
Course PDF - Dentalcare.com
Designing A Comprehensive Health History Mary Govoni, CDA, RDA, RDH, MBA; Wilhemina Leeuw, MS, CDA Continuing Education Units: 2 hours Online Course: www.dentalcare.com/en-US/dental-education/continuing-education/ce76/ce76.aspx Disclaimer: Participants must always be aware of the hazards of using limited knowledge in integrating new techniques or procedures into their practice. Only sound evidence-based dentistry should be used in patient therapy. Over the years, the practice of dentistry has evolved from one of a relatively narrow scope, defined by the boundaries of the oral cavity, to one of comprehensive proportions. We now know that a patient’s oral health can greatly affect their overall health status and vice versa. The information contained in this course should allow the dental professional to design a health history questionnaire or revise an existing questionnaire to be more comprehensive. This course also provides basic information for the professional to remember when interviewing patients and in minimizing the risks associated with treating patients, especially those with medical conditions; and assist in providing safe treatment to all patients in a dental practice. Conflicts of Interest Disclosure Statement • The authors report no conflicts of interest associated with this work. ADAA This course is part of the home-study library of the American Dental Assistants Association. To learn more about the ADAA and to receive a FREE e-membership visit: www.dentalassistant.org ADA CERP The Procter & Gamble Company is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at: http://www.ada.org/cerp 1 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Approved PACE Program Provider The Procter & Gamble Company is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and Membership Maintenance Credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 8/1/2013 to 7/31/2017. Provider ID# 211886 Overview Over the years, the practice of dentistry has evolved from one of a relatively narrow scope, defined by the boundaries of the oral cavity, to one of comprehensive proportions. We now know that a patient’s oral health can greatly affect their overall health status and vice versa. We also know that many medical conditions have oral manifestations that are often the first indicators of systemic disease. In addition, many existing medical conditions have effects on the success or failure of dental treatment. With these facts in mind, it is apparent that a patient’s health history is one of the most important documents in a dental practice. This document is utilized to assess a patient’s current status, evaluate past history and identify current conditions that may alter treatment plans or delay treatment. The health history also aids the dental team in identifying patients with infectious diseases, such as tuberculosis, that can pose serious hazards to the dental team and other patients in a dental practice. It is the legal responsibility of a dentist to obtain a health history from every patient that s/he treats, in order to make informed treatment decisions. Dental assistants are often assigned the task of obtaining this information from patients, are often the first member of the dental team to have contact with patients and many times assist patients in completing their health history forms. Therefore, it is vitally important for assistants to understand the many facets of a comprehensive health history. Learning Objectives Upon completion of this course, the dental professional should be able to: • Explain the importance of the health history and its relationship to patient treatment. • Describe ways in which the patient, dentist and physician can communicate and share important information that may affect treatment of the patient. • Apply legal requirements for obtaining consent for treatment. • Identify certain risk management issues, including record keeping and confidentiality, and compliance with the Health Insurance Portability and Accountability Act (HIPAA). • Describe techniques used for obtaining a health history. • Identify the components of a comprehensive health history, including personal information, medical/ dental past history, family history, current medical/dental status and medications. • List sources of information that may be used as references when reviewing a health history. • Explain which medical conditions may affect treatment planning. • Describe the changes that should be made in treating patients with certain medical conditions. • Summarize the most current guidelines for antibiotic prophylaxis for identifying patients at risk for bacterial endocarditis, and currently recommended medications/dosages. • Explain how the CDC Guidelines for Preventing the Transmission of Tuberculosis in Health Care Facilities will affect treatment of patients who have or are suspected of having infectious tuberculosis. • Discuss how the Americans with Disabilities Act affects the treatment of patients with HIV or AIDS. • Describe different methods for updating health history and the frequency at which it should be done. 2 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Course Contents bacterial/infective endocarditis – Sometimes referred to as subacute bacterial endocarditis (SBE), a microbial infection of the inner lining of the heart. •Glossary • Purpose of the Health History • Legal Requirements for Treatment • Techniques for Obtaining a Health History • Components of a Comprehensive Health History • Classification of Patient's Current Status • Medical Conditions that Affect Dental Treatment • Reference Guides • Updating the Health History •Summary • Appendix A • Appendix B • Appendix C • Course Test Preview • References • About the Authors cardiovascular disease – Collection of diseases that involve the heart and circulatory system. cerebrovascular accident (CVA) – Commonly referred to as a stroke; a disruption of blood flow in the brain or a hemorrhage in the brain. chemotherapeutic agents – Drugs or chemicals used to treat specific diseases, often cancers. chlorhexidine gluconate – Antimicrobial or antiseptic agent used in hand scrubs and mouth rinses. chronic obstructive pulmonary disease (COPD) – Term used to describe diseases of the small airways or bronchioles in the lungs, resulting in obstruction, narrowing or collapse. Glossary age of consent – In most states, 18 years of age, the age at which a person is considered an adult and can enter into contracts and agree to medical treatment. congenital heart defects – Anomalies that are present in the heart at birth, may involve heart valves, chambers or the walls of the heart (e.g., a hole in the heart). AIDS – Acquired immune deficiency syndrome; advanced stage of HIV. coronary artery disease (CAD) – Disease that disrupts the flow of blood in the vessels surrounding the heart, typically with a blockage of the artery. anaphylaxis – Acute, systemic allergic reaction that occurs when a sensitized person is again exposed to the sensitizing agent. dialysis – Treatment for patients with kidney failure, in which the blood is circulated through a machine that filters out the toxins normally removed by the kidney. angioedema – Manifestation of anaphylaxis, characterized by hive-like skin eruptions that are large and swollen both in the dermis or top layer of the skin and the subcutaneous structures. diastolic pressure – The bottom number of blood pressure ration (i.e., 120/80), which measures the pressure in the blood vessel during ventricular relaxation, when the heart is at rest. antibiotic prophylaxis – Regimen of antibiotics that is given prior to certain procedures including some dental procedures, to patients who are at risk for bacterial endocarditis. digital examination – Examination performed with the fingers, by feeling or palpating. atherosclerosis – Condition in which the walls of the artery become thickened, obstructed and/or lose their elasticity. disclaimer – On a patient’s health history means that the patient should sign a statement that he has completed the information to the best of his ability and will hold the dentist harmless if he (the patient) was not truthful and/or accurate on the questionnaire. bacteremia – Sometimes called septicemia, the invasion of the circulation (blood) by bacteria. 3 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 disclosure – With regard to dental treatment means that a dentist must inform patients of all aspects of treatment, benefits, risks and alternatives (as in informed consent). HIV – Human immunodeficiency virus; a retrovirus causing failure of the immune system. hyperglycemia – Increase in the concentration of sugar/glucose in the blood, a feature of diabetes. discrimination – Denying a person access to services based on race, color, sex, national origin, age, size or any other characteristic, including HIV/AIDS status. hypertension – Abnormal elevation of the systolic or diastolic arterial pressure. hypoglycemia – Very low concentration of sugar/ glucose in the blood, usually less than 40mg/100ml of blood; symptoms include nervousness, hunger, weakness, dizziness and fainting. emphysema – Destruction of the alveolar walls of the lungs, resulting from chronic irritation, such as cigarette smoking. epinephrine – Also known as adrenaline, a hormone secreted by the adrenal gland which causes vasodilation of the blood vessels of skeletal muscles, but also vasoconstriction of the arterioles of the skin and mucous membranes, relaxation of the bronchiolar smooth muscles and increased heart rate; used as a vasoconstrictor in local anesthetics to prolong their effect; used to treat allergic reaction to help in relaxing the bronchioles to allow the patient to continue breathing. idiopathic – No known cause. epistaxis – Bleeding from the nose. intravenous – Injecting medication directly into a vein, providing much faster action of the medication. informed consent – Written or implied acceptance of proposed treatment by a physician; includes informing patients about the treatment’s associated risks, alternative treatments and consequences of not having a specific treatment. intramuscular – Giving an injection into the skeletal muscle, (e.g., upper arm or buttock). hemorrhagic disorders – Diseases of the blood in which spontaneous or excessive bleeding occurs. latex/natural rubber latex (NRL) – Milky white fluid that is produced by some seed plants that is the basis for rubber, and is the major component of latex gloves. heart failure (HF) – Once more commonly known as “congestive heart failure;” HF is a cardio-vascular disease characterized by cardiac output that is insufficient to meet the body’s needs, even at rest. myocardial infarction (MI) – Necrosis or death of myocardial tissue, due to disruption of blood/ oxygen flow to the tissues of the heart. hepatitis – Inflammation of the liver; viral hepatitis comes in several forms (A, B, C, D, etc); healthcare workers are encouraged to be vaccinated against HBV. NIOSH N95 Mask – Sometimes referred to as a particulate respirator, a mask that is able to filter out very minute particles from the air; it is a special mask designed for use when working with patients with airborne infectious diseases, such as tuberculosis. HEPA mask – High efficiency particulate air; a mask able to filter out very minute particles from the air; it is a special mask designed for use when working with patients with airborne infectious diseases, such as tuberculosis. orthostatic hypotension – Aka: postural hypotension; a sudden drop in blood pressure caused by a change in body position; for instance, standing too quickly after laying prone for dental treatment. HIPAA – Health Insurance Portability and Accountability Act of 1996; a federal law that allows for greater access to health care insurance coverage and mandates that certain procedures be followed by health care providers to protect the privacy of patients’ health information. palpitation – Perception of the heart action by the patient, a heightened sense of awareness. 4 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Purpose of the Health History paralysis – Loss of movement and/or sensation due to injury or disruption of the central nervous system. The primary purpose of a patient’s health history is to attempt to find out as much about each patient as possible, so that the dental practice can treat the patient safely and knowledgeably. Members of the dental team need to know any and all information about a patient’s current health status, as well as any information about past medical and dental treatment; since all these factors will affect treatment and possibly predict a medical emergency. Protected Health Information (PHI) – Information about patient’s health that may not be released without the patient’s specific written consent for any use other than treatment, payment or operation of the dental practice. rheumatic heart disease – Results from rheumatic fever and causes rigidity or deformity of the heart valves. New patients must complete forms that inform the dental practice of their contact, billing, and personal information including dental and medical history information. In addition, returning patients should be asked to update this information at each visit. The registration and health history are legal documents, as part of the treatment record for each patient. These documents can be subpoenaed in court cases, such as a malpractice suit, or when disciplinary action is taken against a dental professional by a regulatory board. Because these documents can be used as legal evidence, they must be thorough, accurate, and legible. risk management – Procedures and protocols designed to prevent errors in the treatment of patients, including recordkeeping and documentation. seizure – A disorder of brain or cerebral function which causes altered consciousness, convulsions and/or loss of motor control. standard precautions – Protocol for infection control procedures for health care workers in which the health care workers must assume that every patient is a potential carrier of infectious disease and therefore must wear personal protective equipment and sterilize or disinfect items used in the treatment of that patient, regardless of his or her medical history. Under the Health Insurance Portability and Accountability Act of 1996 (HIPAA), these records are also considered protected health information (PHI) and dental practices must take federally mandated steps to protect the privacy of this information. The information may be used in conjunction with treatment of the patient, payment from insurance plans, and the general operation of the dental practice, such as administrative recordkeeping, which is defined by HIPAA as TPO, with a general consent from the patient. If the PHI is to be used for something other than TPO, such as a list of patients that is sold to a marketing company, a patient’s specific written consent must be given for the release of this information. systolic pressure – The top number of blood pressure ration (i.e., 120/80), which measures the pressure in the blood vessel at the point of ventricular contraction of the heart. TPO – Treatment, payment and operations – defined by HIPAA as an appropriate use of protected health information (PHI) with a general consent from a patient. urticaria – Hives, local wheals (round, raised areas) and redness of the skin, typically seen in an allergic reaction. An excellent resource for information regarding HIPAA and compliance requirement for dental practices is the ADA HIPAA Compliance Manual, available from the American Dental Association. The American Dental Assistants Association (ADAA) refers to HIPAA laws and compliance in many continuing education courses as it relates to the topic. These courses are available via the ADAA website at: http://www.dentalassistant. org/?page=CECatalog. vital signs – Results of checking blood pressure, body temperature, respirations, and pulse. xerostomia – Absence of or marked decrease in the production and flow of saliva, which may be the result of medication, stress or radiation therapy to the head and neck. 5 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Aside from the legal and recordkeeping aspects of the health history, this document serves as a bridge of communication between the patient’s medical health care provider and the dentist. When a patient completes a health history form, either as a new patient or returning patient, emphasis is placed on identifying any conditions that may affect that patient’s current dental health, overall health, and ability to receive dental care at the time. If the patient indicates certain medical problems, such as a heart condition, the dental team will ask more probing questions of the patient and the treating physician to assess the appropriateness of proceeding with treatment and to determine if any special precautions must be taken. explain to patients that taking certain medications will have effects on the oral cavity, such as decreased saliva or xerostomia (dry mouth.) When patients understand why the information is so important, they may be less resistant to disclosing it to the dental team. Legal Requirements for Treatment This information assists the dental team in preventing medical emergencies during treatment. In addition, undiagnosed conditions may be detected as a result of completing and reviewing the health history. For example, a patient who feels healthy may have high blood pressure and not be aware of it. Completing or updating a comprehensive health history on each patient, including checking vital signs, may identify patients who need medical intervention to treat their condition. Legal Consent When patients complete a new health history or update an existing history form, it is important to make certain that the patient is of legal age and competency to complete and sign the form. In most states, children under the age of 18 are considered minors. Minor patients, and patients who are mentally incompetent, must have a parent or legal guardian complete and sign their form on their behalf. Since minor patients are sometimes “'dropped off” at the dental office and the parent/ guardian does not stay for the appointment, the dental assistant or team member who schedules the appointment or greets the patient must emphasize to the parent/guardian that the health history form must be completed or updated before any treatment can begin. Because many patients do not realize that their oral health and general health are interrelated, emphasis is placed on compiling this information. A critical task for all dental professionals is to educate their patients on the importance of completing their health history form and providing the dental team with accurate and up-to-date information. This can be accomplished by explaining to patients about the oral manifestations of many diseases, such as diabetes or malnutrition. The dental professional should also Disclosure/Disclaimer At the end of the health history questionnaire the patient should be required to sign a statement that serves as a disclosure that the information is complete and accurate and also a disclaimer that the patient does not hold the dentist or other team members responsible for any errors or omission of information that the patient may have made in completing the form. A sample paper form is illustrated in Figure 1. Additionally, electronicallybased offices will have the patient complete the Figure 1. Health History Disclaimer. 6 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 computerized form that can be time and date stamped to meet this obligation. members who manage that information. First, all paper records must be completed in ink, to avoid the chance of erasure. A pen with permanent ink is preferred, since many ink pens have water soluble ink, which can wash off the record if liquid is spilled or sprayed on it. If a mistake is made on the form, have the patient cross out the incorrect information with a single line and initial it. The correct information can be entered just above or below where the incorrect information was written. Correction fluid or tape should never be used on any patient records. If information is transferred from a form completed by the patient to a computerized patient record, always retain the paper copy completed and signed by the patient or guardian. A better option for a computerized record is to scan and save the original form after each update. Informed Consent Before a dental professional performs any dental procedure on a patient, that patient must give their consent. Informed consent, as it is called, involves gaining the patient’s permission before treatment after all the facts, risks involved, and any alternatives to the proposed procedure have been explained. Informed consent also includes informing the patient of the risks of not having a procedure performed. For example, a patient who refuses a periodontist referral for treatment of their periodontal disease must be informed of the risk of losing their teeth due to disease progression. In many cases, informed consent is implied. In other words, the fact that a patient makes an appointment and allows a dentist, assistant, or hygienist to treat him/her, implies that they gave consent for treatment. Attorneys and risk management specialists, however, recommend that informed consent be in written form (Figure 2). This consent form can be attached to or incorporated into the health history form. Many times, dental specialists utilize customized consent forms that detail the possible risks of the specific procedures that they perform. The only instance where a patient or guardian is not legally required to give informed consent, is when the patient is unconscious and in need of emergency treatment. For example, if a patient is having an allergic reaction to latex, you do not need to have them sign a consent form to administer epinephrine to help save him/her from anaphylaxis and possible death. Some dental practices prefer to send out health history and patient information forms to new patients prior to their appointments, to save time on the day of the appointment. This is an excellent means of managing the appointment time, except if the patients lose or forget to bring the forms with them to their appointment. The form can be made available via the office website or the office can e-mail the form directly to the patient’s e-mail address. For those patients with no access to internet technology, sending a stamped, self-addressed envelope along with the forms and asking the patient to mail them back to the office could alleviate that problem, provided there is enough time for the forms to reach the patient and be returned to the office prior to the patient’s appointment. It is common for new patients to be scheduled for preventive or cleaning appointments at their first visit to a dental practice. If new patients are scheduled for treatment appointments at their Risk Management Because a health history is a legal document, certain criteria must be met by the dental team Figure 2. Consent Form. 7 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 first visit, the business assistant or scheduling coordinator must ask some preliminary health history questions prior to receiving the form completed by the patient. In particular, the practice needs to know whether or not that patient needs antibiotic prophylaxis. The current guidelines from the American Heart Association for prevention of infective (bacterial) endocarditis should be followed. (Appendix A) It is common practice for a patient to carry information about their condition on a wallet card provided to them from their cardiologist. The office should scan a copy of this for the patient record. (Appendix B) public health department; or reporting abuse/ neglect to authorities, as dental professionals are considered mandated reporters. Patients can be reluctant to disclose information about themselves, out of fear of their confidentiality being violated. These patients require the sincere reassurances of all members of the dental team that their privacy will not be invaded and information about them will not be disclosed inappropriately. Title II of HIPAA sets forth specific requirements for protecting the privacy of the patient’s information disclosed on the health history. A dental practice that is a covered entity must have a written privacy policy, which must be given to patients, and explains that the dental practice will not disclose the PHI for any uses other that TPO without the patient’s written consent. Confidentiality and Privacy Doctor-patient privilege requires a dentist to hold in strictest confidence any information disclosed by a patient for purposes of treatment. Therefore, all information contained in the patient’s record, including the health history, is confidential information to be used only in relationship to the patient’s treatment. Patient records must be stored in a secure area that is accessible only to members of the dental team. No information about the patient’s medical or dental conditions should be indicated on the outside of the patient’s record (file folder). Although it is a common practice to indicate allergies or the need for antibiotic prophylaxis on a patient’s file folder, this practice is a violation of patient confidentiality. To alert staff members of certain medical conditions, a “medic alert” sticker could be prominently placed on an inside page of the record or a “flag” placed in a computerized record. But, again, nothing specific, such as “allergic to penicillin” should be indicated on the outside of the folder. This is especially important with regard to transmissible diseases due to the high degree of sensitivity of the information. Legal Ownership of Patient Records A patient’s records, including the health history and radiographic images, are the legal property of the treating dental office. Many patients, however, believe that the records belong to them. Most state statutes in the U.S. stipulate the patient’s right to review and to photocopy their records upon request. Patients also have the right to request that copies of their records (including radiographic images) be sent to a new dentist or to a specialist for treatment or a second opinion. The state attorney general’s office in each state should be contacted to become familiar with that state’s laws concerning access to medical records. Original copies of patient records, especially health histories and radiographic images should not leave the dental practice. If radiographic images are required for submission of insurance claims, make copies using duplicating film, or use double-film packets when exposing images on patients. In some cases, digital images may be submitted. If a dental practice is contacted by another health care provider for information related to confidential patient information, it is best to have that request confirmed in writing and have the patient sign a “release of information” statement, authorizing the dentist to disclose the information. The exceptions to the doctor-patient privilege law are cases in which the public welfare is in jeopardy. Such cases would include reporting an infectious disease (i.e., tuberculosis) to the Under HIPAA, patients have additional rights to review their records and request corrections or clarifications of the information in those records. Again, additional information regarding HIPAA requirements may be obtained from the ADA HIPAA Compliance Manual. 8 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Techniques for Obtaining a Health History Oral Interview Once the health history form is completed, it should be reviewed orally with the patient by the dental professional to clarify the information and verify its accuracy. Several very important questions should always be asked of patients, who may not remember or not consider the information important enough to list on their health history form: 1. What medications/drugs are you currently taking? (Both prescription and over-the-counter, as well as recreational drugs and nutritional supplements) 2. Have you been hospitalized for any reason within the last 6 months? 3. Are you currently under a physician’s care? If yes, then for what reason? Written Questionnaire Since the health history is a legal document, it is important that it be complete, legible, and in ink. This will ensure for clear reading of the information. It is preferable to print these instructions at the top of the health history form, saving time in writing or verbally stating these instructions each time a form is to be completed. When designing or updating a questionnaire, it is advisable to use at least a 12 point type font, which is easier for most patients to read. Selecting a serif font, such as Times New Roman or Arial, will also make the information easier to read. Some dental practices attempt to keep the health history on one side of one 8 ½" X 11" sheet of paper, by using a small font and eliminating some important information. It is advisable to be as comprehensive as possible, using as many pages as necessary. If patients hesitate, because of the length of the form, the dental team member should explain the importance of the information and inform the patients of the need to have a complete picture or summary of their health status. Offering to help patients record the information sometimes alleviates their reluctance. If the office is computerized and the patient can be questioned in a private consultation or treatment area, information about the health history can be asked and entered directly into the computer database. It is important to obtain a hard copy or electronic signature after completion. This information should be highlighted on the health history form for possible consultation with a physician prior to the patient receiving any dental treatment. The section on “Classification of Patient’s Current Status” gives specific information about conditions for which a physician should be consulted prior to treatment. Keep in mind, however, that some patients may not disclose all the necessary information on their health history form. Some information is very sensitive, for example, disclosing one’s HIV+ status or current treatment for a sexually transmitted disease (STD), like syphilis or gonorrhea. Therefore, some patients may not want a dentist to know this information, for fear of this information being disclosed to persons outside of the dental practice. For this reason, a health history cannot be relied on as an indicator of the level of precautions that should be taken for infection control procedures. The theory of Standard Precautions states that all persons should be treated as if they are potentially infectious for bloodborne transmitted diseases, regardless of their medical history. If a new health history form is not sent to the patient ahead of time, the patient should be instructed to arrive approximately 10 minutes before their appointment time in order to complete the necessary forms. For patients not fluent in English, it is important to make certain that someone is available to translate for the patient. This could be a family member or friend of the patient, or a dental team member who may be fluent in the patient’s native language. If the patient is unable to read or write, a dental team member or family member should be available to complete the written questionnaire for the patient. Visual Assessment In addition to verbally reviewing the patient’s written information, dental team members should also be performing a visual assessment of each patient. Questions to be answered include: • Does the patient appear healthy? • Does the patient exhibit signs of exertion when walking from the reception room to an operatory? • Is the patient short of breath/breathing hard/ coughing excessively? 9 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 • Does the patient have any asymmetries of the head/neck or the rest of the body? • Can you see the patient’s fingernails and nail beds? Do they appear pink, or have a bluish tint? • Are the whites of the patient’s eyes yellow instead of white? • Does the patient have trouble hearing or speaking? • Does the patient have problems with manual dexterity? • Does the patient have trouble concentrating? should be checked and recorded on his/her health history form. Adult patients should be checked at each return visit. Many styles of blood pressure devices are available for purchase. Along with the traditional manual set up, the office can also purchase automatically-inflating arm and wrist BP units that provide a digital read out of the systolic/diastolic ratio and the pulse rate to make this task simple and fast for the dental team. Figure 3 illustrates the normal, pre-hypertensive, and hypertensive BP categories established by the American Heart Association. Be aware, however, that some older blood pressure cuffs contain natural rubber latex (NRL) which could cause a sensitivity reaction for latex allergic patients. NRL cuffs should be replaced with a newer, latex-free cuff that will not pose a risk of allergic reactions. As one might guess, all these physical signs have some relationship to systemic conditions, which can affect the patient’s ability to be treated safely. These conditions may also be related to the patient’s current oral health status. For example, a patient with limited manual dexterity will no doubt have trouble with brushing and flossing. Patients who become short of breath walking short distances may have some type of uncontrolled cardiovascular or lung disease, such as chronic obstructive pulmonary disease (COPD). Additionally, several thermometers are on the market for fast temperature readings. Digital types offer a fast reading and can be barriered with a small plastic sleeve. Tympanic (ear) types also have a thin plastic disposable barrier that still offers a one-touch, fast, and accurate reading. Always remember there are three components to obtaining a patient’s health history – written questionnaire; oral interview; visual assessment. Communication Skills Healthcare literacy has become an issue when obtaining record information. Quite often, a patient may not understand the medical or dental conditions you are speaking of and may need extra time and help to understand the concepts Recording Vital Signs Obtaining and recording the patient’s vital signs should always be a part of the patient appointment. As a rule, each new patient’s blood pressure, pulse, temperature, and respiration rate Figure 3. Blood Pressure Categories. This chart reflects blood pressure categories defined by the American Heart Association. 10 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Components of a Comprehensive Health History and terminology. Patients may not even be aware that their condition could be considered a disease that needs special consideration while receiving dental treatment. It is the dental team member’s responsibility to make sure that patients understand the treatment prescribed before obtaining consent for themselves or children. Personal Information There are two classifications of information contained on a health history: personal and medical information. The personal information includes the following: patient name, address, home and cell phone numbers, date of birth, current age, and gender. For adults, the personal information also includes place of employment, business address and phone number, spouse/ partner name, birth date, insurance information (carrier, group number, policy number), and the name of an emergency contact. For minors, the information should also include the name of the patient’s parent or legal guardian, billing and insurance information, and a telephone number at which they can be reached in an emergency. The name of the patient’s primary care physician should also be listed. In the case of patients with specific medical conditions, the name of the specialist(s) treating them should be listed. If applicable, the name of the patient’s previous dentist should be listed, in order for copies of the patient’s previous treatment records and/or radiographic images to be requested. Obtaining personal information from patients, especially for a health history, requires excellent communication skills. Patients should feel comfortable that the dental team member interviewing them is objective, non-judgmental, and sensitive to their needs. The dental team member should make eye contact with the patient when speaking and especially when asking questions of the patient. If patients disclose sensitive information, reassure the patient that this information will be held in the strictest confidence and utilized only in relationship to their dental treatment. When discussing any patient PHI, the dental team must be aware of the setting. PHI must never be discussed with the patient/guardian, among the dental team members, or with other entities within earshot of other any other people. Not only is this breaking the confidentiality of the patient, it is not reassuring to patients that the team protects their health information. Medical Information The medical information necessary on a health history form will be the lengthiest and most timeconsuming for the patient and dental team to complete. It should include the patient’s past history including, for example, whether they have had a previous heart attack; family history (does anyone in the family have cardiovascular disease?); and a list of all medications the patient is currently taking, including over-the-counter (OTC) medications, like antihistamines, antacids, or nutritional supplements. Recent surgeries and treatments such as chemotherapy or radiation should be noted as the patient may be immunocompromised and unable to receive treatment. The last component of the medical history is a review of all the body systems, to determine if there are any conditions that may affect, modify or delay treatment. Table 1 is an example of a review of the body systems. See Appendix C for an example of a Medical Questionnaire. It is important to obtain information on all medicines or drugs the patient may be taking at the time of the appointment. Patients must know that any drug, whether taken legally or illegally can affect the dental treatment and recovery times. Drug toxicity or overdose can occur if the patient is not truthful in disclosing all medications to the dental team. The dental team member must also be cognizant of their non-verbal communication with patients. Even though the dental team member may not verbally indicate a negative response at some information that is disclosed, it may be obvious, or misconstrued by the patient, in their facial expressions. It is imperative to remain professional, to become proficient at staying expressionless and non-judgmental in respect of the patients. These efforts can greatly enhance a patient’s willingness to disclose all information about his/her health status. 11 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Table 1. Review of the body systems. Table 2. Suggested questions to ask patients about their past dental history. Dental Information dentist was, this information may be verified by contacting that dentist. Past History The health history should also contain questions regarding the patient’s past dental experiences. Table 2 lists some suggested questions to ask patients about their past dental history. If the patient has indicated who his/her previous Chief Complaint In order to assess the patient’s understanding of his/her oral health, and also to determine the patient’s expectations, it is important to ask the patient what is his/her chief complaint. 12 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 In other words, why have they come to the dental office? It is significant to ask if they are experiencing pain, swelling, bleeding, sensitivity to hot, cold or sweets, or difficulty biting/chewing. Another central question to ask is if the patient is concerned with his/her appearance. If the patient is in pain, it is important for the dentist to diagnose the source of the pain and to attempt to resolve the problem, or the patient will feel that his/her needs are not being met and may not remain as a patient in the practice. identifying a patient’s health status is illustrated in Table 3. This classification system is based on the patient’s medical history, drug history (medications), physical and clinical examination (vital signs), emotional evaluation, medical consultation, and personal experiences. Patients in ASA Class I are healthy and can be treated without question. Patients in Class II and III have mild and moderate health issues. The dental team should consult with the patient’s physician prior to treating patients in ASA Class II depending on the medical condition. The treating physician(s) of Class III patients must be consulted in preparation of treatment. Nothing may need to be altered, but it is best to verify with the physician. Patients in ASA Class IV should not receive dental treatment until stabilized and away from life-threatening danger. Due to extreme health issues, dental offices will not be treating patients in Classes V or VI (see Figure 4). After thorough review of the health history, each patient should be assigned a classification that is recorded in the treatment record and revised as the patient’s status changes. All members of the dental team should be aware of this classification. Specific information about systemic diseases and conditions is listed in the following sections. Current Conditions Identification of the patient’s chief complaint, along with a clinical oral examination will identify the patient’s current conditions. The oral examination should consist of a visual and manual examination of the mouth, head and neck, a radiographic survey, and complete charting of teeth and supporting structures, including a periodontal charting. Current conditions should be recorded on the treatment record, as well as entering a summary description on the health history, including classification of existing restorations and teeth (e.g., rampant caries or marginal breakdown on existing restorations) and the periodontium (e.g., moderate gingival inflammation, bleeding on probing). It is always imperative to remember that HIPAA laws consider the above information to be protected health information (PHI). Medical Conditions that Affect Dental Treatment Medical Conditions that Affect Dental Treatment Once all the information has been obtained from the patient’s health history, both oral and written questionnaires, the dental team must evaluate Classification of Patient's Current Status A simple classification system created by the American Society of Anesthesiologists for Table 3. ASA Physical Status (PS) Classification System. 13 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Figure 4. Dental Treatment Protocols According to the ASA Classifications. the data and determine if any conditions exist that will affect, alter, or delay any necessary dental treatment. The ASA Classifications chart becomes a useful tool at this time. The following are conditions that will have some affect on dental treatment: regulated, 90-95% of cases; Gestational diabetes occurs during pregnancy and is reversed after delivery. If the patient indicates that they have diabetes, the type must be noted in the history. Patients with uncontrolled diabetes have low resistance to infection and are prone to periodontal disease. They have poor healing response, including excessive bleeding, and may experience hypoglycemia or hyperglycemia during dental treatment. Patients who are undiagnosed diabetics may report the following symptoms: excessive thirst and hunger, increased urination, and higher birth weights in babies. Need for Antibiotic Prophylaxis The current American Heart Association (AHA) guidelines are used to determine the need for and the protocol for antibiotic prophylaxis. The AHA, in conjunction with the American Medical Association and the American Dental Association, have consistently reviewed and revised the type of patients that need to be pre-medicated for dental treatment. Each office should consult with the patient’s physician if unsure of the patient’s status and recommended antibiotic prophylaxis prescriptions. When reviewing a health history, the following questions should be asked of diabetic patients: • Is your diabetes well controlled? • When is the last time your blood glucose was checked? • Are you currently taking oral anti-diabetic medications or insulin injections? • When was the last time you ate? • Did you take your medication on time today? Syncope Syncope, or fainting, is the most common emergency in the dental office. Patients should be asked if they have ever experienced a fainting episode in a dental office, or at any time in their life. It is most commonly associated with heavy coughing, orthostatic hypotension, and medication. Syncope can happen to any person at any age but are more common with pregnant and geriatric patients. It is advisable to keep sources of sugar on hand for hyper or hypoglycemic episodes. Glucose gel from a pharmacy, granulated sugar packets, honey packets, or tubes of cake icing can be easily stored and used in the case of an emergency. Diabetes There are three types of diabetes: Type I is considered insulin dependent, 5-10% of cases; Type II is when the body does not produce enough insulin and, therefore diet and medication may be When questioning diabetic patients before treatment and you find out they have not eaten or taken their insulin, their appointment should 14 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 be rescheduled. Make sure they understand the importance of these steps to maintain a normal blood sugar level during dental treatment. After approximately 8 hours of fasting, an average range is between 70 – 99 mg/dL. If they have eaten an average level should be less that 140 mg/dL. A strategy for making a dental appointment for a diabetic patient is to keep it short and in the early to mid-morning hours when sugar levels are more stable. several medications, particularly vasodilators like nitroglycerin; or beta-blockers, such as propanolol. The stress of a dental visit may cause an angina attack, therefore it is important to minimize patient stress, maximize patient comfort and make certain that the patient has his/her medications available, particularly nitroglycerin. In addition, it is recommended that local anesthetic without epinephrine or other vasoconstrictors be used for these patients, to avoid further constriction of the blood vessels. Patients with unstable or uncontrolled angina should wait for at least 30 days after their angina is stabilized to receive dental treatment. Cardiovascular Disease Patients who state that they have experienced chest pain, shortness of breath, pain that radiates down their neck or arm, have swollen ankles, and/or have high blood pressure are at risk for cardiovascular disease. They may or may not have been diagnosed by a physician. If this patient also indicates that they are a smoker and/or are overweight, the risk is increased. It is recommended that a medical consultation or evaluation be obtained for all patients who indicate some type of cardiovascular disease on their health histories. Additionally, medical consultations should also be obtained for patients who are reporting or exhibiting symptoms of cardiovascular disease, but have not had a definitive diagnosis. Preventing medical crises during dental treatment is the best method of protecting patients who are medically compromised. Myocardial Infarction (MI) is more commonly known as a heart attack. Patients who have experienced a recent myocardial infarction should not receive any dental treatment for a minimum of 6 months after the heart attack. Most fatalities from MI occur within 3-4 months after the attack. Stressful situations, like dental treatment can cause a rupture in the area of infarct, leading to further health problems and possible death. Hypertension is a common condition characterized by high blood pressure. Patients with uncontrolled hypertension are at risk for a stroke (also known as a cerebrovascular accident, or CVA), kidney failure, or heart attack. Since stress will increase blood pressure, dental treatment is contraindicated in patients with severe hypertension. Patients presenting with a systolic pressure between 120 to 139 should be advised to monitor their readings for improvement and see their physician for assessment. As a rule, patients with a systolic pressure greater than 160 and/ or a diastolic pressure greater than 95 should be referred for medical consultation and treatment and dental treatment should be delayed. Rheumatic Heart Disease is a result of rheumatic fever and can cause deformities in the heart valves. Some patients will report taking antibiotics on a regular basis, although this is not a required practice. If the patient reports a history of rheumatic fever, the dental practice must consult with the patient’s physician to determine the extent of the heart involvement. This assessment will determine the need for antibiotic prophylaxis. Congenital Heart Defects place the patient at high risk for bacterial endocarditis. Again, a statement from a physician is advisable to determine the type of defect and to verify the need for prophylactic antibiotics. It is relatively common for patients to have undiagnosed hypertension, making it very important for the dental team to monitor patients’ vital signs during their dental visits. A patient who reports having frequent dizziness, nosebleeds, or headaches may have high blood pressure and may be in need of medical intervention with antihypertensive drugs and/or diuretics. Coronary Artery Disease (CAD) results from atherosclerosis. Patients may report having been diagnosed with angina pectoris, or having chest pain after some type of physical activity or stress. These patients may be taking Heart Failure (HF) was more commonly known as “congestive heart failure” but the American 15 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Heart Association has recently renamed and shortened the title to characterize a broader spectrum of the disease. Depending on the type of HF, patients will typically have swollen ankles and shortness of breath, due to poor circulation and fluids backing up in the lungs. These patients may indicate that they must sleep upright or with several pillows. In these cases, placing them in a supine position for dental treatment may cause them acute distress. HF patients are usually taking one or more diuretic medications to remove fluid. Supplemental oxygen may be needed for these patients and use of nitrous oxide analgesia is contraindicated. Patients who are taking oral anticonvulsant medications, such as Dilantin®, Zarontin®, or Depacon®, may experience gingival hyperplasia. Emphasis must be placed on meticulous home care to prevent serious periodontal problems and the increased need for regular dental visits. Asthma Asthma is a chronic respiratory disorder that results in a narrowing of airways. An asthma attack can be triggered in several ways including environmental allergens, medications, or exercise. Patients with asthma may be prone to an attack or episode brought on by the stress of dental treatment, or exposure to an allergen like latex. The patient must always be instructed to bring his/ her medication/inhaler to each appointment. When the health history is reviewed at the beginning of treatment, the patient should be able to produce the medication or inhaler just in case it is needed. Kidney Disease Patients with kidney disease have impaired renal function, which results in accumulation of fluid and waste products normally excreted by the kidney. Renal problems often result from uncontrolled or undiagnosed diabetes. These patients may experience poor healing, incontinence, cystitis, and excessive bleeding. They may be receiving dialysis treatments or may have had/need a kidney transplant. In either case, the patients may be taking medications, such as anticoagulants or immunosuppressive drugs. Consult with the PDR regarding side effects of the medications and with the patient’s physician if there is a need to prescribe drugs for patients whose primary method of excretion or metabolism is the kidney. The impaired function of the kidney may cause toxic levels of the drug to accumulate in the patient’s tissues. Chronic Obstructive Pulmonary Disease (COPD) The two most common forms of COPD are emphysema and chronic bronchitis. Emphysema is the irreversible enlargement of the air sacs in the lungs making it hard to expel all oxygen during breathing. Chronic bronchitis is characterized as the irreversible condition of narrowed airways. Like patients with HF, those with either of these types of COPD may not be able to breathe easily in a supine position or after walking certain distances. Due to prolonged steroid use to treat their COPD, these patients may have candida infections (thrush) (see Figure 5). Seizure Disorder Seizure disorder is caused by an electrical disturbance in the brain. Any person can experience a seizure in a stressful situation and approximately half of all seizures are considered idiopathic. Epilepsy is a condition commonly associated with a syndrome of associated seizure types. Patients with COPD may need supplemental oxygen and often carry their own supply with When a known epileptic patient is scheduled for treatment, the dental team should determine if the patient has taken his/her anti-seizure medication. These patients should be scheduled for short appointments, when they are well rested. Patients often report an aura before experiencing a seizure. This aura can be a sound, feeling, or smell. Shining a bright light in the patient’s eyes should be avoided, since this has been known to trigger a seizure. Figure 5. Candida Infection. Courtesy of dentalcare.com 16 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 them. However, these patients should not be given high levels of oxygen, since this disease prevents them from metabolizing it. It is important that the COPD patient not receive nitrous oxide and oxygen therapy during dental treatment due to their impaired ability to exhale all gases. suspected of having an active, infectious TB case. If these patients can be referred for treatment in a facility that is specifically designed to treat TB patients (e.g., a hospital setting), it is acceptable for the dental practice to make this referral and not be liable for discriminatory practices. (http://www.cdc.gov/oralhealth/infectioncontrol/ guidelines/slides/101.htm) Infectious Diseases Hepatitis is characterized as an inflammation of the liver. It is a viral disease that appears in several forms. It is referred to as hepatitis A, B, C, D and E. A newer type of virus, non A-E, has been discovered, but not much is known about it at this time. Hepatitis B and C are transmitted through blood or other body fluids, while hepatitis A and E are usually transmitted indirectly through contaminated food and water. Hepatitis D is a piggyback virus that is linked to hepatitis B. Dental health care workers should be vaccinated against hepatitis B, to reduce their risk of infection when treating patients. The dental practice is required by law to pay for this vaccination. There is no vaccine for hepatitis C at this time. There is no way to visually identify every patient who has a potentially infectious disease. And because many patients are not aware if they have hepatitis, or are carriers, it is important to remember to practice standard precautions on every patient. In addition to asking patients on their health history if they have had TB, the patients should also be asked if they have experienced any of the following symptoms: night sweats, unexplained fever, weight loss, or a prolonged or bloody cough. If a patient has experienced any of these symptoms, refer them to a physician for evaluation before proceeding with anything but emergency palliative treatment. If emergency treatment must be performed on a patient suspected of having infectious TB, the following precautions should be taken: • Schedule the patient at the end of the day, as the last patient treated. • All team members present in the treatment room must wear a HEPA or NIOSH N 95 mask. • High volume evacuation and dental dam isolation must be used to reduce aerosols. HIV+ and AIDS is a viral infection that impairs a patient’s immune system, making the patient highly susceptible to other infectious diseases. It is transmitted through blood and other body fluids, which puts dental health care workers at some risk of infection from treating patients. Again, the practice of standard precautions must be followed, since many patients will not disclose their HIV+ status for fear of humiliation or rejection. Remember that information about a patient’s HIV+ status is highly sensitive and must be protected according to HIPAA. The dental team must take every precaution to protect the confidentiality of that patient’s health history. If a patient presents for treatment and reports a combination of fatigue, nausea, fever, dark urine and/or jaundice, they should be referred for medical treatment. When a patient reports a history of hepatitis, consult the PDR and their physician before drugs are prescribed to note if metabolized by the liver, since liver function may be impaired. Tuberculosis (TB) is a bacterial infection that occurs primarily in the lungs, but can occur in other organ systems in the body. It is spread through airborne particles, when an infectious patient coughs, sneezes, talks, or sings. TB is most easily spread in small confined spaces where infectious people share the same airspace with others. Because TB is highly infectious and its airborne transmission is difficult to control, the CDC has issued specific guidelines to help protect health care workers when treating patients. The Americans with Disabilities Act of 1990 protects people with HIV/AIDS infections and other diseases from discrimination in employment and delivery of all types of services, including health care. Although some dental health care workers are fearful of treating AIDS patients, it is illegal not to accept them into a dental practice or to refer them to another practice, unless the In the case of TB, these guidelines state that elective, (non-emergency) dental treatment should be postponed for patients who have or are 17 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 type of treatment is not performed in that practice. For example, if a general dental practice does not perform periodontal surgeries, it is legal to refer HIV+ or AIDS patients to a periodontist, since non-HIV or non-AIDS patients are referred as well. However, if only the HIV+ or AIDS patients are referred for periodontal surgery, this would be considered discriminatory. disease. A patient with one of these disorders will bruise very easily, may experience spontaneous, excessive bleeding, including unprovoked epistaxis (bleeding from the nose). Dental treatment, such as extractions, that may cause bleeding can be risky for these patients. Close monitoring by the physician is necessary. Treatment should be confined to specific areas (e.g., one tooth or quadrant at a time) and transfusion with clotting factors may be necessary prior to treatment. Aspirin must never be prescribed for pain control for these patients, since it is a natural blood thinner and increases bleeding. When treating patients with full blown AIDS, who are typically immunosuppressed, the dental team should take extra precautions to protect the patient from opportunistic infections. These may include wearing sterile surgical gloves rather than nonsterile exam gloves, having the patient use a pretreatment rinse of chlorhexidine gluconate or other mouthwash to prevent bacteremia, and using only sterile water for irrigation rather than from the air/ water syringe, which may contain some bacterial contamination. Allergies Allergies are specific body responses to foreign substances. An allergic reaction may be localized or limited to a skin rash or hives, or may be systemic and life-threatening, as in anaphylaxis. Many patients will indicate on their health history that they are allergic to environmental agents, such as pollen and dust. Many are also allergic to medications, such as codeine or penicillin. When prescribing medications, it is important to review the health history and orally question patients about known drug allergies. Blood Dyscrasias (Diseases) Anemia is a deficiency of red blood cells, caused by vitamin or iron deficiency or bone marrow problems. An anemic patient may have problems with slow wound healing and excessive bleeding. They may report feeling weak and fatigued, and may appear very pale. If a patient exhibits these symptoms a medical evaluation should be recommended. Latex allergies are becoming more common in dental and medical treatment. Repeated exposure to latex or natural rubber latex (NRL) during dental or medical treatment can cause a patient to become allergic. Again, the reaction may be localized, in which the patient’s lips become itchy or swollen from contact with latex gloves or dental dam material. Some patients, however, can experience a very serious anaphylactic reaction where their entire body responds when exposed to the allergen. The most serious symptom of anaphylaxis is swelling of the tongue, which closes off the patient’s airway. Without medical intervention, particularly without administration of epinephrine, patients can die from anaphylaxis. Leukemia is a type of blood cancer, where there is an overgrowth of white blood cells. These white blood cells may displace red blood cells, used to transport oxygen in the blood. These patients may exhibit oral signs, often before other symptoms of their disease. These signs typically include excessive gingival irritation in the absence of other causative agents, like heavy plaque or calculus. Patients with leukemia are very prone to infections, including periodontal infections. In addition, the chemotherapeutic agents used to treat the disease have many side effects, most notably xerostomia (dry mouth). Consult the treating physician before proceeding with treatment. Also consult the PDR for side effects from medications. A health history should ask questions about any allergies the patient may have, including latex, although some patients may not know that they are latex sensitive. Additional questions on the written questionnaire or oral interview may help to determine if this is the case. Patients noting spina bifida or urogenital anomalies are also Hemorrhagic disorders are ailments in which patients experience excessive bleeding, due to a deficiency of clotting factors in their blood. Common bleeding disorders are hemophilia A & B, factor II, V, VII, X, XII, and von Willebrand’s 18 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 associated with latex allergies. Patients should be asked if they have ever experienced stomach cramps, nausea or vomiting after eating bananas, kiwis, water chestnuts, or avocados. These foods contain chemicals similar to those in NRL. Also, ask patients if they have ever experienced any itching after handling balloons or after previous visits to the dentist or physician, where the health care providers wore latex gloves. problems and antihistamines use to treat allergies. Patients taking these medications must be advised about the adverse effects that dry mouth can have on their teeth and oral mucosa and be given tips to counteract these symptoms, especially if their oral hygiene is lacking. In addition, saliva replacements may need to be prescribed. Patients with systemic diseases, such as liver or kidney disease should not be prescribed medications that are metabolized by the liver or excreted by the kidneys. To safely treat latex allergic patients, all members of the dental team who come in direct contact with the patient must wear non-latex (vinyl or other synthetic material) gloves, and non-latex dental dam must be available when used. In addition, the dental team must check all products, such as prophylaxis cups, oxygen masks, and other items to determine whether those products contain latex. Latex-free substitutes are available for most products that currently contain latex, and many products are now labeled as “latex free.” Patients with latex sensitivity or allergy must be scheduled first in the morning before latex powders from other treatment areas are in the air. As latex is used, the powder/dust particles become airborne in the office from gloves being put on and taken off. Performing proper hand hygiene protocols is also important to remove residual latex powder. Epinephrine auto-injectors, or “epi-pens,” should be located in each treatment room, ready to administer immediately to a patient who begins to exhibit signs of an allergic reaction. Reference Guides Merck Manual The Merck Manual is a reference book that lists detailed data (signs and symptoms) of systemic diseases. It can assist the dental team members in understanding the process of a disease, precautions that should be taken and possible medications that the patient may be taking. The Merck Manual is also available online at http:// www.merckmanuals.com/professional/. Physicians’ Desk Reference The Physicians’ Desk Reference or PDR is a reference that gives information on prescription and some non-prescription drugs. The PDR can be used to identify side effects, precautions and drug interactions. It can also be utilized to identify medication by their size, shape and color; in cases where patients do not know the name of a prescription drug they are taking. The PDR is updated yearly and includes mid-year supplements for the newest prescription drugs. It is available in a hardbound book, on CD-ROM, via electronic tablet, or online at http://www.pdr.net/. Patient Medications can cause a reaction at any time. Some of the most important information gained from a health history is an accurate list of medications that a patient is currently taking, both prescription and over-thecounter. However, some patients may not know the names of the medications or not think that it is important to list certain ones. For some elderly patients, it may be advisable to ask the patient to bring all their meds with them, so that an accurate list may be documented. Consult the PDR to identify medications, side effects, precautions, and particularly drug interactions and contraindications. Release of Medical Information from Physician/ HIPAA Privacy Rules Due to the confidentiality of medical information and the physician-patient relationship, all requests for medical consultation information on patients should be made in writing, with the patient’s signature authorizing the release of the information. Figure 6 is a sample release form. In some cases, the release form may be sent to the physician with the patient or through the mail. In other cases, to save time, the form may be sent by fax and returned in this manner. This electronic transmission of protected health information is covered by HIPAA and the dental practice must have a signed consent form signed by the Most medications have some side effects, many of which appear in or affect the oral cavity. Xerostomia is a very common side effect of many prescription medications including those for heart 19 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Figure 6. Sample Release Form. Figure 7. Updating a Health History. patient for the transmission of this information, in addition to the release that must be signed for the physician to release the information to the dental practice. If worded so, the document can be signed one time and kept on file to cover both entities until the patient revokes the authorization. validate the updated information. The dental team member who updates the information should also initial the updates. A common method for facilitating this update is to create a section on the health history form with blank lines for initials and dates (Figure 7). Updating the Health History If it has been 2-3 years since a patient has been treated in the office, it is recommended that the patient complete a new health history form, since there may be many changes, not only to medical information, but to personal information as well. When the patient completes a new questionnaire, it should be attached to the old form. The outdated or “old” form should never be thrown away or destroyed. Each time a patient visits the dental office for treatment, the health history should be updated. If it has been a relatively short time since the patient was seen in the office (weeks or months) the health history can be updated verbally, by asking if there have been any changes and if the patient is taking any new or different medications. Once this information is obtained, the patient must initial and date the health history form, to 20 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Summary questionnaire or revise an existing questionnaire to be more comprehensive. This course also provides basic information for the professional to remember when interviewing patients and in minimizing the risks associated with treating patients, especially those with medical conditions; and assist in providing safe treatment to all patients in a dental practice. The health history is a very important component of the patient record. By using a comprehensive form, the office can properly treat patients and also prevent possible medical emergencies from occurring in the dental office. The information contained in this course should allow the dental professional to design a health history 21 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Appendix A Appendix A. AHA Guidelines for Infective Endocarditis Prophylaxis. 22 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Appendix B Appendix B. Wallet Card. All dental procedures that involve manipulation of gingival tissue or the periapical region of teeth, or perforation of the oral mucosa* PREVENTION OF INFECTIVE (BACTERIAL) ENDOCARDITIS Wallet Card This wallet card is to be given to patients (or parents) by their physician. Healthcare professionals: Please see back of card for reference to the complete statement. *Antibiotic prophylaxis is NOT recommended for the following dental procedures or events: routine anesthetic injections through noninfected tissue; taking dental radiographs; placement of removable prosthodontic or orthodontic appliances; adjustment of orthodontic appliances; placement of orthodontic brackets; and shedding of deciduous teeth and bleeding from trauma to the lips or oral mucosa. Name: _________________________________________ needs protection from INFECTIVE (BACTERIAL) ENDOCARDITIS because of an existing heart condition. Antibiotic Prophylactic Regimens for Dental Procedures Diagnosis: ______________________________________ Prescribed by: __________________________________ Date: __________________________________________ Situation You received this wallet card because you are at increased risk for developing adverse outcomes from infective endocarditis (IE), also known as bacterial endocarditis (BE). The guidelines for prevention of IE shown in this card are substantially different from previously published guidelines. This card replaces the previous card that was based on guidelines published in 1997. The American Heart Association’s Endocarditis Committee together with national and international experts on IE extensively reviewed published studies in order to determine whether dental, gastrointestinal (GI), or genitourinary (GU) tract procedures are possible causes of IE. These experts determined that there is no conclusive evidence that links dental, GI, or GU tract procedures with the development of IE. Regimen—Single Dose 30-60 minutes before procedure Adults Children Oral Amoxicillin 2g 50 mg/kg Unable to take oral medication Ampicillin OR 2 g IM or IV* 50 mg/kg IM or IV Cefazolin or ceftriaxone 1 g IM or IV 50 mg/kg IM or IV Cephalexin**† 2g 50 mg/kg 600 mg 20 mg/kg Azithromycin or clarithromycin 500 mg 15 mg/kg Cefazolin or ceftriaxone† 1 g IM or IV 50 mg/kg IM or IV OR Clindamycin 600 mg IM or IV 20 mg/kg IM or IV Allergic to penicillins or ampicillin— Oral regimen The current practice of giving patients antibiotics prior to a dental procedure is no longer recommended EXCEPT for patients with the highest risk of adverse outcomes resulting from IE (see below on this card). The Committee cannot exclude the possibility that an exceedingly small number of cases, if any, of IE may be prevented by antibiotic prophylaxis prior to a dental procedure. If such benefit from prophylaxis exists, it should be reserved ONLY for those patients listed below. The Committee recognizes the importance of good oral and dental health and regular visits to the dentist for patients at risk of IE. Agent Allergic to penicillins or ampicillin and unable to take oral medication OR Clindamycin OR *IM—intramuscular; IV—intravenous **Or other first or second generation oral cephalosporin in equivalent adult or pediatric dosage. †Cephalosporins should not be used in an individual with a history of anaphylaxis, angioedema or urticaria with penicillins or ampicillin. The Committee no longer recommends administering antibiotics solely to prevent IE in patients who undergo a GI or GU tract procedure. Changes in these guidelines do not change the fact that your cardiac condition puts you at increased risk for developing endocarditis. If you develop signs or symptoms of endocarditis—such as unexplained fever —see your doctor right away. If blood cultures are necessary (to determine if endocarditis is present), it is important for your doctor to obtain these cultures and other relevant tests BEFORE antibiotics are started. Gastrointestinal/Genitourinary Procedures: Antibiotic prophylaxis solely to prevent IE is no longer recommended for patients who undergo a GI or GU tract procedure, including patients with the highest risk of adverse outcomes due to IE. Other Procedures: Procedures involving the respiratory tract or infected skin, tissues just under the skin, or musculoskeletal tissue for which prophylaxis is reasonable are discussed in the updated document (reference below). Antibiotic prophylaxis with dental procedures is reasonable only for patients with cardiac conditions associated with the highest risk of adverse outcomes from endocarditis, including: Adapted from Prevention of Infective Endocarditis: Guidelines From the American Heart Association, by the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease. Circulation, 2007; 116: 1736-1754. Accessible at http://circ. ahajournals.org/cgi/reprint/CIRCULATIONAHA.106.183095. • Prosthetic cardiac valve or prosthetic material used in valve repair • Previous endocarditis • Congenital heart disease only in the following categories: Healthcare Professionals—Please refer to these recommendations for more complete information as to which patients and which procedures need prophylaxis. –Unrepaired cyanotic congenital heart disease, including those with palliative shunts and conduits –Completely repaired congenital heart disease with prosthetic material or device, whether placed by surgery or catheter intervention, during the first six months after the procedure* –Repaired congenital heart disease with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization) The Council on Scientific Affairs of the American Dental Association has approved this statement as it relates to dentistry. • Cardiac transplantation recipients with cardiac valvular disease *Prophylaxis is reasonable because endothelialization of prosthetic material occurs within six months after the procedure. National Center 7272 Greenville Avenue Dallas, Texas 75231-4596 americanheart.org Dental procedures for which prophylaxis is reasonable in patients with cardiac conditions listed above. © 2008, American Heart Association. All Rights Reserved. Lithographed in Canada. 50-1605 0805 23 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Appendix C Appendix C. Medical Questionnaire. MEDICAL QUESTIONNAIRE Patient Name Date Today Please check if you have any of the following problems: □ AIDS / HIV Positive □ Alcoholism □ Allergies Describe □ □ □ □ □ □ □ □ □ □ □ □ □ Anemia Arthritis Artificial heart valves Artificial joints Asthma Back problems Blood disease Cancer Chemotherapy Circulation problems Cortisone treatments Cough, persistent Cough, up blood Known Allergies: □ □ □ □ □ □ □ □ Local anesthetic Aspirin Penicillin Codeine Sulfa Iodine Latex Other: □ Diabetes □ Epilepsy □ Fainting □ Food allergies □ Glaucoma □ Headaches, frequent □ Headaches, migraines □ Heart murmur □ Heart, any problems Describe □ □ □ □ □ □ □ Hemophilia Herpes Hepatitis A B C High blood pressure Jaw pain Kidney disease Liver disease Mitral valve prolapse Nervous problems Pacemaker Psychiatric care Radiation treatment Respiratory disease Rheumatic fever Seizure disorders Shingles Shortness of breath Skin rash Stroke Surgical implants Swelling, feet or ankles Thyroid problems Tobacco use Tuberculosis Ulcers/colitis List any medications you are currently taking: Pre-medication required Consulting Physician Pharmacy Check if you have had any problems with the following: □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ Bad breath Bleeding, sensitive gums Clicking or popping jaw: right or left Food trapped between teeth Grinding or clenching teeth Loose teeth Broken fillings □ □ □ □ □ □ □ Periodontal treatment Sensitivity to cold Sensitivity to hot Sensitivity to sweets Sensitivity to biting Sores in mouth Staining Authorization: I have reviewed the information and answered all questions to the best of my knowledge. I understand this information will be used to determine the dental treatment I receive at this office and may be shared with other medical offices only as necessary. I will notify the office should any information change in the future. Signature of patient, or parent if a minor: Reviewed by: 24 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 Course Test Preview To receive Continuing Education credit for this course, you must complete the online test. Please go to: www.dentalcare.com/en-US/dental-education/continuing-education/ce76/ce76-test.aspx 1. Patients experiencing heart failure will often be taking a diuretic. Antibiotic prophylaxis prior to a dental procedure is still advised for patients with a history of infective endocarditis. a. b. c. d. Both statements are true. The first statement is true. The second statement is false. The first statement is false. The second statement is true. Both statements are false. 2. _______________, is a true statement regarding a health history. 3. The proper protocol for treating a patient who indicates that she/he has had a heart attack within the last 60 days is to _______________. a. b. c. d. e. a. b. c. d. The health history is a legal document Minor patients should not complete or sign their health history form Patients may not be truthful on a health history form A health history determines what infection control measures are used A, B, and C consult with the physician prior to treatment premedicate the patient with antibiotics prior to treatment consult with the physician and delay treatment until 6 months after the heart attack treat as normal, no precautions are necessary 4. When completing a health history on a patient _______________. 5. It is legally acceptable for a patient or guardian not to give informed consent if _______________. a. b. c. d. a. b. c. d. 6. the the the the patient patient patient patient is a minor and the parent is not present is mentally incapacitated is unconscious and needs emergency treatment refuses to sign the informed consent The law that prevents a dentist or his/her employees from disclosing protected health information for reasons other than treatment, payment or health care operations without the patient’s written permission is _______________. a. b. c. d. 7. it should be short and concise so as not to offend the patient it should be completed only on the patient's first visit to the office all information used in conjunction with treatment is the property of the patient all information used in conjunction with treatment is protected by HIPAA Ethics and Jurisprudence Act Americans with Disabilities Act Health Insurance Portability and Accountability Act Dental Practice Act If a dental practice needs additional information about patients from their physician, they should _______________. a. b. c. d. have the patient sign a release information form that is sent to the physician call the physician and have the dentist speak to him/her directly have the patient call the physician and report back to the dentist force the patient to tell as HIPAA laws will not allow a physician to release information to the dentist 25 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 8. The health history is to be updated _______________. 9. If a patient appears to be short of breath while being escorted from the reception area to the treatment room, ____________ might be suspected. a. verbally at each office visit b.yearly c.biannually d. only as the patient reports changes a. a latex allergy b. a diabetic condition c.COPD d. a blood dyscrasia 10. After reviewing a patient’s health history, the dentist determines that the patient is an ASA Class III patient. The next step is _______________. a. b. c. d. to consult the patient’s physician prior to treatment that no special precautions should be taken for the dental team to practice their protocols for medical emergencies the patient should receive prophylactic antibiotics 11. If a diabetic patient presents for treatment and indicates that they did not eat or take their insulin prior to their appointment, the dental assistant should _______________. a. b. c. d. inform the dentist and give orange juice to the patient inform the dentist, who can give the patient an insulin injection call the patient's physician to find out if the patient's disease is well controlled reappoint the patient and remind them that it is very important that they eat and take their insulin before their next appointment 12. ____________ is the first and most important drug to be administered to a patient having an anaphylactic reaction to all allergens. a.Corticosteroids b.Benadryl c.Epinephrine d.Glucose 13. A patient presents for treatment and gives no indication on his health history that he has any type of cardiovascular disease, but his ankles and feet are very swollen. When questioned, the patient indicates that his feet “always look this way.” The patient should be _______________. a. b. c. d. prescribed a diuretic referred for a medical evaluation before proceeding with treatment reassured that it happens to lots of patients assumed to have cardiovascular disease and treat normally 14. A special consideration when treating patients with diabetes and kidney disease is that they may be prone to experience _______________. a. b. c. d. severe xerostomia high incidence of caries excessive bleeding lack of manual dexterity 26 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 15. If a patient indicates that he has had a fever and bloody cough for several weeks, the dentist would _______________. a. b. c. d. suspect that the patient has infectious tuberculosis and defer treatment suspect that the patient has HIV/AIDS and treat normally suspect that the patient has HIV/AIDS and treat with special precautions treat as normal, a bloody cough has no bearing on dental treatment 16. _______________ is a true statement concerning a medical alert label on a patient record folder. a. Place the medical alert sticker on the outside of the patient record folder so the dental team members take extra precautions with regard to infection control b. No alert notice is ever necessary on any part of the patient record c. Place the sticker on the outside of the partient record folder so all dental team members take extra precautions when prescribing medications d. Only place the alert sticker on the inside of the folder to protect the patient’s privacy 17. According to the CDC, elective dental treatment should be postponed on any patient who has or is suspected of having ____________. a.hemophilia b.AIDS c. active TB d. All of the above. 18. If a patient isn’t sure what particular medication he is taking, the dental assistant could show the patient pictures of drugs contained in _______________. a. b. c. d. the Merck Manual a pharmacology textbook the Physicians' Desk Reference The ADA Guide to Dental Therapeutics 19. If a patient indicates a latex allergy, the best time to schedule their dental appointment is _______________ to prevent exposure to airborne latex. a. b. c. d. whenever it is convenient for the patient at the beginning of the day at the end of the day when they are rested 20. A patient may have a latex allergy if they indicate a food allergy to _______________. a.oranges b.apples c.bananas d.pears 21. _______________ is the law or agency that protects the rights of HIV+ and AIDS patients to receive dental and medical treatment. a. b. c. d. Centers for Disease Control and Prevention American Dental Association American Medical Association Americans with Disabilities Act 27 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 22. _______________ is a term used to describe “dry mouth” or lack of saliva. a.Halitosis b.Hyperplasia c.Xerostomia d. Salivary stone 23. Patients with unstable or uncontrolled angina should wait for at least _____ days after their angina is stabilized to receive dental treatment. a.10 b.30 c.60 d.120 24. Medical information should include _______________. a. b. c. d. family medical history current medications past medical history All of the above. 25. As a rule, patients with a systolic pressure greater than _____ and/or a diastolic pressure greater than _____ should be referred for medical consultation and treatment and dental treatment should be delayed. a.120/80 b.160/95 c.170/70 d.150/100 28 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 References 1. Advisory statement. Antibiotic prophylaxis for dental patients with total joint replacements. American Dental Association; American Academy of Orthopaedic Surgeons. J Am Dent Assoc. 1997 Jul; 128(7):1004-8. 2. American Dental Association. HIPAA Compliance Manual. 2002. 3. American Dental Association. Prevention of Infective Endocarditis: Guidelines from the American Heart Association. J Am Dent Assoc. 2007 Jun;138(6);739-45, 747-60. 4. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2007 Jun;138(6):739-45, 747-60. 5. American Heart Association. Understanding Blood Pressure Readings. Updated November 17, 2014. Accessed January 13, 2015. 6. Beers MH, Berkow R. The Merck Manual of Diagnosis and Therapy. 17th Ed. Merck & Company, Inc. 1999. 7. Bird DL, Robinson DS. Modern Dental Assisting. 11th Ed. Elsevier Saunders, St. Louis, MO. 2015. 8. Centers for Disease Control and Prevention. Division of Oral Health. Slide 101: Preventing Transmission of TB in Dental Settings. Guidelines for Infection Control in Dental Health-Care Settings—2003. Slides 99-101. Accessed January 13, 2015. 9. Centers for Disease Control and Prevention. Division of Oral Health. Infection Control. Frequently Asked Questions - Contact Dermatitis and Latex Allergy. Accessed January 13, 2015. 10. Dajani AS, Taubert KA, Wilson W, et al. Prevention of bacterial endocarditis. Recommendations by the American Heart Association. JAMA. 1997 Jun;11;277(22):1794-801. 11. Grimes EB. Medical Emergencies. Essentials for the Dental Professionals. 2nd Ed. Pearson/ Prentice Hall. UpperSaddle River, NJ, 2012. 12. Kleinman DV, Horowitz AM. Oral Health Literacy. Woman Dentist Jour. 2007 Jul;24-28. 13. Little JW, Falace DA. Dental Management of the Medically Compromised Patient, 6th Ed. Mosby Inc. 2002. 14. Malamed SF. Medical Emergencies in the Dental Office. 6th Ed. Mosby. St. Louis, MO. 2007. 15. PDRHealth. Physicians Desk Reference®. Accessed January 13, 2015. 16. Phinney DJ, Halstead JH. Dental Assisting: A Comprehensive Approach. Delmar Cengage Learning, 4th Ed. Clifton Park, NY. 2013. 17. Tyler MT. Editor, Clinician’s Guide to Treatment of Medically Complex Dental Patients. American Academy of Oral Medicine, 2001. 18. US Department of Health and Human Services. Health Insurance Portability and Accountability Act of 1996. Accessed January 12, 2015. 19. Public Law 101-336 Americans with Disabilities Act of 1990. July 26, 1990. Accessed January 12, 2015. 20. Woodall IR. Comprehensive Dental Hygiene Care. 4th Ed.Mosby-Year Book, Inc. 1993. 21. American Heart Association. Infective Endocarditis. Updated October 14, 2014. Accessed January 14, 2015. 22. American Society of Anesthesiologists. ASA Physical Status Classification System. Accessed January 15, 2015. 29 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015 About the Authors Mary Govoni, CDA, RDA, RDH, MBA Mary Govoni, CDA, RDA, RDH, MBA, is an internationally recognized speaker, author and consultant on clinical efficiency, ergonomics, OSHA & HIPAA compliance, infection control and team communication. Mary is a past president and a life member of the American Dental Assistants Association, a member of the American Dental Hygienists Association, a consultant to the American Dental Association Council on Dental Practice, a member of the Organization for Safety and Asepsis Procedures, the National Speakers Association, and the Academy of Dental Management Consultants and the Speaking and Consulting Network. She is also a featured speaker on the ADA Continuing Education and lifelong learning seminar series. Wilhemina Leeuw, MS, CDA Wilhemina Leeuw, MS, CDA is a Clinical Assistant Professor of Dental Education at Indiana University Purdue University, Fort Wayne. A DANB Certified Dental Assistant since 1985, she worked in private practice over twelve years before beginning her teaching career in the Dental Assisting Program at IPFW. She is very active in her local and Indiana state dental assisting organizations. Prof. Leeuw’s educational background includes dental assisting – both clinical and office management, and she received her Master’s degree in Organizational Leadership and Supervision. 30 ® ® Crest + Oral-B at dentalcare.com Continuing Education Course, Revised January 20, 2015





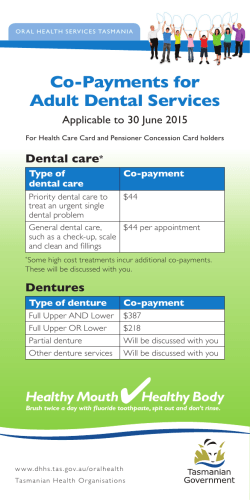
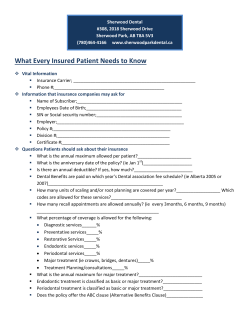



© Copyright 2025