic Benefit package is accessed through a referral
from CoastalCare to an enrolled CoastalCare provider. Once the referral is made, there
are no prior authorization requirements for basic services. Referred individuals can
access a minimum of eight (8) visits for Adults ages 21 and up and sixteen (16) visits for
Children and Adolescents below age 21.
Basic Augmented Services:
71
The Basic Augmented Benefit package includes those services that will be made
available to Medicaid-entitled individuals and, to the extent resources are available, to
non-Medicaid individuals meeting Target Population criteria. An Enrollee requiring this
level of benefit needs additional services than the automatically authorized eight (8) or
sixteen (16) visits in order to maintain or improve his/her level of functioning. An
Authorization for the services is available for this level and will need to be requested
through the CostalCare Utilization Management Department. Authorization is based on
the Enrollee’s need and medical necessity criteria for the service requested.
Enhanced Services:
The Enhanced Benefit package includes those services that will be made available to
Medicaid-entitled individuals and, to the extent resources are available, to nonMedicaid individuals meeting Target Population criteria. Enhanced Benefit services are
accessed through a person centered planning process. Enhanced Benefit services are
intended to provide a range of services and supports, which are more appropriate for
individuals seeking recovery from more severe forms of mental illness, substance abuse
and intellectual and developmental disabilities with more complex service and support
needs as identified in the person-centered planning process. The person-centered plan
also includes both a proactive and reactive crisis contingency plan. Enhanced
servicesinclude those services that are comprehensive, more intensive, and may be
delivered for a longer period of time. An individual may receive services to the extent
that they are not identified as necessary through the person-centered planning process
and are not duplicated in the integrated services offered through the Enhanced Benefit
(e.g., AssertiveCommunity Treatment). The goal is to assure that these individuals’
services are highly coordinated, reflect best practice and are connected to the personcentered plan authorized by CoastalCare.
Target Populations:
Target Population designation is for State funded services, it does not apply to enrollees
who are only receiving Medicaid services. The Provider, through review of screening,
triage and referral information and their assessment, must determine the specific Target
Population for the enrollee according to the Division of MH/DD/SAS Criteria. Each Target
Population is based on diagnostic and other indicators of the enrollee’s level of need. If
the MH/DD/SAS system does not serve these individuals, there is no other system that
will. The MH/DD/SAS system is a public safety net and its resources will be focused on
those most in need.
72
To see the most current version of the Target Population Criteria, go to the IPRS
Website link on the NC Division of MH/DD/SAS home
page:http://www.ncdhhs.gov/mhddsas/iprsmenu/index.htm
Service Definitions
The regulations of a 1915 (b) waiver require that all NC Medicaid State Plan services be
available under the 1915 (b) waiver. When the NC State Medicaid Plan changes the services
covered under the NC MH/DD/SAS Health Plan will also change.
Service Array
For a listing of services, please refer to the most current version of the service arrays by benefit
level and disability. For Mental Health, Substance Abuse and Developmental Disabilities, further
detail can be found in the North Carolina Mental Health/Developmental Disabilities/Substance
Abuse Services Health Plan Operations Manual. For the NC Innovations Waiver, further detail
can be found in the NC Innovations Technical Manual.
Hospital Admissions
Medicaid consumers hospitalized on or after the effective date of enrollment by CoastalCare
will receive authorization for all covered services, including inpatient and related inpatient
services, according to Medical Necessity requirements. CoastalCare shall provide authorization
for all inpatient hospital services to consumers who are hospitalized on the effective date of
disenrollment (whether voluntary or involuntary) until such consumer is discharged from the
hospital.
Medicaid Transportation Services
Transportation services are among the greatest needs identified to assist consumer in accessing
care. It is PBH’s goal to assist consumers in accessing generic public transportation. Providers
are requested to assist in meeting this need whenever possible. The Department of Social
Services in each county has access to Medicaid approved transportation. Transportation is for
medical appointments or getting prescriptions at the drug store. Riders have to call two (2) to
four (4) days ahead to arrange a ride. There is no fee for consumers who are enrolled in
Medicaid. For those who are not enrolled in Medicaid, transportation depends on available
space, and there is a fee.
For information on available transportation in your county please contact the local DSS
http://www.ncdhhs.gov/dss/local/
73
There are no special publically funded medical transportation services in the evening and on
weekends.
CoastalCare Clinical Design Plan
Access, Enrollment and Authorization of
Services
Accessing Routine Services
CoastalCare’s Access Standard for Routine Services is to arrange for services within 7 calendar
days of contact with the Call Center. The geographic access standard for services is 30 miles or
30 minutes driving time in urban areas, and 45 miles or 45 minutes driving time in rural areas.
Enrollment and Referral Process for Routine Needs
1. A resident of CoastalCare’s catchment area calls the 1-866-875-1757 Call Center number
for a referral for services.
2. A consumer’s clinical need may be considered ROUTINE if, but not limited to, an
indication that the consumer meets criteria for the presence of a benefit plan eligible
DSM-IV TR Axis I or II disorder, and the consumer does not meet criteria for an
emergent or urgent response.
3. The Call Center Clinician will search for the consumer in AlphaMCS. If the consumer is
not found in AlphaMCS, the Call Center Clinician will collect and enter the initial
enrollment information on the consumer via the AlphaMCS Enrollment Form, which
contains information from the State mandated Screening, Triage, and Referral tool. If
the consumer is found in AlphaMCS, the Call Center Clinician will update any changes in
demographic information.
4. The Call Center Clinician will assess the consumer’s clinical needs by completing the Call
Center’s Triage Assessment Tool to ensure the consumer is referred to the appropriate
level of service.
74
5. The Call Center Clinician will offer the consumer a choice of three (3) providers (when
available) based on the consumer’s clinical needs, preference in provider
specialty/cultural competency, service availability, and proximity to the consumer.
6. The Call Center Clinician will schedule an appointment with the consumer’s chosen
provider through the provider’s AlphaMCS calendar. If an appointment is not available
within seven (7) calendar days of the chosen provider, the consumer may choose
another provider.
7. If the Call Center Clinician began completing the AlphaMCS Enrollment Form, they will
“hand over” the enrollment form to the chosen provider. The provider will be able to
view the enrollment form in the AlphaMCS Provider Portal and will complete all
required enrollment information, including documentation of Medicaid enrollment or
ability to pay information, as well as completing the “Additional Clinical Page” upon
conducting the assessment. The provider will then submit the completed enrollment
form to CoastalCare’s Enrollment and Eligibility Specialist for review of completeness,
accuracy, and verification of insurance eligibility.
8. The Call Center Clinician will also provide the chosen agency with the Call Center’s
completed Triage Assessment Tool for that consumer through a secure electronic file to
ensure the provider is informed of the clinical needs of the consumer at the time of the
call.
9. The Call Center Clinician will follow up with the consumer within three (3) business days
of the appointment if the chosen provider has indicated through the AlphaMCS Provider
Portal that the consumer did not show or cancelled the appointment. Follow up will
continue and will be documented in AlphaMCS until the Call Center Clinician has
ensured that the consumer has been able to receive the care that is most appropriate to
meet their clinical needs.
CoastalCare Network Providers are held to the following DMA standard regarding Appointment
Wait Time for ROUTINE Referrals: Scheduled -within one hour; Walk-in-within two hours.
Accessing Urgent Services
CoastalCare’s Access Standard for Urgent Services is to arrange for services within 48 hours of
contact with the Call Center. The geographic access standard for services is 30 miles or 30
minutes driving time in urban areas, and 45 miles or 45 minutes driving time in rural areas.
Enrollment and Referral Process for Urgent Needs
75
1. A resident of CoastalCare’s catchment area calls the 1-866-875-1757 Call Center number
for a referral for services.
2. If the consumer calls any other CoastalCare number, and the call is determined URGENT,
that call is immediately transferred to a Call Center Clinician via a “warm transfer”
(Consumer remains on the line without being placed on hold.)
3. A consumer’s clinical need may be considered URGENT if, but not limited to the
following:
Consumer has moderate risk of harm to self or others (e.g. demonstrated risk
factors with offsetting protective factors such as suicidal ideation without intent
and presence of community supports).
Consumer is demonstrating decompensation in functioning due to presence of
psychiatric disorder, however, is not currently at imminent risk.
Consumer of major recent environmental risk factor(s)/stressor(s) that increase
the likelihood of decompensation in functioning due to presence of psychiatric
disorder (e.g. death, serious trauma, major loss to support system).
Consumer is using substances, likely meets criteria for treatment, and is
amenable to same.
Consumer is being released from incarceration and is in need of receiving follow
up for treatment of a psychiatric illness.
Consumer is being discharged from a community hospital, state hospital, or
other crisis service.
Consumer has a risk of loss of current stable living environment that is not
immediate.
4. The Call Center Clinician will search for the consumer in AlphaMCS. If the consumer is
not found in AlphaMCS, the Call Center Clinician will collect and enter the initial
enrollment information on the consumer via the AlphaMCS Enrollment Form, which
contains information from the State mandated Screening, Triage, and Referral tool. If
the consumer is found in AlphaMCS, the Call Center Clinician will update any changes in
demographic information.
5. The Call Center Clinician will assess the consumer’s clinical needs by completing the Call
Center’s Triage Assessment Tool to ensure the consumer is referred to the appropriate
level of service.
6. The Call Center Clinician will offer the consumer a choice of three (3) providers (when
available) based on the consumer’s clinical needs, preference in provider
specialty/cultural competency, service availability, and proximity to the consumer.
However, the Call Center Clinician may determine that referral to Mobile Crisis
Management or to a Crisis Response Center is more appropriate depending on the
consumer’s clinical needs.
76
7. The Call Center Clinician will schedule an appointment with the consumer’s chosen
provider through the provider’s AlphaMCS calendar. If there are no appointments
available within 48 hours, the Call Center will offer the consumer an assessment by
walking in to the chosen provider’s office between 8:00am-3:00pm.
8. The Call Center Clinician will reiterate to the consumer that CoastalCare’s Call Center is
available 24 hours a day and advice the consumer to contact the Call Center at any time
should their situation escalate and require an emergent referral.
9. If the Call Center Clinician began completing the AlphaMCS Enrollment Form, they will
“hand over” the enrollment form to the chosen provider. The provider will be able to
view the enrollment form in the AlphaMCS Provider Portal and will complete all
required enrollment information, including documentation of Medicaid enrollment or
ability to pay information, as well as completing the “Additional Clinical Page” upon
conducting the assessment. The provider will then submit the completed enrollment
form to CoastalCare’s Enrollment and Eligibility Specialist for review of completeness,
accuracy, and verification of insurance eligibility.
10. The Call Center Clinician will also provide the chosen agency with the Call Center’s
completed Triage Assessment Tool for that consumer through a secure electronic file to
ensure the provider is informed of the clinical needs of the consumer at the time of the
call.
11. The Call Center Clinician will follow up with the consumer within one (1) business day of
the appointment if the chosen provider has indicated in the AlphaMCS Provider Portal
that the consumer did not show or cancelled the appointment. Follow up will continue
and will be documented in AlphaMCS until the Call Center Clinician has ensured that the
consumer has been able to receive the care that is most appropriate to meet their
clinical needs.
12. If a consumer requires an urgent referral, the consumer is referred to a provider
regardless of funding status (Medicaid, Medicare, Insurance, etc.)
CoastalCare Network Providers are held to the following DMA standard regarding Appointment
Wait Time for URGENT Referrals: Scheduled Appointment -within one hour; Walk-in - within
two hours.
Accessing Emergent Services
CoastalCare’s Access Standard for Emergency Services is two (2) hours or immediately, for lifethreatening emergencies. The geographic access standard for services is 30 miles or 30 minutes
driving time.
77
In potentially life-threatening emergencies, the consumer’s safety and well-being has priority
over administrative requirements. Eligibility verification will be deferred until the consumer
receives appropriate care.
Enrollment and Referral Process for Emergent Needs
1. A resident, family member or CIT officer of CoastalCare’s catchment area calls the 1866-875-1757 Call Center number for a referral for services.
2. If the caller calls any other CoastalCare number, and the call is determined EMERGENT,
that call is immediately transferred to a Call Center Clinician via a “warm transfer”
(Consumer remains on the line without being placed on hold.)
3. A consumer’s clinical need will be considered EMERGENT and will result in a “warm
transfer” for an immediate Medical or Public Safety Referral if the consumer reports any
of the following:
Consumer is at acute risk of harming self or others, or of being harmed by
others, and there is an imminent risk of death.
Complaints of physical symptoms suggesting life-threatening conditions (e.g.
chest pain) or conditions requiring medical attention (e.g. physical injury,
overdose).
Consumer is in possession of a firearm, other lethal weapon, or other lethal
means with intent to use it and refuses immediate assistance.
Consumer is exhibiting current or high risk of withdrawal symptoms that require
immediate medical intervention (e.g. alcohol, barbiturate, or benzodiazepine
withdrawal). Such symptoms may include history of recent seizures, tactile
disturbances (itching, bugs crawling, pins, burning sensations), auditory
disturbances, visual disturbances (e.g. light sensitivity, seeing things not there),
headache, disorientation to date or situation.
Consumer is experiencing acutely psychotic symptoms, is engaging in risky
behavior, and is refusing community crisis response.
Consumer is in immediate danger of harm by someone else.
Family member or other party is reporting that a person is in immediate danger.
4. A consumer’s clinical need will be considered EMERGENT and will result in a “warm
transfer” for a Community Crisis Response (i.e. Mobile Crisis Management or Crisis
Response Center) if the consumer reports any of the following:
Consumer is at acute risk of harming self or others, or of being harmed by
others, but there is no imminent risk of death (e.g. suicidal ideation with intent
and means, but agreeable to safety plan).
78
5.
6.
7.
8.
Consumer is unable to care for self or is engaging in high risk/dangerous
behavior due to symptoms of mental illness, substance abuse, or developmental
disability.
Presence of acute risk of loss of current stable living environment.
Woman is pregnant and using alcohol or other drugs.
Consumer is actively psychotic.
Consumer is likely to experience withdrawal symptoms that require medical
intervention, but is not in active withdrawal or likely to enter active withdrawal
immediately.
CIT officer is requesting immediate response
The Call Center Clinician will assess the consumer’s clinical needs by completing the Call
Center’s Triage Assessment Tool, including a referral safety and treatment plan, to
ensure the consumer is referred to the appropriate level of service, and there are safety
measures in place until the consumer is assessed by the Medical/Public Safety Provider
or Community Crisis Provider.
The Call Center Clinician will document their actions in AlphaMCS, and if referring to a
Community Response Provider, will forward the completed Triage Assessment Tool for
that consumer through a secure electronic file to them to ensure they are informed of
the clinical needs of the consumer at the time of the call. If the consumer is not already
enrolled in AlphaMCS, the Community Response Provider can complete and submit an
enrollment through the AlphaMCS Provider Portal, or they can contact the Call Center to
complete the enrollment on their behalf once the consumer has been assessed and
stabilized.
The Call Center Clinician will follow up with the Emergency Center or Community Crisis
Provider within two (2) hours of the call. Follow up will continue and will be
documented in AlphaMCS until the Call Center Clinician has ensured that the consumer
has been able to receive the care that is most appropriate to meet their clinical needs.
If a consumer requires an emergent referral, the consumer is referred to a provider
regardless of funding status (Medicaid, Medicare, Insurance, etc.)
Consumers are informed of the crisis services in CoastalCare’s catchment area through various
methods, including the Consumer Handbook, other printed materials, and website postings.
CoastalCare’s Network Providers are held to the following DMA standard regarding
Appointment Wait Time for EMERGENT Referrals: The provider will see all Emergencies within
two (2) hours. If the emergency is life threatening, the provider should contact the appropriate
law enforcement agency, emergency medical services (EMS), or fire and rescue services.
79
Electronic Submission of Enrollments by Providers
For Network Providers with access to the AlphaMCS Provider Portal, the following section
outlines the process for how to submit enrollments for residents within CoastalCare’s
catchment area who present to their agency by phone or in person.
1) Consumers who walk in to a provider site:
a) The provider will assess the consumer for a life threatening situation.
i) If the consumer presents with a life threatening situation, the provider will proceed
with emergency response as clinically indicated.
ii) If the consumer does not present with a life threatening situation, the provider will
determine if the consumer is enrolled with CoastalCare
(i) By checking the enrollment status in the AlphaMCS Provider Portal
(ii) By calling the Call Center and asking about the consumer’s enrollment
status.
b) If the consumer is already enrolled in AlphaMCS, and the provider has verified with the
consumer that they are not actively receiving services from another provider, the
provider will conduct an assessment and request services as per CoastalCare’s
Utilization Management Procedures. The provider should also ensure that the
consumer’s demographic and clinical information is accurate and will complete a Clinical
Update through the AlphaMCS Provider Portal if needed.
c) If the consumer is not enrolled, the provider will complete all required enrollment
information, including documentation of Medicaid enrollment or ability to pay
information, as well as completing the “Additional Clinical Page” upon conducting the
assessment. The provider will then submit the completed enrollment form to
CoastalCare’s Enrollment and Eligibility Specialist for review of completeness, accuracy,
and verification of insurance eligibility.
2) Consumers who call in to a provider site:
a) The provider will assess the consumer for a life threatening situation.
i) If the consumer presents with a life threatening situation, the provider will proceed
with emergency response as clinically indicated.
b) If the consumer does not present with a life threatening situation, the provider will
schedule an appointment for an assessment, verifying with the consumer that they are
not actively receiving services from another provider.
c) At the consumer’s appointment, the provider will determine if the consumer is enrolled
with CoastalCare
i) By checking the enrollment status in the AlphaMCS Provider Portal
ii) By calling the Call Center and asking about the consumer’s enrollment status.
80
d) If the consumer is already enrolled in AlphaMCS, and the provider has verified with the
consumer that they are not actively receiving services from another provider, the
provider will conduct an assessment and request services as per CoastalCare’s
Utilization Management Procedures. The provider should also ensure that the
consumer’s demographic and clinical information is accurate and will complete a Clinical
Update through the AlphaMCS Provider Portal if needed.
e) If the consumer is not enrolled, the provider will complete all required enrollment
information, including documentation of Medicaid enrollment or ability to pay
information, as well as completing the “Additional Clinical Page” upon conducting the
assessment. The provider will then submit the completed enrollment form to
CoastalCare’s Enrollment and Eligibility Specialist for review of completeness, accuracy,
and verification of insurance eligibility.
Registry of Unmet Needs
CoastalCare maintains a Registry of Unmet Needs to track requests for non-emergency services
that have not been met through either state-funded or non-entitled Medicaid categories. The
purpose of the Registry is to allow CoastalCare and providers to coordinate services for
consumers when the demand for services exceeds available State or non-entitled Medicaid
resources, or when service capacity is reached as evidenced by unavailability of a provider for
the service needed. Providers, consumers, or family members may initiate a referral to the
Registry of Unmet Needs by contacting the Call Center at 1-866-875-1757.
Your Responsibility As A CoastalCare Contracted Provider Is To:
Publish and make available the toll free CoastalCare Customer Service and Call Center
numbers for consumers and family members, along with the telephone number for the
Disability Rights of North Carolina
Provide and comply with face-to-face emergency care within two (2) hours (Emergent
Request) of a request for services that is initiated by the Call Center or by the consumer; the
provider must provide face-to-face emergency care immediately for life threatening
emergencies
Provide and comply with initial face-to-face assessments and/or treatment within 48 hours
(Urgent Request) of the date and time a consumer requests your services through the Call
Center or contacts you directly
Provide and comply with initial face-to-face assessments and/or treatment within 5
business days (Routine Request) of the date a consumer requests your services through the
Call Center or contacts you directly
81
Maintain systems and procedures to ensure consumers with scheduled appointments are
being seen within the DMA required wait time of one (1) hour after their scheduled
appointment time
Maintain systems and procedures to ensure consumers who walk in are being seen within
the DMA required wait time of two (2) hours after their arrival
Maintain systems and procedures to ensure, for emergencies providers, staff provide
emergency face-to-face care within the required timeframe of two (2) hours after the
request for care is initiated by the Call Center or the consumer; life threatening
emergencies shall be managed immediately
Ensure there are no barriers to treatment, system navigation is courteous, and the
screening process is the same no matter where the consumer presents to be seen
Maintain systems and procedures to screen and triage consumer needs—whether by phone
or walk in, and schedule that consumer for an appointment within the required timeframes
Be as clear as possible in requests for information or services to enable our Call
Center/Customer Service Office to help you in the most efficient and effective way possible
Acknowledge all appointments scheduled by the Call Center in the AlphaMCS Provider
Portal within 24 hours of the Call Center scheduling the appointment and update the status
of the appointment to indicate the outcome
Follow up with a phone call whenever a consumer misses their first appointment. Send a
letter if unable to contact the consumer by phone and document all attempts to reach the
consumer
CoastalCare’s Responsibility To Providers Is To:
Assess the satisfaction of consumers served
Share natural and community resources for referrals and linkage
Care Coordination
Care Coordination is a function of CoastalCare to outreach and engage the consumers most
vulnerable into the least restrictive levels of care. Care Coordination provides oversight of
individuals who are high risk, high cost and/or who meet special healthcare needs population
criteria ensuring the individual receives the most effective and efficient care possible while
achieving an optimal level of recovery. With a holistic view of the member in mind, Care
Coordinators monitor service delivery, identifying gaps in access, making connections to
necessary and appropriate resources in the community, and ensuring appropriate plan
development. Care Coordinators are responsible for ensuring that a member’s needs are
82
addressed, through establishing linkage to the most appropriate clinical services. Care
Coordinators follow up with members and providers to ensure service engagement, monitor for
goal attainment and the members overall status improvement. Constant monitoring of the
appropriateness and accuracy of the Person Centered Plan/Individual Support Plan based on
the consumer’s needs and status helps the Care Coordinator and the consumer’s treatment
team make timely updates to improve the effectiveness and efficiency of services.
There are three categories of consumer eligibility for Care Coordination:
High Cost per NC General Statutes 122C-115.4 (1).(2) whose treatment plan is expected
to incur cost in the top twenty (20%) percent of expenditures for all consumers in an
age/disability
o Includes Consumers on the Innovations Waiver
High Risk per NC General Statute 122C-115.4 (1).(2) who has been assessed as needing
emergent crisis services three (3) or more times in the previous twelve (12) months
Special Healthcare Needs Pursuant to 42 CFR Part 438.208(c)
o Currently or have been within the past 30 days in a facility operated by the
Department of Correction, Department of Juvenile Justice and Delinquency
Prevention
o Using Drugs by injection within the last 30 days and have an opioid dependence
diagnosis
o Diagnosed within prescribed range and have a current CALOCUS of VI
o Diagnosed within prescribed range and have a current LOCUS of VI
o Diagnosed with substance dependence and have a current ASAM PPC level of
III.7 or II.2-D or higher
o Functionally eligible for, but not enrolled in, the Innovations waiver, and who
are not living in an ICF-MR facility
CoastalCare will identify and refer for care coordination services those consumers having high
cost and/or high risk or who meet the criteria for a Special Healthcare Needs population.
CoastalCare reviews the following information to identify high risk/high cost consumers:
83
Paid claims to identify the top 20% in cost utilization by age and disability
Over or under utilization of services
Community Care of North Carolina (CCNC) database to identify patterns of frequent
hospitalizations, frequent admissions to the Emergency departments and
psychopharmacology utilization.
Local and State Psychiatric/ADATC hospitalizations
High risk report that captures members who meet the established criteria
CoastalCare has two Care Coordination units: one for Intellectual/Developmental Disabilities
and one for Mental Health/Substance Use Disorders.
Functions of Care Coordination include:
Education about all available MH/SA/IDD services and supports, as well as education
about all types of Medicaid and state-funded services
Linkage to appropriate services, providers and monitoring for appropriate care
Linkage to needed psychological, behavioral, educational, and physical evaluations
Development of the Individual Support Plan (ISP) or Person Centered Plan (PCP) in
conjunction with the recipient, family, and other all service and support providers
Monitoring of the ISP, PCP, and health and safety of the consumer
Coordination of Medicaid eligibility and benefits
The Care Coordinator monitors services and plans for the consumer and works with the
consumer and his/her treatment team to adjust these over time as necessary to achieve
positive member outcomes.
Examples of care coordination activities include:
Providing follow up and engagement of high-risk consumers who do not appear for
scheduled appointments
Determining barriers to treatment and helping consumers overcome those barriers
84
Ensuring appropriate assessment and referral for services for consumers for whom a
crisis service is provided as the first service
Providing service monitoring and discharge planning for consumers who are hospitalized
until they are connected with a clinical home
Engaging consumers who frequent the emergency room to ensure they receive ongoing
care that meets their needs instead of the intermittent care provided through ED
services
Ensuring appropriate, clinically sound consumer centered planning
Promoting consumer recovery and community integration
Monitoring consumers across CoastalCare’s system and with external systems including
the medical and primary care systems to ensure best practice service delivery
Making referrals and requests for services based on the solid assessments and plan as
developed by the consumer’s team
Monitoring service activity to see that the consumer received the care that was
indicated.
Quality of Care
Care Coordination plays an important role in Quality of Care concerns. Depending of the level
of concern Care Coordinators conduct a chart review and participate in treatment team
meetings. Care Coordinators utilize Audit Tools
(http://www.ncdhhs.gov/mhddsas/statspublications/presentations/qualityofcare/index.htm)
to determine if an Independent Assessment is needed. If an Independent Assessment is
needed then the Care Coordinator assists in referring the consumer to an Independent Licensed
Professional. In conclusion of the review, the Care Coordinator makes recommendations and
assists the provider if coordinating the best level of care for consumer.
CCNC Collaboration
Care Coordination and Community Care of North Carolina work together to integrate
behavioral health providers and primary care physicians. This includes encouraging, supporting
and facilitating communication between Primary Care Providers (PCPs) and behavioral health
providers. Please refer to the follow link for more information:
http://www.ncdhhs.gov/dma/services/FourQuadrantResponsibilities.pdf. To ensure the
85
collaboration Care Coordinators and the Community Care of North Carolina meet a minimum of
once a month.
System of Care (SOC)
System of Care is a nationally recognized framework for organizing and coordinating services
and resources into a comprehensive and interconnected network. Its goal is to work in
partnership with children, youth, and families who need services or resources from multiple
human service agencies to be safe and successful at home, in school, and in the community,
and through this assistance, make the community a better place to live. Other Mental
Health/Substance Use Disorders, Care Coordination, Coastal Care has two SOC Coordinators
who work to build on individual and community strengths, and makes the most of existing
resources to help children and their families achieve better outcomes.
System of Care is the vehicle to achieve safety, permanence, and well being for children and
families in North Carolina, from legislation, to state and local collaborative groups, to Child and
Family Teams. Collaborative work is being done to ensure that children are successful in their
homes, in school and in their communities. For more information on SOC see:
http://www.ncdhhs.gov/mhddsas/services/serviceschildfamily/Toolbox/intro/i-whatissoc.pdf
System of Care Coordinators
The two CoastalCare’s System of Care (SOC) Coordinators provide information, training, and
technical assistance to the community of child/adolescent mental health and substance use
providers, community agencies, community collaborative committees and other stakeholders
on the principles of System of Care and implementation of these principles to improve the
quality of services to children and adolescents.
The SOC coordinator:
Ensures consumers are linked appropriately to providers and monitors provision of
services and benefits to consumers
Monitors effectiveness of the service delivery system through participation in Child and
Family Team meetings.
Facilitates the Juvenile Justice Mental Health and Substance Abuse Partnership,
Community Collaborative for Brunswick, Carteret, New Hanover, Onslow and Pender
counties and consultation to the five counties’ Departments of Social Services for Child
protective services.
86
Crisis Services
Care Coordination is provided for consumers who are being discharged from state facilities,
hospitals, or crisis services (Emergency Department, NC START, Mobile Crisis) to link them to a
clinical home provider. Care coordinators are assigned to participate in on-site discharge
planning for consumers being discharged from the state hospital (Cherry State Hospital in
Goldsboro), the alcohol and drug treatment center (Walter B. Jones ADATC in Greenville), the
three-way bed contract at New Hanover Behavioral Health Unit and The Harbor (facility based
crisis and detoxification). Care coordinators shall continue to work with the consumer and
medical home until such time as the consumer is connected to a clinical home provider.
Duties include:
Monitor plan implementation periodically to ensure consumers stay linked to services
and supports.
Coordinate consumer transition from one level of care to another; particularly the
transition from an institutional or more restrictive level of to a community service
provider.
Ensure the consumers are linked to a clinical home provider prior to discharge.
Ensure providers engage and provide needed services following discharge.
Innovations and Care Coordination
Care Coordination is provided to consumers on the Innovations Waiver as well as other
consumers meetings, High Risk, High Cost or Special Healthcare Needs.
For consumers on the Innovations waiver, Care Coordination provides the following:
Consulting with team members regarding consumer’s needs and care coordinator’s
efforts on behalf of the consumer on an ongoing basis
Facilitating service delivery process including re-assessment of level of care and annual reevaluation of needs and services
Assisting in selecting a service provider
87
Monitoring to assure quality of care and health, safety and well-being as well as the
continued appropriateness of services and supports including monitoring the ISP,
Individual Budget and monitoring and coordination of all providers of service
Identifying the need for a representative when the consumer desires to direct their own
services and supports
Ensuring ISP identifies how emergency back-up services will be addressed and
coordinating provision of on-call emergency back-up services
Recognizing and reporting critical incidents when necessary
Assisting with grievances when necessary
Answering any questions that arise, addressing problems in service provision, such as
providing technical assistance and coordinating treatment team meetings
Ensuring response to consumer crisis by identified providers and ensuring that needs are
met and any updates to level of care or ISP are made and submitted based on changes in
consumer needs
Assuring access to specialized assessments
Coordinating services with consumer’s CCNC medical home
Arranging other needed Medicaid services
Providing information on rights, responsibilities, and advanced directives
Submitting ISP and authorization request for identified services needed to Utilization
Management Department for service approval and ensuring approval of appropriate
services including that services utilized do not exceed services authorized
In addition Care Coordination monitoring includes:
At least monthly face-to-face visits for new waiver consumers for the first 6 months. Then
on a schedule agreed upon by the ISP team thereafter, but will receive a face-to face visit
no less than quarterly to meet health and safety needs. For months that there is no faceto-face visit, telephone contact will be made to ensure that there is no issues that need to
be addressed and the Care Coordinator will ensure that services utilized do not exceed
services authorized.
88
At least monthly face-to-face for consumers whose services are provided by guardians
and relatives living in the home of the consumer
At least monthly face-to-face visits for consumers living in residential programs
At least monthly face-to-face visits for consumers choosing the Individual Family Directed
Supports option
Intellectual or other Developmental Disabilities (I/DD)
I/DD Care Coordination is also provided for consumers who are being admitted to or discharged
from State Developmental Centers regular admission or specialty units, ICFMR residential
facilities, or emergency services to link them to a clinical home provider. I/DD Care
Coordination is provided to function as an institutional liaison for participation in on-site
discharge planning for consumers being discharged from the State Developmental Centers
(children at Murdoch Developmental Center in Butner, N.C. and adults at Caswell
Developmental Center in Kinston, NC ), and the State Neuro-Medical Center for I/DD adults
(O’Berry Neuro-Medical Center in Goldsboro, N.C.). This care coordinator shall continue to work
with the consumer and the clinical home until such time as the consumer is connected
appropriate services to meet their support
Your responsibility as a CoastalCare Contracted Provider is to:
Actively participate in a person centered planning process with others serving the
individual to develop a comprehensive Person Centered Plan/Individual Support Plan
Development of treatment and/or habilitative programs that are in accordance with the
Person Centered Plan/Individual Support Plan
Communicate with the Care Coordinators about the needs of individuals that you
support
Notify the Care Coordinator of any changes, incidents, other information of significance
related to the consumer that you serve
CoastalCare’s responsibility to Providers is to:
Assessment: DD Care Coordinators will complete or arrange for needed assessments to
identify support needs and to facilitate person centered planning processes. MH/SA
Care Coordinators will complete or arrange for needed clinical assessments for
individuals that have special health care needs in order to identify any ongoing special
conditions that require treatment or monitoring.
89
Ensuring the Development of a Individual Support Plan: DD Care Coordinators will
develop the Individual Support Plan in collaboration with the individual and his/her
support team for consumers on the Innovations waiver. MH/SA Care Coordinators will
ensure that a Person Centered Plan is developed by the Behavioral Health Clinical
Home. (Person Centered Plans should be completed by the designated provider of an
enhanced service.);
Treatment Planning Care Coordination: Both DD and MH/SA Care Coordinators will
coordinate services for individuals that have been identified as needing assistance to
access the care that they need; activities will involve working across the CoastalCare
Network and with other systems of care, including Primary Care.
Monitoring: DD Care Coordinators will complete on site visits to monitor the health and
safety of the individual, to assess the satisfaction of individuals served, and to monitor
implementation of the Individual Support Plan.
Service Definitions and Criteria
Service Definitions describe the services that providers can be paid for in the state’s public
system of MH/IDD/SA services. The definitions include descriptions of:
Required components
Provider requirements
Staffing requirements, including experience, training, education
Service types/settings
Program requirements
Utilization management
Entrance criteria
Continued stay criteria
Discharge criteria
Expected outcomes
Service exclusions
Service Array
Medicaid Services
For a listing of services, please refer to the most current version of the service arrays by benefit
level and disability. For Mental Health, Substance Abuse and Intellectual/Developmental
90
Disabilities, further details can be found in Clinical Coverage Policy No. 8A of the Division of
Medical Assistance website.
See (http://www.ncdhhs.gov/dma/mp/8A.pdf)
1. NC MH/DD/SAS Health Plan – 1915(b) Waiver: The regulations of a 1915 (b) waiver
require that all NC Medicaid State Plan services be available under the 1915 (b) waiver.
When the NC State Medicaid Plan changes the services covered under the NC
MH/DD/SAS Health Plan will also change.
See also http://www.ncdhhs.gov/mhddsas/providers/servicedefs/index.htm
2. NC Innovations Waiver [1915 (c)]: The NC Innovations Waiver is a 1915 (c) Home and
Community based waiver. The services defined under this waiver replace the CAP
services under the NC CAP-MR/DD Waiver Plan. A consumer must be a member of the
NC Innovations Waiver in order to receive these services. Please refer to the most
current version of the Service Definitions on the DMA website.
See also http://www.ncdhhs.gov/dma/mp/8M.pdf
3. B-3 Services: These are Medicaid services that are funded through a separate
capitation payment.
State Funded Benefit Plan
Services available under the State Funded Benefit Plan are available to residents of
CoastalCare’s 5 counties: Brunswick, Carteret, New Hanover, Onslow, and Pender. All individual
consumers receiving services under this plan must be registered and active with CoastalCare
through the enrollment process and the CDW system. The Benefit Plan is designed in order to
promote the availability of scarce resources for a greater number of people. Authorization
requests outside the benefit plan limitations will be returned as unable to process. When a
service has reached budgeted capacity for the month any further authorization requests for
that service will be returned as unable to process. A notice will be posted on the CoastalCare
website any time we have reached our monthly capacity. Annual benefit applies to the state
fiscal year which is July 1 – June 30.
See also http://www.secmh.org/articles/Providers/IPRS/BenefitPlan.pdf and
http://www.secmh.org/articles/Providers/IPRS/SvcCertMnthlyCap.pdf
91
Claims Information
Enrollment and Eligibility Process
Eligibility Determination
All enrollees who have their services paid by CoastalCare must be enrolled in the CoastalCare
system. Directions on patient enrollment can be found in the AlphaMCS Provider Portal
Handbook. The Enrollment Master allows providers to enter all necessary information to enroll
a client.
Individuals who are at 100% ability to pay according to the sliding fee schedule established by
the provider or who have insurance coverage that pays in full for their services, cannot be
enrolled in the CoastalCare system. The individual may receive and pay for their services from a
provider of their choice independent of CoastalCare.
It is the responsibility of the provider to confirm the enrollee’s ability to pay prior to enrolling
that individual into the CoastalCare system. This would require the provider to check the
following items:
Determine if the enrollee has Medicaid or is eligible for Medicaid.
Determine if the enrollee has Medicare or any other third party insurance coverage.
Determine if there is any other payer source – EAP program, worker’s compensation,
court ordered services to be paid by court, etc.
Determine if the enrollee meets CoastalCare criteria for use of state funds to pay for
services. The criteria will be the lack of Medicaid or other third party insurance and the
inability of the individual to pay for a portion of healthcare services based on the Sliding
Fee Schedule established by the provider.
Determine if the enrollee has previously been enrolled in the CoastalCare system.
If the enrollee is eligible for Medicaid or has already been enrolled in the CoastalCare system,
he/she is financially eligible for Medicaid reimbursable services from CoastalCare. Providers
should assist enrollees in applying for Medicaid benefits at their respective county Departments
of Social Services.
Enrollment Data
All providers are required to ensure enrollment data is up-to-date based on CoastalCare
Enrollment Procedures. Reference/training information can be found at
www.coastalcarenc.org by clicking on Training Guides and Training Videos.
92
CoastalCare eligibility staff review each enrollment form and make the determination of
eligibility based on their rules. If the enrollment is approved the submitter is notified by e-mail
and through the Provider Portal if appropriate. If the enrollment staff finds an issue with the
enrollment form, the form will sent back to the submitter via Provider Portal with comments to
allow the submitter to correct and resubmit.
All Medicaid information must be provided when requesting an enrollment. If the enrollee has
third party insurance, including Medicare, this information must be included in the enrollment
request.
Effective Date of Enrollment
Enrollment in the CoastalCare system must be done prior to providing services with the
exception of emergency situations.
Events with service dates prior to the enrollment date will be denied.
Crisis services provided in an emergency situation are an exception to this rule. In these cases,
the provider has seven (7) days to complete the enrollment and indicate the date of enrollment
as the date that the emergency service was provided.
Patient ID
The Patient ID Number identifies the specific enrollee receiving the service and is assigned by
the CoastalCare AlphaMCS system. All claims submitted with incorrect Patient ID Numbers or
for enrollees whose enrollment is no longer active will be denied.
Coordination of Benefits
CoastalCare will be the payer of last resort. Providers are required to pursue all applicable first
and third party payments for services in order to minimize the usage of public resources.
First party payers are the enrollees or their guarantors. Services paid with state funds are
subject to the Sliding Fee Schedule established by the provider.
Third party payers are any other funding sources that can be billed for the services provided to
the enrollee. These payers can include worker’s compensation, disability insurance, or other
health insurance coverage.
All claims must identify the amounts collected from these first and third party payers.
Providers should only request payment for any remaining amount.
Eligibility Determination Process by Provider
Providers should conduct a comprehensive eligibility determination process whenever an
enrollee enters the system. Periodically (no more than every 90 days), the provider should
93
recheck eligibility information to determine if there are any first or third party payers for this
enrollee. It is the provider’s responsibility to monitor this data and to complete Consumer
Updates in the Provider Portal. Billing should be adjusted if there are additional payers.
Obligation to Collect
Providers must make good faith efforts to collect all first and third party funds prior to billing
CoastalCare. First party charges must be reflected on the claim whether they were collected or
not. The CoastalCare AlphaMCS system will incorporate both a Sliding Fee Schedule tracking
function and a Client Deductible tracking function. Both functions will be based on the criteria
as dictated under each Insurance/Benefit Plan.
Reporting of Third Party Payments
Providers are required to record on the claim either the payment or denial information from a
third party payer. Copies of the Electronic Remittance Advice (ERA) or Explanation of Benefits
(EOB) from the insurance company should be retained by the provider if they submit electronic
billing. If paper claims are submitted to CoastalCare the provider will be required to attach
paper copies of the ERA or EOB with the form.
Providers must wait a reasonable amount of time in order to obtain a response from the
insurance company without exceeding the 90 day rule before submitting claims. In the event
that an insurance company pays after a claim has been submitted to CoastalCare, the provider
must notify and reimburse CoastalCare.
Process to Modify
Consumers who become Medicaid eligible are not subject to Sliding Fee Schedules for Medicaid
covered services, and payments should be adjusted immediately when this is determined.
Sliding Fee Schedules
Eligibility for Benefit Determination
All enrollees must be evaluated at the time of enrollment on their ability to pay for services. In
the case of crisis and emergency services, information must be collected at the first clinically
appropriate occasion before submission of the first claim. This determination should be
updated at least every 90 days to minimize the usage of public resources.
Establishment of the Sliding Fee Schedule
Prior to enrollment in the CoastalCare system, each enrollee must have completed the financial
eligibility process to establish any third party coverage and to establish the ability to pay for
services. The combination of an enrollee’s adjusted gross monthly income and the number of
94
dependents determines the payment amount based on the Sliding Fee Schedule established by
the provider.
Authorizations Required for Payment
System Edits
The CoastalCare AlphaMCS system is designed to check for proper authorization data prior to
paying claims. A provider logs into Provider Portal and has the option of creating a new
authorization request for an enrollee or choosing an existing authorization to use as a template.
Providers will be able to utilize the Provider Portal to verify the status of their authorization
requests.
Authorization Number & Effective Dates
Each authorization will be assigned a unique number, start date, and end date. Only services
within this specific authorization will be paid. Dates and/or units outside of these parameters
will be denied.
Units of Service
Each authorization will indicate the maximum number of units that were authorized. As each
claim is processed, the system will perform an edit to make sure that the units being claimed
fall within the units of service authorized and subtract that number of units. The system will
automatically deny claims that do not fall within the authorization limits. Providers should
establish their own internal controls to monitor their authorization usage and requests in order
to prevent claim denials.
Exceptions to Authorization Rule
There are certain services that will be paid without an authorization. These services are limited
in scope and are limited in total number to an enrollee. Once the annual limit has been
reached for an enrollee, all services without a proper authorization will be denied. Providers
must be diligent in tracking these limits in order to avoid denied claims.
Payment of Claims & Claims Inquiries
Clean Claims
A clean claim is a claim that can be processed without obtaining additional information from
the provider of the services or from a third party. It does not include a claim under review for
medical necessity or a claim that is from a provider that is under investigation by a
governmental agency for fraud or abuse. The clean claim criteria is consistent with state
requirements and providers are educated on the agency clean claims criteria through initial
95
orientation, communication memorandums, provider manual, AlphaMCS Provider Portal
Handbook, and the agency web site.
Service Codes & Rates
Provider contracts contain a listing of services which they are eligible to provide. All providers
are reimbursed at the CoastalCare published rates for the service provided unless otherwise
stated in their contract. Providers can submit claims for more than the published rates, but
only the published contracted rate will be paid. If a provider submits a claim for less than the
published rate, the lower rate will be paid. It is the responsibility of the provider to monitor the
publishing of the rates and to make necessary changes accordingly.
Standard Codes for Claims Submission
Refer to CoastalCare website www.coastalcarenc.org for the following:
CPT/HCPCS/Revenue Codes
Diagnosis Codes
Place of Service Codes
Timeframes for Submission of Claims
State Funded Services
The agency shall honor provider billing for state funds that are filed in accordance with the
agency’s contract with the provider. If the provider bills within sixty (60) days of providing a
service, the agency will pay claims in accordance with the prompt pay requirements set forth as
follows: within eighteen (18) calendar days after the agency receives a claim from a provider,
the agency shall either (a) approve payment of the claim, (b) deny the claim, or (c) determine
that additional information is required for making an approval or denial. If the agency approves
the claim, the payment shall be made within thirty (30) calendar days after making approval.
Medicaid Funded Services
The agency shall honor billing for Medicaid funds that are filed in accordance with the agency’s
contract with the provider. If the provider bills within ninety (90) days of providing a service,
the agency will pay claims in accordance with the prompt pay requirements set forth as follows:
within eighteen (18) calendar days after the agency receives a claim from a provider, the
agency shall either: (a) approve payment of the claim, (b) deny the claim, or (c) determine that
additional information is required for making an approval or denial. If the agency approves the
claim, the payment shall be made within thirty (30) days after making approval. The agency
shall ensure that ninety (90) percent of all clean claims for covered services are paid within
thirty (30) days of the date of approval, and that ninety-nine (99) percent of such claims shall be
paid within one hundred eighty (180 days of the date of receipt. The agency will not be
96
responsible for processing or payment of claims that are submitted ninety (90) days after the
date of service unless coordination of benefits is involved (provider waiting on receipt of
payment of denial from third party payer). Date of receipt is the date the agency receives the
claim by Provider Portal or 837. The date paid is the date of the Electronic Fund Transfer (EFT).
Multiple Occurrences of Same Service In a Day
Specific services rendered multiple times in a single day must be (bundled) billed using multiple
units rather than as separate line entries. This process prevents a duplicate billing denial.
NPI (National Provider Identifier)
It is mandatory for providers to obtain an NPI number to submit billing on the CMS-1500 and
UB-04 forms. The AlphaMCS system captures and stores the provider’s and the individual
clinician’s NPI and taxonomy codes. These codes are primarily used in the claim processing
workflows for validating a provider or clinician.
Verification of Receipt of 837 Electronic Billing File
CoastalCare’s system provides the following responses to ensure that the electronic 837 is
accepted into the AlphaMCS system for processing and payment:
997 File – This file acknowledges receipt of the 837 billing file.
824 File – This file contains feedback regarding whether line items in the 837 file have
been accepted or rejected. If an item was rejected, a detailed explanation will be
provided.
In the event that there are errors found in the claim file, only those claims that contain errors
will be rejected and the remaining clean claims will continue on to the AlphaMCS system.
Provider Portal Direct Claims Submission
Providers may directly enter their claims in CMS-1500 or UB-94 format through the Provider
Portal. The provider selects the type of claim they would like to submit and chooses the
enrollee they have served. The provider staff can create a new claim from a blank form or
utilize a previous claim as a template to improve data entry efficiency. The AlphaMCS system
will validate that all required fields have been properly completed.
837 Claims Submission
Detailed instructions are available in the Information Management section of the Provider
Manual. These instructions are very specific on what is required to submit claims electronically
to CoastalCare. The entire testing and approval process is covered in this manual.
CoastalCare will only accept HIPAA compliant transactions as required by law. CoastalCare
provides the following HIPAA transaction files back to providers: 997 (acknowledgement
97
receipt), 824 (line by line acceptance/rejection response), and 835 (electronic version of the
remittance advice).
Process for Submission of Paper Claims
CoastalCare will accept paper claims until providers can transition to electronic claims
processing. An accurate CMS-1500 or UB-04 billing form with correct data elements must be
submitted. CoastalCare staff will use the Internal Direct Data Entry (DDE) in AlphaMCS to enter
the claim for the provider. The provider will be able to see the status of the claim regardless of
the method of entry through the Provider Portal.
Void and Replacement Claims Processing
AlphaMCS includes functioning to void and replace claims. Processing begins based on the
route and initiator of the submission. If the void or replacement claim is a paper claim or
directly entered through Provider Portal, the AlphaMCS data base validates the claim and then
attempts to match it to the original claim, then approves it to move through the claims process.
A 997 report is produced for the provider, and if the claim is validated, it is sent to the
AlphaMCS databse. At this point AlphaMCS attempts to match the claim to the original before
approving the claim to move through the claims process.
Clearinghouse Claims Routing
AlphaMCS will allow providers to utilize clearinghouse services to submit compliant
transactions including claims and eligibility. Transactions submitted through clearinghouse
services will have the responses routed directly to the clearinghouse. The provider will
continue to have full access to the status of the transaction through Provider Portal.
Medicare Override Processing
AlphaMCS will allow CoastalCare to designate services known to not be covered by Medicare or
other insurance plans from requiring third party liability information to be submitted on the
claim. This will allow for those services to be billed directly to CoastalCare without
unnecessarily billing the primary insurance only to wait for a denial.
Claim Denial Inquiries
When a provider has a claim issue/denial question, the first step is to contact their assigned
CoastalCare Claims Specialist for assistance by e-mail. Inquiries are made by sending an e-mail
to helpdesk@coastalcarenc.org and the e-mails are assigned by the Track-It system to the
appropriate Claims Specialist. All documentation regarding the inquiry is documented in the
Track-IT system. If the provider is not satisfied with the resolution by the Claims Specialist, they
should contact the Claims Manager directly. A response is made to the provider within one (1)
business day.
98
Non –clinical claims appeals
Quality Management will maintain a separate formal process to address appeals related to the
non-clinical claims adjudication process. This formal process will be managed by the Appeals
Specialist and will address claim adjudication appeals which shall include a mechanism to receive
and respond to appeals within specified time periods, processes for prioritizing, investigating, and
resolving appeals, protocols for written and verbal notification including explanation of final
results and additional method for further review when applicable.
Response to Claims
835 and Electronic Remittance Advice
AlphaMCS will produce HIPAA compliant Electronic Remittance Advice forms and Outgoing 835
records after claims have been validated and approved through the AlphaMCS Claims
Processing workflow. The generated ERA will be available to providers through Provider Portal.
The 835 file can be used by the provider’s information system staff or vendor to automatically
post payments and adjustment activity to their enrollee accounts. Providers are responsible for
managing and monitoring their accounts receivables.
Checkwrite Schedule and EFT Process
A Checkwrite Schedule is posted on CoastalCare’s website to inform providers of dates of
payment. Direct Deposit is mandatory for all provider payments. An Authorization Agreement
for Direct Deposits is required to be completed by each provider along with a voided check or
bank letter.
Claims Investigations – Fraud & Abuse
Trends of Use & Potential Fraud
One of the primary responsibilities of CoastalCare will be to monitor the Provider Network for
fraud and abuse. CoastalCare is responsible for monitoring and conducting periodic audits to
ensure compliance with all federal and state laws and in particular the Medicare/Medicaid
fraud and abuse laws. Specifically, CoastalCare validates the presence of material information
to support billing of services consistent with Medicaid and State regulations. CoastalCare has
the ability to generate random claims samples for auditing purposes to look for trends or
patterns of abuse.
Audit Process
CoastalCare has the responsibility to ensure that funds are being used for the appropriate level
and intensity of services as well as in compliance with federal, state, and general accounting
rules. The CoastalCare Quality Management Unit is responsible for billing audits for all contract
providers.
99
Voluntary Repayment of Claims
It is the provider’s responsibility to notify CoastalCare in writing of any claims billed in error that
will require repayment/recoupment. Providers are required to complete a Billing Correction
Form. CoastalCare will make adjustments in the system and those adjustments will appear on a
future Remittance Advice.
Reporting to State & Federal Authorities
For each case of reasonably substantiated suspected provider fraud and abuse, CoastalCare is
obligated to provide DMA with the provider’s name and number, the source of the complaint,
the type of provider, the nature of the complaint, the approximate range of dollars involved,
and the legal and administrative disposition of the case.
Repayment Process/Paybacks
The Business Management Department is responsible for the recovery of funds based on any
audit findings. CoastalCare will recoup the amount owed from future claims. If the payback
amount exceeds outstanding provider claims, CoastalCare will invoice the provider for the
amount owed. Providers will have thirty (30) calendar days from the date of the invoice date to
reimburse the funds. If a provider fails to repay the funds identified, CoastalCare reserves the
right to take action to collect the outstanding balance from the provider.
Standards and Regulatory Compliance
Introduction
CoastalCare maintains a Quality Management Program which is a comprehensive, proactive
program that provides the structure, process, resources, and expertise necessary to
systematically define, evaluate, monitor and ensure that high-quality, cost-effective care and
service are provided to consumers. The program is a commitment to continuous quality
improvement principles and requires participation of the Area Board, providers, and staff
members.
The Quality Management Program of CoastalCare is designed to strengthen the mental health,
intellectual/developmental disabilities, and substance abuse service delivery system, increase
the quality of services delivered by network providers, improve service outcomes for
consumers, and facilitate cost-effective care and service in an environment driven by managed
care. As a Local Management Entity (LME) and Managed Care Organization (MCO), CoastalCare
is committed to the provision of a Quality Management Program that focuses on health and
safety, protection of consumer rights, achievement of outcomes, accountability, ongoing
100
system monitoring, and improvement in the system of care as consistent with the mission,
vision, and values of the organization.
Quality Improvement
In a system driven by Continuous Quality Improvement, the Quality Management Program
facilitates the objective and systematic measurement, monitoring, and evaluation of internal
organizational processes as well as services delivered by network providers. Quality
improvement activities are implemented as a result of the findings from these activities and
measured periodically for intervention effectiveness.
Within the organization, quality assurance is used as the foundation for quality improvement
and provides information in guiding the improvement process. Information from quality
assurance activities is utilized as a platform for data reporting and analysis and provides the
opportunity for organizational planning and informed decision-making. Quality Improvement
within the organization not only focuses on adhering to standards and statutory requirements,
but also serves as the mechanism for emphasizing the agency’s commitment to excellence.
CoastalCare Network Providers are also required to maintain a Quality Management Program
that is comprehensive and proactive. The areas identified below provide a description of how
CoastalCare’s Quality Management Department interfaces with the providers in the network.
CoastalCare’s Quality Management Plan describes an in-depth overview of the Quality
Management Program and agency quality management activities and can be found on the
website at www.coastalcarenc.org.
Provider Quality Management Plans
On an annual basis, providers are required to submit their Quality Management Plans to the
CoastalCare QM Department for review. QM staff utilizes the QM Plan Checklist as a tool in
reviewing provider QM Plans and provides feedback on areas of strength and weakness to
assist agencies in developing a viable plan that can be implemented within their organization
for full effect. Technical assistance from the QM Department of CoastalCare is available upon
request. The QM Plan Checklist is available on the CoastalCare website to support the plan
development.
Quality Improvement Projects
The Provider’s Contract with CoastalCare requires all providers to complete three (3) annual
Quality Improvement Projects that demonstrates evidence of performance improvement of
some aspect of organizational processes or structures. Common QI projects are: improving
access to treatment, improving consumer satisfaction scores, decreasing wait times for
101
psychiatric appointments, reducing duplication of paperwork, and implementing performance
measures. The Quality Management Department of CoastalCare reviews the annual QI projects
and monitors the outcomes from the QI Projects submitted by providers. Technical assistance
is provided upon request. The QI Projects Checklist is available on the agency’s website at the
link below to assist providers in reporting in QI projects:
(http://www.CoastalCaremh.org/articles/QualityManagement/ProviderQIProjectChecklist.pdf).
For questions or more information about QI projects or other QI activities you may contact the
QM Systems Manager at (910) 550-2600 or elaine.gillaspie@coastalcarenc.org or the Director
of Quality Management at kim.lewis@coastalcarenc.org.
Performance Measurement
Data Collection and Verification
CoastalCare is committed to quality care on a continuous and scientifically sound basis. In order
to ensure compliance with contract requirements by DMA & DMH, CoastalCare currently
monitors and measures performance indicators within the realms of various domains, such as
Access and Availability, Appropriateness of Services, Quality of Care, Quality of Services, overall
System Performance as well as Satisfaction.
Performance Improvement
In an ongoing effort to ensure and promote a culture of excellence within the realms of internal
as well as external stakeholder performance and service delivery, CoastalCare thrives for full
completion of its various Quality Improvement Projects, according to contractual standards.
In addition to the overall system performance measures noted above, CoastalCare utilizes
multiple measures to collect data on internal departmental performance. Information is
collected quarterly and monthly, and data is entered into report forms and disseminated to the
Management Team, the Quality Management Committee, and the Area Board.
Provider Performance Profile
In monitoring the performance of Providers in its network, CoastalCare utilizes a performance
review system which targets specific quality initiatives for provider performance. Reliant upon
these quality initiatives, providers are ranked by their performance into categories: Gold Star,
Exceptional, Preferred and Routine. CoastalCare also monitors providers utilizing a system,
solely based on Core Performance standards, in accordance with their contract.
102
North Carolina Support Needs Assessment Profile-NC SNAP
NC-SNAP Requirements:
NC-SNAP Assessments are required for all active Consumers with an Intellectual or other
Developmental Disability (I/DD) diagnosis that are receiving I/DD services. Typically the
NC-SNAP Assessment should be done in conjunction with the Person Centered Plan.
NC-SNAP Assessments will be completed in accordance with protocols specified in the
NC-SNAP Examiner’s Guide.
All NC-SNAP Assessments are required to be completed by a Certified NC-SNAP
Examiner.
The Summary Report & Supplemental Information Sheet is required to be submitted
with all NC-SNAP Assessments.
NC-SNAP Assessments and the Summary Report & Supplemental Information Sheets are
required when a consumer enters the I/DD service system. NC-SNAP Assessments and
the NC-SNAP Summary Report & Supplemental Information sheet are due annually or if
a significant change has occurred in the individual’s needs.
The Care Coordinator has the primary responsibility for completing and submitting the
NC-SNAP and NC-SNAP Summary Report & Supplemental Information sheet.
If there is no Care Coordinator, the NC-SNAP Assessment and the Summary Report &
Supplemental Information sheet will be completed by a certified NC-SNAP examiner (in
order of preference):
o Residential Provider
o Day Program Provider
o Respite Provider
o Therapist
The NC-SNAP Summary Report & Supplemental Information sheet is required for all
discharges and transfers.
NC-SNAP Examiner Certification Training
NC-SNAP Certification is only available to those individuals with the appropriate credentials
who are in a position that requires them to complete or review NC-SNAP Assessments as part
of their job responsibilities. Typically, this is a Qualified Professional.
To request NC-SNAP training, email Marianne de la Vega, Medical Records Specialist, at
marianne.delavega@coastalcarenc.org for training registration at the Murdoch Developmental
Center.
103
The following information is needed for the registration of training:
Provider name, Title, and Agency.
Provider phone number, business mailing address, and e-mail address.
Training dates requested with a 1st and 2nd choice of dates.
The Medical Records Specialist will e-mail the provider a confirmation notice of the
training for them to take to the Murdoch Developmental Center, which is required for
admittance.
When requesting refresher training, please include the Examiner Certification number
with the Provider name information.
PLEASE NOTE: Examiner Certification privileges expire after twenty one (21) months of
inactivity.
Submitting Completed NC-Snap Assessments to CoastalCare
The initial NC-SNAP Assessment and Annual Update Assessment is due to CoastalCare within 30
days of the admission or annual due date (i.e. the Provider has 13 months to submit the Annual
Up-date to CoastalCare). The completed NC-SNAP Assessments should be submitted to the QM
Department.
The Provider is to submit only copies of the NC-SNAP Summary Report & Supplemental
Information sheet and the Profile page (front page) of the NC-SNAP Assessment. The Provider
is to keep the originals in the consumer’s record. The provider may submit the NC-SNAP
Assessment and NC-SNAP Summary Report & Supplemental Information sheet to CoastalCare
by one of the following ways:
Fax to 910-550-2665, attention: Marianne de la Vega
Secure email to marianne.delavega@coastalcarenc.org
When a provider submits via fax/email, the provider will receive a confirmation email of receipt
of the assessment. When submitting NC-SNAP assessments, the provider should check each
assessment/Summary Report & Supplemental Information sheet to ensure that all required
fields are accurately and entirely completed. All corrections made to the NC-SNAP should be
lined through, initialed and dated.
A new form should not be used when making corrections unless the assessment becomes
illegible.
Past Due Notices
104
CoastalCare will issue Past Due SNAP Notices on the 1st and 15th of the month. The Provider has
15 calendar days from the date of the Past Due notice to submit the NC-SNAP Assessment and
NC-SNAPs Summary Report & Supplemental Information sheet. If the Consumer has been
discharged or transferred, the Provider must submit the NC-SNAP Summary Report &
Supplemental Information sheet.
Blank NC-SNAP Assessment Forms
An original NC-SNAP Form must be used for all assessments.
CoastalCare receives a 6-month supply of blank NC-SNAP forms in January and July from the NC
Department of Health and Human Services. This is based on the number of active I/DD
consumers in the state NC-SNAP Database plus 1%.
CoastalCare will distribute to each I/DD Provider responsible for NC-SNAP Assessments a 6month supply based on the number of active consumers in the state NC-SNAP Database plus
1%. CoastalCare will notify the providers in December and June of the consumer counts. The
Provider is responsible for notifying CoastalCare if the count is incorrect. The Provider is also
responsible for managing the 6-month supply and must sign a receipt for the blank NC-SNAP
forms.
The Summary Report & Supplemental Information Sheet may be duplicated. This form is
available at CoastalCare’s website under the Provider’s Page at
http://www.CoastalCaremh.org/index.php?content=providers&catid=47&desc=NC-SNAP.
The state tracks the number of NC-SNAP forms requested and the number of assessments
entered into the database.
CoastalCare is responsible for ensuring that all Providers submit the NC-SNAP Assessment
annually as part of the Performance Contract with The Department of Health and Human
Services which is monitored by The Division of Mental Health, Developmental Disabilities, and
Substance Abuse Services.
CoastalCare NC-SNAP Contact information:
Marianne de la Vega
Medical Records Specialist
165 Center Street
Jacksonville, NC 28546
Phone: 910-459-4860
105
Fax: 910-550-2665
E-mail: marianne.delavega@coastalcarenc.org
For additional information about the NC-SNAP, visit the state’s NC-SNAP website at:
http://www.ncdhhs.gov/mhddsas/providers/NCSNAP/index.htm
North Carolina Treatment and Outcomes Program Performance System –NC TOPPS
The North Carolina-Treatment Outcomes and Program Performance System (NC-TOPPS) is the
program by which the North Carolina Division of Mental Health, Developmental Disabilities, and
Substance Abuse Services measure the quality of substance abuse and mental health services
and their impact on individuals’ lives. The web-based NC-TOPPS was implemented statewide in
July 2005 for 100% of adults and children ages 6 years and above who are receiving services for
mental health and/or substance abuse issues. A manual that details all the NC-TOPPS
requirements can be found at:
https://nctopps.ncdmh.net/dev/GettingStartedWithNCTOPPS.asp
Online interviews conducted at initiation, (3 months, 6 months, 12 months), and at the end of
an episode of care provide information on each individual’s service needs and outcomes. The
responsibility for completing NC-TOPPS lies with the consumer’s primary provider agency. The
initial interview must be completed with the consumer at the beginning of an episode of care
during the 1st or 2nd visit. The Update Interviews (3, 6, and 12 months and Bi-Annual are to be
submitted within the appropriate time frame as long as the consumer is receiving treatment. If
the consumer is no longer receiving the qualified treatment, an Episode Completion is
submitted. The NC TOPPS must be administered by a Qualified Professional. For more
information on submitting the NC TOPPS or for training, you may contact Diocles Wells at (910)
550-2664 or at diocles.wells@CoastalCarenc.org.
Performance Monitoring
An important part of CoastalCare’s role as an MCO is to monitor performance of Providers in its
network. The CoastalCare Quality Management Department is charged with data reporting and
analysis and assists the various departments within the organization in monitoring internal
performance as well as the performance of its network providers. Through the use of data,
CoastalCare is able to identify areas of service delivery and outcomes that warrant
improvements. CoastalCare may ask providers to implement specific quality improvement
projects when data findings indicate areas of deficiency. Under these circumstances, the
Quality Management staff will provide guidance and assistance to providers in making
improvements around these identified areas.
106
In monitoring the performance of Providers in its network, CoastalCare utilizes a performance
review system which targets specific quality initiatives for provider performance. It is based on
these quality initiatives, providers are ranked by their performance into categories: Gold Star,
Exceptional, Preferred and Routine. CoastalCare will also monitor the providers with a system
that is Core Performance Based according to their contract.
Monitoring of Incidents
Providers of licensed mental health services and providers of periodic or community based
services are required to report incidents to the MCO in the State’s Incident Response
Improvement Systems (IRIS). IRIS is the web-based electronic incident reporting system for
reporting incidents involving consumers of mental health, developmental disabilities and/or
substance abuse services. Providers must submit all Level II and Level III incident reports in IRIS
and a summary of all Level I incidents must be submitted to CoastalCare quarterly by the 10th
of the month following the end of the quarter.
Information on Incidents In:
Is Due:
First Quarter (July- September)
October 10th
Second Quarter (October – December)
January 10th
Third Quarter (January – March)
April 10th
Fourth Quarter (April- June)
July 10th
Providers are required to develop and maintain a system to collect documentation on any
incident that occurs in relation to a consumer. As part of its quality management process, it is
important for the provider to implement procedures that ensure the review, investigation and
follow up for each incident that occurs through its own internal Quality Management process.
This includes:
A review of all incidents on an ongoing basis to monitor for trends and patterns
Strategies aimed at the reduction/elimination of trends/patterns
Documentation of the efforts at improvement as well as an evaluation of ongoing
progress
Mandatory reporting requirements are followed
Enter Level II and III incidents IRIS
There are specific state laws governing the reporting of abuse, neglect or exploitation of
consumers. It is important that the provider’s procedures include all of these requirements. If a
report alleges the involvement of a provider’s staff in an incident of abuse, neglect or
exploitation, the provider must ensure that consumers’ are protected from involvement with
107
that staff person until the allegation is provided or disproved. The agency must take action to
correct the situation if the report of abuse, neglect or exploitation is substantiated
Incident Reporting
Providers of licensed mental health services – meaning the provider and/or facility has a license
issued by the Division of Health Services Regulation – and providers of periodic services are
required to complete and report incidents to CoastalCare. Private independent practitioners
and clinician and hospitals are not required to report. These reports should not be filed in the
consumer record, but should be filed on site for review during local monitoring.
The state defines incidents as an event at a facility or in a service that is likely to lead to adverse
effects upon a consumer. Incidents are classified into three (3) categories, Level I, II, and III,
according to the severity of the incident:
Level I Incidents:
These incidents are those that do not threaten the health and safety of the consumer or others,
and require routine care. Level I incidents should be reported to the case manager or clinician
involved in the care of the consumer, but do not need to be reported to the Home and Host
LME/MCO. It is required that they be documented and filed on site, these reports will be
reviewed during local monitoring visit. These reports should not be filed in the consumer
record, but should be filed on site for review during local monitoring.
Providers are required to submit to CoastalCare the Level I Incident Quarterly Review Report
Form. This form can be obtained on the Division website or on this Agency’s website as well.
The reports are due in January, April, July, and October. Reports are due to Brandy Wilson at
Jennifer.coston@coastalcarenc.orgby the 10th of the month following the end of the quarter.
Level II Incidents:
These incidents are those that are “any happening, which is not consistent with the routine
operation of a facility or service or the routine care of a consumer that is likely to lead to
adverse effects upon the consumer.” These reports are to be entered into the IRIS website
within 72 hours of the incident. These incidents should also be reported to the case manager
and clinician involved in the care of the consumer. These reports should not be filed in the
consumer record, but should be filed on site for review during local monitoring.
Level III Incidents:
108
These incidents are those that are “any happening, which is not consistent with the routine
operation of a facility or service or the routine care of a consumer, that is likely to lead to
adverse effects upon the consumer, and result in:
Death, permanent physical impairment or psychological impairment to a consumer;
A death, permanent physical impairment or psychological impairment caused by a
consumer or
A threat to public safety caused by a consumer.
For Level III incidents a provider peer review team meeting shall occur within 24 hours of the
incident. The peer review shall review the consumer record, gather additional information if
needed, and file a report in IRIS concerning the incident and notify any other authorities
required by law (DSS, healthcare registry, DJJ, etc). The report needs to be submitted within 24
hours of the incident. These reports should not be filed in the consumer record, but should be
filed on site for review during monitoring visits.
Additional Reporting to the MCO and DMH/DD/SAS:
If an incident is likely to be reported in a newspaper, on television or in other media, or if the
consumer is perceived to be a significant danger to or concern to the community, the provider
in addition to submitting the report in IRIS, is to verbally report the incident to the Grievance
and Incident Specialist at (910) 550-2600 within 24 hours of learning of the incident.
Restrictive Interventions:
There are two types of restrictive interventions, planned and emergency. Restrictive
interventions must be documented in the state IRIS system.
Planned interventions
If there is a therapeutic need for a consumer to have hands on intervention or other rights’
restrictions as on-going interventions it needs to be included as an addendum to the
consumer’s person centered plan. This addendum must be signed by a PhD psychologist or MD
in addition to the person centered plan. It is also required to have the provider’s or
CoastalCare’s Human Rights Committee and guardian approval prior to implementation. These
restrictive intervention plans MUST be submitted to CoastalCare to keep on file.
If the consumer has a planned intervention as part of their documented treatment and the
consumer is not injured during the intervention then this is considered a Level I incident. Again,
109
it is the expectation that these Level I incidents be reported to the case manager/clinician, and
be reported on the Provider Quarterly Level I Report.
Emergency Interventions:
Emergency interventions are those interventions that are not planned, are not part of the
consumers person centered plan and have not been approved for use by a Human Rights
Committee. These incidents are considered level II incidents and must be reported within 72
hours of the incident via IRIS.
Where to report incidents:
Level I quarterly reports should be submitted by the 10th of the month that they are due. These
reports can be mailed or faxed to CoastalCare to the attention of the Grievance and Incident
Specialist or emailed to brandy.wilson@coastalcarenc.orgby the 10th of the month following
the end of the quarter.
Level II incident reports are submitted into IRIS within 72 hours of the incident;
https://iris.dhhs.state.nc.us
All Level III incident reports need to be submitted in IRIS at:
https://iris.dhhs.state.nc.us and notification must be given to CoastalCare within 24 hours of
the event.
All Incident and Death Reporting system information, IRIS information and manuals can be
found on the Division of MH/DD./SAS website:
http://www.ncdhhs.gov/mhddsas/providers/NCincidentresponse/index.htm
Incident Review Process
CoastalCare Quality Management Staff shall review all incidents when received by CoastalCare
for completeness, appropriateness of interventions, achievement of short and long term follow
up both for the individual consumer, as well as the Provider’s service system. If
questions/concerns are noted when reviewing the incident report the Quality Management
Coordinator will work with the Provider to resolve any identified issues/concerns.
If issues/concerns are raised related to consumer care or services or the Provider’s response to
an incident, the Quality Management Department may elect to conduct an investigation and/or
an onsite review of the Provider. If at all possible the review will be coordinated with the
Provider and, if deficiencies are found, the Quality Management and Network Management
Departments will work with the Provider on the implementation of a Plan of Correction (POC).
110
It is strongly encouraged that each provider read the instructions manual for further
information and clarification. CoastalCare will provide training as needed and when changes are
made by the Division of MH/DD/SAS.
The Incident and Death Response Systems Manual and IRIS Manual can be found at NC
MH/DD/SAS: Manuals and Forms. IRIS website locations:
http://www.ncdhhs.gov/mhddsas/providers/NCincidentresponse/index.htm
https://iris.dhhs.state.nc.us
Test and training site:
https://irisuat.dhhs.state.nc.us/
Monitoring to Ensure Quality of Care
The Quality Management Department reviews incidents reported and determines whether any
follow up is needed. The Quality Management Department may conduct investigations of
incidents reported directly by Providers on Incident Reports, as well as reports provided by
consumers, families and the community.
Grievances
The provider must have a Grievance Process to address any concerns of the consumer and the
consumer’s family related to the services provided. Providers must keep documentation on all
grievances received including date received, points of grievances, and resolution information.
Any unresolved concerns or grievances should be referred to the Grievance and Incident
Specialist within the Quality Management Department. The Grievance Process must be
provided to all consumers and families of consumers’ upon admission and upon request. The
provider must advise consumers’ and families that they may contact CoastalCare directly about
any concerns or grievances.
CoastalCare’s Customer Services Line 1-855-250-1539 must be published and made available to
all consumer’s and family members. Additionally, other agencies available to take
grievances/complaints must be posted. These agencies include the
Division of MH/DD/SA Consumer Care Line in Raleigh toll-free at 800-662-7030 or Disability
Rights NC toll-free at 877-235-4210.
111
CoastalCare may receive grievances from providers, stakeholders, consumers, families, legal
guardians, or anonymous sources regarding CoastalCare’s Provider Network, and/or a specific
provider’s services or provider staff. Based on the nature of the grievance, CoastalCare’s Quality
Management Department may choose to form an internal, cross departmental investigative
team to investigate the grievance in order to determine its validity. Investigations may be
announced or unannounced. It is very important that the provider cooperate fully with all
investigative requests. It is important to understand that this is a serious responsibility that is
invested in CoastalCare, and that we must take all grievances very seriously until we are able to
resolve them. CoastalCare’s management of grievances is carefully monitored by the Division of
Medical Assistance (DMA) and the Division of MH/DD/SAS (DMH). Additionally, CoastalCare
maintains a database where all grievances and resolutions are recorded for tracking and
trending.
CoastalCare’s Quality Management Department maintains documentation on all follow up and
findings of any grievance investigation and a written summary will be provided to the provider.
If issues are identified, CoastalCare may be required to refer the matter to other regulatory
agencies, such as Division of Medical Assistance, Division of MH/DD/SAS or Division of Health
Service Regulation, for further investigation and/or the provider involved may be required to
complete a Plan of Correction (POC). Additionally, Human Rights Committee (HRC) has a
responsibility to oversee CoastalCare compliance with federal and state rules regarding
consumer rights, confidentiality, and grievances. The CoastalCare HRC is made up of
consumers, family members and expert advisors who meet at least quarterly.
The CoastalCare HRC reviews and monitors all trends in the use of restrictive
interventions, abuse, neglect and exploitation, deaths and medication errors.
The HRC also makes reports to the CoastalCare Board of Directors and DMA/DMH
The HRC reviews grievances regarding services as an advisor to the Area Director/CEO
Consumers or family members of the consumers that wish to apply to serve on the HRC
may call the CoastalCare Quality Management Department at # (910) 550-2661.
Perception of Care Surveys
The Perception of Care survey is administered to a random selection of consumers each year.
CoastalCare will provide the agencies that are selected to participate with the forms. Providers
are required to provide them to the selected consumers and return the completed forms to
CoastalCare. Providers will be informed of the timelines for submission.
CoastalCare values the satisfaction of consumers, family members, stakeholders with service
provided in the CoastalCare network. CoastalCare has various ways consumers’ satisfaction is
112
measured. These include annual surveys. The goal of these initiatives is to gather feedback on
how various CoastalCare departments perform during random and anonymous monitoring. This
system has provided excellent information that has been used to pinpoint the need for
additional training of staff
Medical Record Requirements/Service Record Standards
The requirements ensure that the Network Provider complies with state and federal laws and
rules for service records, confidentiality, and records retention so that service record standards
are met.
The Providers of services shall maintain a Service Record for each individual served in
accordance with Service Records standards set forth by state or federal law, the DMH/DD/SAS
Division regulations and/or DHHS policy. The original Service Record related to services
provided shall be accessible for review for the purpose of monitoring services rendered.
Service Records shall be retained for the duration and the format according to the LME/MCO
policies, State and Federal Law, and in accordance with the APSM 10-3, Records Retention and
Disposition Schedule for State and Area Facilities. If for any reason the Provider can no longer
maintain the Service Record, the Provider must contact the LME/MCO Medical Records
Specialist, Marianne de la Vega at 910-459-4860 or marianne.delavega@coastalcarenc.org for
further instructions on how to handle the Service Records.
Providers are required to adhere to the APSM 45-2, Records Management and Documentation
Manual for Providers of Publicly-Funded MH/DD/SA Services, CAP-MR/DD Services and Local
Management Entities, the APSM 45-1, Confidentiality Rules for Mental Health, Developmental
Disabilities and Substance Abuse Services, the APSM 10-3, Records Retention and Disposition
Schedule for State and Area Facilities, and the APSM 30-1, Rules For MH/DD/SA Facilities and
Services.
When a provider is found to be out of compliance through a complaint or any other
communication regarding any service record standards and/or confidentiality rules and laws, a
follow-up process will be reported and take place.
State Level Requirements Documents
APSM 30-1
Rules For MH/DD/SA Facilities and Services
APSM 45-1
Confidentiality Rules For MH/DD/SA Services
113
APSM 45-2
Records Management and Documentation Manual
APSM 10-3
Records Retention and Disposition Schedule
GS 122 C
Mental Health, Substance Abuse, Developmental Disabilities Act of 1985
GS 122C-52
Right to Confidentiality
Federal Level Requirements Documents
42 CFR Part 2 Confidentiality Regulation – Substance Abuse Information
45 CFR Part 160 Standards for Privacy of Health Information and 164
Corporate Compliance
Corporate Compliance Program
CoastalCare is committed to upholding the highest level of professional and business standards
within the provider network. Providers are expected to maintain and promote a culture of
ethical practice in all aspects of business operations. Providers are expected to have a
mechanism to ensure compliance with laws, rules and regulations. Providers will conduct
activities to prevent, detect and correct fraud, waste and abuse. Providers of Medicaid services
are required to implement a corporate compliance program as required under federal law.
Primary Areas:
Corporate Compliance is responsible for establishing a centralized mechanism to track and
ensure compliance with all applicable state and federal laws, accreditation standards, rules and
regulations. CorporateCompliance conducts activities to prevent, detect, report and investigate
suspected fraud and abuse. The Compliance Program is intended to provide reasonable
assurance that CoastalCare:
Complies with applicable federal, state and local laws, rules and regulations;
Satisfies the compliance requirements outlined in the contract with the North Carolina
Department of Health and Human Services;
Prevents, detects, and reports known or suspected fraud and abuse or other forms of
misconduct that might expose this agency to significant criminal or civil liability;
114
Promotes self-auditing and self-policing, and provides for voluntary disclosure of
violations of laws, rules or regulations;
Establishes, monitors, and enforces high professional and ethical standards.
Providers must monitor for potential fraud and abuse and take immediate action to address
reports or suspicion. According to 42 CFR Part 455- Program Integrity: Medicaid, The term
“fraud” is defined as an intentional deception or misrepresentation made by a person with the
knowledge that the deception could result in some unauthorized benefit to himself or some
other person. It includes any act that constitutes fraud under applicable Federal or State
law.The term “abuse” is defined as provider practices that are inconsistent with sound fiscal,
business, or medical practices, and result in an unnecessary cost to the Medicaid program, or in
reimbursement for services that are not medically necessary or that fail to meet professionally
recognized standards for health care. It also includes beneficiary practices that result in
unnecessary cost to the Medicaid program.
Corporate Compliance Plan
CoastalCare has a Corporate Compliance Plan to guard against and identify fraud and abuse.
The Plan describes the Corporate Compliance Program, sets the tone for the compliance
culture, reflects Compliance policies, and provides guidance to staff on the Code of Conduct
and specific applicable regulatory requirements including fraud, waste and abuse. The
objective of the Plan is to prevent, detect and correct violations of laws, rules, regulations and
the Code of Conduct. Providers of Medicaid services are required to implement a corporate
compliance program as required under federal law. An effective Corporate Compliance Plan
should include seven basic guidelines according to the U.S. Sentencing Guidelines:
1.
2.
3.
4.
5.
6.
7.
Written policies and procedures,
A designated compliance officer and a compliance committee,
Effective training and education,
Effective lines of communication,
Standards enforced through well-publicized disciplinary guidelines,
Auditing and monitoring, and
Responses to detected offenses and corrective action plans.
Compliance Committee
CoastalCare has a formal Corporate Compliance Committee that oversees the Corporate
Compliance Program. The Corporate Compliance Committee is a standing subcommittee of the
agency’s Quality Management Committee. The Committee conducts an annual compliance
115
audit. The Corporate Compliance Committee annually evaluates the effectiveness of the Plan
and makes revisions as needed.
ComplianceHelp Desk
CoastalCare has a designated Compliance Help Desk that is monitored by the Corporate
Compliance Department. Providers can submit questions and seek guidance on compliance by
contacting compliance@coastalcarenc.org. A response will be given within one business day.
Compliance Reporting Tools
CoastalCare has initiated EthicsPoint, a secure and confidential tool to report matters involving
compliance, ethics, fraud, and abuse. Reports can be made online or by calling the telephone
tip line. EthicsPoint is available 24 hours a day, 7 days a week. The hotline is confidential and
CoastalCare will honor this anonymity in full compliance with the standards. Reports will be
sent to, acted upon and monitored by the Corporate Compliance Department. The Corporate
Compliance Department will forward all credible allegations of fraud along with supporting
documentation to DMA Program Integrity.
To make a report:
Go to: https://secure.ethicspoint.com/domain/en/report_custom.asp?clientid=34587
OR
Call toll-free: 1.855.659.7660
Monitoring and Auditing
CoastalCare conducts internal data integrity checks, audits and compliance investigations.
CoastalCare has adopted a fully operational set of processes that proactively protects the
agency and detects fraud and abuse, which contains both internal and external components.
Investigation and Reporting
When CoastalCare receives information regarding an alleged compliance violation, an
investigation will occur to collect information and determine the validity. The Corporate
Compliance Department will forward all credible allegations of compliance issues and fraud,
waste or abuse along with supporting documentation to the appropriate regulatory bodies.
Code of Ethics
CoastalCare has established a Code of Ethics to promote lawful and ethical behavior by all
employees, area board members, providers and the Consumer and Family Advisory Committee
116
(CFAC) and to ensure that CoastalCare’s business is conducted according to the established
CoastalCare values as well as all applicable rules, regulations and laws.
False Claims Act Education Requirements& Affordable Care Act
Section 6023 of the Deficit Reduction Act (DRA) of 2005 requires providers receiving annual
Medicaid payments of $5 million or more to educate employees, contractors, and agents about
Federal and State fraud and false claims laws and the whistleblower protections available under
those laws. For more information visit the North Carolina Division of Medical Assistance
website at: http://www.ncdhhs.gov/dma/fca/index.htm.
Additionally, the Affordable Care Act and Sessions Law 2011-399, modified this requirement.
The federal rule 455.23 enacted requires ALL Medicaid providers, regardless of the amount
reimbursed, to attest that they met the minimum business requirements necessary to comply
with all federal and state requirements.For more information visit the federal government
website of healthcare.gov at: http://www.healthcare.gov/law/full/index.html
Dispute Resolution Process for Providers
Dispute Resolution is the formal mechanism available to all participating providers to have a
CoastalCare decision to levy sanctions reviewed and/or reconsidered, upon provider request.
The appeal is reviewed by a panel not involved in the original decision. For violation(s)
involving professional competence or conduct sanctioning decisions are reviewed by a twolevel panel system of clinical peers and CoastalCare staff. For violation(s) involving
administrative matters, decisions to levy sanctions are reviewed by a designated CoastalCare
staff member. The dispute resolution mechanism is not available for contractual violations.
Any participating provider may avail themselves of the dispute resolution process, unless the
sanction is classified as undisputable, i.e. involving explicit requirements of the written
agreement, such as maintenance of licensure, insurance coverage or if the provider is convicted
of claims fraud.
Role and Responsibilities of the Network Management Department
The CoastalCare Network Management Department will review documentation regarding
provider audits and investigations. Upon a review of documentation, the Network
Management Department will make recommendations regarding:
o Sanctions and penalties
o Disenrollment from the Network
117
o Lifting of a freeze on referrals or sanction
o The need for additional provider technical assistance or training
o Referral to the Credentialing Committee
CoastalCare shall determine sanctions or penalties to be implemented. Such sanctions may
include, but are not limited to:
o A corrective action plan.
o
o
o
o
o
Suspension of referrals.
Transfer of CoastalCare funded clients to another provider.
Additional monitoring activities
De-credentialing of individual practitioners within the agency.
De-credentialing for the provider agency.
The Network Management Department shall notify the providers of any sanctions levied.
Role and Responsibility of the First and Second Level Peer Review Panels
For professional competence or conduct violations, the 1st level dispute panel will include at
least three qualified individuals, at least one of which must be a participating provider who is
not otherwise involved in network management and who is a clinical peer of the participating
provider who filed the dispute.
Within 5 business days of receipt of the Dispute Resolution Request form, the Network
Management Director will select qualified members for the first level panel. The panel
convenes within 10 business days of the selection of all qualified members. The three members
review all available documentation as a group and deliberate until a consensus is reached. The
review panel will make a determination and document whether the original sanction decision is
appropriate and whether the agency followed the procedure correctly. The Network
Management liaison responds in writing to the provider initiating the dispute within 5 business
days. A decision letter will be sent via certified mail and outlines the final step in the agency’s
dispute resolution process.
If the provider disagrees with the decision and wishes to continue the dispute; a request must
be sent in writing to CoastalCare Network Management department within 10 days of receipt
of the level 1 dispute decision letter. Additional information may be included for consideration
along with the second level dispute request. (See requirements below.)
118
Within 5 business days of receipt of the second-level dispute request, the liaison documents the
request in the providers’ file and forwards the packet to the Network Management Director or
designee. The Network Management Director selects qualified members for a second level
dispute panel within 10 business days. This panel includes; at least three qualified individuals of
whom one of which must be a participating provider who is not otherwise involved in any
previous decisions and who is a clinical peer of the participating provider that has filed the
dispute. These three individuals must not have been involved in the first level panel or original
decision.
The panel convenes within 10 business days of the selection of all qualified members. The three
members review all available documentation as a group and deliberate until a 2:1 consensus is
reached. The review panel will make a determination and document whether the original
sanction decision is appropriate and whether the agency followed the procedure correctly. The
panel documents the decision using the Dispute Resolution Determination form within 2
business days. The provider is notified of the determination by certified mail within 5 business
days of the review. The second level review panel decision is documented in the providers’ file.
The letter will include contact information in the event the provider wishes to pursue a State
level appeal/dispute.
Role and Responsibilities of the Credentialing Committee
The Credentialing Committee may change a provider’s credentialing status (i.e. suspension or
revocation) on the basis of an action or non-action that is found to violate CoastalCare’s
standards of practice. The Credentialing Committee will make reports to the licensing boards
for independent licensed practitioners and based on audit findings.
Role and Responsibility of the Finance Department
The Finance Department may pursue a variety of options to enforce the payback, including
withholding of future claims payments, invoicing and collecting from the provider, or referring
the assessment to a third party collection agency. Collection efforts may include initiating legal
action and obtaining a judgment and execution of the judgment against the provider for the
payback. The Finance Department also has responsibility to assess provider paybacks arising
from Coordination of Benefits (COB) and Sliding Fee Scale audits.
Paybacks Due and Payable upon Completion of the Dispute Resolution Process
All paybacks are due and payable by the Provider upon completion of the
reconsideration.
All reimbursement to the provider shall cease unless and until the required payback is paid in
119
full. Paybacks shall be paid by withholding reimbursement payments due to the Provider or by
direct repayment to CoastalCare, as specified in an approved payment plan. All payments due
to the Provider shall continue to be withheld until either the payback is paid in full or a payback
payment plan is approved in writing.
State Appeal Process
In accordance with General Statute 122C-151.4, if the Provider is not satisfied with the final
CoastalCare decision involving State funded services, the Provider may file an appeal of the
final CoastalCare decision with the State Mental Health/Developmental Disabilities/Substance
Abuse ("MH/DD/SA") Appeals Panel as outlined below at the following address:
Division Director/Appeals Panel
N.C. Division of MH/DD/SAS
3001 Mail Service Center
Raleigh, NC 27699-3001
1. General Statute 122C – 151.4 subsections c (1), (2), (3) provides Consumers,
Contractors and former Contractors the right to file Appeals to the State MH/DD/SA
Appeals Panel after they have exhausted the appeals (Provider Reconsideration or
Consumer Grievance) process at CoastalCare.
a. A contractor or former contractor who claims that an area authority or
county program is not acting or has not acted within applicable State law or
rules in imposing a particular requirement on the contractor on fulfillment of
the contract;
b. A contractor or former contractor who claims that a requirement of the
contract substantially compromises the ability of the contractor to fulfill the
contract;
c. A contractor or former contractor who claims that an area authority or
county program has acted arbitrarily and capriciously in reducing funding for
the type of services provided or formerly provided by the contractor or
former contractor.
2. A Provider wishing to appeal the final CoastalCare decision can file an appeal with
the State MH/DD/SA Appeals Panel as follows:
a. The Provider shall file written notice of appeal with the Director of the Division
of MH/DD/SAS at the address provided above within fifteen (15) calendar days
of the date of the final PBH decision. 10A N.C.A.C. 27G.0810
120
b. File or filing means personal delivery, delivery by certified mail, or delivery by
overnight express mail to the current Director of the N.C. Division of
MH/DD/SAS. A document is deemed filed as of the date of delivery to the
Director. Failure to timely file or to file in conformity with the rules shall be
considered an improper filing and denied. 10A N.C.A.C. 27G.0810 (b).
c. The Division Director will appoint an impartial Panel (the "Panel") to complete an
administrative review and make an administrative review decision on the appeal.
10A N.C.A.C. 27G.0810 (e)-(l).
i. The administrative review decision is appealable by either the Provider or
CoastalCare upon written request for an informal hearing made to the
Chairman of the Panel within 15 business days of the date of the
administrative review decision. 10A N.C.A.C. 27G.0810 (m).
ii. If no appeal is made with 15 business days of the date of the
administrative review decision, the administrative review decision shall
be considered final. 10A N.C.A.C. 27G.0810 (n).
d. The administrative code at 10A N.C.A.C. 27G.0811 provides the process and
procedures for an informal hearing. The Panel will render a hearing decision,
which may be appealed pursuant to N.C. Gen. Stat. § 122C-151.4(f), as set forth
below.
e. The final CoastalCare decision, including the requirement for a payback, is not
stayed by an appeal to the Panel. N.C. Gen. Stat. § 122C-151.4(d),
f. Chapter 150B Appeal: In accordance with N.C. Gen. Stat. § 122C-151.4(f), a
Provider that is dissatisfied with the Panel's hearing decision may file a contested
case under Chapter 150B of the North Carolina General Statutes.
Notwithstanding G.S. 150B-2(1a), CoastalCare as an area authority is considered
an agency for purposes of the limited appeal authorized by this section. The
Secretary shall make a final decision in the contested case.
Definitions
Abuse: Provider practices that are inconsistent with sound fiscal, business, or medical
practices, and result in an unnecessary cost to the Medicaid program, or in reimbursement
for services that are not medically necessary or that fail to meet professionally recognized
standards for health care. It also includes beneficiary practices that result in unnecessary
cost to the Medicaid program. (Guidelines for Addressing Fraud and Abuse in Medicaid
Managed Care, October 2000)
121
Action: An action is defined as an event in which CoastalCare applies sanctions such as the
requirement for a Plan of Correction, payback, or referral freeze. The action is the result of
findings from audits, quality of services evaluations, investigations, or report by outside
investigative authorities. An action also includes a denial (in whole or in part) of a provider’s
request to employ a family member to serve a consumer.
Fraud: A deception or misrepresentation made by a person with the knowledge that the
deception could result in some unauthorized benefit to himself or some other person. It
includes any act that constitutes fraud under applicable Federal or State law. (Guidelines for
Addressing Fraud and Abuse in Medicaid Managed Care, October 2000)
Reconsideration Committee: The Reconsideration Committee and its Chair are appointed
by the Area Director. The Committee has authority to make final determinations on
provider Requests for Reconsideration of CoastalCare Actions.
Reconsideration Review: A review of an action based on the Provider’s Reconsideration
Request and any additional materials presented by the Provider. This process includes a
review of the decisions of the first and second level peer review. The Reconsideration
Committee makes the final determination as to whether the Provider’s request is approved
or denied by CoastalCare.
122
Glossary of Terms
Definitions included in this section are primarily for clarification of terms used in this manual or
references. However many of these definitions are also used in existing state and Area
Authority documents and are included here to be helpful but are not to be considered
comprehensive. Where similar definitions apply to multiple terms, the terms are grouped.
Broad categories are defined with specific elements detailed as a part of the entire definition.
ACCESS – An array of treatments, services and supports is available; consumers know how and
where to obtain them; and there are no system barriers or obstacles to getting what they need,
when they are needed.
ACCREDITATION – Certification by an approved national accrediting organization that has a set
of standards. This is a requirement of select service definitions.
ACTT - Assertive Community Treatment Team – enhanced Medicaid service
ADULT - A person 18 years of age or older, unless the term is given a different definition by
statute, rule, or policies.
ADMINISTRATIVE SERVICES - Services other than the direct provision of MH/DD/SA services
(including case management) to eligible or enrolled persons, necessary to manage the
MH/DD/SA system, including but not limited to: Provider Services and contracting, provider
billing accounting, information technology services, processing and investigating grievances and
appeals, legal services (including any legal representative of the Contractor at Administrative
hearings concerning the Contractors decisions and actions), planning, program development,
program evaluation, personnel management, staff development and training, provider auditing
and monitoring, utilization review and quality management.
ADVOCACY – Activities in support of, or on behalf of, people with mental illness, developmental
disabilities or addiction disorders including protection of rights, legal and other service
assistance, and system or policy changes.
AMERICAN SOCIETY OF ADDICTION MEDICINE (ASAM) - An international organization of
physicians dedicated to improving the treatment of people with substance use disorders by
educating physicians and medical students, promoting research and prevention, and informing
the medical community and the public about issues related to substance use. In 1991, ASAM
published a set of patient placement criteria that have been widely used and analyzed in the
alcohol, tobacco and other drug field.
AOC - Administrative Office of the Courts
123
APPEAL- means a formal request for review of a decision made by the Contractor or a
subcontracted provider related to eligibility for covered services or the appropriateness of
treatment services provided.
APPEALS PANEL - The State MH/DD/SA appeals panel established under NC. G.S.371
AREA AUTHORITY –Local oversight agency of MH/DD/SA services, formerly known as LME
ASSERTIVE ENGAGEMENT – A service offered though CoastalCare’s Benefit Plan. The service
uses an alternative service definition. Assertive Engagement is designed to assist new
consumers with engaging in treatment. This service is available to all disability areas.
ASSESSMENT – A comprehensive examination and evaluation of a person’s needs for
psychiatric, developmental disability or substance abuse treatment, services and/or supports
according to applicable requirements.
AUTHORIZATION - The process by which Utilization Management agrees to a medically
necessary specific service or plan of care based upon best practice. The granted request of a
provider is assigned a number for tracking and linked to the subsequent claim that will be made
for reimbursement. PRE-AUTHORIZATION/PRIOR AUTHORIZATION is the process of approving
use of certain resources in advance rather than after the service has been requested. Approval
for admission to hospitals in an emergent situation is one example. RE-AUTHORIZATION is the
process of submitting a request for services for a consumer who has already received
authorized services. The request shall specify the scope, amount and duration of service
requested and shall indicate the consumer’s progress toward outcomes, the use of natural and
community supports, and how the requested services will support the outcome the individual is
seeking. RETROSPECTIVE AUTHORIZATION is authorization to provide services after the services
have been delivered.
AVAILABILITY-Within the MH/DD/SA service network, the agency has defined availability as the
ability of consumers to receive appropriate care within defined timeframes. An example of an
Availability Goal would be having sufficient provider capacity so that consumers can receive a
needed routine service within 5 days of initiation.
BASIC SERVICES – Mental health, developmental disability or substance abuse services that are
available to North Carolina residents who need them whether or not they meet criteria for
target or priority populations.
BENEFIT PACKAGE OR PLAN – An array of treatments, services and/or supports intended to
meet the needs of target or priority populations. BENEFIT LIMITATIONS are any provision, other
than an exclusion, which restricts coverage, regardless of medical necessity. Covered Benefits
are medically necessary services that are specifically provided for under the provisions of
124
Evidence of Coverage. A covered benefit shall always be medically necessary, but not every
medically necessary service is a covered benefit. For example, some elements of custodial or
maintenance care, which are excluded from coverage, may be medically necessary, but are not
covered.
BEST PRACTICE(S) – Interventions, treatments, services or actions that have been shown by
substantial research or professional consensus to generate the best outcomes or results. The
terms, EVIDENCE-BASED, or RESEARCH-BASED may also be used.
BLOCK GRANT – Funds received from the federal government (or others), in a lump sum, for
services specified in an application plan that meet the intent of the block grant purpose. (Also
referred to as CATEGORICAL FUNDING)
BUSINESS NEEDS OF THE ORGANIZATION - to include the contractual obligations of the agency,
state and federal rules and regulations, accreditation standards, access and availability
standards and goals, the Network Sufficiency and Development Plan and having an adequate
number of choices for consumers within a service, when applicable.
CABHA –Critical Assess Behavioral Healthcare Agency
CARE COORDINATION – The methods utilized to notify other providers of significant events in
the course of care and to enable multiple providers to give integrated care to an individual.
Professionals with a broad knowledge of the resources, services and programs supported by
the public MH/DD/SA system and the community at-large, advocate for access and link
individuals to entitlements and services. It is an administrative Service Management Function
performed by the Contractor for individuals not enrolled or not meeting target population
definitions.
CARF - Council on Accreditation of Rehabilitation Facilities
CATCHMENT AREA - The geographic part of the State served by a specific Contractor. The
GEOGRAPHIC AREA can be a specific county or defined grouping of counties that are available
for contract award. The Contractor is responsible to provide covered services to eligible
residents of their area.
CENTERS FOR MEDICAID AND MEDICARE SERVICES (CMS) - The federal agency responsible for
overseeing the Medicaid and Medicare programs. Formerly, it was known as the Health Care
Financing Administration, (HCFA).
CERTIFICATION – A Statement of approval granted by a certifying agency confirming that the
program/service/agency has met the standards set by the certifying agency. The Contractor or
the NC Council may be the certifying agency for subcontracted Providers.
125
CERTIFIED MAIL –mail with proof of delivery
CFAC – Each LME has a Consumer Family Advisory Committee which is comprised of consumers
and family members representing all disability groups. CFACs meet on a regular basis in their
communities to support and communicate their concerns and provide advice and comment on
all state and local plans.
CHILD - Eligible person who is under the age of I8 unless the term is given a different definition
by statute, rule or policies
CLAIMS MANAGEMENT – The process of receiving, reviewing, adjudicating, INVESTIGATING,
paying, and otherwise processing service claims submitted by network and facility providers.
CLAIM – An itemized Statement of services, performed by a provider network member or
facility, which is submitted for payment. CLEAN CLAIM- means a claim that successfully passes
all adjudication edits.
CLIENT - An individual who is admitted to or receiving public services. “Client” includes the
client’s personal representative or designee and the terms CONSUMER, RECIPIENT and PATIENT
are often used interchangeably.
CLIENTOUTCOMES INVENTORY (COI) – DMH/DD/SAS measurement system for assessing
treatment/services outcomes of mental health and substance abuse service consumers.
CLIENT DATA WAREHOUSE - The DHHS’s source of information to monitor program, clinical and
demographic information on the clients served. The data are also used to respond to
Departmental, Legislative and Federal reporting requirements.
CLINICAL HOME– Treatment provider that is responsible for writing the Person Centered Plan
CLINICAL PRACTICE GUIDELINES – Utilization and quality management mechanisms designed to
aid providers in making decisions about the most appropriate course of treatment for a specific
clinical case. The guidelines or TREATMENT PROTOCOLS are summaries of best practice
research and consensus. They include professional standards for providing care based on
diagnostically related groups. NC has adopted protocols for MH and DD. NC uses ASAM
Guidelines for substance abuse.
COA - Council on Accreditation
CO-MORBID CONDITION, CO-OCCURRING DISORDERS, DUAL DIAGNOSIS –Terms that reflect
the presence of two or more disorders at the same time (e.g. Substance abuse and mental
illness; developmental disability and mental illness; substance abuse and physical health
conditions, etc) and require specialized approaches.
126
COMPLAINT – A report of dissatisfaction with some aspect of the public MH/DD/SA system. The
term DISPUTE is used to indicate a specific complaint about a service or a provider that requires
attention and joint resolution.
COMPREHENSIVE CLINICAL ASSESSMENT (CCA) -- An intensive clinical and functional face-toface evaluation by a Licensed Professional of an individual’s presenting mental health,
developmental disability, and/or substance abuse condition that results in the issuance of a
written report, providing the clinical basis for the development of a Person-Centered Plan [PCP]
and recommendations for services/supports/treatment.
CONFLICT OF INTEREST – A situation where self interest could negatively impact the best
interests of the person being served or the system
CONSENSUS - Majority opinion regarding a group decision. It is not the same as total
agreement.
CONSUMER - An individual who is admitted to or receiving public services. “Consumer”
includes the consumer’s personal representative or designee and the terms CLIENT, RECIPIENT
and PATIENT are often used interchangeably.
CONSUMER/FAMILY ADVISORY COMMITTEE – A Board appointed group of persons receiving
services, families of persons receiving services, advocates and other stakeholders that
participate in meaningful decision making relative to the local program. The group shall meet at
least monthly in a public forum to review data, practices, policies and plans of the Contractor
and make recommendations to the Board from the consumer/family perspective.
CONTRACT- A legal agreement between a payer and a subscribing group or individual which
specifies rates, performance covenants, the relationship among the parties, schedule of
benefits and other pertinent conditions. The contract usually is time limited. A contract is
defined as a document that governs the behavior of a willing buyer and a willing provider. In
this case the Contract is the 2004 Performance Agreement between the Department and the
LME.
CONTRACTOR- An organization or entity agreeing by signature to provide the goods and
services in conformance with the stated contract requirements, NC statute and rules and
federal law and regulations
CONTRACT YEAR - A period from July I of a calendar year through and including June 30 of the
following year
COPAYMENT- The portion of the cost of services which the enrolled person pays directly to the
Contractor or the subcontracted providers at the time-covered services are rendered
127
CORE SERVICES – BASIC SERVICES such as screening, assessment, crisis or emergency services
available to any person who needs them whether or not they are a member of a target or
priority population. The term also includes universal services such as education, consultation
and prevention activities intended to increase knowledge about mental illness, addiction
disorders, or developmental disabilities, reduce stigma associated with them and/or prevent
avoidable disorders.
CORPORATE COMPLIANCE – The systematic local governance plan for detection of fraud and
abuse as defined in the Balanced Budget Act.
CREDENTIALING – The process of approving providers for membership in a network to provide
services to consumers. This term can also refer to a peer competency-based credential such as
a license for professionals.
CRISIS – Response to internal or external stressors and stressful life events that may seriously
interfere with compromise a person’s ability to manage. A crisis may be emotional, physical, or
situational in nature. The crisis is the perception of and response to the situation, not the
situation itself. CRISIS RESPONSE is the immediate action to assess for acute MH/DD/SA service
needs, to assist with acute symptom reduction, and to ensure that the person in crisis safely
transitions to appropriate services. These services are available 24 hours per day, 365 days per
year. These services may be referred to as EMERGENCY services as well. NC requires a CRISIS
PLAN for consumers to promote recovery and to lessen the trauma of emergency events.
CULTURAL COMPETENCE/PROFICIENCY – A process that promotes development of skills,
beliefs, attitudes, habits, behaviors and policies which enable individuals and groups to interact
appropriately, showing that we accept and value others even when we may disagree with
them.
CUSTOMER – Customers may be ULTIMATE CUSTOMERS who are the intended and actual
recipients of the services provided by the public system, INTERNAL CUSTOMERS are those
individuals internal to the system who rely on each other to provide the service to the ultimate
customer; and EXTERNAL CUSTOMERS are those groups and individuals outside the system that
have a stake in the outcomes and products produced by the system. The concept is critical to
proper implementation of
DD –SEE IDD
DEFAULT – The breach of conditions agreed to in this Contract and/or failure tom perform
based upon defined terms and conditions the scope of work specified in the Contract.
DE-INSTITUTIONALIZATION – Release of people from institutions to care, treatment and
supports in local communities. De-institutionalization became national policy with the
Community Mental Health Centers Act of 1963. The 1997 Supreme Court decision in OLMSTEAD
128
V. LC has given new momentum to development of community based services for individuals
who have remained in State hospitals and mental retardation centers because community
services were not available. This movement is often referenced as movement to least restrictive
care or to lower levels of care where safety and community integration are balanced and
supported through the community system of services.
DEMOGRAPHIC DATA SUBMISSION – submission of demographic data of SEC consumers
through the Alpha provider portal
DEPARTMENT OF HEALTH AND HUMAN SERVICES, (DHHS) – North Carolina agency that
oversees State government human services programs and activities.
DEVELOPMENTAL DISABILITY - A severe, chronic disability of a person which: a) is attributable
to a mental or physical impairment or combination of mental and physical impairments; b) is
manifested before the person attains age 22, unless the disability is caused by a traumatic head
injury and is manifested after age 22; c) is likely to continue indefinitely and, d) results in
substantial functional limitations in three or more of the following areas of major life activity:
self-care, receptive and expressive language, capacity for independent living, learning, mobility,
self-direction and economic self sufficiency; and e) reflects the person’s need for a combination
and sequence of special interdisciplinary, or generic care, treatment, or other services which
are of a lifelong or extended duration and are individually planned and coordinated; or f. when
applied to children from birth through four years of age, may be evidenced as a developmental
delay.
DHHS - Department of Health and Human Services.
DIAGNOSTIC AND STATISTICAL MANUAL (DSM IV) – A book published by the American
Psychiatric Association, of special codes that identify and describe MH/DD/SA disorders
DISASTER – A disaster is any natural or human-caused event, which threatens or causes
injuries, fatalities, widespread destruction, distress, and economic loss. Disasters result in
situations that call for a coordinated, multi-agency response. A disaster calls for a response and
resources that usually exceed local capabilities
DIVERSION – Choosing lower cost and/or less restrictive services and/or supports. An example
would be choosing a community program instead of sending a person to a State hospital. The
term is also used when preventing arrest or imprisonment by providing services that restore
functioning and avoid detention. In North Carolina diversion programs are in place in response
to SB859 that prohibits admission of persons with mental retardation to public psychiatric
hospitals.
DIVISION OF MENTAL HEALTH, DEVELOPMENTAL DISABILITIES AND SUBSTANCE ABUSE
SERVICES (DMH/DD/SAS) - A division of the State of North Carolina, Department of Health and
129
Human Services responsible for administering and overseeing public mental health,
developmental disabilities and substance abuse programs and services.
DJJDP - Department Of Juvenile Justice and Delinquency Prevention
DOMAINS - Major areas of concern to the NC public MH/DD/SA system and its mission, goals,
and strategies and for which indicators and measures are developed to examine outcomes of
service in the lives of people served.
DPI - Department of Public Instruction
DSS - Department of Social Services
EARLY PERIODIC SCREENING, DIAGNOSTIC AND TREATMENT SERVICES (EPSDT) – Early and
Periodic Screening, Diagnosis and Treatment is a Medicaid program for Title XIX individuals
under the age of 21. This mandatory preventive child health program for Title XIX children
requires that any medically necessary health care service identified in a screening be provided
to an EPSDT recipient. The MH/DD/SA component of the EPSDT diagnostic and treatment
services for Title XIX members under age 21 years are covered by this contract.
EDUCATION – Activities designed to increase awareness or knowledge about any and all
aspects of mental health, mental illness, developmental disability or substance abuse to
individuals and/or groups. Education and training are also activities or programs delivered to
staff to ensure that service providers are competent to provide services identified as best
practices.
ELIGIBILITY – Determination of the service and/or benefit package an individual may be entitled
to or determination of a class membership that allows entry to certain services and supports.
The determination that individuals meet prescribed criteria for a particular program, set of
services or benefits.
EARLY INTERVENTION - The provision of psychological help to victims/survivors within the first
month after a critical incident, traumatic event, emergency, or disaster aimed at reducing the
severity or duration or event-related distress. For mental health service providers, this may
involve psychological first aid, needs assessment, consultation, fostering resilience and natural
supports, and triage, as well as psychological and medical treatment.
EMERGENCY- Means a situation in which an individual is experiencing a serious mental illness
or a developmental disability, or a child is experiencing a serious emotional disturbance, and
one of the following apply: o The individual can reasonably be expected within the near future
to physically injure himself, herself, or another individual, either intentionally or unintentionally
o The individual is unable to provide himself or herself food, clothing, or shelter, or to attend to
basic physical activities such as eating, toileting, bathing, grooming, dressing or ambulating, and
this inability may lead in the near future to harm to the individual or to another individual. o
130
The individual’s judgment is so impaired that he or she is unable to understand the need for
treatment and, in the opinion of the mental health professional, his or her continued behavior
as a result of the mental illness, developmental disability, or emotional disturbance can
reasonably be expected in the near future to result in physical harm to the individual or to
another individual.
ENHANCED BENEFITS –Services listed in the Medicaid Clinical Coverage Policy 8A.
ENROLLED – Individuals are admitted for service and have been provided at least one service
and assigned a unique identifying number.
FAIR HEARING RIGHTS – Advance and Adequate Notice - The notice to the Contractor in
accordance with DHHS policy and procedure using prescribed forms when denying, reducing,
suspending or terminating covered services that require prior authorization. The Contractor
shall comply with all notice, appeal and continuation of benefits requirements specified by
State and federal law and regulations. FEE FOR SERVICE – A method of payment for health
care. A payer pays the Contractor or a service provider for each reimbursable treatment, upon
submission of a valid claim, and according to agreed upon business rules. The FEE SCHEDULE is
a list of reimbursable services and the rate paid for each service provided.
FEM – Frequency and Extent of Monitoring
FEMA - Federal Emergency Management Agency
FORENSIC – Term used to describe a person with mental illness, developmental disability or
substance abuse who is involved in the criminal justice system. This includes persons found Not
Guilty by Reason of Insanity (NGRI), those who are Incompetent to Stand Trial, or who are in
jails or prisons or referred to the mental health system by criminal courts for evaluation and
treatment.
FORM B – see Demographic Data Submission
FORMULARY – Lists of drugs that are considered preferred therapy for a given condition and
cost effective and are to be used by providers in prescribing medications.
FUNCTIONAL OUTCOMES - The extent to which individuals receiving services and supports
reach their goals. These outcomes generate from DOMAINS as defined earlier related to
desirable life developments that all people wish to achieve, such as safe and affordable
housing, employment or a means of support, meaningful relationships, participation in the life
of the community, etc.
GAPCD - Governor’s Advisory Council for Persons with Disabilities
GENERAL FUND – State funds used by the General Assembly for public programs and initiatives.
131
GEOGRAPHIC ACCESSIBILITY – A measure of access to services, which is generally determined
by drive/travel time or number and type of providers in a service area. The Contract standard is
30 minutes/30 miles.
GRIEVANCES – A formal complaint by a service recipient that shall be resolved in a specified
manner detailed in this Contract.
HEALTH CHOICE – The health insurance program for children in North Carolina that provides
comprehensive health insurance coverage to uninsured low-income children Financing comes
from a mix of federal, State, and other non-appropriated funds.
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) –Public Law 104-191,
1996 to improve the Medicare program under title XVIII of the Social Security Act, the Medicaid
program under title XIX of the Social Security Act, and the efficiency and effectiveness of the
health care system, by encouraging the development of a health information system through
the establishment of standards and requirements for the electronic transmission of certain
health information. The Act provides for improved portability of health benefits and enables
better defense against abuse and fraud, reduces administrative costs by standardizing format of
specific healthcare information to facilitate electronic claims, directly addresses confidentiality
and security of patient information - electronic and paper-based, and mandates “best effort”
compliance.
HIPAA - Health Insurance Portability and Accountability Act
HUD - Housing and Urban Development
HUMAN RIGHTS COMMITTEE – The body established by statute for hearing grievances and
appeals related to rights violations guaranteed by law and under this contract.
IDD – Intellectual or Developmental Disability
INCURRED BUT NOT REPORTED (IBNR) - means liability for services rendered for which claims
have not been received. Refers to claims that reflect services already delivered, but, for
whatever reason, have not yet been reimbursed. Failure to account for these potential claims
could lead to inaccurate financial estimates.
INSURANCE WITHIN MOA
INTEGRATED PAYMENT AND REPORTING SYSTEM (IPRS) - An electronic, web-based system for
reporting services and making payments that will eventually replace the Willie M., Thomas S.,
and Pioneer systems of claims processing The IPRS system will be built on the existing Medicaid
Management Information System (MMIS) currently processing Medicaid claims for the Division
of Medical Assistance, (DMA). The goal of the IPRS project is to replace the existing UCR
132
systems with one integrated system for processing and reporting all MH/DD/SAS and Medicaid
claims.
JOINT COMMISSION ON ACCREDITATION OF HEALTHCARE ORGANIZATIONS (JCAHO) –Agency
that reviews the care provided by hospitals and determines whether accreditation is warranted.
LEAST RESTRICTIVE CARE – The service that can be provided in the most normative setting
while ensuring the safety and well being of the individual LENGTH OF STAY (LOS) – The amount
of time that a person remains in a service program, including hospitals, expressed in days.
LEVEL OF CARE (LOC) - A structured system for evaluating acuity and INTENSITY OF NEED
against the amount, duration and scope of service required by a consumer. For substance
abuse programs, as used in the ASAM criteria for substance abuse, this term refers to four
broad areas of treatment placement, ranging from inpatient to outpatient.
LICENSURE – A State or federal regulatory system for service providers to protect the public
health and welfare. Licensure of healthcare professionals and hospitals are examples.
LOCAL BUSINESS PLAN – In the reformed MH/DD/SA system, a comprehensive plan of local
management entities for mental health, developmental disabilities and substance abuse
services in a certain geographical area (See CoastalCare Strategic Plan)
LOCAL MANAGING ENTITY (LME) - The local administrative agency that plans, develops,
implements, and monitors services within a specified geographic area according to the terms of
this Contract including the development of a full range of services and/or supports for both
insured and uninsured individuals.
LOCAL QUALITY MANAGEMENT COMMITTEE – A cross system group of stakeholders including
the LME, providers, consumers, and family members that reviews data and trends to make
recommendations for continuous improvement in the system of care and supports.
MANAGEMENT REPORTS – Collections of data that are benchmarked to enable the agency to
compare performance against standards and to seek continuous improvement. The reports
should be comprehensive incorporating timeliness, utilization and penetration rates, customer
satisfaction, functional outcomes and compliance with various standards and terms inherent in
this Contract.
MEDICAID – A jointly funded federal and State program that provides medical expense
coverage to low-income individuals, certain elderly people and people with disabilities The
Federal government requires that the State/local government match the federal government
funds. In North Carolina, this is approximately 60% federal/40% State/local match. People
qualifying for Medicaid are “entitled” to supports and services based upon a State Medicaid
Plan that is approved by the Federal Government. That Plan describes the services and benefits
the individual is entitled to receive and the conditions of service provision.
133
MEDICAL DIRECTOR – A Board Certified Psychiatrist responsible for establishing and overseeing
medical policy throughout the system under the terms of this Contract.
MEDICAL NECESSITY - Criteria established to ensure that treatment is essential and appropriate
for the condition or disorder for which the treatment is provided. The criteria reference the
scope, amount and duration of service appropriate for levels of acuity and rehabilitative care.
MEDICARE – A federal government hospital and medical expense insurance plan primarily for
elderly people and people with long term disabilities. MEMBER HANDBOOK – A document
developed and disseminated by the Contractor according to parameters established in this
Contract to inform potential eligible and enrolled persons of their rights, responsibilities and
treatment coverage.
MEMORANDUM OF AGREEMENT (MOA) or MEMORANDUM OF UNDERSTANDING (MOU) – A
written document, signed by two or more parties, containing policies and/or procedures for
managing issues that impact more than one agency or program.
MH - Mental Health
MMIS - Medicaid Management Information System
MONITORING – Routine or focused review of documentation of services delivered by provider
agencies.
MPN – Medicaid Provider Number
MST - Multi-Systemic Therapy
NATIONAL COMMITTEE FOR QUALITY ASSURANCE (NCQA) - A non-profit organization created
to improve patient care quality and health plan performance in partnership with system
management plans, purchasers, consumers, and the public sector.
NATIONAL PRACTITIONER DATA BANK (NPDB) – A database maintained by the federal
government that contains information on physicians and other medical practitioners against
whom medical malpractice claims have been settled or other disciplinary actions that have
been taken.
NATURAL AND COMMUNITY SUPPORTS – Composed of places, things, and particularly people
who are part of our interdependent community lives and whose relationships are reciprocal in
nature.
NCQA - National Council for Quality Assurance
NEEDS ASSESSMENT - A process by which an individual or system (e.g., an organization or
community) examines existing resources to determine what new resources are needed or how
to reallocate resources to achieve a desired goal.
134
NORTH CAROLINA SUPPORT NEEDS ASSESSMENT PROFILE (NC-SNAP) – Assessment
instrument used to determine the care or supports needed by a person with developmental
disabilities.
NPI – National Provider Identifier
OPERATIONAL AND FINANCIAL REVIEW - Review of the Contractor conducted by DMH/DD/SAS
to assess compliance with contract requirements. OUTREACH - Programs and activities to
identify and encourage enrollment of individuals in need of MH/DD/SA services and/or to
encourage people who have left service prematurely to return.
PAC – Provider Advisory Council
PATIENT PLACEMENT CRITERIA (PPC) - Standards of, or guidelines for, alcohol, tobacco and
other drug (ATOD) abuse treatment that describe specific conditions under which patients
should be admitted to a particular level of care (admission criteria), under which they should
continue to remain in that level of care (continued stay criteria), and under which they should
be discharged or transferred to another level (discharge / transfer criteria). PPC generally
describe the settings, staff, and services appropriate to each level of care and establish
guidelines based on ATOD diagnosis and other specific areas of patient assessment.
PCP - Person Centered Plan
PCPM – Per Citizen Per Month. The basis on which the Contractor is paid for administrative
functions under the terms of some contracts
PEER REVIEW – The analysis of clinical care by a group of that clinician’s professional
colleagues. The provider’s care is generally compared to applicable standards of care, and the
group’s analysis is used as a learning tool for the members of the group.
PENETRATION – The extent to which the system serves those individuals expected to have a
specific medical condition, in this case persons with developmental disabilities, persons with
mental illnesses and persons with substance abuse disorders.
PERFORMANCE INDICATORS - Measurable evidence of the results of activities related to
particular areas of concern as indicated in this Contract. The measures are quantitative
indicators of the quality of care provided that consumers, payers, regulators and others could
use to compare the care or provider to other care or providers.
PERFORMANCE STANDARDS- Benchmarks an agency or provider is expected to meet. The
standards define regulatory expectations and in meeting them the agency or provider may
meet a required level for “certification” or “accreditation”.
PERSON-CENTERED PLANNING - A process focused on learning about an individual’s whole life,
not just issues related to the person’s disability. The process involves assembling a group of
135
supporters selected by the consumer who are committed to supporting the person in pursuit of
desired outcomes. Planning includes discovering strengths and barriers, establishing timelimited and identifying and gaining access to supports from a variety of community resources
prior to utilizing the community MHO/DD/SA system to assist the person in pursuit of the life
he/she wants. Person-centered planning results in a written plan that is agreed to by the
consumer and that defines both the natural and community supports and the services being
requested from the public system to achieve the consumer’s desired outcomes. The plan is
used as the basis for requesting an authorization for services.
PHYSICAL DEPENDENCE - Condition in which the brain cells have adapted as a result of
repeated exposure to a drug and consequently require the drug in order to function. If the drug
is suddenly made unavailable, the cells become hyperactive. The hyperactive cells produce the
signs and symptoms of drug withdrawal.
PLAN OF CORRECTION (POC) – A written response to findings of an audit or review that specify
corrective action, time frames and persons responsible for achieving the desired outcomes.
PREVALENCE – The estimated degree of incidence of a condition in a given population.
PREVENTION – Activities aimed at teaching and empowering individuals and systems to meet
the challenges of life events and transitions by creating and reinforcing healthy behaviors and
lifestyles and by reducing risks contributing mental illness, developmental disabilities and
substance abuse. Universal Prevention programs reach the general population; Selective
Prevention programs target groups at risk for mental illness, developmental disabilities and
substance abuse; Indicated Prevention programs are designed for people who are already
experiencing mental illness or addiction disorders.
PSR - Psychosocial Rehabilitation
RESPONSIBLE CLINICIAN - An assigned professional deemed competent and credentialed by the
Contractor to serve as a fixed point of accountability for the consumer’s PCP, monitoring and
outreach.
PRIMARY CARE - (a) Basic or general health care usually rendered by general practitioners,
family practitioners, internists, obstetricians and pediatricians—often referred to as primary
care practitioners. (b) Professional and related services administered by an internist, family
practitioner, obstetrician-gynecologist or pediatrician in an ambulatory setting, with referral to
secondary care specialists, as necessary.
PRIMARY SOURCE VERIFICATION – A process through which an organization validates
credentialing information from the organization that originally issued the credential to the
practitioner
136
PRINCIPLE DIAGNOSIS - The Principal/Primary Diagnosis is the condition established after study
to be chiefly responsible for occasioning the admission of the patient to the hospital for care.
Since the Principal/Primary Diagnosis represents the reason for the patient's stay, it may not
necessarily be the diagnosis which represents the greatest length of stay, the greatest
consumption of hospital resources, or the most life-threatening condition. Since the
Principal/Primary Diagnosis reflects clinical findings discovered during the patient's stay, it may
differ from Admitting Diagnosis.
In the case of admission to the hospital-based ambulatory surgery service or freestanding
ambulatory surgery center, the Principal/Primary Diagnosis is that diagnosis established to be
chiefly responsible for occasioning the admission to the service or center for the specific
procedure.
In the case of emergency department visits, the Principal/Primary Diagnosis Code is that
diagnosis established to be chiefly responsible for occasioning the visit to the Emergency
Department.
PRIORITY POPULATIONS – Groups of people within target populations who are considered
most in need of the services available within the system.
PRIVILEGING – Process for determining, usually through training and supervision that an
individual provider has the necessary skills and knowledge to offer designated services and can
provide them without supervision.
PROMPT SERVICES - Services provided when needed. For target or priority populations, routine
appointments within 14 days, initial hospital discharge visits within 3 days, urgent visits within 2
days, emergent visits immediately and no later than 24 hours qualify as prompt.
PROVIDER – A person or an agency that provides MH/DD/SA services, treatment, and supports
under a subcontract to the LME.
OPERATIONS MANUAL – A document attached to a subcontract for the purpose of explaining
how to work with the local system, the requirements for service delivery, authorization, claims
submission, etc.
PROVIDER PROFILING – The process of compiling data on individual provider patterns of
practice and comparing those data with expected patterns based on national or local statistical
norms. The data may include medication prescribed, hospital length of stay, size of caseload,
and other services. Some data may be compiled for use by consumers in choosing preferred
providers based on performance indicators.
PUBLIC MENTAL HEALTH, DEVELOPMENTAL DISABILITIES AND SUBSTANCE ABUSE SERVICES
SYSTEM – The network of managing entities, service providers, government agencies,
137
institutions, advocacy organizations, and commissions and boards responsible for the provision
of publicly funded services to consumers
QA - Quality Assurance
QI - Quality Improvement
QIC - Quality Improvement Committee
QM - Quality Management
QP – Qualified Professional
QPN - Qualified Provider Network
QUALIFIED PROVIDER NETWORK – The group of subcontractors subcontracted by a Contractor
to provide supports and services to persons for whom the Contractor authorizes care.
QUALITY ASSURANCE (QA) - Involves periodic monitoring of compliance with standards.
QUALITY IMPROVEMENT (QI) - Process to assure that services, administrative processes, and
staff are constantly improving and learning new and better ways to provide services and
conduct business. As distinct from QA, the purpose of QI, also referred to as continuous quality
improvement (CQI) is to continuously improve the process and outcome (quality) of
treatments, services, and supports provided to consumers and administrative functions.
QUALITY OF CARE-as defined by the Institute of Medicine: “Quality of care is the degree to
which health services for individuals and populations increase the likelihood of desired health
outcomes and are consistent with current professional knowledge.”
QUALITY OF SERVICE-which may include factors such as hours of operation, ease of access to
the premises, service continuum, accreditation and staff credentials.
QUALITY MANAGEMENT (QM) - The framework for assessing and improving services and
supports, operations, and financial performance. Processes include: QUALITY ASSURANCE, and
QUALITY IMPROVEMENT.
RECOVERING STAFF - Counselors with and without educational degrees working in the
substance abuse treatment fields who are in recovery.
RECOVERY – A personal process of overcoming the negative impact of a disability despite its
continued presence. Like the victim of a serious accident who undergoes extensive physical
therapy to minimize the impact of damaging injuries, people with active addictions as well as
serious, disabling mental illnesses and developmental disabilities can also make substantial
138
recovery through symptom management, psychosocial rehabilitation, other services and
supports, and encouragement to take increasing responsibility for self.
REFERRAL - Establishing a link between a person and another service or support by providing
authorized documentation of the person’s needs and recommendations for treatment,
services, and supports. It includes follow–up in a timely manner consistent with best practice
guidelines.
REGISTER – The process of gathering initial data and entering an individual into the service
system.
REVENUES – Money earned through reimbursements paid for by covered services or other local
sources, such as grants, etc.
RFP/RFI – Request for Proposal/ Request for Information
SA - Substance Abuse
SAPT - Substance Abuse Prevention and Treatment
STR - SCREENING/TRIAGE – An abbreviated assessment or series of questions intended to
determine whether the person needs referral to a provider for services based on eligibility
criteria and acuity level. A screening may be done face-to-face or by telephone, by a clinician or
paraprofessional who has been specially trained to conduct screenings. Screening is a core or
basic service available to anyone who needs it whether or not they meet criteria for target or
priority populations.
SEAMLESS - Treatment system without gaps or breaks in service, such that persons being
served transition smoothly and with ease from one treatment component to another.
SELF-DETERMINATION – The right to and process of making decisions about one’s own life.
SENTINEL EVENT – CRITICAL INCIDENT, UNUSUAL INCIDENT, ETC. A sentinel event may include
any type of incident that is clinically undesirable and avoidable. Sentinel events signal episodes
of reduced quality of care. Many organizations monitor medication errors, review of deaths,
accidents, evacuation drill responses, rights violations, medical emergencies, use of restraint or
seclusion, behavior management etc. The purpose of sentinel event monitoring is to discover
root causes and implement a continuous improvement process to prevent further events.
SEVERELY EMOTIONALLY DISTURBED (SED) – A designation for people less than 18 years of age
who, because of their diagnosis, the length of their disability and their level of functioning, are
at the greatest risk for needing services.
SEVERELY MENTALLY ILL (SMI) – Refers to adults with a mental illness or disorder that is
described in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, that impairs
or impedes functioning in one or more major areas of living and is unlikely to improve without
139
treatment, services and/or supports. People with serious mental illness are a target or priority
population for the public mental health system for adults.
SERIOUSLY AND PERSISTENTLY MENTALLY ILL (SPMI) – Refers to people with a mental illness
or disorder so severe and chronic that it prevents or erodes development of functional
capacities in primary aspects of daily life such as personal hygiene and self care, decisionmaking, interpersonal relationships, social transactions, learning and recreational activities.
SPECIALIST REVIEW – A consultation or second opinion rendered by a member of the UM staff
when an authorization request falls outside the defined criteria for service selection, amount or
duration.
STANDARD OF CARE – A diagnostic and/or treatment consensus that a clinician should follow
when providing care based upon the discipline’s peer group organization, such as the APA or
NASW.
STATE – Refers to the State of North Carolina.
STATE FUNDED – funded by the state of North Carolina (non-Medicaid)
STATE MENTAL HEALTH AUTHORITY – The single State agency designated by each State’s
governor to be responsible for the administration of publicly funded mental health programs in
the State. In North Carolina that agency is the Department of Health and Human Services.
STATE MENTAL HEALTH, DEVELOPMENTAL DISABILITIES AND SUBSTANCEABUSE SERVICES
PLAN – Plan for Mental Health, Developmental Disabilities and Substance Abuse Services in
North Carolina. This Statewide plan forms the basis and framework for MH/DD/SA services
provided across the State.
STATE OR LOCAL CONSUMER ADVOCATE - The individual carrying out the duties of the State
Local Consumer Advocacy Program Office
STATE PLAN - Annual (each fiscal year) updated comprehensive MH/DD/SAS systems reform
plan derived from the systems reform statue and titled “Blueprint for Change”.
STATE PLAN (MEDICAID) - The written agreements between the State of NC and CMS which
describe how the NC DMH/DD/SAS programs meet all CMS requirements for participation in
the Medicaid program and the Children’s Health Insurance Program.
STRATEGIC PLAN -an organization's process of defining its strategy, or direction, and making
decisions on allocating its resources to pursue this strategy, including its capital and people
SUBSTANCE ABUSE(SA) – The DSM IV defines substance abuse as occurring if the person 1)
uses drugs in a dangerous, self defeating, self destructive way and 2) has difficulty controlling
his use even though it is sporadic, and 3) has impaired social and/or occupational functioning all
within a one year period.
140
THE SUBSTANCE ABUSE AND MENTAL HEALTH ADMINISTRATION OF THE FEDERAL
GOVERNMENT (SAMHSA) - SAMHSA is an agency of the U.S. Department of Health and Human
Service. It is the federal umbrella agency of the Center for Substance Abuse Treatment, Center
for Substance Abuse Prevention and the Center for Mental Health Services.
SUBSTANCE ABUSE PREVENTION AND TREATMENT BLOCK GRANT (SAPTBG) -A federal
program to provide funds to States to enable them to provide substance abuse services
SUBSTANCE DEPENDENCE - DSM IV defines substance dependence as requiring the presence of
tolerance, withdrawal, and/or continuous, compulsive use over a 1 year period.
SUBCONTRACT - Any contract between the Contractor (Contractor) and a third party for the
performance of all or a specified part of this Contract. The SUBCONTRACTOR means any third
party engaged by the Contractor, in a manner conforming to the SEC contract requirements for
the provision of all or a specified part of covered services under this Contract.
SYNAR AMENDMENT – Section 1926 of the Public Health Service, is administered through the
Substance Abuse Prevention and Treatment (SAPT) Block Grant and requires States to conduct
specific activities to reduce youth access to tobacco products. The Secretary of the US
Department of Health and Human Services is required by statute to withhold SAPT Block Grant
funds (40% penalty) from States that fail to comply with the SYNAR Amendment.
SYSTEMIC CHANGE- A change related to the whole organization
TARGET POPULATIONS – Groups of people with disabilities with attributes considered most in
need of the services available within the system; populations as identified in federal block grant
language. NON-TARGET POPULATION are those individuals with less severe disorders that can
be adequately and most cost effectively treated by the private sector, primary physicians or by
using generic community resources.
TRANSITION – The time in which an individual is moving from one life/development stage to
another. Examples are the change from childhood to adolescence, adolescence to adulthood
and adulthood to older adult.
UM - Utilization Management
UNIFORM PORTAL ACCESS - The standardized process and procedures used to ensure
consumer access to, and exit from, public services in accordance with the State Plan.
UTILIZATION MANAGEMENT (UM) - Process to regulate the provision of services in relation to
the capacity of the system and needs of consumers. This process should guard against underutilization as well as over-utilization of services to assure that the frequency and type of
services fit the needs of consumers. The administration of services or supplies which meet the
following tests: they are appropriate and necessary for the symptoms, diagnosis, or treatment
141
of the medical condition; they are provided for the diagnosis or direct care and treatment of
the medical condition; they meet the standards of good medical practice within the medical
community in the service area; they are not primarily for the convenience of the plan member
or a plan provider; and they are the most appropriate level or supply of service which can safely
be provided. This function is carried out by professionals qualified in disciplines related to the
care being authorized and requires their use of tools such as service definitions, level of care
criteria, etc.
UTILIZATION - The use of services. Utilization is commonly examined in terms of patterns or
rates of use of a single service or type of service. Use is expressed in rates per unit of
population at risk for a given period such as the number of admissions to the hospital per 1,000
persons per year, or the number of services provided per 1,000 persons by a system of care
annually.
UTILIZATION REVIEW (UR) –An analysis of services, through systematic case review, with the
goal of reviewing the extent to which necessary care was provided and unnecessary care was
avoided. The examination of documents and records to assure that services that were
authorized were in fact provided in the right amount, duration and scope, within the time
frames allotted; and that consumers benefit from the service. The review also examines
whether the actual request for authorization was valid in its assessment of the consumer and
the intensity of need. There are a variety of types of reviews that may occur concurrent with
the care being provided, retrospectively or in some cases prospectively if there are questions
about the authorization.
VERIFICATION OF EXPERIENCE –primary source confirmation of information that has been
provided by a potential employee to serve as work experience that would contribute to
qualifications for Qualified Mental Health/Substance Abuse/Developmental Disability
Professional status or to meet service definition requirements
142
Appendices
143
Official Communication Memos
CoastalCare Communication Memos can be found on the CoastalCare website on the provider
page.
144
Code of Ethics Policy
COASTALCARE
Section: Administration
Policy No. 105
Subject: Code of Ethics
Effective Date: July 12, 2012
Reference: URAC Core 4, 27
PURPOSE:
The purpose of this policy is to establish the agency expectations regarding staff behavior in
carrying out their official duties on behalf of the public for whom the agency serves.
POLICY:
It is the policy of this agency that employees act with ethical responsibility in the execution of their
duties; that decisions are made within the proper channels of the agency structure according to the
guidance of agency policies; that employment is not used for personal gain so that the public may
have confidence in the integrity of this public agency.
Therefore it is required that:
Employees shall act in accordance with the ethics of his/her profession as established by
the relevant licensing board.
Employees shall demonstrate compassion, honesty, integrity and respect in their dealings
with consumers, providers and the public.
Employees shall protect consumer confidentiality within the constraints of the law.
Employees shall not utilize their position with the agency for personal gain.
Any violation of this policy shall be deemed unacceptable personal conduct and will result in
disciplinary action up to or including termination of employment.
Revision History:
145
Revision
0
Date
Description of changes
05/28/2009
Initial Release
11/18/2010
Annual Area Board Review
10/27/2011
Annual AB Review
07/12/2012
Adopted by CoastalCare Area Board
146
Federal State and Local Requirements
Below is a comprehensive list of federal, state and local requirements for CoastalCare
and providers. It serves as sufficient and necessary direction to providers for accessing
pertinent rules, regulations and standards. These documents change based on legislative
action, change in federal and state policy, and procedures. There is a mutual
responsibility for CoastalCare and providers to each routinely check these items for
updates on requirements. If a Provider has problems obtaining or understanding the
information referenced in this section, please contact your liaison.
Federal Rules and Regulations
Rule / Regulation
Source Access
42 Code of Federal
Regulations(CFR) 434.6 and
438.6
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=7f8797ace4aef69f7dcc39e
dc5bfbc06&tpl=/ecfrbrowse/Title42/42cfr4
38_main_02.tpl
http://www.gpo.gov/fdsys/pkg/CFR-2011title42-vol4/pdf/CFR-2011-title42-vol4sec438-10.pdf
Managed Care Organization
Contract Requirements
42 Code of Federal
Regulations(CFR) 438
Subpart F
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=7f8797ace4aef69f7dcc39e
dc5bfbc06&rgn=div6&view=text&node=4
2:4.0.1.1.8.6&idno=42
Grievances and Appeals
42 Code of Federal
Regulations(CFR) 438.114(d)
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=7f8797ace4aef69f7dcc39e
dc5bfbc06&rgn=div8&view=text&node=4
2:4.0.1.1.8.3.106.6&idno=42
Emergency and Post-Stabilization
Care Services
42 Code of Federal
Regulations(CFR) 438.206 438.208 and 438.210
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
Access Standards
42 Code of Federal
Regulations(CFR) 438.208
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=7f8797ace4aef69f7dcc39e
dc5bfbc06&rgn=div8&view=text&node=4
2:4.0.1.1.8.4.106.6&idno=42
Coordination and Continuity of
Care
42 Code of Federal
http://ecfr.gpoaccess.gov/cgi/t/text/text-
Structure and Operations Standards
42 Code of Federal
Regulations(CFR) 438
42 Code of Federal
Regulations(CFR)
438.10(c)(5)
Brief Description
Managed Care
Interpreter Services - special needs
147
Regulations(CFR) 438.214,
438.218, 438.224, 438.226,
and 438.230
Rule / Regulation
idx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
Source Access
Brief Description
42 Code of Federal
Regulations(CFR) 438.236,
438.240 and 438.242
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
Measurements and Improvement
Standards
42 Code of Federal
Regulations(CFR) 438.240
Quality Assessment and
Performance Improvement Program
Standards
42 Code of Federal
Regulations(CFR) 438.610(a)
and (b)
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=04802f56faafe4c208ec4ca9a8a4ef
76&c=ecfr&tpl=/ecfrbrowse/Title42/42tab
_02.tpl
http://www.gpo.gov/fdsys/pkg/CFR-2011title42-vol4/pdf/CFR-2011-title42-vol4sec438-610.pdf
42 Code of Federal
Regulations(CFR) 447.45 and
Section 1902(a) (37)(A) of
the Social Security Act
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr;sid=6c7c5c6b3672320dd28022
43e5e5793f;rgn=div5;view=text;node=42
%3A4.0.1.1.12;idno=42;cc=ecfr
Timely Claims Payment Standard
42 Code of Federal
Regulations(CFR) 438.310
through 438.370
42 Code of Federal
Regulations(CFR) 455
Subpart A
42 Code of Federal
Regulations(CFR) 456 and
438 Subpart D
42 Code of Federal
Regulations (CFR) 438.10
42 Code of Federal
Regulations(CFR) 483.430(a)
42 Code of Federal
Regulations (CFR) Part 2
Confidentiality of Alcohol
and Drug Abuse Patient
http://www.ssa.gov/OP_Home/ssact/title19
/1902.htm
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&rgn=div6&view=text&node=4
2:4.0.1.1.13.1&idno=42
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr;sid=6c7c5c6b3672320dd28022
43e5e5793f;rgn=div5;view=text;node=42
%3A4.0.1.1.14;idno=42;cc=ecfr
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr;sid=6c7c5c6b3672320dd28022
43e5e5793f;rgn=div5;view=text;node=42
%3A4.0.1.1.8;idno=42;cc=ecfr#42:4.0.1.1.
8.1.106.5
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=0d2c79637fea4d732992f2
a39cee7b04&rgn=div5&view=text&node=
42:5.0.1.1.2&idno=42#42:5.0.1.1.2.9.7.5
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=4da168159410f50d6815d
4a79a0da210&rgn=div5&view=text&node
=42:1.0.1.1.2&idno=42
External Quality Review Standards
Prohibited affiliations with
individuals debarred by Federal
agencies
Medicaid Agency Fraud Detection
and Investigation Program
Utilization Control
Information Requirement Standards
- New Enrollee Information
Participation: Facility Staffing
(Intermediate Care Facility for the
Mental Retarded (ICF-MR) for
Qualified MR Professional
Federal regulations upon the
disclosure and use of drug abuse
patient records
148
Records
5 United States Code
(U.S.C.)§ 1-13
(Public Law 95-452)
http://www.law.cornell.edu/uscode/html/us
code05a/usc_sup_05_5_10_sq2.html
Outlines mission of the Office of
Inspector General
Inspector General Act of
1978
Rule / Regulation
Source Access
5 United States Code (U.S.C.) http://www.osc.gov/haStateLocalStatute.ht
§ 1501 – 1508
m
Brief Description
Restricts the political activity of
individuals principally employed by
state or local executive agencies
Federal Political Activities
Act (Hatch Act)
31 United States Code
(U.S.C.). 3729-3733
http://www.taf.org/federalfca.htm
Federal False Claims Act
http://www.law.cornell.edu/uscode/text/31/
subtitle-III/chapter-38
Administrative remedy against any
person who makes, or causes to be
made, a false claim or written
statement to any of certain Federal
agencies
41 United States Code
(U.S.C.)
http://www.gpo.gov/fdsys/pkg/USCODE2010-title41/pdf/USCODE-2010title41.pdf
Public contracts
42 United States Code
(U.S.C.)68
http://www.law.cornell.edu/uscode/pdf/lii_
usc_TI_42_CH_68.pdf
Outlines measures, designed to
assist the efforts of affected States
in expediting the rendering of aid,
assistance, and emergency services,
and the reconstruction and
rehabilitation of devastated areas
Act to improve
patient safety and reduce incidence
of events that adversely effect
patient safety
Federal False Claims Act
31 United States Code
(U.S.C.)3801-3812
Program Fraud Civil
Remedies Act of 1986
Disaster Relief
42 United States Code
(U.S.C.)299b–21, Section
922-926
The Patient Safety and
Quality Improvement Act of
2005
42 United States Code
(U.S.C.)1320a-7 and
Section 1128 of the Social
Security Act
42 United States Code
(U.S.C.)1320a-7a
http://www.pso.ahrq.gov/statute/pl10941.pdf
http://www.law.cornell.edu/uscode/text/42/
1320a-7
http://www.socialsecurity.gov/OP_Home/s
sact/title11/1128.htm
http://www.law.cornell.edu/uscode/text/42/
1320a-7a
Exclusion of certain individuals and
entities from participation in
Medicare and State health care
programs
Civil Monetary Penalties
149
Civil Monetary Penalties Law
(CMPL)
42 United States Code
(U.S.C.)1320a-7b(b)
http://www.law.cornell.edu/uscode/text/42/
1320a-7b
Illegal remunerations
Anti-Kickback Statue
42 United States Code
(U.S.C.)§ 2000d –2000d-7
http://www.justice.gov/crt/about/cor/coord/
titlevistat.php
Prohibits discrimination on the
basis of race, color, and national
origin in programs and activities
receiving federal financial
assistance.
Title VI of the Civil Rights
Act of 1964
Rule / Regulation
Source Access
Brief Description
42 United States Code
(U.S.C.). § 2000e – 2000e17
http://www.justice.gov/crt/about/emp/docu
ments/Title_VII_Statute.pdf
Prohibits employment
discrimination based on race, color,
religion, sex and national origin
Title VII of the Civil Rights
Act of 1964
45 Code of Federal
Regulations (CFR)
Subchapter C Parts 160,
162& 164
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?sid=057089847e76aa7928738f0754a9
2896&c=ecfr&tpl=/ecfrbrowse/Title45/45c
frv1_02.tpl
Federal Guidelines for
Administrative Data Standards and
Related Requirements
Standards for Privacy of
Health Information
American Recovery and
Reinvestment Act of 2009
http://www.hhs.gov/recovery/overview/ind
ex.html
Created to “jumpstart” economy,
create/save jobs, and put down
payment on addressing longneglected challenges
Equal Opportunity for Individuals
with Disabilities
Index to all sections and titles of the
Act
Medicaid Integrity Program
Americans with Disabilities
Act (ADA) of 1990
Balanced Budget Act of 1997
Section 1936 of the Social
Security Act
http://www.ada.gov/pubs/adastatute08.pdf
http://thomas.loc.gov/cgibin/query/z?c105:H.R.2015.ENR:
http://www.ssa.gov/OP_Home/ssact/title19
/1936.htm
http://www.cms.gov/DeficitReductionAct/
Downloads/CMIP2009-2013.pdf
Comprehensive Medicaid Integrity
Plan for FY2009-2013 fraud, waste,
and abuse of the Medicaid program.
http://www.ncdhhs.gov/dma/program%20i
ntegrity/Special%20Bulletin102011.pdf
Special Bulletin-Program Integrity
Unit
41 United States Code
(U.S.C.). Chapter 10, Section
701
http://www.gpo.gov/fdsys/pkg/USCODE2009-title41/pdf/USCODE-2009-title41chap10-sec701.pdf
Drug-free Workplace Requirements
Drug-Free Workplace Act of
1998
Emergency Support Function
#8
http://www.fema.gov/pdf/emergency/nrf/nr
f-esf-08.pdf
Outlines mechanisms for
coordinated Federal assistance to
supplement State, tribal, and local
Centers for Medicare &
Medicaid Services (CMS)
Medicaid Integrity Program
150
resources in response to a public
health and medical disaster
Promoting Quality and Efficient
Healthcare in Federal Government
Administered or Sponsored Health
Care Programs. CMS Quality
Framework
Executive Order 13410
http://archive.hhs.gov/valuedriven/index.ht
ml
Fair Labor Standards Act
(FLSA)
http://www.dol.gov/whd/regs/statutes/Fair
LaborStandAct.pdf
Family and Medical Leave
Act (FMLA)
http://ecfr.gpoaccess.gov/cgi/t/text/textidx?c=ecfr&sid=d178a2522c85f1f401ed3f
3740984fed&rgn=div5&view=text&node=
29:3.1.1.3.54&idno=29
The establishment of fair labor
standards in employments
(05/2011)
Outlines to take job-protected,
unpaid leave, or substitute
appropriate paid leave for “eligible”
employees of a covered employer
Source Access
Brief Description
Health Information
Technology for Economic
and Clinical Health
(HITECH) Act
http://www.hhs.gov/ocr/privacy/hipaa/adm
inistrative/enforcementrule/hitechenforcem
entifr.html
Health Information Technology for
Economic and Clinical Health
(HITECH) Act
Health Insurance Portability
and Accountability Act
(HIPAA) of 1996
http://www.hhs.gov/ocr/privacy/hipaa/adm
inistrative/statute/index.html
Homeland Security
Presidential Directive/HSPD5
Occupational Safety and
Health (OSH) Act of 1970
http://www.fas.org/irp/offdocs/nspd/hspd5.html
Standards and requirements for
transmitting certain health
information to improve the
efficiency and effectiveness of the
health care system while
protecting patient privacy
Management of Domestic Incidents
Rule / Regulation
Office of Management and
Budget – Circular A-133
Office of Management and
Budget – Circular A-87
http://www.osha.gov/pls/oshaweb/owasrch
.search_form?p_doc_type=OSHACT&p_t
oc_level=0&p_keyvalue=&p_status=CUR
RENT
http://www.whitehouse.gov/sites/default/fil
es/omb/assets/OMB/circulars/a133_compli
ance/2011/Compliance_Supplement_Marc
h-2011.pdf
http://www.whitehouse.gov/omb/circulars_
a087_2004
Office of Workers’
Compensation Programs
http://www.dol.gov/owcp/
Patient Protection and
http://www.healthcare.gov/law/full/
Safe and healthful working
conditions for working men and
women
Provides for the issuance of a
Compliance Supplement to assist
auditors in performing the required
audits
Standards for determining costs for
Federal awards carried out through
grants, cost reimbursement
contracts, and other agreements
with State and local governments
Outlines the four major disability
compensation programs which
provide wage replacement benefits,
medical treatment, vocational
rehabilitation and other benefits to
certain workers or their dependents
Quality, affordable healthcare for
151
Affordable Care Act
(PPACA)
all Americans
Public Law 103-227
Part C
http://www2.ed.gov/policy/elsec/leg/esea0
2/pg56.html
Smoking prohibition
Public Law 106-390
http://www.disastersrus.org/fema/stafact.ht
m
Federal Emergency Management
Findings, Declarations and
Definitions
Robert T. Stafford Disaster
Relief and Emergency
Assistance Act
http://www.au.af.mil/au/awc/awcgate/crs/rl
33090.pdf
Public Law 109-171
http://www.gpo.gov/fdsys/pkg/PLAW109publ171/pdf/PLAW-109publ171.pdf
Federaland State Roles in
Declarations of an
Emergency(2005)
Key Medicaid Program Revisions
Deficit Reduction Act (DRA)
of 2005
Rule / Regulation
Public Law 111-5, Section
5006 of the American
Recovery and Reinvestment
Act (ARRA)
Public Law 111–152
Source Access
Brief Description
http://www.gpo.gov/fdsys/pkg/PLAW111publ5/pdf/PLAW-111publ5.pdf
Services by Indian Health Care
Providers
http://www.gpo.gov/fdsys/pkg/PLAW111publ152/pdf/PLAW-111publ152.pdf
Section 1867 of the Social
Security Act
http://www.ssa.gov/OP_Home/ssact/ssacttoc.htm
http://www.ssa.gov/OP_Home/ssact/title18
/1867.htm
Section 1877 of the Social
Security Act
http://www.socialsecurity.gov/OP_Home/s
sact/title18/1877.htm
Guidelines to help lower the
funding requirement for compliance
program to anyone who receives
any federal funding
Allows private individuals to file
lawsuits under the Federal False
Claims Acts on behalf of the federal
and state governments to recover
funds stolen through fraud.
Table of Contents for the Social
Security Act
Examination and Treatment for
Emergency Medical Conditions and
Women in Labor
Limitation on certain physician
referrals
Stark Law
Title 19 of the Social Security
Act
http://www.ssa.gov/OP_Home/ssact/title19
/1900.htm
Grants to States for Medical
Assistance (Sections 1900 -1946)
http://www.ssa.gov/OP_Home/ssact/title19
/1903.htm
Disclosure of business transaction
information - parties of interest
Health Care and Education
Reconciliation Act of 2010
Qui Tam or Whistleblower
Provisions
Social Security Act
Sections 1903(m) (2) (A)
(viii) and 1903(m) (4) of the
Social Security Act
http://baronandbudd.com/areas-ofpractice/qui-tam-false-claims-act/qui-tamwhistleblower-provisions/
Public Health Service Act
152
Section 1905(r)(5) of the
Social Security Act
http://www.ssa.gov/OP_Home/ssact/title19
/1905.htm
EPSDT Services
The Rehabilitation Act of
1973, Section 503
http://www.dol.gov/compliance/laws/comp
-rehab.htm
U.S. Sentencing Guidelines
http://www.ussc.gov/Guidelines/index.cfm
Act prohibits discrimination and
requires employers to take
affirmative action to hire, retain,
and promote qualified
individuals with disabilities.
Sentencing guidelines, legal
offenses, penalties
State Rules/Regulations
Rule / Regulation
Source Access
10A North Carolina
Administrative Code (NCAC)
26B
http://reports.oah.state.nc.us/ncac/title%20
10a%20%20health%20and%20human%20services
/chapter%2026%20%20mental%20health,%20general/subchap
ter%20b/subchapter%20b%20rules.html
Rule / Regulation
Source Access
Brief Description
NC Mental Health Confidentiality
Rules
Brief Description
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8-A
http://www.ncdhhs.gov/dma/mp/8A.pdf
Enhanced Mental Health and
Substance Abuse Services
(08/2011)
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8B
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8C
http://www.ncdhhs.gov/dma/mp/8B.pdf
Inpatient Behavioral Health
Services Provided
http://www.ncdhhs.gov/dma/mp/8C.pdf
Outpatient Behavioral Health
Services Provided by Direct
Enrolled Providers
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8D-1
http://www.ncdhhs.gov/dma/mp/8D1.pdf
Psychiatric Residential Treatment
Facilities for Children under the
Age of 21
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8D-2
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8E
http://www.ncdhhs.gov/dma/mp/8D2.pdf
Residential Treatment Services
http://www.ncdhhs.gov/dma/mp/8E.pdf
Intermediate Care Facilities for
Individuals with Mental Retardation
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8L
http://www.ncdhhs.gov/dma/mp/8L.pdf
Targeted Case Management for
Mental Health and Substance Abuse
153
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8M
http://www.ncdhhs.gov/dma/mp/8M.pdf
Community Alternatives Program
for Persons with Mental Retardation
and Developmental Disabilities
(CAP- MR/DD)
Division of Medical
Assistance (DMA) Clinical
Coverage Policy 8N
http://www.ncdhhs.gov/dma/mp/8n.pdf
Intellectual and Developmental
Disabilities Targeted Case
Management
Division of Medical
Assistance (DMA) Clinical
Coverage Policy – 8O
http://www.ncdhhs.gov/dma/mp/A4.pdf
Services for Individuals with
Intellectual and Developmental
Disabilities with Mental Health or
Substance Abuse Co-Occurring
Disorders
Division of Medical
Assistance (DMA) Medicaid
Bulletins
http://www.ncdhhs.gov/dma/bulletin/index
.htm
N.C. Medicaid general and special
bulletins
NC Division of MH/DD/SAS
Policies
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Policy/index.htm
NC Division of MH/DD/SAS
Policies
NC Statewide Technical
Architecture – Security
Domain
http://www.ncsta.gov/library/pdf/Security.
pdf
Guidelines to implement proven
security policies, procedures and
controls
Rule / Regulation
Source Access
Brief Description
NCDivision of MH/DD/SAS
North Carolina Department of
Health and Human Services
(DHHS) and LME
Performance Contract
Attachment I – Scope of
Work
Attachment II –
Performance
Expectations
Attachment III –
Financing
Attachment IV – Data
Use Agreement
Attachment V –
Informatics Center
System Access
Agreement
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Contracts/DHHSLMESFY11Contract.pdf
Performance Contracts and outline
of contract reporting requirements
NCDivision of MH/DD/SAS
– Block Grant Audit Tools
for Substance Abuse and
Community Mental Health
http://www.ncdhhs.gov/mhddsas/providers
/Audits/index.htm
Index of State audits and
monitoring assessments
154
NCDivision of MH/DD/SAS
– Community Alternatives
Program for Persons with
MR/DD (CAP MR/DD)
Manuals
http://www.ncdhhs.gov/mhddsas/provide
rs/CAPMRDD/cap-waiverforumfacts9-2408.pdf
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/cap-compmanual7-21.pdf
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/cap-supportsmanual721.pdf
NCDivision of MH/DD/SAS
– Community Systems
Progress Reports
NCDivision of MH/DD/SAS
– Developmental Disabilities
Service Definitions
NCDivision of MH/DD/SAS
– Disaster preparedness
Response and Recovery Plan
for the State
NCDivision of MH/DD/SAS
– Guide to Standardized
Administration of the
Frequency & Extent
Monitoring Tool and the
Provider Monitoring Tool
Overview of New CAP-MR/DD
Waivers
2008 CAP-MR/DD
Comprehensive Waiver (Released
7/21/10)
2008 CAP-MR/DD
Supports Waiver (Released
7/21/10)
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Reports/DivisionInitiativeReports/c
ommunitysystems/index.htm
http://www.ncdhhs.gov/mhddsas/providers
/developmentaldisabilities/index.htm
Quarterly progress report on
performance indicators as outlined
in the contract
Index of information regarding
Developmental Disabilities
http://www.ncdhhs.gov/mhddsas/services/
disasterpreparedness/
Information for State Disaster
Preparedness
http://www.ncdhhs.gov/mhddsas/providers
/providerendorsement/revisedfempmtmanual11-12-10.pdf
Senate Bill 163 monitoring process
and specific instructions on the use
of each tool
Rule / Regulation
Source Access
Brief Description
NCDivision of MH/DD/SAS
– Implementation Updates
http://www.ncdhhs.gov/mhddsas/impleme
ntationupdates/index.htm
Index of Enhanced benefit services
updates
NC Division of MH/DD/SAS
– LME and Provider Contract
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Contracts/contractlmeprovider.pdf
Outlines provider contract
requirements
NC Department of Health and
Human Services/Division of
Medical Assistance and
Managed Care Organization
(MCO) Contract
NCDivision of MH/DD/SAS
– Performance Contract
Report/Data Submission
Requirement Reports
NCDivision of MH/DD/SAS
– Provider Monitoring
http://www.ncdhhs.gov/dma/lme/MCOFIN
ALContract10042011.pdf
Outlines MCO contract
requirements
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Reports/DivisionInitiativeReports/
pc-reports/index.html
Quarterly schedule of report
submission requirements as
outlined in contract
http://www.ncdhhs.gov/mhddsas/providers
/providermonitoring/index.htm
Index of review tools for the
North Carolina Gold Star
Rating and Monitoring Process
for Providers (07/2012)
155
North Carolina
Administrative Rules –
APSM 10-6
http://www.records.ncdcr.gov/local/2011
_10_LMESchedule_Official.pdf
North Carolina
Administrative Rules –
APSM 30-1
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/apsm30-1_11-11.pdf
Records Retention and Disposition
Schedule
NCDivision of MH/DD/SAS Local
Management Entity (10/2011)
Rules for MHDDSA Facilities &
Services (11/2011)
North Carolina
Administrative Rules –
APSM 45-1
North Carolina
Administrative Rules –
APSM 45-2
North Carolina
Administrative Rules –
APSM 75-1
North Carolina
Administrative Rules –
APSM 95-2
North Carolina Division of
Health Service Regulation
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/apsm451confidentialityrules1-1-05total.pdf
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/rmdmanual-final.pdf
Confidentiality Rules for
MH/DD/SA Services Manual
(01/2005)
Record Management and
Documentation Manual (03/2009)
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/Archive/apsm751budget7-95.pdf
http://www.ncdhhs.gov/mhddsas/statspubli
cations/Manuals/apsm95-2clrights7-03.pdf
Area Program Budgeting and
Procedures Manual (07/1995)
North Carolina False Claims
Act
(House Bill 1135)
http://www.ncleg.net/Sessions/2009/Bills/
House/PDF/H1135v8.pdf
North Carolina General
Statutes 75-65
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=75-65
North Carolina General
Statute 108A-70.10
http://www.ncleg.net/gascripts/Statutes/Sta
tutesTOC.pl?Chapter=0108A
Rule / Regulation
http://www.ncdhhs.gov/dhsr/
Source Access
Client Rights Rules in Community
MH/DD/SA Services Manual
(07/2003)
Oversees medical, mental health
and adult care facilities, emergency
medical services, and local jails
Act that deters and punishes
persons who make false or
fraudulent claims for payment by
the state.
Protection from Security Breaches
NC Medicaid Fraud
Brief Description
North Carolina General
Statute 108C
http://www.ncga.state.nc.us/Sessions/2011/
Bills/Senate/PDF/S496v5.pdf
Medicaid and Health Choice
Provider Requirements
North Carolina General
Statutes 121, Section 5 & 132
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=121-5
Public Records & Archives
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=132
North Carolina General
Statutes 122C
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=122C
North Carolina General
Statutes 126
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=126
North Carolina General
Statutes 132-1.10
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=132-1.10
Public Records
Mental Health, Developmental
Disability, and Substance Abuse
Act of 1985
State Personnel System
Social Security Numbers and Other
Personal Identifying Information
156
North Carolina General
Statute 147-64.7
http://www.ncga.state.nc.us/enactedlegislat
ion/statutes/pdf/byarticle/chapter_147/artic
le_5a.pdf
State auditor access to persons and
records
North Carolina General
Statutes 159; Article 3
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=159
Local Government Budget and
Fiscal Control Act
North Carolina General
Statutes 166a-6
http://www.ncleg.net/gascripts/statutes/stat
utelookup.pl?statute=166a-6
North Carolina State of Disaster
North Carolina Health Care
Personnel Registry
https://www.ncnar.org/index1.jsp
Registry of unlicensed health care
workers, reportable allegations
registry
157






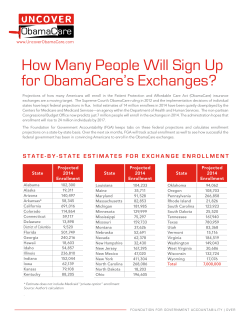



© Copyright 2025