
Prosocial Development in Relation to Children’s and Mothers’ Psychological Problems
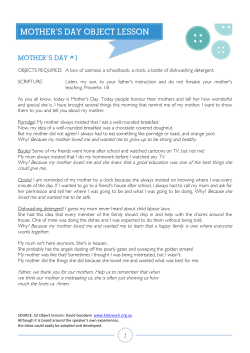
Child Development, September/October 2003, Volume 74, Number 5, Pages 1314 – 1327 Prosocial Development in Relation to Children’s and Mothers’ Psychological Problems Dale F. Hay and Susan Pawlby The study tested whether children’s prosocial behavior was negatively or positively related to children’s and mothers’ psychological problems. Participants were 149 London families when mothers were pregnant and followed up in infancy and at ages 4 and 11. Children’s cooperation at 4 and general prosocial tendencies at 11 were negatively associated with externalizing problems but unrelated to internalizing problems. A subgroup of children who were more prosocial than average expressed clinically significant worries about family members. Maternal depression decreased prosocial behavior in the eyes of adults, but children of depressed mothers saw themselves to be prosocial. Early cooperation protected children against later risk for externalizing problems, even when their early behavioral problems were taken into account. Are prosocial children free from psychological problems? Different answers might be provided to this question, depending on whether prosocial action is seen as emotionally regulated and socially competent behavior or, in some circumstances, as a sign of overconcern for the well-being of others. One aim of this study was to examine links between children’s prosocial behavior and their emotional and behavioral problems, from early childhood to early adolescence. A second aim was to determine whether mothers’ own psychological problems inhibit or facilitate children’s prosocial behavior at either point in development. In addressing these questions, we defined prosocial behavior as a broad domain of ‘‘behaviors that are positively responsive to others’ needs and welfare. y At a descriptive level, they are behaviors that are helpful and affiliative responses to others: responses to signs of suffering, need, or danger in another person or animal, such as, assisting, sharing, being kind and considerate, comforting, cooperating, Dale F. Hay, School of Psychology, Cardiff University; Susan Pawlby, Section of Perinatal Psychiatry, Institute of Psychiatry. The study began as a Ph.D. thesis by D. Sharp; follow-ups were conducted under the leadership of R. Kumar, who is now deceased. The research reported in this paper was supported by the Medical Research Council through Project Grants G89202999N and G9539876N to R. Kumar, D. Sharp, and D.Hay, and Child Psychiatry Unit funding to D. Hay. We thank Gesine Schmücker, Alice Mills, Helen Allen, and Anne O’Herlihy for help with data collection, and Adrian Angold, Gordon Keeler, and Peter Wendell at Duke University for help with the analysis of the interview data. We are grateful to the families who have participated in the South London Child Development Study for so many years. Correspondence concerning this article should be addressed to Dale Hay, School of Psychology, Cardiff University, Cardiff, Wales, CF10 3YG, United Kingdom. Electronic mail may be sent to haydf@cardiff.ac.uk. protecting someone from harm, rescuing someone from danger, and feeling empathy and sympathy’’ (Radke-Yarrow & Zahn-Waxler, 1986, p. 208). In longitudinal analyses of an urban community sample of British children, we used a multimethod, multi-informant approach to study prosocial behavior at two time points. We focused on one form of prosocial behaviorFcooperationFin early childhood. Cooperation entails working positively with other people to meet a mutual goal and thereby conveys benefits on others as well as the self (Staub, 1978). Many prosocial behaviors occur at low frequency, under particular situational constraints, but cooperation can be observed reliably in the context of brief experimental tasks (Staub, 1978) and thus can be observed systematically within a community sampling frame. Cooperation with other children and adults, and the related concept of cheerful ‘‘committed compliance’’ to reasonable requests are important aspects of prosocial development in the early years (Kochanska, Aksan, & Koenig, 1995; Rheingold, Cook, & Kowlowitz, 1987). Young children’s cooperation is positively associated with sharing (Hay, 1979) and sympathy (Murphy, 1937), and thus serves as a marker of more general prosocial tendencies. We studied a broader domain of children’s prosocial activities at age 11, as rated by mothers, teachers, and children. Standardized questionnaires have been used in past research on individual differences in prosocial behavior, showing internal consistency across prosocial items and discriminant validity between prosocial and problem scales, with r 2003 by the Society for Research in Child Development, Inc. All rights reserved. 0009-3920/2003/7405-0006 Prosocial Development and Psychological Problems moderate consistency across informants (R. Goodman, 1994; Tremblay, Vitaro, Ganon, Piché, & Royer, 1992). Prosocial Behavior and Children’s Psychological Problems The evidence regarding links between children’s prosocial behavior and psychological problems is contradictory. Prosocial behavior is linked to emotional regulation (Eisenberg et al., 1995; Fabes, Eisenberg, Karbon, Troyer, & Switzer, 1994), social competence (Chen, Li, Li, & Liu, 2000; Eisenberg et al., 1996), and moral reasoning (Carlo, Koller, Eisenberg, DaSilva, & Frolich, 1996; Miller, Eisenberg, Fabes, & Shell, 1996). In line with these findings, prosocial behavior, as one dimension of psychological adjustment, should be inversely correlated with behavioral and emotional problems. The absence of prosocial behavior in childhood predicts disruptive behavior and criminality in later life (Haemaelaeinen & Pulkinnen, 1996). Children with disruptive behavior are less likely than other children to be prosocial (Hastings, Zahn-Waxler, Robinson, Usher, & Bridges, 2000; Hughes, White, Sharpen, & Dunn, 2000; Vinnick & Erickson, 1992), and children with internalizing problems show prosocial behavior at low rates (LaFreniere, Provost, & Dubeau, 1992). In early adolescence, emotional distress is negatively related to prosocial behavior (Wentzel & McNamara, 1999). However, under some circumstances, prosocial behavior is accompanied by behavioral and emotional problems. For example, in some samples, children with externalizing problems showed prosocial behavior to the same extent as or more than other children (e.g., Del’Homme, Sinclair, & Kasari, 1994; Zahn-Waxler, Cole, Welsh, & Fox, 1995). When faced with conflict, disruptive girls showed high levels of prosocial behavior (Zahn-Waxler et al., 1994). Boys with attention deficit hyperactivity disorder (ADHD) were just as likely as other boys to show prosocial behavior (Buhrmester, Whalen, Henker, MacDonald, & Hinshaw, 1992), although stimulant medication reduced their levels of social engagement. It has also been observed that fear and sadness predict prosocial traits (Rothbart, Ahadi, & Hershey, 1994). Tests of associations between prosocial behavior and psychological problems rest on the assumption that individual differences in both domains are robust and stable over time. It is well known that behavioral problems in early childhood predict later delinquency and disorder (e.g., Moffitt & Caspi, 2001). There is also recent evidence for long-term 1315 continuities in prosocial behavior (Côté, Tremblay, Nagin, Zoccolillo, & Vitaro, 2002; Eisenberg et al., 1999). The longitudinal design used here permits tests for associations across the two domains at two time points. We also examined whether prosocial behavior in early childhood protected children against the risk of psychopathology in early adolescence. Maternal Mental Health Problems and Prosocial Development In evaluating the evidence for positive or negative associations between children’s prosocial behavior and psychological problems, it is important to take into account other psychopathology in the family. In particular, maternal depression is associated with adverse family climates and less optimal patterns of parent – child interaction (S. Goodman & Gotlib, 1999). Under these conditions, children’s prosocial development may not proceed normally. In general, positive home environments foster prosocial tendencies. Prosocial behavior is more frequent in children whose parents provide inductive reasoning (Hart, DeWolf, & Burts, 1992), acceptance of the child (Chen & Rubin, 1994), and support for the child’s relationships with peers (Ladd & Hart, 1992). Children’s prosocial behavior is associated with authoritative parenting (Dekovic & Janssens, 1992; Hastings et al., 2000) and with the modeling and reinforcement of sympathetic behavior by mothers (Eisenberg et al., 1992). Maternal depression might interfere with the provision of sensitive, authoritative parenting and therefore disrupt prosocial development. If so, the children of depressed mothers might show more psychological problems and less prosocial behavior. Support for this view was provided by analyses of a large British community sample, which demonstrated a significant negative correlation between mothers’ depressive symptoms and children’s prosocial tendencies, both measures rated by mothers (Dunn, DeaterDeckard, Pickering, O’Connor, Golding & the ALSPAC Study Team, 1998). Nevertheless, prosocial behavior can also emerge under stressful circumstances. Prosocial behavior between siblings occurs when parents quarrel (Cummings & Smith, 1994), and siblings become important sources of support for each other when their parents separate and divorce (e.g., Kier & Lewis, 1998). More generally, prosocial behavior may flower under highly adverse social conditions, such as war: Elevated rates of prosocial behavior are reported by children whose lives were disrupted by 1316 Hay and Pawlby war in Lebanon (Macksoud & Aber, 1996) and Croatia (Raboteg-Saric, Zuzul, & Kerestes, 1994). In line with this body of evidence, it is possible that the needs of a depressed mother may foster prosocial tendencies, at least for a while. Under some circumstances, maternal depression is linked to children’s empathic reactions (T. Dix, June 28, 2002, personal communication; Radke-Yarrow, Zahn-Waxler, Richardson, Susman, & Martinez, 1993; Zahn-Waxler, Cummings, McKnew, & RadkeYarrow, 1984). Indeed, children of depressed parents may become preoccupied with the parents’ problems, thus shouldering excessive prosocial responsibilities (Zahn-Waxler, Cole, & Barrett, 1991) and in some cases exhibiting internalizing problems themselves (Klimes-Dougan & Bolger, 1998). To the extent that the children of depressed mothers are generally at risk for depression and other disorders (S. Goodman & Gotlib, 1999; Rice, Harold, & Thapar, 2002), it seems possible that these children’s prosocial behavior might be associated with their own psychopathology. In addressing these issues, it is important to examine qualitative as well as quantitative features of children’s responses to other people. Children of depressed mothers who may have to take care of siblings and the mother herself may do so at some cost to themselves. In particular, they may become anxious about the possible harm that might befall their family members. We examined whether children were more likely to worry about family members when their mothers were depressed, whether their worries were positively or negatively associated with other forms of prosocial behavior, and whether worrying about others was more characteristic of girls than of boys. We recorded the incidence of clinically significant worries about other people, which is a clinical symptom of separation anxiety disorder but might also be viewed as an excessive form of prosocial concern for others. Children who show such extreme worry about their loved ones might show other forms of prosocial behavior but might also have other internalizing problems (Klimes-Dougan & Bolger, 1998). Maternal depression may exaggerate gender differences in prosocial behavior (Zahn-Waxler et al., 1991), and girls’ worries about other people may sometimes verge on the unmitigated communion shown by some women who focus on others at cost to their own health (Helgeson & Fritz, 1998). Thus, we examined whether girls and boys were equally likely to worry about the well-being of family members. The Importance of the Child’s Perspective The fact that informants about children’s prosocial behavior show only moderate consistency (e.g., R. Goodman, 1994; Tremblay et al., 1992) suggests that the perception of prosocial behavior in oneself or another is itself a complex social judgment. When children, parents, and teachers were asked to classify behaviors as prosocial or antisocial, less agreement was found in the classification of prosocial as opposed to antisocial behavior, both within and between each category of informant (Warden, Christie, Kerr, & Low, 1996). It is particularly important to canvass the child’s perspective. Children who grow up under adverse circumstances may see themselves as cooperative and sympathetic, even if their behavior is not always judged to be so by other observers. For example, in response to a story completion task, maltreated children saw themselves as likely to show positive responses to people in distress; this was despite the fact that maltreated children are generally not seen to be sympathetic in response to peers’ distress (Macfie et al., 1999). A similar discrepancy between the child’s view of the self and views by others may characterize the children of depressed mothers. Thus, in the present study, we tested for differences among informants as well as combining information from different sources to reveal the links between children’s prosocial behavior and their psychological problems. Method Design Analyses were undertaken within a representative urban sample of British children. Children’s prosocial behavior and psychological problems were assessed at two time points, when the children were nearly 4 and 11 years of age. The mother’s mental health was assessed at various points throughout the study, allowing for a diagnosis of maternal depression in the child’s lifetime and a rating of her psychological functioning at each time point. The Families The families participated in an ongoing, prospective longitudinal study of child development in two communities in South London (Sharp, 1993; Sharp et al., 1995). The families were recruited at routine prenatal check-ups, with 179 chosen at random for full psychiatric assessments before and after childbirth. In the families, 171 women gave birth to live Prosocial Development and Psychological Problems infants and 149 (87%) who were assessed at 3 months postpartum were followed up at later time points. When the child was 11 years old, 134 (90%) were available for follow-up, and 89% of those had also participated when the child was 4 years old. In 1 family the child had died, in another the child had been taken into care by the Social Services and access was denied, 2 had withdrawn from the study before the first birthday, 7 had moved abroad or could not be traced, and 4 were not willing to participate. The mother’s mean age at the start of the study was 25.8 (SD 5 5.1, range 5 16 – 43). Characteristics of the sample are presented in Table 1. In many ways, the sample is representative of the general population in Great Britain, where approximately 90% of the population lives in urban areas (Office for National Statistics, 2003). Family structure was almost identical to national norms at birth (Office for National Statistics, 2000) and, at 4 years of age, to findings in a very large community sample in the English county of Avon (Dunn et al., 1998). The rate of children’s psychological problems at age 4 was also in line with norms from that study. In other ways, the sample is representative of the sociocultural mix of a large metropolitan area. National Table 1 Characteristics of the Sample Variable Child’s sex Child’s birth order Sibling status at age 11 Marital status at birth Marital status at age 11 Parent in household at 11 Social class Maternal education Ethnicity Parental employment Description 53% female 47% firstborn 90% with siblings (median 5 2, range 5 1 – 7) 63% married, 29% cohabiting, 8% single 58% married (89% to biological father) 14% cohabiting (39% to biological father) 28% single-parent household 56% two biological parents 40% biological mother 2% biological father 2% other guardians 89% working class (Goldthorpe & Hope, 1974) 72% basic qualifications, 14% further education 72% White British, 6% White, nonBritish, 22% other (Caribbean, African, South Asian, East Asian) 75% at least one parent employed 58% maternal employment 1317 surveys show that, in the United Kingdom as a whole, the majority of families (62%) view themselves as working class, as opposed to middle class (K. Prandy, June 26, 2002, personal communication). The proportion of working class families is higher in this sample, which also includes several high-status, affluent families. The sample is also more culturally diverse than the United Kingdom as a whole, where approximately 7% of the population belongs to ethnic minorities (Office for National Statistics, 2000). Procedure A multimethod, multi-informant strategy was adopted. Experimental, observational, interview, and questionnaire methods were used, and informants included parents; teachers; testers; and, at age 11, the children themselves. Pregnancy and the first postnatal year. The mothers were interviewed at 14 and 36 weeks of pregnancy, and at 3 and 12 months postpartum (for details see Sharp, 1993). The Clinical Interview Schedule (CIS; Goldberg, Cooper, Eastwood, Kedward, & Shepherd, 1970) was used to assess the mother’s psychopathology. Fourth birthday. The families were visited at home when the children were approaching their fourth birthday. The mother’s current and past psychopathology was assessed, using the Schedule of Affective Disorders and Schizophrenia (SADS – L; Spitzer, Endicott, & Robbins, 1978). Mothers also rated the child’s psychological problems, using the Child Behavior Checklist (CBCL; Achenbach, 1988). The assessment of the child at age 4 consisted of a standardized cognitive test, the McCarthy Scales of Children’s Abilities (McCarthy, 1972), and an experimental cooperation task. After the cognitive test, the tester, who had not interviewed the mother and was unaware of her psychiatric history, rated the child’s cooperativeness. In the experimental task, pairs of mothers and children were asked to cooperate to copy a picture of a house, using an Etch-A-Sketch toy (Stevenson-Hinde & Shouldice, 1995). Mother and child were each assigned a dial to use, and told that they might not use the other person’s dial so that each person could only draw vertical or horizontal lines. By using their dials at the same time, they could produce diagonal lines. This procedure creates a situation in which two people must work together to meet interdependent goals and therefore meets the criteria of the classic definition of cooperation (Deutsch, 1949), which provides the conceptual basis for most experimental 1318 Hay and Pawlby cooperative tasks (e.g., Brownell & Corriger, 1990; Rose-Krasnor, Rubin, Booth, & Coplan, 1996). 11th birthday. When the child was age 11, one researcher assessed the mother’s mental health currently and retrospectively to the last visit, and her level of functioning in the week preceding the interview. The mothers also reported on the child’s psychological problems and prosocial behavior, using the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1999). The mother was also interviewed in much more detail about the child’s clinically significant psychological problems, using the Child and Adolescent Psychiatric Assessment (CAPA; Angold et al., 1995). A second researcher, unaware of the mother’s psychiatric history, interviewed the child. The SDQ was read to the child as part of an interview that also included the CAPA. All parents gave permission for the class teachers to complete the SDQ. Teachers’ reports were available for all but one child, who was taught at home. Measures Cooperativeness in early childhood. The primary measures of prosocial behavior at age 4 were the tester’s rating of cooperativeness during the cognitive test and an observational measure of cooperation with the mother during the Etch-A-Sketch task. The Tester’s Rating of Children’s Behavior (TRCB; Wolke, 1990) had been adapted from a rating scale of infant behavior (Wolke, Skuse, & Mathisen, 1990). Cooperativeness with the tester was rated on a 9-point scale ranging from very resisting and uncooperative (1) to very cooperative, readily and enthusiastically entering into the tasks (9). Behaviors shown by mothers and children during the Etch-A-Sketch task were rated using an observational coding system specifically designed for the study (Sharp et al., 1995). Two 9-point scales, measuring the child’s engagement in and persistence at the cooperative task, were summed to produce a composite measure of the child’s contribution to the cooperative task. Behaviors indicating the child’s cooperation with the mother included looking at and listening to her, as signs of mutual engagement; incorporating her suggestions, directions, and demands; and turn taking and reciprocity. In other words, these ratings reflect the extent to which the child engaged with the mother in the mutual task and persisted in attempting to attain the mutual goal. Observers of the video records were unaware of the mother’s diagnostic status. Observer agreement, measured by intraclass correlation coef- ficients, was .87 and .72 for engagement and persistence, respectively. General prosocial tendencies at age 11. When the child was age 11, a more general assessment of prosocial behavior was made, using the SDQ. The SDQ is a 25-item questionnaire on prosocial behaviors and symptoms of childhood disorder (R. Goodman, 1999; R. Goodman, Meltzer, & Bailey, 1998). The prosocial scale consists of 5 items: (1) considerate of other people’s feelings; (2) shares readily with other children (treats, toys, pencils, etc.); (3) helpful if someone is hurt, upset or feeling ill; (4) kind to younger children; and (5) often volunteers to help others (parents, teachers, other children). Past research has demonstrated internal consistency of the prosocial scale and its discriminant validity in terms of negative associations with the problem scales of the SDQ (e.g., Dunn et al., 1998). In the present study, the prosocial scale showed acceptable levels of internal consistency (a 5 .68 for children, a 5 .85 for teachers, and a 5 .72 for mothers). Children’s ratings of prosocial behavior were correlated with teachers’ ratings, r(129) 5 .26, po.002, and with mothers’ ratings, r(126) 5 .19, po.03. Teachers’ ratings were significantly correlated with mothers’ ratings, r(125) 5 .44, po.001. Measures of the child’s psychological problems. When the child was age 4, mothers rated the child’s behavioral and emotional problems on the CBCL. Higher scores indicate more problems. Because the children in this study were not quite 4 years of age at the time of assessment, the 2- to 3-year-old version of the CBCL was used. The internalizing and externalizing subscales were highly correlated in this sample, r(114) 5 .78, po.001. Measures of the child’s psychological problems at age 11 were obtained from the SDQ and CAPA. The SDQ scales provide continuous measures of children’s behaviors across the normal and abnormal range. For the purpose of the present study, the conduct problems and hyperactivity scales were summed to form a general measure of externalizing problems. The composite measure showed good internal consistency, a 5 .72 for children, a 5 .90 for teachers, and a 5 .82 for mothers. In all cases the consistency of the composite externalizing measure was better than that achieved by the original scales. The emotional problems scale was used as a measure of internalizing problems (a 5 .60 for children, a 5 .72 for teachers, and a 5 .66 for mothers). The CAPA is a semistructured diagnostic interview that takes on average 2 to 3 hr to complete. The Prosocial Development and Psychological Problems interviewer asks a series of questions about family structure and relationships, peer relations, and problems in the domains of several clinical disorders, including ADHD, conduct disorder, oppositional-defiant disorder, anxiety disorders, and depression. The parent and child, who were interviewed separately, were asked to recount details about particular behaviors and events during the last 3 months. Interviewers used operational criteria to determine if and when a symptom of clinical significance occurred, when it had begun, and how long it persisted. Thus, whereas the SDQ provides continuous measures about the child’s behavior throughout the normal range, the CAPA is designed to detect symptoms of childhood psychiatric disorder, according to Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria. The analysis of the CAPA measures was conducted on the subsample of 122 families in which both parent and child had successfully completed the interview. Measures of externalizing and internalizing symptoms reported by parent and child were obtained, using definitions retained from the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev. [DSM – III – R]; American Psychiatric Association, 1987), in which the distinction between internalizing and externalizing problems had been made. Because most children did not manifest severe psychiatric symptoms, these distributions were skewed; therefore, logarithmic transformations were used in subsequent analyses. We also identified children with particularly severe problems, meeting Diagnostic and Statistical Manual of Mental Disorders (4th ed. [DSM – IV]; American Psychiatric Association, 1994) criteria for emotional disorders and disruptive behavior disorders (DBD). Mothers’ and children’s joint reports were used to identify children meeting caseness criteria. Computer algorithms were used to determine which children met the operational definitions of DSM – IV disorders. ‘‘Worries about family members’’ at age 11. When the child was age 11, a self-report measure of worrying about family members was obtained from the child’s CAPA interview. In the separation anxiety section of the CAPA, a series of questions tap the child’s excessive worries about possible harm that might befall attachment figures. Symptomatic behaviors include ‘‘unrealistic and persistent worry or fear about possible harm befalling major attachment figures’’ or ‘‘rising at night to check that attachment figures are still present and/or free from harm.’’ The interviewer probes for particular instances of such behavior and uses operational criteria to determine 1319 whether the child was showing this symptom of separation anxiety. Diagnostic algorithms used information about this symptom in combination with other symptoms to assess the child’s caseness for separation anxiety disorder. The occurrence of this symptom alone does not provide a diagnosis of separation anxiety disorder. Here, we examined the presence of this clinically significant symptom as an index of the child’s self-reported tendency to feel great anxiety about the welfare of family members. Measures of maternal depression. The interviews used in pregnancy and immediately after the birth of the child using the CIS permitted contemporaneous diagnoses of depression using International Classification of Diseases (ICD-9) criteria. The interviews given at 4 and 11 years of age, using the SADS – L provided contemporaneous and lifetime diagnoses of depression in line with research diagnostic criteria (RDC) criteria. Both sets of criteria identify clinically significant cases of depression. The CIS was developed for use in community settings (Goldberg et al., 1970). In this study, the women were asked about 10 specific psychiatric symptoms occurring in the 2-week period before the interview; the interviewer also rated 12 manifest abnormalities of behavior and affect shown during the interview. A rating was made on a 5-point scale for each of the 10 symptoms, after establishing the frequency, severity, and duration of each. The ratings produced a total weighted score and a case – noncase distinction. An ICD-9 diagnosis of depression was then assigned to cases (World Health Organization, 1978). The SADS – L (Spitzer et al., 1978) was used at the 4- and 11-year-old assessments to provide detailed information about the respondent’s mental health, both current and retrospective. Diagnoses of depression in line with RDC were made after discussion with an adult psychiatrist (R. Kumar). In addition, a continuous measure of the mother’s psychological functioning in the weeks preceding the 4- and 11year assessments was provided by the Global Assessment Scale (GAS; Endicott, Spitzer, Fleiss, & Cohen, 1976). This rating scale evaluates the overall functioning of a participant during a specified period on a continuum (1 to 100) from psychological or psychiatric sickness to health. Higher scores reflect better levels of functioning. The contemporaneous and retrospective assessments of maternal depression at various points in the study produced two summary variables: (a) current functioning (the mother’s GAS scores at the 4- and 11-year assessments) and (b) depression during the child’s lifetime (caseness for depression, 1320 Hay and Pawlby using either ICD-9 or RDC criteria, at any point since the child’s birth). Data Analysis Construction of composite variables. When examining correlations over time and across the domains of prosocial behavior and psychological problems, reliability is increased if composite measures are used. The assessments of cooperation at age 4 were analyzed separately, as they were only modestly correlated and were conducted in very different contexts. However, because the reports of prosocial behavior at age 11 all derive from the SDQ, a principal components analysis was conducted, yielding a single prosocial factor, which accounted for 53% of the variance in the informants’ reports. The factor score was used in subsequent tests for association between prosocial behavior and psychological problems. Similarly, to achieve more reliable measures of the children’s psychological problems, we combined information across informants and methods. The three informants’ reports of externalizing and internalizing problems on the SDQ and the logarithmically transformed measures of externalizing and internalizing symptoms on the CAPA were entered into a principal components analysis. Because of the theoretical distinction between internalizing and externalizing problems, a two-factor solution was sought. The analysis indeed yielded two orthogonal factors, accounting for 50.2% of the variance in the informants’ reports on the two instruments, which were then used as composite measures of internalizing and externalizing problems. Tests for links between prosocial behavior and psychological problems. To address the first aim of the study, the analysis for links between children’s prosocial behavior and their psychological problems, the composite measure of prosocial behavior was correlated with the composite measures of internalizing and externalizing symptoms. The children’s severe problems of clinical concern were dichotomous variables (diagnoses of disorder and presence of the key symptom of worrying about family members). Therefore, the relationship between these dichotomous measures of the child’s mental health and prosocial behavior was assessed through tests of differences between ill and well children, using t tests and analysis of variance (ANOVA) in cases in which the child’s sex was included in the model. Tests for the influence of maternal depression. To meet the second aim of the studyFanalysis for the effects of the mother’s illness on prosocial behavior FANOVAs were used to test for the effects of maternal depression on each measure of cooperation at age 4. When the child was age 11, because of the importance of retaining the child’s perspective, the effects of the mother’s illness were assessed with respect to each informant’s report. The main effect of informant and the interaction of informant with maternal depression were tested in a repeatedmeasures ANOVA. Long-term prediction of children’s psychological problems. A final set of analyses addressed both aims of the study longitudinally, testing whether cooperative behavior in early childhood predicted the composite measures of externalizing and internalizing symptoms in early adolescence, taking into account the mother’s history of depression. Multiple regression analyses controlled for the effects of the child’s gender, the mother’s depression, and the child’s earlier problems. Results Links Between Children’s Prosocial Behavior and Their Psychological Problems Cooperativeness at age 4. Children who were more engaged in the cooperative task with their mothers had significantly fewer problems on the CBCL, r(112) 5 – .18, po.05. In particular, they had fewer externalizing problems (Table 2), although that association only approached statistical significance. The tester’s rating of cooperativeness was not significantly linked to the child’s problems. General prosocial tendencies at age 11. Prosocial children were no more or less likely than other children to have emotional problems. There was no significant association between the composite prosocial score and the composite measure of internalizing problems (Table 2). Furthermore, children diagnosed with clinically significant emotional disorder were no more or less likely than other children to show prosocial behavior. Twenty children (16.4% of those with complete CAPA data) met diagnostic criteria for an emotional disorder on the basis of the mothers’ and children’s joint reports on the CAPA interview. A 2 2 ANOVA was used to test for the effects of diagnostic status and the child’s sex on the composite measure of prosocial tendencies. There was no effect of the child’s diagnosis of an emotional disorder, nor of the child’s sex, nor a significant interaction. In contrast, prosocial behavior was inversely related to externalizing problems (Table 2). Furthermore, the negative relation between externalizing Prosocial Development and Psychological Problems 1321 Table 2 Pairwise Correlations Between Measures of Prosocial Behavior and Problems at Ages 4 and 11 (Pearson r, N) Measure 1.Cooperation with mother at 4 2. Cooperation with tester at 4 3. Prosocial score at 11 4. CBCL externalizing score at 4 5. CBCL internalizing score at 4 6. Externalizing factor score at 11 7. Internalizing Factor score at 11 Variable M Variable SD 1 2 0.19 (115) 3 4 5 6 7 0.09 (109) 0.18+ (112) 0.13 (112) 0.30 (105) 0.07 (105) .00 (107) 0.12 (114) 0.16+ (114) 0.15 (107) 0.07 (107) 0.24 (109) 0.21 (109) 0.78 (114) 0.56 (118) 0.42 (106) 0.07 (118) 0.10 (106) 0.30 (106) 0.19+ (106) 0.00 (118) 12.0 4.8 5.3 2.0 0.0 1.0 49.6 10.2 49.9 9.8 0.0 1.0 0.0 1.0 po.10. po.05. po.01. po.001. + problems and prosocial behavior was also found with respect to clinically significant disorder. Twenty children (16.4% of those with complete CAPA data) were diagnosed with DBD according to DSM – IV criteria. Of these, 9 (45%) were comorbid for an emotional disorder, kappa 5 .34, po.001. A 2 2 ANOVA tested for the effects of diagnosis with DBD and the child’s sex on children’s general prosocial tendencies. Children with DBD were significantly less prosocial than other children, M 5 – 0.66 (SD 5 1.17) versus M 5 0.14 (SD 5 0.88), F(1, 114) 5 10.75, po.001. There was no effect of the child’s sex and no interaction between sex and diagnosis. Worries about family members. Extreme anxiety about others, as measured by self-reported worries about harm that might befall attachment figures, was shown by 14 children in the sample (10.9%): 7 boys (11.7%) and 7 girls (10.3%). Links between extreme worries about family members and more general prosocial tendencies, as measured by the prosocial factor score, were examined (Table 3). Children who worried about the well-being of family members were significantly more prosocial than other children, t(119) 5 – 2.34, po.02. The children who worried about family members had significantly fewer externalizing problems than other children, t(20) 5 2.30, po.03, (degree of freedom is adjusted because equality of variance was not assumed), but experienced a greater number of internalizing problems, t(116) 5 – 3.74, po.001. Their problems were severe. Most of the children who worried about family members (69%) met DSM – IV criteria for an emotional disorder, as opposed to only 10% of other children, w(1) 5 29.64, po.001, odds ratio 5 20.04 (confidence interval 5 5.29 – 75.98). (The symptom of worrying about family members was not by itself sufficient to diagnose separation anxiety disorder.) This association was significant for both sexes, with 67% of boys and 71% of girls who worried about family members meeting criteria for an emotional disorder, w(1) 5 12.75, po.001 for boys and w(1) 5 16.91, po.001 for girls. Maternal Depression and Children’s Prosocial Behavior Are the associations between children’s prosocial behavior and their own psychological problems mirrored by links between children’s prosocial behavior and their mothers’ own problems? Cooperativeness at age 4. There was no association between maternal depression and cooperation at age 4. Fifty-seven women (51.8% of those with complete data) met criteria for depression between the child’s birth and fourth birthday, as measured by the CIS at 3 and 12 months, or by the SADS – L, using RDC criteria to diagnose depression between 12 months and 4 years. A 2 2 multivariate analysis of variance (MANOVA) testing for the main effects of gender and the mother’s diagnosis on the two measures of cooperativeness showed that the children of depressed mothers were no more or less cooperative than other children. The two sexes did not differ, nor did the mother’s history of depression interact with the child’s sex to influence cooperation at age 4. 1322 Hay and Pawlby Table 3 Prosocial and Problem Factor Scores for Children Who Do and Do Not Express Clinically Significant Worries About Family Members Children with extreme worries Other children (N 5 14) (N 5 114) Dependent variable Prosocial composite Externalizing problems Internalizing problems M SD M SD M SD 0.56 0.79 0.36 0.66 0.83 1.03 0.05 0.94 0.04 1.03 0.10 0.95 Note. The values represent factor scores on each dependent variable for the two groups of children. po.05. po.001. Furthermore, the mother’s current mental state, as measured by the GAS rating, was not associated with the child’s cooperation with the mother at age 4, r(114) 5 .04, nor with the tester, r(116) 5 – .06. Children’s general prosocial tendencies at age 11. There was no effect of maternal depression on the prosocial factor score. Rather, as predicted, the direction of the relation between maternal depression and the children’s general prosocial tendencies at age 11 depended on the informant being questioned (Figure 1). By the time the child was 11 years old, 75 mothers in the sample (57.7%) had met criteria for depression on at least one occasion. A 2 2 3 repeatedmeasures MANOVA, with the mother’s caseness and the child’s sex as between-subjects factors and informant as a within-subjects factor, revealed a significant interaction between the mother’s caseness and the identity of the informant, multivariate F(2, 118) 5 3.11, po.05. Planned contrasts indicated a significant difference between mothers’ and children’s own ratings of prosocial behavior, F(1, 119) 5 6.08, po.02. Mothers with a history of depression saw their children as less prosocial, but the children of depressed mothers saw themselves as more prosocial than other children. There was no three-way interaction with the child’s sex. A similar pattern was found with respect to mothers’ current psychological functioning. Mothers who were functioning better rated their children as more prosocial, r(125) 5 .20, po.02; teachers also rated children of well-functioning mothers as more prosocial, r(126) 5 .20, po.02. However, children’s own assessments of their prosocial tendencies were unrelated to their mothers’ current psychological functioning, r(127) 5 .01. Figure 1. The three informants’ reports of prosocial behavior at age 11, as a function of the mother’s depression during the child’s lifetime. Worrying about family members. Children’s worries about family members were not significantly associated with the mother’s current mental state, nor with the mother’s caseness for depression. Extreme anxiety about family members was not shown by the 4 children whose mothers had attempted suicide in the last 7 years. Does Maternal Depression Moderate the Links Between Children’s Prosocial Behavior and Psychological Problems? We tested the possibility that children of depressed mothers might be especially likely to show a profile of behavior that includes both prosocial tendencies and problematic behavior. In other words, for the children of depressed women, prosocial behavior might be positively related to psychological problems. However, no evidence was found in support of this proposal. Prosocial tendencies and externalizing problems were negatively related, r 5 – .45, po.001 for the children of well mothers, and r 5 – .63, po.001 for the children of depressed mothers. Against expectations, a positive association between prosocial behavior and emotional problems was found for the children of mothers who had not been depressed, r 5.44, po.001. Subsequent analyses showed that this was especially true for the sons of the well mothers, r(24) 5 .59, po.002. Early Cooperation and Risk for Later Psychological Problems Finally, we tested for long-term relations between cooperation in early childhood and psychological problems in early adolescence. Children who were more cooperative with their mothers at age 4 had Prosocial Development and Psychological Problems fewer externalizing problems at age 11, r(108) 5 – 30, po.002. There was no association between cooperation at age 4 and internalizing problems at age 11. The tester’s rating of cooperativeness did not predict externalizing or internalizing problems. The relation between early cooperation and later externalizing problems was explored in more detail. Linear regression was used to evaluate the contribution of early cooperation to the prediction of later externalizing problems, controlling for the child’s sex, the mother’s history of depression, the interaction between those two variables, and the child’s early behavioral problems and current prosocial tendencies. The dependent variable for this analysis was the composite measure of externalizing problems at age 11. The child’s sex, along with the mother’s diagnosis of depression and the interaction between sex and diagnosis, centered with respect to the means of each variable, were entered on the first step. Both measures of early cooperation were entered on the second step, and the total CBCL score was entered on the third step (the high correlation between the externalizing and internalizing scales introduced collinearity problems if both were included in the model). Finally, as a measure of current prosocial behavior, the prosocial factor score was included at the final step. Results from the final model are presented in Table 4. Introduction of predictors at each step led to significant R2 change; thus, the inclusion of the measure of observed cooperation with the mother was a significant predictor of the child’s later externalizing problems, even when the child’s sex and the mother’s diagnosis had been taken into account, t 5 – 3.22, po.002, R2 change 5 .09, po.005. Furthermore, when the measure of early behavioral Table 4 The Prediction of the Child’s Externalizing Problems at Age 11 Predictor variable B Child’s sex Mother’s caseness Caseness Sex Cooperation with mother Cooperation with tester CBCL problems at 4 Prosocial score at 11 .24 .20 .14 .04 .02 .02 .47 (95% Confidence Interval) ( ( ( ( ( .56 .12 .75 .07 .10 (.00 ( .63 to to to to to to to .08) .52) .46) .01) .06) .04) .31) b .12 .10 .04 .19 .04 .19 .48 Note. The table summarizes the contribution of each predictor variable at the final step, N 5 104, R2 5 .49, adjusted R2 5 .44, standard error of estimate 5 0.75. B 5 unstandardized weight in regression analysis; CBCL 5 Child Behavior Checklist. po.05. po.01. po.001. 1323 problems and the age 11 composite measure of prosocial tendencies were incorporated in the regression model at the final step, the level of cooperation with the mother at age 4 still remained a significant predictor of externalizing problems at age 11 (Table 4). In the final model, the child’s sex was no longer a significant predictor of externalizing problems at age 11. Rather, externalizing problems were predicted by the level of cooperation with the mother at age 4, the mother’s rating of the child’s problems at age 4, and the child’s current prosocial behavior. An analogous linear regression analysis revealed that internalizing problems at age 11 were not significantly influenced by the predictor variables. The only significant univariate predictor was the mother’s caseness for depression, t 5 2.25, po.03, which was no longer significant when the child’s CBCL problems score at age 4 was included in the model. Thus, early cooperation predicted externalizing but not internalizing problems at age 11. Discussion The preceding longitudinal analyses clearly demonstrate that prosocial children show low rates of externalizing problems. This association began to emerge in early childhood and was clearly observed in early adolescence, across instruments and informants. In this sample, early cooperation was a protective factor against later disruptive behavior, and its unique effects were not mediated by continuities in either disruptive or prosocial behavior over time. Active cooperation in the preschool years reflects emotionally regulated, socially competent engagement with the social world and may set the child on a course of successful interactions that promote general psychological adjustment. These findings add to the growing body of information about longterm continuities in prosocial behavior over the childhood and adolescent years, which have focused on helpfulness (Côté et al., 2002) and sharing (Eisenberg et al., 1999). However, conclusions to be drawn are necessarily constrained by the fact that, in the present study, only two limited measures of one form of prosocial behavior were taken at the age 4 assessment. It is not clear whether cooperative behavior with siblings or peers, as opposed to adults, would have similar predictive power, nor whether a similarly long-term protective function could be discerned for other forms of prosocial behavior. These data suggest, however, that longitudinal studies of prosocial development might 1324 Hay and Pawlby profit from a focus on cooperation as well as other, more extensively studied forms of prosocial behavior. Although prosocial children were not very disruptive, it was not the case that prosocial behavior was invariably a marker of psychological adjustment. Some prosocial children were well adjusted and others had emotional problems. Early cooperativeness did not protect the children from developing emotional problems in early adolescence. It is important to note that prosocial boysFparticularly those who were not exposed to maternal depressionFmay be at special risk for emotional problems. Longitudinal analyses of a large sample of children in Québec showed that only a minority of boys showed prosocial behavior at consistently high rates across childhood (Côté et al., 2002). To the extent that prosocial boys’ behavior runs counter to gender stereotypes and actual peer group norms, they may experience peer rejection. Alternatively, boys with emotional problems may be more likely than other children to use prosocial strategies to gain peer acceptance. In future work it will be important to study gender differences not just in the overall level of prosocial behavior but in their relation to other traits and problems. This study demonstrated that children who reported being extremely anxious about loved ones often manifested serious emotional disorder but also were more likely to show prosocial behavior than other children. The worries expressed by these children were very serious, indeed. Qualitative analysis of these children’s comments during the interview indicated that they were worried about their family members being hit, mugged, raped, or killed. The children’s reports also revealed aspects of self-sacrifice, with the children interrupting their own sleep or giving up pleasurable activities to check on the well-being of their family members. For example, one child expressed concerns that his mother ‘‘could slip on the kitchen floor and be unconscious and nobody would know.’’ He commented that ‘‘I try to get home as soon as I can,’’ even to the extent of not playing soccer with his friends. These analyses have identified an important subgroup of emotionally troubled boys and girls in this community sample who were significantly more prosocial and less disruptive than average. This study provided mixed evidence regarding a link between maternal depression and children’s prosocial development. The direction of the relationship depended on the period of development being examined, the nature of the prosocial measure, and the informant being questioned. In early childhood, no significant links between maternal mental health and children’s cooperation could be discerned. This stands in contrast to the findings of a major community study of British 4-year-olds, where maternal depression was negatively associated with mothers’ ratings of children’s prosocial behavior (Dunn et al., 1998), but in that study both measures were based on maternal questionnaires. The finding also stands in contrast with suggestions in other studies that there might sometimes be a positive association between maternal depression and young children’s responses to distress (e.g., T. Dix, June 28, 2002, personal communi Radke-Yarrow et al., 1993). Finally, in view of the possibility that the children of depressed mothers might develop excessive forms of prosocial behavior, it is important to note that the children of depressed mothers were not more likely than other children to express clinically significant worries about family members. It proved important to canvass the opinions of the children themselves as well as the opinions of their mothers and teachers. In early adolescence, the adult informants reported that the children of depressed mothers were less prosocial than other children. In contrast, the children of depressed mothers saw themselves as more prosocial than other children. This is similar to the finding that maltreated children see themselves as prosocial agents in response to other people’s distress, even though their observed behaviors are not particularly prosocial (Macfie et al., 1999). Mothers and, especially, teachers no doubt compare children’s prosocial tendencies against their own expectations and social norms. A long history of interaction with a depressed parent (and the related family upheaval that often entails) may indeed promote disruptive behavior and reduce prosocial tendencies, perhaps especially in response to the challenges of the classroom. Yet, children who grow up with depressed parents may also be called on to assist and comfort their parents and siblings in many ways. They may see themselves quite rightly as helpful, sympathetic people. It is tempting to see the children’s reports as less reliable than those of adults, but the degree of consistency across informants argues against this view. Rather, it seems that children’s reports of prosocial behavior are drawing on different sources of evidence than those used by the adult raters. Different informants use different implicit definitions of prosocial behavior (Warden et al., 1996). Children’s perceptions of themselves as prosocial are important in their own right, and the self-perceptions of children who have experienced family adversity Prosocial Development and Psychological Problems are of particular interest. They may lead to distorted working models of one’s responsibility for the care of others (Macfie et al., 1999), but positive selfperceptions might also provide a source of resilience in the face of difficult family circumstances. In future work, it will be important to examine the effects of maternal health problems using a broader array of measures of prosocial behavior, including direct observation, experimental tasks, and peer nominations. Although standardized measures of prosocial tendencies, such as the SDQ prosocial scale, show good levels of reliability (R. Goodman, 1994; Ladd & Profilet, 1996; Tremblay et al., 1992), it is clear that different measures are differentially sensitive to particular causal influences. In particular, factors that influence self-reports differ from those that influence more objective measures (e.g., Eisenberg & Lennon, 1983). Situational reactions, especially as assessed by psychophysiological measures, do not always correlate with dispositional prosocial behavior (Holmgren, Eisenberg, & Fabes, 1998). A broad approach to the assessment of prosocial behavior in childhood and adolescence is clearly needed. In summary, our prospective longitudinal study of an urban British sample demonstrated complex links between prosocial tendencies and psychological problems as children moved from childhood to adolescence. Low rates of prosocial behavior were characteristic of children with DBDs, but higher than average rates of prosocial behavior, plus extreme levels of concern for family members, were shown by a subgroup of children with severe emotional problems. Some troubled children are prosocial, and prosocial children, though unlikely to be disruptive, are not universally free of mental health problems. References Achenbach, T. M. (1988). Child Behavior Checklist for ages 4 – 16. Burlington: University of Vermont. American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.), Washington, DC: Author. American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.), Washington, DC: Author. Angold, A., Prendergast, M., Cox, A., Harrington, R., Simonoff, E., & Rutter, M. (1995). The Child and Adolescent Psychiatric Assessment (CAPA). Psychological Medicine, 25, 739 – 753. Dunn, J., Deater-Deckard, K., Pickering, K., O’Connor, T. G., Golding, J., & the ALSPAC Study Team. (1998). Children’s adjustment and prosocial behaviour in step-, 1325 single-parent and non-stepfamily settings: Findings from a community sample. Journal of Child Psychology and Psychiatry, 38, 965 – 980. Brownell, C. A., & Corriger, M. S. (1990). Changes in cooperation and self-other differentiation during the second year. Child Development, 6, 1164 – 1174. Buhrmester, D., Whalen, C., Henker, B., MacDonald, V., & Hinshaw, S. P. (1992). Prosocial behavior in hyperactive boys: Effects of stimulant medication and comparison with normal boys. Journal of Abnormal Child Psychology, 20, 103 – 121. Carlo, G., Koller, S. R., Eisenberg, N., DaSilva, M. S., & Frolich, C. B. (1996). A cross-national study on the relations among prosocial moral reasoning, gender role orientations, and prosocial behaviors. Developmental Psychology, 32, 231 – 240. Chen, X., Li, D., Li, Z-Y, & Liu, M. (2000). Sociable and prosocial dimensions of social competence in Chinese children: Common and unique contributions to social, academic, and psychological adjustment. Developmental Psychology, 36, 302 – 314. Chen, X., & Rubin, K. H. (1994). Family conditions, parental acceptance, and social competence and aggression in Chinese children. Social Development, 3, 269 – 290. Côté, S., Tremblay, R. E., Nagin, D., Zoccolillo, M., & Vitaro, F. (2002). The development of impulsivity, fearfulness, and helpfulness during childhood: Patterns of consistency and change in the trajectories of boys and girls. Journal of Child Psychology and Psychiatry, 43, 609 – 618. Cummings, E. M., & Smith, D. (1994). The impact of anger between adults on siblings’ emotions and social behavior. Journal of Child Psychology and Psychiatry, 34, 1425 – 1433. Dekovic, M., & Janssens, J. M. (1992). Parents’ childrearing style and child’s sociometric status. Developmental Psychology, 28, 925 – 932. Del’Homme, M. A., Sinclair, E., & Kasari, C. (1994). Preschool children with behavioral problems: Observation in instructional and free play contexts. Behavioral Disorders, 19, 221 – 232. Deutsch, M. (1949). A theory of cooperation and competition. Human Relations, 21, 129 – 152. Eisenberg, N., Fabes, R. A., Carlo, G., Troyer, D., Speer, A. L., Karbon., M., et al. (1992). The relations of maternal practices and characteristics to children’s vicarious emotional responsiveness. Child Development, 63, 583 – 602. Eisenberg, N., Fabes, R. A., Karbon, M., Murphy, B. C., Wosinski, M., Polazzi, L., et al. (1996). The relations of children’s dispositional prosocial behavior to emotionality, regulation, and social functioning. Child Development, 67, 974 – 992. Eisenberg, N., Fabes, R. A., Murphy, B., Maszk, P., Smith, M., & Karbon, M. (1995). The role of emotionality and regulation in children’s social functioning: A longitudinal study. Child Development, 66, 1360 – 1384. 1326 Hay and Pawlby Eisenberg, N., Guthrie, I. K., Murphy, B., Shepard, S., Cumberland, A., & Carlo, G. (1999). Consistency and development of prosocial dispositions: A longitudinal study. Child Development, 70, 1360 – 1372. Eisenberg, N., & Lennon, R. (1983). Gender differences in empathy and related capacities. Psychological Bulletin, 94, 100 – 131. Endicott, J., Spitzer, R. L., Fleiss, J. L., & Cohen, J. (1976). The Global Assessment Scale. A procedure for measuring overall severity of psychiatric disorders. Archives of General Psychiatry, 33, 766 – 771. Fabes, R. A., Eisenberg, N., Karbon, M., Troyer, D., & Switzer, G. (1994). The relations of children’s emotional regulation to their vicarious emotional responses and comforting behaviors. Child Development, 65, 1678 – 1693. Goldberg, D., Cooper, B., Eastwood, M. T., Kedward, H. B., & Shepherd, M. (1970). A standardised psychiatric interview for use in community surveys. British Journal of Preventive Social Medicine, 24, 18 – 23. Goldthorpe, J. H., & Hope, K. (1974). The social grading of occupations. Oxford, England: Oxford University Press. Goodman, R. (1994). A modified version of the Rutter Parent Questionnaire. Including extra items on children’s strengths: A research note. Journal of Child Psychology and Psychiatry, 35, 1483 – 1494. Goodman, R. (1999). The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. Journal of Child Psychology and Psychiatry, 40, 791 – 799. Goodman, R., Meltzer, H., & Bailey, V. (1998). The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. European Child and Adolescent Psychiatry, 7, 125 – 130. Goodman, S. H., & Gotlib, I. H. (1999). Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review, 106, 458 – 490. Haemaelaeinen, M., & Pulkinnen, L. (1996). Problem behavior as a precursor of male criminality. Development and Psychopathology, 8, 443 – 455. Hart, C. H., DeWolf, M., & Burts, D. C. (1992). Linkages among preschoolers’ playground behavior, outcome expectations, and parental disciplinary strategies. Early Education and Development, 3, 265 – 283. Hastings, P. D., Zahn-Waxler, C., Robinson, J., Usher, B., & Bridges, D. (2000). The development of concern for others in children with behavioral problems. Developmental Psychology, 36, 531 – 546. Hay, D. F. (1979). Cooperative interactions and sharing between very young children and their parents. Developmental Psychology, 15, 647 – 655. Helgeson, V. S., & Fritz, H. L. (1998). A theory of unmitigated communion. Personality and Social Psychology Review, 2, 173 – 183. Holmgren, R.A, Eisenberg, N., & Fabes, R. A. (1998). The relations of children’s situational empathy-related emotion to dispositional prosocial behaviour. International Journal of Behavioural Development, 22, 169 – 193. Hughes, C., White, A., Sharpen, J., & Dunn, J. (2000). Antisocial, angry, and unsympathetic: ‘‘Hard-to-manage’’ preschoolers’ peer problems and possible cognitive influences. Journal of Child Psychology and Psychiatry, 41, 169 – 179. Kier, C., & Lewis, C. (1998). Preschool sibling interaction in separated and married families: Are same-sex pairs or older sisters more sociable? Journal of Child Psychology and Psychiatry, 39, 191 – 201. Klimes-Dougan, B., & Bolger, A. K. (1998). Coping with maternal depressed affect and depression: Adolescent children of depressed and well mothers. Journal of Youth and Adolescence, 27, 1 – 15. Kochanska, G., Aksan, N., & Koenig, A. L. (1995). A longitudinal study of the roots of preschoolers’ conscience: Committed compliance and emerging internalization. Child Development, 66, 1752 – 1769. Ladd, G. W., & Hart, C. (1992). Creating informal play opportunities: Are parents’ and preschoolers’ initiations related to children’s competence with peers? Developmental Psychology, 28, 1179 – 1187. Ladd, G., & Profilet, S. M. (1996). The Child Behavior Scale: A teacher-report measure of young children’s aggressive, withdrawn, and prosocial behaviors. Developmental Psychology, 32, 1008 – 1024. LaFreniere, P. J., Provost, M. A., & Dubeau, D. (1992). From an insecure base: Parent-child relations and internalizing behaviour in the preschool. Early Development and Parenting, 1, 137 – 148. Macfie, J., Toth, S. L., Rogosch, F. A., Robinson, J., Emde, R. N., & Cicchetti, D. (1999). Effect of maltreatment on preschoolers’ narrative representations of responses to relieve distress and of role reversal. Developmental Psychology, 35, 460 – 465. Macksoud, M. S., & Aber, J. L. (1996). The war experiences and psychosocial development of children in Lebanon. Child Development, 67, 70 – 88. McCarthy, D. (1972). Manual for the McCarthy scales of children’s abilities. New York: Psychological Corporation. Miller, P. A., Eisenberg, N., Fabes, R. A., & Shell, R. (1996). Relations of moral reasoning and vicarious emotion to young children’s prosocial behavior toward peers and adults. Developmental Psychology, 32, 210 – 219. Moffitt, T. E., & Caspi, A. (2001). Childhood predictors differentiate life-course persistent and adolescent-limited antisocial pathways among males and females. Development and Psychopathology, 13, 355 – 375. Murphy, L. (1937). Social behavior and child personality. New York: Columbia University Press. Office for National Statistics. (2000). Social trends pocketbook. Wales: Her Majesty’s Stationers Office. Office for National Statistics. (2003). From http:// www.statistics.gov.uk. Raboteg-Saric, Z., Zuzul, M., & Kerestes, G. (1994). War and children’s aggressive and prosocial behaviour. European Journal of Personality, 8, 201 – 212. Radke-Yarrow, M., & Zahn-Waxler, C. (1986). The role of familial factors in the development of prosocial Prosocial Development and Psychological Problems behavior: Research findings and questions. In D. Olweus, J. Block, & M. Radke-Yarrow (Eds.), Development of antisocial and prosocial behavior: Research, theories, and issues (pp. 207 – 233). New York: Academic Press. Radke-Yarrow, M., Zahn-Waxler, C., Richardson, D. T., Susman, E., & Martinez, P. (1993). Caring behavior in children of clinically depressed and well mothers. Child Development, 65, 1405 – 1414. Rheingold, H. L., Cook, K., & Kolowitz, V. (1987). Commands activate the behavior and pleasure of two-year-old children. Developmental Psychology, 23, 146 – 151. Rice, R., Harold, G., & Thapar, A. (2002). The genetic aetiology of childhood depression: A review. Journal of Child Psychology and Psychiatry, 43, 65 – 79. Rose-Krasnor, L., Rubin, K. H., Booth, C. L., & Coplan, R. (1996). The relation of maternal directiveness and child attachment security to social competence in preschoolers. International Journal of Behavioral Development, 19, 309 – 325. Rothbart, M. K., Ahadi, S. A., & Hershey, K. L. (1994). Temperament and social behavior in childhood. MerrillPalmer Quarterly, 40, 21 – 39. Sharp, D. (1993). Childbirth-related emotional disorders in primary care: A longitudinal prospective study. Unpublished doctoral dissertation, University of London. Sharp, D., Hay, D. F., Pawlby, S., Schmücker, G., Allen, H., & Kumar, R. (1995). The impact of postnatal depression on boys’ intellectual development. Journal of Child Psychology and Psychiatry, 36, 1315 – 1336. Spitzer, R. L., Endicott, J., & Robbins, E. (1978). The Schedule for Affective Disorders and Schizophrenia – Lifetime version (SADS – L) (3rd ed.), New York: Biometric Research. Staub, E. (1978). Positive social behavior and morality: Social and personal influences. New York: Academic Press. Stevenson-Hinde, J., & Shouldice, A. (1995). Maternal interactions and self-reports related to attachment classification at 4.5 years. Child Development, 66, 583 – 596. Tremblay, R. E., Vitaro, F., Gagnon, C., Piché, C., & Royer, N. (1992). A prosocial scale for the Preschool Behaviour Questionnaire: Concurrent and predictive correlates. 1327 International Journal of Behavioural Development, 15, 227 – 245. Vinnick, L. A., & Erickson, M. T. (1992). Relationships among accumulated lifetime life events, prosocial skills, and behavior problems in elementary school children. Journal of Child and Family Studies, 1, 141 – 154. Warden, D., Christie, D., Kerr, C., & Low, J. (1996). Children’s prosocial and antisocial behaviour, as perceived by children, parents and teachers. Educational Psychology, 16, 365 – 378. Wentzel, K. R., & McNamara, C. C. (1999). Interpersonal relationships, emotional distress, and prosocial behavior in middle school. Journal of Early Adolescence, 19, 114 – 125. Wolke, D. (1990). Tester’s rating of child behavior: Scoring manual. Unpublished manuscript. Wolke, D., Skuse, D., & Mathison, B. (1990). Behavioural style in failure to thrive infants: A preliminary communication. Journal of Pediatric Psychology, 15, 237 – 253. World Health Organization. (1978). Mental disorders: Glossary and guide to their classification in accordance with the ninth revision of international classification of diseases. Geneva, Switzerland: Author. Zahn-Waxler, C., Cole, P., & Barrett, K. C. (1991). Guilt and empathy: Sex differences and implications for the development of depression. In K. Dodge & J. Garber (Eds.), Emotion regulation and dysregulation (pp. 243 – 272). Cambridge, England: Cambridge University Press. Zahn-Waxler, C., Cole, P. M., Richardson, D. T., Friedman, R. J., Michel, M. K., & Belouad, F. (1994). Social problemsolving in disruptive preschool children: Reactions to hypothetical situations of conflict and distress. MerrillPalmer Quarterly, 40, 98 – 119. Zahn-Waxler, C., Cole, P. M., Welsh, J. D., & Fox, N. A. (1995). Psychophysiological correlates of empathy and prosocial behaviors in preschool children with behavior problems. Development and Psychopathology, 7, 27 – 48. Zahn-Waxler, C., Cummings, E. M., McKnew, D., & RadkeYarrow, M. (1984). Altruism, aggression, and social interactions in young children with a manic-depressive parent. Child Development, 55, 112 – 122.











© Copyright 2025