
Exercise ventilation inefficiency in heart failure: pathophysiological and clinical significance Review *
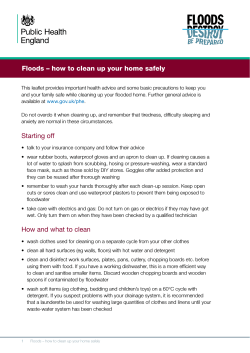
Review European Heart Journal (2007) 28, 673–678 doi:10.1093/eurheartj/ehl404 Exercise ventilation inefficiency in heart failure: pathophysiological and clinical significance ´rard2* Gabriele Tumminello1, Marco Guazzi1, Patrizio Lancellotti2, and Luc A. Pie 1 Cardiopulmonary Unit, Cardiology Division, University of Milano, San Paolo Hospital, 20142 Milano, Italy and 2 Department `ge, Belgium of Cardiology, University Hospital Sart Tilman, Boite 35 CHU, B-4000 Lie Received 24 May 2006; revised 8 September 2006; accepted 7 November 2006; online publish-ahead-of-print 23 November 2006 KEYWORDS Heart failure; Ventilation; Exercise; Periodic breathing Introduction Heart failure (HF) is a complex syndrome characterized by myocardial dysfunction and an impaired regulatory function of multiple organ systems. Exercise ventilation inefficiency is a hallmark manifestation of HF that provides additive clinical and prognostic value.1 The abnormal ventilatory response to exercise is identified by an increased slope of ventilation vs. CO2 production (VE/VCO2) to incremental workload.2 The origin of an increased and inefficient ventilatory response to incremental exercise is multifactorial and no definitive agreement on its pathogenetic bases has yet been provided. Recently, interest has also been addressed to the clinical significance of an oscillatory ventilatory and gas exchange kinetics; a pattern that resembles Cheyne Stokes respiration during sleep.3 This article highlights current proposed pathogenetic views for an abnormal ventilatory response to exercise in patients with left ventricular (LV) dysfunction, with emphasis on their clinical correlates and potential perspectives. Increased VE/VCO2 slope Measuring VE/VCO2 slope is of peculiar clinical relevance because this variable has been repeatedly identified as a strong and independent prognostic marker in a large subset of HF patients with exercise limitation of mild-tointermediate severity.4–12 Mathematically, the VE/VCO2 * Corresponding author. Tel: þ32 4 366 71 94; fax: þ32 4 366 71 95. E-mail address: lpierard@chu.ulg.ac.be slope is determined by three factors: the amount of CO2 produced (VCO2), the physiological dead space/tidal volume ratio (VD/VT), and the arterial CO2 partial pressure (PaCO2) ˙E ¼ 863 V ˙CO2/ according to the following equation: V [PaCO2 (1–VD/VT)]. Three different mechanisms for an increased ventilatory requirement to a given CO2 production have been reported (Figure 1): (i) increased dead space and consequent waste ventilation;10,11,13 (ii) early occurrence of haematic lactic acidosis,11 and (iii) abnormal chemoreflex and/or metaboreflex activity.14,15 In HF patients, a reduction in static lung mechanics (i.e. reduced vital capacity and forced expiratory volume in 1 s) is a common finding.11 The occurrence of restrictive lung changes is implicated in a lower rate of increase in tidal volume (VT), higher respiratory rate (RR), and dead space to tidal volume ratio (VD/VT) for a given workload.13 Consonant with an increased dead space ventilation is the demonstration that lung interstitial fibrosis and remodelling of alveolar-capillary membrane are additional features of changes occurring at the lung level.16,17 Thus, the abnormalities in alveolar gas membrane conductance along with the occurrence of ventilation/perfusion mismatch due to the combination of impaired regional lung perfusion and abnormal increase in pulmonary capillary pressure seem to be implicated in the increased ventilatory requirement during exercise.18 A limited increase in cardiac output is certainly the initial determinant of exercise intolerance and muscle fatigue in these patients. The imbalance between cardiac output and metabolic request by working muscles explains the development of early lactic acidosis during exercise, favoured by & The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: journals.permissions@oxfordjournals.org Downloaded from by guest on October 15, 2014 Heart failure (HF) is a complex syndrome characterized by myocardial dysfunction and a poor prognosis. Among multiple markers of severity, an exercise ventilation inefficiency has important clinical and prognostic value. The pathophysiology determining exercise ventilatory inefficiency is complex and not definitively clarified. Three different mechanisms have been identified: (i) increased dead space, (ii) early occurrence of lactic acidosis, and (iii) abnormal chemoreflex and/or metaboreflex activity. Besides its prognostic value, abnormal ventilation can be influenced by pharmacological and non-pharmacological therapies such as b-blockers, selective cyclic 30 –50 guanosine monosphosphate phosphodiesterase inhibitors, physical training, and nocturnal continuous positive airway pressure. There is an increasing interest for the exercise periodic breathing, which is frequently associated with HF syndrome and has prognostic importance. The precise mechanisms sustaining exercise periodic breathing are not fully defined but ventilatory and metabo-haemodynamic hypotheses have been proposed. 674 G. Tumminello et al. Figure 1 concomitant muscle deconditioning and increased type IIb muscular fibres expression.19 Early lactic acidosis may explain the occurrence of an increased inefficient ventilation since the early stages of exercise. It has been demonstrated that patients with severe HF exhibit a significant PaCO2 reduction at peak exercise8,12,20,21 and even during a submaximal constant workload at 50 W.22 Evidence for a major putative role of lactic acidosis in the augmented ventilatory response is supported by the finding of reduced PaCO2 levels in HF compared with control subjects. PaCO2 is stable or gradually increase during an incremental exercise up to the beginning of respiratory compensation for lactic acidosis. Subsequently, for the higher levels of developing lactic acidosis, PaCO2 decreases accordingly until exercise termination. The demonstration that patients with a lower PaCO2 at peak exercise are those exposed at a high risk of death10 supports this hypothesis. This mechanism is nevertheless debated. Wensel et al.23 recently showed that during the recovery phase of exercise, high levels of lactate do not correlate with VE/ VCO2 slope. Moreover, the decrease in PaCO2 may also be primarily related to the hyperventilatory response necessary to overcome ventilation–perfusion mismatch and high dead space ventilation.11,24 There is, however, no doubt that most of the pathophysiological evidence for an increase in the ventilatory response to exercise is related to an impaired breathing control. This may occur at several levels and involve the peripheral25 and/or central26 chemoreflex control as well as the increased neural reflexogenic activity arising from working muscle ergoreceptors.27 Chemoreflex deregulation may occur early in the natural history of HF. In 60 patients14 with ischaemic heart disease without overt HF, VE/VCO2 slope was found to correlate with the level of central chemosensitivity. Changes in VE/VCO2 slope correlated with an improved chemoreflex sensitivity after a 3-month period of exercise training. Although an increased chemoreflex activation in patients with overt HF is well established, the relative contributory role of central vs. peripheral activation is still undefined. Interestingly, Ciarka et al.15 have recently reported that in heart transplant recipients, central chemoreflex activity may reverse to normal despite persistent peripheral impairment, which correlates positively with the increased VE/VCO2 during exercise. Overactivaton of ergoreceptors (amielinic fibres located in the skeletal muscles) to metabolic products such as Kþ and Hþ triggers a series of reflex responses such as sympathetic activation, vasoconstriction, and hyperventilation.27 Ergoreflex activation independently correlates with VE/ VCO2 slope and inversely with exercise tolerance in HF patients.28 The central nervous system processing involvement in the deregulated ventilatory response to exercise has been evaluated. Rosen et al.29 did not report major differences between the regional brain activation at rest, after exercise, and during isocapnic hyperventilation in HF patients and controls. Leptin, an hormone that may be involved in the control activity of central chemosensitivity, was found be a marker of increased VE/VCO2 slope.30 Impaired ventilation during exercise is a common finding in HF patients even in right HF due to primary pulmonary hypertension (PPH). PPH patients present a ventilation profile similar to HF patients, consisting in increased VE/ VCO2 slope, ventilated dead space, and concomitant reduced PaCO2. The difference between the two patterns is the underlying pathophysiological mechanisms. PPH results primarily from the abnormalities of pulmonary vasculature consisting in intimal fibrosis, medial hypertrophy leading to increased pulmonary vascular resistances, and loss of the physiological vasodilator response to exercise. These changes determine a ventilation/perfusion Downloaded from by guest on October 15, 2014 Mechanisms involved in the genesis of increased VE/VCO2 slope and EPB. PaCO2, arterial partial pressure of CO2; for details see text. Exercise ventilation inefficiency in HF mismatch and increased VD/VT ratio, due to hypoperfusion of ventilated alveoli, resulting in an increased VE/VCO2 ratio.31 Another trigger for the increased ventilatory response to exercise is the early lactic acidosis at low work rate32 and the consequent production of CO2 due to the bicarbonate dissociation, as it buffers the newly formed lactic acid. The last mechanisms are the arterial hypoxemia and failure in delivering the requested O2 to the exerting muscles due to: (i) reduced pulmonary capillary bed with short red blood cell transit, (ii) possible right-to-left shunt through a patent foramen ovale,33 and (iii) failure in cardiac output.32 The right ventricle is unable to increase the pulmonary and consequent systemic blood flow against the elevated vascular resistance. Interestingly, the role of an impaired chemoreflex and ergoreflex control in PPH has not been tested.34 Nevertheless, in PPH patients, VE/VCO2 better correlates with the NYHA class than the resting pulmonary haemodynamics.32 The ventilatory pattern is also important for unmasking the presence of a right-to-left shunt as evidenced by an abrupt decrease in end-tidal CO2 with concomitant increase in endtidal O2 and respiratory exchange ratio (RER).33 VE/VCO2 slope: prognostic relevance and therapeutic implications VE/VCO2 slope appears to be favourably influenced by beta-blockade, an intervention that improves prognosis despite unchanged exercise performance and peak VO2.41 In a retrospective analysis performed in 614 HF patients, an association was found between b-blocker administration and an improved ventilatory efficiency.42 Multiple explanations have been proposed for this favourable interaction. b-Blockers may attenuate catecholamine activation of central and peripheral chemoreceptors.43 Moreover, HF is associated with cardiac b-adrenoceptor desensitization and the process may also involve the pulmonary system;44 a resensitization receptor process induced by b-blockers may favourably influence pulmonary ventilation–perfusion matching and haemodynamics during exercise, leading to a more efficient ventilation during exercise. An intriguing hypothesis is the postulated effects of b-blockers on metabolic activity.45 In the early and intermediate exercise stages, energy is supplied predominantly by fatty acids while at further exercise stages, it is supplied by carbohydrates. Fatty acid oxidation yields to an RER, which is given by VCO2/VO2 ratio of 0.7 compared with 1.0 when glucose is the only energy substrate. Sympathetic nervous system activation during exercise shifts the metabolic substrate towards carbohydrate utilization pathway. b-Blockers may delay the switch from fatty acid to carbohydrate substrate utilization keeping exercise VCO2/VO2 ratio at lower levels. As a result, for a given O2 consumption, less CO2 is produced. In other words, an improved ventilation efficiency could be driven by a lower CO2 production due to a prolonged utilization of fatty acid substrate. Modulation of the nitric oxide pathway by selective cyclic 30 250 guanosine monophosphate phosphodiesterase inhibition, such as sildenafil, has provided evidence for a VE/ VCO2 slope lowering effect. This therapeutic effect was found to correlate with an improvement in alveolarcapillary membrane conductance.39 Non-pharmacological therapy that directly influences the inefficient ventilation includes physical training and nocturnal continuous positive airway pressure (CPAP). Treating central sleep apnoea with CPAP improves inefficient ventilation46 probably through a combined positive effect on LV ejection fraction,47 sympathetic activity, and chemosensitivity.48 Similarly, exercise-training programs improve inefficient ventilation by several mechanisms: (i) reduced sympathetic nerve activity and catecholamine concentration,49 (ii) restoration of normal muscular metabolism,50 (iii) reduction in metabolic mediators involved in ergoreflex activation,51 and (iv) improved alveolar-capillary membrane diffusion properties.40 Exercise periodic breathing Figure 2 Examples of ventilatory response to exercise: ( S ) healthy subject: maximal oxygen consumption is 40 mL/min/kg, VE/VCO2 slope 24; () mild HF patient (NYHA class 2) with preserved exercise capacity and ventilation: maximal oxygen consumption 29 mL/min/kg, VE/VCO2 slope 25; (V) severe HF patient (NYHA class 3) with reduced exercise capacity and hyperventilation: maximal oxygen consumption 16 mL/min/kg, VE/VCO2 slope 41. There is an increasing interest for an abnormal breathing disorder, identified as exercise periodic breathing (EPB), which may be observed in HF patients (Figure 3). Since 1986, Weber described a particular ‘saw-toothed’ ventilatory response to exercise in some HF patients.52 EPB ventilation is characterized by oscillations in ventilation, VO2 and VCO2, with a period and amplitude that may be quite different across HF populations. Its definition and classification remain quite arbitrary and definitive criteria are still needed. Kremser et al.53 classified the periodism as an oscillation of 1 min, a .15% amplitude of the resting Downloaded from by guest on October 15, 2014 VE/VCO2 slope (Figure 2) has repeatedly emerged as an independent powerful prognostic marker in HF patients with intermediate exercise limitation. Following the landmark paper published by Mancini et al.35 in the early 1990s, the prognostic superiority of VE/VCO2 slope over peak VO2 has been progressively documented and strengthened by a series of studies. As originally proposed by Chua et al.,4 the large majority of these studies have identified and confirmed the prognostic value of a cut-off of 34. Remarkably, VE/VCO2 slope provides incremental prognostic value in patients with preserved peak VO2 (.18 mL/min/ kg)36 and in patients with diastolic HF.37 Although the exercise ventilation inefficiency is not considered as a specific target of HF therapeutic strategies, an improvement in VE/VCO2 slope has been demonstrated after several therapeutic approaches.38–40 675 676 G. Tumminello et al. severe sleep-disordered breathing (apnoea–hypopnea index . 30/h). In this study, a tight pathogenic link between EPB and oscillatory sleep-disordered breathing was observed. The finding of EPB may, therefore, help in the decision making for further investigations, such as screening for a sleep apnoea syndrome. However, several questions on this ventilatory abnormality remain unanswered, such as the real incidence of this phenomenon, the uncertain criteria for EPB definition, its prognostic importance compared with VE/VCO2 slope, and the most effective therapeutic approach.64 Figure 3 Example of EPB in a HF patient. value, and a duration of up to 66% of the exercise protocol. Leite et al.54 diagnosed EPB based on the presence of frequent (at least three cycles), regular (standard deviation of three consecutive cycle lengths within 20% of their average), and ample (minimal amplitude of 5 L/min) minute ventilation oscillations. EPB pathophysiology and prognostic relevance HF is frequently associated with functional mitral regurgitation (MR), which can be due to several mechanisms such as valve annular dilatation, LV distortion, and mitral deformation.65 MR yields to a significant rise in pulmonary venous, capillary, and arterial pressures.66,67 MR quantification is usually performed at rest and despite a relevant and compelling pathophysiological background, it is often overlooked that MR may abruptly rise during exercise. Notably, the degree of MR at rest is not predictive of exercise-induced changes in MR65 and a strong correlation has been reported between MR exercise-induced changes and transtricuspid pressure gradient.68 The excessive rise in pulmonary wedge pressure18 and pulmonary artery pressure69 is likely related to an increased ventilation during exercise and dyspnoea sensation. Many HF patients, without significant MR at rest, may develop a functional MR during exercise resulting in worsening of dyspnoea and hyperventilation.69 In order to better quantify the role of functional MR in the development of dyspnoea during exercise in the individual patient, the appreciation of functional MR may be integrated with a contemporary evaluation of the effective ventilation during exercise. Remarkably, the occurrence of exertional hyperventilation may potentially suggest the presence of functional MR, which could play a role in the hyperventilatory response. Finally, the presence of functional MR is a further relevant marker for the prognostic stratification of HF patients by predicting the occurrence of acute pulmonary oedema70 and guarded prognosis.71 Conclusions HF syndrome is a complex syndrome involving several organ systems. Exercise limitation is a typical manifestation that is accompanied by increased significant dyspnoea and ventilation inefficiency. Characterization of abnormalities in exercise ventilation may help clinicians to better define clinical condition and risk stratification. Conflict of interest: none declared. References 1. Coats A. Why ventilatory inefficiency matters in chronic heart failure? Eur Heart J 2005;26:426–427. 2. Sun XG, Hansen JE, Garatachea N, Storer TW, Wasserman K. Ventilatory efficiency during exercise in healthy subjects. Am J Respir Crit Care Med 2002;166:1443–1448. Downloaded from by guest on October 15, 2014 The precise mechanisms sustaining EPB are unclear but ventilatory and metabo-haemodynamic hypotheses have been proposed (Figure 1). The ventilatory hypothesis is based on the demonstration of instability of ventilatory control due to an abnormal chemoreceptors feedback. Fluctuating afferent signalling to ventilatory centres could promote oscillatory patterns in VO2 and VCO2. In experimental conditions, an increase in chemoreceptor discharge induced an oscillatory ventilation that was abolished by hyperoxia.55 Ponikowski et al.56 identified a link between an enhanced chemosensitivity and an oscillatory breathing at rest. Modulation or blockade of peripheral chemoreflex activity by hyperoxia or dihydrocodeine can reduce or abolish the oscillatory ventilatory pattern. The impaired feedback in the ventilatory control could also involve a prolonged circulatory time. A long lung-to-ear circulatory delay has been reported in HF patients and could induce a desynchronization between the lung and the ventilatory control system leading to a periodic respiration.57 Moreover, administration of milrinone, a positive inotropic and vasodilatatory agent, is capable of abolishing the periodic breathing in HF patients.58 Some data are, however, against this hypothesis. Gases oscillatory kinetics do not seem to be synchronous with the ventilatory kinetics and voluntary simulated periodic breathing failed to reproduce the magnitude and phase of spontaneous oscillations of HF patients.59 Francis et al.60 reported that the magnitude and the synchronism between metabolic and ventilatory fluctuations in spontaneous periodic breathing are also reproducible with a voluntary periodic breathing if the latter is corrected for the workload at which the ventilation is performed. Nonetheless, echocardiographic and radionuclide studies have provided evidence of stroke volume fluctuations.61,62 In patients with severe HF evaluated for heart transplantation, EPB was found to be the single predictor of cardiac death.54 In a recent report by Corra et al.,63 periodic breathing prevalence was 21% among 150 HF patients, 78% of whom presenting with central sleep apnoea and Future implications: mitral regurgitation and excessive exercise ventilation Exercise ventilation inefficiency in HF 24. Tanabe Y, Hosaka Y, Ito M, Ito E, Suzuki K. Significance of end-tidal PCO2 response to exercise and its relation to functional capacity in patients with chronic heart failure. Chest 2001;119:811–817. 25. Ponikowski P, Chua TP, Piepoli M, Ondusova D, Webb-Peploe K, Harrington D, Anker SD, Volterrani M, Colombo R, Mazzuero G, Giordano A, Coats AJ. Augmented peripheral chemosensitivity as a potential input to baroreflex impairment and autonomic imbalance in chronic heart failure. Circulation 1997;96:2586–2594. 26. Narkiewicz K, Pesek CA, van de Borne PJ, Kato M, Somers VK. Enhanced sympathetic and ventilatory responses to central chemoreflex activation in heart failure. Circulation 1999;100:262–267. 27. Piepoli M, Clark AM, Volterrani M, Adamopoulos S, Sleight P, Coats AJ. Contribution of muscle afferents to the hemodynamic, autonomic, ventilatory responses to exercise in patients with chronic heart failure. Circulation 1996;93:940–952. 28. Chua TP, Clark AL, Amadi AA, Coats AJ. Relation between chemosensitivity and the ventilatory response to exercise in chronic heart failure. J Am Coll Cardiol 1996;27:650–657. 29. Rosen SD, Murphy K, Leff AP, Cunningham V, Wise RJ, Adams L, Coats AJ, Camici PG. Is central nervous system processing altered in patients with heart failure? Eur Heart J 2004;25:952–962. 30. O’Donnell CP, Tankersley CG, Polotsky VP, Schwartz AR, Smith PL. Leptin, obesity, and respiratory function. Respir Physiol 2000;119: 163–170. 31. Ting H, Sun X, Chuang M, Lewis D, Hansen J, Wasserman K. A noninvasive assessment of pulmonary perfusion abnormality in patients with primary pulmonary hypertension. Chest 2001;119:824–832. 32. Sun X, Hansen J, Oudiz R, Wasserman K. Exercise pathophysiology in patients with primary pulmonary hypertension. Circulation 2001;104: 429–435. 33. Sun X, Hansen J, Oudiz R, Wasserman K. Gas exchange detection of exercise-induced right-to-left shunt in patients with primary pulmonary hypertension. Circulation 2002;105:54–60. 34. Guazzi M, Opasich C. Functional evaluation of patients with chronic pulmonary hypertension. Ital Heart J 2005;6:789–794. 35. Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr, Wilson JR. Value of peak oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991;83:778–786. 36. Ponikowski PP, Chua TP, Francis DP, Capucci A, Coats AJ, Piepoli MF. Muscle ergoreceptor overactivity reflects deterioration in clinical status and cardiorespiratory reflex control in chronic heart failure. Circulation 2001;6:2324–2330. 37. Guazzi M, Arena R, Myers J. Cardiopulmonary exercise testing in the clinical and prognostic assessment of diastolic heart failure. J Am Coll Cardiol 2005;46:1883–1890. 38. Coats AJ, Adamopoulos S, Radaelli A, McCance A, Meyer TE, Bernardi L, Solda PL, Davey P, Ormerod O, Forfar C. Controlled trial of physical training in chronic heart failure. Circulation 1992;85:2119–2131. 39. Guazzi M, Tumminello G, DiMarco F, Fiorentini C, Guazzi MD. The effect of phosphodiesterase-5 inhibition with sildenafil on pulmonary hemodynamics and diffusion capacity, exercise ventilation efficiency, and oxygen uptake kinetics in chronic heart failure. J Am Coll Cardiol 2004; 44:2339–2348. 40. Guazzi M, Reina G, Tumminello G, Guazzi MD. Improvement of alveolarcapillary membrane diffusing capacity with exercise training in chronic heart failure. J Appl Physiol 2004;97:1866–1873. 41. Agostoni PG, Guazzi M, Bussotti M, De Vita S, Palermo P. Carvedilol reduces the inappropriate increase of ventilation during exercise in heart failure patients. Chest 2002;122:2062–2067. 42. Wolk R, Johnson BD, Somers VK, Allison TG, Squires RW, Gau GT, Olson LJ. Effects of b-blocker therapy on ventilatory responses to exercise in patients with heart failure. J Card Failure 2005;5:333–339. 43. Butland RJ, Pang JA, Geddes DM. The selectivity of the beta-adrenoceptor for ventilation in man. Br J Clin Pharmacol 1982; 14:707–711. 44. Turki J, Green SA, Newman KB, Meyers MA, Liggett SB. Human lung cell beta 2 adrenergic receptors desensitize in response to in vivo administred beta-agonist. Am J Physiol 1995;269:L709–L714. 45. Clark AL, Cleland JGF. b-Blockers exercise ventilation in chronic heart failure. J Card Failure 2005;5:340–342. 46. Arzt M, Schulz M, Wensel R, Montalvan S, Blumberg FC, Riegger GA, Pfeifer M. Nocturnal positive airway pressure improves ventilatory efficiency during exercise in patients with chronic heart failure. Chest 2005;127:794–802. Downloaded from by guest on October 15, 2014 3. Bradley TD. The ups and downs of periodic breathing. Implication for mortality in heart failure. J Am Coll Cardiol 2003;41:2182–2184. 4. Chua TP, Ponikowski P, Harrington D, Anker SD, Webb-Peploe K, Clark AL, Poole-Wilson PA, Coats AJ. Clinical correlates and prognostic significance of the ventilatory response to exercise in CHF. J Am Coll Cardiol 1997;29:1585–1590. 5. Robbins M, Francis G, Pashkow FJ, Snader CE, Hoercher K, Young JB, Lauer MS. Ventilatory and heart rate response to exercise. Better predictors of heart failure mortality than peak oxygen consumption. Circulation 1999;100:2411–2417. 6. Kleber FX, Vietzke G, Wernecke KD, Bauer U, Opitz C, Wensel R, Sperfeld A, Glaser S. Impairment of ventilatory efficiency in heart failure: prognostic impact. Circulation 2000;101:2803–2809. 7. Ponikowski P, Francis DP, Piepoli MF, Davies LC, Chua TP, Davos CH, Florea V, Banasiak W, Poole-Wilson PA, Coats AJ, Anker SD. Enhanced ventilatory response to exercise in patients with chronic heart failure and preserved exercise tolerance. Marker of abnormal cardiorespiratory reflex control and predictor of poor prognosis. Circulation 2001;103: 967–972. 8. Gitt AK, Wasserman K, Kilkowski C, Kleemann T, Kilkowski A, Bangert M, Schneider S, Schwarz A, Senges J. Exercise anaerobic threshold and ventilatory efficiency identify heart failure patients for high risk of early death. Circulation 2002;106:3079–3084. 9. Francis DP, Shamim W, Davies LC, Piepoli MF, Ponikowski P, Anker SD, Coats AJ. Cardiopulmonary exercise testing for prognosis in chronic heart failure: continuous and independent prognostic value from VE/ VCO2 slope and peak VO2. Eur Heart J 2000;21:154–161. 10. Guazzi M, Reina G, Tumminello G, Guazzi MD. Exercise ventilation inefficiency and cardiovascular mortality in heart failure: the critical independent prognostic value of the arterial CO2 partial pressure. Eur Heart J 2005;26:472–480. 11. Wasserman K, Zhang YY, Gitt A, Belardinelli R, Koike A, Lubarsky L, Agostoni PG. Lung function and exercise gas exchange in chronic heart failure. Circulation 1997;96:2221–2227. 12. Wilson JR, Ferraro N. Exercise intolerance in patients with chronic heart failure: relation to oxygen transport and ventilatory abnormalities. Am J Cardiol 1983;51:1358–1563. 13. Myers J, Salleh A, Buchanan N, Smith D, Neutel J, Bowes E, Froelicher VF. Ventilatory mechanisms of exercise intolerance in chronic heart failure. Am Heart J 1992;124:710–719. 14. Tomita T, Takaki H, Hara Y, Sakamaki F, Satoh T, Takagi S, Yasumura Y, Aihara N, Goto Y, Sunagawa K. Attenuation of hypercapnic carbon dioxide chemosensitivity after postinfarction exercise training: possible contribution to the improvement in exercise hyperventilation. Heart 2003;89:404–410. 15. Ciarka A, Cuylits N, Vachiery JL, Lamotte M, Degaute JP, Naeije R, van de Borne P. Increased peripheral chemoreceptors sensitivity and exercise ventilation in heart transplant recipients. Circulation 2006; 113:252–257. 16. Guazzi M. Alveolar-capillary membrane dysfunction in heart failure: evidence of a pathophysiologic role. Chest 2003;124:1090–1102. 17. Guazzi M, Reina G, Tumminello G, Guazzi MD. Alveolar-capillary membrane conductance is the best pulmonary function correlate of exercise ventilation efficiency in heart failure patients. Eur J Heart Fail 2005; 7:1017–1022. 18. Wada O, Asanoi H, Miyagi K, Ishizaka S, Kameyama T, Seto H, Sasayama S. Importance of abnormal lung perfusion in excessive exercise ventilation in chronic heart failure. Am Heart J 1993;125:790–798. 19. Lipkin DP, Jones DA, Round JM, Poolen-Wilson PA. Abnormalities of skeletal muscle in patients with chronic heart failure. Int J Cardiol 1988;18:187–195. 20. Wilson JR, Ferraro N, Weber KT. Respiratory gas analysis during exercise as a noninvasive measure of lactate concentration in chronic congestive heart failure. Am J Cardiol 1983;51:1639–1643. 21. Perego GB, Marenzi GC, Guazzi M, Sganzerla P, Assanelli E, Palermo P, Conconi B, Lauri G, Agostoni PG. Contribution of PO2, P50 and Hb to changes in arteriovenous O2 content during exercise in heart failure. J Appl Physiol 1996;80:623–631. 22. Hachamovitch R, Brown HV, Rubin SA. Respiratory and circulatory analysis of CO2 output during exercise in chronic heart failure. Circulation 1991; 84:605–612. 23. Wensel R, Francis DP, Georgiadou P, Scott A, Genth-Zotz S, Anker SD, Coats AJ, Piepoli MF. Exercise hyperventilation in chronic heart failure is not caused by systemic lactic acidosis. Eur J Heart Fail 2005;7: 1105–1111. 677 678 59. Ben-Dov I, Siestsema KE, Casaburi R, Wasserman K. Evidence that circulatory oscillations accompany ventilatory oscillations during exercise in patients with heart failure. Am Rev Respir Dis 1992;145:776–781. 60. Francis DP, Davies LC, Piepoli M, Rauchhaus M, Ponikowski P, Coats AJ. Origin of oscillatory kinetics of respiratory gas exchange in chronic heart failure. Circulation 1999;100:1065–1070. 61. Maze SS, Kotler MN, Parry WR. Doppler evaluation of changing cardiac dynamics during Cheyne-Stokes respiration. Chest 1989;95:525–529. 62. Yajima T, Koike A, Sugimoto K, Miyahara Y, Marumo F, Hiroe M. Mechanism of periodic breathing in patients with cardiovascular disease. Chest 1994;106:142–146. 63. Corra U, Pistono M, Mezzani A, Braghiroli A, Giordano A, Lanfranchi P, Bosimini E, Gnemmi M, Giannuzzi P. Sleep and exertional periodic breathing in chronic heart failure prognostic importance and interdependence. Circulation 2006;113:44–50. 64. Guazzi M. Letter regarding article ‘Sleep and exertional periodic breathing in chronic heart failure: prognostic importance and interdependence’. Circulation 2006;114:e53. 65. Lancellotti P, Lebrun F, Pie ´rard LA. Determinants of exercise-induced changes in mitral regurgitation in patients with coronary artery disease and left ventricular dysfunction. J Am Coll Cardiol 2003; 42:1921–1928. 66. Weber KT, Janicky JS. Cardiopulmonary Exercise Testing. Valvular Heart Disease. Philadelphia: WB Saunders; 1986. p197–219. 67. Enriquez-Sarano M, Rossi A, Seward J, Bailey K, Tajik AJ. Determinants of pulmonary hypertension in left ventricular dysfunction. J Am Coll Cardiol 1997;29:153–159. 68. Lebrun F, Lancellotti P, Pie ´rard L. Quantitation of functional mitral regurgitation during bicycle exercise in patients with heart failure. J Am Coll Cardiol 2001;38:1685–1692. 69. Hasuda T, Okano Y, Yoshioka T, Nakanishi N, Shimizu M. Pulmonary pressure-flow relation as a determinant factor of exercise capacity and symptoms in patients with regurgitant valvular heart disease. Int J Cardiol 2005;99:403–407. 70. Pie ´rard LA, Lancellotti P. The role of ischaemic mitral regurgitation in the pathogenesis of acute pulmonary edema. N Engl J Med 2004;351:21–28. 71. Lancellotti P, Ge ´rard PL, Pie ´rard LA. Long-term outcome of patients with heart failure and dynamic functional mitral regurgitation. Eur Heart J 2005;26:1528–1532. Downloaded from by guest on October 15, 2014 47. Naughton MT, Liu PP, Bernard DC, Goldstein RS, Bradley TD. Treatment of congestive heart failure and Cheyne-Stokes respiration during sleep by continuous positive airway pressure. Am J Respir Crit Care Med 1995; 151:92–97. 48. Naughton MT, Benard DC, Liu PP, Rutherford R, Rankin F, Bradley TD. Effect of nasal CPAP on sympathetic activity in patients with heart failure and central sleep apnea. Am J Respir Crit Care Med 1995; 152:473–479. 49. Belardinelli R, Georgiou D, Purcaro A. Low dose dobutamine echocardiography predicts improvement in functional capacity after exercise training in patients with ischaemic cardiomyopathy: prognostic implication. J Am Coll Cardiol 1998;31:1027–1034. 50. Davey P, Meyer T, Coats A, Adamopoulos S, Casadei B, Conway J, Sleight P. Ventilation in chronic heart failure: effects of physical training. Br Heart J 1992;68:473–477. 51. Adamopoulos S, Coats AJ, Brunotte F, Arnolda L, Meyer T, Thompson CH, Dunn JF, Stratton J, Kemp GJ, Radda GK. Physical training improves skeletal muscle metabolic abnormalities in patients with chronic heart failure. J Am Coll Cardiol 1993;23:1101–1106. 52. Weber KT, Szidon JP. Exertional dyspnea. In: Weber KT, Janicky JS, eds. Cardiopulmonary Exercise Testing. Philadelphia, PA: WB Saunders; 1986. p.299. 53. Kremser CB, O’Toole MF, Leef AR. Oscillatory hyperventilation in severe congestive heart failure secondary to idiopathic cardiomyopathy or to ischaemic cardiomyopathy. Am J Cardiol 1987;5:900–905. 54. Leite JJ, Mansur AJ, de Freitas HF, Chizola PR, Bocchi EA, Terra-Filho M, Neder JA, Lorenzi-Filho G. Periodic breathing during incremental exercise predicts mortality in patients with chronic heart failure evaluated for cardiac transplantation. J Am Coll Cardiol 2003;41:2175–2181. 55. Lahiri S, Hsiao C, Zhang R, Mokashi A, Nichino T. Peripheral chemoreceptors in respiratory oscillations. J Appl Physiol 1985;58:1901–1908. 56. Ponikowski P, Anker SD, Chua TP, Francis D, Banasiak W, Poole-Wilson PA, Coats AJ, Piepoli M. Oscillatory breathing patterns during wakefulness in patients with chronic heart failure. Circulation 1999;100:2418–2424. 57. Hall MJ, Xie A, Rutherford R, Ando S, Floras JS, Bradley TD. Cycle length of periodic breathing in patients with and without congestive heart failure. Am J Respir Crit Care Med 1996;154:376–381. 58. Ribeiro JP, Knutzen A, Rocco MB, Hartley I, Colucci WS. Periodic breathing during exercise in severe heart failure: reversal with milrinone or cardiac transplantation. Chest 1987;92:555–556. G. Tumminello et al.








© Copyright 2025